Embed Size (px)
Citation preview

Bridging Clinic and Community
presented by
Consor&um for Older Adult Wellness

• Private, non-‐profit organiza1on since 2007 • Partners with over 80 statewide partners
• FQHC, PCP, Centura, Behavioral Health • Trains and implements evidence-‐based programs
with 150 leaders • Stanford model for self-‐management of chronic
condi1ons • Na1onal Diabetes Preven1on Program

Making Sense of Healthcare Transforma1on
ACA: Affordable Care Act ACO: Accountable Care Organiza1on
RCCO: Regional Care Coordina1ng Organiza1on
PMPM: Per Member Per Month
PPPM: Per Person Per Month
ROI: Return on Investment
Payment Reform
Bundling
Care Transi1ons
Dual Eligibles
Care Coordina1on
PCMH:
Pa>ent Centered Care Pa>ent Centered Medical Home
Pa>ent Centered Medical Neighborhood

2014 NCQA MUST PASS Cer1fica1on Process
• PCMH 1, Element A: Pa1ent-‐Centered Appointment Access.
• PCMH 2, Element D: The Prac1ce Team. • PCMH 3, Element D: Use Data for Popula1on
Management. • PCMH 4, Element B: Care Planning and Self-‐Care
Support. • PCMH 5, Element B: Referral Tracking and Follow-‐Up. • PCMH 6, Element D: Implement Con1nuous Quality
Improvement.

Self-‐Management
For our purposes today: Self-‐management is what I do, or do not do, when I am not with my health care
provider.

Engaging the individual is the best way
to successfully impact clinical outcomes…
as opposed to process measures.

Self-‐Management Support
For our purposes today: Self-‐management support is how the community-‐based organiza1on, the prac1ce, and the health system, can support me in making be[er choices.

Steps to Implemen1ng Self-‐Management Support
Use the 3 measures of READINESS
• Community Partner Readiness • Prac1ce Readiness • Pa1ent Readiness

1. The Community Partner Evaluate your own READINESS
• COAW Program Coordinators working with local partners
• Statewide network of trained leaders in CDSMP/NDPP
• Funding opportuni1es • Mechanism (CRDS) for tracking referrals and communica1on log
• Staff in-‐services, i.e. messaging, pa1ent readiness • Ongoing support/problem-‐solving

10
Improving the lives of 10 million older adults by 2020 © 2015 National Council on Aging
Examples of SM Support to Clinic
• Messaging-‐ MA Guide
• Engaging Pa1ents-‐ real and perceived barriers • How to Refer vs Recommend • Strategies for Improving Communica1ons-‐ get
permission, cultural competency, Mo1va1onal Interviewing
• Self-‐Management Support-‐ barriers, pa1ent willingness, resources
• Basics of Goal Sebng

2. The Clinical Partner Evaluate the Prac1ce READINESS
• Gebng Started and Introduc1ons • Establish a Rela1onship • Prac1ce Readiness/Buy-‐in • Engage En1re Care Team • Iden1fy Clinical Leader/ Champion • Review Quick Basics on CDSMP/NDPP

The Clinical Partner Evaluate the Prac1ce READINESS
• Move Beyond Assump1ons • Promote Referrals vs Recommenda1ons
• Time and Money Cost • Set Clinic Goals (Use self-‐management tools)
– Ac1on Plans – Brainstorm – Decision-‐making – Problem Solving

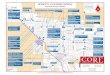
Front Desk
MA Interac>ons
Provider Time
Document
Ø Is there a form showing self-‐management opportuni1es?
Ø Posi1ve conversa1ons, sebng the stage for ac1on planning, or introducing the plan
Ø Who does the char1ng? Ø Who gives the pa1ent the copy of their goal ? Ø Referrals? Ø Logs, brochures, back-‐up info?
Check out
Ø Discuss the plan or confirm the plan Ø Reinforce the importance of sebng do-‐able plans Ø Reinforce the importance of pa1ent involvement Ø Referrals
Clinical workflow example

3. The Pa1ent Evaluate the Pa1ent READINESS
Not at all Confident
1
¡
2
¡
3
¡
4
¡
5
¡
6
¡
7
¡
8
¡
9
¡
10
¡
Totally Confident
Not at all Confident
1
¡
2
¡
3
¡
4
¡
5
¡
6
¡
7
¡
8
¡
9
¡
10
¡
Totally Confident
Sample Questions: 2.1 How confident are you that you can keep the fatigue caused by your
condition from interfering with the things you want to do? 2.2 How confident are you that you can keep the physical discomfort or
pain of your condition from interfering with the things you want to do?

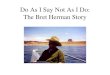
Provider introduces CDSMP/DPP opportunity to
pa1ent.
Pa1ent agrees and signs referral form.
COAW and clinic meet to discuss self-‐
management.
Referral form sent to COAW -‐HIPAA compliant.
COAW Coordinator contacts referred pa1ent and enrolls
in class. COAW communicates with prac1ce weekly regarding
pa1ents who decline scheduling for class.
Pa1ent a[ends CDSMP/DPP.
As part of the CDSMP/DPP program, pa1ent writes a le[er to
Provider describing what he/she has
learned.
COAW mails pa1ent le[ers to Provider with program explana1on.
Provider uses le[er for follow-‐up with pa1ent in self-‐management.
Referral Process

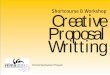
Referral Form

Provider introduces CDSMP/DPP opportunity to
pa1ent.
Pa1ent agrees and signs referral form.
COAW and clinic meet to discuss self-‐
management.
Referral form sent to COAW-‐HIPAA compliant.
COAW Coordinator contacts referred pa1ent and enrolls
in class. COAW communicates with prac1ce weekly regarding
pa1ents who decline scheduling for class.
Pa1ent a[ends CDSMP/DPP.
As part of the CDSMP/DPP program, pa1ent writes a le[er to
Provider describing what he/she has
learned.
COAW mails pa1ent le[ers to Provider with program explana1on.
Provider uses le[er for follow-‐up with pa1ent in self-‐management.
Referral Process


Provider introduces CDSMP/DPP opportunity to
pa1ent.
Pa1ent agrees and signs referral form.
COAW and clinic meet to discuss self-‐
management.
Referral form sent to COAW-‐ HIPAA compliant.
COAW Coordinator contacts referred pa1ent and enrolls
in class. COAW communicates with prac1ce weekly regarding
pa1ents who decline scheduling for class.
Pa1ent a[ends CDSMP/DPP.
As part of the CDSMP program, pa1ent writes a le[er to
Provider describing what he/she has
learned.
COAW mails pa1ent le[ers to Provides with program explana1on.
Provider uses le[er for follow-‐up with pa1ent in self-‐management.
Referral Process


Provider introduces CDSMP/DPP opportunity to
pa1ent.
Pa1ent agrees and signs referral form.
COAW and clinic meet to discuss self-‐
management.
Referral form sent to COAW-‐ HIPAA compliant.
COAW Coordinator contacts referred pa1ent and enrolls
in class. COAW communicates with prac1ce weekly regarding
pa1ents who decline scheduling for class.
Pa1ent a[ends CDSMP/DPP.
As part of the CDSMP/DPP program, pa1ent writes a le[er to
Provider describing what he/she has
learned.
COAW mails pa1ent le[ers to Provider with program explana1on.
Provider uses le[er for follow-‐up with pa1ent in self-‐management.
Referral Process


Provider introduces CDSMP/DPP opportunity to
pa1ent.
Pa1ent agrees and signs referral form.
COAW and clinic meet to discuss self-‐
management.
Referral form sent to COAW-‐ HIPAA compliant.
COAW Coordinator contacts referred pa1ent and enrolls
in class. COAW communicates with prac1ce weekly regarding
pa1ents who decline scheduling for class.
Pa1ent a[ends CDSMP/NDPP.
As part of the CDSMP/NDPP program, pa1ent
writes a le[er to Provider describing what he/she has
learned.
COAW mails pa1ent le[ers to Provider with program explana1on.
Provider uses le[er for follow-‐up with pa1ent in self-‐management.
Referral Process

My Name___ Mary Smith_____________ Today’s Date__ January 8, 2012_____
Dear Health Care Providers,
I wanted to let you know that I have been attending the Healthier Living Colorado™ class to help me better manage my own health. Today we are in our final class of the 6 weekly sessions and we are sending you our thoughts about our chronic conditions, taking care of ourselves, and what we want our Health Care Providers to know about what we are learning and doing. What I have learned about my health is: This isn’t going to go away just because I take a pill three times a day. I can make some changes in how I deal with the pain. Eating a few more fruits has helped my digestion. I didn’t know that my chronic condition was affected by: Worrying about what I can’t do won’t help me any. I need to fix my sights on
what I enjoy doing. I am working on being more positive. It has been nice to
talk with others with similar concerns.
The things that have helped me the most to manage my chronic conditions are: Exercising a little more has helped my knees. I am going to keep with it and
maybe take a water exercise class. I’ve been using a pill box so I keep track of
when I am taking the pills better—I didn’t know it would hurt me to skip some.
My Action Plan for the next six months is: Long term goal: This is my life and I want to stay as healthy as I can for as long as I can. I want to lower my blood pressure so I can be here to see my grandkids graduate from college Specific action step: Walk with a neighbor to the library and back.
How much/often? 3 times a week When? Monday, Wednesday and Saturday
Confidence Level (0-‐10): 9
COAW will forward this letter to your provider listed below: My health care provider’s name and address is: Dr. Smart 1234 Main St. Denver 80202
Consortium for Older Adult Wellness 2575 S. Wadsworth Blvd. Lakewood, CO 80227 888-‐900-‐COAW(2629) Fax: 303-‐984-‐5962 [email protected]

Provider introduces CDSMP/DPP opportunity to
pa1ent.
Pa1ent agrees and signs referral form.
COAW and clinic meet to discuss self-‐
management.
Referral form sent to COAW-‐ HIPAA compliant.
COAW Coordinator contacts referred pa1ent and enrolls
in class. COAW communicates with prac1ce weekly regarding
pa1ents who decline scheduling for class.
Pa1ent a[ends CDSMP/DPP.
As part of the CDSMP/DPP program, pa1ent writes a le[er to
Provider describing what he/she has
learned.
COAW mails pa1ent le[ers to Provider with program explana1on.
Provider uses le[er for follow-‐up with pa1ent in self-‐management.
Referral Process

• 5-‐year program/16 workshops • 6 trained staff/4 clinics • Quarterly mee1ngs/Pre & Post
Confidence Survey • “Improved confidence in taking
medica1ons” • New ac1vi1es: walking, biking, new
friends, lose weight • 2015 Award-‐ Outstanding
Prac>ce
University Family Medicine
University of Colorado
Health

Workshop Wizard • Organize like a whiz with a Centralized Referral System • Soiware as a Service • Developed based on specific needs of implemen1ng evidence based programs

Provider introduces CDSMP/DPP opportunity to
pa1ent.
Pa1ent agrees and signs referral form.
COAW and clinic meet to discuss self-‐management.
Referral form sent to COAW -‐HIPAA compliant.
COAW Coordinator contacts referred
pa1ent and enrolls in class.
COAW communicates with prac1ce weekly regarding pa1ents who decline scheduling for class.
Pa1ent a[ends CDSMP/DPP.
As part of the CDSMP/DPP program, pa1ent writes a le[er to
Provider describing what he/she has learned.
COAW mails pa1ent le[ers to Provider with program explana1on.
Provider uses le[er for follow-‐up with pa1ent in self-‐management.

Provider introduces CDSMP/DPP opportunity to
pa1ent.
Pa1ent agrees and signs referral form.
COAW and clinic meet to discuss self-‐
management.
Referral form sent to COAW -‐HIPAA compliant.
COAW Coordinator contacts referred pa1ent and enrolls
in class. COAW communicates with prac1ce weekly regarding pa1ents who decline scheduling for class.
Pa1ent a[ends CDSMP/DPP.
As part of the CDSMP/DPP program, pa1ent writes a le[er to
Provider describing what he/she has
learned.
COAW mails pa1ent le[ers to Provider with program explana1on.
Provider uses le[er for follow-‐up with pa1ent in self-‐management.

Provider introduces CDSMP/DPP opportunity to
pa1ent.
Pa1ent agrees and signs referral form.
COAW and clinic meet to discuss self-‐
management.
Referral form sent to COAW -‐HIPAA compliant.
COAW Coordinator contacts referred pa1ent and enrolls
in class. COAW communicates with prac1ce weekly regarding pa1ents who decline scheduling for class.
Pa1ent a[ends CDSMP/DPP.
As part of the CDSMP/DPP program, pa1ent writes a le[er to
Provider describing what he/she has
learned.
COAW mails pa1ent le[ers to Provider with program explana1on.
Provider uses le[er for follow-‐up with pa1ent in self-‐management.

Provider introduces CDSMP/DPP opportunity to
pa1ent.
Pa1ent agrees and signs referral
form.
COAW and clinic meet to discuss self-‐
management.
Referral form sent to COAW -‐HIPAA compliant.
COAW Coordinator contacts referred pa1ent and enrolls
in class. COAW communicates with prac1ce weekly regarding pa1ents who decline scheduling for class.
Pa1ent a[ends CDSMP/DPP.
As part of the CDSMP/DPP program, pa1ent writes a le[er to Provider describing
what he/she has learned.
COAW mails pa1ent le[ers to Provider with program explana1on.
Provider uses le[er for follow-‐up with pa1ent in
self-‐management.

Provider introduces CDSMP/DPP opportunity to
pa1ent.
Pa1ent agrees and signs referral
form.
COAW and clinic meet to discuss
self-‐management.
Referral form sent to COAW -‐HIPAA compliant.
COAW Coordinator contacts referred pa1ent and enrolls
in class. COAW communicates with prac1ce weekly regarding pa1ents who decline scheduling for class.
Pa1ent a[ends CDSMP/DPP.
As part of the CDSMP/DPP
program, pa1ent writes a le[er to
Provider describing what he/she has
learned.
COAW mails pa1ent le[ers to Provider with program explana1on.
Provider uses le[er for follow-‐up with pa1ent
in self-‐management.

Provider introduces CDSMP/DPP opportunity to
pa1ent.
Pa1ent agrees and signs referral form.
COAW and clinic meet to discuss self-‐management.
Referral form sent to COAW -‐HIPAA compliant.
COAW Coordinator contacts referred
pa1ent and enrolls in class.
COAW communicates with prac1ce weekly regarding
pa1ents who decline scheduling for class.
Pa1ent a[ends CDSMP/DPP.
As part of the CDSMP/DPP program, pa1ent writes a le[er to
Provider describing what he/she has
learned.
COAW mails pa1ent le[ers to Provider with program explana1on.
Provider uses le[er for follow-‐up with pa1ent in self-‐
management.
My Name___ Mary Smith_____________ Today’s Date__ January 8, 2012_____
Dear Health Care Providers,
I wanted to let you know that I have been attending the Healthier Living Colorado™ class to help me better manage my own health. Today we are in our final class of the 6 weekly sessions and we are sending you our thoughts about our chronic conditions, taking care of ourselves, and what we want our Health Care Providers to know about what we are learning and doing. What I have learned about my health is: This isn’t going to go away just because I take a pill three times a day. I can make some changes in how I deal with the pain. Eating a few more fruits has helped my digestion. I didn’t know that my chronic condition was affected by: Worrying about what I can’t do won’t help me any. I need to fix my sights on
what I enjoy doing. I am working on being more positive. It has been nice to
talk with others with similar concerns.
The things that have helped me the most to manage my chronic conditions are: Exercising a little more has helped my knees. I am going to keep with it and
maybe take a water exercise class. I’ve been using a pill box so I keep track of
when I am taking the pills better—I didn’t know it would hurt me to skip some.
My Action Plan for the next six months is: Long term goal: This is my life and I want to stay as healthy as I can for as long as I can. I want to lower my blood pressure so I can be here to see my grandkids graduate from college Specific action step: Walk with a neighbor to the library and back.
How much/often? 3 times a week When? Monday, Wednesday and Saturday
Confidence Level (0-‐10): 9
COAW will forward this letter to your provider listed below: My health care provider’s name and address is: Dr. Smart 1234 Main St. Denver 80202
Consortium for Older Adult Wellness 2575 S. Wadsworth Blvd. Lakewood, CO 80227 888-‐900-‐COAW(2629) Fax: 303-‐984-‐5962 [email protected]

Closing the Loop

• 5-‐year program/all pa1ent referrals to Tomando and TCD
• 10 workshops/13 average a[endance/other sites
• 10 bilingual Health Educators • 4 FQHC clinic sites/ 1 Health
Ed Manager • Fully sustainable model

Goals for New Mexico DOH
• Establish EBP-‐Centralized Referral & Data System • Accommodate Provider and Self-‐referrals
English and Spanish
• HIPAA compliant phone, fax, website and EHR link • Referral follow-‐up includes 3 pa1ent contacts, class
enrollment, FAQ by COAW staff • Develop statewide strategic plan for clinical and
community partnerships

Ques1ons?