Embed Size (px)
Citation preview
Brian O'Neill and Alex Gillespie Simulating naturalistic instruction: the case for a voice mediated interface for assistive technology for cognition Article (Accepted version) (Refereed)
Original citation: O'Neill, Brian and Gillespie, Alex (2008) Simulating naturalistic instruction: the case for a voice mediated interface for assistive technology for cognition. Journal of assistive technologies, 2 (2). pp. 22-31. ISSN 1754-9450 © 2008 Pier Professional This version available at: http://eprints.lse.ac.uk/38691/ Available in LSE Research Online: Jan 2012 LSE has developed LSE Research Online so that users may access research output of the School. Copyright © and Moral Rights for the papers on this site are retained by the individual authors and/or other copyright owners. Users may download and/or print one copy of any article(s) in LSE Research Online to facilitate their private study or for non-commercial research. You may not engage in further distribution of the material or use it for any profit-making activities or any commercial gain. You may freely distribute the URL (http://eprints.lse.ac.uk) of the LSE Research Online website. This document is the author’s final manuscript accepted version of the journal article, incorporating any revisions agreed during the peer review process. Some differences between this version and the published version may remain. You are advised to consult the publisher’s version if you wish to cite from it.
1
Running head: Simulating naturalistic instruction Simulating naturalistic instruction: The case for a voice mediated interface for assistive technology for cognition Dr Brian O’Neill1 West of Scotland Mobility and Rehabilitation Centre Southern General Hospital 1345 Govan Road Glasgow, G51 4TF UK Tel: + 44 1412012391 Fax: + 44 1412012649 [email protected] Dr Alex Gillespie Department of Psychology University of Stirling Scotland, FK9 4LA UK
1 Author for correspondence

2
Title: Simulating naturalistic instruction: The case for a voice mediated interface for assistive technology for cognition
Abstract
A variety of brain pathologies can result in difficulties performing complex
behavioural sequences. Assistive technology for cognition (ATC) attempts support of
complex sequences with the aim of reducing disability. Traditional ATCs are
cognitively demanding to use and thus have had poor uptake. A more intuitive
interface may allow ATCs to reach their potential. Insights from psychological
science may be useful to technologists in this area. We propose that an auditory-
verbal interface is more intuitive than a visual interface and reduces cognitive
demands on users. Two experiments demonstrate a novel ATC, the General User
Interface for Disorders of Execution (GUIDE). GUIDE© is novel because it simulates
normal conversational prompting to support task performance. GUIDE© provides
verbal prompts and questions and voice recognition allows the user to interact with
GUIDE. Research with non-cognitively impaired participants and a single participant
experiment with a person with vascular dementia provide support for using interactive
auditory-verbal interfaces. Suggestions for the future development of auditory-verbal
interfaces are discussed.
Keywords: Assistive technology, executive function, GUIDE©, complex behaviour,
verbal interface

3

4
Title: Simulating naturalistic instruction: The case for a voice mediated interface for assistive technology for cognition
Difficulties carrying out goal-directed behaviour lead to a high degree of disability for
which there exist few treatment options. These difficulties are manifest in groups such
as traumatic brain injury (Evans, 2003), schizophrenia (Semkovska, Bedard, Godbout,
Limoge & Stip, 2003; Krabbendam, de Vugt, Derix & Jolles, 1999) learning disability
(Cavalier & Ferretti, 1993) and the dementias, contributing to the high degree of
personal care required by persons in these groups.
In samples of those with physical and cognitive disability, use of assistive
technologies is associated with reduced need for personal assistance (Hoenig, Taylor
& Sloan, 2003). However systems designed to support cognitive function can often be
cognitively demanding, highlighting the need for systems to be useable by those with
more severe cognitive disability (LoPresti, Mihailidis & Kirsch, 2004).
Traditional scheduling technology is complex to use. Diaries require users to recall
where they are, remember to enter a prompt, remember to check the diary and monitor
task completion. Recipes schedule sub-steps of a goal state. However they also
require decoding of the written steps and information storage in working memory to
underpin performance.
The applicaion of digital technology to cognitive rehabilitation has also been limited
by the cognitive demands of interfaces. Personal digital assistants (PDAs) and
5
palmtops are designed to extend the cognitive abilities of those without impairment
and have a learning curve which places them beyond many with cognitive deficits.
Designs of simplified interfaces has allowed use by those with learning disability to
aid with time management (Davies, Stock, Wehmeyer 2002). Prospective memory
aids have benefits in reducing omissions of to-be-performed behaviours. Specifically
text prompts delivered to portable systems such as pagers and mobile phones increase
the hit rate of target behaviours (Evans, 2003). These systems are useful for those
with intact reading and direction of attention. For those with yet more severe
cognitive difficulties we suggest that systems based on auditory-verbal interfaces may
be more appropriate.
Executive Function, Language & Scaffolding
Developmental psychologists studying executive function emphasise its basis in
language, and more particularly private speech (i.e., speech directed at self rather than
an interlocutor). This developmental account was initially proposed by Vygotsky and
Luria (1930/1994; Luria,1961). Although language evolved for communication,
Vygotsky and Luria speculate that it has a secondary function enabling humans to talk
themselves through complex tasks, thus facilitating the execution of complex
purposive and planned behaviour.
Research on child development supports a relation between language and executive
function (Hughes, 1996, 2002; Barkley, 1997; Jones, Rothbart & Posner, 2003;
Zelazo, Muller, Frye & Marcovitch, 2003). Children engage in private speech when
problem solving and this increases in probability with increasing task complexity
6
(Berk & Garvin, 1984). There is also a prevalence of private speech problems
amongst children who are at risk for attention and behaviour problems (Winsler, Diaz,
Atencio, McCarthy & Chabay, 1985) and amongst children who do worse at tasks
(Frauenglass & Diaz, 1985). In adults without cognitive impairment, introducing a
secondary task which disrupts private speech disrupts performance on a planning task
(Phillips, Wynn, Gilhooly, Della Sala & Logie, 1999).
Vygotsky and Luria proposed that the child initially has minimal executive control,
and that executive control is that provided by other people, such as parents and carers.
The verbal and visual actions of these carers guide the child’s behaviour, providing a
‘scaffold’ (Berk & Winsler, 1995; Gillespie, 2006; Zittoun, Gillespie, Cornish &
Psaltis, 2007). There are activities that the child is unable to perform alone, but is able
to perform with appropriate guidance. Such activities constitute the ‘zone of proximal
development’ and scaffolding operates in this zone. The scaffold comprises mainly of
verbal guidance. Verbal guidance is used to direct attention, set sub-goals, initiate
monitoring, and correct errors. Children develop through this verbal scaffold by
internalising the guidance so that they become able to verbally guide their own
behaviour (Gillespie, 2007). The monitoring and regulation of behaviour initially
occurs between the child and the carer, but with development becomes an intra-
psychological function, namely, executive function.
The relevance of the concepts of scaffolding and the zone of proximal development
for rehabilitation have been recognised (Stone, 1998; Young et al., 2002). In the same
way that there are problems which children are unable to solve alone, but which they
are able to solve with verbal guidance, so there people with a variety of cognitive
7
deficits who confront activities of daily living which they are unable to perform alone,
but which they are able to perform with appropriate verbal guidance. We suggest that
carers are often guiding patients at the limits of the patient's ability, providing
cognitive support by using verbal prompts to scaffold patients’ executive function.
Initiation, problem-solving, generativity, planning, sequencing, organization, self-
monitoring, error correction and behavioural inhibition are functions taken on by the
carer if these are deficient in the cared-for. The basic cognitive abilities that the
patient must possess in order to gain from this instruction are language
comprehension, maintenance of a single command in mind and verbally mediated
motor programming. Carers successfully support, or scaffold, individuals with
executive dysfunction in carrying out activities of daily living by instruction (Gitlin,
et al., 2002). In this sense, carers are often acting as highly refined ‘assistants for
cognition’. Our aim has been to try and simulate the verbal scaffolding and guidance
provided by carers.
Developing an Auditory-Verbal Interface
Assistive technologies for cognition, also known as cognitive prosthetics, have the
potential to revolutionise the management of cognitive disabilities (Gregor & Newell,
2004). Prospective memory aids facilitate the performance of a behaviour at a time in
the future which might otherwise be forgotten. Traditional prospective memory aids
are commonly used and include paper notes, diaries, calendars, alarms and reminders
(Evans, Wilson, Needham & Brentnall, 2003). These examples of traditional assistive
technology have been augmented in recent years by digital assistive technology.
8
Personal digital organisers and voice recorders can now undertake the function of
several of the traditional assistive technologies, such as temporal prompting and thus
recall of the to-be-performed behaviour (Kapur, Gilisky & Wilson, 2004; Yasuda et
al., 2002). Computer systems allow central storage of schedules to be delivered as text
prompts at the point when a behaviour requires to be carried out. The effectiveness of
pager prompts as used in the proprietary Neuropage system has been demonstrated to
increase achievement of target behaviours (Wilson, Emslie, Quirk, & Evans, 2001).
Similarly the MEMEX project, utilising text messaging to mobile phones, has
demonstrated effectiveness in improving attendance at appointments and medication
compliance (Pijnenborg, Withaar, Evans, van den Bosch & Brouwer, 2007).
LoPresti, Mihailidis and Kirsch (2004) suggest that ATCs have not been achieving
their full potential in the main, due to the complexity of the ATC devices. Rather than
reducing cognitive load, they often increase the cognitive burden by requiring users
interact with complex and unfamiliar devices. Accordingly, these authors call for
future ATC devices to be more sensitive in orienting to their cognitively impaired
users (see also, Scherer, 2001).
Based on our review of the available ATCs we argue that they are biased toward
visual interfaces. Visual interfaces are attention demanding. Attentional function
predicts use of cognitive aids in sample of people with acquired brain injury (Evans,
Wilson, Needham & Brentnall, 2003). Yet the main ATCs, such as Neuropage
(Wilson, Emslie, Quirk, & Evans, 2001) and MemoJog (Inglis et al., 2002), require
users to interact with the ATC device via a screen. Users usually receive information
via the screen, and give feedback to the device via the screen. Visual interfaces are
9
good if the user’s visual system is free and the user is familiar with such interaction.
However, in cases where a user is engaged in a task (such as dressing, food
preparation, transfer or donning a limb) interacting with a computer screen entails a
shift of visual attention and an interruption of the ongoing task, thus increasing the
cognitive load of the task. Where users are unfamiliar with computers, the device will
also be unintuitive contributing to low uptake.
We argue, on the basis of the literature on scaffolding, that an effective way forward
is for ATCs to model the cognitive support provided by carers, or ‘assistants for
cognition’. First, the cognitive scaffolding provided by carers is verbal, not visual, and
thus does not lead the patients’ visual attention away from the task at hand. Second,
given the evidence presented about the close relationship between executive function
and language, we speculate that prompting in the verbal medium rather than the visual
medium provides a more direct augmentation of executive function. Third, the verbal
guidance provided by carers is in a familiar mode of interaction, namely,
communicative interaction, and thus there is no learning curve. Finally, the
scaffolding provided by carers is task-focused and tailored to the individual, that is to
say each verbal prompt is contextually relevant to the immediate sub-goal that the
user is engaged in. Written instructions, flow charts or diagrams, on the other hand,
often present all the prompts and guidance at the same time, for example on the one
sheet of paper or flow chart. Such information overload is avoided in the auditory
medium because the linearity inherent in the auditory medium ensure that only one
prompt is presented at a time.
10
GUIDE©
We have developed an ATC that simulates the type of guidance provided by carers.
The device is called GUIDE© - General User Interface for Disorders of Execution.
The GUIDE© uses the most generalizable interface known for guiding users through
complex tasks, namely verbal guidance. The GUIDE© prompts users, asks users
questions and accepts verbal responses. The GUIDE© uses the verbal responses to
direct the deployment of subsequent prompts and questions. Delivering prompts and
questions to users verbally (rather than visually) entails less cognitive load, and does
not require users to switch task-focus (such as shifting from task to viewing a screen
or a card). The GUIDE© is designed to augment task focus, not to interrupt it. The
GUIDE© does not disempower users, by undermining their agency, rather the
GUIDE© empowers users. The GUIDE© prompts users with simple questions,
requiring the user to engage in the task in order to answer. The range of answers that
the GUIDE© accepts is deliberately limited, so as to reduce cognitive load. An
assumption is that verbal responses are comparatively easy for users, requiring the
least cognitive load and are similar to verbal interactions with carers
The GUIDE© is in the tradition of COACH (Mihailidis, Barbenel & Fernie, 2004) in
that it is focused upon a particular task and uses verbal prompts. The GUIDE©
incorporates Mihailidis, Barbenel and Fernie’s (2004, p. 166) recommendations for
constructing a verbal prompting system: prompts are provided at different levels of
detail, prompts are tailored to the individual user, prompts only pertain to one action
at a time, and prompts are phrased in a terminology that is familiar. The GUIDE©
also goes beyond these recommendations by virtue of attempting explicitly to
11
simulate the scaffolding support provided by carers. The prompts used by the
GUIDE© are modelled on the prompts provided by carers. Users interact with the
GUIDE© in the same way that they do with carers, namely, verbal exchange.
Specifically, this means that many of the prompts are actually questions, and these
questions require a verbal response from the user. The questions engage the user and
are intended to stimulate and augment, rather than command.
Research on a range of ATCs has tended to conclude that generic systems come into
problems both due to the particularities of the task to be achieved and particularities
of the patient (Cole, 1999; Mihailidis, Barbenel & Fernie, 2004). In order to avoid
such problems protocols are carefully constructed to address the task to be achieved
by the user.
Technologically, the GUIDE© has four components: hardware, voice recognition
software, an action pathway used to ‘scaffold’ users behaviour, and the GUIDE©
software program, running on a PC, that coordinates the parts. The action pathway
module within the GUIDE© stores steps and checks based on observations of
competent performance of the task. Verbal prompts are recorded and stored on the
PC. Verbal responses are processed via voice recognition software.
In order to develop our argument that audio-verbal interfaces are particularly suited to
ATCs which target behavioural sequences which require visual attention, we present
data from two recent studies using GUIDE© (Dickie, Tyler, O’Neill & Gillespie,
submitted; O’Neill & Gillespie, submitted). The first presents the results of a study of
adults without cognitive impairment carrying out a novel task with a distracting
12
secondary task comparing GUIDE use with following written instructions. The
second presents a case study of a man with vascular dementia carrying out a self-care
behaviour which he failed to acquire in rehabilitation as usual.
Study 1: Using GUIDE© with non-impaired adults
Design: A between-participants design was used with participants randomly allocated
to two groups. The task was to make an elaborate smoothie. One group received only
written instructions while the other group received the same instructions via the
GUIDE©. Periodic distraction was simulated in both conditions with a random
number generation task.
Participants: 26 participant sample of convenience (mean age 26; range19 to 43; 17
males, 9 females) randomly allocated to one of two groups. The Written Instruction
Group comprised 10 male and 3 female. The GUIDE© Group comprised 7 male and
6 female. No significant age differences existed between the groups.
Procedure: Before beginning the task participants were trained in the use of GUIDE©
for about 10 minutes. Training of the voice recognition software also occurred at this
time. The five commands were repeated 15 times each to reach an adequate level of
recognition. The task occurred in a kitchen with all equipment and ingredients
present. During the smoothie making task, participants were asked to generate a
random number between 34 and 43 every 30 seconds, throughout the experiment.
13
Scoring: Three indices of performance were independently rated: Percentage of steps
completed successfully; frequency of hesitations, other than when reading or listening
to prompts, of greater duration than 10 seconds; and mean time per step of the task.
Inter-rater reliability, measured with Pearson’s correlation coefficient was high for
number of correct steps (r=0.92, p<.001), for deviations (r=0.95, p<.001) and for
hesitations (r=.73, p<.001).
Following completion of the task, participants completed a questionnaire designed to
assess the participants’ feelings towards the method of instruction they experienced,
whether written instructions or the Guide© device. This questionnaire was scored by
counting the total number of positive and negative comments reported by the
participant.
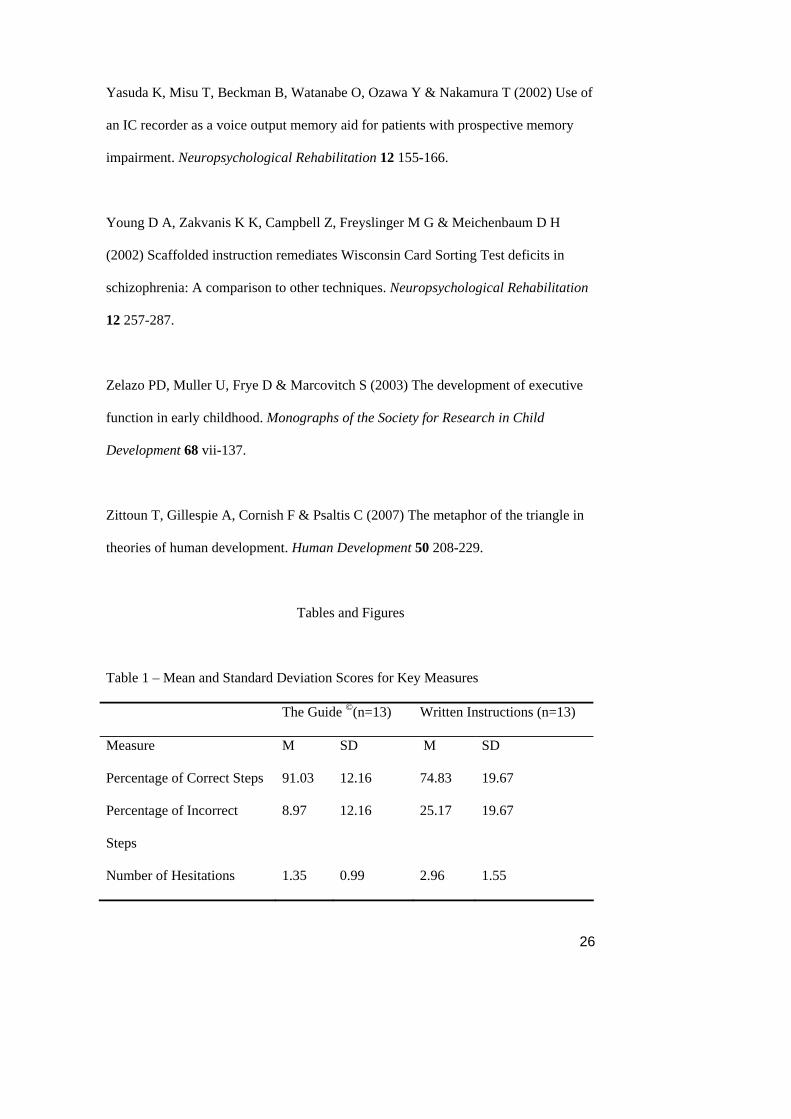
Results: Table 1 shows the group means for percentage of correct steps and incorrect
steps, number of hesitations and average time per step.
[insert Table 1 about here]
For the number of steps completed correctly, the Guide© performed significantly
better than the written instructions (F(1) = 6.375, p<0.05). The number of hesitations
show by users of the Guide© was significantly fewer than those shown by the group
following written instructions (F(1) = 12.084, p<0.05). The average time per step was
not significantly different, however there was a trend towards the Guide© steps being
completed more quickly than those in the written instruction group (F(1) = 1.326,
p>0.05). The mean number of positive comments given in the questionnaires was 2.5
14
for the Guide© (SD 1.31) and 1.0 for the written instructions (SD 1.04). This was
significantly different (F(1) = 9.581, p<0.05).
Study 2: Using GUIDE© with a cognitively impaired user
Participant: A 67 year old man (BB) who underwent bilateral transtibial amputations
due to peripheral arterial disease and comorbid diabetes a year prior to this
intervention. Following amputation he had received out-patient rehabilitation in a
specialist centre for post-amputation rehabilitation three times weekly for 8 weeks.
This consisted of instruction from a physiotherapist on the correct donning of his
prosthetic limbs and mobilization using a variety of supportive walking aids. He
consistently made errors in donning his prosthetic limbs and omitted critical safety
checks. He was thus advised by his physiotherapists that he was not to don his
prostheses without supervision. A standard neuropsychological assessment
(RANDOLPH, 1998) demonstrated impairments across several cognitive domains
with visuospatial function, attention and delayed memory lying in the extremely low
range.
Provision of visual sequence prompts (a series of client-viewpoint photographs of
correct steps) was tried for six limb donning attempts. He was unable to benefit from
these. We suspect that this was due to the attentional demands of shifting attention
from current task to the visual cues.
Task: A standardized sequence was developed for prosthetic limb donning, following
interview with physiotherapists and prosthetists. This was then instantiated as a
15
computer-stored sequence GUIDE© and delivered to the patient via wireless
headphones.
Design: A single participant baseline-intervention experiment was employed.
Baseline data were gathered by video recording on-task behaviour. These videos were
scored, using a customised Sequence Performance Scale, for a. percent correct b.
errors of omission, c. deviations from sequence, d. repetitions and e. time to fit limb to
give data points for statistical analysis (Semkovska et al., 2003). Inter-rater reliability
for this measure ranged from 0.73 to 0.77 across the indices of the measure. The
intervention trials were randomly allocated within the sequence of trials.
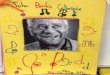
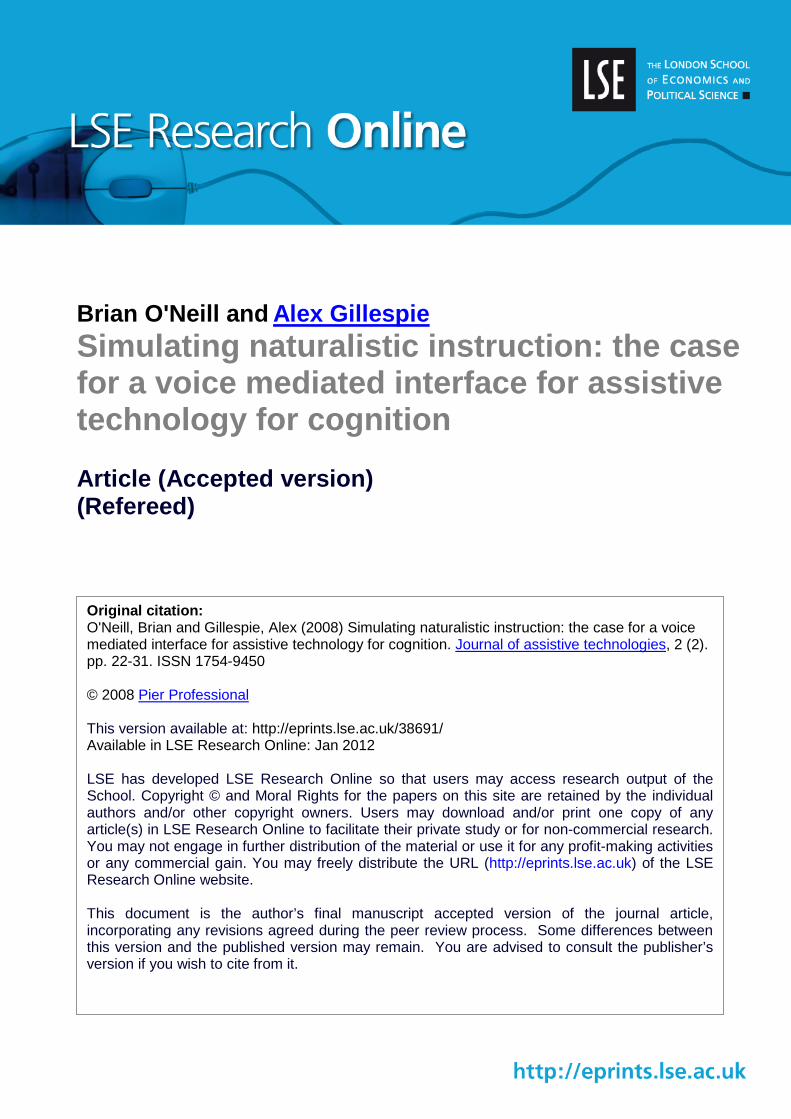
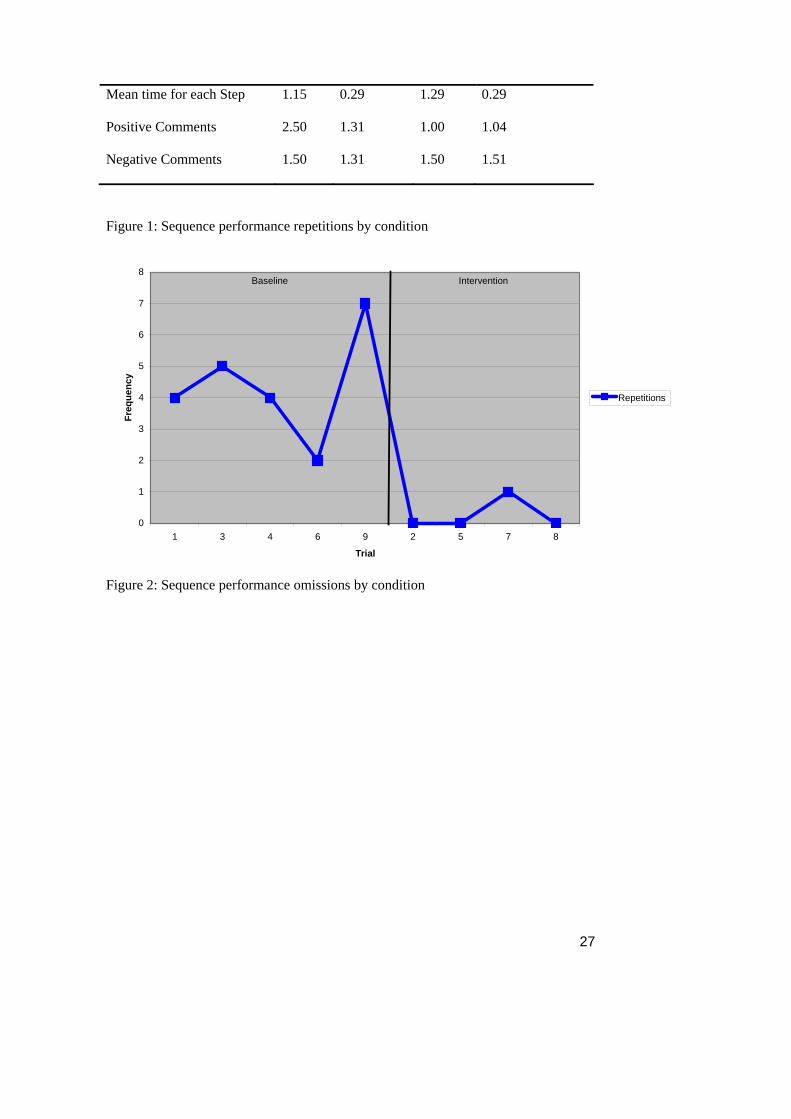
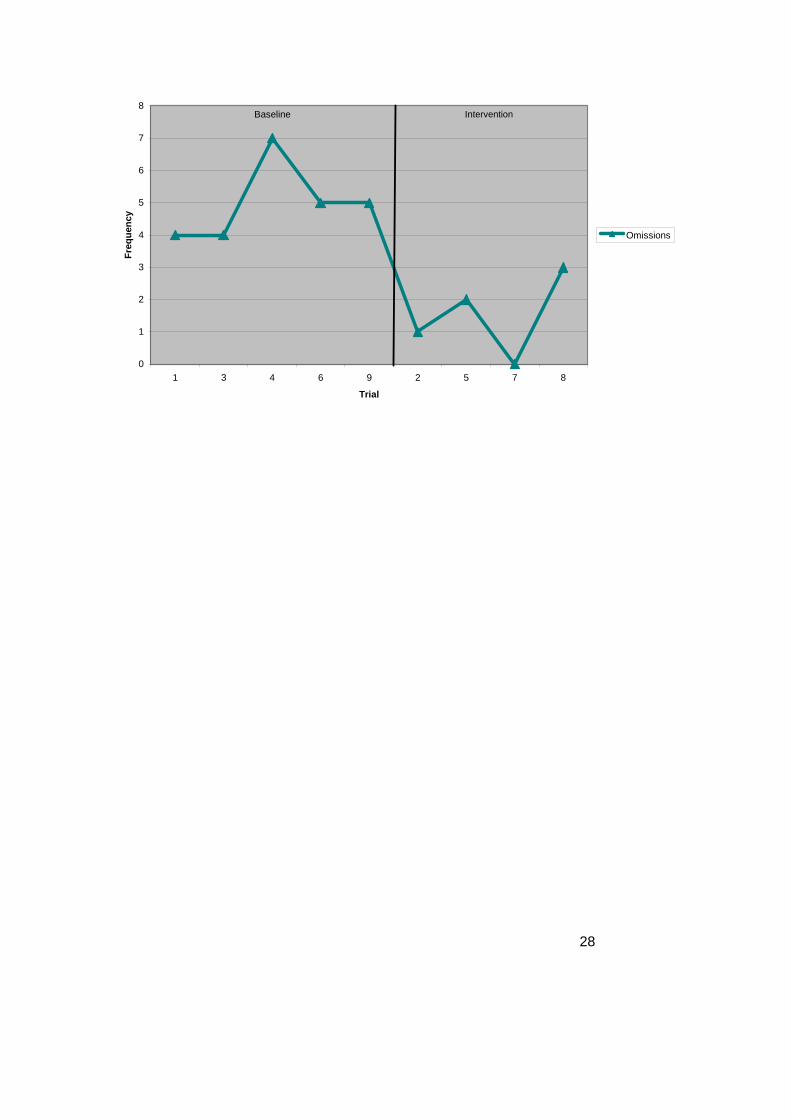
Results: The participant’s performance scores by trial are shown in Figures 1 and 2.
On the x axis one can see the trial number, separated into baseline on the left and
intervention on the right. BB was on average 81% correct in the baseline and 94%
correct on the intervention trials. An exact probability test for randomized trials
(Todman & Dugard, 2001) found that GUIDE© use was associated with statistically
significant reductions in repetitions of previous steps (p<0.05) and omissions of
sequence steps (p<0.05). Reduction in deviations from the ideal sequence approached
significance (p=0.061). Time to don the prostheses was reduced from a mean of 12
minutes in baseline to 9.25 minutes on GUIDE© trials. An Efficiency Index (Total
Correct / Total Time) also changed significantly between conditions (p<0.05).
[Insert Figures 1 about here]
[Insert Figure 2 about here]
16
Discussion
Both of our preliminary studies show benefits of using a voice mediated prompting
system over sequence performance without. This was in the context of imposed
distractors in Study 1 and in a participant with cognitive impairment in Study 2.
Taken together, these studies show the feasibility of using an auditory-verbal interface
in ATC design for contexts of high distraction and cognitive impairment.
The GUIDE© demonstrates potential as a rehabilitation tool. Cognitive problems
compromise rehabilitation outcome in conditions such as cerebrovascular accident
(Paolucci et al., 1996) and post-amputation (O’Neill, 2008). For many of these
conditions rehabilitation is labour intensive due to the need for repeated instruction or
supervision to prevent errors. Computer assisted guidance of repeated instruction
could thus allow patients to engage autonomously in rehabilitation relevant tasks.
The success of the GUIDE©, we suggest, stems from the verbal interface. While the
mode of verbal interaction is novel for ATCs, it is familiar for users. BB adapted to
the use of the GUIDE© in the first session. While many other ATCs have reported
difficulties in training users and long learning curves (LoPresti, Mihailidis & Kirsch,
2004), we suspect this has been due to the lack of familiarity with the interface. A
second advantage with the verbal interface, which we argued in the introduction, is
that it provides a relatively direct route to augmenting executive function because
there is evidence to suggest that executive function is in fact heavily verbally
17
mediated. The success of the GUIDE© is consistent with such an association.
Moreover, during the trials when BB was not using the GUIDE© the researchers
noted an increased tendency for BB to talk himself through the task. This talk was
loud enough to be heard by the researchers. Such utterances are in line with research
which has shown that children facing a complex task tend to talk themselves through
the task (Berk & Garvin, 1984; Vygotsky & Luria, 1994; Winsler & Naglieri, 2003),
thus again supporting the link between executive function and verbal mediation which
the GUIDE© is based upon.
All users in the above studies showed good tolerance of the system. In Study 1 more
positive comments were made with regard the GUIDE© than the written instructions.
It is hypothesised that a verbal guidance system is tolerated because the delivery of
prompts is similar to the experience of private speech, which underpins normal
problem solving (Phillips, Wynn, Gilhooly, Della Sala & Logie, 1999). BB
commented after some trials using the GUIDE© ‘how did I do?’ or ‘I did well there’.
This contrasted with his previous thanking of the instructor or making disparaging
comments about them in the event of poor performance. It thus appears likely that
persons using the system may be able to attribute success to the actions of the self
rather than use of the system. This is promisingly indicates that users may experience
personal satisfaction attaining a goal using the system, despite being scaffolded to do
so.
The acceptability of having a sequence step cued by a verbal stimulus appears good.
What is less clear is the acceptability of making verbal responses to control cue
deployment. Each of the participants performed the focal task alone apart from the
18
presence of the experimenter and it remains a possibility that users may feel self-
conscious if using the system in earshot of others. Future research is needed to
examine the extent to which using the device in public settings is perceived as
stigmatising.
The emulation of carers’ verbal guidance of behaviour in the field of assistive
technology for cognition is rare. Orpwood, Adlam, Gibbs and Hagan (2001) used
recorded carers’ voices to remind persons with dementia of omissions triggered by
sensors. For example a bath sensor triggered the recording: “Don’t forget you’ve left
the bath running mum”. Literature search did not elicit any research assessment of the
effectiveness of such devices although the initial case studies are promising. To our
knowledge our system is the first to accept users’ verbal responses to control output.
We would argue that some control of the output is an important feature. Being unable
to control the voice directing behaviour may be noxious and disempowering.
Perception of an assistive technology is an important determinent of use (e.g. Scherer,
2002) and we argue that the acceptability of devices (e.g. monitoring systems,
prompters etc.) should be to the fore of any assessment of their efficacy.
The studies reported here demonstrate the orthotic function of the system.
Performance-with was only compared to performance-without and there was no
examination of learning effects. However, for individuals with better memory
function the system might also restore performance of complex sequences. Errorless
learning, wherein performance errors are minimised for the memory impaired learner,
has evidence to suggest efficacy in teaching ordered semantic information (Kessels &
De Haan, 2003) and behavioural sequences (Maxwell, Masters, Kerr & Weedon,
19
2001). The system can guide error free performance and might thus be used to support
errorless learning. Directions can be gradually replaced by question prompts with
these faded out in turn, incrementally increasing the amount to be recalled.
The range of potential applications is difficult to estimate but appears wide. All
complex behavioural sequences which can be verbally described are open to the
application. For future research we suggest identifying and then augmenting those
behaviours which formal and informal carers are currently providing verbal
scaffolding for. In depth analysis of carer providers as ‘assistants for cognition’ might
provide further clues as to the most appropriate modes of questioning and prompting.
Also studies of the self-talk that normally accompanies the prefromance of a complex
behavioural sequence are needed. The motivation for this research is to construct the
simplest and most intuitive interface for ATCs. To this end, the future development of
ATC interfaces, we suggest, should focus upon the auditory-verbal interface to
simulate both carer instruction and the internal verbal control of sequence
performance.
References
Barkley R A (1997) ADHD and the nature of self-control. New York: The Guilford
Press.
Berk L E & Garvin R A (1984) Development of private speech among low-income
Appalachian children. Developmental Psychology 20 271-286.
20
Berk L E & Winsler A (1995) Scaffolding children's learning: Vygotsky and early
childhood education. Washington: National Association for the Young Children.
Cavalier A R & Ferretti R P (1993) The use of an intelligent cognitive aid to facilitate
the self management of vocational skills by high school students with severe learning
disabilities. In RESNA'93 Annual Conference. Arlington, VA: RESNA Press.
Cole E (1999) Cognitive prosthetics: An overview to a method of treatment.
NeuroRehabilitation 12 39-51.
Crepeau F & Scherzer P (1993) Predictors and indicators of work status after
traumatic brain injury: A meta-analysis. Neuropsychological Rehabilitation 3 5-35.
Davies D, Stock S, Wehmeyer M (2002) Enhancing independent time-management
skills in those with mental retardation using a palmtop personal computer. Mental
Retardation 40 (5) 358-65
Evans J J (2003) Rehabilitation of executive deficits. In B. A. Wilson (Ed.)
Neuropsychological Rehabilitation. Abingdon: Swets and Zeitlinger.
Evans J J, Wilson B A, Needham P, & Brentnall S (2003) Who makes good use of
memory aids? Results of a survey of people with acquired brain injury. Journal of the
International Neuropsychology Society 9 925-935.
21
Frauenglass M H & Diaz R M (1985) Self-regulatory functions of children's private
speech: A critical analysis of recent challenges to Vygotsky's theory. Developmental
Psychology 21 357-364.
Gillespie A (2006) Games and the development of perspective taking. Human
Development 49 87-92.
Gillespie A (2007) The social basis of self-reflection. In J. Valsiner & A. Rosa (Eds.),
The Cambridge Handbook of Sociocultural Psychology. Cambridge: Cambridge
University Press.
Gitlin L, Winter L, Dennis M, Corcoran M, Schinfeld S & Hauck W W (2002)
Strategies used by families to simplify tasks for individuals with Alzheimer's disease
and related disorders: Psychometric analysis of the Task Management Strategy Index
(TMSI). The Gerontologist 42 61-70.
Gregor P & Newell A (2004) Introduction. Neuropsychological Rehabilitation 14 1-3.
Hoenig H, Taylor D & Sloan F (2003) Does assistive technology substitute for
personal assistance in the disabled elderly? American Journal of Public Health 93 (2)
330-337.
Hughes C (1996) Control of action and thought: Normal development and
dysfunction in autism: A research note. Journal of Child Psychology and Psychiatry
37 229-236.
22
Hughes C (2002) Executive functions and development: Emerging themes. Infant and
Child Development 11 201-209.
Inglis E, Szymkowiak A, Gregor P, Newell A, Hine N, Shah P, Evans J J & Wilson B
A (2003) Issues surrounding the user-centred development of a new interactive
memory aid. Universal Access in the Information Society 2 226-234.
Jones L B, Rothbart M K, & Posner M I (2003) Development of executive attention in
preschool children. Developmental Science 6 (5) 498-504.
Kapur N, Glisky E L, & Wilson B A (2004) Technological memory aids for people
with memory deficits. Neuropsychological Rehabilitation 14 41-60.
Kessels R P C & de Haan E H F (2003) Implicit Learning in Memory Rehabilitation:
A Meta-Analysis on Errorless Learning and Vanishing Cues Methods. Journal of
Clinical and Experimental Neuropsychology 25 805-814.
Krabbendam L, de Vugt M E, Derix M M & Jolles J (1999) The behavioural
assessment of the dysexecutive syndrome as a tool to assess executive functions in
schizophrenia. Clinical Neuropsychology 13 370-375.
Lezak M D (2003) Neuropsychological Assessment, 4th Edition. Oxford: Oxford
University Press.
23
LoPresti E, Mihailidis A, Kirsch N (2004) Assistive Technology for Cognitive
Rehabilitation: State of the Art. Neuropsychological Rehabilitation 14 (1/2) 5-39.
Luria A (1961) The role of speech in the regulation of normal and abnormal
behaviour. London: Pergamon Press.
Maxwell J, Masters R, Kerr E & Weedon E (2001) The implicit benefits of learning
without errors. The Quarterly Journal of Experimental Psychology 54 1049-1068.
Mihailidis A, Barbenel J C & Fernie G (2004) The efficacy of an intelligent cognitive
orthosis to facilitate handwashing by persons with moderate to severe dementia.
Neuropsychological Rehabilitation 14 135-171.
O’Neill, B (2008) Cognition and Mobility Rehabilitation following Lower Limb
Amputation. In: Gallagher, Desmond and MacLachlan (Eds.) Psychoprosthetics:
State of the Knowledge. London: Springer.
Orpwood R, Adlam T, Gibbs C & Hagan S (2001) User-centred design of support
devices for people with dementia for use in a Smart House. In Marincek C, Buhler C,
Knops H & Andrich R (Eds) Assistive Technology –Added Value To The Quality of
Life. Amsterdam: IOS Press.
Paolucci S, Antonucci G, Guariglia C, Magnotti L, Pizzamiglio L & Zoccolotti P
(1996) Facilitatory effect of neglect rehabilitation on the recovery of left hemiplegic
stroke participants: A cross-over study. Journal of Neurology 243 308-396.
24
Phillips L, Wynn V, Gilhooly K, Della Sala S, & Logie R (1999) The role of memory
in the tower of London task. Memory 7 209-231.
Pijnenborg G H, Withaar F K, Evans J J, van den Bosch R J, & Brouwer W H (2007)
SMS text messages as a prosthetic aid in the cognitive rehabilitation of schizophrenia.
Rehabilitation Psychology 52 236-240
Scherer M J (2001) Assistive technology: Matching device and consumer for
successful rehabilitation. Washington: American Psychological Association.
Semkovska M, Bedard M A, Godbout L, Limoge F & Stip E (2003) Assessment of
executive dysfunction during activities of daily living in schizophrenia. Schizphrenia
Research 69 289-300.
Shallice T (1982) Specific Impairments of Planning. Philosophical Transactions of
the Royal Society of London B 298 199-209.
Singer B D & Bashir A S (1999) What are executive functions and self-regulation and
what do they have to do with language-learning disorders? Language, Speech, and
Hearing Services in Schools 30 265-273.
Stone C A (1998) The metaphor of scaffolding: Its utility for the field of learning
disabilities. Journal of Learning Disabilities 331 344-364.
25
Tierney M, Snow W, Charles J, Moineddin R & Kiss A (2007) Neuropsychological
predictors of self-neglect in cognitively impaired older people who live alone. The
American Journal of Geriatric Psychiatry 15 140-148.
Todman J B & Dugard P (2001) Single Case and Small-n Experimental Designs: A
Practical Guide to Randomisation Tests. London, Lawrence Erlbaum Associates.
Vygotsky L S & Luria A (1930/1994) Tool and symbol in child development. In Van
de Veer R & Valsiner J (Eds.) The Vygotsky Reader. Oxford: Blackwell.
Wilson B A, Emslie H C, Quirk K & Evans J J (2001) Reducing everyday memory
and planning by means of a paging system: a randomized control crossover study.
Journal of Neurology Neurosurgery and Psychiatry 70 477-482.
Winsler A, Diaz R M, Atencio D J, McCarthy E M & Chabay L A (2000) Verbal self-
regulation over time in preschool children at risk for attention and behavior problems.
Journal of Child Psychology and Psychiatry 41 875-886.
Winsler A & Naglieri J (2003) Overt and covert verbal problem-solving strategies:
Developmental trends in use, awareness and relations with task performance in
children aged 5 to 17. Child Development 74 659-678.
Woodruff-Pak D S (1997) The Neuropsychology of Ageing. Oxford: Blackwell.
26
Yasuda K, Misu T, Beckman B, Watanabe O, Ozawa Y & Nakamura T (2002) Use of
an IC recorder as a voice output memory aid for patients with prospective memory
impairment. Neuropsychological Rehabilitation 12 155-166.
Young D A, Zakvanis K K, Campbell Z, Freyslinger M G & Meichenbaum D H
(2002) Scaffolded instruction remediates Wisconsin Card Sorting Test deficits in
schizophrenia: A comparison to other techniques. Neuropsychological Rehabilitation
12 257-287.
Zelazo PD, Muller U, Frye D & Marcovitch S (2003) The development of executive
function in early childhood. Monographs of the Society for Research in Child
Development 68 vii-137.
Zittoun T, Gillespie A, Cornish F & Psaltis C (2007) The metaphor of the triangle in
theories of human development. Human Development 50 208-229.
Tables and Figures
Table 1 – Mean and Standard Deviation Scores for Key Measures
The Guide ©(n=13) Written Instructions (n=13)
Measure M SD M SD
Percentage of Correct Steps 91.03 12.16 74.83 19.67
Percentage of Incorrect
Steps
8.97 12.16 25.17 19.67
Number of Hesitations 1.35 0.99 2.96 1.55
27
Mean time for each Step 1.15 0.29 1.29 0.29
Positive Comments 2.50 1.31 1.00 1.04
Negative Comments 1.50 1.31 1.50 1.51
Figure 1: Sequence performance repetitions by condition
0
1
2
3
4
5
6
7
8
1 3 4 6 9 2 5 7 8
Trial
Freq
uenc
y
Repetitions
Baseline Intervention
Figure 2: Sequence performance omissions by condition
28
0
1
2
3
4
5
6
7
8
1 3 4 6 9 2 5 7 8
Trial
Freq
uenc
y
Omissions
Baseline Intervention