Embed Size (px)
Citation preview
J O U R N A L O F T H E A M E R I C A N C O L L E G E O F C A R D I O L O G Y V O L . 6 6 , N O . 1 2 , 2 0 1 5
ª 2 0 1 5 B Y T H E A M E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N D A T I O N I S S N 0 7 3 5 - 1 0 9 7 / $ 3 6 . 0 0
P U B L I S H E D B Y E L S E V I E R I N C . h t t p : / / d x . d o i . o r g / 1 0 . 1 0 1 6 / j . j a c c . 2 0 1 5 . 0 8 . 0 0 2
Downloaded From: http://co
REVIEW TOPIC OF THE WEEK
Bridging Anticoagulation
Primum Non NocereStephen J. Rechenmacher, MD, James C. Fang, MD
ABSTRACT
Fro
rep
Lis
Ma
nte
Chronic oral anticoagulation frequently requires interruption for various reasons and durations. Whether or not to bridge
with heparin or other anticoagulants is a common clinical dilemma. The evidence to inform decision making is limited,
making current guidelines equivocal and imprecise. Moreover, indications for anticoagulation interruption may be
unclear. New observational studies and a recent large randomized trial have noted significant perioperative or peripro-
cedural bleeding rates without reduction in thromboembolism when bridging is employed. Such bleeding may also
increase morbidity and mortality. In light of these findings, physician preferences for routine bridging anticoagulation
during chronic anticoagulation interruptions may be too aggressive. More randomized trials, such as PERIOP2 (A Double
Blind Randomized Control Trial of Post-Operative Low Molecular Weight Heparin Bridging Therapy Versus Placebo
Bridging Therapy for Patients Who Are at High Risk for Arterial Thromboembolism), will help guide periprocedural
management of anticoagulation for indications such as venous thromboembolism and mechanical heart valves. In the
meantime, physicians should carefully consider both the need for oral anticoagulation interruption and the practice of
routine bridging when anticoagulation interruption is indicated. (J Am Coll Cardiol 2015;66:1392–403) © 2015 by the
American College of Cardiology Foundation.
M ore than 35 million prescriptions for oralanticoagulation (OAC) are written eachyear in the United States (1). Conditions
being treated with OAC include atrial fibrillation, me-chanical heart valves, venous or arterial thromboem-bolism, and ventricular assist devices. In any givenyear, 15% to 20% of these patients will undergoan invasive procedure or surgery that interruptstheir chronic OAC, putting them at increased riskfor thromboembolism (TE), hemorrhage, and death(2,3). Perioperative or periprocedural (hereafter com-bined simply as periprocedural) anticoagulation man-agement is a common clinical dilemma, often leadingto significant adverse events. The clinical relevanceof this common dilemma and the lack of definitiveevidence to guide medical decision making hasfinally led to the conduct of pertinent clinical trials,1 of which has been recently completed (4). How-ever, current guidelines from the American Heart
m the Division of Cardiovascular Medicine, University of Utah Health Scie
orted that they have no relationships relevant to the contents of this pap
ten to this manuscript’s audio summary by JACC Editor-in-Chief Dr. Vale
nuscript received July 22, 2015; accepted August 3, 2015.
nt.onlinejacc.org/ by James Januzzi on 09/22/2015
Association, American College of Cardiology, HeartRhythm Society, and American College of Chest Phy-sicians have yet to incorporate the findings of thistrial and remain based upon observational studiesand expert opinion (5,6). Yet, the guidelines dolargely agree upon 3 important principles:
1. OAC should not be interrupted for procedures withlow bleeding risk.
2. Patients at highest risk for TE without excessivebleeding risk should consider bridging. Conversely,those at low risk for TE should not be bridged.
3. Intermediate-risk cases (Table 1) should bemanaged by individually considering patient- andprocedure-specific risks for bleeding and TE.
Patients at low risk for TE should not create aclinical dilemma. Yet, physician surveys of peri-procedural bridging preferences demonstrate thatapproximately 30% of physicians choose to bridge
nces Center, Salt Lake City, Utah. Both authors have
er to disclose.
ntin Fuster.
AB BR E V I A T I O N S
AND ACRONYM S
INR = international normalized
ratio
LVAD = left ventricular assist
device
NOAC = novel oral
anticoagulant
OAC = oral anticoagulation
TE = thromboembolism
VTE = venous
thromboembolism
J A C C V O L . 6 6 , N O . 1 2 , 2 0 1 5 Rechenmacher and FangS E P T E M B E R 2 2 , 2 0 1 5 : 1 3 9 2 – 4 0 3 Bridging Anticoagulation
1393
Downloa
patients at low risk for TE due to overestimation ofthrombosis risk (7–9). There is even greater hetero-geneity of practice in those patients with intermedi-ate or unclear risks of bleeding or TE. Currentevidence, including the recently completed BRIDGEtrial (Bridging Anticoagulation in Patients WhoRequire Temporary Interruption of Warfarin Therapyfor an Elective Invasive Procedure or Surgery) (seelater discussion), suggests that periproceduralbleeding rates are significantly higher than throm-bosis rates in this group (2,4,10–16).
The goal of this review is not to detail the timing,doses, or specifics of bridging anticoagulation. Rather,we will review the data available to specific questionsthat arise in clinical practice to better individualizedecision making and reduce adverse events. We havelimited the scope of the discussion to anticoagulantmanagement. The periprocedural management of an-tiplatelet agents has been reviewed elsewhere (5,17).
CONFIRMING OAC INDICATIONS
When determining the optimal periprocedural anti-coagulation strategy, a critical first step is to fullyappreciate the indication for chronic OAC. In somecases, OAC may no longer be required. For example, apatient may present for a procedure who has been onwarfarin for a single provoked deep vein thrombosisthat occurred more than 6 months prior. In such asituation, discontinuation of OAC is most appropriateand will simplify periprocedural anticoagulationmanagement.
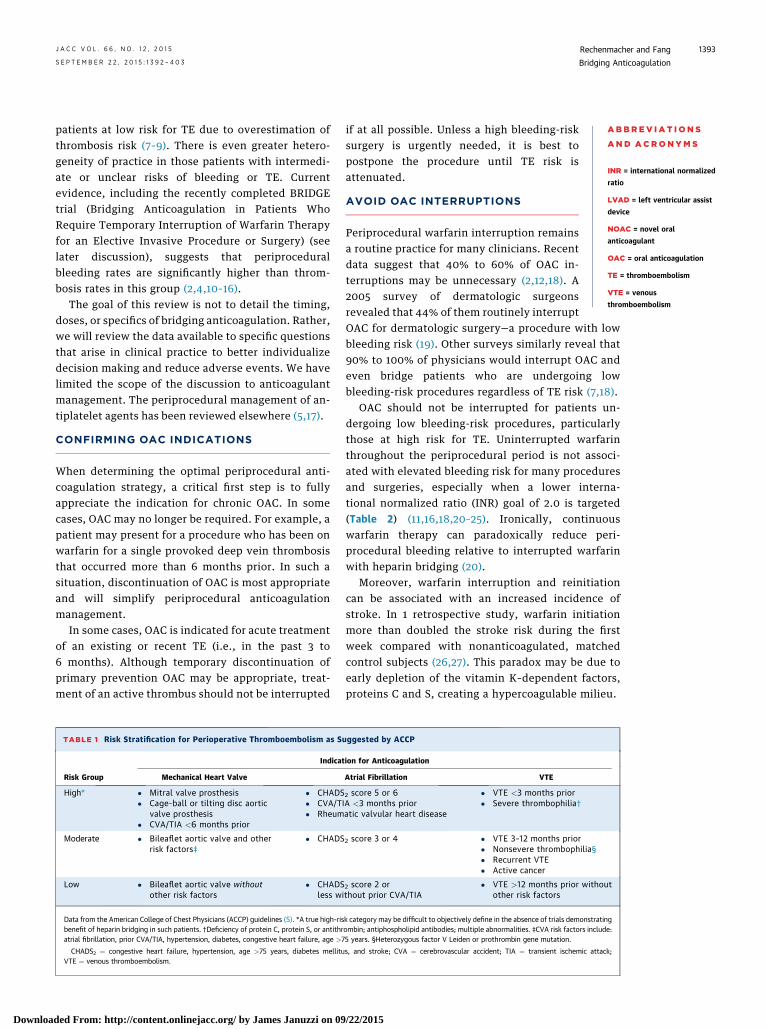
In some cases, OAC is indicated for acute treatmentof an existing or recent TE (i.e., in the past 3 to6 months). Although temporary discontinuation ofprimary prevention OAC may be appropriate, treat-ment of an active thrombus should not be interrupted
TABLE 1 Risk Stratification for Perioperative Thromboembolism as S
Risk Group
Indicat
Mechanical Heart Valve
High* � Mitral valve prosthesis� Cage-ball or tilting disc aortic
valve prosthesis� CVA/TIA <6 months prior
� CHADS� CVA/T� Rheum
Moderate � Bileaflet aortic valve and otherrisk factors‡
� CHADS
Low � Bileaflet aortic valve withoutother risk factors
� CHADSless w
Data from the American College of Chest Physicians (ACCP) guidelines (5). *A true high-risbenefit of heparin bridging in such patients. †Deficiency of protein C, protein S, or antithratrial fibrillation, prior CVA/TIA, hypertension, diabetes, congestive heart failure, age >7
CHADS2 ¼ congestive heart failure, hypertension, age >75 years, diabetes mellituVTE ¼ venous thromboembolism.
ded From: http://content.onlinejacc.org/ by James Januzzi on 09
if at all possible. Unless a high bleeding-risksurgery is urgently needed, it is best topostpone the procedure until TE risk isattenuated.
AVOID OAC INTERRUPTIONS
Periprocedural warfarin interruption remainsa routine practice for many clinicians. Recentdata suggest that 40% to 60% of OAC in-terruptions may be unnecessary (2,12,18). A2005 survey of dermatologic surgeonsrevealed that 44% of them routinely interrupt
OAC for dermatologic surgery—a procedure with lowbleeding risk (19). Other surveys similarly reveal that90% to 100% of physicians would interrupt OAC andeven bridge patients who are undergoing lowbleeding-risk procedures regardless of TE risk (7,18).OAC should not be interrupted for patients un-dergoing low bleeding-risk procedures, particularlythose at high risk for TE. Uninterrupted warfarinthroughout the periprocedural period is not associ-ated with elevated bleeding risk for many proceduresand surgeries, especially when a lower interna-tional normalized ratio (INR) goal of 2.0 is targeted(Table 2) (11,16,18,20–25). Ironically, continuouswarfarin therapy can paradoxically reduce peri-procedural bleeding relative to interrupted warfarinwith heparin bridging (20).
Moreover, warfarin interruption and reinitiationcan be associated with an increased incidence ofstroke. In 1 retrospective study, warfarin initiationmore than doubled the stroke risk during the firstweek compared with nonanticoagulated, matchedcontrol subjects (26,27). This paradox may be due toearly depletion of the vitamin K–dependent factors,proteins C and S, creating a hypercoagulable milieu.
uggested by ACCP
ion for Anticoagulation
Atrial Fibrillation VTE
2 score 5 or 6IA <3 months prioratic valvular heart disease
� VTE <3 months prior� Severe thrombophilia†
2 score 3 or 4 � VTE 3–12 months prior� Nonsevere thrombophilia§� Recurrent VTE� Active cancer
2 score 2 orithout prior CVA/TIA
� VTE >12 months prior withoutother risk factors
k category may be difficult to objectively define in the absence of trials demonstratingombin; antiphospholipid antibodies; multiple abnormalities. ‡CVA risk factors include:5 years. §Heterozygous factor V Leiden or prothrombin gene mutation.
s, and stroke; CVA ¼ cerebrovascular accident; TIA ¼ transient ischemic attack;
/22/2015
TABLE 2 Procedures Amenable to Uninterrupted
Therapeutic Warfarin
Endoscopy
Biopsies
Endovascular interventions
Percutaneous coronary interventions
Cardiac electrophysiology studies and ablations
Cardiac device implantation (pacemakers, defibrillators,loop recorders)
Cataract surgery
Dermatologic surgery
Dental extractions
Epidural anesthetics and likely other interventional painmanagement techniques
Minor noncardiac surgeries
Total knee arthroplasty
Arthroscopic surgery
Rechenmacher and Fang J A C C V O L . 6 6 , N O . 1 2 , 2 0 1 5
Bridging Anticoagulation S E P T E M B E R 2 2 , 2 0 1 5 : 1 3 9 2 – 4 0 3
1394
Downloaded From: http://co
Relatively major operations may also toleratecontinuation of OAC. For example, certain orthopedicsurgeries may also prove tolerant to uninterruptedOAC therapy. Rhodes et al. (22) retrospectivelyanalyzed 77 patients undergoing total knee arthro-plasty; 38 patients remained on warfarin throughoutthe perioperative period. They found no significantdifference in the rates of blood transfusion, woundcomplications, or reoperation between the 2 groups.
Randomized studies appear to confirm these ob-servations. Two randomized prospective trials havebeen conducted to directly compare the safety andefficacy of uninterrupted warfarin versus bridgingwith heparin. In a 2007 study, 214 patients on OACundergoing dental extraction were randomized toeither continue warfarin or to stop warfarin andbridge with heparin (23). Interrupted warfarin withoutbridging was not studied. There were no TE events ineither group, consistent with the low rate of TE seenin other studies. Importantly, nearly one-half of thepatients were at presumably high TE risk, with eitherprosthetic valves or atrial fibrillation with valvulardisease. The rate of bleeding was also similar betweenpatients with uninterrupted warfarin versus thosewith heparin bridging (7.34% vs. 4.76%, respectively;p > 0.05).
BRUISE CONTROL (Bridge or Continue Coumadinfor Device Surgery Randomized Controlled Trial),published in 2013, randomized 681 high-risk patientsundergoing pacemaker or defibrillator implantationto either uninterrupted OAC or interrupted OAC withheparin bridging (20). Due to the high TE risk of thestudy population, there was again no arm of inter-rupted OAC without bridging. The investigators foundthat heparin produced more than 4� as many clini-cally significant pocket hematomas than in those onuninterrupted warfarin (16% vs. 3.5%; p < 0.001).
ntent.onlinejacc.org/ by James Januzzi on 09/22/2015
Strokes and transient ischemic attacks occurred in 2patients on uninterrupted warfarin (0.3%), with nostatistically significant difference between thegroups.
Nevertheless, in many circumstances, interruptionof chronic anticoagulation will be necessary to avoidexcessive procedural- or surgical-related bleeding.To justify bridging anticoagulation, the risk of TEwhile off of anticoagulation should be great enoughto justify the bleeding risk of bridging. However, asoutlined in the following text, the TE risk is generallymodest and outweighed by the risk of bridging-associated bleeding.
WHAT IS THE CLOTTING AND BLEEDING RISK
IN THE PERIPROCEDURAL PERIOD?
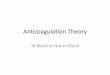
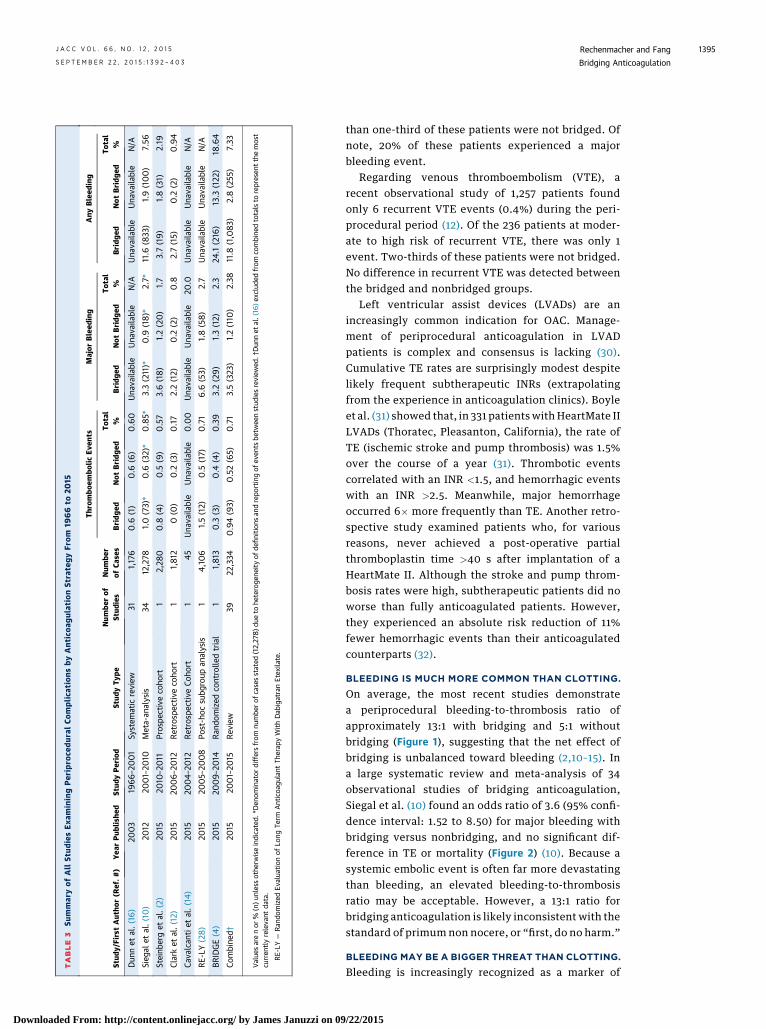
PERIPROCEDURAL TE IS UNCOMMON. The actualrate of periprocedural TE for unbridged OAC in-terruptions is rare, estimated at approximately 0.53%from our review of over 23,000 OAC interruptions in70 studies from 1966 to 2015 (Table 3, Figure 1A)(2,4,10–16,28). From the same database, the rate of TEfor patients who are bridged is slightly higher at0.92%. The actual rate is likely higher in the absenceof bridging but is biased in these observationalstudies by the clinician’s impression of greater TE riskthat drives the decision to bridge.
Rates of bleeding and TE vary by OAC indication(Figure 1B). For atrial fibrillation, an individual’s dailyrisk of stroke or transient ischemic attack can beapproximated by dividing the annual stroke risk by365 days. Although one might expect more thrombosisin the periprocedural period by invoking Virchow’striad, observational studies have not borne thishypothesis out. For example, in ORBIT-AF (OutcomesRegistry for Better Informed Treatment of AtrialFibrillation) (2), the periprocedural cohort observed a0.35% 30-day stroke rate. Using the average ORBIT-AFCHA2DS2-VASc score of 4.1, corresponding to anannual stroke risk of approximately 4.2%, the calcu-lated 30-day stroke risk is surprisingly similar at 0.35%.
For mechanical heart valves, the perioperative riskof TE is approximately 1% (11). Older studies (mostlyfrom the 1970s and 1980s) suggested a higher inci-dence of perioperative TE. However, these olderstudies included patients with higher-risk valves,such as cage-ball and tilting disc valves, which wouldhave been far more common in that time period (29).In a more contemporary study of 45 patients withmechanical aortic and/or mitral valves who wereundergoing central nervous system surgeries be-tween 2004 and 2012, there were no TE events duringan average anticoagulation gap of 7 days (14). More
TABLE
3Su
mmar
yof
All
Stud
iesEx
aminingPer
ipro
cedur
alCo
mplica
tion
sby
Ant
icoa
gulat
ionSt
rate
gyFr
om19
66
to20
15
Stud
y/FirstAut
hor(R
ef.#
)Yea
rPub
lishe
dSt
udyPeriod
Stud
yTy
peNum
berof
Stud
ies
Num
ber
ofCa
ses
Thro
mbo
embo
licEv
ents
Major
Bleed
ing
Any
Bleed
ing
Bridg
edNot
Bridg
edTo
tal
%Bridg
edNot
Bridg
edTo
tal
%Bridg
edNot
Bridg
edTo
tal
%
Dun
net
al.(16)
2003
1966–20
01
System
atic
review
311,176
0.6
(1)
0.6
(6)
0.60
Una
vaila
ble
Una
vaila
ble
N/A
Una
vaila
ble
Una
vaila
ble
N/A
Sieg
alet
al.(10)
2012
2001–20
10Meta-an
alysis
3412,278
1.0
(73)*
0.6
(32)*
0.85*
3.3(211)*
0.9
(18)*
2.7*
11.6
(833
)1.9(100)
7.56
Steinb
erget
al.(2)
2015
2010
–20
11Prospe
ctiveco
hort
12,28
00.8
(4)
0.5
(9)
0.57
3.6(18)
1.2(20)
1.7
3.7(19)
1.8(31)
2.19
Clarket
al.(12)
2015
2006–20
12Retrosp
ective
coho
rt1
1,812
0(0
)0.2
(3)
0.17
2.2(12)
0.2
(2)
0.8
2.7(15)
0.2
(2)
0.94
Cava
lcan
tiet
al.(14)
2015
2004–
2012
Retrosp
ective
Coho
rt1
45Una
vaila
ble
Una
vaila
ble
0.00
Una
vaila
ble
Una
vaila
ble
20.0
Una
vaila
ble
Una
vaila
ble
N/A
RE-LY
(28)
2015
2005–20
08
Post-hoc
subg
roup
analysis
14,10
61.5(12)
0.5
(17)
0.71
6.6
(53)
1.8(58)
2.7
Una
vaila
ble
Una
vaila
ble
N/A
BRIDGE(4)
2015
2009–20
14Ran
domized
controlle
dtrial
11,813
0.3
(3)
0.4
(4)
0.39
3.2(29)
1.3(12)
2.3
24.1
(216
)13.3
(122
)18
.64
Combine
d†20
1520
01–20
15Rev
iew
3922
,334
0.94(93)
0.52(65)
0.71
3.5(323
)1.2(110
)2.38
11.8
(1,083)
2.8(255
)7.33
Value
sarenor
%(n)un
less
othe
rwiseindicated.
*Den
ominator
differsfrom
numbe
rof
casesstated
(12,27
8)d
ueto
heteroge
neityof
definition
san
drepo
rtingof
even
tsbe
twee
nstud
iesreview
ed.†
Dun
net
al.(16
)exclude
dfrom
combine
dtotalsto
represen
tthemost
curren
tlyreleva
ntda
ta.
RE-LY
¼Ran
domized
Evalua
tion
ofLo
ngTe
rmAnticoa
gulant
Therap
yWithDab
igatranEtex
ilate.
J A C C V O L . 6 6 , N O . 1 2 , 2 0 1 5 Rechenmacher and FangS E P T E M B E R 2 2 , 2 0 1 5 : 1 3 9 2 – 4 0 3 Bridging Anticoagulation
1395
Downloaded From: http://content.onlinejacc.org/ by James Januzzi on 09
than one-third of these patients were not bridged. Ofnote, 20% of these patients experienced a majorbleeding event.
Regarding venous thromboembolism (VTE), arecent observational study of 1,257 patients foundonly 6 recurrent VTE events (0.4%) during the peri-procedural period (12). Of the 236 patients at moder-ate to high risk of recurrent VTE, there was only 1event. Two-thirds of these patients were not bridged.No difference in recurrent VTE was detected betweenthe bridged and nonbridged groups.
Left ventricular assist devices (LVADs) are anincreasingly common indication for OAC. Manage-ment of periprocedural anticoagulation in LVADpatients is complex and consensus is lacking (30).Cumulative TE rates are surprisingly modest despitelikely frequent subtherapeutic INRs (extrapolatingfrom the experience in anticoagulation clinics). Boyleet al. (31) showed that, in 331 patients with HeartMate IILVADs (Thoratec, Pleasanton, California), the rate ofTE (ischemic stroke and pump thrombosis) was 1.5%over the course of a year (31). Thrombotic eventscorrelated with an INR <1.5, and hemorrhagic eventswith an INR >2.5. Meanwhile, major hemorrhageoccurred 6� more frequently than TE. Another retro-spective study examined patients who, for variousreasons, never achieved a post-operative partialthromboplastin time >40 s after implantation of aHeartMate II. Although the stroke and pump throm-bosis rates were high, subtherapeutic patients did noworse than fully anticoagulated patients. However,they experienced an absolute risk reduction of 11%fewer hemorrhagic events than their anticoagulatedcounterparts (32).
BLEEDING IS MUCH MORE COMMON THAN CLOTTING.
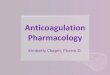
On average, the most recent studies demonstratea periprocedural bleeding-to-thrombosis ratio ofapproximately 13:1 with bridging and 5:1 withoutbridging (Figure 1), suggesting that the net effect ofbridging is unbalanced toward bleeding (2,10–15). Ina large systematic review and meta-analysis of 34observational studies of bridging anticoagulation,Siegal et al. (10) found an odds ratio of 3.6 (95% confi-dence interval: 1.52 to 8.50) for major bleeding withbridging versus nonbridging, and no significant dif-ference in TE or mortality (Figure 2) (10). Because asystemic embolic event is often far more devastatingthan bleeding, an elevated bleeding-to-thrombosisratio may be acceptable. However, a 13:1 ratio forbridging anticoagulation is likely inconsistent with thestandard of primum non nocere, or “first, do no harm.”
BLEEDING MAY BE A BIGGER THREAT THAN CLOTTING.
Bleeding is increasingly recognized as a marker of
/22/2015

FIGURE 1 Rates of Periprocedural Thromboembolism and Bleeding
12%
10%
8%
6%
4%
2%
0%
Even
t Rat
e
0.52%1.18%
2.80%
0.94%
3.52%
Not Bridged Bridged
11.83%
Thromboembolism
Major Bleeding
Any Bleeding
4%
3%
2%
1%
0%
Even
t Rat
e
0.65%
2.26%
0.76%
1.14% 1.13%
3.32%Thromboembolism
Major Bleeding
A
B
Afib VTE Mechanical Valves
Comparison of periprocedural event rates by bridging strategy (A) and oral anticoagulation
indication (B). Rates represent pooled data from Clark et al. (12), Steinberg et al. (2),
Cavalcanti et al. (14), Wysokinski et al. (11), RE-LY (Randomized Evaluation of Long Term
Anticoagulant Therapy With Dabigatran Etexilate) (28), and BRIDGE (4). Overall bleeding
rates were not available by individual oral anticoagulation indication. Afib ¼ atrial fibril-
lation; VTE ¼ venous thromboembolism.
Rechenmacher and Fang J A C C V O L . 6 6 , N O . 1 2 , 2 0 1 5
Bridging Anticoagulation S E P T E M B E R 2 2 , 2 0 1 5 : 1 3 9 2 – 4 0 3
1396
Downloaded From: http://co
poor outcomes (33,34). For example, anticoagulation-related hemorrhage has been clearly associated withincreased morbidity and mortality in the publishedmedical, interventional, and surgical data and, inmany cases, overwhelms the benefits of the anti-coagulation (3,33,35–37). Approximately 10% of majorbleeding events in patients anticoagulated for VTEultimately end in death—ironically comparable to themortality rate from recurrent VTE (8). In a studyanalyzing 3,037 atrial fibrillation patients taking OAChospitalized at 584 centers, investigators retrospec-tively discovered that 14 patients died who hadreceived heparin bridging compared with no deaths incontrol subjects who did not receive heparin(p < 0.005) (34). Hospital length of stay was increasedby 19.3% in association with unfractionated heparin
ntent.onlinejacc.org/ by James Januzzi on 09/22/2015
(p < 0.003). Also, compared with uninterruptedwarfarin, bridging anticoagulation correlates withincreased hospital cost ($41.72 � $37.81 vs. $1,114.60 �$164.90) (21).
Despite the evidence that: 1) TE events are rare inthe periprocedural period; 2) hemorrhage is far morecommon than TE with bridging; and 3) there is noclear antithrombotic benefit with bridging, it remainsa common and highly variable practice.
CONTEMPORARY BRIDGING PRACTICES ARE
HIGHLY VARIABLE
Traditional contemporary anticoagulation clinicsreport an average time in therapeutic range of only65% (38). In 1 study, 23% of INR values were below 2.0(39). Therefore, the average patient on chronicwarfarin therapy spends more than 84 days/year in asubtherapeutic range. Yet, cumulative annual TErates are modest at approximately 1% when all pa-tients with atrial fibrillation in such programs areconsidered (40). It is worth noting that the lengthof time warfarin is interrupted for a procedure istypically <5 days (13). Although it is not commonpractice to bridge subtherapeutic patients in theoutpatient setting, many clinicians default to bridgingduring these short periprocedural periods—ironically,a time when patients are at greater risk of bleeding.
The threshold for bridging in current clinicalpractice is too low (8). Moderate- and even low-riskpatients are often being bridged by default, “just tobe safe.” Paradoxically, this practice is producingpreventable adverse bleeding events with littlebenefit for thrombosis prevention. Clark et al. (12)recently described a large retrospective cohort of1,812 procedures with chronic OAC interruption (12).They found that 73% of patients bridged for VTE wereat low risk for recurrence. In addition, they may nothave required OAC interruption in the first place,given that 39% of those procedures are similar tothose listed in Table 2.
Steinberg et al. (2) analyzed the ORBIT-AFregistry—a large prospective observational atrialfibrillation cohort including 2,803 OAC interruptionsfor various procedures. They similarly found thatpatients were being bridged indiscriminately, asevidenced by the similar CHA2DS2-VASc scoresbetween the bridged and nonbridged groups. Ifpatients’ individual bleeding risks were beingconsidered, one would have expected the averageCHA2DS2-VASc score to be higher in the bridgedgroup. In addition, in patients whose OAC was inter-rupted for various procedures, bridging was associ-ated with a 4-fold risk of bleeding (5% vs. 1.3%;

FIGURE 2 Odds Ratios for Major Bleeding and Thromboembolic Events With Bridging
Study or Subgroup Bridging No Bridging Odds Ratio Odds RatioEvents Total Events Total Weight M-H, Random, 95% CI M-H, Random, 95% CI
0.005 0.1 1 10 200Favors Bridging Favors No Bridging
0.005 0.1 1 10 200Favors Bridging Favors No Bridging
Daniels et al., 2009Garcia et al., 2008Jaffer et al., 2010McBane et al., 2010Wysokinski et al., 2008
154
13146
342108229514
204
52324
2131185263261182
24.9%15.3%21.0%17.9%
20.8%
1.91 [0.68, 5.33]22.75 [4.12, 125.68]
5.22 [1.47, 18.54]3.63 [0.82, 16.08]
1.35 [0.37, 4.86]
Total (95% CI) 1397 2104 100.0% 3.60 [1.52, 8.50]Total eventsHeterogeneity: Tau2 = 0.50; Chi2 = 8.41, df = 4 (P = 0.08); I2 = 52%Test for overall effect: Z = 2.92 (P = 0.004)
52 16
Daniels et al., 2009Garcia et al., 2008Jaffer et al., 2010Marquie et al., 2006McBane et al., 2010Tompkins et al., 2010Varkarakis et al., 2005Wysokinski et al., 2008
401
010
103
34210822911451415525
204
17326634
2131185263114261513762182
8.8%5.2%8.2%4.6%
40.5%9.4%4.7%
18.6%
2.51 [0.28, 22.60]0.72 [0.04, 12.76]0.38 [0.04, 3.68]0.20 [0.01, 4.14]0.84 [0.30, 2.35]0.55 [0.07, 4.59]
4.25 [0.21, 84.56]0.66 [0.15, 3.01]
Total (95% CI) 1691 3493 100.0% 0.80 [0.42, 1.54]Total eventsHeterogeneity: Tau2 = 0.00; Chi2 = 3.68, df = 7 (P = 0.82); I2 = 0%Test for overall effect: Z = 0.67 (P = 0.50)
19 32
A Major Bleeding
B Thromboembolic EventsStudy or Subgroup Bridging No Bridging Odds Ratio Odds Ratio
Events Total Events Total Weight M-H, Random, 95% CI M-H, Random, 95% CI
Forest plot for major bleeding from Siegal et al. (10) demonstrates a significant odds ratio of 3.6 for patients receiving bridging anticoagulation (A). There
is no significant difference in thromboembolic events between bridging and nonbridging (B). CI ¼ confidence interval; M-H ¼ Mantel-Haenszel.
Reprinted with permission from Siegal et al. (10).
J A C C V O L . 6 6 , N O . 1 2 , 2 0 1 5 Rechenmacher and FangS E P T E M B E R 2 2 , 2 0 1 5 : 1 3 9 2 – 4 0 3 Bridging Anticoagulation
1397
Downloa
adjusted odds ratio: 3.84; p < 0.0001) with no sig-nificant difference in TE events (2).
THE BRIDGE TRIAL
In support of the mounting observational data, therecently published landmark BRIDGE trial now pro-vides the most compelling evidence that routinebridging in moderate-risk patients is harmful. In theBRIDGE trial—a randomized, double-blinded, placebo-controlled noninferiority study—1,884 atrial fibrilla-tion patients (valvular and nonvalvular) who wereundergoing a procedure with planned warfarininterruption were randomized to anticoagulationbridging with the low molecular-weight heparin,dalteparin, or placebo (4). The reasons for OACinterruption were not specified, but importantly,89.4% underwent procedures designated as “lowbleeding risk.” The average CHADS2 (congestiveheart failure, hypertension, age >75 years, diabetesmellitus, stroke) score was 2.3, making the study
ded From: http://content.onlinejacc.org/ by James Januzzi on 09
population largely moderate risk for TE. Theprimary endpoints were arterial thromboembolismand major bleeding.
The rate of arterial TE in the placebo group wasnoninferior to the bridging group (0.4% vs. 0.3%;p ¼ 0.01 for noninferiority). Major and minor bleedingin the placebo group was significantly less than inthe bridging group (1.3% vs. 3.2%; p ¼ 0.005; 12%vs. 20.9%; p ¼ 0.001; respectively). There was nomeasurable difference among myocardial infarction,deep vein thrombosis, pulmonary embolism, or death.
This study confirms that no bridging is noninferiorto bridging for preventing TE and is superior forreducing bleeding. The assumption that any in-creased bleeding caused by bridging is justified by adecrease in TE has been challenged by the BRIDGEtrial. It appears that bridging in moderate-risk atrialfibrillation populations causes harm without benefit.
An important limitation of the BRIDGE trialwas that the population studied was limited to pa-tients whose anticoagulation indication was atrial
/22/2015
CENTRAL ILLUSTRATION Bridging Anticoagulation: Algorithms for Periprocedural Interrupting and Bridging Anticoagulation
YN
N
N
Y
Y N
YN
Y
Y N
Periprocedural patient on chronic oral anticoagulation (OAC)
Discontinue OAC indefinitely Do not interrupt OAC Interrupt OAC
Do not bridge Consider bridging
Interrupt OAC, consider reversal agent and proceed to surgery
DECI
SION
TO
INTE
RRUP
T OA
CDE
CISI
ON T
O BR
IDGE
WIT
H AN
TICO
AGUL
ANTS
Is thromboembolic risk low?
Is surgeon willing to operate with uninterrupted OAC?
Is a high-bleeding risk procedure required emergently?
Is OAC still required?
What is the risk of bleeding with uninterrupted OAC?HighIntermediateLow
What is the daily thromboembolic risk?HighIntermediateLow
Is atrial fibrillation the indication for OAC?
Rechenmacher, S.J. et al. J Am Coll Cardiol. 2015; 66(12):1392–403.
Does the thromboembolic risk clearlyoutweigh the increased bleeding risk from bridging?
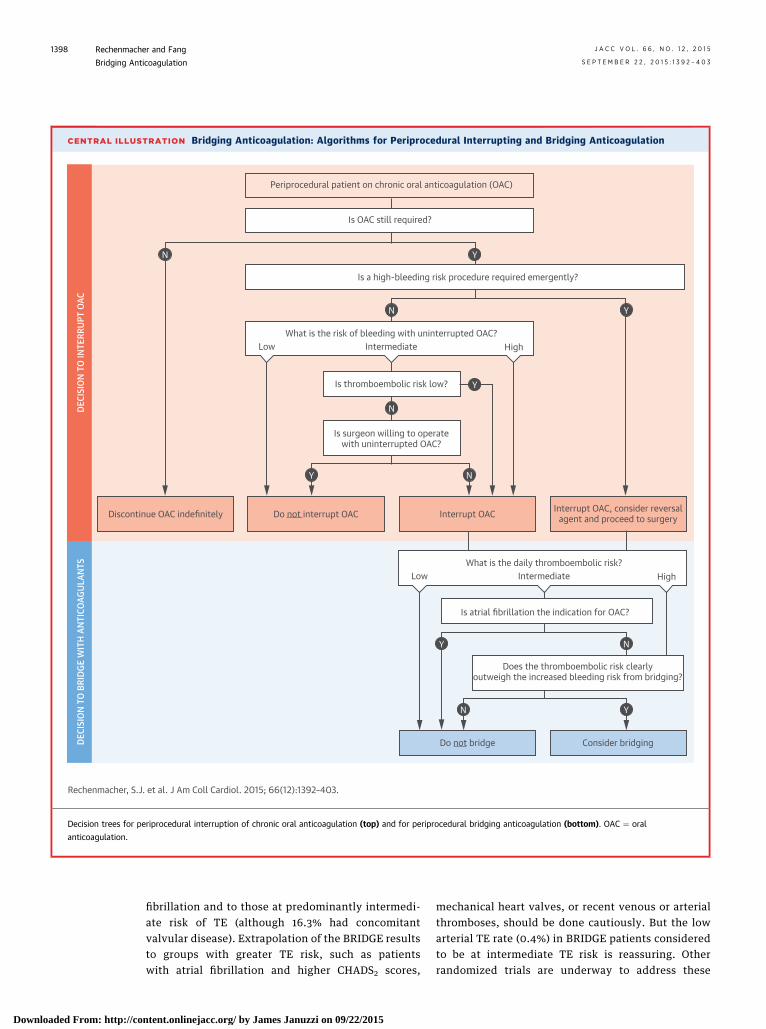
Decision trees for periprocedural interruption of chronic oral anticoagulation (top) and for periprocedural bridging anticoagulation (bottom). OAC ¼ oral
anticoagulation.
Rechenmacher and Fang J A C C V O L . 6 6 , N O . 1 2 , 2 0 1 5
Bridging Anticoagulation S E P T E M B E R 2 2 , 2 0 1 5 : 1 3 9 2 – 4 0 3
1398
Downloaded From: http://co
fibrillation and to those at predominantly intermedi-ate risk of TE (although 16.3% had concomitantvalvular disease). Extrapolation of the BRIDGE resultsto groups with greater TE risk, such as patientswith atrial fibrillation and higher CHADS2 scores,
ntent.onlinejacc.org/ by James Januzzi on 09/22/2015
mechanical heart valves, or recent venous or arterialthromboses, should be done cautiously. But the lowarterial TE rate (0.4%) in BRIDGE patients consideredto be at intermediate TE risk is reassuring. Otherrandomized trials are underway to address these
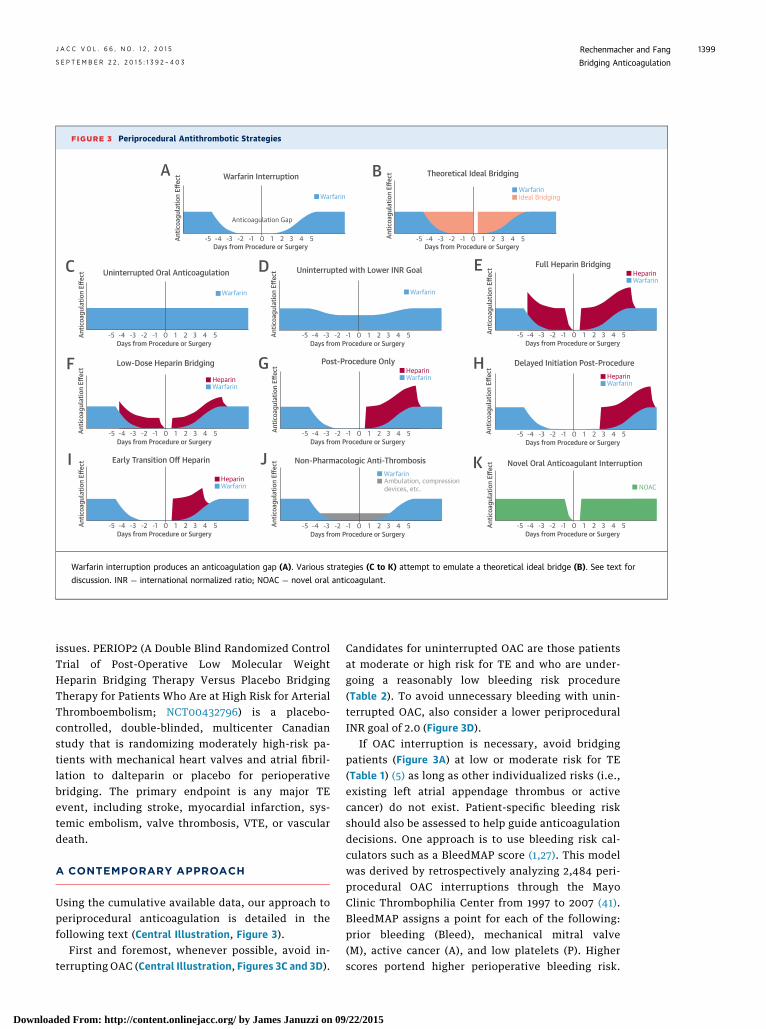
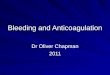
FIGURE 3 Periprocedural Antithrombotic Strategies
-5 -4 -3 -2 -1 0 1 2 3 4 5Days from Procedure or Surgery
Antic
oagu
latio
n Eff
ect Warfarin Interruption
Anticoagulation Gap
Warfarin
A
-5 -4 -3 -2 -1 0 1 2 3 4 5Days from Procedure or Surgery
Antic
oagu
latio
n Eff
ect Theoretical Ideal Bridging
WarfarinIdeal Bridging
B
-5 -4 -3 -2 -1 0 1 2 3 4 5Days from Procedure or Surgery
-5 -4 -3 -2 -1 0 1 2 3 4 5Days from Procedure or Surgery
Antic
oagu
latio
n Eff
ect
Antic
oagu
latio
n Eff
ectUninterrupted Oral Anticoagulation Uninterrupted with Lower INR Goal
Warfarin Warfarin
C D
-5 -4 -3 -2 -1 0 1 2 3 4 5Days from Procedure or Surgery
Antic
oagu
latio
n Eff
ect Full Heparin Bridging
WarfarinHeparin
E
-5 -4 -3 -2 -1 0 1 2 3 4 5Days from Procedure or Surgery
Antic
oagu
latio
n Eff
ect Low-Dose Heparin Bridging
WarfarinHeparin
F
-5 -4 -3 -2 -1 0 1 2 3 4 5Days from Procedure or Surgery
-5 -4 -3 -2 -1 0 1 2 3 4 5Days from Procedure or Surgery
Antic
oagu
latio
n Eff
ect
Antic
oagu
latio
n Eff
ect
Post-Procedure Only Delayed Initiation Post-ProcedureWarfarinHeparin
WarfarinHeparin
G H
-5 -4 -3 -2 -1 0 1 2 3 4 5Days from Procedure or Surgery
-5 -4 -3 -2 -1 0 1 2 3 4 5Days from Procedure or Surgery
Antic
oagu
latio
n Eff
ect
Antic
oagu
latio
n Eff
ectEarly Transition Off Heparin Non-Pharmacologic Anti-Thrombosis
WarfarinHeparin
WarfarinAmbulation, compressiondevices, etc.
I J
-5 -4 -3 -2 -1 0 1 2 3 4 5Days from Procedure or Surgery
Antic
oagu
latio
n Eff
ect Novel Oral Anticoagulant Interruption
NOAC
K
Warfarin interruption produces an anticoagulation gap (A). Various strategies (C to K) attempt to emulate a theoretical ideal bridge (B). See text for
discussion. INR ¼ international normalized ratio; NOAC ¼ novel oral anticoagulant.
J A C C V O L . 6 6 , N O . 1 2 , 2 0 1 5 Rechenmacher and FangS E P T E M B E R 2 2 , 2 0 1 5 : 1 3 9 2 – 4 0 3 Bridging Anticoagulation
1399
Downloa
issues. PERIOP2 (A Double Blind Randomized ControlTrial of Post-Operative Low Molecular WeightHeparin Bridging Therapy Versus Placebo BridgingTherapy for Patients Who Are at High Risk for ArterialThromboembolism; NCT00432796) is a placebo-controlled, double-blinded, multicenter Canadianstudy that is randomizing moderately high-risk pa-tients with mechanical heart valves and atrial fibril-lation to dalteparin or placebo for perioperativebridging. The primary endpoint is any major TEevent, including stroke, myocardial infarction, sys-temic embolism, valve thrombosis, VTE, or vasculardeath.
A CONTEMPORARY APPROACH
Using the cumulative available data, our approach toperiprocedural anticoagulation is detailed in thefollowing text (Central Illustration, Figure 3).
First and foremost, whenever possible, avoid in-terrupting OAC (Central Illustration, Figures 3C and 3D).
ded From: http://content.onlinejacc.org/ by James Januzzi on 09
Candidates for uninterrupted OAC are those patientsat moderate or high risk for TE and who are under-going a reasonably low bleeding risk procedure(Table 2). To avoid unnecessary bleeding with unin-terrupted OAC, also consider a lower periproceduralINR goal of 2.0 (Figure 3D).
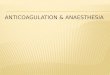
If OAC interruption is necessary, avoid bridgingpatients (Figure 3A) at low or moderate risk for TE(Table 1) (5) as long as other individualized risks (i.e.,existing left atrial appendage thrombus or activecancer) do not exist. Patient-specific bleeding riskshould also be assessed to help guide anticoagulationdecisions. One approach is to use bleeding risk cal-culators such as a BleedMAP score (1,27). This modelwas derived by retrospectively analyzing 2,484 peri-procedural OAC interruptions through the MayoClinic Thrombophilia Center from 1997 to 2007 (41).BleedMAP assigns a point for each of the following:prior bleeding (Bleed), mechanical mitral valve(M), active cancer (A), and low platelets (P). Higherscores portend higher perioperative bleeding risk.
/22/2015

FIGURE 4 Major Event Rates by BleedMAP Score
12
8
4
00 1—2 ≥3
BleedMAP Score
Rates of Major Hemorrhage
All patientsBridged
Rates of Thromboembolism
All patientsBridged
1.2
0.8
0.4
00 1—2 ≥3
BleedMAP Score
A
B
A higher BleedMAP score correlated with increased bleeding both in patients receiving
bridging anticoagulation (salmon) and in all patients (blue) (A). Thromboembolism did not
occur with high BleedMAP scores and was rare in general (B). Reprinted with permission
from Tafur et al. (41).
Rechenmacher and Fang J A C C V O L . 6 6 , N O . 1 2 , 2 0 1 5
Bridging Anticoagulation S E P T E M B E R 2 2 , 2 0 1 5 : 1 3 9 2 – 4 0 3
1400
Downloaded From: http://co
Conveniently, higher BleedMAP scores also correlatewith lower TE rates (Figure 4).
The net clinical benefit of bridging patients at“high risk” for TE (Table 1) remains unknown and is notyet supported by clinical trial evidence. It should benoted that observational data has yet to demonstratethat bridging meaningfully reduces TE events, evenin populations with high TE risk (2,10,12,16). Incontrast, excessive hemorrhagic events have beenwell described. However, until clinical trial evidenceis available, we recommend following guideline re-commendations to consider individualizing bridginganticoagulation in specific high-risk patients (Table 4).For example, it might be reasonable to considerbridging in those with an unacceptably high TE risk(i.e., active or recent arterial TE or mechanical mitral
ntent.onlinejacc.org/ by James Januzzi on 09/22/2015
valve), with a reasonably low bleeding risk, and whorequire OAC interruption for more than a few days at atime (Central Illustration). Limited data suggest thatmechanical valves at high risk for TE (i.e., mechanicalmitral valves or tilting disc valves) may exhibit arelatively favorable bleeding-to-thrombosis profilewhen bridged. However, these data are retrospective(11,14). Whether or not to bridge patients with atrialfibrillation and a high CHADS2 score remains unclear;PERIOP2 may help clarify this question. Althoughwe generally support the current guidelines in high-risk patient groups, until further evidence is moredefinitive, we strongly encourage providers to care-fully assess bleeding risk in the context of poorlydefined thrombotic risk during the OAC interruptionperiod.
When bridging is deemed necessary, more conser-vative bridging strategies should be entertained,such as low-dose heparin (Figure 3F) (42), post-procedure–only heparin (Figure 3G), delayed initia-tion of post-procedure heparin (Figure 3H), and earlytransitioning off of heparin as the INR approaches 2.0,rather than after (Figure 3I) (5,15,42–44). Health careproviders should also consider nonpharmacologicalapproaches (i.e., ambulation and compression stock-ings) to reduce thrombotic risk when OAC interrup-tion is necessary (Figure 3J). Bleeding avoidancestrategies and nonpharmacological approaches can beeffective (45).
NOVEL ANTICOAGULANTS IN THE
PERIPROCEDURAL PERIOD
Novel oral anticoagulants (NOACs) will be increasinglyencountered in periprocedural scenarios. NOACs arepoised to replace warfarin for the treatment of atrialfibrillation and VTE (1,46). Multiple investigatorshave reviewed perioperative NOACs interruptions inatrial fibrillation populations (27,28,47–49). NOACinterruptions occurred frequently in the RE-LY(Randomized Evaluation of Long Term AnticoagulantTherapy With Dabigatran Etexilate), ROCKET-AF(Rivaroxaban Once-Daily, Oral, Direct Factor Xa In-hibition Compared With Vitamin K Antagonism forPrevention of Stroke and Embolism Trial in AtrialFibrillation), and ARISTOTLE (Apixaban for Reduc-tion in Stroke and Other Thromboembolic Eventsin Atrial Fibrillation) studies—25%, 33%, and 34%,respectively. Patients in these large trials did notexperience increased TE or bleeding events peri-operatively, whether bridged or unbridged—eventhose undergoing major or urgent surgical pro-cedures (28,48). Given their pharmacokinetic simi-larities to low molecular-weight heparins (Figure 3K),
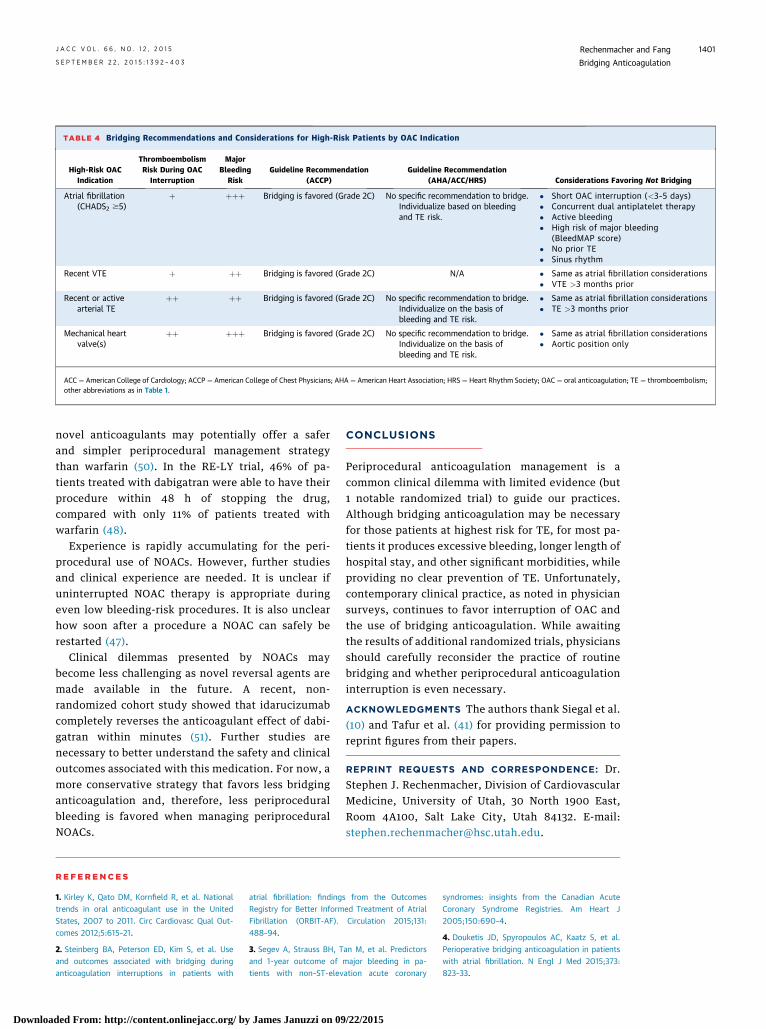
TABLE 4 Bridging Recommendations and Considerations for High-Risk Patients by OAC Indication
High-Risk OACIndication
ThromboembolismRisk During OAC
Interruption
MajorBleeding
RiskGuideline Recommendation
(ACCP)Guideline Recommendation
(AHA/ACC/HRS) Considerations Favoring Not Bridging
Atrial fibrillation(CHADS2 $5)
þ þþþ Bridging is favored (Grade 2C) No specific recommendation to bridge.Individualize based on bleedingand TE risk.
� Short OAC interruption (<3–5 days)� Concurrent dual antiplatelet therapy� Active bleeding� High risk of major bleeding
(BleedMAP score)� No prior TE� Sinus rhythm
Recent VTE þ þþ Bridging is favored (Grade 2C) N/A � Same as atrial fibrillation considerations� VTE >3 months prior
Recent or activearterial TE
þþ þþ Bridging is favored (Grade 2C) No specific recommendation to bridge.Individualize on the basis ofbleeding and TE risk.
� Same as atrial fibrillation considerations� TE >3 months prior
Mechanical heartvalve(s)
þþ þþþ Bridging is favored (Grade 2C) No specific recommendation to bridge.Individualize on the basis ofbleeding and TE risk.
� Same as atrial fibrillation considerations� Aortic position only
ACC ¼ American College of Cardiology; ACCP ¼ American College of Chest Physicians; AHA ¼ American Heart Association; HRS ¼ Heart Rhythm Society; OAC ¼ oral anticoagulation; TE ¼ thromboembolism;other abbreviations as in Table 1.
J A C C V O L . 6 6 , N O . 1 2 , 2 0 1 5 Rechenmacher and FangS E P T E M B E R 2 2 , 2 0 1 5 : 1 3 9 2 – 4 0 3 Bridging Anticoagulation
1401
Downloa
novel anticoagulants may potentially offer a saferand simpler periprocedural management strategythan warfarin (50). In the RE-LY trial, 46% of pa-tients treated with dabigatran were able to have theirprocedure within 48 h of stopping the drug,compared with only 11% of patients treated withwarfarin (48).
Experience is rapidly accumulating for the peri-procedural use of NOACs. However, further studiesand clinical experience are needed. It is unclear ifuninterrupted NOAC therapy is appropriate duringeven low bleeding-risk procedures. It is also unclearhow soon after a procedure a NOAC can safely berestarted (47).
Clinical dilemmas presented by NOACs maybecome less challenging as novel reversal agents aremade available in the future. A recent, non-randomized cohort study showed that idarucizumabcompletely reverses the anticoagulant effect of dabi-gatran within minutes (51). Further studies arenecessary to better understand the safety and clinicaloutcomes associated with this medication. For now, amore conservative strategy that favors less bridginganticoagulation and, therefore, less periproceduralbleeding is favored when managing periproceduralNOACs.
ded From: http://content.onlinejacc.org/ by James Januzzi on 09
CONCLUSIONS
Periprocedural anticoagulation management is acommon clinical dilemma with limited evidence (but1 notable randomized trial) to guide our practices.Although bridging anticoagulation may be necessaryfor those patients at highest risk for TE, for most pa-tients it produces excessive bleeding, longer length ofhospital stay, and other significant morbidities, whileproviding no clear prevention of TE. Unfortunately,contemporary clinical practice, as noted in physiciansurveys, continues to favor interruption of OAC andthe use of bridging anticoagulation. While awaitingthe results of additional randomized trials, physiciansshould carefully reconsider the practice of routinebridging and whether periprocedural anticoagulationinterruption is even necessary.
ACKNOWLEDGMENTS The authors thank Siegal et al.(10) and Tafur et al. (41) for providing permission toreprint figures from their papers.
REPRINT REQUESTS AND CORRESPONDENCE: Dr.Stephen J. Rechenmacher, Division of CardiovascularMedicine, University of Utah, 30 North 1900 East,Room 4A100, Salt Lake City, Utah 84132. E-mail:[email protected].
RE F E RENCE S
1. Kirley K, Qato DM, Kornfield R, et al. Nationaltrends in oral anticoagulant use in the UnitedStates, 2007 to 2011. Circ Cardiovasc Qual Out-comes 2012;5:615–21.
2. Steinberg BA, Peterson ED, Kim S, et al. Useand outcomes associated with bridging duringanticoagulation interruptions in patients with
atrial fibrillation: findings from the OutcomesRegistry for Better Informed Treatment of AtrialFibrillation (ORBIT-AF). Circulation 2015;131:488–94.
3. Segev A, Strauss BH, Tan M, et al. Predictorsand 1-year outcome of major bleeding in pa-tients with non–ST-elevation acute coronary
/22/2015
syndromes: insights from the Canadian AcuteCoronary Syndrome Registries. Am Heart J2005;150:690–4.
4. Douketis JD, Spyropoulos AC, Kaatz S, et al.Perioperative bridging anticoagulation in patientswith atrial fibrillation. N Engl J Med 2015;373:823–33.

Rechenmacher and Fang J A C C V O L . 6 6 , N O . 1 2 , 2 0 1 5
Bridging Anticoagulation S E P T E M B E R 2 2 , 2 0 1 5 : 1 3 9 2 – 4 0 3
1402
Downloaded From: http://co
5. Douketis JD, Spyropoulos AC, Spencer FA, et al.Perioperative management of antithrombotictherapy: antithrombotic therapy and prevention ofthrombosis, 9th ed: American College of ChestPhysicians evidence-based clinical practice guide-lines. Chest 2012;141:e326S–50S.
6. January CT, Wann LS, Alpert JS, et al. 2014AHA/ACC/HRS guideline for the management ofpatients with atrial fibrillation: a report of theAmerican College of Cardiology/American HeartAssociation Task Force on Practice Guidelines andthe Heart Rhythm Society. J Am Coll Cardiol 2014;64:e1–76.
7. Douketis JD, Crowther MA, Cherian SS,Kearon CB. Physician preferences for perioperativeanticoagulation in patients with a mechanicalheart valve who are undergoing elective noncar-diac surgery. Chest 1999;116:1240–6.
8. Brotman DJ, Streiff MB. Overuse of bridginganticoagulation for patients with venous throm-boembolism: first, do no harm. JAMA Intern Med2015;175:1169–70.
9. Shaikh AY, McManus DD. A bridge too far?Findings of bridging anticoagulation use and out-comes in the Outcomes Registry for BetterInformed Treatment of Atrial Fibrillation (ORBIT-AF). Circulation 2015;131:448–50.
10. Siegal D, Yudin J, Kaatz S, et al. Periproceduralheparin bridging in patients receiving vitamin Kantagonists: systematic review and meta-analysisof bleeding and thromboembolic rates. Circula-tion 2012;126:1630–9.
11. Wysokinski WE, McBane RD II. Periproceduralbridging management of anticoagulation. Circula-tion 2012;126:486–90.
12. Clark NP, Witt DM, Davies LE, et al. Bleeding,recurrent venous thromboembolism, and mortalityrisks during warfarin interruption for invasiveprocedures. JAMA Intern Med 2015;175:1163–8.
13. Garcia DA, Regan S, Henault LE, et al. Risk ofthromboembolism with short-term interruption ofwarfarin therapy. Arch Intern Med 2008;168:63–9.
14. Cavalcanti R, Rosenbaum B, Benzel E,Varma N. “Safe period” of anticoagulation with-drawal in patients with mechanical heart valve(s).J Am Coll Cardiol 2015;65 Suppl 10:A2035.
15. Jaffer AK, Brotman DJ, Bash LD, et al. Varia-tions in perioperative warfarin management: out-comes and practice patterns at nine hospitals. AmJ Med 2010;123:141–50.
16. Dunn AS, Turpie AG. Perioperative manage-ment of patients receiving oral anticoagulants: asystematic review. Arch Intern Med 2003;163:901–8.
17. Schouten O, van Domburg RT, Bax JJ, et al.Noncardiac surgery after coronary stenting: earlysurgery and interruption of antiplatelet therapyare associated with an increase in major adversecardiac events. J Am Coll Cardiol 2007;49:122–4.
18. Manchikanti L, Benyamin RM, Swicegood JR,et al. Assessment of practice patterns ofperioperative management of antiplatelet andanticoagulant therapy in interventional pain man-agement. Pain Physician 2012;15:E955–68.
ntent.onlinejacc.org/ by James Januzzi on 0
19. Kirkorian AY, Moore BL, Siskind J, Marmur ES.Perioperative management of anticoagulant ther-apy during cutaneous surgery: 2005 survey ofMohs surgeons. Dermatol Surg 2007;33:1189–97.
20. Birnie DH, Healey JS, Wells GA, et al. Pace-maker or defibrillator surgery without interruptionof anticoagulation. N Engl J Med 2013;368:2084–93.
21. Coyle D, Coyle K, Essebag V, et al. Costeffectiveness of continued-warfarin versusheparin-bridging therapy during pacemaker anddefibrillator surgery. J Am Coll Cardiol 2015;65:957–9.
22. Rhodes DA, Severson EP, Hodrick JT, et al.Discontinuation of warfarin is unnecessary in totalknee arthroplasty. Clin Orthop Relat Res 2010;468:120–6.
23. Bajkin BV, Popovic SL, Selakovic SD. Ran-domized, prospective trial comparing bridgingtherapy using low-molecular-weight heparin withmaintenance of oral anticoagulation duringextraction of teeth. J Oral Maxillofac Surg 2009;67:990–5.
24. Di Biase L, Burkhardt JD, Santangeli P, et al.Periprocedural stroke and bleeding complicationsin patients undergoing catheter ablation of atrialfibrillation with different anticoagulation man-agement: results from the Role of Coumadin inPreventing Thromboembolism in Atrial Fibrillation(AF) Patients Undergoing Catheter Ablation(COMPARE) randomized trial. Circulation 2014;129:2638–44.
25. Cheng A, Nazarian S, Brinker JA, et al.Continuation of warfarin during pacemaker orimplantable cardioverter-defibrillator implanta-tion: a randomized clinical trial. Heart Rhythm2011;8:536–40.
26. Azoulay L, Dell’Aniello S, Simon TA, Renoux C,Suissa S. Initiation of warfarin in patients withatrial fibrillation: early effects on ischaemicstrokes. Eur Heart J 2014;35:1881–7.
27. Patel MR, Hellkamp AS, Lokhnygina Y, et al.Outcomes of discontinuing rivaroxaban comparedwith warfarin in patients with nonvalvular atrialfibrillation: analysis from the ROCKET AF trial(Rivaroxaban Once-Daily, Oral, Direct Factor XaInhibition Compared With Vitamin K Antagonismfor Prevention of Stroke and Embolism Trial inAtrial Fibrillation). J Am Coll Cardiol 2013;61:651–8.
28. Douketis JD, Healey JS, Brueckmann M, et al.Perioperative bridging anticoagulation duringdabigatran or warfarin interruption among pa-tients who had an elective surgery or procedure.Substudy of the RE-LY trial. Thromb Haemost2015;113:625–32.
29. Douketis JD. Perioperative anticoagulationmanagement in patients who are receiving oralanticoagulant therapy: a practical guide for clini-cians. Thromb Res 2002;108:3–13.
30. Stehlik J, Johnson SA, Selzman CH. Goldstandard in anticoagulation assessment of leftventricular assist device patients? How aboutbronze. J Am Coll Cardiol HF 2015;3:323–6.
31. Boyle AJ, Russell SD, Teuteberg JJ, et al. Lowthromboembolism and pump thrombosis with theHeartMate II left ventricular assist device: analysis
9/22/2015
of outpatient anti-coagulation. J Heart LungTransplant 2009;28:881–7.
32. Slaughter MS, Naka Y, John R, et al.Post-operative heparin may not be requiredfor transitioning patients with a HeartMate IIleft ventricular assist system to long-termwarfarin therapy. J Heart Lung Transplant 2010;29:616–24.
33. Prandoni P, Trujillo-Santos J, Sanchez-Cantalejo E, et al. Major bleeding as a predictor ofmortality in patients with venous thromboembo-lism: findings from the RIETE Registry. J ThrombHaemost 2010;8:2575–7.
34. Smoyer-Tomic K, Siu K, Walker DR, et al.Anticoagulant use, the prevalence of bridging,and relation to length of stay among hospitalizedpatients with non-valvular atrial fibrillation. Am JCardiovasc Drugs 2012;12:403–13.
35. Chatterjee S, Wetterslev J, Sharma A, et al.Association of blood transfusion with increasedmortality in myocardial infarction: a meta-analysisand diversity-adjusted study sequential analysis.JAMA Intern Med 2013;173:132–9.
36. Mehran R, Pocock S, Nikolsky E, et al. Impactof bleeding on mortality after percutaneous cor-onary intervention results from a patient-levelpooled analysis of the REPLACE-2 (RandomizedEvaluation of PCI Linking Angiomax to ReducedClinical Events), ACUITY (Acute Catheterizationand Urgent Intervention Triage Strategy), andHORIZONS-AMI (Harmonizing Outcomes WithRevascularization and Stents in Acute MyocardialInfarction) trials. J Am Coll Cardiol Intv 2011;4:654–64.
37. Stone GW, Clayton TC, Mehran R, et al.Impact of major bleeding and blood transfusionsafter cardiac surgery: analysis from the AcuteCatheterization and Urgent Intervention TriagestrategY (ACUITY) trial. Am Heart J 2012;163:522–9.
38. Pinho-Costa L, Moreira S, Azevedo C, et al.APOLLO I: anticoagulation control in atrial fibril-lation. Rev Port Cardiol 2015;34:337–45.
39. Nelson WW, Desai S, Damaraju CV, et al. In-ternational normalized ratio stability in warfarin-experienced patients with nonvalvular atrialfibrillation. Am J Cardiovasc Drugs 2015;15:205–11.
40. Aguilar MI, Hart R. Oral anticoagulants forpreventing stroke in patients with non-valvularatrial fibrillation and no previous history ofstroke or transient ischemic attacks. CochraneDatabase Syst Rev 2005:CD001927.
41. Tafur AJ, McBane R 2nd, Wysokinski WE, et al.Predictors of major bleeding in peri-proceduralanticoagulation management. J Thromb Haemost2012;10:261–7.
42. Malato A, Saccullo G, Lo Coco L, et al. Patientsrequiring interruption of long-term oral anti-coagulant therapy: the use of fixed sub-therapeutic doses of low-molecular-weightheparin. J Thromb Haemost 2010;8:107–13.
43. Skeith L, Taylor J, Lazo-Langner A, Kovacs MJ.Conservative perioperative anticoagulation man-agement in patients with chronic venous throm-boembolic disease: a cohort study. J ThrombHaemost 2012;10:2298–304.

J A C C V O L . 6 6 , N O . 1 2 , 2 0 1 5 Rechenmacher and FangS E P T E M B E R 2 2 , 2 0 1 5 : 1 3 9 2 – 4 0 3 Bridging Anticoagulation
1403
Downloa
44. Deerhake JP, Merz JC, Cooper JV, et al. Theduration of anticoagulation bridging therapy inclinical practice may significantly exceed thatobserved in clinical trials. J Thromb Thrombolysis2007;23:107–13.
45. Marso SP, Amin AP, House JA, et al. Associa-tion between use of bleeding avoidance strategiesand risk of periprocedural bleeding amongpatients undergoing percutaneous coronaryintervention. JAMA 2010;303:2156–64.
46. Yeh CH, Gross PL, Weitz JI. Evolving useof new oral anticoagulants for treatmentof venous thromboembolism. Blood 2014;124:1020–8.
ded From: http://content.onlinejacc.org/ by
47. Healey JS, Brambatti M. Periprocedural man-agement of oral anticoagulation in patients withatrial fibrillation: approach in the era of new oralanticoagulants. Can JCardiol 2013;29 7Suppl:S54–9.
48. Healey JS, Eikelboom J, Douketis J, et al.Periprocedural bleeding and thromboembolicevents with dabigatran compared with warfarin:results from the Randomized Evaluation of Long-Term Anticoagulation Therapy (RE-LY) random-ized trial. Circulation 2012;126:343–8.
49. Granger CB, Lopes RD, Hanna M, et al. Clinicalevents after transitioning from apixaban versuswarfarin to warfarin at the end of the Apixaban forReduction in Stroke and Other Thromboembolic
James Januzzi on 09/22/2015
Events in Atrial Fibrillation (ARISTOTLE) trial. AmHeart J 2015;169:25–30.
50. Schulman S, Carrier M, Lee AY, et al. Periop-erative management of dabigatran: a prospectivecohort study. Circulation 2015;132:167–73.
51. Pollack CV Jr., Reilly PA, Eikelboom J, et al. Idar-ucizumab for dabigatran reversal. N Engl JMed 2015;373:511–20.
KEY WORDS bleeding, bridging,perioperative, periprocedural,thromboembolism