Embed Size (px)
Citation preview

Breast Cancer:
Weight and Exercise
Anne McTiernan, MD, PhD
Fred Hutchinson Cancer Research Center
Seattle, WA

Associations of Obesity with
Overall & Breast Cancer Specific
Survival

Survival Obese vs. Non-obese Breast Cancer Patients by Hormone
Receptor
Niraula et al. BCRT
2012;134:769-81

Survival Obese vs. Non-obese Breast Cancer Patients
by Menopausal Status
Niraula et al. BCRT 2012;134:769-81

Breast Cancer Specific Survival Obese vs. Non-obese Breast
Cancer Patients by Hormone Receptor
Niraula et al. BCRT 2012;134:769-81

Breast Cancer Specific Survival Obese vs. Non-obese Breast
Cancer Patients by Menopausal Status
Niraula et al. BCRT 2012;134:769-81

BMI & Recurrence: Non-inflammatory Locally
Advanced and Inflammatory: MD Anderson (N=602)
Dawood S et al. Clin Cancer Res 2008;14:1718-1725
©2008 by American Association for Cancer Research

Obesity & Treatments

Obesity in N0, ER+ Breast Cancer:
Tamoxifen Efficacy

Copyright © American Society of Clinical Oncology
Litton, J. K. et al. J Clin Oncol; 26:4072-4077 2008
Survival by BMI: Neoadjuvant Breast Cancer Patients MD Anderson Series

de Azambuja et al. Br Ca Res Treat 2009
BMI in node-positive breast cancer
patients treated with docetaxel and
doxorubicin-containing adjuvant
chemotherapy: BIG 02-98 trial,
N=2,887
A: overall survival
B: disease-free survival

Overweight/obese by Treatment (tamoxifen, anastrozole) & Survival:
ABCSG-12 Trial (n=1803 Premenopausal Patients)
Pfeiler G et al. JCO 2011;29:2653-2659
©2011 by American Society of Clinical Oncology

ATAC Trial Anastrozole vs Tamoxifen by BMI: All & Distant Recurrences
Sestak I et al. JCO 2010;28:3411-3415
©2010 by American Society of Clinical Oncology

Weight Change after Diagnosis and
Breast Cancer Prognosis
• 4/8 studies: significant decreased survival/ increased recurrence with weight gain
• Nurses Health Study, n=5204, followed ~ 9 years, risk or death for BMI gain in non-smokers: – 0.5 -2.0 kg/m2: 1.35
– > 2.0 kg/m2: 1.64
• LACE cohort, stage 1-3, n=1689, followed ~ 7 years – Weight loss > 10%: 2.5 x increased risk of death in ER-
/PR- patients
Chlebowski, Aiello, McTiernan JCO 2002;20(4):1128-1143
Kroenke et al. J. Clin Onc 2005;23(7):1370-8.
Caan B et al. Ca Causes Cont 2008:19:1319–1328

Other Potential Adverse Effects of
Obesity in Breast Cancer
• Wound complications
• Lymphedema
• Radiation therapy challenges?
• Endometrial cancer in tamoxifen users
• Congestive heart failure in patients treated with doxorubicin
• Increased risk for coronary disease, diabetes, stroke, hypertension, osteoarthritis, several cancers, decreased quality of life

Weight & Prognosis: Summary
• Overweight/obese/underweight ↓ prognosis
• Weight gain after diagnosis ↔
• Purposeful weight loss after diagnosis ???

Weight & Prognosis: Summary
• Associations seen in: – Pre-menopausal
– Postmenopausal
– All stages
– Hormone receptor positive & negative
– Varied treatments including surgery, chemotherapy, hormonal agents
– Population & clinical trial cohorts
Chlebowski, Aiello, McTiernan JCO 2002;20(4):1128-1143
Niraula et al. BCRT 2012;134:769-81

Potential Mechanisms of Obesity-
Prognosis Link
• Estrogens, androgens
• Hyper-insulinemia, insulin resistance,
diabetes, pre-diabetes
• Inflammatory markers
• Diet/physical activity
• Inadequate chemotherapy dosing

Chemotherapy Dosing:
ASCO Guidelines • Up to 40% of obese patients receive limited
chemotherapy doses that are not based on
actual body weight.
• Full weight–based cytotoxic chemotherapy
doses should be used to treat obese patients
with cancer.
• No evidence that short or long-term toxicity
is increased among obese patients receiving
full weight–based doses.
Griggs et al. JCO 2012; 30(13):1553-61

HEAL Cohort
• 1183 newly diagnosed breast cancer patients
• 3 centers: FHCRC, New Mexico, Los Angeles
• Population-based (registries)
• Multi-ethnic
• Followed for ~ 10 years post-diagnosis
• Assessing effect on prognosis of:
– weight, physical activity, metabolic hormones, inflammation, sex hormones, nutrition, vitamin D

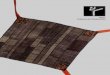
Risk of Breast Cancer Death by C-peptide
(HEAL, 571 stage I-IIIa patients,
followed up mean 4.1 years)
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
C-peptide
Ha
za
rd
Ra
tio
< 1.7 ng/mL
1.7-2.5 ng/mL
> 2.5 ng/mL
Diabetics
P trend = 0.03
Irwin et al. J Clin Oncol 2011; 29(1):47-53

• 512 early stage breast cancer
• no known diabetes
Fasting Glucose and Breast Cancer Outcomes
Quartile DDFS OS
Mean Range HR
(adjusted)*
(95% CI) HR
(adjusted)*
(95% CI)
4.5 3.5-4.7 1 1
4.9
5.2
5.7
4.7-5.1
5.1-5.4
5.4-11.6
1.28
1.50
1.88
(1.02-1.60)
(1.04-2.17)
(1.06-3.35)
1.26
1.46
1.81
(0.93-1.70)
(0.89-2.40)
(0.83-3.93)
p=0.027 unadjusted
p=0.034 adjusted
p=0.036 unadjusted
p=0.014 adjusted
* adjusted for age, T, N, grade, hormone receptor, chemotherapy, hormone
therapy
Goodwin PJ et al. J Clin Oncol 2012
Results:
Population:

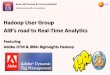
Risk of Death by C-Reactive Protein (HEAL, 734
stage I-IIIa patients, followed up mean 3.8 years)
0
0.5
1
1.5
2
2.5
Met-hr/wk
Ha
za
rd
Ra
tio
< 1.2 mg/L
1.3-3.8 mg/L
> 3.9 mg/L
Pierce et al. J Clin Oncol 2009; 27(21):3437-44.
P trend =0.01

HEAL Study Weight Change (kg) in 2 Years
after Diagnosis, by Stage
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
Stage
in situ
Stage I
Stage II-IIIa
Irwin, M. L. et al. J Clin Oncol; 23:774-782 2005
P=0.004

Low-Fat Diet and Breast Cancer
Prognosis: the WINS Study
• Clinical trial
• 2,437 women with early stage breast cancer
• Recruited from 37 U.S. sites
• 48-79 years old
• Randomly assigned to low-fat diet or control
group
• 6 lb. greater weight loss at 12 mos. in intervention
vs. control women
• Followed for up to 5 years
• Risk of death was significantly reduced by 24
percent in diet patients vs. controls

High Vegetable/Lower Fat Diet:
the WHEL Study
• Multi-site clinical trial
• 3088 women with early stage breast cancer
• 18-70 years old
• Randomly assigned to high vegetable/fruit/fiber,
low-fat diet or control group
• Followed for a mean 7.3 years
• Little change in diet vs. control diets
• No effect of diet on prognosis
Pierce et al. JAMA. 2007 Jul 18;298(3):289-98.

Alcohol & Breast Cancer Prognosis
• Recent findings suggest alcohol use (> 1 drink/d)
associated with:
– Increased recurrence
– Increased contralateral/2nd primary breast cancer
• Moderate alcohol use may be associated with
reduced mortality
Li et al. JCO 2009;27:5312-5318.
Kwan et al. JCO 2010;28(29):4410-6.
Barnett et al. JCO 2008; 26:3310-6.

Physical Activity
& Breast Cancer Survival
Ballard-Barbash R, et al. JNCI Jun 6;104(11):815-40

Exercise Effects in Breast Cancer Survivors
• Aerobic exercise:
– Improves fitness, mood, overall quality of life
– Reduces weight (moderately) and fatigue
– Increases lean mass
• Resistance (strength) training:
– Decreases lymphedema episodes & symptoms
– Increases strength
• Combined aerobic + resistance:
– Decreases arthralgia in aromatase inhibitor users
Galvao et al. JCO 2005;23:899-909 (review).
Schmitz K et al. N Engl J Med 2009;361:664-73.
Courneya et al. JNCI 2013 Dec 4;105(23):1821-32.
Irwin ML et al. JCO (in press)

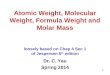
Total Physical Activity Before and After
Diagnosis in Breast Cancer Survivors by
Treatment (HEAL)
1515.5
16
16.517
17.518
18.5
1919.5
20
Surgery Surgery +
Radiation
Surgery +
Chemo
Treatment
Hou
rs/w
eek
Before Diagnosis
After Diagnosis
P<.05
P<.05
Irwin M. et al. Cancer 2003;97:1746-57

Treatments Available for Conditions
(None FDA Approved for Breast Cancer)
• Reduce/treat obesity:
– Reduced calorie diet
– Physical activity
– Weight loss therapies (extreme obesity or co-morbidities)
• Xenical/Alli (orlistat, blocks fat absorption – prescription & OTC)
• Qsymia (topiramate, an anti-convulsant & phentermine, an appetite
suppressant)
• Belviq (lorcaserin hydrochloride, activates serotonin 2C receptor)
• Bariatric surgery
• Note: all for adding to diet & exercise weight loss program
• Medications to treat obesity mediators:
– Excess insulin (Metformin - NCIC trial ongoing)
– Inflammation (Statins, NSAIDS)

Implementing Lifestyle Change
• Reduced calorie (~ 1200-1800 kcal/day)
• Increased physical activity (>150 minutes/week moderate intensity)
• Strength training does not increase lymphedema (progress slowly)
• Weekly meetings with counselor
• Self-monitoring:
– Daily diet logs – all foods and drinks
– Weighing at least weekly
– Daily exercise logs - recreational/walking activity
• Goal 7%-10% weight loss in 6 months
• Studies in breast cancer survivors show lower weight loss than in persons without cancer

Conclusions: Clinical Guidelines • During chemo/radiation:
– Avoid weight gain unless underweight
– Exercise as tolerated: start slowly, increase slowly
• After or no chemo/radiation:
– Lose weight if BMI > 25.0 through calorie reduction +
increased physical activity
– Aerobic exercise at least 30 min/day, 5 days/wk
– Gradually increase to moderate intensity (e.g. brisk
walking, biking, fast dancing)
• Long-term survivors: weight loss may lower
adverse prognosis biomarkers
• Keep alcohol to 1 drink/day or less