Embed Size (px)
Citation preview
Intensive and Critical Care Nursing (2004) 20, 133—143
ORIGINAL ARTICLE
Bridging the gap between the intensive care unitand general wards—the ICU Liaison Nurse
Anna Green*, Liz Edmonds
Western Hospital, Gordon Street, Footscray, Vic. 3011, Australia
Accepted 23 February 2004
KEYWORDSICU discharge;Practice innovation;Advanced practice;Nurse practitioner;Expanded role
Summary The acute care system in our public hospitals has seen an increase in acuityfor multiday patients with associated pressure on access to the intensive care unit(ICU) beds for both elective and emergency patients.When an ICU bed has not been available at this hospital, it has resulted in elective
surgery being cancelled and/or emergency patients requiring an ICU admission beingtransferred to other hospitals. Apart from the problems either of these situationscan cause to patients and their families, both government and hospital managementsexpect that access to an ICU (or other) bed will be available for patients in ourcommunity who require this level of care.To maximise access to our ICU beds it was necessary to ensure that length of stay
(LOS) in ICU was kept to the minimum required for each individual patient and thatre-admission rates to ICU for preventable complications were reduced.This paper relates our experience of developing and introducing an advanced prac-
tice nursing position (the ICU Liaison Nurse) in 1998, to oversee the transition ofpatients discharged from ICU to the general wards. Between 1997 and 2002 with thedevelopment of the ICU Liaison Nurse (ICU LN) post, medical readmissions to ICU werereduced from 2.3 to 0.5%. It is now 5 years since the position was introduced and therole has evolved over this time so that today the ICU LN not only bridges the gapbetween ICU and ward-based care, but when necessary can be involved in the careof patients on the ward whose condition has deteriorated to the point where transferinto ICU may be necessary.© 2004 Elsevier Ltd. All rights reserved.
Background
Western Hospital is a 310-bed teaching hospitalaffiliated with Melbourne University and is one ofthree hospitals and two nursing homes situated inMelbourne’s western suburbs that form the West-ern Health Service.
*Corresponding author. Tel.: +61-3-8345-6588;fax: +61-3-8345-6336.
E-mail address: [email protected] (A. Green).
The Western Health ICU is currently an 11-bedadult unit which accepts patients from any of theemergency departments of the three hospitalswithin Western Health which treat over 100,000emergency presentations annually. A busy gen-eral and specialty elective surgery service also hasexpectations that elective patients requiring ICUwill gain access to an ICU bed post-surgery whenrequired.In late 1996 frustration was expressed by the Di-
rector of ICU regarding the high number of emer-
0964-3397/$ — see front matter © 2004 Elsevier Ltd. All rights reserved.doi:10.1016/j.iccn.2004.02.007

134 A. Green, L. Edmonds
gency patients requiring ICU who were transferredto other hospitals and the inability of ICU to acceptall booked elective surgery patients who requiredsome time in ICU.Timely access to ICU beds was hindered and LOS
for ICU patients was often longer than necessarybecause ICU patients who could be transferredto the wards still required close observation andcomparatively more complex care than routinelyprovided at ward level. Experience had shown thatre-admission rates to ICU for patients with pre-ventable complications were high if patients weredischarged earlier–—particularly between Friday af-ternoons and Monday mornings when medical andallied health staffing levels were less than thoseprovided Monday to Friday.The major reasons given by the ICU Director at
Western Hospital, for the prolonged LOS in ICUwere:
• Fluid and electrolyte management;• Respiratory care, particularly tracheostomy care;• Complex drug therapies difficult for ward-basedstaff to manage;
• Pain management.
The Director of ICU believed that both LOS in ICUand re-admission rates to ICU could be reduced ifan experienced ICU nurse were available to supportward-based staff in managing this group of patientswhile the patients still had complex care needs.The role of the ICU Liaison Nurse (ICU LN) was de-
signed to facilitate the transition from the ICU tothe general wards for patients and their families,and to act as a resource for junior medical staff andward-based nurses while they provided care for pa-tients who still had complex needs. The focus ofthe ICU LN is on collaboration with the multidisci-plinary team to ensure appropriate and timely man-agement of acutely ill patients, including, timelyadmission of patients into ICU. The initial proposalto provide 24-h ICU LN cover over the 7 days of theweek was considered prohibitive, and in 1998 ap-proval was finally given to provide an ICU LN for 10 hper day, 7 days per week.This article will explore the evolution of the role
of the ICU LN since its inception in 1998 up to thepresent day.
Setting up the post
Literature review
Initially it is worth considering the implementationof similar roles and/or functions to that of the ICU
LN role. An analysis of available literature indicatesthat;
• In 1995, the American Nurses Association (ANA)and American Association of Critical Care Nurses(AACCN) officially recognised the role of theAcute Care Nurse Practitioner (King et al., 1996).Also in 1995 the first national certification ex-amination for nurses practicing in the AcuteCare Nurse Practitioner (ACNP) role was offered(Kleinpell-Nowell, 1999). These advanced prac-tice nurses provide care to complex, acutely illpatients, in a variety of care settings such asCoronary Care Units, intensive care units andEmergency Departments. The focus of the ACNPincludes advanced physical assessment, diagnos-tic reasoning, therapeutic management and inte-gration of care across the acute care continuum(King, 2001; Kleinpell, 1997; Piano et al., 1996).
• In 1995 the Royal Melbourne Hospital in Victoria,Australia developed an ICU Clinical Nurse Consul-tant (CNC) role. This position had the dual re-sponsibility of psycho-social support for patients,staff and others whilst in ICU as well as reviewingthese patients when discharged to the ward. Tomeet the dual functions of this role, the positionwas filled by a qualified Intensive Care nurse witha degree in psychology (Schlicht, 1995).
• In 2001 the United Kingdom introduced Outreachteams in an attempt to improve care for acutelyill patients in the ward environment and to fa-cilitate more timely admission to critical care(Anderson et al., 2002; Coombs and Dillon, 2002).
• In addition to the above nursing led services therehas also been the development of the medicalemergency teams (MET) in Sydney, Australia whorespond to early adverse clinical signs in an at-tempt to identify at risk patients for cardiopul-monary arrest (Buist et al., 2002; Hillman et al.,1996).
• In February 2001 the Alfred Hospital in Mel-bourne, Australia introduced the ICU LN positionbased on the Western Hospital model (Barbettiand Choate, 2002).
The Western Health ICU LN model would appearto function in a similar way to the USA ACNP model.Unlike the USA model however, the Western HealthICU LN has responsibilities for patients outside ofthe critical care areas, i.e. functions from the timea patient is ready for discharge from ICU to the gen-eral wards (and conversely from the general wardsinto ICU) and works across all medical/surgical spe-cialties in an advisory and supportive role for theprovision of care to acutely ill patients with com-plex care needs.

Bridging the gap between the intensive care unit and general wards 135
Role requirements
Once funding was approved for the position, aposition guide was developed and recruitment un-dertaken. An essential requirement for the posi-tion was that applicants had to have a formal ICUpost-basic qualification with a minimum of 5 yearsclinical experience in an ICU. As this was a newposition with a degree of autonomy of practice,the successful applicants had to have confidence intheir abilities and knowledge and be self-directedin the practice of case-managing patients dis-charged from ICU within what was a traditionalward-based medical model.Initially, the ICU LN reported to a divisional man-
ager who had responsibility for ICU. Subsequently,this was placed within the Education Centre to gainmore acceptance of the role by ward staff who nowviewed it as separate from ICU. This proved to be amistake as it created confusion in the minds of wardstaff who were not sure if the ICU LNs were NurseEducators, and in the eyes of other Nurse Educatorswho saw the ICU LNs as ‘another pair of hands’ asfar as education responsibilities were concerned.A year after the position commenced, the deci-
sion to place the ICU LNs within a clinical divisionof the organisational structure was ratified and thisis where it still lies.
Consultations with other specialists
The first few weeks after commencement of therole was used as a preparatory and introductoryphase. This enabled the two nurses employed intothe position to discuss and decide short and longterm goals (including the way in which they wouldfunction), establish data collection tools, set up arudimentary data base and introduce the role tohospital clinical staff.Introducing the role to the clinical staff proved
the most challenging as unlike other traditional ad-vanced practice nursing roles (e.g. Diabetic Edu-cator, Wound Care Consultant, Stomal Therapist,etc.) which are established posts well understoodby staff, this role was new, and staff did not haveany pre-conceived knowledge of its function.During this introductory phase the ICU LNs intro-
duced themselves and their role to all of the NurseUnit Managers and Allied Health Managers. Theyorganised appropriate times to meet with othernurses/allied health staff to educate them aboutthe role and how it would assist them in providingcare to acutely ill patients. Posters that outlinedwhen and how to contact the ICU LNs were de-veloped and distributed around the ward areasand formal presentations arranged to target junior
medical staff. Poor attendance by medical staff atthese sessions resulted in their almost completelack of awareness and understanding of the role.
Assessing issues on the ward and thereforeneed
Prior to the introduction of the ICU LN the practicehad been for ICU patients to be discharged to theirspecialty ward regardless of the workload and/orexpertise on the ward at that time, or if a bed wasnot available on that ward, discharge to any wardwhere a bed was available. This method of alloca-tion to a ward often resulted in poor outcomes forpatients (including re-admission to ICU), becausethe local knowledge of any given ward’s situation inregard toworkload or clinical expertise was not con-sidered when discharging the patient from ICU. Intheir hospital-wide role, the ICU LNs became rapidlyaware of local practices in relation to fluid regimes,drug infusions and other therapies and came to un-derstand nursing workload pressures, staff-mix andclinical expertise availability on any given ward.
Implementing the ICU LN role
Explicit role clarity
The ICU LNs decided that attendance at the morn-ing multidisciplinary ICU ward round daily wouldenable them to identify those patients due for dis-charge to a ward. The purpose of attending theICU ward round rapidly progressed to active par-ticipation in the decision-making process of whenpatients could be discharged to a ward and consid-eration of which wards would be able to providethe care that individual patients required at thetime of discharge from ICU.The ICU LNs assess all patients prior to transfer
from ICU and at times will recommend that somepatients should remain in ICU while at other timesthey will indicate that some patients not initiallyconsidered ready for transfer, can be safely trans-ferred to a ward. The confidence and accuracy ofthe ICU LNs in this process has progressed not onlybecause of their experience in case-managing thesepatients in the ward and their local knowledge ofthe wards, but also because of their method ofpatient assessment.Early on the ICU LNs developed a nurse-scoring
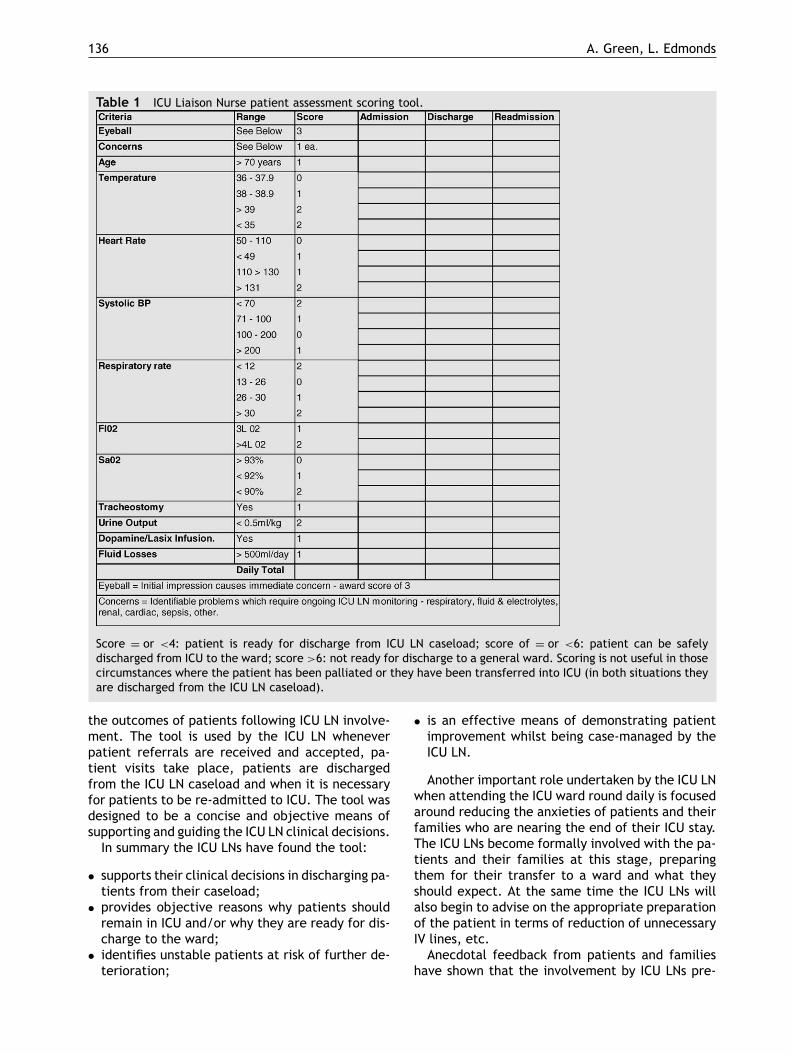
patient assessment tool (Table 1) to provide anobjective means of determining the patient’s sta-tus. This tool is used to identify discharge criteriafor patients from ICU, discharge from the ICU LNcaseload once on the ward, and to compare with
136 A. Green, L. Edmonds
Table 1 ICU Liaison Nurse patient assessment scoring tool.
Score = or <4: patient is ready for discharge from ICU LN caseload; score of = or <6: patient can be safelydischarged from ICU to the ward; score >6: not ready for discharge to a general ward. Scoring is not useful in thosecircumstances where the patient has been palliated or they have been transferred into ICU (in both situations theyare discharged from the ICU LN caseload).
the outcomes of patients following ICU LN involve-ment. The tool is used by the ICU LN wheneverpatient referrals are received and accepted, pa-tient visits take place, patients are dischargedfrom the ICU LN caseload and when it is necessaryfor patients to be re-admitted to ICU. The tool wasdesigned to be a concise and objective means ofsupporting and guiding the ICU LN clinical decisions.In summary the ICU LNs have found the tool:
• supports their clinical decisions in discharging pa-tients from their caseload;
• provides objective reasons why patients shouldremain in ICU and/or why they are ready for dis-charge to the ward;
• identifies unstable patients at risk of further de-terioration;
• is an effective means of demonstrating patientimprovement whilst being case-managed by theICU LN.
Another important role undertaken by the ICU LNwhen attending the ICU ward round daily is focusedaround reducing the anxieties of patients and theirfamilies who are nearing the end of their ICU stay.The ICU LNs become formally involved with the pa-tients and their families at this stage, preparingthem for their transfer to a ward and what theyshould expect. At the same time the ICU LNs willalso begin to advise on the appropriate preparationof the patient in terms of reduction of unnecessaryIV lines, etc.Anecdotal feedback from patients and families
have shown that the involvement by ICU LNs pre-

Bridging the gap between the intensive care unit and general wards 137
and post-ICU transfer to the wards is a major fac-tor in reducing relocation stress both by address-ing their specific concerns regarding moving to award and in answering questions about their stayin ICU.On completion of the ICU ward round, patients on
the ICU LN caseload who are already on the wardsare reviewed. The number of reviews a patient mayrequire will depend on their complexity and re-sponse to treatment. Typically the review processconsists of the initial pre- and post-ICU dischargevisits, followed by daily morning and evening re-views. On each occasion the ICU Liaison Scoring toolis used as a means of recording objective evidenceas to the patient’s condition.
Building rapport and acceptance levels
The initial visit post-transfer from ICU is importantto allay any anxieties the patient and family mayhave in their new location, and to consult with thenurse caring for the patient to clarify any issuesthey might have regarding the patient’s manage-ment. At this time the ICU LN will draw attentionto any potential problems the patient could en-counter, communicating these also to the nursein charge and the covering medical staff. Lastlyif the patient was transferred to the ward toolate in the day for the parent unit to review, theICU LN will request necessary biochemistry testsfor the morning in time for review by the parentunit.The morning visit by the ICU LN comprises a full
patient assessment to determine the patient’s sta-tus, need for subsequent visits and their frequency.If problems are identified they are addressed at thetime of the visit. If the problems are non-urgentin nature they are discussed with the nurse caringfor the patient so that the parent unit can be in-formed during their morning round. If the problemsare urgent (i.e. have potential to lead to acute de-terioration in the patient’s condition) the ICU LNwill contact the parent unit’s medical staff imme-diately. At this time the ICU LN will discuss assess-ment findings and recommend a management planthat may include initiation of therapeutic changesto medications/IV fluids, radiology or pathology in-vestigations, etc.Assessment findings following each patient visit
by the ICU LN are recorded in the patient’s med-ical record under a distinctive coloured adhesivelabel with the ICU LN title which easily identifiestheir entries. These notes are an important recordregarding the patient assessment, any concernsidentified, treatment recommendations and dis-cussions with medical staff. Included in this docu-
mentation are requests for notification to medicalstaff and the ICU LN regarding reportable obser-vations. The ICU LN records are utilised by themultidisciplinary team in assessing the patient’sprogress and in providing information to nightduty nursing staff when the ICU LN position is notcovered.Despite the educational and promotional activ-
ities undertaken to inform all clinical staff aboutthe new position, in the early days there wereobvious misunderstandings and anxiety about thepurpose of this new position. Ward-based nurseswere most apprehensive thinking that it would re-sult in earlier discharge of ICU patients to the wardswith an associated increase to their already busyworkload.It was more than 3 months after the ICU LN
had begun ‘case-managing’ the ICU patients dis-charged to their wards, before the ward-basednursing staff began to fully understand and ap-preciate the value of the role not only to theirpatients but also to their own practice. This ac-ceptance by nursing staff resulted from increasedexposure to the ICU LNs who they found supportedthem in caring for the complex patients on theirwards.The ward-based nurses also found that the ICU LN
would respond quickly when contacted for advice,and would provide informal education on caring foracutely ill patients or trouble-shooting biomedicalequipment. They appreciated the rapid responseprovided when caring for the acutely unstable pa-tient which at times escalated to the ICU LNs mon-itoring these patients on their ward over severalhours while waiting for an ICU bed to become avail-able.Acceptance by medical staff took much longer
and was inconsistent over the first 18 months to2 years. Perhaps the major turning point towardsacceptance by the medical consultants occurred ata formal presentation by the ICU LNs during ‘GrandRounds’’ where presented data collected over theprevious 2 years demonstrated improved outcomesfor their patients because of ICU LN involvement.What followed the presentation was an intensequestioning period that clarified for all presentwhat the ICU LN role was intended to accomplish.A key point for the consultants was that deteri-oration in their patient’s condition was detectedearlier and referred to the relevant medical staffby the ICU LNs.Today the ICU LNs are considered by medical,
nursing and allied health staff to be a valuable re-source and part of the multidisciplinary team thatprovides care to unstable patients in the ward en-vironment.
138 A. Green, L. Edmonds
Meeting educational needs
Prior to the appointment of the ICU LNs, variationsin nursing expertise across the various wards inhib-ited timely transfers from ICU. A notable exampleof this and the positive influence of the ICU LNs inchanging nursing practice was the provision of careon the wards to patients who have undergone a tra-cheostomy. The only ward with nurses with suffi-cient expertise and confidence to manage these pa-tients was the respiratory ward. This led to patientsstaying longer in ICU until a bed was available onthat ward.Prior to ICU LNs commencing in their role, read-
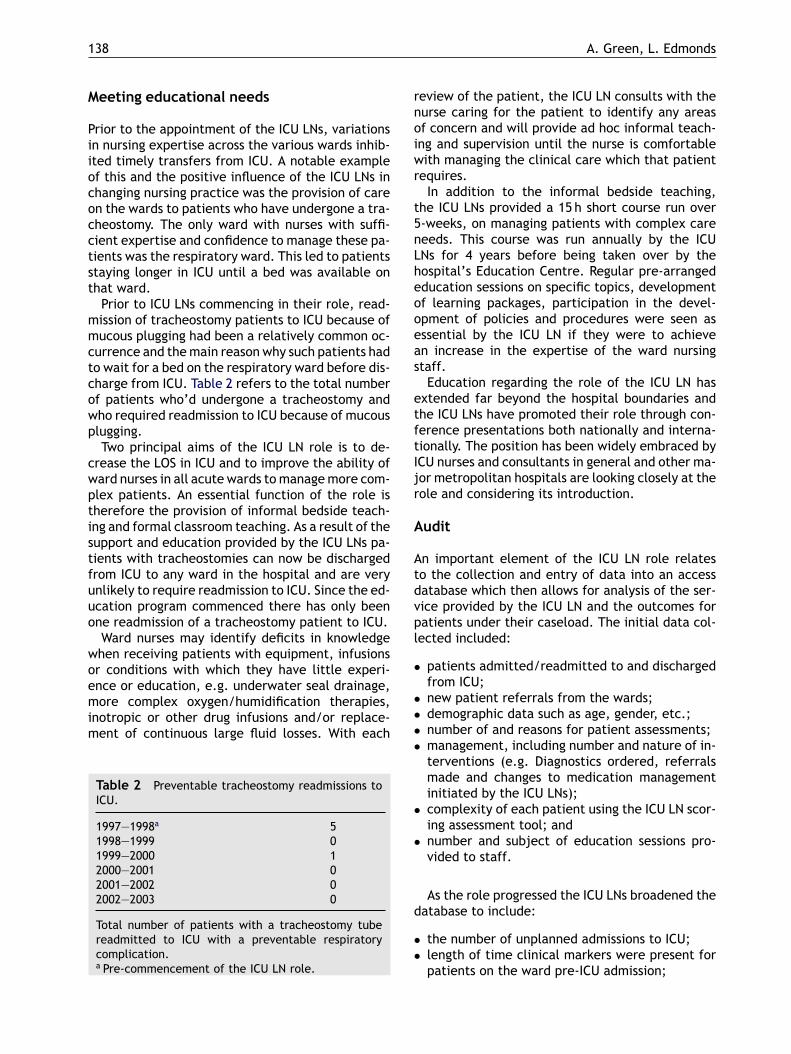
mission of tracheostomy patients to ICU because ofmucous plugging had been a relatively common oc-currence and themain reason why such patients hadto wait for a bed on the respiratory ward before dis-charge from ICU. Table 2 refers to the total numberof patients who’d undergone a tracheostomy andwho required readmission to ICU because of mucousplugging.Two principal aims of the ICU LN role is to de-
crease the LOS in ICU and to improve the ability ofward nurses in all acute wards tomanagemore com-plex patients. An essential function of the role istherefore the provision of informal bedside teach-ing and formal classroom teaching. As a result of thesupport and education provided by the ICU LNs pa-tients with tracheostomies can now be dischargedfrom ICU to any ward in the hospital and are veryunlikely to require readmission to ICU. Since the ed-ucation program commenced there has only beenone readmission of a tracheostomy patient to ICU.Ward nurses may identify deficits in knowledge
when receiving patients with equipment, infusionsor conditions with which they have little experi-ence or education, e.g. underwater seal drainage,more complex oxygen/humidification therapies,inotropic or other drug infusions and/or replace-ment of continuous large fluid losses. With each
Table 2 Preventable tracheostomy readmissions toICU.
1997—1998a 51998—1999 01999—2000 12000—2001 02001—2002 02002—2003 0
Total number of patients with a tracheostomy tubereadmitted to ICU with a preventable respiratorycomplication.a Pre-commencement of the ICU LN role.
review of the patient, the ICU LN consults with thenurse caring for the patient to identify any areasof concern and will provide ad hoc informal teach-ing and supervision until the nurse is comfortablewith managing the clinical care which that patientrequires.In addition to the informal bedside teaching,
the ICU LNs provided a 15 h short course run over5-weeks, on managing patients with complex careneeds. This course was run annually by the ICULNs for 4 years before being taken over by thehospital’s Education Centre. Regular pre-arrangededucation sessions on specific topics, developmentof learning packages, participation in the devel-opment of policies and procedures were seen asessential by the ICU LN if they were to achievean increase in the expertise of the ward nursingstaff.Education regarding the role of the ICU LN has
extended far beyond the hospital boundaries andthe ICU LNs have promoted their role through con-ference presentations both nationally and interna-tionally. The position has been widely embraced byICU nurses and consultants in general and other ma-jor metropolitan hospitals are looking closely at therole and considering its introduction.
Audit
An important element of the ICU LN role relatesto the collection and entry of data into an accessdatabase which then allows for analysis of the ser-vice provided by the ICU LN and the outcomes forpatients under their caseload. The initial data col-lected included:
• patients admitted/readmitted to and dischargedfrom ICU;
• new patient referrals from the wards;• demographic data such as age, gender, etc.;• number of and reasons for patient assessments;• management, including number and nature of in-terventions (e.g. Diagnostics ordered, referralsmade and changes to medication managementinitiated by the ICU LNs);
• complexity of each patient using the ICU LN scor-ing assessment tool; and
• number and subject of education sessions pro-vided to staff.
As the role progressed the ICU LNs broadened thedatabase to include:
• the number of unplanned admissions to ICU;• length of time clinical markers were present forpatients on the ward pre-ICU admission;
Bridging the gap between the intensive care unit and general wards 139
• ICU and hospital length of stay; and• ICU and hospital outcomes (i.e. Discharge desti-nation).
The unplanned admissions into ICU are an or-ganisational key performance indicator that is re-ported monthly to the hospital management teamwith the aim of identifying preventable system fail-ures where process changes can be implemented toaddress these factors.
Effectiveness of the role
Analysis of data collected
Over the 5 years since the ICU LN role was in-troduced, there have been an average of 875discharges from ICU and an average of 105 newreferrals for non-ICU patients have been made tothe ICU LNs each year (total caseload of 980 peryear). On average 3 visits per ICU discharged pa-tient are required before the patient is ready tobe discharged from the ICU LN caseload but thishas ranged between 1 and 40 visits per patient.The average time per patient visit is 30min but thetime can range between 5min and 3 h.Specific problems exhibited by patients during
each visit were identified by the ICU LN and themostcommon problems were respiratory concerns, car-diac/haemodynamic instability, fluid & electrolyteabnormalities and renal failure.The ICU LNs receive referrals for patients whose
condition is causing concern and who have not beenin the ICU unit, i.e. not on the ICU LN caseload(Table 3). The authors believe that the increasingnumber of referrals over the last 2 years is a reflec-tion of several things including:
• widespread knowledge/acceptance of the ICULNs role by all clinical disciplines;
• the ability of ward nurses to manage increasinglycomplex patients;
Table 3 Referrals to the ICU LNs.
Discipline 1998—1999 1999—2000 2000—2001 2001—2002 2002—2003
Medical 19 28 34 55 64Nursing 63 62 38 68 139Allied health 10 1 7 6 23Pain service 0 0 11 10 13
Total 92 91 90 139 239
This table refers to number of non-ICU discharged patients who are referred to the ICU LN because of some concernregarding the patient’s condition.
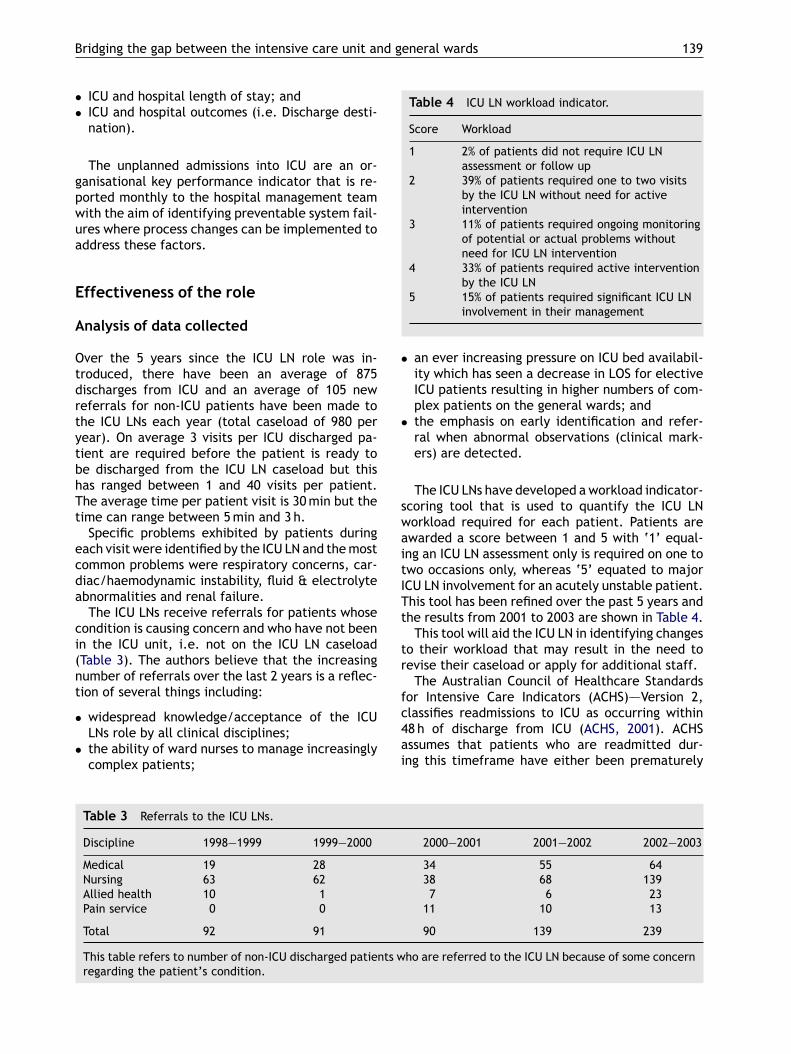
Table 4 ICU LN workload indicator.
Score Workload
1 2% of patients did not require ICU LNassessment or follow up
2 39% of patients required one to two visitsby the ICU LN without need for activeintervention
3 11% of patients required ongoing monitoringof potential or actual problems withoutneed for ICU LN intervention
4 33% of patients required active interventionby the ICU LN
5 15% of patients required significant ICU LNinvolvement in their management
• an ever increasing pressure on ICU bed availabil-ity which has seen a decrease in LOS for electiveICU patients resulting in higher numbers of com-plex patients on the general wards; and
• the emphasis on early identification and refer-ral when abnormal observations (clinical mark-ers) are detected.
The ICU LNs have developed aworkload indicator-scoring tool that is used to quantify the ICU LNworkload required for each patient. Patients areawarded a score between 1 and 5 with ‘1’ equal-ing an ICU LN assessment only is required on one totwo occasions only, whereas ‘5’ equated to majorICU LN involvement for an acutely unstable patient.This tool has been refined over the past 5 years andthe results from 2001 to 2003 are shown in Table 4.This tool will aid the ICU LN in identifying changes
to their workload that may result in the need torevise their caseload or apply for additional staff.The Australian Council of Healthcare Standards
for Intensive Care Indicators (ACHS)–—Version 2,classifies readmissions to ICU as occurring within48 h of discharge from ICU (ACHS, 2001). ACHSassumes that patients who are readmitted dur-ing this timeframe have either been prematurely
140 A. Green, L. Edmonds
discharged from ICU, or are a reflection of inad-equate ward care, and are therefore classified aspreventable.From their long experience with patients pre- and
post-ICU discharge the ICU LNs gained first-handknowledge pertaining to reasons for patient read-mission to ICU and believe that preventable read-missions can occur after the 48 h period. This ledto the ICU LNs re classifying readmissions into thefollowing groups:
• Preventable readmissions as those patients whowere either prematurely discharged from ICU(i.e. Clinical markers present on ICU discharge)or ward management was inadequate or inappro-priate (delay in treatment of clinical markers);
• Non-preventable readmissions included patientswho returned to theatre, had surgical complica-tions or disease progression; and
• Unclassifiable included patients who had a com-bination of the above two groups.
Using this new classification of readmissions theICU LNs found that over the last 5 years only 32% ofall readmissions were preventable (an average of12% within 48 h and an average of 20% after 48 h).Their conclusion is that only a one-third of all read-missions is preventable and that readmission to ICUcan occur at any stage during the patients’ hospitaladmission.To look solely at readmissions as only those which
fall within 48 h does not provide a true representa-tion of a hospital’s readmission rate. Preventablereadmissions to ICU can and do occur at any timewithin a patient’s hospital stay. Evaluation of notonly readmission rates, but also all unplanned ad-missions into ICU from ward areas, including pres-ence of clinical markers is useful, as this can givean indication of less than optimal patient manage-ment from which strategies and process change canbe initiated.
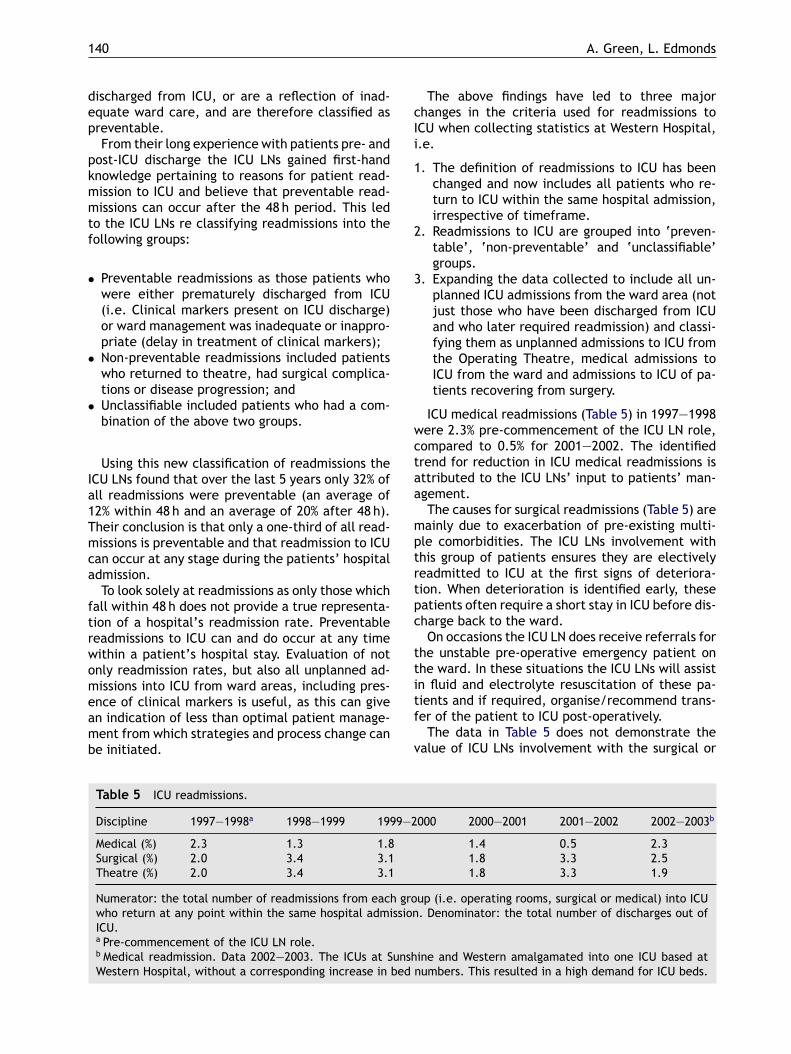
Table 5 ICU readmissions.
Discipline 1997—1998a 1998—1999 1999—2000 2000—2001 2001—2002 2002—2003b
Medical (%) 2.3 1.3 1.8 1.4 0.5 2.3Surgical (%) 2.0 3.4 3.1 1.8 3.3 2.5Theatre (%) 2.0 3.4 3.1 1.8 3.3 1.9
Numerator: the total number of readmissions from each group (i.e. operating rooms, surgical or medical) into ICUwho return at any point within the same hospital admission. Denominator: the total number of discharges out ofICU.a Pre-commencement of the ICU LN role.b Medical readmission. Data 2002—2003. The ICUs at Sunshine and Western amalgamated into one ICU based atWestern Hospital, without a corresponding increase in bed numbers. This resulted in a high demand for ICU beds.
The above findings have led to three majorchanges in the criteria used for readmissions toICU when collecting statistics at Western Hospital,i.e.
1. The definition of readmissions to ICU has beenchanged and now includes all patients who re-turn to ICU within the same hospital admission,irrespective of timeframe.
2. Readmissions to ICU are grouped into ‘preven-table’, ‘non-preventable’ and ‘unclassifiable’groups.
3. Expanding the data collected to include all un-planned ICU admissions from the ward area (notjust those who have been discharged from ICUand who later required readmission) and classi-fying them as unplanned admissions to ICU fromthe Operating Theatre, medical admissions toICU from the ward and admissions to ICU of pa-tients recovering from surgery.
ICU medical readmissions (Table 5) in 1997—1998were 2.3% pre-commencement of the ICU LN role,compared to 0.5% for 2001—2002. The identifiedtrend for reduction in ICU medical readmissions isattributed to the ICU LNs’ input to patients’ man-agement.The causes for surgical readmissions (Table 5) are
mainly due to exacerbation of pre-existing multi-ple comorbidities. The ICU LNs involvement withthis group of patients ensures they are electivelyreadmitted to ICU at the first signs of deteriora-tion. When deterioration is identified early, thesepatients often require a short stay in ICU before dis-charge back to the ward.On occasions the ICU LN does receive referrals for
the unstable pre-operative emergency patient onthe ward. In these situations the ICU LNs will assistin fluid and electrolyte resuscitation of these pa-tients and if required, organise/recommend trans-fer of the patient to ICU post-operatively.The data in Table 5 does not demonstrate the
value of ICU LNs involvement with the surgical or
Bridging the gap between the intensive care unit and general wards 141
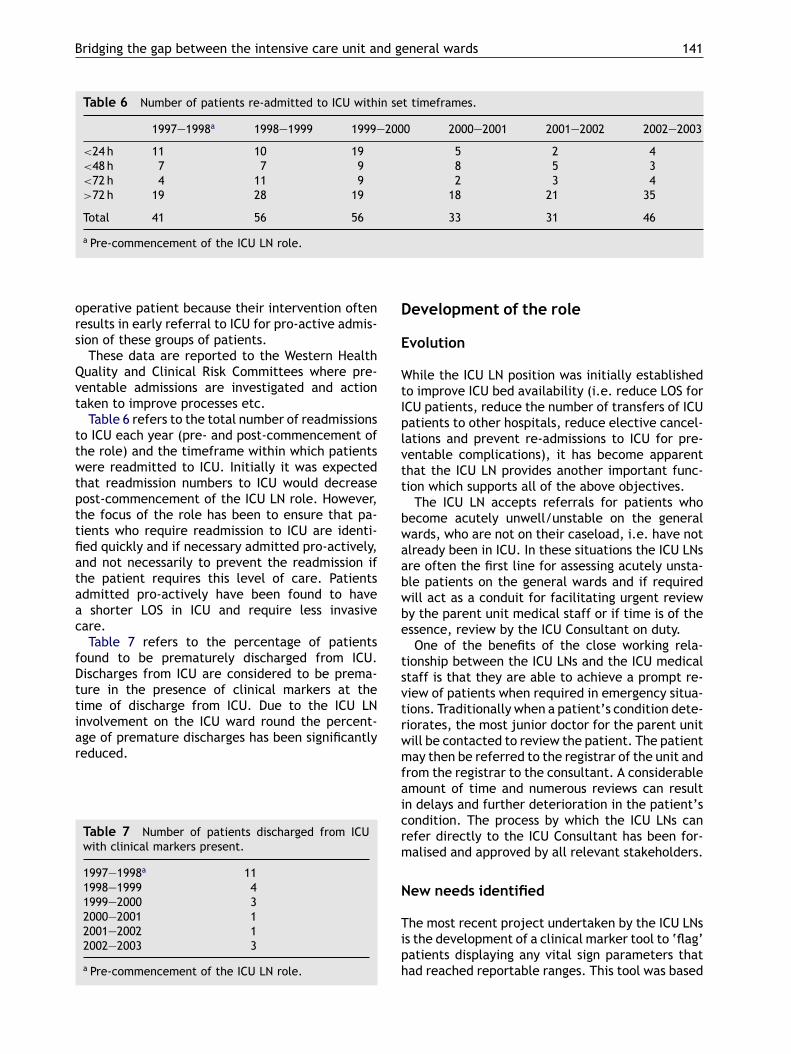
Table 6 Number of patients re-admitted to ICU within set timeframes.
1997—1998a 1998—1999 1999—2000 2000—2001 2001—2002 2002—2003
<24 h 11 10 19 5 2 4<48 h 7 7 9 8 5 3<72 h 4 11 9 2 3 4>72 h 19 28 19 18 21 35
Total 41 56 56 33 31 46
a Pre-commencement of the ICU LN role.
operative patient because their intervention oftenresults in early referral to ICU for pro-active admis-sion of these groups of patients.These data are reported to the Western Health
Quality and Clinical Risk Committees where pre-ventable admissions are investigated and actiontaken to improve processes etc.Table 6 refers to the total number of readmissions
to ICU each year (pre- and post-commencement ofthe role) and the timeframe within which patientswere readmitted to ICU. Initially it was expectedthat readmission numbers to ICU would decreasepost-commencement of the ICU LN role. However,the focus of the role has been to ensure that pa-tients who require readmission to ICU are identi-fied quickly and if necessary admitted pro-actively,and not necessarily to prevent the readmission ifthe patient requires this level of care. Patientsadmitted pro-actively have been found to havea shorter LOS in ICU and require less invasivecare.Table 7 refers to the percentage of patients
found to be prematurely discharged from ICU.Discharges from ICU are considered to be prema-ture in the presence of clinical markers at thetime of discharge from ICU. Due to the ICU LNinvolvement on the ICU ward round the percent-age of premature discharges has been significantlyreduced.
Table 7 Number of patients discharged from ICUwith clinical markers present.
1997—1998a 111998—1999 41999—2000 32000—2001 12001—2002 12002—2003 3
a Pre-commencement of the ICU LN role.
Development of the role
Evolution
While the ICU LN position was initially establishedto improve ICU bed availability (i.e. reduce LOS forICU patients, reduce the number of transfers of ICUpatients to other hospitals, reduce elective cancel-lations and prevent re-admissions to ICU for pre-ventable complications), it has become apparentthat the ICU LN provides another important func-tion which supports all of the above objectives.The ICU LN accepts referrals for patients who
become acutely unwell/unstable on the generalwards, who are not on their caseload, i.e. have notalready been in ICU. In these situations the ICU LNsare often the first line for assessing acutely unsta-ble patients on the general wards and if requiredwill act as a conduit for facilitating urgent reviewby the parent unit medical staff or if time is of theessence, review by the ICU Consultant on duty.One of the benefits of the close working rela-
tionship between the ICU LNs and the ICU medicalstaff is that they are able to achieve a prompt re-view of patients when required in emergency situa-tions. Traditionally when a patient’s condition dete-riorates, the most junior doctor for the parent unitwill be contacted to review the patient. The patientmay then be referred to the registrar of the unit andfrom the registrar to the consultant. A considerableamount of time and numerous reviews can resultin delays and further deterioration in the patient’scondition. The process by which the ICU LNs canrefer directly to the ICU Consultant has been for-malised and approved by all relevant stakeholders.
New needs identified
The most recent project undertaken by the ICU LNsis the development of a clinical marker tool to ‘flag’patients displaying any vital sign parameters thathad reached reportable ranges. This tool was based

142 A. Green, L. Edmonds
on criteria developed for the MET model but mod-ified to capture patients at an even earlier stageof the disease process (Hourihan et al., 1995). Themodifications were made following a 3-month anal-ysis of all unplanned admissions into ICU at West-ern Hospital to see what vital sign abnormalitiespatients displayed prior to their admission to ICU.Review of this data demonstrated that the ‘sudden’deterioration in a patient’s condition and subse-quent transfer to ICU was in fact preceded by manyhours of abnormal observations that had either notresponded to treatment or had not been recognisedfor their significance. All unplanned admissions toICU were found to have had at least one and some-times several of these abnormal observations (clini-cal markers) which included a decrease in consciousstate, systolic blood pressure<90, heart rate>120,respiratory rate >30, O2Sa <90% in oxygen, and uri-nary output <30ml for two consecutive hours.The data clearly supported the view that dete-
rioration was being detected and managed late inthe physiological process where intubation and in-vasive monitoring were more likely to be required.The ICU LNs believed that earlier identification ofthese patients with appropriate intervention wouldhave either prevented the ICU admission or resultedin less invasive management and a shorter stay inICU.Presentation of this data together with recom-
mendations has led to a decision to introduce anearly warning system modified from the ‘‘MET’’ ap-proach. This system is called ‘‘Clinical Markers’’and involves ward staff alerting medical staff when-ever a patient exhibits any one of the six clinicalmarkers. If the parent unit are unable to attendwithin 15min, or if these clinical markers are unre-solved the ICU LNs are notified.When there is no ICULN on duty the ICU Registrar is notified. Unlike theMET approach this has not replaced the hospital’scardiac arrest team for cardiopulmonary arrests ormedical emergencies. The Clinical Marker systemwas introduced by the ICU LNs in February 2003 anddata relating to this initiative is currently being col-lected.The ICU LNs were successful in 2000 with a sub-
mission to the health department of the StateGovernment of Victoria in obtaining a substantialgrant to assist in the establishment and evalua-tion of Nurse Practitioner roles. The ICU LN modelfocused on formalising the extended practices ofadvanced patient assessment, referral privileges,ordering of diagnostics and therapeutic medicationmanagement. From the beginning of their involve-ment in the Nurse Practitioner project, the ICU LNshave been active at both local and overseas level,in assisting nurses at other hospitals to develop and
introduce the ICU LN role within their own hospitalsand to embrace the concept of Nurse Practitioner.On reflection acceptance of the ICU LN role by
clinical staff was delayed because of insufficienteducation and promotion. Presentations at medi-cal forums, i.e. ‘‘grand rounds’’ and ‘‘medical stafforientation programs’’ should have been included.Communication to all staff about the new role bythe Chief Executive Officer in his weekly newslet-ter to staff as well as in the monthly hospital mag-azine should have been included in an effort to in-crease awareness among medical staff. These av-enues have all been utilised subsequently by the ICULNs to inform staff about grants obtained, confer-ence presentations and extending the current roleto that of nurse practitioner.Although a 7-day per week service is provided,
hours of coverage are restricted. Over night whenthere is no coverage, the ICU LNs refer ‘‘at risk’’patients to the ICU Registrar for overnight review.Anecdotal evidence suggests that this informal ar-rangement between the ICU LNs and the ICU Regis-trars is sufficient to meet the current needs of West-ern Hospital, however should the size of the unit in-crease or the workload of the ICU Registrar changethen this arrangement would need to be reviewed.
Conclusion
The ICU LN role is unique as it interacts withall areas of the hospital that provide care forthe complex patient. The ICU LNs collaborationwith the multi disciplinary team has enabled acost-effective, timely and integrated approach tomanaging the acute patient pre- and post-ICU care.Since it’s inception in 1998, the role of the
ICU LNs has evolved to that of Nurse Practitionerstatus and has shown enhanced health care deliv-ery by demonstrating improved patient outcomes.These outcomes include an increase in ICU bedavailability by ensuring that suitable patients cannow be discharged over the weekend period, areduction in the number of preventable ICU admis-sions/readmissions, improved ward managementof the tracheostomy patient and improved supportand educational opportunities for staff in managingcomplex patients.The latest trend in 2003 in Australia is the intro-
duction of both the MET and ICU LN models into theone hospital. This year has seen the expansion ofthe ICU LN model to respond to increased referralsfollowing the introduction of a clinical marker tooladapted from the MET concept. With the implemen-tation of the clinical marker tool and future plansto contact General Practitioners in the community

Bridging the gap between the intensive care unit and general wards 143
in notifying them of patient progress post-ICU dis-charge the ICU LNs are evaluating their workload toput a business plan forward in employing additionalstaff into the ICU LN position.The ICU LNs believe that this role offers a legit-
imate career path for expert ICU nurses. The posi-tion is professionally satisfying, challenging, allowsthe nurse to maintain their ICU knowledge base,gives some autonomy of practice, improves the linesof communication not only between ICU and thewards, but between all clinical disciplines and pro-vides for a variety of practice, i.e. clinical, man-agement, research and teaching.The ICU LNs at Western are pioneers in the de-
velopment and extension of this innovative model.Research will continue to analyse the potential ben-efits such roles have in the care of the acutely illpatients’ pre, during and post-ICU care.
References
Anderson K, Atkinson D, McBride J, Moorse S, Smith S. Setting upan outreach team in the UK. Crit Care Nurs Eur 2002;2(1):8—12.
Barbetti J, Choate K. ICU Liaison Nurse role at the Alfred. RoyalCollege of Nursing, Australia. Natl Nurs Networks NewslettIncorporat Chap 2002;5(1):9.
Buist MD, Moore GE, Bernard SA, Waxman BP, Anderson JN,Nguyen TV. Effects of a medical emergency team on re-
duction of incidence of and mortality from unexpectedcardiac arrests in hospital: preliminary study. Br Med J2002;324:387—90.
Coombs M, Dillon A. Crossing boundaries, re-defining care:the role of the critical care outreach team. J Clin Nurs2002;11(3):387—93.
Hillman KM, Bishop G, Lee A, Daffurn K, Bauman A, CrispinC, Ince L, Bristow P, Hourihan F. Identifying the generalward patient at high risk of cardiac arrest. Clin Intens Care1996;7:242—3.
Hourihan G, Bishop G, Hillman KM, Daffurn K, Lee A. The med-ical emergency team: a new strategy to identify and inter-vene in high-risk patients. Clin Intens Care 1995;6(6):269—72.
King JE, Lancaster L, Pierce J, Norman LD. Removing the wallsand expanding the boundaries: a curriculm [sic] model foracute care nurse practitioners. N&HC: Perspect Commun1996;17(6):304—7.
King JE. Advanced practice. Acute care nurse practitioners: anidea whose time has come! Tennessee Nurse 2001;20(1):20—1.
Kleinpell R. Acute-care nurse practitioners: roles and practiceprofiles. AACN Clin Issues 1997;8(1):156—62.
Kleinpell-Nowell R. Longitudinal survey of acute carenurse practitioner practice: year 1. AACN Clin Issues1999;10(4):515—20.
Piano MR, Kleinpell R, Johnson JA. The acute care nurse prac-titioner and management of common health problems: aproposal. Am J Crit Care 1996;5(4):289—92.
Schlicht K. Clinical nurse consultant: next step for the nursingprofession. Crit Times 1995;4(4):1—2.
The Australian Council on Healthcare Standard. Determine thepotential to improve the quality of care in Australian healthcare organizations, 2nd ed. Health Services Research Group,University of Newcastle, NSW; 2001.





























