Embed Size (px)
Citation preview
European Journal of Obstetrics & Gynecology and Reproductive Biology, 29 (1988) 215-279
Elsevier
ET0 00681
Breast-feeding following spontaneous and induced labour
J.J. Out *, M.E. Vierhout 2 and H.C.S. Wallenburg 2 ’ Departments of Medical Psychology and Psychotherapy and ’ Obstetrics and Gynecology,
Erasmu University Medical School, Rotterdam, The Netherlank
Accepted for publication 24 May 1988
275
Summary
Carrying out the intention to breast-feed was assessed in 185 mothers divided into four groups according to whether labour was spontaneous, with or without oxytocin augmentation, or induced, either by their own choice or on the advice of their obstetrician. Intention to breast-feed was abandoned most frequently by women in whom labour had been electively induced. As the difference with the other groups could not be explained by obstetric factors, it is concluded that motivational factors may have played a part.
Breastfeeding; Elective induction of labour
Introduction
Nasal administration of oxytocin has been shown to enhance human lactation [lo] but it is not known whether oxytocin has a stimulating effect on breast-feeding when it is used to induce labour. In view of the half-life in plasma of less than 15 min [5], a direct biochemical effect seems unlikely.
Cartwright [2] and Yudkin et al. [12] found no differences between the relative frequency of breast-feeding following induction of labour as compared to sponta- neous onset of labour. On the other hand, Ounsted et al. [7] found that women carried out their intention to breast-feed more often after spontaneous labour than after labour induced for obstetric reasons with oxytocin (38%) or prostaglandin E, (62%). These authors offer two putative explanations: (1) infants born to women who had had a difficult delivery or Caesarean section were often given their first
Correspondence: J.J. Out, Department of Medical Psychology and Psychotherapy, Erasmus University
Medical School, P.O. Box 1738, 3000 DR Rotterdam, The Netherlands.
0028-2243/88/$03.50 0 1988 Elsevier Science Publishers B.V. (Biomedical Division)
276
feeds from a bottle in order to allow the mother to rest; this occurred more often in mothers with induced labour; (2) the same endocrine factors could be involved in the chain of events leading to spontaneous onset of labour and to initiation of lactation‘; for that reason success in establishing breast-feeding may be less easy for mothers after induced labour.
In a study on the elective induction of labour described previously [g-9,11], psychological differences were demonstrated to exist between women choosing induction of labour and women opting for a spontaneous onset. Women in the first group appeared to put less trust in their reproductive functions and to be less educated than women in the second group. The relative frequency of breast-feeding was highest in women who delivered after spontaneous onset of labour. The present study was based on the patient population selected for the previously published investigation on elective induction of labour [8,9] and designed to assess differences in relative frequencies of breast-feeding between women with induced and women with spontaneous onset of labour.
Patients and methods
Patients For the previously reported study on elective induction of labour [8,9] 383
women attending the antenatal clinic of the University Hospital Dijkzigt, Rotter- dam, were selected in the 36th week of gestation. Only healthy women with a Dutch cultural background and an uncomplicated pregnancy with a fetus in cephalic position were enrolled in the study. Twenty-six women who met the criteria of an uncomplicated pregnancy in the 36th week were excluded because of the occurrence of obstetric complications in the final weeks of pregnancy. Of the remaining 357 women, 185 women stated their intention to breast-feed in a questionnaire that was completed in the 36th week of pregnancy. According to the actual mode of labour, these 185 women were divided into four groups: 1. Women whose labour was induced according to their wishes (elective induction
of labour, 29 women). 2. Women who had their labour induced because their obstetrician advised them to
do so in view of minor pregnancy-related complaints, although no genuine obstetric reasons were present (advised induction of labour, 20 women).
3. Women with spontaneous onset of labour in whom uterine activity was aug- mented with oxytocin infusion (augmented labour, 31 women).
4. Women with spontaneous onset of labour without oxytocin-augmented uterine activity (spontaneous labour, 105 women).
Methods
In women with elective or advised induction cervical ripeness was assessed with the use of the BURNHILL score [l]. When the cervix was considered ‘ripe’ - a score greater than four - the date for induction of labour was set. At the time of induction the membranes were artificially ruptured, and a fluid-filled open-tip catheter was introduced transcervically into the amniotic cavity for the recording of
277
uterine activity. An electrode was attached to the fetal scalp for fetal heart-rate monitoring. Uterine contractions were induced with intravenous infusion of an
incremental dose of oxytocin starting with 2 mU/min, until uterine activity of 150-200 Montevideo units was obtained. In women with clinically insufficient
uterine contractions, labour was augmented with intravenous infusion of an incre-
mental dose of oxytocin. Information about breast-feeding was obtained from the nursing staff and
confirmed in an interview with the women 3 to 4 days after delivery. Carrying
through an intention to breast-feed was defined as having actually started to
breast-feed; any serious attempt was included. Information about the duration of breast-feeding was obtained from a questionnaire mailed 6 months after delivery and returned by 92% of the women. Differences in outcome between groups were
statistically evaluated with the Chi-square method or with Haberman’s analysis of
adjusted residuals if more than two groups were compared (an adjusted residual of
+ 1.96 is significant at a 0.05 level [3,6]). A value of p < 0.05 was always chosen as
the level of significance.
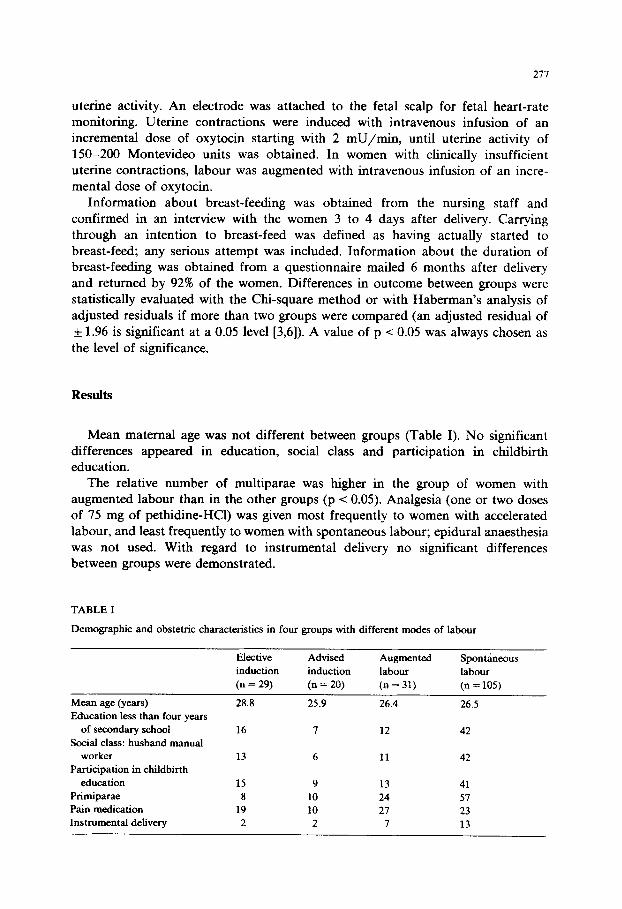
Mean maternal age was not different between groups (Table I). No significant differences appeared in education, social class and participation in childbirth education.
The relative number of multiparae was higher in the group of women with augmented labour than in the other groups (p < 0.05). Analgesia (one or two doses of 75 mg of pethidine-HCl) was given most frequently to women with accelerated
labour, and least frequently to women with spontaneous labour; epidural anaesthesia was not used. With regard to instrumental delivery no significant differences between groups were demonstrated.
TABLE I
Demographic and obstetric characteristics in four groups with different modes of labour
Mean (years) age Education less than four years
of secondary school Social class: husband manual
worker Participation in childbirth
education
Primiparae Pain medication
Instrumental delivery
Elective Advised
induction induction
(n = 29) (n = 20)
28.8 25.9
16 7
13 6
15 9
8 10 19 10
2 2
Augmented Spontaneous labour labour (n = 31) (n = 105)
26.4 26.5
12 42
11 42
13 41 24 51 27 23
7 13
278
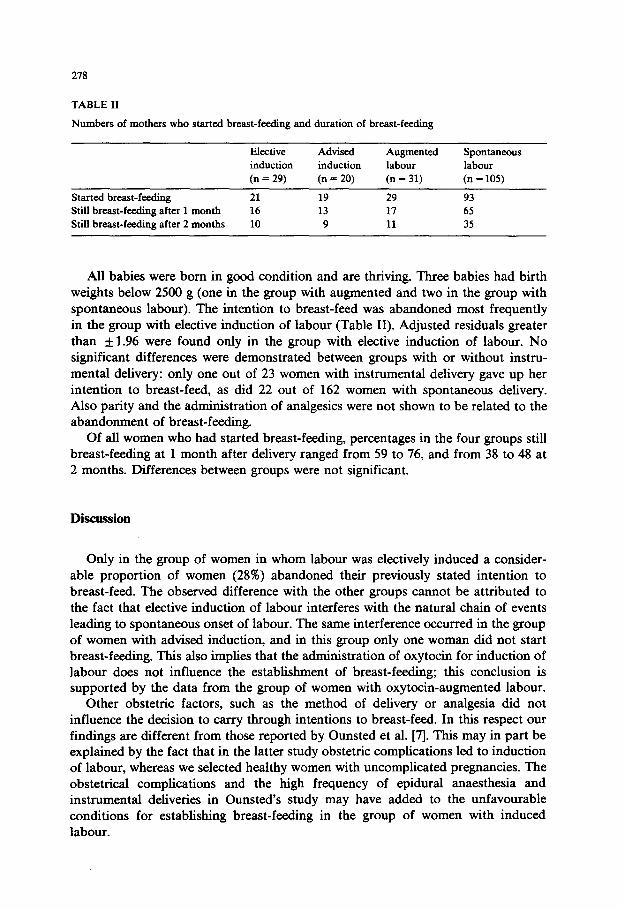
TABLE II
Numbers of mothers who started breast-feeding and duration of breast-feeding
Elective Advised induction induction
(n = 29) (n = 20)
Augmented labour
(n = 31)
Spontaneous
labour
(n = 105)
Started breast-feeding 21 19 29 93
Still breast-feeding after 1 month 16 13 17 65
Still breast-feeding after 2 months 10 9 11 35
All babies were born in good condition and are thriving. Three babies had birth weights below 2500 g (one in the group with augmented and two in the group with spontaneous labour). The intention to breast-feed was abandoned most frequently in the group with elective induction of labour (Table II). Adjusted residuals greater than f 1.96 were found only in the group with elective induction of labour. No significant differences were demonstrated between groups with or without instru- mental delivery: only one out of 23 women with instrumental delivery gave up her intention to breast-feed, as did 22 out of 162 women with spontaneous delivery. Also parity and the administration of analgesics were not shown to be related to the abandonment of breast-feeding.
Of all women who had started breast-feeding, percentages in the four groups still breast-feeding at 1 month after delivery ranged from 59 to 76, and from 38 to 48 at 2 months. Differences between groups were not significant.
Discussion
Only in the group of women in whom labour was electively induced a consider- able proportion of women (28%) abandoned their previously stated intention to breast-feed. The observed difference with the other groups cannot be attributed to the fact that elective induction of labour interferes with the natural chain of events leading to spontaneous onset of labour. The same interference occurred in the group of women with advised induction, and in this group only one woman did not start breast-feeding. This also implies that the administration of oxytocin for induction of labour does not influence the establishment of breast-feeding; this conclusion is supported by the data from the group of women with oxytocin-augmented labour.
Other obstetric factors, such as the method of delivery or analgesia did not influence the decision to carry through intentions to breast-feed. In this respect our findings are different from those reported by Ounsted et al. [7]. This may in part be explained by the fact that in the latter study obstetric complications led to induction of labour, whereas we selected healthy women with uncomplicated pregnancies. The obstetrical complications and the high frequency of epidural anaesthesia and instrumental deliveries in Ounsted’s study may have added to the unfavourable conditions for establishing breast-feeding in the group of women with induced labour.
279
In more favourable conditions, as they occurred in our study, personality characteristics and attitudes seem more important to explain differences in frequency of breast-feeding. Women who ask for elective induction of labour appear to put less trust in their reproductive functions [9] than women who await the spontaneous onset of labour. Once women have opted for assistance to start their labour, not
relying upon nature, they may also easily abandon their previously stated preference for a natural mode of feeding their baby.
In view of the unmistakeable advantage of breast-feeding in most circumstances
[4], women considering elective induction of their labour should be counselled with
regard to this possible course of events if they have an intention to breast-feed.
References
1 BurnhiB MS, Danezis J, Cohen J. Uterine contractility during labor studied by intra-amniotic fluid
pressure recordings. Am J Obstet Gynecol 1962;83:561-571.
2 Cartwright A. The dignity of labour? A study of childbearing and induction. London: Tavistock
Publications, 1979.
3 Everitt BS. The analysis of contingency tables. London: Chapman and Hall, 1977.
4 Garfield E. Breast is best. Part 1. Merits of mother’s milk. Curr Content Clin Pratt 1986;14 (No.
20):3-12.
5 Goodman L. Gilman A, eds. The pharmacological basis of therapeutics (5th cdn). New York:
MacMillan, 1975.
6. Haberman SJ. The analysis of residuals in cross-classified tables. Biometrics 1977;29:205-220.
7 Ounsted MK, Hendrick AM, Mutch LMM, Calder AA, Good FJ. Induction of labour by different
methods in primiparous women. I. Some perinatal and postnatal problems. Early Hum Dev
1978;2:227-239.
8 Out JJ, Vierhout ME, Verhage F, Duivenvoorden HJ, Wallenburg HCS. Elective induction of labor: a
prospective clinical study. II: Psychological effects. J. Perinat Med 1985;13:163-170.
9 Out JJ, Vierhout ME, Verhage F, Duivenvoorden HJ, Wallenburg HCS. Characteristics and motives
of women choosing elective induction of labour. J Psychosom Res 1986;30:375-380.
10 Ruis H, Rolland R, Doesburg W, Broeders G, Corbey R. Oxytocin enhances onset of lactation among
mothers delivering prematurely. Br Med J 1981;283:340-342.
11 Vierhout ME, Out JJ, Wallenburg HCS. Elective induction of labor: a prospective clinical study. I:
Obstetric and neonatal effects. J Perinat Med 1985;13:155-162.
12 Yudkin P, Frumar AM, Anderson ABM, Tumbull AC. A retrospective study of induction of labour.
Br J Obstet Gynaecol 1979;86:257-265.












![Breast Feeding Guidelines[1]](https://img.pdfslide.us/doc/110x75/577d371d1a28ab3a6b94d9ec/breast-feeding-guidelines1.jpg)