Embed Size (px)
Citation preview

Breast Uplift (Mastopexy)
Procedure Aim and Information Mastopexy (Breast Uplift)
The breast is made up of fat and glandular tissue covered with skin. Breasts may change with variable influences from hormones, weight change, pregnancy, and
gravitational effects on the breast tissue.
Firm breasts often have more glandular tissue and a tighter skin envelope. Breasts become softer with age because the glandular tissue gradually makes way for
fatty tissue and the skin also becomes less firm.
Age, gravity, weight loss and pregnancy may also influence the shape of the breasts causing ptosis (sagging).
Sagging often involves loss of tissue in the upper part of the breasts, loss of the round shape of the breast to a more tubular shape and a downward migration of
the nipple and areola (dark area around the nipple).
A mastopexy (breast uplift) may be performed to correct sagging changes in the breast by any one or all of the following methods:
1. Elevating the nipple and areola 2. Increasing projection of the breast 3. Creating a more pleasing shape to the breast
Mastopexy is an elective surgical operation and it typifies the trade-‐offs involved in plastic surgery. The breast is nearly always improved in shape, but at the cost of
scars on the breast itself.
A number of different types of breast uplift operations are available to correct various degrees of sagginess.
Small degrees of sagginess can be corrected with a breast enlargement (augmentation) only if an increase in breast size is desirable,
or with a scar just around the nipple with or without augmentation. Augmentation increases fullness of the breast and slightly raises
the nipple and areola.
Larger degrees of sagginess will need larger scars on the breasts to correct the problem. A short vertical scar is commonly used, with
or without breast augmentation.
The Procedure
A mastopexy (breast uplift) rejuvenates the breasts by reshaping, uplifting, and tightening sagging, drooping breasts that have lost shape and volume.
The size of the areola (the dark skin circling the nipple) can also be reduced to give a more pleasing appearance. Often no breast tissue is removed with a
mastopexy.
Mastopexy is an operation that is performed under a general anaesthetic. The procedure takes between 2 and 3 hours and can be performed in conjunction with a
breast augmentation.
Mastopexy can be performed as a day surgery procedure or an overnight stay in hospital.
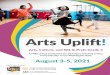
The left breast before the uplift The nipple is lifted into its new position The skin below the nipple is closed to leave
a vertical scar

Prior to performing the surgery, your surgeon will mark on the breasts where the incisions are to be made and where the
nipple/areola should be. You will be sitting in an upright position.
The location of the incisions will vary from person to person depending on the degree of ptosis (drooping), the laxity of the tissues,
size of the areola, and your surgeon's experience, preference and recommendation.
You should discuss this with your surgeon prior to your operation.
The most common technique used for breast uplift include a vertical only incision or a circumareolar (around the areola) incision.
When breast augmentation is performed in conjunction with a mastopexy, an implant is placed in a pocket created under the breast
tissue or beneath the pectoral (chest wall) muscle. This does not affect the incisions.
Dressings and drains will be in place for at least 24 hours after which time a supportive bra is worn.
Recovery time varies with the individual person.
At the time of surgery any tissue removed may be sent to pathology for testing. Costs incurred for this service will be the
responsibility of the patient.
Alternative Treatment
A mastopexy is elective surgery and alternative treatment would consist of not undergoing the surgery or wearing a supportive bra
to uplift the breasts.
If breasts are large and sagging, a breast reduction should be considered.
Risks and potential complications are associated with alternative surgical forms of treatment.
Risks of Surgery All surgery is associated with some risk.
It is important that you understand that there are risks involved with any surgery. Whilst the majority of individuals undergoing surgery do not experience any complications, a minority do and there cannot be any
guarantees in surgery.
With every type of surgery the best possible outcome is sought. The importance of having a highly qualified surgeon and
professional surgical team and facility cannot be overestimated.
Risk to benefit
The choice to undergo a surgical procedure should be based on the comparison of the risk to the potential benefit to you.
Make sure that you take time to read and understand how each potential complication can impact on your life and try to make the risk to benefit comparison
specifically for yourself.
Impact of complications
The risks of surgery involve possible inconvenience if a complication occurs. It may result in an extension of your recovery period and in some cases may need
further surgery. Infrequently, complications may have a permanent effect on your final result.
Financial risks
Financial risks are involved with any surgery. Private health insurance is strongly recommended. If you do not have private health insurance then a complication or
further surgery will add to the overall cost of your surgery.
Risks related to general health
Your general health will impact on the possible risks of surgery. Many of the risks associated with surgery can be predicted. However, your general health plays a
vital role to the outcome of your surgery.
Age carries a greater risk with any surgery. Being overweight carries a greater surgical risk. Other medical conditions such as high blood pressure, high cholesterol,
diabetes, heart and lung disease may also increase your surgical risk.
Smoking greatly increases all risks and complications of surgery.
What else?
Finally other factors, that may not be obvious, can influence the outcome of your surgery and the risks are beyond anyone's control.
Specific Risks of Mastopexy Nipple placement and shape
The shape and position of the nipple-‐areola complex may not be satisfactory following mastopexy.
Nipples may appear too high on the breast if subsequent sagging of the breast occurs.
On the other hand the nipples may be too low on the breast.
Occasionally areola distortion may be present following surgery.
Additional surgery may be required to correct these problems.
Nipple and areola loss

Skin and nipple loss due to necrosis (death of cells in tissue) occurs infrequently.
Tissue loss will require frequent dressing changes or further surgery to remove the non-‐healed tissue.
Skin grafting may be necessary.
This complication is more common in smokers, after infection or after unrecognised bleeding in the breast.
Nipple sensation
Following surgery you may experience a loss of sensation to the skin of the breast and the nipple. Sensory loss is usually temporary but may be permanent. In
some people increased sensation (hypersensitivity) to the nipples occurs after surgery. This settles with time.
Asymmetry
It is normal to have some degree of breast asymmetry before surgery.
The difference in breast size may persist or become more prominent after surgery.
A small reduction in breast volume may be necessary at the time of mastopexy to achieve symmetry.
Asymmetry may become more marked in the first few months due to swelling.
Additional surgery may be required to correct persistent asymmetry.
Contour deformities
Contour deformities may be caused by differences in breast volume and the skin envelope.
Projections of bulging tissue at either end of the scar may occur. They generally improve with time.
Revision by surgery under local anaesthetic may be required.
Epithelial cysts
Small epithelial cysts and recurrent infections may rarely form along the vertical suture line. Surgical excision may be required.
Scars
Scars are initially red, raised and lumpy. It takes anywhere from 3 months to 2 years for scars to fade and mature. The permanent scar will vary from individual to individual. Unsatisfactory scars sometimes occur and often relate to circumstances beyond the control of the
patient or the surgeon. Scars may stretch, they may be uneven, thick or keloid. Your own history of scarring may be an indicator of what to expect. Scar revision can
improve unsatisfactory scars but will never get rid of them. Late changes of shape and volume
The lower half of the breast skin may stretch, increasing the amount of breast tissue below the nipple and causing the nipple to point upward.
This complication often relates to the inherent laxity in the skin and is unpredictable.
The breast shape and volume may change slightly with weight fluctuation, pregnancy, and aging.
Further surgery may be required to correct this problem.
Recurrent droopiness (ptosis)
The benefits of mastopexy may be temporary and droopiness may recur within 2 years, but not to the same degree as before your operation. Pregnancy and
breast feeding after mastopexy will result in breast and skin changes and recurrence of droopiness. Further surgery may be necessary to correct recurrent
droopiness and may involve additional scars or a small implant.
Future pregnancy and breast feeding
Mastopexy is not known to interfere with pregnancy or breastfeeding.
Pregnancy and breast feeding after mastopexy will result in breast and skin changes and recurrence of droopiness.
Persistent pain
Following breast uplift surgery, abnormal scarring in skin and the deeper tissues of the breast may produce pain. Uncommonly persistent pain of unknown or
ambiguous cause may develop and may be difficult or impossible to correct.
Breast implants
Risks associated with breast implants are covered in a separate presentation.
Breast disease
Breast disease and breast cancer can occur independently of mastopexy.
It is recommended that all women perform periodic self examination of their breasts, have mammography according to Australian Cancer Society guidelines, and
to seek professional care should a breast lump be detected.
Women of breast screening age or those with a family history of breast cancer should have a mammogram before the operation.
Firmness
Excessive firmness of the breast can occur after surgery due to internal scarring or scarring around a breast implant if one is used. The occurrence of this is not

predictable. Additional treatment including surgery may be necessary.
Undesirable result
There is the possibility that you may be disappointed with the results from mastopexy surgery.
Disappointments relate to scars, breast shape, or recurrent ptosis.
There are many variable conditions that may influence the long-‐term result of mastopexy.
Secondary surgery may be necessary to perform additional tightening or repositioning of the breasts.
Fat necrosis
Infrequently small areas of underlying fat in the breast lose blood supply and undergo fat necrosis (death).
The occurrence of this is unpredictable. Areas of fat necrosis may present as infection, fluid filled cysts, or areas of hard tissue (lumps). The lumps may calcify and cause confusion with breast cancer.
Further surgery will be required.
Delayed healing
Some areas of the breast skin or nipple region may not heal normally and may take a long time to heal. Delays to wound healing may relate to sutures under the
skin, tension at the inverted T-‐junction, infection, and smoking
Smokers have a greater risk of skin loss and wound healing complications. Areas of wound breakdown can take up to 6 weeks to heal. Regular dressings during this
time will be required. Surgery in the future may be required to improve the scarring.
Risks common to all operations Discomfort and pain
The severity and duration of post-‐operative pain varies with each individual. Mild to moderate discomfort or pain is normal after any
surgery and can be expected after mastopexy.
If the pain becomes severe and is not relieved by pain medication you may have a complication. In this case you should contact your
surgeon.
Nausea and vomiting Nausea and vomiting typically relate to the anaesthetic and usually settles quickly. In some cases persisting nausea and vomiting may relate to pain relieving
medication or other medications like antibiotics. Infection may also cause nausea and vomiting.
If nausea and vomiting persist you may develop dehydration. You should contact your surgeon if nausea and vomiting persist.
Swelling and bruising
Moderate swelling and bruising are normal after any surgery and can be expected after mastopexy. Severe swelling and bruising may indicate bleeding or possible
infection. Discolouration from bruising may take several weeks to resolve.
Swelling and bruising are expected to settle faster by wearing a tight fitting bra or garment and with application of arnica ointment to the breast skin for the first 4
weeks following the operation.
Intermittent swelling after mastopexy may persist for several months after surgery.
Bleeding and haematoma
Bleeding is always possible after any operation. Some bleeding will result in bruising. Continued bleeding may result in continuous
ooze from the suture line or from the drain holes sites or may result in a collection of blood under the skin.
You should notify your surgeon if bleeding after surgery persists.
Small collections of blood under the skin usually absorb spontaneously. A large collection of blood (haematoma) may produce
pressure and complications to healing of the skin.
Most haematomas occur in the first 24 hours and may require aspiration or surgical drainage in an operating room and a general anaesthetic to drain the
accumulated blood.
The presence of a haematoma, even if evacuated, may predispose to infection and antibiotics are often recommended.
Infrequently haemorrhage can happen 7 to10 days following mastopexy. Possible factors for late bleeding include infection, extreme physical exertion, aspirin
ingestion or an un-‐recognized bleeding disorder.
Aspirin, anti-‐ inflammatory tablets and mega doses of certain vitamins (vitamin E) can influence blood clotting and cause excessive bleeding. It is recommended
that you do not take any aspirin, similar drugs like cartia, astrix or non-‐steroidal anti-‐inflammatory medications for ten days before surgery, as this contributes to a
greater risk of bleeding, bruising, swelling and infection. A single tablet is enough to increase the risk of bleeding.
If you take an anticoagulant like heparin or warfarin, you will need to discuss these medications with your surgeon prior to your mastopexy surgery.
Hypertension (high blood pressure) that is not under good medical control may also cause bleeding during or after surgery.
Seroma
Yellow fluid (seroma) may accumulate in the breast if augmentation with a breast implant is performed together with the mastopexy. A seroma following this

surgery may relate to trauma or vigorous exercise, especially in the first month following surgery.
The accumulated fluid will cause swelling and pain in the breast.
While the body absorbs small seromas with rest, larger ones need needle drainage or additional surgery to drain the fluid from around the breast implant in the
breast.
A seroma may contribute to infection.
Inflammation and infection
Infection may occur after any surgery.
Most infections occur within 3 to 5 days after surgery and may cause swelling, redness and tenderness in the skin around the suture
lines. A surface infection may only require antibiotic ointment.
Occasionally an offensive discharge may occur from the suture line. Deeper infections will require treatment with antibiotics. Some
deep infections and development of an abscess (collection of pus) will require additional surgery under an anaesthetic to drain the
abscess and remove dead tissue in an operating room.
Infection may cause wound breakdown or skin slough (loss). Both wound breakdown and skin slough will result in delays to healing and possible increase in
scarring.
Additional surgery to deal with wound breakdown and skin slough will be required. Additional surgery may involve skin grafting. More scarring, and further surgery
can be expected in the long term.
Some surgeons will prescribe prophylactic (preventative) antibiotics to be used around the time of mastopexy surgery.
Crusting along incision lines
Crusting along suture lines should be prevented with frequent and regular washing of your suture lines with antibacterial soap
(sapoderm, gamophen) and application of antibiotic ointment or soft white paraffin if required. Careful drying of the suture lines on
the breast with a clean towel will be required to prevent moisture.
Numbness
Small sensory nerves to the skin surface are occasionally disturbed when the incision for a mastopexy is made, or interrupted by
undermining of the skin during surgery. Numbness of the skin of the breast gradually returns -‐ usually within 3 months as the nerve
endings heal spontaneously. Return of sensation may sometimes take up to 2 years and may be permanent.
Itching Itching and occasional small shooting electrical sensations within the skin frequently occur as the nerve endings heal. Ice, skin moisturisers and massages are
frequently helpful. These symptoms are common during the recovery period and may persist for several weeks after surgery.
Fat necrosis
Fat necrosis is the formation of dead fatty tissue inside the breast and occurs because of lack of blood supply to the fat in that area.
Fat necrosis may predispose to infection, seroma (when the dead fat liquifies) and may prevent prevent wound healing.
Surgery may be needed to remove areas of fat necrosis.
Unsatisfactory internal scarring may occur following necrosis.
Factors associated with increased necrosis include infection, smoking and diabetes.
Wound separation or delayed healing
Any surgical wound, during the healing phase may separate or heal unusually slowly for a number of reasons or due to complications. This can occur as a result of
inflammation, infection, wound tension, excess external pressure and decreased circulation. Some people may experience slow healing due to unrelated medical
problems. Smokers have a greater risk of skin loss and wound healing complications.
Wound separation may also occur after suture removal.
Wound separation will require frequent wound dressings and healing will be delayed. If delayed healing occurs, recovery time will be prolonged, (weeks to
months), and the final outcome of surgery may be affected. More scarring can be expected.
Further surgery may be required to remove any non-‐healed tissue and to obtain wound closure. Skin grafting may also be required to achieve wound closure.
Poor scars will result following wound healing problems and additional surgery may be desired 6 to 12 months after the initial surgery to improve scarring.
Increased risk for smokers
Smokers have a greater chance of infection, skin slough (loss), underlying fat loss (necrosis), and poor wound healing, because of
decreased skin circulation. Bleeding and haematoma formation are more common in smokers than non-‐smokers.
Smoking also predisposes to life threatening complications like deep vein thrombosis (DVT), pulmonary embolism, pneumonia or
massive infection.
It is strongly recommended that you cease smoking 4 weeks prior to and 4 weeks after your surgery.
Sensitivity or allergy to dressings and tape
Skin or localised allergies may occur to topical antiseptic solutions, suture materials, soaps, ointments, tapes or dressings used during or after surgery. Such
problems are unusual and are usually mild and easily treated. Please advise your surgeon of any skin irritation, itch, blisters or redness that may develop beneath

your dressings. Allergic reactions resolve after removal of the causative agent and may require additional treatment.
Suture complications
Suture reaction or local infection may occur when subcutaneous sutures (sutures under the skin) are used. Exposed sutures will require suture removal for local
healing to progress. Skin sutures may become buried under the skin during healing and subcutaneous sutures may not dissolve (stitch granuloma). Additional
surgery may be necessary to remove buried sutures or granulomas. Suture marks in the skin can occur if skin sutures or staples are used to close your surgical
incision.
Skin scarring
All surgical incisions produce scarring and although scars are inevitable, some are worse than others, and the quality of the final scars
is unpredictable and not entirely under the control of the surgeon. Some areas on the body scar more than other areas, and some
people scar more than others.
Scars may be worse if there is a tendency to keloid scarring, in the younger person or if there has been a delay in healing due to
infection or wound breakdown.
Your own history of scarring should give you some indication of what you can expect. Please ask your surgeon about scar management.
Red and discoloured scars
The appearance of your surgical scar will change during the various stages of wound healing. Some scars become more red and somewhat raised and excessive
between six weeks and three months.
After six months the scar may begin to fade in their colour intensity. Scars on the breast may take up to 2 years to get as good as they will get. Scars are
permanent. Scars will remain permanently visible to a lesser or greater extent, depending on the outcome.
A brown discolouration in a scar usually settles with time. White scars are permanent and there is no known satisfactory treatment. Please ask your surgeon about
scar management.
Abnormal scars
Abnormal scars may occur even though careful surgical techniques are used and uncomplicated wound healing occurs after surgery.
Scars may be unattractive because they are raised, thick (hypertrophic or keloid), stretched (wide), depressed, or of a different
colour to the surrounding skin. An abnormal scar may have visible suture marks. Abnormal scars may occur both within the skin and
the deeper tissues.
Abnormal scars occur more commonly in some skin types, in the younger patient or if there has been a delay in healing due to
infection or wound breakdown. Most scars improve with time but some may require additional treatment.
Thick scars may respond to taping, placement of silicone sheeting onto the scars, serial injection of steroid into the scars or surgical scar revision. Wide scars may
require scar revision surgery to improve their appearance. Surgical scar revision may be disappointing especially in the younger patient.
Please ask your surgeon about scar management.
Asymmetry
The human body is normally asymmetrical. Despite surgical allowance for correction, the normal variation from one side of the body to the other will be reflected
in the results obtained from your mastopexy surgery . Perfect symmetry may not be attainable after mastopexy.
Injury to deeper structures
Blood vessels, nerves and muscles may be injured during mastopexy. The incidence of such injuries is rare.
Post-‐operative fatigue and depression
It is normal for people to occasionally experience feelings of depression for a few days after surgery, especially when the early
postoperative suture line, swelling and bruising is seen. The post-‐operative emotional low improves with time. Physical recovery
from any operation and anaesthetic is gradual.
The undesirable result
The undesirable result occurs because of limitations of the human tissues and skin. On the other hand you may be disappointed with
the results of surgery if they have not met your expectations.
Your expectations may leave you dissatisfied with the results of your mastopexy, despite having an adequate surgical result. Additional surgery may or may not
improve the results of surgery.
The unfavourable result
The unfavourable result may relate to under correction, asymmetry, recurrence of the original problem or scar related problems. Additional surgery may be
required to improve your results.
Need for revisional surgery
Every surgery has associated risks and complications that you need to be aware of. Should a complication occur, additional surgery or
other treatment might become necessary.
Revisional procedures are less predictable and involve more risks. You must consider any revisional surgery carefully after discussion
with your surgeon.
The practice of medicine and surgery is not an exact science. Although good results are expected, there is no guarantee or warranty
expressed or implied, on the results that may be obtained.

If revisional surgery is required, you may incur further surgical, anaesthetic, pathology and hospital fees. These fees may be covered
if you have private health insurance, depending on your level of cover.
These fees will be your responsibility; so careful financial planning is required before you embark on any form of surgery.
Private Health Insurance is strongly advised for any surgery. Please speak to your surgeon regarding the costs of treating
complications.
Chronic pain
Following surgery, abnormal scarring in the skin and deeper tissues may trap nerves and produce pain. Uncommonly, persistent or chronic pain that is of an
unknown or ambiguous cause may develop.
This type of chronic pain may be difficult or impossible to correct.
Long-‐term effects
There are many variable conditions that may influence the long-‐term result of your mastopexy surgery. Subsequent alterations to your body contour may occur as
the result of aging, sun exposure, weight gains or weight loss, pregnancy, illness or other circumstances not related to your surgery.
Additional surgery or other treatments in some cases may be required to maintain or improve the results of your operation.
Deep Vein Thrombosis
A deep vein thrombosis is a blood clot occurring in the deep veins of the legs/calves. It causes pain and swelling in the affected leg
and is potentially life threatening.
Treatment for deep vein thrombosis is essential and involves blood-‐thinning agents. Complications of a deep venous thrombosis
include clots spreading from the legs to the lungs or heart and may cause shortness of breath, chest pain or death.
If you are undergoing surgery, the risk of deep vein thrombosis relates to the type of surgery and the duration of the procedure.
Some people are more prone to developing deep venous thrombosis than others. These people may be of advanced age or people who have had a deep vein
thrombosis in the past. Varicose veins are a risk factor as are certain medications like hormone replacement therapy and the oral contraceptive pill.
Smoking increases the risk of forming a deep vein thrombosis as well. Preventive treatment for deep vein thrombosis may be recommended and may consist of
compression stockings, early ambulation or blood thinning agents.
Your risk of DVT will be automatically calculated by this web site, and shall be presented to you later.
Anaesthetic related risks
Anaesthetic complications, although uncommon, do occur and should be discussed thoroughly with your anaesthetist prior to your
surgery.
Allergic reactions to drugs used in anaesthesia are rare (1 in 10,000).
Systemic reactions may also occur to drugs used during surgery and prescription medicines.
Allergic reactions may require additional treatment.
It is possible to get a sore throat from the tube that is used to administer anaesthesia.
You may develop a painful or infected intravenous site.
Other anaesthetic complications should be discussed with the anaesthetist.
Life threatening complications
Life threatening (or fatal, in some circumstances) complications like pulmonary embolism, cardiac arrhythmia, heart attack, stroke or massive infection are rare.
These complications will require additional treatment.
Pulmonary (lung) complications
Pulmonary complications are uncommon and may occur secondary to either a blood clot starting in the legs (pulmonary embolism), aspiration of stomach
secretions or partial collapse of the lungs after general anaesthesia.
Before Your Operation Organise yourself for after your surgery
Organise how you will get to and from hospital.
Arrange to have someone at home with you for at least 2 or 3 days after you leave hospital.
Organise help with your shopping, laundry, housework, pets, lawns, etc.
Get all your pre-‐operative tests
Arrange leave from work and any financial chores as required.
Your Health
Surgery and anaesthesia impose stress on your body.
The state of your health will be determined how well your body will cope with this stress.
It is important that you maximise your general health by exercising, not smoking and having regular checks with your GP, so that conditions such as hypertension,
diabetes etc can be controlled.

Smoking
Smoking increases the risk of post-‐operative complications after surgery. It is recommended that you stop smoking for 4 weeks prior
to your surgery and for 4 weeks after.
If you need help to give up smoking, speak to your G.P. who can prescribe medication to help you, speak your chemist who can advise
you about nicotine replacement therapies or call the national QUIT LINE on 13 18 48.
Hospital
Depending on your pain tolerance and your home situation, it may be in your best interest to stay overnight in hospital. When in hospital you may have a urinary
catheter, drains, a drip for fluid and pain relief and in some cases an epidural catheter for pain relief. Drain tubes and dressings are likely to be removed before you
are discharged from hospital.
Fasting, fluids, food
Fasting for surgery means that you cannot eat any food, or drink any fluid, after midnight the night before your surgery. A stomach
full of fluid or food will mean that your anaesthetic may be dangerous and your procedure may be delayed or cancelled.
Adults who are fasting should have nothing solid to eat, and drink no milk-‐containing fluids for 6 hours prior to an operation. You may
have up to 1 glass of water per hour up to 3 hours prior to surgery.
If you are in hospital a sign over your bed will read "fasting", "nil by mouth" or "NBM".
If you take medications in the morning, these should be taken as normal on the morning of your operation with a sip of water at 6
am.
NB. Diabetic tablets and insulin should be withheld while you are fasting. When you brush your teeth in the morning, spit out any water rather than swallowing it.
Medications
You will be required to list all your medications by writing down the name, the dose and the day each medication is taken. If this is
too difficult for you, ask your regular doctor to make a list of your current medications for you. It is important that you also bring all
your medications to hospital with you.
Continue to take all your routine medications up to the time of admission to hospital EXCEPT blood thinning tablets like
warfarin/coumadin. These medications must be stopped 5 days before surgery. You should discuss these medications with your
surgeon.
Tablets like aspirin, astrix, plavix, iscover, cardiprin, and tablets for arthritis, rheumatism and gout, like brufen, Clinoril, feldene, indocid, orudis and voltaren must
be stopped 10 days before surgery.
If you are not sure about your medications and the effect that they may have on your surgery please seek advice from your surgeon in advance of your surgery.
Other medications
Antibiotics and small doses of blood thinning agents may be prescribed prior to your surgery.
Diabetes mellitus
If you have diabetes you must tell your surgeon prior to your admission date. You must also tell the staff at the time of your
admission. Special arrangement will be made for you as necessary.
Your blood sugar levels will be monitored from the time you start fasting until normal eating resumes. Do not take any diabetic
tablets on the morning of your surgery.
Skin preparation
You may be required to shower at home with an anti-‐bacterial soap such as sapoderm or gamophen prior to your surgery. The same soap can be used after your
surgery as well.
You may be required to have a shower in hospital with an antiseptic solution before your surgery. You may have to have hair on your body shaved for your
procedure. Do not attempt to shave yourself before coming to hospital.
A responsible person
A responsible person may be required to accompany you home after surgery. A responsible person is an adult who understands the
postoperative instructions given to them and is physically and mentally able to make decisions for your welfare when appropriate.
Travel
You will need to arrange for a responsible adult to drive you after your surgery. A suitable vehicle is a car or similar. A taxi is only
acceptable if someone OTHER than the taxi driver accompanies you. Public transport such as a bus is NOT acceptable.
General exercise
It is important that you maintain your fitness and you should continue your normal activities prior to your surgery. If time permits you may try to increase your fitness level gradually. Your fitness will be of benefit to your overall recovery after surgery. Walking is an excellent way
of improving fitness and is recommended.
Pain relief in hospital
It is expected that you will have pain and discomfort after your surgery. The amount and severity of pain will vary from person to

person.
Narcotics (morphine, pethidine, fentanyl) are used to relieve pain. Narcotics are not addictive in the amounts required to relieve
pain.
You may be given a PCA (Patient controlled analgesia). A PCA allows you to regulate the amount of medication that you need to control your discomfort. This is achieved by pushing a button to administer a pre-‐
prescribed dose of narcotic through your intravenous drip.
It is important to limit the amount of discomfort that you have, so that you are able to do your breathing and general exercises as directed by your physiotherapist.
Any initial severe pain and discomfort will be managed with intravenous medication such as morphine, pethidine or fentanyl. Removal of tubes and drains usually
results in a significant reduction of pain. The PCA machine is usually replaced with pain relieving tablets before discharge from hospital.
Pain relief at home
Pain, aches and discomfort may still be present when you leave hospital and may continue for several weeks. It is important when
you are at home to maintain control over your pain, aches and discomforts.
Drugs for pain relief vary in strength and can "generally" be related to pain severity, BUT remember also that individuals have
differing responses to pain and pain relieving medications.
As a guide and for your knowledge, the range of medication by drug strength from weakest to strongest is as follows:
Mild pain relief will be required for mild pain.
Such pain relieving medication includes panadol, paracetamol, panamax and panadeine.
Moderate pain relief may require medications such as digesic, panadeine forte, tramyl, endone or oxycodone.
You need to be aware that some pain relieving medications may contribute to persisting nausea and vomiting and will contribute to constipation in the post-‐
operative period.
Anti-‐inflammatory drugs such as vioxx, celebrex, brufen, naprosyn and indocid will contribute to effective pain relief when taken with mild pain relieving tablets.
If you have persistent unrelieved pain you may need to be seen by a doctor to exclude another cause for the pain.
Constipation
If you normally take medication for bowel problems you will need to bring these medications to hospital with you. It is common to develop constipation after
surgery that may require treatment.
Prevention of constipation begins on the day of surgery and continues until the bowel returns to "normal" function, which is usually once the need for pain
medication ceases.
Medications for constipation such as coloxyl and senna or lactulose can be purchased from the local chemist without a prescription.
Eat fresh fruit and vegetables, take extra fibre and increase your exercise. Drink plenty of water, providing you are not on restricted fluids for any reason.
Other
It is important that you try to retain your identity as a normal person whilst you are in hospital. Make sure that you ask plenty of questions about what is happening
to you.
Feel free to share your concerns with the nurses, doctors and other professionals that are involved in your care.
After Your Operation On waking
You will have dressings over your breasts. Small drain tubes will come out at each side of the chest. You may be placed in a head up
position with pillows behind your head.
Discomfort
You can expect to have some discomfort when you wake up after a mastopexy. You will be placed in a position where your head is
elevated. This position helps to reduce swelling and pain in the breasts.
You will need to remember to move your legs to keep the circulation flowing and to take deep breaths to expand the lungs.
Care should be taken when moving around in bed. Rolling from side to side is preferable to lifting your body. Using our arms to lift your body may cause pain.
T.E.D. stockings
You will be fitted with TED stockings before your mastopexy surgery and you will wake from surgery with the stockings on.
TED stockings help to prevent blood clots from forming in the legs. TED stockings should be worn whilst you are immobile and you may be required to wear the
stockings for up to 2 weeks following surgery.
Garment
Your surgeon may fit you with a bra or similar garment after the dressings have been removed. The bra provides support for the breasts while they heal. The
support reduces pain and swelling of the breasts after surgery. The bra or garment should be worn day and night for about 2 weeks after surgery.
It may be removed to allow you to have a shower. Depending on the advice of your surgeon, the bra may have to be worn during the day for 4 to 6 weeks following
your operation.
For continuing support after this time comfortable supportive bras may need to still be worn for up to 3 months following surgery.

Pain relief
You will need to take painkillers as provided.
It is recommended that you avoid aspirin or aspirin based products, as they will promote bruising and bleeding.
The usual medications given in the postoperative period consist of panadol, panadeine, panadeine forte, panamax, digesic, and endone. These medications may
be combined with anti-‐inflammatory medications such as vioxx, celebrex, or brufen.
Make sure that you have a postoperative pain regime at the time of discharge and that you understand the medications that you are taking and what they are
designed to do for you.
Sleeping tablets
One or two sleeping tablets (normison, temazepam, ativan) may be taken at night, if necessary, to help with sleeping in the first few
days after surgery.
Other medications
Your surgeon may prescribe a course of prophylactic (preventative) antibiotics.
Nausea and vomiting
Nausea and vomiting may be due to the anaesthetic or post-‐operative medication (like pain killers or antibiotics).
Apart from being unpleasant, vomiting will cause pain in the breasts.
Medication to prevent nausea and vomiting may be required. If prolonged, nausea and vomiting may be related to a complication like infection and may cause dehydration. You need to inform your surgeon of prolonged
nausea and vomiting.
Bruising Bruising of the body (breasts, upper abdomen) after mastopexy surgery is usually maximal at approximately 48 hours after surgery. Most bruises will resolve by 2
weeks. Gentle massage with a moisturising lotion (sorbolene), or arnica cream may help to dissipate bruising.
Bleeding or ooze
There may be ooze of blood from any of the suture lines or from the drain tube holes. Any ooze should resolve within 24 to 48 hours.
Persistent or offensive ooze should be reported to your surgeon.
Swelling
Swelling can occur for 4 to 6 weeks after mastopexy and sometimes, intermittent swelling may take up to 12 months to settle.
Please ask your surgeon how long swelling should take to resolve. Swelling lasting longer than this time may be due to a
complication, and should be reported to your surgeon.
Ice packs
At home a mouldable cold pack or a small bag of frozen peas wrapped in a tea towel may help to reduce swelling, bruising, and pain.
Cold packs can be applied to the breasts (for 20 minutes every 1 to 2 hours) in the first 48 hours after surgery to help minimise
swelling and bruising. The cold packs should not hurt.
If cold packs are uncomfortable, don't use them as often. After a few days gentle daily massage with a bland moisturising cream after your shower will help to resolve bruising and any
lumpiness.
Dressings and Drains
Dressings and drains following mastopexy may be removed as early as 24 to 48 hours after your surgery. If there is a lot of drainage,
then the drains will remain for longer. Please ask your surgeon how long the dressings need to stay on. Steri-‐strips or tapes may be
present on the suture line and will need to be changed regularly.
Check with your surgeon if you are able to shower.
Sutures
Sutures may be beneath the skin and will absorb with time. The aim of absorbable sutures beneath the skin is to provide wound support for a longer time than skin sutures, so that scar stretch
can be minimised.
Occasionally the body will want to extrude these sutures. A sore or a pimple on the suture line may indicate an underlying suture
trying to break through the skin. This suture can be removed as soon as it breaks through the skin. Antibiotic ointment or betadeine
may be required along with a small dressing until the area heals. Infrequently a lump forms related to a suture that has not dissolved
(a stitch granuloma). This stitch granuloma may need to be excised as a local anaesthetic procedure.
Sutures or staples may be present in the skin. These sutures or staples will require removal at some stage after your surgery. The normal time frame is anywhere
between 7 days to 10 days depending on the surgery and the location on the breast. Suture removal is usually arranged with the surgeon.
Some surgeons place Steri-‐strips over the suture line. Steri-‐strips are meant to stay intact and are usually removed one week after surgery.
You may be able to shower.

Blistering from Steri-‐strips may occur.
If this happens the Steri-‐strips will be removed and an alternative dressing will be applied.
Cleaning
Having a shower and getting your sutures wet may be permitted by your surgeon after the dressings (and drains) have been
removed. An antibacterial soap (sapoderm, gamophen) may be recommended.
You will need to pay attention to washing the suture line. Suture lines should be carefully dried with a clean towel.
If your suture line has steri-‐strips or tape, wash over the tape and dry it.
Occasionally the suture line may become red and ooze. If this occurs tapes are usually removed and antibiotic ointment or betadeine
may be required. Your surgeon may prescribe antibiotics as well.
Some surgeons will prefer you to keep your sutures dry. Please check with your surgeon and ensure you follow your surgeon's
instructions about wound care.
Travel
A mastopexy is performed under general anaesthesia and can be performed as day surgery.
If you are going home after day surgery a family member or friend must drive you because you have had an anaesthetic and someone
should stay overnight with you for the same reason. You may need help from a relative or friend at home during the first few days
after your mastopexy.
If you have any questions about these matters, please speak to your surgeon.
Anaesthetic effects
The effects of an anaesthetic may still be present 24 hours after your mastopexy, even if you do not feel them. Your reflexes will be slower and you are at risk of
injury. It is illegal to drive while under the influence of a drug (even a prescribed one) and you could be charged.
Do not make important decisions or sign legal documents for 24 hours after an anaesthetic. Take care with alcohol intake after surgery because medications and
alcohol may interact with the residual anaesthetic. Discuss your normal medications with the anaesthetist.
Readmission to hospital
Rarely you may need to be re-‐admitted unexpectedly to hospital. The most common cause is persistent nausea and vomiting, anxiety, the need for unexpected
additional pain relief or for treatment of unexpected complications of surgery such as bleeding, wound problems or infection.
Activity
Too much activity too soon will risk delays in healing or increase the risk of complications. Try to walk slowly at first. Sleeping head up
and with pillows behind your head should continue for two weeks after surgery. Try to avoid any straining or rushing around.
You may go to the bathroom, walk around the house sit and watch TV, etc., but no matter how good you feel do not clean the house,
engage in heavy manual work, go to the gym etc. for 4 weeks following your surgery. This also applies to sexual activity.
Sport
Slow walking on the flat for exercise is often therapeutic in the early post-‐operative period. Your body will dictate whether you are
able to safely recommence your exercise program. More strenuous exercise like fast walking, running or swimming may commence
after 4 to 6 weeks.
More strenuous exercise like tennis or contact sports can commence after 6 to 8 weeks. As a general rule: if it hurts, don't do it.
Please ask your surgeon when you can start exercising.
Localised sore areas in the breasts are not uncommon.
Sun exposure
If fresh scars are exposed to the sun, they will tend to become darker and take longer to fade. Sunscreen on sun-‐exposed scars can
help to fade scars. Take extra care and precautions if you are planning to tan, as some areas of your body may be temporarily numb
after surgery and you will not "feel" a sunburn developing.
Diet
Your post-‐operative diet should consist of fluids initially then soft food that is easy to prepare. If you have any postoperative nausea,
carbonated sodas and dry crackers may settle the stomach. Small frequent meals will be more suitable and comfortable.
Vitamins
Although not proven, there is some suggestion that multivitamins prior to and after surgery may aid in wound healing. Avoid mega
dosing on vitamins prior to surgery.
Smoking
Smoking reduces capillary blood flow to the skin and may result in delays to wound healing or complications of your mastopexy. Smoking not only affects wound
healing; it also increases the risk of bleeding, wound infections, post-‐operative chest infections. Any coughing may disrupt the muscle repair. Smoking also
increases the risk of developing a blood clot in the legs that can travel to the lungs. It is recommended that you cease smoking at least 4 weeks prior to your
surgery and for 4 weeks after.
Alcohol

Medications and alcohol may interact with the residual anaesthetic and prescription pain medicine.
Alcohol also dilates blood vessels and may increase the risk of postoperative bleeding.
It is recommended that you avoid alcohol for the first three days after surgery and restrict your alcohol intake for the first month.
Driving
It is recommended that you do not drive for a certain period of time after a mastopexy. To be able to drive safely you must have full
use of your reflexes to drive, and any post-‐operative discomfort will inhibit your reflexes.
If pain will inhibit them, don't drive. In the interest of safety whilst driving, and legally, you must wear a seat belt across the chest.
You may resume driving when you feel you are able, but it is advisable to discuss this with your surgeon or check with the road traffic
authority first.
Recovery time
You must allow yourself adequate recovery time. You will have restriction to mobility for up to 2 weeks. Too much activity too soon will increase the risk of
complications such as seroma (if implants are present), bleeding, infection and delayed healing. It would be wise to ensure you have adequate time off work. You
must also allow sufficient time for your body to recover from the effects of anaesthesia and surgery.
Discuss the expected time for recovery with your surgeon prior to your surgery and allow plenty of time for adequate recovery.
Healing
Everyone heals at a different rate. The ability to heal is variable and depends upon a number of factors such as your genetic background, your weight, your overall
state of health and lifestyle (exercise, diet, smoking, drinking, etc.). Your attention to preparing yourself for surgery will be manifest in your post-‐operative
recovery. Many people believe the surgeon "heals" the patient. Not one person can make another heal. Your cooperation and close attention to pre and post-‐
operative instructions is extremely important and is in your best interest.
Following instructions
A major factor in the course of healing is whether you follow the instructions given by your surgeon and the nurses in the surgery.
Such guidelines are designed to promote the healing process and to prevent the occurrence of anything that may interfere with your recovery. It is imperative that you recognise that you are a partner in this process and have a responsibility to follow instructions carefully. The instructions, based on broad experience, are designed to give you the best opportunity for healing without delay or surprise.
Depression
Depression is a normal reaction to surgery. The third day following your surgery may be the worst. You may be teary.
It is not uncommon to experience a brief period of "let-‐down" or depression after any surgery.
You may subconsciously have expected to look and feel better "instantly," even though you rationally understood that this would not
be the case.
Day 3 post surgery may be the worst.
As healing occurs, these thoughts usually disappear quickly.
If you feel depressed, understanding that this is a "natural" phase of the healing process may help you to cope with this emotional state.
Support from family and friends Support from family and friends can be very helpful, but because they may not understand what constitutes a normal postoperative course, their comments may
unintentionally create emotional turmoil for you.
The staff at the surgery and your surgeon will tell you honestly how you are doing and what to expect.
Please trust in your surgeon's knowledge and experience when your progress is discussed with you.
Complications
Complications are infrequent. When complications occur, it is seldom a consequence of poor surgery or poor postoperative care. Complications are more likely to
be a result of the variable healing capacity or a failure to follow post-‐operative instructions. You will be assisted in every way possible if a complication occurs.
Should the unexpected occur, please understand that it is important to follow the advice of your surgeon and nursing staff in order to treat it as effectively as
possible. Your surgeon and the nursing staff will ensure that you have support and assistance during this difficult time.
Appointments
It is very important that you follow the schedule of appointments established for you after surgery. Appointments to see the nurse
or the surgeon should be made before or immediately after discharge from hospital. The review appointment may be the next day
or up to one week following surgery.
If no appointment has been made, you must ensure that you contact your surgeon and make a follow up appointment. If you have
any concerns don't feel that you are bothering the surgeon or the staff.
If need be, you can be seen prior to any arranged review appointment to sort out any concerns.

Revisional Surgery
Occasionally the result of your surgery may not be totally perfect. If you feel that you can focus on the overall degree of
improvement instead of any small lack of perfection, then you will reap the benefits of the results of your operation. If small
imperfections will prevent you focusing on the degree of improvement after your surgery you probably should not have had an
operation.
Your surgeon will use their expertise and experience in their surgical techniques to achieve the best results and ensure their patients
receive the most advanced surgical techniques available. They keep updated by attending, national and international aesthetic
conferences and seminars regularly.
The surgery performed may not necessarily relate to the methods that are sometimes promoted, or advertised in popular
magazines, newspaper articles or on television.
The rate of revisional surgery, even in the most skilled surgical hands, can never be zero because patient and surgeon can control only some aspects of the
outcome.
Minor adjustments or additional revisions following cosmetic surgery may be necessary in up to 5% of patients. Revisional surgery is performed after the first postoperative year (12 months after surgery) because resolution of swelling and stabilisation of the final
appearance takes at least that long.
During the first year after surgery irregularities, asymmetries or poor contours may sufficiently improve without surgery, so very small imperfections following
surgery should not be revised.
Revisional procedures are less predictable and involve more risks. You must consider any revisional surgery carefully after discussion with your surgeon.
If revisional surgery is required you may incur further surgical, anaesthetic, pathology and hospital fees. These fees may be covered if you have private health
insurance, depending on your level of cover. These fees will be your responsibility and you will need careful financial planning you before you embark on any form
of cosmetic surgery. Private Health Insurance is strongly advised for any cosmetic surgery.