Embed Size (px)
Citation preview
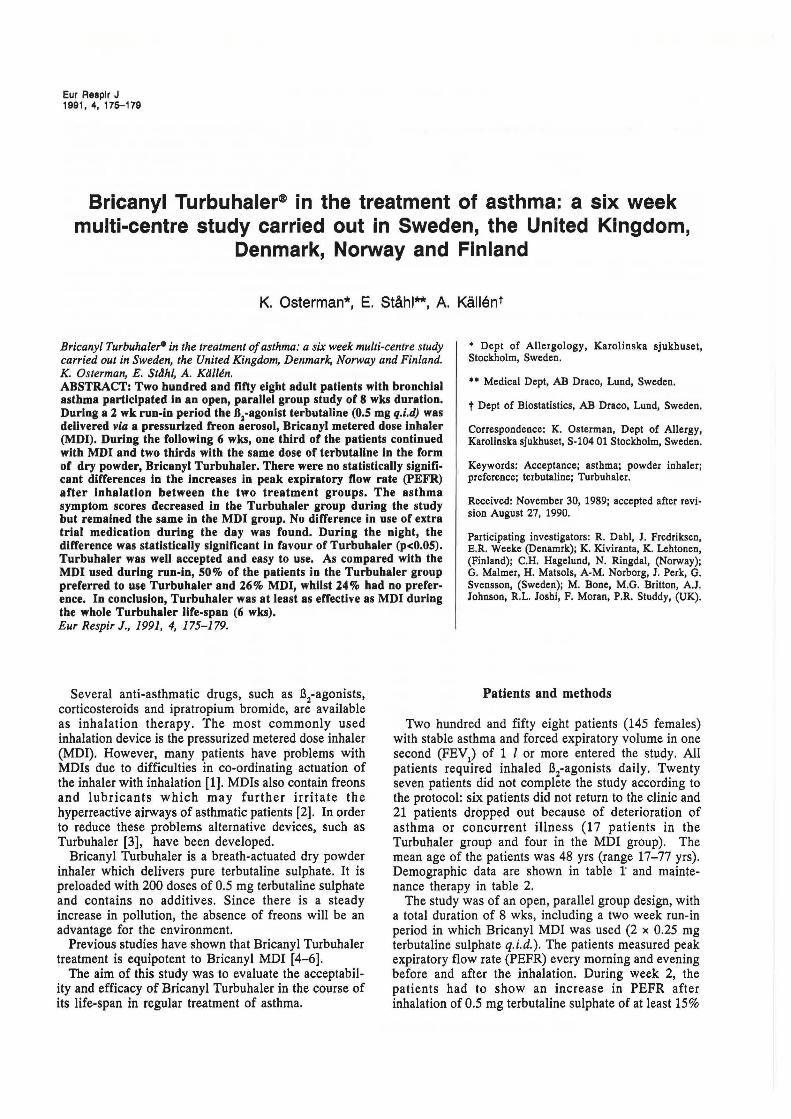
Eur Resplr J 1991, 4, 175--179
Bricanyl Turbuhaler® in the treatment of asthma: a six week multi-centre study carried out in Sweden, the United Kingdom,
Denmark, Norway and Finland
K. Osterman*, E. StAhl**, A. Kallent
Bricanyl Turbuhaler* in the treatment of asthma: a six week multi-centre study carried out in Sweden, the United Kingdom, Denmark, Norway and Finland. K. Osterman, E. Stdhl, A. Kiillen. ABSTRACT: Two hundred and fifty eight adult patients with bronchial asthma participated In an open, parallel group study of 8 wks duration. During a 2 wk run-in period the 8
3-agonlst terbutaline (0.5 mg q.i.d) was
delivered via a pressurized freon aerosol, Bricanyl metered dose inhaler (MDI). During the following 6 wks, one third of the patients continued with MDI and two thirds with the same dose of terbutallne in the form of dry powder, Bricanyl Turbuhaler. There were no statistically significant differences in the increases in peak expiratory flow rate (PEFR) after inhalation between the two treatment groups. The asthma symptom scores decreased in the Turbuhaler group during the study but remained the same in the MDI group. No difference in use of extra trial medication during the day was found. During the night, the difference was statistically significant in favour of Turbuhaler (p<O.OS). Turbuhaler was well accepted and easy to use. As compared with the MDI used during run-in, SO% of the patients in the Turbubaler group preferred to use Turbubaler and 26% MDI, whilst 24% had no preference. In conclusion, Turbuhaler was at least as effective as MDI during the whole Turbuhaler life-span (6 wks). Eur Respir J., 1991, 4, 175-179.
• Dept of Allergology, Karolinska sjukhuset, Stockholm, Sweden.
• • Medical Dept, AB Draco, Lund, Sweden.
t Dept of Biostatistics, AB Draco, Lund, Sweden.
Correspondence: K. Osterman, Dept of Allergy, Karolinska sjukhuset, S-104 01 Stockholm, Sweden.
Keywords: Acceptance; asthma; powder inhaler; preference; terbutaline; Turbuhaler.
Received: November 30, 1989; accepted after revision August 27, 1990.
Participating investigators: R. Dahl, J. Fredriksen, E.R. Weeke (Denamrk); K. Kiviranta, K. Lehtonen, (Finland); C.H. Hagelund, N. Ringdal, (Norway); G. Malmer, H. Matsols, A-M. Norborg, J. Perk, G. Svensson, (Sweden); M. Bone, M.G. Britton, A.J. Johnson, R.L. Joshi, F. Moran, P.R. Studdy, (UK).
Patients and methods Several anti-asthmatic drugs, such as 132-agonists,
corticosteroids and ipratropium bromide, are available as inhalation therapy. The most commonly used inhalation device is the pressurized metered dose inhaler (MDI). However, many patients have problems with MDis due to difficulties in co-ordinating actuation of the inhaler with inhalation [1]. MDis also contain freons and lubricants which may further irritate the hyperreactive airways of asthmatic patients [2]. In order to reduce these problems alternative devices, such as Turbuhaler [3], have been developed.
Bricanyl Turbuhaler is a breath-actuated dry powder inhaler which delivers pure terbutaline sulphate. It is preloaded with 200 doses of 0.5 mg terbutaline sulphate and contains no additives. Since there is a steady increase in pollution, the absence of freons will be an advantage for the environment.
Two hundred and fifty eight patients (145 females) with stable asthma and forced expiratory volume in one second (FEV
1) of 1 l or more entered the study. All
patients required inhaled 132-agonists daily. Twenty seven patients did not complete the study according to the protocol: six patients did not return to the clinic and 21 patients dropped out because of deterioration of asthma or concurrent illness (17 patients in the Turbuhaler group and four in the MDI group). The mean age of the patients was 48 yrs (range 17-77 yrs). Demographic data are shown in table t and maintenance therapy in table 2.
Previous studies have shown that Bricanyl Turbuhaler treatment is equipotent to Bricanyl MDI [4-6].
The aim of this study was to evaluate the acceptability and efficacy of Bricanyl Turbuhaler in the course of its life-span in regular treatment of asthma.
The study was of an open, parallel group design, with a total duration of 8 wks, including a two week run-in period in which Bricanyl MDI was used (2 x 0.25 mg terbutaline sulphate q. i.d. ). The patients measured peak expiratory flow rate (PEFR) every morning and evening before and after the inhalation. During week 2, the patients had to show an increase in PEFR after inhalation of 0.5 mg terbutaline sulphate of at least 15%
176 K. OSTERMAN, E. STAHL, A. KALIEN
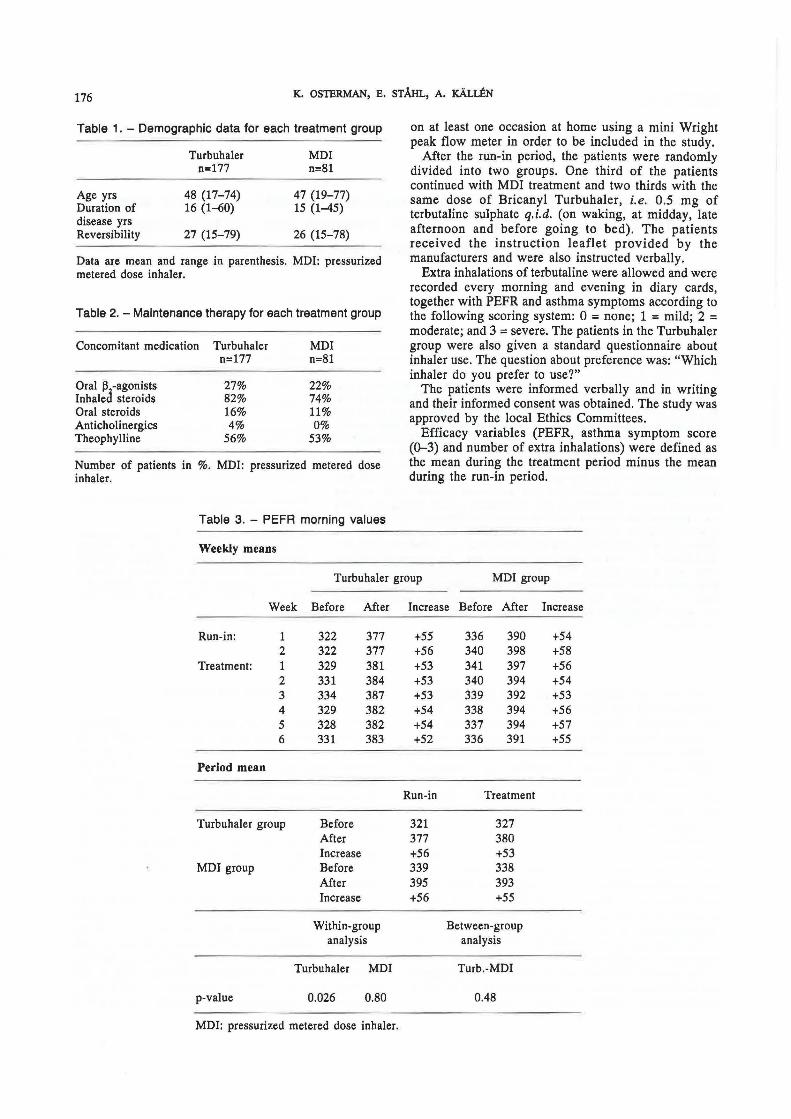
Table 1. - Demographic data for each treatment group
Turbuhaler MDI n=177 n=81
Age yrs 48 (17-74) 47 (19-77) Duration of 16 (1-60) 15 (1-45) disease yrs Reversibility 27 (15-79) 26 (15-78)
Data are mean and range in parenthesis. MDI: pressurized metered dose inhaler.
Table 2. - Maintenance therapy for each treatment group
Concomitant medication Turbuhaler MDI n=177 n=81
Oral j3 -agonists 27% 22% Inhaled steroids 82% 74% Oral steroids 16% 11% Anticholinergics 4% 0% Theophylline 56% 53%
Number of patients in %. MDI: pressurized metered dose inhaler.
Table 3. - PEFR morning values
Weekly means
on at least one occasion at home using a mini Wright peak flow meter in order to be included in the study.
After the run-in period, the patients were randomly divided into two groups. One third of the patients continued with MDI treatment and two thirds with the same dose of Bricanyl Turbuhaler, i.e. 0.5 mg of terbutaline sulphate q.i.d. (on waking, at midday, late afternoon and before going to bed). The patients received the instruction leaflet provided by the manufacturers and were also instructed verbally.
Extra inhalations of terbutaline were allowed and were recorded every morning and evening in diary cards, together with PEFR and asthma symptoms according to the following scoring system: 0 = none; 1 = mild; 2 = moderate; and 3 = severe. The patients in the Turbuhaler group were also given a standard questionnaire about inhaler use. The question about preference was: "Which inhaler do you prefer to use?"
The patients were informed verbally and in writing and their informed consent was obtained. The study was approved by the local Ethics Committees.
Efficacy variables (PEFR, asthma symptom score (0--3) and number of extra inhalations) were defined as the mean during the treatment period minus the mean during the run-in period.
Turbuhaler group MDI group
Week Before After Increase Before After Increase
Run-in: 1 322 377 +55 336 390 +54 2 322 377 +56 340 398 +58
Treatment: 1 329 381 +53 341 397 +56 2 331 384 +53 340 394 +54 3 334 387 +53 339 392 +53 4 329 382 +54 338 394 +56 5 328 382 +54 337 394 +57 6 331 383 +52 336 391 +55
Period mean
Run-in Treatment
Turbuhaler group Before 321 327 After 377 380 Increase +56 +53
MDI group Before 339 338 After 395 393 Increase +56 +55
Within-group Between-group analysis analysis
Turbuhaler MDI Turb.-MDI
p-value 0.026 0.80 0.48
MDI: pressurized metered dose inhaler.
A SIX WEEK TREATMENT WITII BRICANYL TURBUHALER 177
PEFR
Run-In Treatment
350
325
300
275 8 15 22 29 36 43 50 Day a
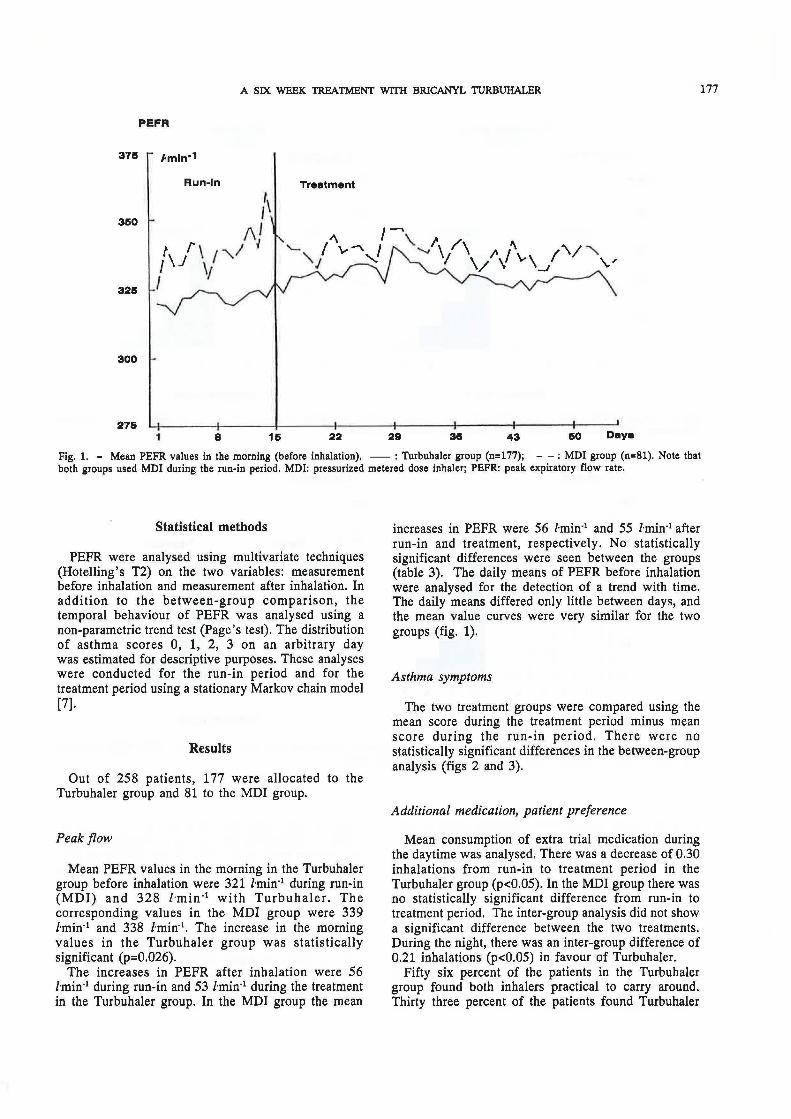
Fig. 1. - Mean PEFR values in the morning (before inhalation). - : Turbuhaler group (n=177); - - : MDI group (n=Sl). Note that both groups used MDI during the run-in period. MDI: pressurized metered dose inhaler; PEFR: peak expiratory flow rate.
Statistical methods
PEFR were analysed using multivariate techniques (Hotelling's T2) on the two variables: measurement before inhalation and measurement after inhalation. In addition to the between-group comparison, the temporal behaviour of PEFR was analysed using a non-parametric trend test (Page's test). The distribution of asthma scores 0, 1, 2, 3 on an arbitrary day was estimated for descriptive purposes. These analyses were conducted for the run-in period and for the treatment period using a stationary Markov chain model [7].
Results
Out of 258 patients, 177 were allocated to the Turbuhaler group and 81 to the MDI group.
Peak flow
Mean PEFR values in the morning in the Turbuhaler group before inhalation were 321 lmin·1 during run-in (MDI) and 328 l·min·1 with Turbuhaler. The corresponding values in the MDI group were 339 lmin·1 and 338 Z.min·1• The increase in the morning values in the Turbuhaler group was statistically significant (p=0.026).
The increases in PEFR after inhalation were 56 Z.min·1 during run-in and 53 lmin·1 during the treatment in the Turbuhaler group. In the MDI group the mean
increases in PEFR were 56 lmin·1 and 55 lmin·1 after run-in and treatment, respectively. No statistically significant differences were seen between the groups (table 3). The daily means of PEFR before inhalation were analysed for the detection of a trend with time. The daily means differed only little between days, and the mean value curves were very similar for the two groups (fig. 1).
Asthma symptoms
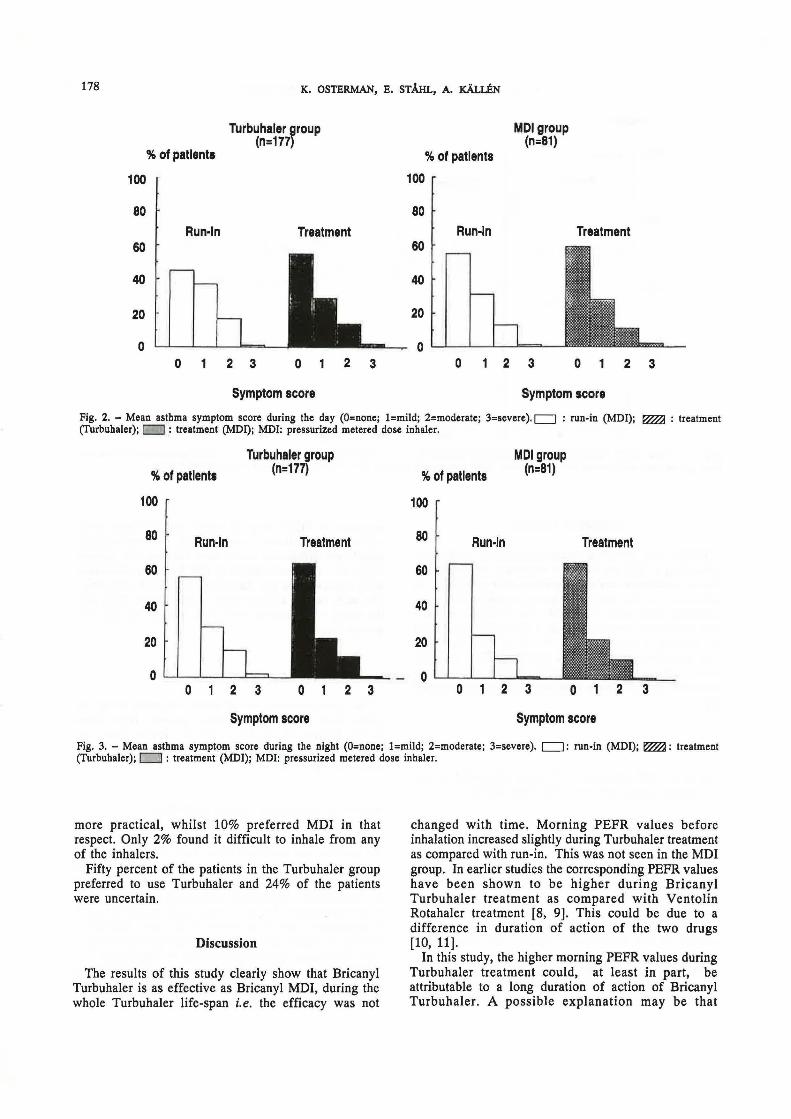
The two treatment groups were compared using the mean score during the treatment period minus mean score during the run-in period. There were no statistically significant differences in the between-group analysis (figs 2 and 3).
Additional medication, patient preference
Mean consumption of extra trial medication during the daytime was analysed. There was a decrease of 0.30 inhalations from run-in to treatment period in the Turbuhaler group (p<0.05). In the MDI group there was no statistically significant difference from run-in to treatment period. The inter-group analysis did not show a significant difference between the two treatments. During the night, there was an inter-group difference of 0.21 inhalations (p<0.05) in favour of Turbuhaler.
Fifty six percent of the patients in the Turbuhaler group found both inhalers practical to carry around. Thirty three percent of the patients found Turbuhaler
178 K. OSTERMAN, E. STAin., A. KALI.EN
Turbuhaler roup MOl group (n=177 (n=81)
% of patients % of patients
100 100
80 80
Run-In Treatment Run-In Treatment 60 60
40 40
20 20
0 0 0 1 2 3 0 2 3 0 1 2 3 0 1 2 3
Symptom score Symptom score
Fig. 2. - Mean asthma symptom score during the day (O=none; l=mild; 2=moderate; 3=severe). CJ : run-in (MDI); ~ : treatment (Turbuhaler); [=:J : treatment (MDI); MDI: pressurized metered dose inhaler.
% of patients
100
80 Run-In
60
40
20
0 0
Turbuhaler group (n=177)
Treatment
2 3 0 2 3
Symptom score
MOl group
% of patients (n=81)
100
80 Run-In Treatment
60
40
20
0 0 1 2 3 0 2 3
Symptom score
Fig. 3. - Mean asthma symptom score during the night (O=none; l=mild; 2=moderate; 3=severe). c::::J: run-in (MDI); ~: treatment (Turbuhaler); r.::::;J : treatment (MDI); MDI: pressurized metered dose inhaler.
more practical, whilst 10% preferred MDI in that respect. Only 2% found it difficult to inhale from any of the inhalers.
Fifty percent of the patients in the Turbuhaler group preferred to use Turbuhaler and 24% of the patients were uncertain.
Discussion
The results of this study clearly show that Bricanyl Turbuhaler is as effective as Bricanyl MDI, during the whole Turbuhaler life-span i.e. the efficacy was not
changed with time. Morning PEFR values before inhalation increased slightly during Turbuhaler treatment as compared with run-in. This was not seen in the MDI group. In earlier studies the corresponding PEFR values have been shown to be higher during Bricanyl Turbuhaler treatment as compared with Ventolin Rotahaler treatment [8, 9]. This could be due to a difference in duration of action of the two drugs [10, 11].
In this study, the higher morning PEFR values during Turbuhaler treatment could, at least in part, be attributable to a long duration of action of Bricanyl Turbuhaler. A possible explanation may be that

A SIX WEEK TREATMENT WITH BRICANYL TURBUHALER 179
Turbuhaler is easier to use [12] and therefore more drug can reach the airways.
The reduction in asthma symptoms score and need for extra inhalations in the present study also indicate a favourable duration of action of Bricanyl Turbuhaler.
However, since this was an open study it can not be excluded that the improvement in lung function as well as in asthma symptoms during Turbuhaler treatment in the present study, could be due to patient expectation of the new inhaler.
Turbuhaler was well accepted by the patients, which is in agreement with a previous study [12]. Turbuhaler was preferred by twice as many patients as MDI in the present study. This is in accordance with the results from previous studies [13, 14].
In conclusion, this study showed that Bricanyl Turbuhaler is an effective and well accepted treatment in the long-term therapy of asthma. The preferences, asthma symptom scores and reduced need for extra inhalations all show a tendency in favour of Bricanyl Turbuhaler compared with Bricanyl MDI.
References
1. Crompton GK. - Problems patients have using pressurized aerosol inhalers. Eur J Respir Dis, 1982, 63 (Suppl. 119), 101-109. 2. Yarbrough J, Mansfield LE, Ting S. - Metered dose inhaler induced bronchospasm in asthmatic patients. Ann Allergy, 1985, 55, 25-27. 3. Wetterlin KIL. - Turbuhaler: a new powder inhaler for administration of drugs to the airways. Pharm Res, 1988, 5, (8), 506-508. 4. Johnsen CR, Weeke ER. - Turbuhaler: a new device for dry powder terbutaline inhalation. Allergy, 1988, 43, 392-395. 5. Persson G, Gruvstad E, StAhl E.- A new multiple dose powder inhaler, (Turbuhaler®), compared with a pressurized inhaler in a study of Terbutaline in asthmatics. Eur Respir J, 1988, 1, 681-684. 6. Osterman K, Norborg A· M, StAhl E.- A multiple dose powder inhaler (Turbuhaler®), compared with a conventional aerosol. An acceptance study in asthmatics. Allergy, 1989, 44, 294-297. 7. Andersen EB. - Discrete statistical models with social science application. North-Holland, 1980. 8. Anani A, Higgins AJ, Crompton GK.- Breath-actuated inhalers: comparison of terbutaline Turbuhaler with salbutamol Rotahaler. Eur Respir J, 1989, 2, 640-642.
9. Stallaert RALM. - The Bricanyl Turbuhaler, efficacy and acceptability compared to the Ventolin Rotahaler. Abstract. ICACI XIII Congress, Montreux, October 1988. 10. Schwarz F, Engler R, Villiger B. Turbuhaler ®. -A new concept in inhalation therapy. Abstract, Davos, April 1988. 11. Simonsson BG et al. - Double-blind trial with increasing doses of salbutamol and terbutaline aerosols in patients with reversible airway obstruction. Acta Med Scand, 1972, 192, 371-376. 12. Crompton GK. - New inhalation devices. (Editorial). Eur Respir J, 1988, 1, 679-680. 13. Warner JO, Chetcuti P. - Efficacy and acceptability of terbutaline sulphate Turbuhaler in children. In: A New Concept in Inhalation Therapy. S.P. Newman et al. eds, 1987. 14. Ribeiro LB. -A comparison of Bricanyl Turbuhaler and Berotec dry powder inhaler in asthmatic children. Eur Respir J, 1989, 2 (Suppl. 8), Abstract No. 990.
Le Turbuhaler~ de Bricany~ dans le traitement de l'asthme. Une etude multicentrique de six semaines conduite en Suede, en Grande-Bretagne, au Danemark, en Norvege et en Finlande. K. Osterman, E. Stdhl, A. Kiillen. RESUME: Deux cent-cinquante-huit adultes atteints d'asthme bronchique ont participe tt une etude ouverte, en groupe parallele, d'une duree de huit semaines. L'etude a demarre par une periode de mise en route de deux semaines pendant laquelle la terbutaline (betal agoniste) a ete administree tt raison de 5mg quatre fois par jour par un aerosol pressurise au freon, le Bricanyl MDI. Pendant les six semaines suivantes, un tiers des patients a continue a employer le MDI, et les deux tiers ont re~u la meme dose de terbutaline sous forme de poudre seche par le Turbuhaler. L'on n'a pas note de difference statistiquement significative dans les augmentations du DEP avant et apres inhalation entre les deux groupes de traitement. Les scores des symptomes d'asthme ont diminue dans le groupe Turbuhaler pendant I' etude, m a is sont res test inchanges dans le groupe MDI. L'on n'a pas observe de difference d'utilisation des medications hors essai pendant le jour entre Ies deux groupes. Pendant la nuit la difference etait statistiquement significative en faveur du Turbuhaler (p<0.05). Le Turbuhaler a ete bien supporte et s'est avere facile a utiliser. Compare au MD! utilise pendant la periode de mise en route, 50% des patients du groupe Turbuhaler lui ont donne la preference, 26% ont prefere le MD!, tandis que 24% n'avaient pas de preference. En conclusion, cette etude montre que le Turbuhaler est au moins aussi effectif que MD! pendant toute la periode de vie du Turbuhaler (6 semaines). Eur Respir J., 1991, 4, 175-179.