Embed Size (px)
Citation preview
REVIEW
Breast cancer experience and survivorship among AsianAmericans: a systematic review
Kuang-Yi Wen & Carolyn Y. Fang & Grace X. Ma
Received: 2 June 2013 /Accepted: 11 October 2013 /Published online: 9 November 2013# Springer Science+Business Media New York 2013
AbstractIntroduction Breast cancer is the most common cancer inAsian American women, and the number of Asian Americanbreast cancer survivors is rapidly increasing. Although AsianAmericans are one of the fastest growing and mostheterogeneous ethnic groups in the United States, limited dataexist in regard to their breast cancer experience and survivorship.Methods A systematic review of the breast cancer experienceliterature was conducted and included studies of AsianAmericans or their subgroups as a major category of studyparticipants. Of the 125 studies reviewed, 10 qualitativestudies, 10 quantitative studies, 5 studies that used a mixed-method approach, and 1 intervention study met the criteria forinclusion.Results Qualitatively, Asian Americans reported unmet physicaland emotional needs and challenges during survivorship.Quantitative studies consistently found that socioeconomicstatus, cultural health beliefs, immigration stress, acculturationlevel, English proficiency, social support, and spiritualityassociated with Asian American breast cancer patients' healthbehaviors and health-related quality of life (HRQOL). Studiesalso revealed significant variation in breast cancer reaction andHRQOL within Asian American subgroups.Conclusions Although research on Asian American breastcancer experience and survivorship is sparse, we concludedthat Asian Americans experience disrupted HRQOL followingbreast cancer diagnosis and treatment, interwoven with their
cultural and socio-ecological system, and that programsfocused on improving cancer survivorship outcomes amongthis ethnic minority group are limited. Most studies haveconcentrated on the West coast population, and there issignificant underrepresentation of longitudinal and interventionstudies. Implications for study design, measurement, and futureresearch areas are also included.Implications for Cancer Survivors The results highlight a needto understand ethnic differences and to take into account social,cultural, and linguistic factors in breast cancer survivorshipexperiences among Asian American subgroups as a means todevelop culturally relevant and linguistically appropriateinterventions designed to improve HRQOL.
Keywords Survivorship . Breast cancer . Asian Americans .
Literature review
Introduction
Breast cancer is the most common form of cancer amongwomen of all racial and ethnic groups and the second leadingcause of cancer death in the United States [1]. Although theincidence rate of breast cancer has been declining among otherUS populations, the incidence rates are increasing dramaticallyfor specific Asian American subgroups [2, 3]. Despiteadvances in the early diagnosis and treatment of breast cancerand increasing numbers of Asian American breast cancersurvivors [4], fewer studies have focused on the breast cancerexperience of Asian American as compared to Caucasian andAfrican American women [5, 6]. This gap in knowledge isattributed to challenges in overcoming language barriers,differences in socio-cultural backgrounds, a lack of availableresources, and stereotypes about positive health profiles in theAsian American community, all of which contribute to cancerhealth disparities in the Asian American population [7–9].
K.<Y. Wen (*) : C. Y. FangCancer Prevention and Control Program, Fox ChaseCancer Center, 333 Cottman Avenue, Robert C. Young Pavilion,Philadelphia, PA 19111, USAe-mail: [email protected]
G. X. MaDepartment of Public Health, Center for Asian Health,Temple University, Philadelphia, PA 19122, USA
J Cancer Surviv (2014) 8:94–107DOI 10.1007/s11764-013-0320-8

Breast cancer demands significant physical and mentaladjustment and disrupts patients' quality of life [10]. Thediagnosis andmanagement of breast cancer might be especiallychallenging for Asian Americans in light of their culturallyspecific beliefs about cancer, limited access to linguisticallyappropriate medical services, a low level of acculturation, andeconomic difficulties [11, 12]. Because Asian Americans areone of the fastest growing and most heterogeneous ethnicgroups in the USA, and because Asian Americans have a largepresence among first-generation immigrants and underservedgroups with low literacy and limited medical care access, it isimportant to understand the breast cancer experiences andoutcomes of breast cancer survivors among this group.
Health-related quality of life (HRQOL) is a commonly usedframework to evaluate the impact of cancer and its treatment oncancer survivorship. Ashing-Giwa's Contextual Model ofHRQOL provides a structure that expands the traditionalHRQOL framework by including cultural and socio-ecologicaldimensions [13]. Guided by the Contextual Model of HRQOL,we aimed primarily to review the research conducted to date andto identify knowledge gaps in the current Asian American breastcancer survivorship literature. The Contextual Model has eightdimensions: four individual-level dimensions and four system-level dimensions. The individual-level contextual dimensionsconsist of individual-level factors and perceptions in regard tothe experience of cancer survivorship, including physical,emotional, and medical-related factors, as well as health practiceand medical adherence. The system-level dimensions includeselected contextual factors external to the individual that aredemonstrated to impact on the survivorship experience,including demographic and socio-ecological variables (i.e.,socio-economic status and social support), cultural variables(i.e., language, acculturation, health belief, and spirituality), andhealth care system variables (i.e., health care access andcommunication and satisfaction with provider). The ContextualModel of HRQOLwas used as a framework for summarizing thefindings of this review. Attention was focused on AsianAmerican ethnic subgroups that may account for differences intheir responses to breast cancer. Given the paucity of research onthis population, we searched for intervention studies in additionto qualitative and quantitative studies. Future research areas anddirection are discussed in the context of the review findings.
Methods
Data sources and search
We conducted a systematic review of the English languageliterature to locate studies that described the breast cancerpatient's experiences, reported HRQOL outcomes, or evaluatedthe interventions in terms of their potential to improve thesurvivorship experience for Asian American women in the
USA. According to the US Census, the term “Asian” refers topeople having origins in any of the countries from the Far East,Southeast Asia, or the Indian subcontinent. In addition tonationalities, Asian groups also include ethnic terms. Inidentifying studies of Asian Americans with breast cancer forthis review, we included both immigrants from Asian countriesto the USA and Americans of Asian descent. Four searchengines, PubMed, Google Scholar, PsychoInfo, and Web ofScience, were searched to identify literature published betweenJanuary 1995 and February 2013. We used a search strategythat combined the terms of each of the three concepts relevantto our research objective, such as Concept One: breast cancerexperience, breast cancer management, or breast cancersurvivorship; Concept Two: Asian, Chinese, Korean,Japanese, Vietnamese, Filipino, Cambodian, Malaysian,Pakistan, Thai, or Indian; and Concept Three: qualitativeinterview, quantitative survey, or intervention. Referencesections of relevant review articles and included studies alsowere scanned to identify additional eligible studies.Dissertations, book chapters, and conference abstracts wereexcluded.
Study selection and data extraction
Title and abstracts were reviewed by the first author todetermine the eligibility for inclusion in this review. Inclusioncriteria for articles were (1) qualitative or quantitative researchstudy that examined the needs, experience, or HRQOL-relatedfactors or research on an intervention to improve patientoutcomes; (2) provided data on Asian Americans or AsianAmerican subgroup breast cancer survivors, from newlydiagnosed up to unlimited years post-diagnosis; (3) researchconducted in the USA.
Of the 125 studies that were identified and reviewed, 26studies met our criteria. Studies were coded by the first authoron 13 predefined categories previously employed in a reviewstudy on HRQOL in Hispanic breast cancer survivors [14].The second author reviewed all 26 studies and correspondingcoding. Disagreements were resolved by consensus orreference to the third author.
Results
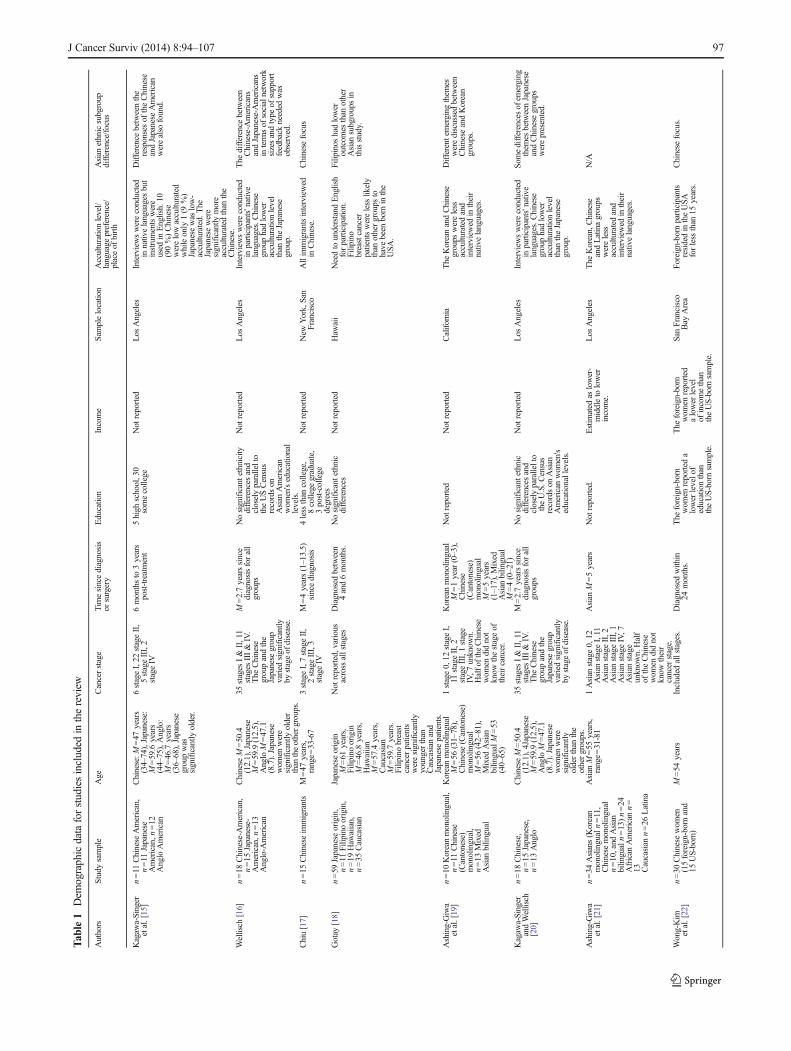
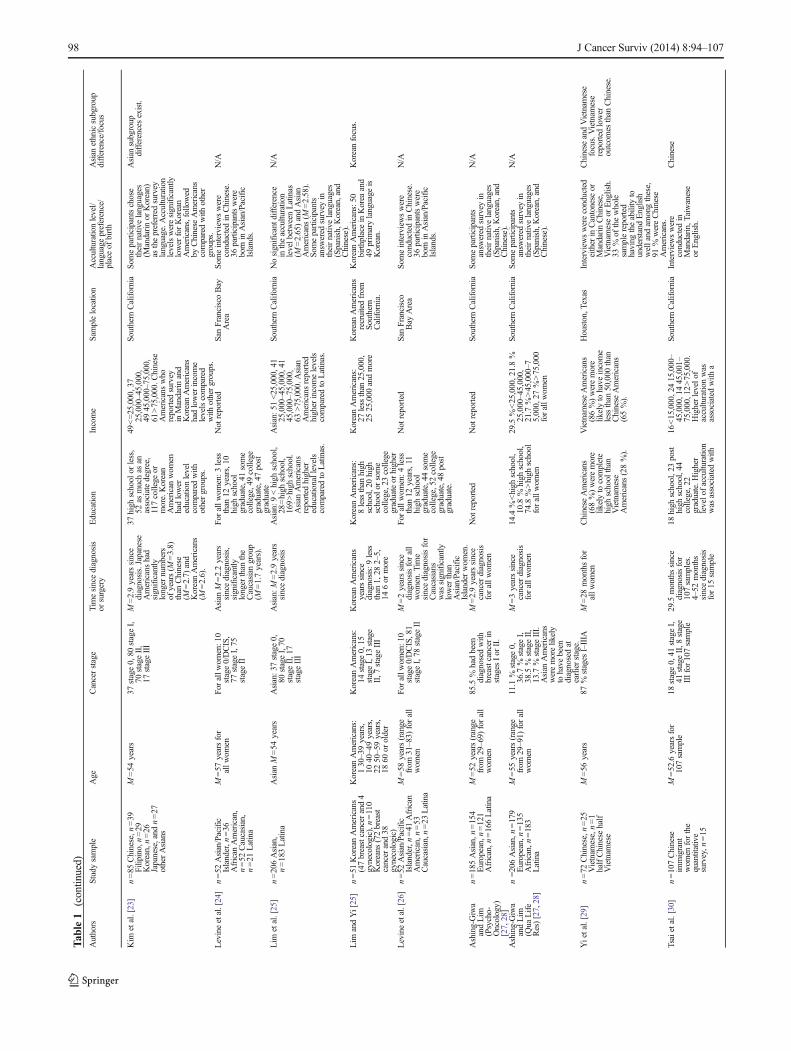
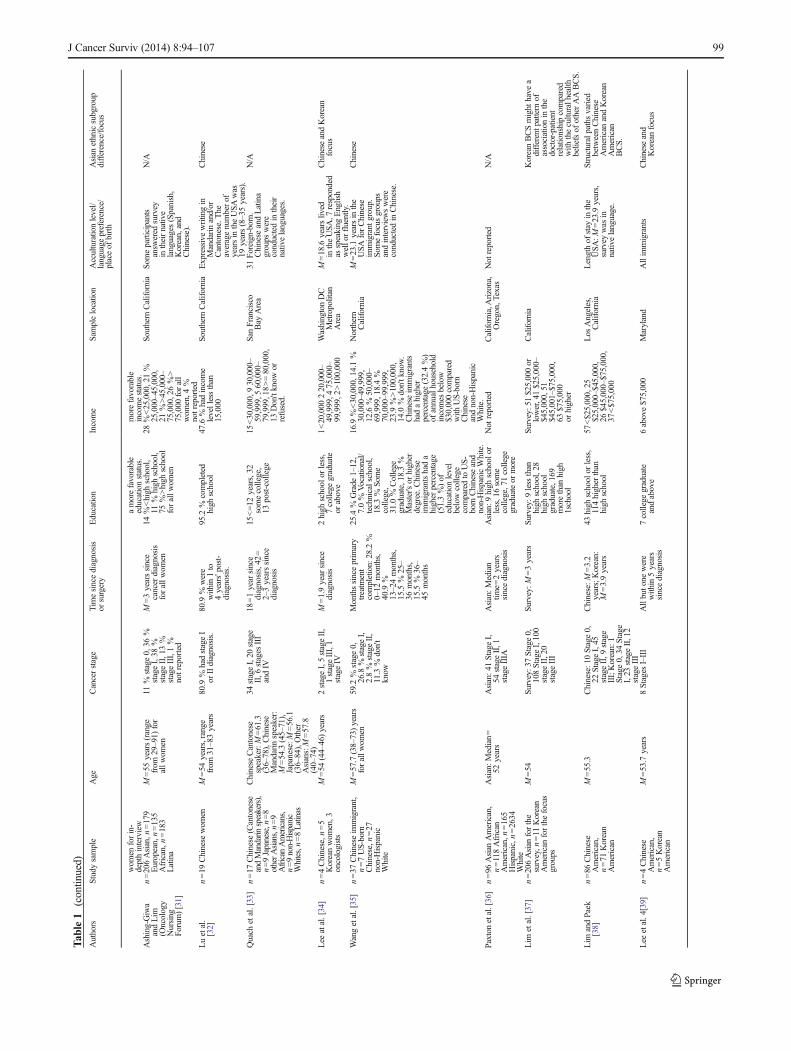
For socio-demographic and cancer-related descriptive data oneach study's sample, see Table 1 and for information onresearch design and a summary of findings, see Table 2. The26 identified studies included 10 qualitative studies, 10quantitative cross-sectional studies, 5 mixed-method studiesthat used both qualitative and quantitative approaches, and 1intervention pilot study. Of all the studies, 16 reported theirfindings from 5 identical or overlapping samples. A total of 14studies included multi-ethnic samples as a means to explore
J Cancer Surviv (2014) 8:94–107 95

differences among Asian American and Asian Americansubgroup, Caucasian, African, and Hispanic survivors.However, we discuss only Asian American-specific resultsin this review, including 12 studies focused exclusively onAsian Americans or Asian American subgroups. The majorityof the studies (n =22) were exclusively conducted with orincluded participants from California. The sample sizes ofAsian American participants in the 10 qualitative studiesranged from 9 to 70 women with two studies focusedexclusively on the Chinese population. Among the 10quantitative studies, the sample size of the Asian Americanpopulation ranged from 47 to 206, with one study focusedexclusively on the Korean population. The sample size forAsian Americans among the 5 mixed-method studies rangedfrom 22 to 206 (n =206 was only for the quantitative part ofLim et al.'s study [37]), with one study focused exclusively onthe Chinese population. The only intervention study identifiedin this review was a pilot study of an expressive writingintervention among Chinese American breast cancer survivors(n =19) [32]. Among the 26 studies, most women had early-stage breast cancer, and their diagnosis duration varied, withsome newly diagnosed samples (<1 year) and some longer-term survivors (>4 years). A total of 18 studies allowedparticipants to complete the study in their native languages.Six studies assessed and reported acculturation levels amongparticipants.
Results are organized by the Contextual Model of HRQOL'sindividual-level and system-level dimensions. We reviewedqualitative and quantitative findings within each dimension.Any comparisons between Asian Americans and other ethnicgroups were documented within each dimension. To take intoaccount the diversity and heterogeneity among Asian Americansubgroups, an additional section, “Differences among AsianAmerican subgroups”, was included. Intervention andlongitudinal studies were summarized in an individual sectionas well.
Individual-level dimensions
Physical health
Fatigue, irritability, memory loss, decreased energy level,recurring pain, and decreased QOL were reported as sideeffects of breast cancer treatment by Asian American women[21]. Wang et al. reported that Chinese American women,including both immigrants and US-born Chinese, experiencedpain and side effects from radiation, surgery, and hormonaltherapy [35]. In particular, Chinese immigrant women wereless likely to have their physical issues resolved, as comparedto Caucasians and US-born Chinese, due to their culturalnorms [35]. Among a Chinese and Vietnamese sample,94 % reported experiencing symptoms with high prevalenceof severe intensity [29]. In terms of physical QOL, one study
conducted in Hawaii reported that Filipino women have worseoutcomes in terms of nausea/vomiting and symptom countthan do Japanese, Hawaiian, and Caucasian women [18].However, compared with Hispanics in another study, AsianAmerican women expressed fewer physical difficulties causedby breast cancer treatments [25].
Emotional health
The findings related to emotional health included anxiety,distress, fear of recurrence, and mental/emotional healthQOL. Asian American women reported their sadness andreluctance to recall their breast cancer experience, theiranxiety during exams, and their fear of cancer recurrenceand death [21]. Another qualitative study that examinedHRQOL after treatment among Chinese and CaucasianAmericans found that women's emotional concerns aboutrecurrence or metastasis were caused by physical distress[35]. Through an interview approach, Lee et al. found thatChinese and Korean American women reported that negativeemotions are barriers that impede good HRQOL [39].Emotional well-being was found to be directly associated withphysical QOL in a cross-sectional quantitative study thatincluded Asian American women [27]. In addition, AsianAmerican women reported similar levels of depressivesymptoms and had the same levels of rehabilitation problemsfollowing treatment as did the Caucasian women [15].
Ashing-Giwa and Lim reported that worry about theconditions getting worse or cancer recurrence as well asunhappiness or lack of peacefulness were reported as the mostbothersome concerns across all ethnic breast cancer survivorsin their study, including Asian Americans [31]. Among amulti-ethnic sample, Filipino women had significantly loweremotional functioning than did Caucasian, Japanese, orHawaiian women [18]. However, compared with Hispanics,Asian American women expressed less emotional distress[25]. Similarly, another quantitative study reported that,compared to Caucasians and African Americans, AsianAmericans showed the second-lowest level of emotionalwell-being, while Hispanic women exhibited the lowest level[28]. Although there were documented deficiencies in theiremotional outcomes, Asian American breast cancer survivorssought psychosocial services at a significantly lower rate thandid Caucasians [15, 16] and exhibited greater difficulty inseeking emotional help from family, friends, and healthprofessionals [27].
Cancer-specific medical factors
No study was identified that examined the effect of medicalfactors such as disease characteristics and treatment types onAsian American breast cancer survivor's experiences orHRQOL. It was found, however, that Asian American women
96 J Cancer Surviv (2014) 8:94–107
Tab
le1
Dem
ographicdataforstudiesincluded
inthereview
Authors
Study
sample
Age
Cancerstage
Tim
esincediagnosis
orsurgery
Education
Income
Sam
plelocation
Acculturationlevel/
language
preference/
placeof
birth
Asian
ethnicsubgroup
difference/focus
Kagaw
a-Singer
etal.[15]
n=11
Chinese
American,
n=11
Japanese
American,n
=12
Anglo
American
Chinese:M
=47
years
(34–74),Japanese:
M=59.6
years
(44–75),Anglo:
M=46.7
years
(36–68),Japanese
groupwas
significantly
older.
6stageI,22
stageII,
5stageIII,2
stageIV
6monthsto
3years
post-treatment
5high
school,30
somecollege
Not
reported
Los
Angeles
Interviewswereconducted
innativelanguagesbut
instrumentswere
used
inEnglish.10
(90%)Chinese
werelowacculturated
whileonly
1(9
%)
Japanese
was
low-
acculturated.The
Japanese
were
significantly
more
acculturatedthan
the
Chinese.
Differencebetweenthe
responsesof
theChinese
andJapanese
American
werealso
found.
Wellisch
[16]
n=18
Chinese-A
merican,
n=15
Japanese-
American,n
=13
Anglo-A
merican
Chinese
M=50.4
(12.1),Japanese
M=59.9(12.5),
Anglo
M=47.1
(8.7).Japanese
wom
enwere
significantly
older
than
theothergroups.
35stages
I&
II,11
stages
III&
IV.
The
Chinese
groupandthe
Japanese
group
varied
significantly
bystageof
disease.
M=2.7yearssince
diagnosisforall
groups
Nosignificantethnicity
differencesand
closelyparallelto
theUSCensus
recordson
Asian
American
wom
en'seducational
levels.
Not
reported
Los
Angeles
Interviewswereconducted
inparticipants'native
languages.Chinese
grouphadlower
acculturationlevel
than
theJapanese
group.
The
difference
between
Chinese-Americans
andJapanese-A
mericans
interm
sof
socialnetwork
sizesandtype
ofsupport
feedback
needed
was
observed.
Chiu[17]
n=15
Chinese
immigrants
M=47
years,
range=
33-67
3stageI,7stageII,
2stageIII,3
stageIV
M=4years(1–13.5)
sincediagnosis
4less
than
college,
8college
graduate,
3post-college
degrees
Not
reported
New
York,San
Francisco
Allim
migrantsinterviewed
inChinese.
Chinese
focus
Gotay
[18]
n=59
Japanese
origin,
n=11
Filipinoorigin,
n=19
Haw
aiian,
n=35
Caucasian
Japanese
origin
M=61
years,
Filipinoorigin
M=46.8
years,
Haw
aiian
M=57.4
years,
Caucasian
M=59.7
years.
Filipinobreast
cancerpatients
weresignificantly
youngerthan
Caucasian
and
Japanese
patients.
Not
reported,various
across
allstages
Diagnosed
between
4and6months.
Nosignificantethnic
differences
Not
reported
Haw
aii
Needto
understand
English
forparticipation.
Filipino
breastcancer
patientswereless
likely
than
othergroups
tohave
been
born
inthe
USA
.
Filipinos
hadlower
outcom
esthan
other
Asian
subgroupsin
thisstudy.
Ashing-Giwa
etal.[19]
n=10
Koreanmonolingual,
n=11
Chinese
(Cantonese)
monolingual,
n=13
Mixed
Asian
bilingual
Koreanmonolingual
M=56
(31–78),
Chinese
(Cantonese)
monolingual
M=56
(42 –81),
Mixed
Asian
bilingualM=53
(40–65)
1stage0,12
stageI,
11stageII,2
stageIII,1stage
IV,7
unknow
n.Halfo
fthe
Chinese
wom
endidnot
know
thestageof
theircancer.
Koreanmonolingual
M=1year(0–3),
Chinese
(Cantonese)
monolingual
M=5years
(1–17),M
ixed
Asian
bilingual
M=4(0–21)
Not
reported
Not
reported
California
The
KoreanandChinese
groups
wereless
acculturatedand
interviewed
intheir
nativelanguages.
Different
emerging
them
eswerediscussedbetween
Chinese
andKorean
groups.
Kagaw
a-Singer
andWellisch
[20]
n=18
Chinese,
n=15
Japanese,
n=13
Anglo
Chinese
M=50.4
(12.1),4Japanese
M=59.9(12.5),
Anglo
M=47.1
(8.7).Japanese
wom
enwere
significantly
olderthan
the
othergroups.
35stages
I&
II,11
stages
III&
IV.
The
Chinese
groupandthe
Japanese
group
varied
significantly
bystageof
disease.
M=2.7yearssince
diagnosisforall
groups
Nosignificantethnic
differencesand
closelyparallelto
theU.S.C
ensus
recordson
Asian
American
wom
en's
educationallevels.
Not
reported
Los
Angeles
Interviewswereconducted
inparticipants'native
languages.Chinese
grouphadlower
acculturationlevel
than
theJapanese
group.
Som
edifferencesof
emerging
them
esbetweenJapanese
andChinese
groups
werepresented.
Ashing-Giwa
etal.[21]
n=34
Asians(K
orean
monolingualn=11,
Chinese
monolingual
n=10,and
Asian
bilingualn=13)n=24
African
American
n=
13 Caucasian
n=26
Latina
Asian
M=55
years,
range=
31-81
1Asian
stage0,12
Asian
stageI,11
Asian
stageII,2
Asian
stageIII,1
Asian
stageIV,7
Asian
stage
unknow
n.Half
oftheChinese
wom
endidnot
know
their
cancerstage.
Asian
M=5years
Not
reported.
Estim
ated
aslower-
middleto
lower
income.
Los
Angeles
The
Korean,Chinese
andLatinagroups
wereless
acculturatedand
interviewed
intheir
nativelanguages.
N/A
Wong-Kim
etal.[22]
n=30
Chinese
wom
en(15foreign-born
and
15US-born)
M=54
years
Included
allstages.
Diagnosed
within
24months.
The
foreign-born
wom
enreported
alowerlevelo
feducationthan
theUS-born
sample.
The
foreign-born
wom
enreported
alowerlevel
ofincomethan
theUS-bornsample.
SanFrancisco
Bay
Area
Foreign-born
participants
residedin
theUSA
forless
than
15years.
Chinese
focus.
J Cancer Surviv (2014) 8:94–107 97
Tab
le1
(contin
ued)
Authors
Study
sample
Age
Cancerstage
Tim
esincediagnosis
orsurgery
Education
Income
Sam
plelocation
Acculturationlevel/
language
preference/
placeof
birth
Asian
ethnicsubgroup
difference/focus
Kim
etal.[23]
n=85
Chinese,n
=39
Filipino,n
=29
Korean,n=26
Japanese,and
n=27
otherAsians
M=54
years
37stage0,80
stageI,
70stageII,
17stageIII
M=2.9yearssince
diagnosis.Japanese
Americanshad
significantly
longernumbers
ofyears(M
=3.8)
than
Chinese
(M=2.7)
and
KoreanAmericans
(M=2.6).
37high
school
orless,
52as
muchas
anassociatedegree,
117college
ormore.Korean
American
wom
enhadlower
educationlevel
comparedwith
othergroups.
49<=25,000,37
25,000–45,000,
4945,000–75,000,
61>75,000.C
hinese
Americanswho
reported
survey
inMandarinand
KoreanAmericans
hadlowerincome
levelscompared
with
othergroups.
Southern
California
Someparticipantschose
theirnativelanguages
(Mandarinor
Korean)
asthepreferredsurvey
language.A
cculturation
levelsweresignificantly
lowerforKorean
Americans,followed
byChinese
Americans
comparedwith
other
groups.
Asian
subgroup
differencesexist.
Levineetal.[24]
n=52
Asian/Pacific
Islander,n
=36
African
American,
n=52
Caucasian,
n=21
Latina
M=57
yearsfor
allw
omen
Forallw
omen:1
0stage0/DCIS,
77stageI,75
stageII
Asian
M=2.2years
sincediagnosis,
significantly
longerthan
the
Caucasian
group
(M=1.7years).
Forallw
omen:3
less
than
12years,10
high
school
graduate,41some
college,49college
graduate,47post
graduate
Not
reported
SanFranciscoBay
Area
Someinterviewswere
conductedin
Chinese.
36participantswere
born
inAsian/Pacific
Islands.
N/A
Lim
etal.[25]
n=206Asian,
n=183Latina
Asian
M=54
years
Asian:3
7stage0,
80stageI,70
stageII,17
stageIII
Asian:M
=2.9years
sincediagnosis
Asian:9
<high
school,
28=high
school,
169>high
school.
Asian
Americans
reported
higher
educationallevels
comparedto
Latinas.
Asian:5
1<25,000,41
25,000–45,000,41
45,000–75,000,
63>75,000.A
sian
Americansreported
higherincomelevels
comparedto
Latinas.
Southern
California
Nosignificantd
ifference
intheacculturation
levelb
etweenLatinas
(M=2.65)andAsian
Americans(M
=2.58).
Som
eparticipants
answ
ered
survey
intheirnativelanguages
(Spanish,K
orean,and
Chinese).
N/A
Lim
andYi[25]
n=51
KoreanAmericans
(47breastcancerand4
gynecologic),n
=110
Koreans
(72breast
cancerand38
gynecologic)
KoreanAmericans:
130–39years,
1040–49years,
2250–59years,
1860
orolder
KoreanAmericans:
14stage0,15
stageI,13
stage
II,7
stageIII
KoreanAmericans
yearssince
diagnosis:9less
than
1,28
2–5,
146or
more
KoreanAmericans:
8lessthan
high
school,20high
school
orsome
college,23college
graduateor
higher
KoreanAmericans:
27less
than
25,000,
2525,000
andmore
KoreanAmericans
recruitedfrom
Southern
California.
KoreanAmericans:50
birthplace
inKorea
and
49prim
arylanguage
isKorean.
Koreanfocus.
Levineetal.[26]
n=52
Asian/Pacific
Islander,n
=41
African
American,n
=53
Caucasian,n
=23
Latina
M=58
years(range
from
31–83)
forall
wom
en
Forallw
omen:1
0stage0/DCIS,81
stageI,78
stageII
M=2yearssince
diagnosisforall
wom
en.T
ime
sincediagnosisfor
Caucasians
was
significantly
lowerthan
Asian/Pacific
Islanderwom
en.
Forallw
omen:4
less
than
12years,11
high
school
graduate,44some
college,52college
graduate,48post
graduate.
Not
reported
SanFrancisco
Bay
Area
Someinterviewswere
conductedin
Chinese.
36participantswere
born
inAsian/Pacific
Islands.
N/A
Ashing-Giwa
andLim
(Psycho-
Oncology)
[27,28]
n=185Asian,n
=154
European,n=121
African,n
=166Latina
M=52
years(range
from
29–69)
forall
wom
en
85.5
%hadbeen
diagnosedwith
breastcancerin
stages
Ior
II.
M=2.9yearssince
cancerdiagnosis
forallw
omen
Not
reported
Not
reported
Southern
California
Someparticipants
answ
ered
survey
intheirnativelanguages
(Spanish,K
orean,and
Chinese).
N/A
Ashing-Giwa
andLim
(Qua
Life
Res)[27,28]
n=206Asian,n
=179
European,n=135
African,n
=183
Latina
M=55
years(range
from
29–91)
forall
wom
en
11.1
%stage0,
36.7
%stageI,
38.5
%stageII,
13.7
%stageIII.
Asian
Americans
weremorelikely
tohave
been
diagnosedat
earlierstage.
M=3yearssince
cancerdiagnosis
forallw
omen
14.4
%<high
school,
10.8
%high
school,
74.8
%>high
school
forallw
omen
29.5
%<25,000,21.8%
25,000–45,000,
21.7
%>45,000–7
5,000,27
%>75,000
forallw
omen
Southern
California
Someparticipants
answ
ered
survey
intheirnativelanguages
(Spanish,K
orean,and
Chinese).
N/A
Yietal.[29]
n=72
Chinese,n
=25
Vietnam
ese,n=1
halfChinese
half
Vietnam
ese
M=56
years
87%
stages
I–IIIA
M=28
monthsfor
allw
omen
Chinese
Americans
(68%)weremore
likelyto
complete
high
school
than
Vietnam
ese
Americans(28%).
Vietnam
eseAmericans
(86%)weremore
likelyto
have
income
less
than
50,000
than
Chinese
Americans
(65%).
Houston,T
exas
Interviewswereconducted
eitherin
Cantonese
orMandarinChinese,
Vietnam
eseor
English.
33%
ofthewhole
samplereported
having
theability
tounderstand
English
welland
amongthese,
91%
wereChinese
Americans.
Chinese
andVietnam
ese
focus.Vietnam
ese
reported
lower
outcom
esthan
Chinese.
Tsaietal.[30]
n=107Chinese
immigrant
wom
enforthe
quantitative
survey,n
=15
M=52.6
yearsfor
107sample
18stage0,41
stageI,
41stageII,8
stage
IIIfor107sample
29.5
monthssince
diagnosisfor
107samples.
4–52
months
sincediagnosis
for15
sample
18high
school,23post
high
school,44
college,22
graduate.H
igher
levelo
facculturation
was
associated
with
16<15,000,2415,000–
45,000,1445,001–
75,000,12>75,000.
Higherlevelo
facculturationwas
associated
with
a
Southern
California
Interviewswere
conductedin
Mandarin,Taiwanese
orEnglish.
Chinese
98 J Cancer Surviv (2014) 8:94–107
Tab
le1
(contin
ued)
Authors
Study
sample
Age
Cancerstage
Tim
esincediagnosis
orsurgery
Education
Income
Sam
plelocation
Acculturationlevel/
language
preference/
placeof
birth
Asian
ethnicsubgroup
difference/focus
wom
enforin-
depthinterview
amorefavorable
educationstatus.
morefavorable
incomestatus.
Ashing-Giwa
andLim
(Oncology
Nursing
Forum)[31]
n=206Asian,n
=179
European,n=135
African,n
=183
Latina
M=55
years(range
from
29–91)
for
allw
omen
11%
stage0,36
%stageI,38
%stageII,13%
stageIII,1%
notreported
M=3yearssince
cancerdiagnosis
forallw
omen
14%<high
school,
11%
high
school,
75%>high
school
forallw
omen
28%<25,000,21%
25,000–45,000,
21%>45,000–
75,000,26%>
75,000
forall
wom
en,4
%notreported
Southern
California
Someparticipants
answ
ered
survey
intheirnative
languages(Spanish,
Korean,and
Chinese).
N/A
Luetal.
[32]
n=19
Chinese
wom
enM=54
years,range
from
31–83years
80.9
%hadstageI
orIIdiagnosis.
80.9
%were
within
1to
4years'post-
diagnosis.
95.2
%completed
high
school
47.6
%hadincome
levellessthan
15,000
Southern
California
Expressivewritingin
Mandarinand/or
Cantonese.T
heaveragenumberof
yearsin
theUSA
was
19years(8–35years).
Chinese
Quach
etal.[33]
n=17
Chinese
(Cantonese
andMandarin
speakers),
n=9Japanese,n
=8
otherAsians,n=9
African
Americans,
n=9non-Hispanic
Whites,n=8Latinas
Chinese
Cantonese
speaker:M=61.3
(36–78),Chinese
Mandarinspeaker:
M=54.3(45–71),
Japanese:M
=56.1
(36–84),Other
Asians:M=57.8
(40–74)
34stageI,20
stage
II,6
stages
III
andIV
18=1yearsince
diagnosis,42
=2–3yearssince
diagnosis
15<=12
years,32
somecollege,
13post-college
15<30,000,9
30,000–
59,999,5
60,000–
79,999,18>=80,000,
13Don'tknow
orrefused.
SanFrancisco
Bay
Area
31Foreign-born.
Chinese
andLatina
groups
were
conductedin
their
nativelanguages.
N/A
Lee
atal.[34]
n=4Chinese,n
=5
Koreanwom
en,3
oncologists
M=54
(44–46)years
2stageI,5stageII,
1stageIII,1
stageIV
M=1.9yearsince
diagnosis
2high
school
orless,
7college
graduate
orabove
1<20,000
220,000–
49,999,4
75,000–
99,999,2
>100,000
WashingtonDC
Metropolitan
Area
M=18.6
yearslived
intheUSA
,7responded
asspeaking
English
wello
rfluently.
Chinese
andKorean
focus
Wangetal.[35]
n=37
Chinese
immigrant,
n=7US-born
Chinese,n
=27
non-Hispanic
White
M=57.7(38–73)years
forallw
omen
59.2
%stage0,
26.8
%stageI,
2.8%
stageII,
11.3
%don't
know
Monthssinceprim
ary
treatm
ent
completion:
28.2
%0–12
months,
40.9
%13–24months,
15.5
%25–
36months,
15.5
%36–
45months
25.4
%Grade
1–12,
7.0%
Vocational/
technicalschool,
18.3
%So
me
college,
31.0
%College
graduate,18.3%
Master's
orhigher
degree.C
hinese
immigrantshada
higherpercentage
(51.3%)of
educationlevel
belowcollege
comparedto
US-
born
Chinese
and
non-HispanicWhite.
16.9
%<30,000,14.1%
30,000–49,999,
12.6
%50,000–
69,999,18.4%
70,000–99,999,
23.9
%>100,000,
14.0
%don'tk
now.
Chinese
immigrants
hadahigher
percentage
(32.4%)
ofannualhousehold
incomes
below
$30,000compared
with
US-born
Chinese
andnon-Hispanic
White.
Northern
California
M=23.1
yearsin
the
USA
forChinese
immigrant
group.
Som
efocusgroups
andinterviewswere
conductedin
Chinese.
Chinese
Paxtonetal.[36]
n=96
Asian
American,
n=118African
American,n
=165
Hispanic,n=2634
White
Asian:M
edian=
52years
Asian:4
1StageI,
54stageII,1
stageIIIA
Asian:M
edian
time=
2years
sincediagnosis
Asian:9
high
school
orless,16some
college,71college
graduateor
more
Not
reported
California,Arizona,
Oregon,Texas
Not
reported
N/A
Lim
etal.[37]
n=206Asian
forthe
survey,n
=11
Korean
American
forthefocus
groups
M=54
Survey:3
7Stage
0,108StageI,100
stageII,20
stageIII
Survey:M
=3years
Survey:9
less
than
high
school,28
high
school
graduate,169
morethan
high
1school
Survey:5
1$25,000or
lower,41$25,000–
$45,000,51
$45,001–$75,000,
63$75,000
orhigher
California
KoreanBCSmight
have
adifferentp
attern
ofassociationin
the
doctor-patient
relationshipcompared
with
theculturalh
ealth
beliefsof
otherAABCS.
Lim
andPaek
[38]
n=86
Chinese
American,
n=71
Korean
American
M=55.3
Chinese:1
0Stage0,
22StageI,45
stageII,9
stage
III;Korean:
1Stage0,34
Stage
I,23
stageII,12
stageIII
Chinese:M
=3.2
years;Korean:
M=3.9years
43high
school
orless,
114higherthan
high
school
57<$25,000,25
$25,000–$45,000,
26$45,000–$75,000,
37<$75,000
Los
Angeles,
California
Lengthof
stay
inthe
USA
:M=23.9
years,
survey
was
innativelanguage.
Structuralpathsvaried
betweenChinese
American
andKorean
American
BCS.
Lee
etal.4[39]
n=4Chinese
American,
n=5Korean
American
M=53.7
years
8Stages
I–III
Allbuto
newere
within
5years
sincediagnosis
7college
graduate
andabove
6above$75,000
Maryland
Allim
migrants
Chinese
and
Koreanfocus
J Cancer Surviv (2014) 8:94–107 99

chose lumpectomy and adjuvant therapy at a significantlylower rate than did Caucasian women [15, 19].
Health efficacy
Health efficacy is the ability to engage in behaviors to promotegood health, prevent disease, and negotiate optionaltreatments and preferences with providers. In qualitativestudies, Asian Americans reported a lack of knowledge aboutbreast cancer and its treatment and a lack of resources inregard to managing survivorship [19]. In regard to treatmentdecision-making communication, Asian American womenalso were less likely to be assertive and were mostly relianton physicians to make breast cancer treatment decisions [34].Limited English proficiency was also reported as a majorbarrier to understanding breast cancer information andtreatment decision making [34].
In terms of health promotion behaviors during survivorship,Lim et al. found that both Asian and Hispanic Americanwomen reported changes in their diet patterns; further, AsianAmericans were more likely to increase their physical activitylevels and enhance their stress management skills [25].Similarly, Paxton et al. reported that more Asian Americanbreast cancer survivors met the guidelines for physical activitythan did Hispanic or African American survivors [36]. Further,health beliefs, doctor–patient relationship, and shared decisionmaking were influential factors in regard to adopting healthylifestyle practices during survivorship among Asian Americanbreast cancer survivors [37]. Information on alternativetherapies and relaxation skills also was reported as needed byChinese and Korean American women during breast cancersurvivorship [39].
System-level dimensions
Demographic and socio-ecological factors
Consistent with the existing literature on the breast cancerexperience, younger women had higher distress levels amongAsian American breast cancer survivors [15]. As forsocioeconomic status (SES), studies documented that AsianAmerican immigrants or those with lower acculturationreported a lower level of education and income than did US-born Asians with breast cancer [22, 23, 30, 35]. Further, SESindicators (income and education) were found to influence lifeburden and physical QOL among a multi-ethnic sample,including Asian American breast cancer survivors [27].Similarly, survivors with lower income level, lower educationlevel, or who were unemployed were likely to have less-favorable emotional well-being [31].
Within the framework of the Contextual Model, socialsupport is proposed to mitigate the negative impact of canceron HRQOL. Social support is recognized as central for
recovery, coping, and good QOL by Asian American breastcancer survivors [19, 21, 22], but they reported a lack of socialsupport [39], had greater difficulty requesting help fromothers, and sought psychosocial services at a significantlylower rate than did Caucasians [15, 16]. Support groupservices were reported as desired [39] and utilized [17, 19];but compared with Caucasian women, Asian Americanwomen have smaller social network size and compositionfrom limited sources of support [15, 16].
Cultural factors
Our review found a consistent relationship between the healthof Asian American breast cancer survivors and theiracculturation level, which is determined by place of birth,length of residency, or English proficiency. For example, theFilipino women in the Gotay et al. study were less likely tohave been born in the USA and had lower emotional andphysical outcomes than did the other groups [18]. Kim et al.also found lower HRQOL among less-acculturated women ina mixed-Asian group [23]. Other studies found that highlyacculturated Asian American breast cancer survivors receivedgreater social support [30, 40], which is recognized as centralto good HRQOL by Asian American women [22]. Further,foreign-born Chinese women are more likely to define QOLin terms of financial security as compared to US-born Chinesewomen, who frame QOL in terms of interpersonalrelationships [22]. English proficiency was reported as asignificant factor in symptom distress and HRQOL among aChinese and Vietnamese American group [29].
Culture also influences how Asian Americans react tobreast cancer and perceive their health. Asian Americanwomen reported feelings of self-consciousness andinadequacy, and perceived cancer as a stigma, not openlydiscussable with their families [21, 22]. Further, Asian culturaland gender socialization dictates that Asian American womenbe self-sacrificing and nurturing of their husband and family,serving as caregivers with obligations, not as dependents [19,20]. Compared with Latinas, Asian American women weremore likely to believe that their family and culturalbackground plays a role in their health [25]. Tsai et al. reportedthat traditional cultural beliefs persistently influence howChinese Americans interpret and cope with breast cancer intheir given sociocultural environment; as in their study,acculturation was found to be related to health beliefs, socialsupport, and life stress [30].
Spirituality also was an important influence among AsianAmericans. Family closeness, traditional Chinese values,religion, and Chinese support groups were recognized asspiritual resources among Chinese immigrant women withbreast cancer [17]. In multi-ethnic samples, Levine et al. foundthat more Asian American women reported that they werespiritual [24], were more likely to pray, felt closer to God, and
100 J Cancer Surviv (2014) 8:94–107
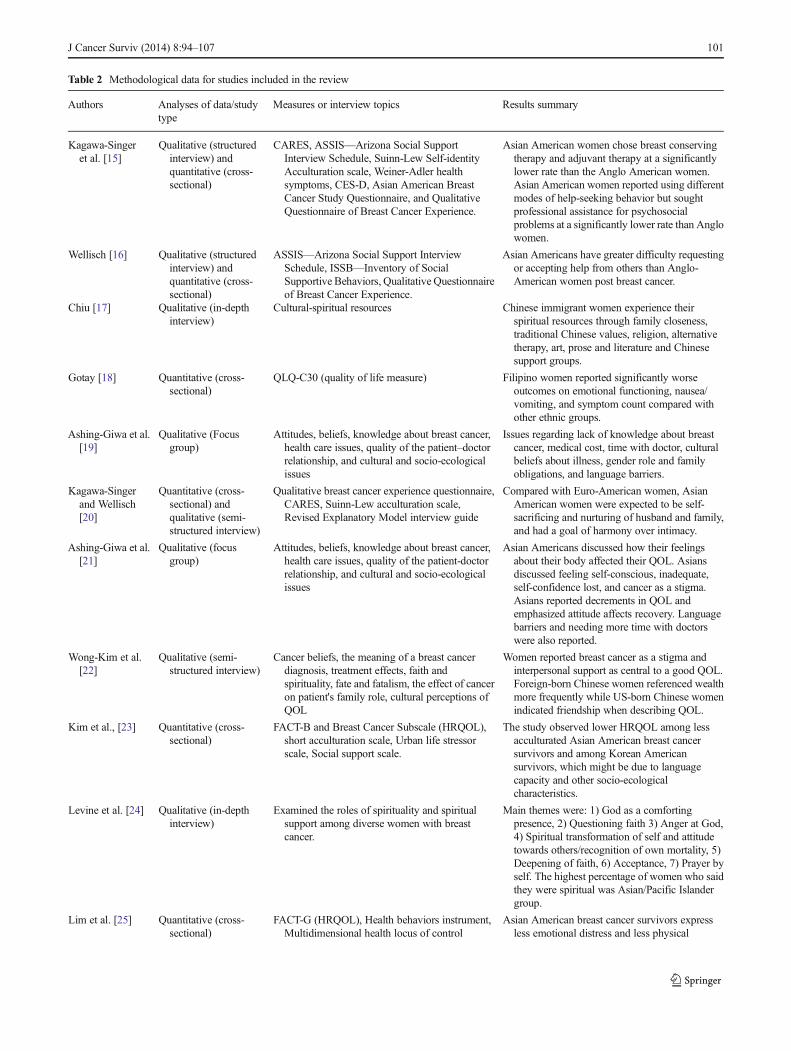
Table 2 Methodological data for studies included in the review
Authors Analyses of data/studytype
Measures or interview topics Results summary
Kagawa-Singeret al. [15]
Qualitative (structuredinterview) andquantitative (cross-sectional)
CARES, ASSIS—Arizona Social SupportInterview Schedule, Suinn-Lew Self-identityAcculturation scale, Weiner-Adler healthsymptoms, CES-D, Asian American BreastCancer Study Questionnaire, and QualitativeQuestionnaire of Breast Cancer Experience.
Asian American women chose breast conservingtherapy and adjuvant therapy at a significantlylower rate than the Anglo American women.Asian American women reported using differentmodes of help-seeking behavior but soughtprofessional assistance for psychosocialproblems at a significantly lower rate than Anglowomen.
Wellisch [16] Qualitative (structuredinterview) andquantitative (cross-sectional)
ASSIS—Arizona Social Support InterviewSchedule, ISSB—Inventory of SocialSupportive Behaviors, Qualitative Questionnaireof Breast Cancer Experience.
Asian Americans have greater difficulty requestingor accepting help from others than Anglo-American women post breast cancer.
Chiu [17] Qualitative (in-depthinterview)
Cultural-spiritual resources Chinese immigrant women experience theirspiritual resources through family closeness,traditional Chinese values, religion, alternativetherapy, art, prose and literature and Chinesesupport groups.
Gotay [18] Quantitative (cross-sectional)
QLQ-C30 (quality of life measure) Filipino women reported significantly worseoutcomes on emotional functioning, nausea/vomiting, and symptom count compared withother ethnic groups.
Ashing-Giwa et al.[19]
Qualitative (Focusgroup)
Attitudes, beliefs, knowledge about breast cancer,health care issues, quality of the patient–doctorrelationship, and cultural and socio-ecologicalissues
Issues regarding lack of knowledge about breastcancer, medical cost, time with doctor, culturalbeliefs about illness, gender role and familyobligations, and language barriers.
Kagawa-Singerand Wellisch[20]
Quantitative (cross-sectional) andqualitative (semi-structured interview)
Qualitative breast cancer experience questionnaire,CARES, Suinn-Lew acculturation scale,Revised Explanatory Model interview guide
Compared with Euro-American women, AsianAmerican women were expected to be self-sacrificing and nurturing of husband and family,and had a goal of harmony over intimacy.
Ashing-Giwa et al.[21]
Qualitative (focusgroup)
Attitudes, beliefs, knowledge about breast cancer,health care issues, quality of the patient-doctorrelationship, and cultural and socio-ecologicalissues
Asian Americans discussed how their feelingsabout their body affected their QOL. Asiansdiscussed feeling self-conscious, inadequate,self-confidence lost, and cancer as a stigma.Asians reported decrements in QOL andemphasized attitude affects recovery. Languagebarriers and needing more time with doctorswere also reported.
Wong-Kim et al.[22]
Qualitative (semi-structured interview)
Cancer beliefs, the meaning of a breast cancerdiagnosis, treatment effects, faith andspirituality, fate and fatalism, the effect of canceron patient's family role, cultural perceptions ofQOL
Women reported breast cancer as a stigma andinterpersonal support as central to a good QOL.Foreign-born Chinese women referenced wealthmore frequently while US-born Chinese womenindicated friendship when describing QOL.
Kim et al., [23] Quantitative (cross-sectional)
FACT-B and Breast Cancer Subscale (HRQOL),short acculturation scale, Urban life stressorscale, Social support scale.
The study observed lower HRQOL among lessacculturated Asian American breast cancersurvivors and among Korean Americansurvivors, which might be due to languagecapacity and other socio-ecologicalcharacteristics.
Levine et al. [24] Qualitative (in-depthinterview)
Examined the roles of spirituality and spiritualsupport among diverse women with breastcancer.
Main themes were: 1) God as a comfortingpresence, 2) Questioning faith 3) Anger at God,4) Spiritual transformation of self and attitudetowards others/recognition of own mortality, 5)Deepening of faith, 6) Acceptance, 7) Prayer byself. The highest percentage of women who saidthey were spiritual was Asian/Pacific Islandergroup.
Lim et al. [25] Quantitative (cross-sectional)
FACT-G (HRQOL), Health behaviors instrument,Multidimensional health locus of control
Asian American breast cancer survivors expressless emotional distress and less physical
J Cancer Surviv (2014) 8:94–107 101
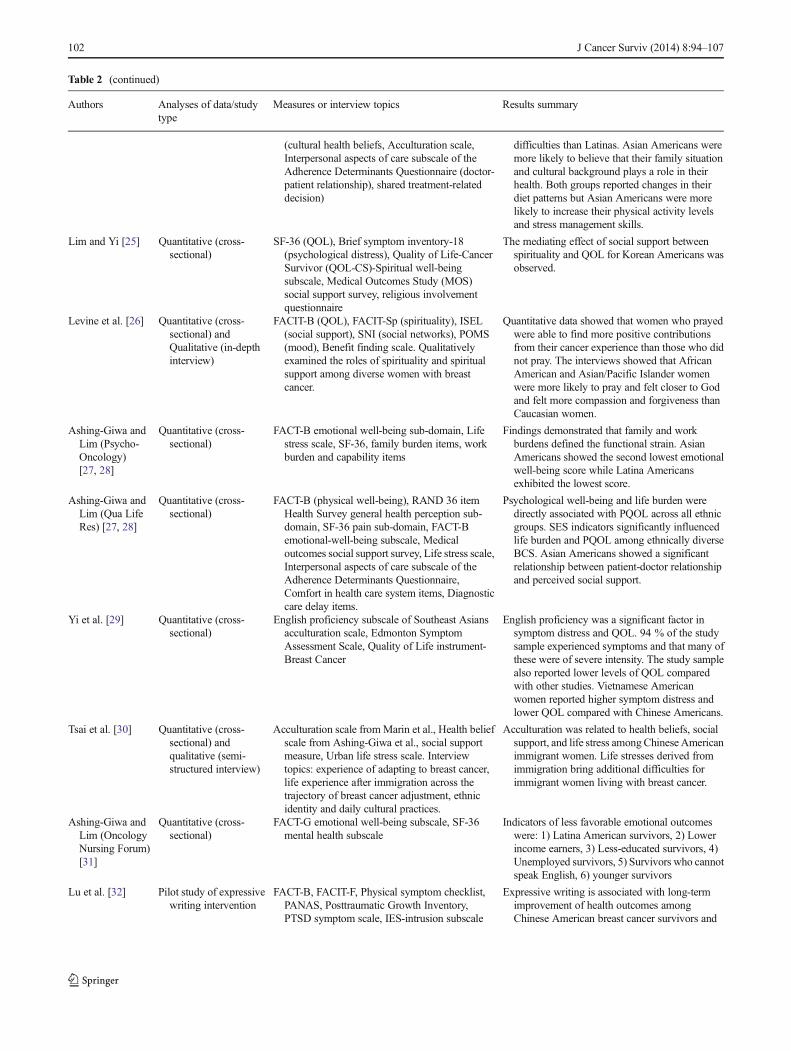
Table 2 (continued)
Authors Analyses of data/studytype
Measures or interview topics Results summary
(cultural health beliefs, Acculturation scale,Interpersonal aspects of care subscale of theAdherence Determinants Questionnaire (doctor-patient relationship), shared treatment-relateddecision)
difficulties than Latinas. Asian Americans weremore likely to believe that their family situationand cultural background plays a role in theirhealth. Both groups reported changes in theirdiet patterns but Asian Americans were morelikely to increase their physical activity levelsand stress management skills.
Lim and Yi [25] Quantitative (cross-sectional)
SF-36 (QOL), Brief symptom inventory-18(psychological distress), Quality of Life-CancerSurvivor (QOL-CS)-Spiritual well-beingsubscale, Medical Outcomes Study (MOS)social support survey, religious involvementquestionnaire
The mediating effect of social support betweenspirituality and QOL for Korean Americans wasobserved.
Levine et al. [26] Quantitative (cross-sectional) andQualitative (in-depthinterview)
FACIT-B (QOL), FACIT-Sp (spirituality), ISEL(social support), SNI (social networks), POMS(mood), Benefit finding scale. Qualitativelyexamined the roles of spirituality and spiritualsupport among diverse women with breastcancer.
Quantitative data showed that women who prayedwere able to find more positive contributionsfrom their cancer experience than those who didnot pray. The interviews showed that AfricanAmerican and Asian/Pacific Islander womenwere more likely to pray and felt closer to Godand felt more compassion and forgiveness thanCaucasian women.
Ashing-Giwa andLim (Psycho-Oncology)[27, 28]
Quantitative (cross-sectional)
FACT-B emotional well-being sub-domain, Lifestress scale, SF-36, family burden items, workburden and capability items
Findings demonstrated that family and workburdens defined the functional strain. AsianAmericans showed the second lowest emotionalwell-being score while Latina Americansexhibited the lowest score.
Ashing-Giwa andLim (Qua LifeRes) [27, 28]
Quantitative (cross-sectional)
FACT-B (physical well-being), RAND 36 itemHealth Survey general health perception sub-domain, SF-36 pain sub-domain, FACT-Bemotional-well-being subscale, Medicaloutcomes social support survey, Life stress scale,Interpersonal aspects of care subscale of theAdherence Determinants Questionnaire,Comfort in health care system items, Diagnosticcare delay items.
Psychological well-being and life burden weredirectly associated with PQOL across all ethnicgroups. SES indicators significantly influencedlife burden and PQOL among ethnically diverseBCS. Asian Americans showed a significantrelationship between patient-doctor relationshipand perceived social support.
Yi et al. [29] Quantitative (cross-sectional)
English proficiency subscale of Southeast Asiansacculturation scale, Edmonton SymptomAssessment Scale, Quality of Life instrument-Breast Cancer
English proficiency was a significant factor insymptom distress and QOL. 94 % of the studysample experienced symptoms and that many ofthese were of severe intensity. The study samplealso reported lower levels of QOL comparedwith other studies. Vietnamese Americanwomen reported higher symptom distress andlower QOL compared with Chinese Americans.
Tsai et al. [30] Quantitative (cross-sectional) andqualitative (semi-structured interview)
Acculturation scale fromMarin et al., Health beliefscale from Ashing-Giwa et al., social supportmeasure, Urban life stress scale. Interviewtopics: experience of adapting to breast cancer,life experience after immigration across thetrajectory of breast cancer adjustment, ethnicidentity and daily cultural practices.
Acculturation was related to health beliefs, socialsupport, and life stress amongChinese Americanimmigrant women. Life stresses derived fromimmigration bring additional difficulties forimmigrant women living with breast cancer.
Ashing-Giwa andLim (OncologyNursing Forum)[31]
Quantitative (cross-sectional)
FACT-G emotional well-being subscale, SF-36mental health subscale
Indicators of less favorable emotional outcomeswere: 1) Latina American survivors, 2) Lowerincome earners, 3) Less-educated survivors, 4)Unemployed survivors, 5) Survivors who cannotspeak English, 6) younger survivors
Lu et al. [32] Pilot study of expressivewriting intervention
FACT-B, FACIT-F, Physical symptom checklist,PANAS, Posttraumatic Growth Inventory,PTSD symptom scale, IES-intrusion subscale
Expressive writing is associated with long-termimprovement of health outcomes amongChinese American breast cancer survivors and
102 J Cancer Surviv (2014) 8:94–107
felt more compassion and forgiveness than did Caucasianwomen [26]. Further, women who prayed were able to findmore positive contributions from their cancer experience thanthose who did not pray [26]. Consistent with the findings ofAshing-Giwa and her colleagues, Asian American womenwho participated in focus groups believed in the positiveeffects of prayer and used prayer to cope with their breastcancer [19, 21].
Healthcare system factors
A consistent finding among qualitative studies is that AsianAmericans generally reported limited English proficiency as abarrier to accessing health information and quality of healthcare as well as to doctor–patient communication and medicaldecision making [19, 21, 33, 34]. Identified healthcare systemissues included insurance and medical costs, limited time with
Table 2 (continued)
Authors Analyses of data/studytype
Measures or interview topics Results summary
participants perceived the intervention to beappropriate and valuable.
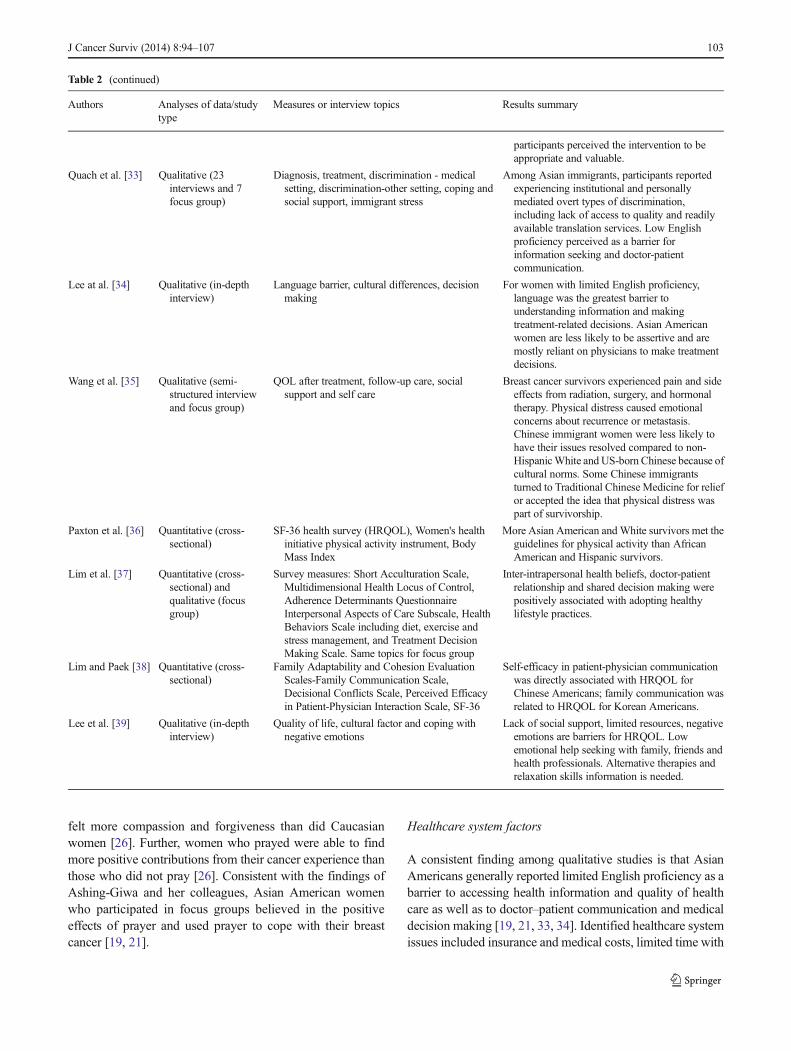
Quach et al. [33] Qualitative (23interviews and 7focus group)
Diagnosis, treatment, discrimination - medicalsetting, discrimination-other setting, coping andsocial support, immigrant stress
Among Asian immigrants, participants reportedexperiencing institutional and personallymediated overt types of discrimination,including lack of access to quality and readilyavailable translation services. Low Englishproficiency perceived as a barrier forinformation seeking and doctor-patientcommunication.
Lee at al. [34] Qualitative (in-depthinterview)
Language barrier, cultural differences, decisionmaking
For women with limited English proficiency,language was the greatest barrier tounderstanding information and makingtreatment-related decisions. Asian Americanwomen are less likely to be assertive and aremostly reliant on physicians to make treatmentdecisions.
Wang et al. [35] Qualitative (semi-structured interviewand focus group)
QOL after treatment, follow-up care, socialsupport and self care
Breast cancer survivors experienced pain and sideeffects from radiation, surgery, and hormonaltherapy. Physical distress caused emotionalconcerns about recurrence or metastasis.Chinese immigrant women were less likely tohave their issues resolved compared to non-HispanicWhite and US-born Chinese because ofcultural norms. Some Chinese immigrantsturned to Traditional Chinese Medicine for reliefor accepted the idea that physical distress waspart of survivorship.
Paxton et al. [36] Quantitative (cross-sectional)
SF-36 health survey (HRQOL), Women's healthinitiative physical activity instrument, BodyMass Index
More Asian American andWhite survivors met theguidelines for physical activity than AfricanAmerican and Hispanic survivors.
Lim et al. [37] Quantitative (cross-sectional) andqualitative (focusgroup)
Survey measures: Short Acculturation Scale,Multidimensional Health Locus of Control,Adherence Determinants QuestionnaireInterpersonal Aspects of Care Subscale, HealthBehaviors Scale including diet, exercise andstress management, and Treatment DecisionMaking Scale. Same topics for focus group
Inter-intrapersonal health beliefs, doctor-patientrelationship and shared decision making werepositively associated with adopting healthylifestyle practices.
Lim and Paek [38] Quantitative (cross-sectional)
Family Adaptability and Cohesion EvaluationScales-Family Communication Scale,Decisional Conflicts Scale, Perceived Efficacyin Patient-Physician Interaction Scale, SF-36
Self-efficacy in patient-physician communicationwas directly associated with HRQOL forChinese Americans; family communication wasrelated to HRQOL for Korean Americans.
Lee et al. [39] Qualitative (in-depthinterview)
Quality of life, cultural factor and coping withnegative emotions
Lack of social support, limited resources, negativeemotions are barriers for HRQOL. Lowemotional help seeking with family, friends andhealth professionals. Alternative therapies andrelaxation skills information is needed.
J Cancer Surviv (2014) 8:94–107 103

providers, and lack of medical translation services [19, 21, 33,34]. In particular, Quach et al. reported that Asian Americanimmigrants with breast cancer perceived discrimination byhealth care providers as a result of these immigrants' havinglow English proficiency, limited education, as an immigrant(outsider), and lower economic status [33]. In contrast, inAshing-Giwa et al.'s focus group study, most of the womendid not feel that they were discriminated against or treateddifferently when accessing care but did feel that their healthinsurance, financial situation, and knowledge of their illnessaffected the quality of care received [19]. In quantitativeresearch, the doctor–patient relationship was found to besignificantly associated with social support [27] and withadopting healthy lifestyle practices [37].
Differences among Asian American subgroups
In regard to comparisons between Chinese and other AsianAmerican subgroups, two studies reported the differences inthe type of preferred feedback and in social network utilizationbetween Chinese and Japanese breast cancer patients [15, 16].Chinese women tend to need less advice and generally receivesocial support from family. Japanese women need lesspositive feedback, have smaller social network size, and aremore likely to obtain social support from co-workers andfriends, less so from family. Yi et al. also documented thatChinese women reported lower symptom distress and higherHRQOL as compared with Vietnamese women [29]. Chineseand Korean women exhibited different reactions to breastcancer, according to Ashing-Giwa et al. [19]. In terms of therelationship between communication and HRQOL, self-efficacy in doctor–patient communication was associated withHRQOL for Chinese women, while family communicationwas related to HRQOL for Korean women [38].
Further, in a quantitative study of a mixed group of AsianAmerican breast cancer survivors, lower HRQOL wasobserved among Korean women [23].Using a mixed-methods approach, Lim et al. found that the cultural healthbeliefs of Korean women has a different association with thedoctor–patient relationship than it does among other AsianAmerican subgroups [37].
Intervention and longitudinal studies
In the only intervention study that we identified in theliterature, Lu et al. evaluated the potential benefits of anexpressive writing intervention among Chinese-speakingbreast cancer survivors [32]. Despite the small sample size(n =19), the findings indicated that participants reported highcompliance and satisfaction, and the intervention wasassociated with improved HRQOL outcomes. No longitudinalstudies that assessed survivorship-related outcomes among
Asian American breast cancer survivors were found in oursearch.
Discussion
Summary of findings
The present review is the first to summarize the survivorshipliterature among Asian American breast cancer survivorsusing a Contextual Model of HRQOL. A total of 26 studieswere included, of which 16 used five identical or overlappingsamples [15, 16, 19–21, 23–28, 30, 31, 34, 37, 39].Synthesizing the findings is challenging due to the variabilityamong the study approaches and sample sizes as well as thecultural diversity of the Asian American subgroups.
Asian Americanwomenwith breast cancer have significantphysical needs, and they are less likely to have them resolved,as compared to Caucasians and US-born Asian Americans[21, 35]. Commonly reported breast cancer treatment sideeffects, including fatigue and pain, were experienced byAsian American women and required attention from healthcare providers [18, 21, 29, 35]. However, because healthcareservices are obtained through a combination of governmentand private insurers, Asian Americans, especially those whorecently immigrated and who have limited Englishproficiency and are not familiar with US healthcare policies,may have difficulty navigating the medical system andinteracting with providers. As highlighted in the Institute ofMedicine report [41], cancer patient follow-up care is usuallyfragmented and without a strategy to assist patients innavigating survivorship. For Asian Americans with limitedEnglish proficiency and limited insurance coverage, effectivesurvivorship communication with oncologists and primarycare physicians is extremely challenging. Thus, the significantexpansion of the Asian American breast cancer survivorpopulation in the coming years will require better-coordinated and patient-centered follow-up care. Futureresearch is needed to examine the cultural relevance ofsurvivorship care plans developed for Asian Americanpopulations.
The studies in our review indicate that Asian Americanbreast cancer survivors reported levels of emotional distressand fear of recurrence comparable to those of Caucasianwomen [15, 21]. Further, although cultural practices, such asspirituality and family closeness, may have benefits for breastcancer survivorship, they also can have a negative impact onhow Asian Americans react to breast cancer and seek help.Asian Americans with breast cancer reported sources ofdistress that included feeling ashamed and stigmatized as wellas a need to engage in self-sacrificing behavior to avoiddisrupting harmony [20, 22]. Some Asian American womenreported a lower rate of seeking professional services for
104 J Cancer Surviv (2014) 8:94–107

psychosocial problems than did Caucasian woman [15], whileother studies reported that Asian American women did utilizesupport group services [17, 19] when available and expressedtheir desire for such resources when asked [39]. Thesefindings challenge the stereotype of limited acceptability ofsupport groups among Asian Americans. It may be that thedisparity is caused by the unavailability of mental health careservices that are culturally competent for these AsianAmericans in need. Further, culturally relevant and faith-based cancer support groups have been adopted in addressingthe needs of breast cancer survivors from other ethnic/racialminority groups, including African and Hispanic Americans[42, 43]. In Australia, Kwok et al. recently reported that aculturally sensitive and linguistically appropriate supportgroup was well received by Chinese Australian breast cancerpatients [44]. They concluded that one of the most crucialelements that improved the support group attendance rate andengagement was the provision of culturally sensitiveinformation corresponding to women's beliefs and norms.Therefore, given that coping strategies vary among culturalgroups, providing culturally and linguistically appropriatesupport groups that are accessible and congruent with thevalues and beliefs of Asian American subgroups is critical.
Limitations in the existing literatures and future directions
We noted significant gaps in the existing literature: first, only asmall number of studies included adequate samples of AsianAmerican subgroups despite the fact that differences in breastcancer survivorship responses and outcomes are presentamong subgroups of Asian American women [15, 16,18–20, 23, 29, 37, 38]. This could be due, in part, to thechallenges of recruiting immigrant women—particularly ifimmigration status serves as a barrier to women's willingnessto participate in research—although this issue was not raisedin any of the studies reviewed. In addition, few studies havespecifically examined the survivorship experiences ofAmerican-born Asian populations. More research is neededto explore potential intragroup differences within the largerAsian American breast cancer population, especially in lightof the projections that Asian Americans will become one ofthe fastest growing and most heterogeneous ethnic groups inthe USA [45]. Second, 16 studies reported on identical oroverlapping samples (five datasets), which may have inflatedthe study findings in the literature. Third, the majority of thestudies were conducted in California, which limits thegeneralizability of the findings to non-California populations.Research on breast cancer survivorship for populations inregions of the USA beyond California, including otherAsian-concentrated states such as New York and New Jerseyis warranted. Fourth, most of the studies used translatedmeasures/questions; however, as individuals from differentAsian American subgroups may interpret questions differently
or have different response patterns that might impact on themeasure's cross-cultural utility [46, 47], we need to assess if theavailable instruments are culturally appropriate and are validmeasures in the Asian American breast cancer population.
There was no published study utilizing a longitudinal designidentified by this review; thus, longitudinal studies are criticallyneeded to assess change in Asian American breast cancersurvivor's experiences and HRQOL over time. This will providevaluable information on how and when to best meet their needsthroughout the cancer trajectory. In addition, research is neededto assess long-term survivorship outcomes among Asians (5 ormore years since the diagnosis of cancer [48]), as almost allstudies in this review included women within 5 years ofdiagnosis. Research on the changes in needs and in HRQOLfollowing cancer diagnosis, during treatment, at treatmentcompletion, and during short-term and long-term survivorshipamong Asian American subgroups is warranted, particularly tounderstand when Asians are at risk for poorer HRQOL and howinterventions might be beneficial. For example, insurance,language, and barrier-to-care issues might be especiallyprevalent during early diagnosis. Fear of recurrence is likely tobe more pertinent later in cancer survivorship.
Further, there is a growing body of work on nutrition andexercise for Caucasian breast cancer populations. Future studiesare needed to investigate how positive dietary change orincreased level of physical activity affects survivorship amongAsian American women with breast cancer. In addition toresearch on individual-level interventions that take into accountthe demographics usually associated with the availability ofcommunity and institutional resources, we also need researchthat focuses on system-level influences to reduce disparities andimprove HRQOL among Asian American survivors. Forexample, more cancer screening and surveillance services needto be accessible to Asian Americans in their community andmore Asian language interpreters need to be available in thehealth care system. Further, to increase participant engagementin research, researchers need to employ culturally relevantapproaches (community-based participatory research) and noveltechnologies (mobile health programs), particularly inintervention studies. In particular, data show that AsianAmericans have a higher rate of Smartphone adoption than allother ethnicities [49]. Use of mobile technologies to facilitatebreast cancer management among Asian American women hasgreat potential to reduce the disease burden and healthdisparities.
Our findings should be interpreted in the context of thelimitations of this review. First, although we searched fourmajor bibliographic databases, we may have overlooked somestudies that were published in smaller journals that were notindexed in traditional sources. Second, given that the AsianAmerican sample size in multi-ethnic studies was relativelysmall, finding results specific to Asian or Asian Americansubgroups was challenging.
J Cancer Surviv (2014) 8:94–107 105

Conclusions
To the best of our knowledge, the present review is among thefirst to synthesize the literature on Asian American breastcancer survivors' experience and outcomes, based on theContextual Model of HRQOL. Although Asian Americanbreast cancer survivorship research is emerging, the lack oflongitudinal and intervention research as well as research onAsian subgroups within a heterogeneous population stronglysuggests future research efforts are needed in these areas.Based on the existing literature, we concluded that AsianAmericans experience disrupted HRQOL following breastcancer diagnosis and treatment, interwoven with their culturaland socio-ecological system, and that intervention studiesfocused on improving cancer survivorship outcomes amongthis ethnic minority group are limited. Some studies in thisreview reported that Asian Americans would like to attendbreast cancer support groups and receive survivorship-relatedinformation about stress management and relaxation if suchresources were accessible to them [17, 39]. Although we havea growing body of literature on the efficacy of psychosocialstress management interventions among samples primarily ofCaucasian women [50, 51], research is critically needed todetermine whether these interventions can be culturallyadopted for Asian Americans or Asian subgroups. Wereported findings focused on specific domains of theContextual Model of HRQOL and suggest potential targetsamenable to intervention development and testing. Evidencesuggests that Asian Americans are at higher risk for poorHRQOL following a breast cancer diagnosis, compared tonon-Hispanic and Caucasian women, and that they havelimited resources. We recognize that there is a critical needto build on the existing research as a means to developculturally tailored and linguistically appropriate interventionsto improve HRQOL and to reduce health disparities amongthis rapidly growing ethnic minority population.
Acknowledgments Kuang-YiWen is currently funded byAHRQ grant1K01HS019001. This work was supported in part by the NIH-NCI'sCommunity Network Program Center, ACCHDC (U54CA153513, PI:Dr. Grace Ma) and NIH P30 CA06927. We are indebted to Alison Petokand Kathy Ireton for their technical and administrative assistance.
References
1. Siegel R, Naishadham D, Jemal A. Cancer statistics. CA Cancer JClin. 2012;62:10–29.
2. Deapen D, Liu L, Perkins C, Bernstein L, Ross RK. Rapidly risingbreast cancer incidence rates among Asian-American women. Int JCancer. 2002;99:747–50.
3. Liu L, Zhang J, Wu AH, Pike MC, Deapen D. Invasive breast cancerincidence trends by detailed race/ethnicity and age. Int J Cancer.2012;130:395–404.
4. Smith BD, Smith GL, Hurria A, Hortobagyi GN, Buchholz TA.Future of cancer incidence in the United States: burdens upon anaging, changing nation. J Clin Oncol. 2009;27:2758–65.
5. Powe BD, Hamilton J, Hancock N, Johnson N, Finnie R, Ko J, et al.Quality of life of African American cancer survivors: a review of theliterature. Cancer. 2007;109:435–45.
6. Montazeri A. Health-related quality of life in breast cancer patients: abibliographic review of the literature from 1974 to 2007. J Exp ClinCancer Res. 2008;27:32.
7. Yu ES. Health of the Chinese elderly in America. Res Aging. 1986;8:84–109.
8. Nguyen TT, Somkin CP, Ma Y. Participation of Asian-Americanwomen in cancer chemoprevention research: physician perspectives.Cancer. 2005;104:3006–14.
9. Tu SP, Chen H, Chen A, Lim J, May S, Drescher C. Clinical trials:understanding and perceptions of female Chinese-American cancerpatients. Cancer. 2005;104:2999–3005.
10. Reich M, Lesur A, Perdrizet-Chevallier C. Depression, quality of lifeand breast cancer: a review of the literature. Breast Cancer Res Treat.2008;110:9–17.
11. Wong-Kim E, Sun A, DeMattos MC. Assessing cancer beliefs in aChinese immigrant community. Cancer Control. 2003;10:22–8.
12. Ma GX, Shive SE, Wang MQ, Tan Y. Cancer screening behaviorsand barriers in Asian Americans. Am J Health Behav. 2009;33:650–60.
13. Ashing-Giwa KT. The contextual model of HRQoL: a paradigm forexpanding the HRQoL framework. Qual Life Res. 2005;14:297–307.
14. Yanez B, Thompson EH, Stanton AL. Quality of life among Latinabreast cancer patients: a systematic review of the literature. J CancerSurviv. 2011;5:191–207.
15. Kagawa-Singer M, Wellisch DK, Durvasula R. Impact of breastcancer on Asian American and Anglo American women. Cult MedPsychiatry. 1997;21:449–80.
16. Wellisch D, Kagawa-Singer M, Reid SL, Lin YJ, Nishikawa-Lee S,Wellisch M. An exploratory study of social support: a cross-culturalcomparison of Chinese-, Japanese-, and Anglo-American breastcancer patients. Psychooncology. 1999;8:207–19.
17. Chiu L. Spiritual resources of Chinese immigrants with breast cancerin the USA. Int J Nurs Stud. 2001;38:175–84.
18. Gotay CC, Holup JL, Pagano I. Ethnic differences in quality of lifeamong early breast and prostate cancer survivors. Psychooncology.2002;11:103–13.
19. Ashing-Giwa KT, Padilla G, Tejero J, Kagawa-Singer M.Understanding the breast cancer experience of Asian Americanwomen. Psychooncology. 2003;12:38–58.
20. Kagawa-SingerM,Wellisch DK. Breast cancer patients' perceptions oftheir husbands' support in a cross-cultural context. Psychooncology.2003;12:24–37.
21. Ashing-Giwa KT, Padilla G, Tejero J, Kraemer J, Wright K,Coscarelli A, et al. Understanding the breast cancer experience ofwomen: a qualitative study of African American, Asian American,Latina and Caucasian cancer survivors. Psychooncology. 2004;13:408–28.
22. Wong-Kim E, Sun A, Merighi JR, Chow EA. Understanding quality-of-life issues in Chinese women with breast cancer: a qualitativeinvestigation. Cancer Control. 2005;12 Suppl 2:6–12.
23. Kim J, Ashing-Giwa KT, Kagawa Singer M, Tejero JS. Breast canceramong Asian Americans: is acculturation related to health-relatedquality of life? Oncol Nurs Forum. 2006;33:E90–9.
24. Levine EG, YooG, Aviv C, EwingC, Au A. Ethnicity and spiritualityin breast cancer survivors. J Cancer Surviv. 2007;1:212–25.
25. Lim JW, Gonzalez P, Wang-Letzkus MF, Ashing-Giwa KT.Understanding the cultural health belief model influencing healthbehaviors and health-related quality of life between Latina andAsian-American breast cancer survivors. Support Care Cancer.2009;17:1137–47.
106 J Cancer Surviv (2014) 8:94–107
26. Levine EG, Aviv C, Yoo G, Ewing C, Au A. The benefits of prayeron mood and well-being of breast cancer survivors. Support CareCancer. 2009;17:295–306.
27. Ashing-Giwa KT, Lim JW. Predicting physical quality of life amonga multiethnic sample of breast cancer survivors. Qual Life Res.2010;19:789–802.
28. Ashing-Giwa KT, Lim JW. Exploring the association betweenfunctional strain and emotional well-being among a population-based sample of breast cancer survivors. Psychooncology. 2010;19:150–9.
29. Yi JK, Swartz MD, Reyes-Gibby CC. English proficiency,symptoms, and quality of life in Vietnamese- and Chinese-American breast cancer survivors. J Pain Symptom Manage.2011;42:83–92.
30. Tsai TI, Morisky DE, Kagawa-Singer M, Ashing-Giwa KT.Acculturation in the adaptation of Chinese-American women tobreast cancer: a mixed-method approach. J Clin Nurs. 2011;20:3383–93.
31. Ashing-Giwa KT, Lim JW. Examining emotional outcomes among amultiethnic cohort of breast cancer survivors. Oncol Nurs Forum.2011;38:279–88.
32. Lu Q, Zheng D, Young L, Kagawa-Singer M, Loh A. A pilot study ofexpressive writing intervention among Chinese-speaking breastcancer survivors. Health Psychol. 2012;31:548–51.
33. Quach T, Nuru-Jeter A, Morris P, Allen L, Shema SJ, Winters JK,et al. Experiences and perceptions of medical discrimination among amultiethnic sample of breast cancer patients in the Greater SanFrancisco Bay Area, California. Am J Public Health. 2012;102:1027–34.
34. Lee S, Chen L, Ma GX, Fang CY. What is lacking in patient-physician communication: Perspectives from Asian Americanbreast cancer patients and oncologists. J Behav Health. 2012;1:102–9.
35. Wang JH, Adams I, Huang E, Ashing-Giwa K, Gomez SL, Allen L.Physical distress and cancer care experiences among Chinese-American and non-Hispanic White breast cancer survivors.Gynecol Oncol. 2012;124:383–8.
36. Paxton RJ, Phillips KL, Jones LA, Chang S, Taylor WC, CourneyaKS, et al. Associations among physical activity, bodymass index, andhealth-related quality of life by race/ethnicity in a diverse sample ofbreast cancer survivors. Cancer. 2012;118:4024–31.
37. Lim JW, Baik OM, Ashing-Giwa KT. Cultural health beliefs andhealth behaviors in Asian American breast cancer survivors: a mixed-methods approach. Oncol Nurs Forum. 2012;39:388–97.
38. Lim JW, Paek MS. The relationship between communication andhealth-related quality of life in survivorship care for Chinese-
American and Korean-American breast cancer survivors. SupportCare Cancer. 2013;21:1157–66.
39. Lee S, Chen L, Ma GX, Fang CY, Oh Y, Scully L. Challenges andneeds of Chinese and Korean American breast cancer survivors: in-depth interviews. N Am J Med Sci (Boston). 2013;6:1–8.
40. Lim JW,Yi J, Zebrack B.Acculturation, social support, and quality oflife for Korean immigrant breast and gynecological cancer survivors.Ethn Health. 2008;13:243–60.
41. Hewitt ME, Ganz P, Institute of Medicine (US), American Society ofClinical Oncology, American Society of Clinical Oncology, Instituteof Medicine Symposium on Cancer Survivorship. From cancerpatient to cancer survivor: lost in transition. Washington, DC:National Academies Press; 2006.
42. Barg FK, Gullatte MM. Cancer support groups: meeting the needs ofAfrican Americans with cancer. Semin Oncol Nurs. 2001;17:171–8.
43. Nápoles-Springer AM, Ortíz C, O'Brien H, Díaz-Méndez M.Developing a culturally competent peer support intervention forSpanish-speaking Latinas with breast cancer. J Immigr MinorHealth. 2009;11:268–80.
44. KwokC, HoM. Development and evaluation of a culturally sensitivesupport group programme for Chinese-Australian women with breastcancer: a pilot study. Eur J Cancer Care (Engl). 2011;20:795–802.
45. US Department of Commerce. (2010) Facts for features: Asian/Pacific American Heritage Month: May 2010. Available from:http://www.census.gov/newsroom/releases/archives/facts_for_features_special_editions/cb10-ff07.html. Accessed 22 Oct 2013.
46. Kagawa-Singer M. Improving the validity and generalizability ofstudies with underserved U.S. populations expanding the researchparadigm. Ann Epidemiol. 2000;10(8 Suppl):S92–103.
47. Hahn EA, Cella D. Health outcomes assessment in vulnerablepopulations: measurement challenges and recommendations. ArchPhys Med Rehabil. 2003;84(4 Suppl 2):S35–42.
48. Mols F, Vingerhoets AJ, Coebergh JW, van de Poll-Franse LV.Quality of life among long-term breast cancer survivors: a systematicreview. Eur J Cancer. 2005;41:2613–9.
49. America's new mobile majority: a look at smartphone owners in theU.S. Reported by Nielsen. 2012, http://www.nielsen.com/us/en/newswire/2012/who-owns-smartphones-in-the-us.html. Accessedon May/13/2013.
50. AntoniMH, Lechner SC, Kazi A,Wimberly SR, Sifre T, UrcuyoKR,et al. How stress management improves quality of life after treatmentfor breast cancer. J Consult Clin Psychol. 2006;74:1143–52.
51. Fors EA, Bertheussen GF, Thune I, Juvet LK, Elvsaas IK, Oldervoll L,et al. Psychosocial interventions as part of breast cancer rehabilitationprograms? Results from a systematic review. Psychooncology.2011;20:909–18.
J Cancer Surviv (2014) 8:94–107 107