Embed Size (px)
Citation preview

This article was downloaded by: [University of Washington Libraries]On: 09 August 2013, At: 16:50Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House,37-41 Mortimer Street, London W1T 3JH, UK
Biodemography and Social BiologyPublication details, including instructions for authors and subscription information:http://www.tandfonline.com/loi/hsbi20
Breastfeeding behavior and infant survival withemphasis on reverse causation bias: Some evidencefrom NigeriaClement Ahiadeke a , Douglas T. Gurak b & Steven J. Schwager ca Population Dynamics Unit, ISSER, University of Ghana, P.O. Box 74, Legon, Ghanab Population and Development Program, Cornell University, 133 Warren Hall, Ithaca, NY, 14853,USAc Biometrics Unit, Cornell University, 337 Warren Hall, Ithaca, NY, 14853, USAPublished online: 23 Aug 2010.
To cite this article: Clement Ahiadeke , Douglas T. Gurak & Steven J. Schwager (2000) Breastfeeding behavior and infantsurvival with emphasis on reverse causation bias: Some evidence from Nigeria, Biodemography and Social Biology, 47:1-2,94-113, DOI: 10.1080/19485565.2000.9989012
To link to this article: http://dx.doi.org/10.1080/19485565.2000.9989012
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) contained in thepublications on our platform. However, Taylor & Francis, our agents, and our licensors make no representationsor warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of the Content. Anyopinions and views expressed in this publication are the opinions and views of the authors, and are not theviews of or endorsed by Taylor & Francis. The accuracy of the Content should not be relied upon and should beindependently verified with primary sources of information. Taylor and Francis shall not be liable for any losses,actions, claims, proceedings, demands, costs, expenses, damages, and other liabilities whatsoever or howsoevercaused arising directly or indirectly in connection with, in relation to or arising out of the use of the Content.
This article may be used for research, teaching, and private study purposes. Any substantial or systematicreproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form to anyoneis expressly forbidden. Terms & Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions

Breastfeeding Behavior and Infant Survivalwith Emphasis on Reverse Causation Bias:Some Evidence from Nigeria
Clement Ahiadeke, Douglas T. Gurak, and Steven J. Schwager
Population Dynamics Unit, ISSER, University of Ghana, P.O. Box 74, Legon, Ghana; Population andDevelopment Program, Cornell University, 133 Warren Hall, Ithaca, NY 14853, USA; BiometricsUnit, Cornell University, 337 Warren Hall, Ithaca, NY 14853, USA
ABSTRACT: The possibility of selection bias in the estimation of the effects of breastfeeding onsubsequent survival is implied by the clinical evidence that children who are healthier at birthare more likely to be breastfed than their less healthy counterparts who may be prone to difficul-ties in sustaining breastfeeding. This paper addresses an important problem in understandingthe association of breastfeeding and child survival with regard to reverse causation. It utilizesdata on the reported reason for weaning to assess the degree to which reverse causality may beresponsible for observed associations. The analysis indicates that children who are weaned in theneonatal period because of illness or weakness to suckle, experience a much higher risk of dyingthan others. This is not mainly because of the cessation of breastfeeding, but because of the origi-nal factor, being their illness. Any biases imparted by an initial selection mechanism appear,therefore, to have influence on the effectiveness of breastfeeding behavior.
INTRODUCTION
Demographic and public health com-munities generally agree that breastfeed-ing provides early protection against dis-ease for infants in environments wherethe alternatives to breast milk can easilybe contaminated by poor household con-ditions (Habicht et al., 1988). Factorsspecific to the mother and child, such asmother and child's health status at thetime of delivery, can influence the choiceto initiate breastfeeding and its duration(Lantz et al., 1992). Reverse causationbias is said to occur when the infant istoo sick to suckle, so that death leads to"weaning" rather than the reverse (Hol-land, 1987; Montgomery et al., 1986;Milman and Cooksie, 1987; VanLanding-ham et al., 1991). It arises from a child'sinability to initiate or sustain breastfeed-ing and can therefore be complicated bythe child's initial health status.
The relationship between breastfeed-ing cessation (due to ill health) andmortality is not simultaneous, but ratherrecursive; changes in breastfeeding be-havior may not alter health outcome in-stantly, but only after a time lag. If thereare unobserved factors influencing healthstatus and the type of decision made byparents to discontinue breastfeeding, anydirect links between breastfeeding andhealth outcome may be confounded byunmeasured variables in the data. Re-verse causation addresses the bias that re-sults from death due to the cessation ofbreastfeeding by infants who become ill.The causal model assumes that neonatalillness can result in the death of the childeither directly (through illness) or indi-rectly (as a result of the cessation ofbreastfeeding, which is known to imparthealth benefits to the infant). Both the di-rect effect (illness to mortality) and theindirect effect of illness (operating via
94
Dow
nloa
ded
by [
Uni
vers
ity o
f W
ashi
ngto
n L
ibra
ries
] at
16:
50 0
9 A
ugus
t 201
3

Vol. 47, No. 1-2 Breastfeeding Behavior 95
cessation of breastfeeding) can producehigh mortality. In addressing the issue ofreverse causation bias, we want to deter-mine the impact of breastfeeding cessa-tion vis-a-vis the illness factor on thechild's health status prior to death. Thispaper addresses the problem in under-standing the association of breastfeedingcessation due to illness and child mortal-ity. It utilizes data on the reported reasonfor weaning to assess the degree to whichreverse causality may be responsible forobserved associations.
REVERSE CAUSALITY ANDBREASTFEEDING BEHAVIOR
Successful breastfeeding is the resultof complex psychological and physicalinteractions between the baby and themother, so that difficulties for either canlead to discontinuation (Jelliffe and Jel-liffe, 1978). Two mutually reinforcing re-flex actions govern the process of breast-feeding initiation: the child's sucklingstimulates the mother's let-down reflexand the resultant milk flow encouragesthe child to continue. In healthy babies,the suckling reflex is strongest in the first30 minutes after birth (Leefsma, 1980).Delay in the time of first feeding can leadto difficulties in initiating and in continu-ing breastfeeding. Unhealthy babies oftenhave particularly weak suckling reflexesand are therefore likely to find breast-feeding more difficult than healthy ba-bies. Alternative feeding and separationfrom the mother may also exacerbate anyinitial difficulties. As a consequence, in-fants who have trouble initiating breast-feeding at birth experience higher failurerates (of breastfeeding) at all subsequentdurations.
Reverse causation complicates theanalysis of the links between breastfeed-
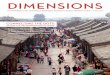
ing and infant mortality. While it is clearthat mortality is the dependent variable,the causal model (at least, its nucleus) iscomplex as is suggested in Figure 1. Theissue of "reversed causation" is not thatone really wants to know whether thestrongest effect is merely the direct effect(i.e., illness to mortality) or the indirecteffect (operating via cessation of breast-feeding), as is shown in Panel A of Figure1. Rather, we want to determine the im-pact of breastfeeding cessation vis-a-visthe illness factor on the child's health sta-tus prior to death as presented in Panel B.Children who are ill may cease to breast-feed either as a result of their own weak-ness (inability to suckle) or by their par-ents' choice. The literature on feedingpractices that include avoiding breast-feeding during illness of the child almostalways produces very few cases (Navedand Kumar, 1994; Adair, Popkin andGuilkey, 1993). From Panel B in Figure1, wasting can trigger illness or vice-versa. Weaning the child (stoppingbreastfeeding) can lead to wasting or ill-ness, either one of which can lead todeath. In the absence of prospective orpanel data, the literature contains threeapproaches to the study of breastfeedingand its impact on child survival that canbe used in studying the distortions pro-duced by reverse causation bias.
The first approach focuses on measur-ing the intentions of pregnant women toinitiate breastfeeding and to breastfeedfor a given duration (Baranowski et al.,1983; Lizarraga et al., 1992; Romero-Gwynn and Carias, 1989). The secondapproach focuses on the initiation and du-ration of breastfeeding, investigating thereasons for not initiating or for discontin-uing breastfeeding. Studies of this typefrequently examine the correlates of theinitiation or duration of breastfeeding
Dow
nloa
ded
by [
Uni
vers
ity o
f W
ashi
ngto
n L
ibra
ries
] at
16:
50 0
9 A
ugus
t 201
3

NeonatalIllness
Panel A
Breastfeeding
Mortality
Panel B
IllnessNot due toweanine
Malnutritionwastine
Stopbreastfeeding Death
OrSurvival
FIG. 1.—Pathways of how breastfeeding can affect child survival.
W5%
ESS'D
ownl
oade
d by
[U
nive
rsity
of
Was
hing
ton
Lib
rari
es]
at 1
6:50
09
Aug
ust 2
013

Vol. 47, No. 1-2 Breastfeeding Behavior 97
(Stewart et al., 1991; Adair et al., 1993).The third approach is to ask women di-rectly the reasons why they did notbreastfeed or why they stopped breast-feeding (Winikoff et al., 1988; Wright etal., 1993; Greiner et al., 1981). Each ofthese approaches has advantages and dis-advantages that result from the limita-tions of the data. The Demographic andHealth Survey (DHS) project makes itpossible to combine elements from thesethree methodological approaches to studyreverse causation bias and child survivalin developing countries. Quality datafrom most developing countries, in par-ticular, countries of sub-Saharan Africa,have been scarce, and the question of re-verse causation bias has not been ade-quately addressed.
Apart from its contraceptive benefits,breastfeeding improves child survival bydecreasing the infant's exposure to conta-minated food and water and by lengthen-ing the interval between births, whichreduces premature weaning and siblingcompetition for food, and also reduces nu-tritional depletion of the mother (Habichtet al., 1986). These potential benefits aregreatest in developing countries with lowcontraceptive prevalence, little supple-mentation of breast milk, low nutritionalstatus of mothers, and cultural taboosagainst sexual relations for the durationof breastfeeding (Huffman and Lam-phere, 1984; Palloni and Milman, 1986).
Holland (1987) attempted to minimizethe problem of reverse causation bias forinfants in age groups beyond 1-2 monthsby conditioning the analysis on breast-feeding behavior prior to the start of eachage interval. This approach, however,cannot be used in the first age interval.Children who have never been breastfedwill exhibit relatively high mortality, be-cause some of them will have been too
sick at birth to initiate suckling. In princi-ple, this bias could be reduced by askingwomen why they never breastfed their in-fants. Holland did remove those infantswho were not breastfed because "thechild died." However, it seems likely thatthe response "too sick to suckle" maysometimes be a rationalization, especiallyif the child died (VanLandingham et al.);if so, removing such infants would resultin a bias in the other direction.
Other research suggests that the prob-lem of reverse causation does not sub-stantially exaggerate the strong effect ofbreastfeeding on child health. Millmanand Cooksie (1987), using data from thesame Malaysian Family Life Survey(MFLS) as Holland, found that control-ling for a number of proxy measures forthe child's health status at birth had littleinfluence on the effect of breastfeedingon infant survival. Using a different ap-proach, Montgomery et al. (1986) testedthe same MFLS data for selection biasand concluded that "the direct influenceof breastfeeding on survival remains ofoverwhelming importance even after cor-rections for selection bias are made."'
Perhaps the best form of data availablefor addressing the reverse causationissue is event history data. Forste (1994)analyzed the causal ambiguity betweenbreastfeeding and survival using an event-history technique applied to a Gompertzfunction. Mortality, the dependent vari-able, was analyzed in two ways. First, in-fants who died during the first month oflife or were less than one month old atthe time of the interview were included ashaving survived one month. In the secondapproach, only those infants who hadsurvived at least one month of life at the
1Correction for selection bias assumes largely thatillness determines breastfeeding behavior.
Dow
nloa
ded
by [
Uni
vers
ity o
f W
ashi
ngto
n L
ibra
ries
] at
16:
50 0
9 A
ugus
t 201
3

98 Ahiadekeetal. Social Biology
time of the interview were included. Thelogic of this procedure is that the causaldirection between breastfeeding anddeath is ambiguous in the neonatal casesincluded in the first approach. However,because breastfeeding is begun shortlyafter birth, the second approach containsonly cases in which death is known tohave followed the beginning of lactation.Comparisons between the two approachesindicate the degree of breastfeeding biasthat arises during the first month of life.Forste's conclusion is that "illness is adominant factor influencing mortality" inthe neonatal period and that the "inclu-sion of neonates can exaggerate the effectof breastfeeding on mortality."2
In the analysis presented here, thecausal ambiguity is tested using severaldifferent models with two different datasets. To account for the fact that previousfindings may be sensitive to the choiceof model, two estimation equation ap-proaches were explored: proportionalhazard model using event history dataand a random-effects logit model.
DATA AND METHODS
This paper addresses the influence ofreverse causation bias on the estimatedeffects of breastfeeding behavior on in-fant survival in Nigeria. The data usedhere are drawn from the 1990 NigerianDemographic and Health Survey (FederalOffice of Statistics and Macro Interna-tional Inc., 1992) and the Enugu Health-Seeking Behavior Survey (1991) cover-ing a sub-region of Nigeria. The DHSprogram is an ongoing worldwide collab-orative effort between the governmentsof the survey countries and the Institute
2Many infants die during the first month of life be-fore breastfeeding is begun, thus, death determineswhether breastfeeding occurs and not otherwise.
for Resource Development (Macro Inter-national, Calverton, Maryland) with fi-nancial support from the United Statesgovernment. The Nigerian DHS is a na-tionally representative sample of 8,781women aged 15-49 years. The informa-tion collected includes: demographiccharacteristics of the survey respondent, areproductive history, knowledge and useof contraception, fertility preferences,maternal care during pregnancy and de-livery, breastfeeding, vaccination statusof children, prevalence and treatment ofdiarrhea, fever, and cough in children,and height and weight of children.
A smaller sample consisting of 2,011Igbo women who had live births duringthe five years prior to the survey date wasemployed as a supplement to the Niger-ian DHS. The Enugu study, which con-ducted a survey methodologically similarto the DHS, is more specific to the Igboethnic group in eastern Nigeria and con-tains as detailed morbidity information asthe DHS. The instrument was designedspecifically to measure health-seeking be-havior among Igbo women who had livebirths during the five years before thesurvey. It can therefore serve to confirmfindings at the local level that obtain inthe larger national survey. The inclusionof the Enugu data is also to help in theconstruction of the different models em-ployed in the analysis.
The sampling characteristics of theDHS provide generalizable results andpermit the examination of the subgroupson which research interest is focused. Inaddition, the nature of the fertility historymakes it possible to specify the correcttiming of most explanatory variables.This is because DHS coded age at deathin completed months, thus removing anyrestrictions on estimated hazard models.In addition, the DHS provides much
Dow
nloa
ded
by [
Uni
vers
ity o
f W
ashi
ngto
n L
ibra
ries
] at
16:
50 0
9 A
ugus
t 201
3

Vol. 47, No. 1-2 Breastfeeding Behavior 99
more specific information on prenatal andpostnatal health practices, breastfeeding,and anthropometric indicators than wereavailable in previous studies. In otherwords, the data on hand utilize informa-tion on the reported reason for weaningthe child to assess the degree to which re-verse causality may be responsible forobserved associations.
OUTCOME VARIABLE
The outcome variable of interest is thesurvival status of children in the age in-terval 0-12 months at the time of the sur-vey. For each birth, the child's survivalstatus at the time of the survey was ob-tained. If deceased, the child's age atdeath was recorded: in days if less thanone month, in months if less than twoyears, or in years. If alive, the child's ageat last birthday was obtained. Date ofbirth, survival status, and age at deathwere used as identifiers for each interval(between 0-12 months of age): (1) birthsexposed to the risk of death in the entireinterval; and (2) among these births,those who experienced death at the end ofa particular age interval between 0-12months (defined by the analytic modelspresented below). Because children whodie in the interval cannot possibly be ex-posed to the risk of death throughout theinterval, their contribution to exposure islimited, and hence was dropped from theanalysis. Children who died at the end ofthe interval were assumed to have beenbreastfed for a period up to the point be-fore death.
EXPLANATORY VARIABLES
Both the DHS and the Enugu surveycollected information on many variablesthat are useful for investigating child sur-vival and breastfeeding behavior. Of thefive categories of proximate mortality de-
terminants identified by Mosley andChen (1984), variables representing fourwere included in DHS: maternal factors(age, parity, and birth spacing), environ-mental factors (source of drinking waterand material of the dwelling units), nutri-tional status (breastfeeding practices andanthropometric measurements), and per-sonal illness control (circumstances sur-rounding childbirth, child immunizations,and illness treatment).
Breastfeeding information from boththe DHS and the Enugu survey can be an-alyzed in two ways. It could be ascer-tained whether a woman was still breast-feeding her most recent child at the timeof the survey. On the assumption thatwomen do not breastfeed one child afterthe birth of the next, current status breast-feeding information (yes/no) can be usedto determine the proportion of childrenwho are still breastfed by single monthsof age at interview (John et al., 1988). Onthe other hand, retrospectively reportedages of weaning for children who are nolonger breastfeeding can also be used.
There has been considerable debateabout the validity and reliability of re-sponses to survey questions regarding theduration of breastfeeding and the reasonsfor not initiating or for discontinuingbreastfeeding (Lesthaeghe and Page,1980). Information collected in many ret-rospective surveys (in many developingcountries) has indicated that substantialproportions of breastfeeding durationswere concentrated around digits whichare multiple of three or six (heaping), andthese findings have been interpreted bythe analysts as evidence for defectivedata (Lesthaeghe and Page, 1980). None-theless, those data have been used byresearchers because they are "objective,"unlike data on reported reasons for stop-ping breastfeeding, which are perceived
Dow
nloa
ded
by [
Uni
vers
ity o
f W
ashi
ngto
n L
ibra
ries
] at
16:
50 0
9 A
ugus
t 201
3

100 Ahiadeke et al. Social Biology
by some as "subjective." While the objec-tive data on initiation and duration ofbreastfeeding have provided a rationalefor their use by researchers, the "subjec-tive" breastfeeding data have been ques-tioned with arguments that invoke theiraccuracy and reliability. However, de-tailed studies of methodological aspectsof the measurement of reasons of breast-feeding cessation carried out in the 1970s(Winikoff et al., 1988; Greiner et al.,1981; Romero-Gwynn and Carias, 1989)and as part of the current DHS program(Macro International Inc., 1993) do notsuggest that these data are seriouslyflawed.
Analyzing the MFLS-1 and MFLS-2data in an attempt to understand the linksbetween the "subjective" and "objective"data on breastfeeding patterns, DaVanzoand Defo (1996) concluded that there is"remarkable similarity in the distributionsof reported reasons for no or short breast-feeding."3 The authors found in both sur-veys that no/insufficient breastmilk is themost frequently given reason for no orshort breastfeeding. Maternal and childhealth and mortality, inconvenience tomother, mother's employment, and thechild not wanting to breastfeed are theother reasons given for no/short breast-feeding in the two surveys. The authorsalso found a positive association betweenlow birth weight and the likelihood of notinitiating or continuing breastfeeding.Health reasons were also reported as areason for not initiating or continuingbreastfeeding among women who had noprenatal care visits. These findings areconsistent with evidence that suggests aclose association between health condi-tions at birth of the mother and the child
3Reported reasons for stopping breastfeeding in-clude mainly death of child, illness of mother, and in-sufficient milk.
and the probability of initiating andcontinuing breastfeeding. Health reasonswere also reported as a reason for not ini-tiating or continuing breastfeeding amongwomen who had no prenatal care visits.These findings are consistent with evi-dence that suggest a close association be-tween health conditions of the motherand the child at birth and the probabilityof initiating and continuing breastfeeding.In short, the literature suggests stronglythat most of the reasons given for notinitiating or for discontinuing breastfeed-ing are not seriously flawed, and that theyby and large serve their intended pur-poses. Data on reason-specific breastfeed-ing practices are, in effect, informativenot only in verifying hypotheses aboutthe influences on breastfeeding patternsgenerated from prospective data, but alsoin supplementing information on factorsthat covary with duration of breastfeedingthat are collected by retrospective surveyslike the DHS and the Enugu survey.
For the data on hand, information onduration of weaning was collected for allbirths in the five years preceding thesurvey. The inclusion of all births that oc-curred during a fixed time period preced-ing the survey avoids biasing results up-ward by excluding births to women withshort birth intervals. In our analysis, carewas taken to include only those childrenfor whom the required breastfeeding in-formation was available.
OTHER EXPLANATORY VARIABLES
Prenatal and postnatal indicators rele-vant to healthy birth outcomes includethe timing of prenatal health care, birthweight, and breastfeeding. Previous re-search suggests that timely prenatal careand the changes in health practices it mayinduce are important for healthy birthoutcomes (Singh et al., 1985). In fact, for
Dow
nloa
ded
by [
Uni
vers
ity o
f W
ashi
ngto
n L
ibra
ries
] at
16:
50 0
9 A
ugus
t 201
3

Vol. 47, No. 1-2 Breastfeeding Behavior 101
those women most likely to experiencehigh-risk pregnancies, the quantity andquality of care may be critical in promot-ing healthy birth outcomes (Gortmaker,1979). High-risk mothers include thosewho are poorly educated, unmarried, oryoung at the time of conception. Compli-cations in pregnancy are more likely tooccur for women who receive late prena-tal care (the third trimester of pregnancy)or no prenatal care at all. Prenatal care isassociated with higher birth weight (Gort-maker, 1979), which in turn is related to alower risk of infant death. Two causescan generally be hypothesized as con-tributing to unequal prenatal care in de-veloping countries: inadequacies of thehealth care system and the correspondingurban bias. Gortmaker (1979) found thatwomen with disadvantaged backgrounds(rural and/or illiterate) may be less wellintegrated into society, as indicated bytheir sparse interactions with social orga-nizations, institutions, and agencies. Thus,they may possess fewer skills and lessknowledge in seeking prenatal care. Theprobability of a child's mother practicinghealthy behavior while pregnant thereforeseems likely to be affected by many so-cioeconomic and demographic factors,such as the economic status of the house-hold, maternal educational attainment, thebirth order of the child, and the age of themother at the child's birth. A dichoto-mous variable indicating whether prena-tal care was obtained in the first trimesterwas created to measure the direct effectof health practices on mortality.
Birth weight reflects intrauterinepathology, prematurity, and ability to sur-vive illnesses immediately after birth(Gibson, 1990). It is also related to sizelater in infancy and hence to the abilityto survive infectious illnesses in post-neonatal infancy. Low birth weight (less
than 2,500g) was indicated in the analysisby a dichotomous variable. Because thehealth consequences of low birth weightdraw attention to the importance of its as-sociations with birth interval, birth order,and the age of the mother at birth of thechild, these latter variables are also in-cluded in the analysis. For example, se-lective breastfeeding behavior is likely tointeract with the mother's age at birth ofthe child, parity, and birth interval. Inparticular, maternal age at the time of thechild's birth is expected to influence theextent of and reason-specific breastfeed-ing duration in at least two ways: First, ateenage mother may be less aware ofappropriate breastfeeding practices and,lacking the appropriate advice, may bemore likely to stop breastfeeding (if initi-ated at all) if she fails to produce milkafter a few attempts; hence "no milk"may be given as the reason for stoppingbreastfeeding. Secondly, we expect thatprimiparas (women who have given birththe first time) should be more likely to re-port "no milk" as a reason for not initiat-ing or for stopping breastfeeding. Thechild's birth order is also expected to af-fect his or her health status through itsimpact on breastfeeding and hence nutri-tion. This occurs because higher birth or-der children can suffer from increasedstrain on family resources, particularlythe time available for child care.
An examination of diet and feedingpractices must address three issues:(1) whether the child received breast milkfor some interval of time; (2) whether itreceived any other form of milk in theinterval; and (3) whether the child hasbegun to receive solid or semisolid foodsin the specified interval of time. Thevariables considered here include durationof unsupplemented and supplementedbreastfeeding and type of supplemental or
Dow
nloa
ded
by [
Uni
vers
ity o
f W
ashi
ngto
n L
ibra
ries
] at
16:
50 0
9 A
ugus
t 201
3

102 Ahiadeke et al. Social Biology
weaning foods. DHS asked about earlyinitiation of suckling; timely first suck-ling (defined as suckling within 1 hour ofbirth) was measured by the variablecolostrum. For both Nigeria and Enugu,the answers to the question "What is thereason for never or for stopping breast-feeding?" are useful for examining re-verse causation bias because the reportedreason for weaning can now be employedin a direct analysis.
Individual skills, health, and time arethe three basic elements that determinethe productivity of household members.Measures of parents' time and health sta-tus are usually not available in DHS-typesurveys, but skills are typically measuredby the level of education attained by par-ents. Maternal health and nutritional sta-tus affect the health and survival of thechild through the biological links be-tween the mother and infant during preg-nancy and lactation. A mother's responsi-bility for her own care during pregnancyand the care of her child through thechild's most vulnerable life stages havedirect relevance for child survival.Mother's level of education can, there-fore, affect the child's survival status byinfluencing her attitudes and choices onprenatal medical visits, breastfeeding, foodpreparation, washing of clothes,. bathingthe baby, and sickness care, and by in-creasing her skills in health care practicesrelated to nutrition, hygiene, preventivecare, and disease treatment. The variousmeasures of breastfeeding behavior andmortality and their definitions are sum-marized in Table 1.
MODEL BUILDING ANDESTIMATION
Although the central focus of thisstudy is to examine the link between re-
verse causation and breastfeeding behav-ior on the health outcome of the child, thecausal mechanism is embedded in acomplex causal framework that includesproximate as well as background vari-ables. Problems of model specificationcan arise in assessing the effects ofbreastfeeding on infant mortality. Be-cause breastfeeding is important for nutri-tional, immunity, and hygienic purposes(in an infectious environment), control-ling for associated factors like birthorder, birth interval, and mother's age atthe birth of her child is important.
Parity and mother's age at the child'sbirth are potential sources of distortionsbecause both are related to the length of agiven birth interval, and simultaneouslyexert effects on the risk of mortality (Leeet al., 1988). In addition, both variablesinfluence the existence and duration ofbreastfeeding, thus creating the potentialfor artifactual effects between the latterand the risk of mortality (Palloni andTienda, 1985; Hobcraft et al., 1983). Asecond potential problem arises from in-appropriate representation of the underly-ing causal mechanisms reflecting the ef-fect of breastfeeding on infant mortality.In some cases, breastfeeding never startsbecause conditions in utero precipitatedeath immediately after birth. Fetalgrowth deficiencies and immaturity pro-duce births subject to a high risk of mor-tality even before breastfeeding begins.In these cases, death leads to no breast-feeding rather than the reverse. All ofthese problems can lead to model mis-specification and simultaneity bias that, ifuncorrected, may exaggerate the positiveeffects of breastfeeding on child survival.
The effect of breastfeeding on infantand child mortality also poses censoringproblems that can bias the estimates andtests. This happens because the length of
Dow
nloa
ded
by [
Uni
vers
ity o
f W
ashi
ngto
n L
ibra
ries
] at
16:
50 0
9 A
ugus
t 201
3

TABLE 1
DEFINITION OF VARIABLES USED TO ADDRESS THE REVERSE CAUSATION ISSUE IN THE MORTALITY MODELS
VARIABLES OPERATIONAL DEFINITION COMMENTS
OutcomeMortality (births 0 months)Mortality (births 0-12 months)
Mortality (births 1-12 months)
ExplanatoryBF stopped because of illness
BF stopped for other reasons
ControlsAge of mother at child's birth
Colostrum
Birth order
Birth interval
BackgroundEducation of mother
Prenatal careTetanus injection
Prenatal visits
Place of delivery
Infant detailsSex of child
Period in days, weeks, or less than one month when death occurredPeriod in months from birth to death; right-censored at interviewdata or age 12 monthsPeriod in months from age one month after birth to first birthday;cases are right-censored at date of interview or age 12 months
A time-dependent covanate accounting for whether BF started orstopped or never began for reasons of illness onlyA time-dependent covariate to account for other reasons whyBF stopped
Child's birthdate in century months minus mother's DOB incentury months. Categories: <19; 19-29; and >29 yearsDummy variable indicating if baby was put to breast soonafter delivery
Indicated by a set of dummy codes for births prior to the indexchild, who is breastfed
Indicator variables for the intervals <18 months; 18-24 months;> 24 months
A set of dummy codes to capture: no schooling; primary;secondary and higher education
Dummy for whether mother was given tetanus injection (=1)at pregnancy
A dummy variable indicating if mother made a visit during thefirst trimesterA set of dummy codes to indicate where baby was delivered:Hospital/clinic; Home; Other
Dummy variable indicating sex of the index birth
Assumed to have survived one monthTo account for neonatal mortality
Infants who died in the first month of life wereexcluded because of censoring
To show that illness determined BF behavior
Mainly to exclude the illness variable
To monitor selection bias due to age bounds ofmother and childcare practicesIndicates how soon breastfeeding began
Omitted category is mostprevalent group
Monitors the role of gestational age and low birthweight babies
A proxy for mother's knowledge of health andchildcare
To monitor tetanus infection, a serious infant killer
Monitors fetal health until birth
Home delivery is the category omitted
Can monitor biological differences at birth
f
aB
eraWS-3.o1
Dow
nloa
ded
by [
Uni
vers
ity o
f W
ashi
ngto
n L
ibra
ries
] at
16:
50 0
9 A
ugus
t 201
3

104 Ahiadeke et al. Social Biology
time a child breastfeeds is subject to therisks of weaning and death. The averageduration of breastfeeding among thosewho die before a specified age is gener-ally shorter than among those who sur-vive beyond that age, because deathtruncates breastfeeding. This produces anartificial association between breastfeed-ing duration and mortality. This bias canbe assessed by comparing the survivalof children beyond a specified age withwhether or not they breastfed up to thatage. The statistical procedures adoptedaddress some of the issues raised.
RANDOM EFFECTS LOGIT MODELS
In studying a problem such as reversecausality, the scientific issue is the dis-tinction between whether the strongesteffect of illness causing death or the indi-rect effect (operating via cessation ofbreastfeeding) do have differential impacton mortality. Although children who areweaned in the neonatal period (or neverbreastfed) because of illness or weaknessto suckle may experience equally highrisks of death, as in the direct case of ill-ness causing death, it is not clear howmuch the cessation of breastfeeding (dueto illness) contributes to death. In this re-gard the objective must be to determinewhether there is significant associationwith death through the cessation of breast-feeding. The dependence of the marginalexpectation of each variable on healthstatus becomes the focal issue in theanalysis. To reduce the influence of con-founders, regression analysis must adjustfor characteristics operating through ces-sation of breastfeeding and those directlydue to illness.
For a binary data, most people wouldstart with a simple standard logit function
for the outcome variable y (death in ourcase), we guess, but we want to think interms of conditional models in whichcausal ordering is paramount. The pre-ferred approach here is to work with con-ditional models containing random ef-fects. In these models, information fromother causes of death (y±\ k # j , say) ispassed quite naturally to the regressionfor y- via the random effect e;, withoutforcing any particular closed form on thedependence of y- on {y^; k ¥= j} .
In effect, the causal ambiguity istested first on the data using a random ef-fects logit technique with several differ-ent models. The random effects modelapproach is also useful in accounting forcorrelation, overdispersion, and subject-specific inference (Kuk, 1995). Over thefirst 12 months of life, the risk of dyingusually exhibits a striking monotonic de-cline and endogenous causes of death aresupplanted by exogenous ones (Trusselland Hammerslough, 1983). It is thereforeappropriate to study breastfeeding behav-ior in the first 12 months of life. Follow-ing the example of Montgomery et al.(1986), we used the random effects logittechniques to describe a child's state attime t months of age by a pair of zero-onerandom variables (Bt, S t), where B t
equals 1 if a child is breastfed at time t, 0otherwise, and S, equals 1 if the child isstill alive at time t, 0 otherwise. Modelsusing the Nigerian data measure lactationfor three different time periods, namelyage in days but less than one month atdeath (Model 1), 0-12 months (Model 2),and 1-12 months (Model 3), respectively.
It is well known in the demographicand medical professions that the progno-sis for survival of low birth weight babiesis much worse than that for normal birthweight babies (Bern, 1971). Birth weight
Dow
nloa
ded
by [
Uni
vers
ity o
f W
ashi
ngto
n L
ibra
ries
] at
16:
50 0
9 A
ugus
t 201
3

Vol. 47, No. 1-2 Breastfeeding Behavior 105
carries information not only on the child'sown health and hence on the prognosisfor successful breastfeeding and survival,but also on factors that are specific to thefamily (Singh et al., 1985). Shared familybackground may, to a large extent, be dueto common uterine environment and tocommon practices of the mother or fam-ily during pregnancy, in which nutritionis of key importance (Leichting et al.,1975).
Simultaneity problems are avoided bytaking mortality within each age segmentas a function of conditions prevailing atthe onset of the segment. Thus, to be in-cluded in the analysis for the age interval1—12 months, the infant must have sur-vived through the first month of life.These divisions will also suppress the si-multaneity bias affecting the relation be-tween following birth interval and therisk of death of the (index) child (Palloniand Tienda, 1985). First births are treatedseparately from other births because theymay be subjected to somewhat higher-than-average mortality risks (Hobcraft,McDonald, and Rutstein, 1983). Theproblem of censoring is also reducedwhen the breastfeeding variables aregrouped into age segments.
Analyzing these models involves char-acterizing the dependence of death ofchildren on explanatory variables and de-scribing the associations between theresponse and explanatory variables. Theresponse is health outcome of the child(with dead = 1 and surviving = 0). Ran-dom effects logit models define the loga-rithm of the odds of dying in various agesegments as a function of the explanatoryvariables, allowing us to estimate the ef-fects of these variables. Let Y i k be the bi-nary indicator of the health outcome forbreastfeeding child k in household j in
cluster i. A random effects logit modelcan thus be written as:
logit Pr(Y i jk=lPM + pG
where S is the vector of variables repre-senting selection (or breastfeeding) fac-tors, M the vector of maternal factors(e.g., age at birth), G the vector of preg-nancy factors (like prenatal care), D thevector of variables representing infant de-tails (e.g., birth order), and P the vector ofbackground factors (e.g., maternal educa-tion). The unobservable random effect e-is assumed to be common to the jthhousehold in the ith cluster. The correla-tion between e- and e^ (k # j) and thevariance of ey determine the design ef-fects for each sample.
SURVIVAL CURVES
We plotted the survival curves forseven groups of breastfeeding infants, us-ing the Stata procedure "Kapmeier" (Stat-aCor, 1995): (1) weaned, (2) mother ill,(3) insufficient milk, (4) mother pregnant,(5) child ill, (6) mother working, and (7)still breastfeeding. The formula for thesesurvival curves is:
where d. is the number of deaths at time jamong breastfeeding children and n̂ isthe number of observations at risk ofdeath. To obtain dj and n,, we let k =1,....,N index the individual observa-tions. Define nkj to be 1 if child k is aliveat time j and 0 otherwise, and dkj to be 1if child k died at time j and 0 otherwise.Then d- = £kdk- and n̂ = 2knkj. Theprocedure merely counts the alive obser-vations and the number dying at each
Dow
nloa
ded
by [
Uni
vers
ity o
f W
ashi
ngto
n L
ibra
ries
] at
16:
50 0
9 A
ugus
t 201
3

106 Ahiadeke et al. Social Biology
specified time. Thus for example, if achild died at time j , he/she is presumedalive just before time j and is assumeddead just after j . This distinction is cru-cial here because the curves presented be-low are defined at time j and so a childwho dies at time j and was breastfed untildeath will be categorized as still breast-feeding before j but not after. The prob-lem here is one of status (which is thesame for a period of time) versus events(which happen at a point in time).
RESULTS
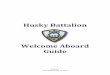
Figure 2 shows the Kaplan-Meier sur-vival curves for the seven breastfeedinggroups defined above. Note, for reasonsgiven above, that the number of womenwho wean in month 0 or 1 is likely to besmall, and of these, none may describethe reason for weaning as, say, "motherill" (Group 2, Figure 2) or "mother work-ing" (Group 6, Figure 2) so that in theend, there may be no survival curves forsome groups (as can be seen from Figure2). This product-limit estimate of the sur-vival curve produces a descending stepfunction where each drop indicates thenumber of deaths. Of particular interest isthe curve for Group (5), children whowere reported ill at the time of the survey.It reflects the survival status of thosechildren who were ill in the early monthsand died over the course of the first 12months. The fact that this curve dropsfaster than any other group's curve is anindication of the fact that should breast-feeding be hampered in this group ofchildren, they are the ones who will sur-vive the least. The graph shows that mostof the children in Group (5) died beforetheir first birthday, and all of those whosurvived the first birthday did not reachtheir second birthday.
The Group (4) category, pregnancy, isan important reason for cessation ofbreastfeeding between 6 and 12 monthsof life; it is the closest to Group (5) insteepness. The other curves do not appearto fall steeply, which suggests that childsurvival is least hampered in these cate-gories. The graph shows on the wholethat not only do the influences of thegrouping criteria on infant and childsurvival vary with age of the child, butthey also vary with the reasons reportedfor initiating or stopping breastfeedingwithin a given age interval.
We compared the survival curves ofthe various groups by computing the log-rank statistics under the assumption thatthe underlying survival curves are thesame, using the x2 statistic (Peto andPike, 1973). The results indicate that thegroups are indeed different in both theirreason-specific and age-specific breast-feeding behavior (p < 0.01 in each case).For the control group (still breastfeed-ing), there were 16 observed deaths, butonly 3.68 would be expected if these chil-dren had the same survival rate as allother categories of children. This indi-cates that breastfeeding for a longer pe-riod (here, 6 or more months) has a bene-ficial effect on infant survival.
We now examine the estimated logitmodels in Table 2 for Nigeria as a wholeand Table 3 for Enugu, a subregion ofNigeria, to gain more insight into thebreastfeeding bias attributable to illness.Because it is difficult to discern thecausal relationship between breastfeedingand illness or death during the first monthof life, the models were constructed to re-flect the effect of the inclusion of theneonates. Children who experience healthcomplications immediately after birthmay never begin breastfeeding at all. Ifsuch children experience recurrent illness
Dow
nloa
ded
by [
Uni
vers
ity o
f W
ashi
ngto
n L
ibra
ries
] at
16:
50 0
9 A
ugus
t 201
3

Vol. 47, No. 1-2 Breastfeeding Behavior 107
1.00 -
£0.75-
nID
oa 0.50
0.25-
0.00 -
Notes: Group 1Group 2Group 3Group 4Group 5Group 6Group 7
I...T T T T 1 .J j | ^ 7 7 7 7 7 7
Age (in months breastfed)
weanedmother i l l *insufficient milkmother pregnantchild i l lmother working*s t i l l breastfeeding
*See text for the explanation of the absence of Groups 2 and 6curves.
FIG. 2.—Kaplan-Meier survival curves for reason-specific breastfeeding infants.
or die early, an association between neverhaving breastfed and failure to survivewill be observed, regardless of the actualeffects of breastfeeding. Removing thisbias requires controlling for the healthstatus of the child at birth and shortlythereafter. The rationale for omitting theage category 0 months in the subsequentmodel is that those children who survivedthe first month of life were less likely toexperience conditions that would simulta-neously affect their health and theirmothers' breastfeeding behavior. Model 1(Table 2) for the Nigerian data clearly in-cludes all children who died beforereaching the age of one month. With thebenefit of hindsight, one expects effectsestimated controlling for health condi-
tions at birth to change estimates consid-erably in comparison to those estimatedwithout any controls. Model 2 includesall children aged 0-12 months whileModel-3 excludes children aged 0 monthsfor the Nigerian data. In the case ofEnugu, Model 1 (Table 3) includes allchildren aged 0-12 months while Model2 includes children aged 1-12 monthsonly.
REVERSE CAUSATION
AND BREASTFEEDING
An examination of the coefficients forlactation in Model 1 (Table 2) for Nigeriashows that the inclusion of younger chil-dren increases the size of the effects ofthe illness variable greatly. For Nigeria,
Dow
nloa
ded
by [
Uni
vers
ity o
f W
ashi
ngto
n L
ibra
ries
] at
16:
50 0
9 A
ugus
t 201
3

TABLE 2'ACTORS ON Jl
NIGERIA (DHS)
COVARIATES Beta
Model 1< 1 moiuh
SE
AGE AT DEATH
Model 20-12 months
Beta SE Beta
Model 31-12 months
SE
Breastfeeding stopped (still=0)Mother illInsufficient milkChild illOther reasons
Fed colostrum (no=0)Birth weight (<2,500g)Age at birth (18-29=0)
< 18 years30+ years
Birth order (1st birth=O)2-34+
Previous child died (yes=O)Prenatal care (yes=O)Tetanus vaccination (no=0)Education (no=0)
PrimaryHigher
InterceptNo. of observationsLog likelihood
0.273*0.437*0.719***0.510
-0.383-0.344
0.237-0.138*
-0.148**-0.277-0.253**
0.599***-0.320*
0.129-0.211
0.587610
-236.0
0.1290.2340.0470.4730.2910.403
0.3090.068
0.0490.1850.0810.0870.161
0.1250.201
0.2660.4220.638***0.3760.3720.320
0.2290.135*
0.143**0.2730.249**0.563***0.329*
0.1270.2130.419
3276-1020.6
0.2320.3880.0830.3650.2930.397
0.3120.063
0.0900.1880.0970.1890.160
0.1220.209
0.2590.4200.336**0.2980.2590.318
0.2200.131*
0.142**0.2720.2320.524**0.332*
0.1230.2170.417
3235-1009.8
0.2310.3850.0910.2370.2760.392
0.3130.060
0.0500.1890.1070.2350.157
0.1200.209
> = p , 0.10; • • = p < 0.05; • • • = p < 0.01GO%
Ew5'D
ownl
oade
d by
[U
nive
rsity
of
Was
hing
ton
Lib
rari
es]
at 1
6:50
09
Aug
ust 2
013

Vol. 47, No. 1-2 Breastfeeding Behavior 109
the odds of death increased by a factor of2.1 (=exp(0.719)) from the baselinevalue when a breastfeeding child aged< 1 month is weaned because he becomesill (p < 0.01). From Table 2, the odds ofdeath for breastfeeding children who be-come ill increase by a slightly smallerfactor of 1.9 (=exp(0.638), p < 0.01)when the age at death range is widenedfrom 0 months to 0-12 months. The in-crease in the odds of death is further re-duced to a factor of 1.4 (=exp(0.336), p
< 0.05) when children aged 0 months areexcluded from the equation. For Nigeria,the level of significance decreases withthe exclusion of the young infants (agedless than one month). For Enugu, Model1 (Table 3) shows that the odds of deathfor children aged 0-12 months increaseby a factor of 26.7 (p < 0.01) for weanedchildren who are too ill to breastfeed.Table 3 further shows for Enugu that theodds of death to weaned breastfeedingchildren who become ill increase by a
TABLE 3RANDOM EFFECT LXXJIT MODELS OF BREASTFEEDING STATUS AND RELATED FACTORS ON
CHILD MORTALITY FOR MOST RECENT BIRTHS: ENUGU 1991
VARIABLE
Why BF stopped (still BF=0)Insufficient milkMother too illChild too illOther reasons
Birth order (1st birth=O)2-34 or more
Age at birth (18-29=0)<18 years30+ years
Previous child died (yes=0)No death
Prenatal care (yes=0)No care
Tetanus vaccination (yes=0)No vaccination
Education (no=0)PrimaryHigher
InterceptNumber of casesLog likelihood
0-12 months
Model 1Beta
0.8330.390**3.283***
-0.237**
-0.530**-0.244
0.370**-0.217
-0.397***
0.378**
0.572***
0.125-0.233*
-4.3391933
-202.2
SE
0.7060.1890.5170.081
0.1550.193
0.1330.201
0.090
0.103
0.132
0.1220.109
ACE AT DEATH
J—12 months
Model 2Beta
0.9750.2131.627**
-0.133***
-0.519**-0.230
0.473-0.139*
-0.286**
0.359*
0.553**
0.121-0.232*
-4.2941898
-197.3
SE
0.7880.2250.5170.036
0.1500.190
0.2210.059
0.093
0.189
0.187
0.1200.109
NOTE: BF = Breastfeeding*=/><0.10;** =p<0.05; •**=/><0.01
Dow
nloa
ded
by [
Uni
vers
ity o
f W
ashi
ngto
n L
ibra
ries
] at
16:
50 0
9 A
ugus
t 201
3

110 Ahiadeke et al. Social Biology
TABLE4ESTIMATED HAZARD MODELS OF BREASTFEEDING EFFECTS AND RELATED FACTORS ON MORTALITY OF
CHILDREN AGED 0-12 MONTHS BEFORE THE SURVEY: ENUGU 1991
COVAMATE
Model 1"
Hazard ratio
Model 2
Hazard ratio
Still breastfeedingNo illness*Child ill4
Other reasons4
Age at birth26 or more years<19 years19-25 years
Birth order1st order2-3 order4+ order
EducationNo educationPrimaryHigher
dfAG2
BICNumber of cases
1.02.3
0.8**
1.02.6**0.8**
1.01.7*1.6
1.00.70.6**
9
3304.82082
1.01.93.6***0.7***
1.02.5**0.6***
1.01.5*1.3
1.00.70.6**
1522.3
3310.72111
NOTES: "This model excludes 29 observations for which children were too ill to suckle; but were finally included in Model 2'Time-varying covariate (excluding children weaned as a result of illness)• = p < 0.10; • • = p < 0.05; • • • = p < 0.01.
dramatically smaller factor of 5.1 whenthe age at death does not include deathsin the neonatal period. It appears thatchanging breastfeeding practices as a re-sult of illness can increase a child's sus-ceptibility to death more in the youngerage segment. The sizes of the coefficientsstrongly suggest that the problem of re-verse causation is strongest during theneonatal period.
Based on the results of tables 2 and 3,prior illness does appear to influence theeffect of breastfeeding on mortality, par-ticularly in the neonatal segment. To fur-
ther confirm our findings on the questionof the magnitude of this influence, anevent history approach was similarly ap-plied to the Nigerian and Enugu data sets.The approach was to transform the datawith births as observations because at thetime of the survey, the duration of breast-feeding had not been completed for somebirths. For other births, breastfeeding wasterminated prematurely by the death ofthe infant. The event history model re-sults (not presented here but availablefrom the authors) show findings similarto the random effect models.
Dow
nloa
ded
by [
Uni
vers
ity o
f W
ashi
ngto
n L
ibra
ries
] at
16:
50 0
9 A
ugus
t 201
3

Vol. 47, No. 1-2 Breastfeeding Behavior 111
TABLE5ESTIMATED HAZARD MODELS FOR THE COVARIATES OF CHILD MORTALITY FOR SAMPLE OF
MOST RECENT BIRTHS: NIGERIA DHS 1991
VARIABLE
Why breastfeeding stoppedStill breastfeedingChild ill1
Other reasons1
Fed colostrumYes, colostrumWaited
Birth order1st birth2-3 births4 + births
Birth interval25 months or more<18 months18-24 months
Birth weight> 2,500 gramsLess than 2,500g
Previous child diedYesNo
Age at birth18-29 years<18 years30+ years
Tetanus vaccinationNo vaccinationYes vaccination
Number of casesLog likelihood
0-12 months
Model 1Hazard ratio
1.001.53***1.28
1.001.37
1.000.61**1.13
1.001.17**0.57
1.001.32**
1.000.73*
1.001.21*0.55
1.000.69*
8041-1262.3
AGE AT DEATH
3-12 months
Model 2Hazard ratio
1.001.22**1.05
1.001.15
1.000.60**1.13
1.001.15*0.63
1.001.09*
1.000.69*
1.001.020.33
1.000.54**
8033-1206.6
NOTE: 'Time-dependent covariate* = / > < 0.10; • • = / ? < 0.05; • • • = p < 0.001
SUMMARY AND CONCLUSIONS
It is often concluded that the lack ofbreastfeeding could be the cause of theelevated mortality among infants. Thisproblem arises because it is not known
whether the decision never to breastfeedor to stop breastfeeding is made bychoice or necessitated by illness of thechild. Some of the information necessaryfor analyzing this problem was availablefor both the Nigerian DHS and the Enugu
Dow
nloa
ded
by [
Uni
vers
ity o
f W
ashi
ngto
n L
ibra
ries
] at
16:
50 0
9 A
ugus
t 201
3

112 Ahiadeke et al. Social Biology
survey. The results presented above showthat the risk of mortality is much higherfor breastfeeding children who were illduring the neonatal segment than it is fornormal breastfeeding children of thesame age. The analysis shows that lowbirthweight babies are more likely to dis-continue breastfeeding or not to initiate itat all in the early days after birth.
The question of how important any bi-ases imparted by an initial selectionmechanism are to the survival of a breast-feeding child would more likely havenegative implications for low birthweight and sick babies than for normalbirth weight babies. This observation alsosupports the immunological and bio-chemical evidence that the benefits ofbreastfeeding are likely to be greatest inthe early part of the first year of life,when the infant's enzymatic systems arenot fully developed and its defensesagainst disease are weak.
In tradition African societies such asthose in Nigeria, there are few studiesthat document whether or not a motherwould withhold breast milk from thechild in the event that the child is ill. Wewould imagine that mothers who do notbreastfeed their children in the event that
the children are ill have to do so as thelast resort. The group of children whosebreastfeeding had to be curtailed in oursample was selectively small and perhapsbiased. They may largely be childrenwhose mothers were not healthy enoughto breastfeed. They may also be childrenwho, because of some special disability,could not suckle. The risk associated withsuch conditions probably exaggerated thesurvival.
It is, however, important to stress thatas useful as the approach to the studymay be, it does not completely eliminatethe possibility that the reported effects ofbreastfeeding on survival are confoundedby weaning due to illness. The bias may,in fact, be shifted in the other direction.Perhaps a carefully designed panel of datacould resolve the issue once and for all.
ACKNOWLEDGMENTS
The authors gratefully acknowledge theNigerian Federal Office of Statistics andMacro International Inc., Maryland for accessto the Nigerian Demographic and Health Sur-vey data. The first author also acknowledgesthe financial support given by the RockefellerFoundation while at the Population and De-velopment Program, Cornell University.
REFERENCES
ADAIR, L., B. POPKIN, and D. GUILKEY. 1993. Theduration of breastfeeding: how is it affectedby biological, socioeconomic, health sector, andfood industry factors? Demography 30:63-72.
BARANOWSKI, T., D. BEE, D. RASSIN ET AL. 1983.Social support, social influence, ethnicity, andthe breastfeeding decision. Soc. Sci. Med.21:1599-1672.
BEM, R. T. 1971. Some mathematical propertiesof weight for height indices used in measuresof adiposity. Brit. J. Prevent. Soc. Med. 25:42-50.
DAVANZO, J., and B. K. DEFOE. 1996. An assess-ment of the correlates of age-specific and reason-specific breastfeeding practices in Malaysia.Santa Monica, CA: Rand Corporation.
DAVANZO, J., J. P. HABICHT, and W. P. Butz. 1984.Assessing socioeconomic correlates of birth-
weight in Peninsular Malaysia: ethnic differ-ences and changes over time. Soc. Sci. Med.18:387-404.
FEDERAL OFFICE OF STATISTICS AND MACRO INTER-NATIONAL INC. 1992. Nigerian Demographicand Health Survey 1990, Calverton, Maryland:FOS and MI.
FORSTE, R. 1994. The effects of breastfeeding andbirth spacing on infant and child mortality inBolivia. Pop. Stud. 48:497-511.
GIBSON, R. S. 1990. Principles of Nutritional As-sessment. New York: Oxford University Press.
GORTMAKER, S. 1979. The effects of prenatal careupon the health of the newborn. Am. J. Pub.Health 69:653-660.
GREINER, T., P. ESTERIK, and M. LATHAM. 1981.The insufficient milk syndrome: an alternativeexplanation. Med. Anthropol. 5:233-242.
Dow
nloa
ded
by [
Uni
vers
ity o
f W
ashi
ngto
n L
ibra
ries
] at
16:
50 0
9 A
ugus
t 201
3

Vol.47,No..l-2 Breastfeeding Behavior 113
HOBCRAFT, J., J. W. MCDONALD, and S. O. RUT-STEIN. 1983. Child-spacing effects on infant andearly child mortality. Pop. Index, 49:585-618.
HABICHT, J. P., J. DAVANZO, and W. P. BUTZ. 1986.Does breastfeeding really save lives or are ap-parent benefits due to biases? Am. J. Epidemiol.123:279-290.
. 1988. Mother's milk and sewage: their in-teractive effects on infant mortality. Pediatrics18:456-461.
HOLLAND, B. 1987. Breastfeeding and infant mor-tality: a hazard model analysis of the case ofMalaysia. Soc. Biol. 34: 93-98.
HUFFMAN, S., and B. LAMPHERE. 1984. Breastfeed-ing preference and child survival. In W. H.Mosley and L. Chen (eds.), Child Survival: Stra-tegies for Research, A Supplement to Volume 10Pop. Develop. Rev., p. 93-116. Cambridge:Cambridge University Press.
JELLIFFE, D. B., and E. F. JELLIFFE. 1978. HumanMilk in the Modern World. Oxford, U.K.: Ox-ford University Press.
JOHN, A. M., J. A. MENKEN, and J. TRUSSELL. 1988.Estimating the distribution of interval length:current-status and retrospective history data.Pop. Stud. 42:115-127.
KALBFLEISCH, J. D., and B. L. PRENTICE. 1980. TheStatistical Analysis of Failure Time Data. JohnWiley & Sons: New York, 1980.
KUK, A. Y. C. 1995. Asymptotically unbiased esti-mation in generalized linear models with ran-dom effects. Journal of the Royal Statistical So-ciety Series B57:395-407.
LANTZ, P., M. PARTIN, and A. PALLONI. 1992. Us-ing retrospective surveys for estimating the ef-fects of breastfeeding and childspacing on infantand child mortality. Pop. Stud. 46:121-139.
LEE, K., R. M. FERGUSON, M. CORPUZ ET AL. 1988.Maternal age and incidence of low birthweightat term: a population study. Am. J. Obstet. Gy-necol. 158:84-89.
LEEFSMA, M. 1980. The influence of hospital rou-tine on success and breastfeeding. In S. Freirand A. I. Eidelman (eds.), Human Milk, Its Bio-logical and Social Value, p. 24-33. ExcerptaMedica.
LEICHTING, A., J. P. DELGADO. R. E. KLEIN ET AL.1975. Effects of food supplementation duringpregnancy on birthweight. Pediatrics 56:508-512.
LESTHAEGHE, R. J., and H. J. PAGE. 1980. The post-partum non-susceptible period: developmentand application of model schedules. PopulationStudies 34:143-169.
LiZARRAGA, J., J. MAEHR, D . WHIGARD ET AL.1992. Psychological and economic factors asso-ciated with infant feeding intentions of adoles-cent mothers. J. Adoles. Health 13:676-688.
MILMAN, S., and E. C. COOKSIE. 1987. Birth weightand the effect of birth spacing and breastfeeding
on infant mortality. Stud. Fam. Plan. 18: 202-213.
MONTGOMERY, M., T. RICHARDS, and H. I. BRAUM.1986. Child health, breastfeeding and survival inMalaysia: a random effect logit approach. J.Am. Stats. Assn. 81:297-311.
MOSLEY, W. H., and L. CHEN. 1984. An analyticalframework for the study of child survival in de-veloping countries. Population and Develop-ment Review Supplement to Volume 10:25-45.
NAVED, R., and S. KUMAR. 1994. Determinants ofpositive and negative deviance in child nutri-tion. International Food Policy Research Insti-tute (IFPRI), Washington, D.C. Mimeo.
PALLONI, A., and S. MILLMAN. 1986. Effects ofinter-birth intervals and breastfeeding on infantand early childhood mortality. Pop. Stud.40:215-236.
PALLONI, A., and M. TIENDA. 1985. The effects ofbreastfeeding and pace of childbearing on mor-tality of early ages. Demography 23:31-43.
PETO, R., and M. C. PIKE. 1973. Conservatism ofthe approximation of the chi-square in the log-rank test for survival data or tumor incidencedata. Biometrics 29:579-584.
ROMERO-GWYNN, E., and L. CARIAS. 1989. Breast-feeding intentions and practices among Hispanicmothers in Southern California. Pediatrics84:626-630.
SCHWARZ, G. 1978. Estimating the dimensions of amodel. Annals of Statistics 6:461-464.
SINGH, S., A. TORRES, and J. D. FORREST. 1985. Theneed for prenatal care in the United States: evi-dence from the 1985 maternal natality survey.Fam. Plan. Perspect 17:118-124.
STATACOR. 1995. Statistical Software Release 4.0,College Station, TX: Stata Corporation.
STEWART, S. K. ET AL. 1991. Influences on the ex-tent of breastfeeding: a prospective study in thePhilippines. Demography 28:181-193.
TRUSSELL, J., and B. HAMMERSLOUGH. 1983. A haz-ard model analysis of the covariates of infantand child mortality in Sri-Lanka. Demography20:1-26.
VANLANDINGHAM, M., J. TRUSSELL, and L.GRUMMER-STRAW. 1991. Contraceptive andhealth benefits of breastfeeding: a review of therecent evidence. Int. Fam. Plan. Perspect.17:131-136.
WINIKOFF, B., M. CASTLE, and V. LANKARAN (eds.).1988. Feeding Infants in Four Societies: Causesand Consequences of Mother's Choices. NewYork: Greenwood Press.
WRIGHT, A., C. CLARK, and M. BAUER. 1993. Ma-ternal employment and infant feeding practicesamong the Navajo. Medical Anthropology Quar-terly 7:260-271.
Dow
nloa
ded
by [
Uni
vers
ity o
f W
ashi
ngto
n L
ibra
ries
] at
16:
50 0
9 A
ugus
t 201
3