Embed Size (px)
Citation preview

Review
10.1517/14656560903167957 © 2009 Informa UK Ltd ISSN 1465-6566 2479All rights reserved: reproduction in whole or in part not permitted
Breastcancer:beyondthecuttingedgeGerald M HigaWest Virginia University, Mary Babb Randolph Cancer Center, Schools of Pharmacy and Medicine, Morgantown, WV 26506-9520, USA
Remarkable progress has been made in the treatment of breast cancer over the past 100 years. The ability to probe at the genomic level increased our understanding of the disease but the improved survival outcomes can also be attributed to screening programs, which have altered the pattern of diagnosis and prognosis, and to a number of groundbreaking clinical trials. Indeed, the latter are largely responsible for the most startling paradigm reversals in oncology; namely, that optimal benefit can be achieved with minimal, rather than maximal, intervention. As such, surgical lumpectomy can replace the radical mastectomy, sentinel node biopsy may circumvent the need for complete (axillary) nodal dissection, hormonal therapy – depending on tumor sensitivity to endocrine manipulation – is likely to be beneficial without the addition of chemotherapy, and some targeted therapies can be used selectively in those most likely to benefit. However, despite the advances, controversies remain; patients die; and cure remains elusive.
Keywords: adjuvant therapy, aromatase inhibitor, chemoprevention, clinical trials, EGFR, estrogen receptor (ER), HER2, hormonal therapy, microtubule, progesterone receptor (PgR), sentinel node, tamoxifen, trastuzumab, VEGF
Expert Opin. Pharmacother. (2009) 10(15):2479-2498
1. Introduction
Breast cancer is arguably the most publicized (and politicized) malignant disease affecting women in industrialized countries of the world. Even in Japan, where the disease is less prevalent, the incidence rate of breast cancer differs by locale; being higher in ‘Westernized’ areas and lower in ‘rural’ portions of the island-nation. Furthermore, ethnic-specific incidence rates of breast cancer among Asian women who migrated to the United States have in some cases (reported in Japanese women) surpassed those of white women or are increasing (observed in Filipino and Korean women) as the migrant women become more acculturated [1,2]. While the search for cause and cure is not uncommon for cancers in general, the quest in breast cancer has taken on Quixote-like characteristics. Undaunted by uncertainties, basic science and clinical research have continued to improve the odds of surviving the disease.
The impetus for undertaking this endeavor was to prepare a review in which the contents would be both informative and instructive. The reader will gain an appre-ciation for our increased, although by no means complete, understanding of the disease. In addition, this article highlights a number of ground-breaking clinical trials that changed treatment standards as well as areas where uncertainty still exists.
2. Epidemiology
Breast cancer is the most frequently occurring malignancy among women in the United States and for reasons not completely understood the incidence of invasive disease has been decreasing (albeit slightly) over the past 5 years [3]. In 2008,
1. Introduction
2. Epidemiology
3. Treatment
4. Pharmacologic targets of
breast cancer
5. Conclusions
6. Expert opinion
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y SU
NY
Ups
tate
Med
ical
Uni
vers
ity o
n 08
/16/
14Fo
r pe
rson
al u
se o
nly.

Breastcancer:beyondthecuttingedge
2480 ExpertOpin.Pharmacother.(2009) 10(15)
approximately 183,000 new cases were diagnosed in the US, and 40,000 patients died as a result of progression or compli-cations of the disease. Despite the high prevalence and being the second leading cause of cancer deaths, breast cancer is not the most lethal malignant disease in women. Nevertheless, the statistics are quite striking in that every 15 min five women will be diagnosed with breast cancer and one patient will die because of the disease.
2.1 RiskfactorsAlthough a number of risk factors (Table 1) are allegedly associated with the development of breast cancer, three of the most important appear to be related to age, estrogens, and genes. Of all the risk factors that have been linked to the disease, age is still the single most important [4,5]. The impact of age on breast cancer incidence, however, requires some clarification. Whereas the life-time risk of developing breast cancer among Caucasian and African–American women is approximately 1 in 8 and 1 in 10, respectively [6], the incidence rate is 7 – 15 times higher as women approach 40 years of age, and approximately 25 – 30 times higher during the perimenopausal years than in their 20-something-year-old counterparts [7]. Because the incidence of breast cancer continues to rise after menopause, the current median age at diagnosis is 61 years. Although deferentially referred to as the silver years of life, a gloomy forecast may be brewing. Approximately 20% of the US population will be over 60 years old by the year 2030, and it is estimated that the absolute number of new breast cancer diagnoses will double by the year 2050.
While estrogens are unequivocally linked to the well-being of women, an equally strong association between the hormones and breast cancer also exists. The latter conclusion is supported by various forms of evidence. Experimentally, breast cancer cells have been shown to proliferate when exposed to estro-gens in vitro [8]; epidemiologically, the risk factor associated with early menarche/late menopause has been attributed to
Table1.Riskfactorsforbreastcancer.
High(relatively)
Increasing ageBreast cancer in a first-degree relativeAtypical ductal or lobular hyperplasiaLobular carcinoma in-situPrior history of breast cancerBRCA1 and BRCA2 mutationsIncreasing mammographic breast density
Low(relatively)
Early menarche/late menopauseElevated levels of estrogens and androgensAge at first live birth over 30 y or nulliparityDiet and alcohol consumptionPostmenopausal obesityExercise
a longer duration of exposure to estrogens [9] and, clinically, to the tumor regression that occurs following estrogen-deprivation strategies [10-12]. Besides the beneficial and detrimental effects of estrogens, another paradox is apparent in breast cancer. Although strongly implicated in the pathogenesis of disease, not all breast cancers retain estrogen-dependent regulation of cell proliferation at the time of diagnosis. Moreover, that a relatively high proportion of patients with estrogen receptor (ER)-positive breast cancers do not respond to anti-estrogen strategies refutes the notion that the absence of the ER alone can explain tumor insensitivity to hormonal therapy [13].
Finally, in the early 1990s, specific mutations were identified in two tumor suppressor genes (BRCA1 and BRCA2) respon-sible for familial breast and ovarian cancers. However, their full impact on managing, testing, and counseling carriers of these mutations is still unresolved [14,15]. Mutations in two other candidate genes that appear to confer high risk for breast cancer include PTEN (phosphatase and tensin homolog) and TP53 (tumor protein 53), both of which encode proteins that function as key regulators of cell division. In reality, mutations of the latter two genes account for only a minority of inherited breast cancers [16]. Although the total number of oncogenes is small, genome-wide studies may be able to iden-tify other breast-cancer-susceptibility genes that are associated with an increased risk of the disease [17-19].
Risk factors notwithstanding, it is somewhat surprising that, other than age, the majority of women diagnosed with breast cancer do not have any of the purported high-risk factors. Moreover, the identified risk factors (in total) are believed to explain only half of all breast cancer incidences [20].
3. Treatment
3.1 EarlybreastcancerAlthough improvement in 5- and 10-year survival rates has frequently been attributed to earlier detection, controversy exists regarding the degree of benefit ascribed to screening mammography [21-23]. None the less, the hallmark clinical trials that changed the standard [24-27], as well as the concept that breast cancer was a systemic disease at the time of (early) diagnosis, led to two major innovations in managing patients with early disease: first, utilization of breast-conserving surgery; and second, application of systemic adjuvant therapy.
Surgical mastectomy, which varies in extent, has been the primary therapeutic modality for more than a century [28]. Over the past 30 years, the results of clinical trials have clearly demonstrated that less aggressive surgery (i.e., lumpectomy) plus radiation to residual breast tissue was as effective as Halstead mastectomy. At the same time, although usually good, the overall prognosis of patients with operable breast cancer differs with respect to a number of tumor-specific characteristics including: size; expression of the estrogen and progesterone receptors (PgR), HER2/neu, and proteins linked to cell division such as Ki-67; as well as to nuclear grade, S-phase fraction, and ploidy [29]. However, the single most
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y SU
NY
Ups
tate
Med
ical
Uni
vers
ity o
n 08
/16/
14Fo
r pe
rson
al u
se o
nly.

Higa
ExpertOpin.Pharmacother.(2009) 10(15) 2481
Table2.Systemicadjuvanttherapyinbreastcancer[38,162-169].
Endocrinetherapy
All patients with hormone receptor-positive tumors should be treated with hormonal therapy. There is increasing evidence that patients with luminal A breast cancers, regardless of node status, may not need chemotherapy. Hormonal therapy should follow the completion of chemotherapy in patients who are destined to be treated with both types of agents
Tamoxifen, 20 mg daily for 5 years Unresolved question in premenopausal women: Is tamoxifen alone optimal? Are the combinations of tamoxifen and ovarian ablation or ovarian ablation plus aromatase inhibitor (AI) superior to monotherapy tamoxifen?
Tamoxifen 20 mg daily for 5 yearsorTamoxifen 20 mg daily for 2 – 3 years + anastrozole 1 mg daily, letrozole 2.5 mg daily or exemestane 25 mg daily for 2 – 3 yearsorTamoxifen 20 mg daily for 5 years + AI for 5 years
Unresolved question in postmenopausal women: Which of these regimens should be considered standard?Longer duration of therapy may be better, but at what cost?
Chemotherapy
Cytotoxic chemotherapy is the only option currently available for patients with ‘triple-negative’ breast cancers. Use of anthracycline- and taxane-containing regimens represents the current standard (although not necessarily embraced by all) for patients with node-positive tumors. The regimens listed are meant to be representative rather than exhaustive
Doxorubicin 60 mg/m2 IV + cyclophosphamide 600 mg/m2 IV; both agents given every 21 days × 4 cycles
‘AC’
Doxorubicin 60 mg/m2 IV + cyclophosphamide 600 mg/m2 IV; both agents given every 21 days, cycles 1 – 4 followed by paclitaxel 175 mg/m2 IV over 3 h q 21 days, cycles 5 – 8
‘AC → T’
Docetaxel 75 mg/m IV over 1 h + doxorubicin 50 mg/m2 IV + cyclophosphamide 500 mg/m2 IV; all agents given every 21 days × 6 cycles
‘TAC’
Chemotherapyplusanti-HER2therapy
Targeting HER2 significantly improves disease-free and overall survival, regardless of nodal status. Anti-HER2 therapy may be given concurrently with taxane- and non-anthracycline-containing regimens or following anthracycline-based regimens. Nonetheless, questions regarding targeted therapy of HER2 such as the optimal duration of therapy remain. Other issues are posed below
Doxorubicin 60 mg/m2 IV + cyclophosphamide 600 mg/m2 IV; both agents given every 21 days, cycles 1 – 4 followed by paclitaxel 175 mg/m2 IV over 3 h, cycles 5 – 8 + trastuzumab 4 mg/kg IV over 90 min, then 2 mg/kg IV over 30 min q week for more 51 weeks
‘AC → TH’ Does the increased benefit of giving trastuzumab in the context of anthracycline override the increased risk of cardiotoxicity? At the same time tumors that co-amplify topoisomerase II appear to benefit from anthracyclines
Doxorubicin 60 mg/m2 IV + cyclophosphamide 600 mg/m2 IV; both agents given every 21 days, cycles 1 – 4 followed by paclitaxel 80 mg/m2 IV over 3 h q week × 12 weeks, then trastuzumab 4 mg/kg IV over 90 min, then 2 mg/kg IV over 30 min q week for more 51 weeks
‘AC → T → H’ Do outcomes differ with sequential or concurrent trastuzumab?
Docetaxel 75 mg/m2 IV over 1 h + carboplatin AUC 6 IV over 30 min; both agents given every 21 days x 6 cycles + trastuzumab 4 mg/kg IV over 90 min on day 1 of cycle one, then 2 mg/kg IV over 30 min q week for more 51 weeks
‘TCH’ regimen Are agents that target both HER1 and HER2 better than trastuzumab?
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y SU
NY
Ups
tate
Med
ical
Uni
vers
ity o
n 08
/16/
14Fo
r pe
rson
al u
se o
nly.

Breastcancer:beyondthecuttingedge
2482 ExpertOpin.Pharmacother.(2009) 10(15)
important prognostic factor associated with disease-free survival (DFS) and overall survival (OS) is the extent of axillary node involvement. While results of early clinical trials indicated that the removal of at least six to ten nodes was required to optimize clinical staging and local control of disease, the procedure was also associated with a number of complica-tions including arm edema, loss of sensation, and shoulder dysfunction [24,30]. Over the past 10 years, the procedure known as sentinel node biopsy has gained widespread acceptance because of the specificity associated with assessment of a single node and the low postsurgical morbidity [31,32]. It should be emphasized that this minimal procedure is performed in order to evaluate the need, not as a substitution, for complete axillary node dissection. The minimal resection, however, is not without controversy regarding technique, patient selection, clinical approach, and staging accuracy.
While radiation is considered standard in patients who have breast-conserving surgery, addition of systemic therapy, which further reduces the rate of local recurrence, also produces an added benefit of increasing overall survival [33-36]. The survival advantages observed in clinical trials provided the following insights related to systemic adjuvant therapy: i) the decline in breast-cancer mortality appears to be related to administra-tion of anthracycline-containing chemotherapy regimens [37]; ii) the addition of a taxane to anthracyclines is associated with improved DFS and OS endpoints [38,39]; iii) aromatase inhibi-tors represent a new standard for postmenopausal women with hormone-dependent breast cancer [40], although taxomifen is still the endocrine therapy of choice for premenopausal women, ongoing clinical trials are evaluating whether addition of ovarian ablation or ovarian ablation plus an aromatase inhibi-tor is more effective than tamoxifen alone; and iv) the use of trastuzumab in the adjuvant setting results in significant prolon-gation of DFS and OS [41-43]; improved pathologic responses have also been reported with neoadjuvant trastuzumab in patients with HER2-overexpressing tumors [44-46].
The above conclusions are highlighted because the approach to adjuvant therapy has undergone significant changes over the past decade. In 2000, a consensus panel of breast-cancer experts recommended that adjuvant chemotherapy be consid-ered for most, if not all, women with invasive tumors ≥ 1 cm in size. Although the use of systemic therapy in the adjuvant setting (Table 2) reduces the risk of relapse and death due to breast cancer, a notable difference exists between hormonal therapy and chemotherapy. When hormonal therapy, tamoxifen in particular, is taken for 5 years, the overall risk of disease recurrence is decreased by almost 50%; the risk of dying from breast cancer is decreased by 25% [47]. Although these outcomes are confined primarily to patients with hormone receptor-positive disease, the clinical benefits were achieved regardless of menopausal status, nodal status, or administration of chemotherapy. The benefits resulting from chemotherapy alone are also significant; approximate reductions in risk of relapse and death are 25% and 15%, respectively [23,33-36,48]. The latter finding, however, suggests that the absolute benefit
of chemotherapy is not only smaller but also contributes modestly to the improved outcomes for many patients regardless of axillary lymph node status. Nevertheless, many patients with early breast cancer would accept drug-related toxicities to achieve the modest overall benefits [49,50].
Because the risks are not insignificant, investigators have been searching for ways to identify patients who will benefit most from chemotherapy, while enabling others to avoid cyto-toxic agents without altering their prognoses. Imprints of the first step toward realizing this goal are grounded in the finding that histologically similar breast cancer cells often display a distinct array of gene-expression patterns [51]. Furthermore, genomic analyses have elucidated a number of molecular aberrations that appear to link tumor subtypes with clinical behavior (Table 3) [52-54].
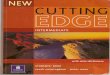
The potential of these genomic studies has been partially realized with the commercial availability of three gene-expression assays: Oncotype DX™ (Genomic Health), MammaPrint™ (Agendia BV), and H/I™ (AvariaDX). Of the three, Oncotype DX™ provides the most compelling evidence that a subset of patients – especially those with ER-positive, lymph-node-negative tumors – derive little or no benefit from adjuvant chemotherapy when compared to the use of hormonal therapy alone [55]. Some newer data also suggest this is true for patients with lymph-node-positive disease [56]. Although pre-liminary, current data are used to illustrate what may be a better approach to managing patients with early breast cancer (Figure 1). In addition, identification of the ‘triple-negative’ (i.e., ER-negative, PR-negative, and HER2-negative) subtype of breast cancers is now believed to be associated with a poorer prognosis than HER2-positive tumors.
In essence, the incriminating molecular evidence, which alleges that genomic heterogeneity is responsible for the marked variability in tumor behavior, response to treatment, and clinical outcome, may also reveal unique fingerprints that could be used to identify patients with poorer prognoses, guide selection of therapeutic interventions, and, hopefully, improve survival.
3.2 LocallyadvancedbreastcancerBy definition, locally advanced breast cancer includes all patients with stage IIIB breast cancer; however, the classification does not comprise a homogeneous disease entity. Consider for instance that ‘locally advanced’ disease could have occurred over variable periods of time; shorter for tumors with an aggressive, rapidly proliferating phenotype, longer due to neglect of indolent, slow-growing tumors. Furthermore, like the imprecise borders that render the disease inoperable, some patients with stage IIIA tumors may also embedded in the fringes of the definition.
Whereas clinical outcomes with surgery and radiation therapy were frequently discouraging, the application of neo-adjuvant chemotherapy, with the appropriate use of agents targeting the estrogen and HER2 receptors, has resulted in considerable benefit in patients who were almost certain to do poorly [55,57,58]. As this strategy not only has the potential
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y SU
NY
Ups
tate
Med
ical
Uni
vers
ity o
n 08
/16/
14Fo
r pe
rson
al u
se o
nly.

Higa
ExpertOpin.Pharmacother.(2009) 10(15) 2483
to render inoperable tumors resectable and to increase rates of breast-conserving therapy, but also to lower rates of recurrence and cancer-related deaths, the use of systemic therapy prior to surgery presumably affects a stage of disease where microme-tastasis is already present. Thus, systemic and local therapies form the combined modality approach to patients with locally advanced breast cancer. Preoperative systemic therapy also provides the clinician with a unique opportunity to assess real-time tumor response, an appraisal that cannot be performed during the course of adjuvant therapy. However, clinical
response (i.e., based on physical or radiographic examination) does not always correlate with pathologic response (residual disease found on histologic examination). It is conceivable that in the future new molecular markers may be useful as predictors of tumor response [59].
Although not as high as for patients with lower-stage disease, the 5- and 10-year DFS for patients with locally advanced breast cancer suggests that better outcomes are associated with similar prognostic factors, including nodal involvement, tumor size, growth rate, and degree of differentiation.
Table3.Breastcancersubtypesbasedongenomicanalysis.
Biochemical Genesexpression Relativeprognosis Adjuvanttherapy
‘Luminal-like’
Type A ER+ + keratin 8/18 Low cell growth-related genes (e.g., mitotic kinesin-like protein-1 etc.)
Good Hormonal alone
Type B ER+ (and possibly HER2+) + keratin 8/18
High proliferative genes (e.g., TNFR-associated factor 3; Ki-67; etc.)
Poorer compared to type A
Chemohormonal + anti-HER2 (if HER2+)
‘Basal-like’
ER-; PR-; HER2- + keratin 5/6 High proliferative genes (e.g., topoisomerase IIα; MMP7; cell division control protein 2 [CDC2]; PCNA
Poorer compared to luminal type A
Chemotherapy
HER2-positive
HER2+; ER- TGRβ1-induced anti-apoptotic factor 1; TNFr-associated factor 4; growth factor receptor-bound protein 7 etc.)
Poor Chemotherapy + anti-HER2
Primary operable breast cancer
Surgery ± radiation
Premenopausal Postmenopausal
Luminal A Luminal B Basal HER2+
Node + or – Node + or –
*Hormonal ±chemotherapy
Hormonal +chemotherapy
Node + or –
Chemotherapy +anti-HER2 (if +)
ER +
Luminal A Luminal B
Node + or –
Aromataseinhibitor ±
chemotherapy
Node + or –
Aromataseinhibitor +
chemotherapy
Basal HER2+
Node + or –
Chemotherapy +anti-HER2 (if +)
ER –ER + ER –
Figure1.Adjuvanttherapyalgorithmbasedongenomicanalyses.*Optimal hormonal therapy (i.e., tamoxifen alone, or ovarian ablation combined with either tamoxifen or an aromatase inhibitor) remains uncertain. Optimal
chemotherapy regimen not yet determined. Patient ability to tolerate treatment should be considered.
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y SU
NY
Ups
tate
Med
ical
Uni
vers
ity o
n 08
/16/
14Fo
r pe
rson
al u
se o
nly.

Breastcancer:beyondthecuttingedge
2484 ExpertOpin.Pharmacother.(2009) 10(15)
A distinct clinicopathologic disease is an entity known as inflammatory breast cancer. The appearance of spongy dermal edema and erythema plus the absence of a palpable breast mass has been mistaken for an infectious process. Interestingly, clusters of this type of breast cancer found in North Africa suggest that the disease may have a viral etiology. Although not believed to be linked to inflammatory breast cancer, the strongest evidence that viruses may play a role in the patho-genesis of breast cancer derives from reports of mouse mam-mary tumor virus (MMTV)-like antigenic reactivity, as well as the presence of sequence homology to MMTV genes in samples of human breast tumors [60]. The Epstein–Barr virus (EBV) has also been localized to tumor cells in a series of breast cancers [61]. Nevertheless, a viral etiology has never been established, in large part because of the inconsistency and variability of research findings.
Truly an inoperable disease at the time of diagnosis, objective responses can be achieved in up to 80% of patients treated with neoadjuvant chemotherapy, most of whom will then become candidates for surgical resec-tion [45,62,63]. Combined modality postsurgical treatment has resulted in a dramatic improvement in 5-year survival compared to those who do not receive any form of systemic therapy.
Because patients with locally advanced breast cancer have benefited from neoadjuvant therapy, the therapeutic strategy has also been applied to patients with early (i.e., stage I or II) breast cancer. Although the number of patients who could have breast-conserving surgery (and who would not other-wise been candidates for such a procedure) was increased, presurgical systemic therapy with doxorubicin and cyclo-phosphamide did not improve DFS and OS [64,65]. Even the addition of a third agent (i.e., docetaxel) did not impact survival outcomes [66]. However, subset analysis of patients who achieved a pathologic complete response (pCR) indicates significantly superior DFS and OS with the two- and three-drug regimens. That attaining a pCR appears to be an important predictor of survival suggests that patients with HER2-positive operable breast cancer could also benefit from preoperative systemic therapy with an agent (i.e., tras-tuzumab) targeting the receptor. Over the past 4 years, several groups have reported significantly higher pCRs in small numbers of patients who received trastuzumab as part of the treatment regimen [44,45]. These early findings were supported by results from a large Phase III clinical trial that was presented recently [46]. Compared to chemotherapy alone, patients who received chemotherapy plus trastuzumab have significantly higher pCR rates (20% vs 39%; p = 0.002) and event-free survival rates, 53% vs 70% [hazard ratio (HR) 0.56; p = 0.006]. Furthermore, in contrast to one of the early studies [44], the improved outcomes in this trial was observed in patients regardless of concomitant ER status. Although not currently approved for use in this setting, it is likely that trastuzumab will receive FDA approval as part of neoadjuvant therapy in the near future.
3.3 AdvancedbreastcancerSince 1990, the annual reduction in deaths due to breast cancer has been 2.2%; whereas the 5-year survival rates have increased by 10% over the same period of time. When the latter is analyzed by nodal status, the 5-year survival rates exceed 95% and 75% in patients with node-negative and node-positive disease, respectively [3]. Even in patients with distant metastasis (beyond the nodes), the median duration of survival has doubled from 18 to 36 months over a 20-year period ending in 2000 [67]. Depending on site of metastasis, approximately 25% of patients with metastatic disease are still alive 5 years later.
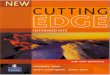
Statistics notwithstanding, breast cancer has served as a model of the (relative) success in oncology, part of which is due to the continued investment in developing effective new agents aimed at novel, and sometimes not so unique, molecular constructs in the tumor cell domain. An algorithm for the treatment of patients with metastatic breast cancer is sum-marized in Figure 2 (note the major difference between the early and advanced breast cancer algorithms is nodal involvement).
When the disease is no longer considered curable, the primary goal of therapy is maintenance or improvement of patient quality of life. However, prolongation of survival is possible with a number of systemic options (Table 4). It is important to emphasize that actual prolongation of survival may be related to factors independent of treatment, such as ER and HER2 receptor status. Furthermore, in a small subset of patients, the length of survival may also be biased by biologically more indolent tumors.
A number of caveats are noted with regard to the choice of systemic therapy. First, hormone-dependent breast cancer is not a homogeneous, all-or-nothing, entity. Thus, the mere presence of the estrogen receptor (ER) in the primary tumor does not necessarily indicate endocrine-responsiveness although hormonal therapy is usually the primary treatment modality [13]. Furthermore, response rates vary depending on tumor expres-sion of the receptors in the following descending order: ER+/PR+ > ER+/PR- > ER-/PR+ [68]. Although responses have been observed in patients with double receptor-negative tumors, hormonal intervention is not recommended in this setting. Sufficient evidence now exist to support the use of aromatase inhibitors as front-line therapy for postmenopausal women (Table 4).
Second, the timing of endocrine therapy in patients with hormone receptor-positive tumors may depend on the sites and burden of metastatic disease, as well as on patient symp-toms, performance status, and personal preferences. For example, in patients with bone-only metastasis (excluding spinal metas-tasis causing cord compression) hormonal therapy may be the initial treatment of choice; and even if chemotherapy is given first, as in patients with extensive visceral tumor involvement, hormonal therapy can be considered later.
Third, nearly all patients with hormone-responsive tumors will, inevitably, develop hormone refractory disease. Interestingly, resistance to tamoxifen, the prototypical anti-estrogen, does
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y SU
NY
Ups
tate
Med
ical
Uni
vers
ity o
n 08
/16/
14Fo
r pe
rson
al u
se o
nly.

Higa
ExpertOpin.Pharmacother.(2009) 10(15) 2485
not necessarily result from the loss of functional estrogen receptors. There is an interesting possibility that overex-pression of HER2 may mediate tumor cell escape from endocrine sensitivity.
Fourth, even in patients with extensive disease at diagnosis, other forms of therapy (i.e., radiation or surgery) may be initiated prior to systemic therapy in certain situations.
Fifth, although response rates with anthracycline- or taxane-containing chemotherapy-only regimens are generally better than other agents in the treatment of advanced breast cancer, higher responses do not necessarily translate into longer overall survival. Furthermore, single agents administered sequen-tially appear to be as good as combination therapy [69]. None of the chemotherapy regimens listed in Table 4 can be con-sidered ‘standard’ as the results of key randomized clinical trials indicate remarkable therapeutic benefits with combinations that include either capecitabine or gemcitabine [70,71].
3.4 PreventionofbreastcancerAlthough the improved survival rates and the declining mor-tality from breast cancer are noteworthy, two other statistics add another perspective to the disease. First, < 10% of all patients diagnosed with breast cancer have metastatic disease at the time of presentation; and second, approximately one-third of the patients with early-stage disease eventually relapse. Thus, these two groups will account for the patients who will ultimately succumb to the disease.
Intuitively, mortality from breast cancer will be even lower if the disease could be prevented or were altogether less common. One strategy that can reduce the risk of developing the disease, especially in women with BRCA1 and BRCA2 mutations is surgery [72,73]. Although risk reduction can be achieved with prophylactic bilateral mastectomy, some patients
have still developed breast cancer after the surgical proce-dure. Thus, although substantial, the reduction in risk is not absolute [74,75].
Three clinical studies, each based on the association between estrogens and breast cancer, have demonstrated that chemo-prevention can reduce the risk of developing invasive breast cancer in patients at high risk for the disease [76-78]. Despite these historic findings, the response to using tamoxifen or raloxifene has been tepid, often bordering on indifference. The lack of a uniform buy-in is frequently attributed to concerns about the toxicities of treatment. Tethered to this concern is the fact that large numbers of otherwise healthy women would need to be treated to reduce the incidence of a relatively small absolute number of cancers. Because the issue of routine prophylaxis for high-risk women is largely dependent on the benefits and risks of treatment, it is rea-sonable to reconsider the negative aspects of chemoprevention. First, a comparative trial between tamoxifen and raloxifene in postmenopausal women has shown that while breast cancer risk reduction is comparable, therapy with raloxifene is not associated with an increased risk of endometrial cancer [78]. It is also important to note that development of this second malignancy does not appear to be increased in premeno-pausal women treated with tamoxifen. Second, only tamox-ifen has been shown to reduce the risk of breast cancer in premenopausal women. Third, whereas most toxicities of tamoxifen occur during the period of treatment, the carry-over effect of risk-reduction benefits extends far beyond the treat-ment period [79]. In essence, the therapeutic index improves substantially with time. Fourth, genomic studies focusing on polymorphisms of CYP2D6 may have identified a subset of patients who should not be treated with tamoxifen [80-82]. This finding also suggests that high-risk patients who are
Metastatic breast cancer
Premenopausal Postmenopausal
Luminal A Luminal B Basal HER2+
*Hormonal ±chemotherapy
*Hormonal +‡chemotherapy
Chemotherapy +anti-HER2 (if +)
ER +
Luminal A Luminal B
Aromataseinhibitor ±
‡chemotherapy
Aromataseinhibitor +
chemotherapy
Basal HER2+
Chemotherapy +anti-HER2 (if +)
ER –ER + ER –
Figure2.Metastaticbreastcanceralgorithm.*Optimal hormonal therapy (i.e., tamoxifen alone or ovarian ablation combined with either tamoxifen or an aromatase inhibitor) remains uncertain. ‡Benefits from chemotherapy appear small; optimal regimen not yet determined and patient ability to tolerate treatment should be considered.
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y SU
NY
Ups
tate
Med
ical
Uni
vers
ity o
n 08
/16/
14Fo
r pe
rson
al u
se o
nly.

Breastcancer:beyondthecuttingedge
2486 ExpertOpin.Pharmacother.(2009) 10(15)
Table4.Systemictherapyformetastaticbreastcancer[170-190].
Endocrinetherapy
Therapy of choice for all patients with hormone receptor-positive tumors, small volume (i.e., bone-only or asymptomatic visceral) disease. The regimens listed are meant to be representative rather than exhaustive
Tamoxifen, 20 mg p.o. daily, ± oophorectory or LHRH agonist Front-line therapy for premenopausal women. Chemotherapy indicated only when rapid cytoreduction is desired, e.g., in patients with impending organ failure; however, concurrent administration of anti-estrogens or AIs with chemotherapy is not recommended
Anastrozole 1 mg daily, letrozole 2.5 mg daily or exemestane 25 mg daily
Front-line for postmenopausal women (tamoxifen can also considered for first-line therapy)
Chemotherapy
Because of heterogeneous tumor and host features, there is no single optimal strategy for all patients. Use of the following regimens should be guided by rational decision-making with the primary goal of palliating tumor-related symptoms. The advantages of combination regimens over single agent therapy (i.e., higher response rates, longer time to disease progression, and modest improvement in overall survival) are counterbalanced by more toxicity. The regimens listed are meant to be representative rather than exhaustive
Doxorubicin 60 mg/m2 IV (slow push) every 3 weeks Tumor outcomes comparable to single agent paclitaxel
Paclitaxel 80 mg/m2 IV over 1 h every week × 4 doses every 28 daysPaclitaxel 175 mg//m2 IV over 24 h every 3 weeks
Superior outcomes are achieved with weekly (compared to three- weekly paclitaxel given over 3 h or 24 h)Pretreat with H1 and H2 receptor antagonists
Docetaxel 100 mg/m2 IV over 1 h every 3 weeks Tumor outcomes superior to paclitaxel given every 3 weeks but with worse toxicity
Capecitabine 1250 mg/m2 twice daily, days 1 – 14 of a 21-day cycle
Active, well-tolerated oral agent. Major toxicities involve dermis (hand–food syndrome) and gastrointestinal tract (diarrhea and stomatitis)
Nab-paclitaxel 260 mg/m2 IV over 30 min every 21 days Higher response rates and time to progression compared to 3-weekly paclitaxel. No drug-related hypersensitivity reactions
Doxorubicin 60 mg/m2 IV + cyclophosphamide 600 mg/m2 IV; both agents given every 21 days
‘AC’ often considered to be the ‘control’ or ‘comparator’ regimenEpirubicin is the anthracycline more frequently used in Europe
Doxorubicin 60 mg/m2 IV + paclitaxel 175 mg/m2 IV over 3 h; both agents given every 21 days
Disease outcomes not superior to ‘AC’; more toxic than ‘AC’(Epirubicin + paclitaxel regimen used in Europe). Pretreat with H1 and H2 receptor antagonists
Doxorubicin 50 mg/m2 IV + docetaxel 75 mg/m2 IV 1 h; both agents given every 21 days
Although response rates and time to progression endpoints are better, overall survival not improved. More toxic than ‘AC’Epirubicin + docetaxel regimen used in Europe
Gemcitabine 1250 mg/m2 IV over 30 min on days 1 and 8 + paclitaxel 175 mg/m2 IV over 3 h; both agents given every 21 days
Highly active doublet; significant but manageable toxicityGemcitabine has considerable anti-tumor activity as single agentPretreat with H1 and H2 receptor antagonists
Capecitabine 1250 mg/m2 b.i.d., days 1 – 14 + docetaxel 75 mg/m2 IV over 1 h; both agents given every 21 days
Anti-tumor outcomes similar to gemcitabine + docetaxel but more toxic (attributable to the capecitabine component)
Capecitabine 1000 mg/m2 b.i.d., days 1 – 14 + ixabepilone 40 mg/m2 over 1 h: both agents given every 21 days
Highly active doublet; significant neurologic and hematopoietic toxicity in patients with liver dysfunction. Pretreat with H1 and H2 receptor antagonists. Ixabepilone has activity as a single agent
Paclitaxel 90 mg/m2 days 1, 8, 15 + bevacizumab 10 mg/kg days 1 and 15; cycles repeated every 4 weeks
Improved progression-free survival compared to paclitaxel alone; overall survival did not reach statistical significance; relatively toxic but manageable
HER2-positivedisease
Use of trastuzumab in patients with underlying cardiac disease, those who have been previously treated with an anthracycline or those receiving concurrent treatment with this class of agents is associated with an increased risk of cardiotoxicity
Trastuzumab 4 mg/kg IV over 90 min, then 2 mg/kg IV over 30 min every week
Active and well-tolerated as monotherapy.Cardiotoxic
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y SU
NY
Ups
tate
Med
ical
Uni
vers
ity o
n 08
/16/
14Fo
r pe
rson
al u
se o
nly.

Higa
ExpertOpin.Pharmacother.(2009) 10(15) 2487
apt to develop ER-positive breast cancers and, in who, the application of these agents will be most beneficial, could also be identified.
4. Pharmacologictargetsofbreastcancer
4.1 EstrogenreceptorCurrently, two different estrogen receptors have been identified, ERα and ERβ, although much less is known about signaling through the latter. Whereas isolation of the ER was crucial for understanding the hormone’s molecular mechanism of action, the discovery also became the most tangible guide for appreciating how hormone receptors could mediate tumor dependence on estrogens. Activation of ER-mediated tran-scription occurs through two separate pathways, one involving estradiol (classical genomic), and the other one that is gaining increasing attention, by growth factor receptors such as members of the Erb family (alternative non-genomic). Full activation of transcription, however, requires a large number of other molecules [83-85]. Intra-nuclear binding of the estrogen–ER complex to a portion of DNA known as the estrogen response elements results in several biologic effects, including stimula-tion of mammary gland duct growth [86]. This finding was a clue that the proliferative effect on tumor cells could also be mediated through the same receptor.
Estrogen deprivation is believed to be the operative mode of all hormonal therapies in the treatment of breast cancer. Hence, pharmacologic agents that directly or indirectly deprive tumor cells of estrogens have significantly improved tumor and health-related quality of life outcomes in patients with early and advanced breast cancer.
4.1.1 TamoxifenTamoxifen, a selective estrogen receptor modulator, or SERM, binds to ER with lower affinity than the endogenous hor-mones. The tamoxifen–ER complex then homodimerizes and translocates to the nucleus. The anti-tumor effect of
tamoxifen is believed to be mediated by two active metabolites – endoxifen and 4-hydroxytamoxifen – that inhibit co-activator binding and suppress transcription of AF-2 (hormone-dependent activation function 2). Notably, formation of these two metabolites, which is dependent on functional CYP2D6, is associated with the development of hot flashes and improved disease control [82]. Moreover, several genetic polymorphisms of CYP2D6 (i.e., alleles *3, *4, *5, and *6), as well as some members of the selective serotonin reuptake inhibitors class of drugs, have been identified that correlate with significantly reduced ability to produce the major anti-estrogenic metabolites [87-89].
The ER also has a region known as AF-1 (hormone-independent transcriptional activation function 1), which explains the agonist effects of tamoxifen, promoting a beneficial effect on bone and inducing a detrimental effect on the uterus. Tamoxifen is still the systemic hormonal therapy of choice in premenopausal women and an appropriate alternative in postmenopausal women intolerant to, or with disease pro-gressing on, aromatase inhibitors. Of interest is the molecular finding that overexpression of EGFR (epidermal growth factor receptor; HER1) and HER2 – two members of the ErbB receptor family – is associated with increased ‘cross-talk’ with the ER, which may contribute to the development of tamoxifen resistance [90-92]. This issue is discussed later.
4.1.2 Aromatase inhibitorsUnlike tamoxifen, which can be applied without regard to menopausal status, the use of armoatase inhibitors (AIs), e.g., anastrozole (Arimidex™), letrozole (Femara™), and exemestane (Aromasin™) is indicated only for the treatment of hormone-sensitive breast cancer in postmenopausal women. The reasons for this are physiological and pathological. Even though aromatase occupies the final step in the conversion of androgens to estrogens, extraordinary differences related to the regulation of enzyme synthesis and the primary site(s) of hormone production exist. While most, if not all, circulating
Trastuzumab 4 mg/kg IV over 90 min, then 2 mg/kg IV over 30 min every week + paclitaxel 175 mg/m2 IV over 3 h (paclitaxel given every 3 week)
Highly active regimen. Modest increase in risk of cardiac toxicity
Trastuzumab 4 mg/kg IV over 90 min, then 2 mg/kg IV over 30 min every week + vinorelbine 25 mg/m2 IV over 10 min every week
Highly active as first-, second- or third-line therapy. Efficacy and tolerability comparable to paclitaxel regimens. Vinorelbine dosage adjusted based on neutrophil count
Trastuzumab 4 mg/kg IV over 90 min, then 2 mg/kg IV over 30 min every week + docetaxel 35 mg/m2 IV over 1 h on weeks 1, 2, 3, 5, 6, 7 of each 8-week cycle
Active as first-line therapy. Efficacy and tolerability comparable to paclitaxel-containing regimen
Trastuzumab 6 mg/kg IV over 90 min day 1 + capecitabine 1250 mg/m2 twice daily days 1 – 4; cycle repeated every 21 days
Highly active regimen with most toxicity attributable to capecitabine
Lapatinib 1250 mg q.d. continuously + capecitabine 1000 mg/m2 twice daily, days 1 – 14; cycle repeated every 21 days
Combination superior to capecitabine alone in patients with HER2-positive disease progressing on trastuzumab. Hint of CNS activity
Table4.Systemictherapyformetastaticbreastcancer[170-190](continued).
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y SU
NY
Ups
tate
Med
ical
Uni
vers
ity o
n 08
/16/
14Fo
r pe
rson
al u
se o
nly.

Breastcancer:beyondthecuttingedge
2488 ExpertOpin.Pharmacother.(2009) 10(15)
estrogens in the postmenopausal woman are of extra-gonadal origin, approximately 80% of all estrogens are derived from the ovaries in premenopausal women. Moreover, only ovarian aromatase appears to be under the control of pituitary gonadotrophins [93]. The concern about using AIs in pre-menopausal women relates to the belief that these agents might not completely obliterate estrogen production [94]. In addition, competitive inhibition or inactivation of aromatase in women with functioning ovaries provides hypothalamic–pituitary feed-back resulting in increased release of luteinizing hormone (LH) and follicle-stimulating hormone (FSH), which might lead to the development of ovarian cysts [95]. Determination of menopause with absolute certainty is another issue and is especially problematic in patients with breast cancer who are in their fifth decade of life, as well as those in whom treatment is ongoing or has recently been completed [96]. A report discussing this dilemma was recently published and demon-strated the recovery of menses with the use of an AI in patients with biochemical confirmation of ovarian suppression [97].
Knowledge of endocrine regulation of aromatase notwith-standing, the menopausal-dependent application of AIs might still not be absolute. The recognition that AIs cause a reflex increase of gonadotrophins in patients with functioning ovaries led to translation of the concept that castration in combina-tion with an AI would not only be therapeutically feasible but also beneficial in premenopausal women with hormone-dependent breast cancer. A number of small exploratory studies utilizing a medical castration strategy (gonadotrophin-releasing hormone, GnRH, agonist) with or without an AI have been published [98-100]. All investigators reported the combination reduced serum estrogen levels to a greater degree than GnRH alone. Notably, some patients with disease progressing on GnRH alone achieved objective responses with the addition of an AI. While assessment of menopausal status is unques-tionably important, our ability to accurately determine an individual’s status by biochemical measurements alone is not as convincing as previously believed.
In postmenopausal women, the newer aromatase inhibitors have surpassed tamoxifen as the agent of choice [101]. Two points are highlighted with regard to the AIs. First, overall survival benefits (as opposed to DFS) have not, to date, been shown in most of the clinical trials; and second, the lower incidence of carcinogenic and thromboembolic events with AI therapy is partially offset by higher rates of muscular and skeletal complaints. Thus, the relegation of tamoxifen to second-line therapy may be of less significance as most patients are likely to be treated with both types of agents during the course of their disease. Emergence of this type of sequential therapy is better appreciated in the adjuvant setting (see Table 2) [102-105].
4.2 TheErbBfamilyThe ErbB family of receptor tyrosine kinases (RTK) is a homologous group that includes EGFR (HER1), HER2, HER3, and HER4. Molecularly, all members have a short
transmembrane region that connects the extracellular ligand-binding region to the intracellular kinase domain. Physiologically, the ErbB RTKs are known to contribute to the development of a number of important organs and tissue systems. In mammary tissue, each receptor has a different function in gland development. Whereas EGFR promotes ductal growth, signaling through HER2 contributes to lobuloalveolar differ-entiation and lactation [106,107]. Pathologically, there is evidence that both receptors have a role in human neoplasia. First, high levels of the EGFR and HER2 have been observed in breast cancer as well as a number of other solid tumors [108]. Second, whereas overexpression of EGFR leads to a transformed phe-notype, amplification of the HER2 oncogene or overexpression of the oncoprotein conveys tumor cell growth and survival advantages [109]. In particular, the significance of the latter, and its correlation with shortened DFS and OS was notable in two ways. First, approval of a sophisticated technique that could reliably assess HER2 oncogene amplification [110] and second, development of trastuzumab, a targeted-inhibitor of the HER2 receptor [111,112].
4.2.1 TrastuzumabTrastuzumab (Herceptin®, Genentech, Inc.) recognizes and binds with high affinity to an epitope on the extracellular domain of HER2. Notably, trastuzumab does not ‘compete’ with an endogenous ligand for the receptor binding site because none has, as yet, been identified. Nonetheless, this receptor is quite remarkable. Overexpressed in approximately 20 – 25%, of breast cancers, HER2 can form homodimers that are constitutively active, thus being able to drive tumor proliferation without an activating ligand. Success of the molecular concept in practice was realized with trastuzumab as monotherapy or in combination with chemotherapy in patients with metastatic breast cancer [113,114]. The most impor-tant data were obtained in a pivotal Phase III trial, which showed that addition of trastuzumab to chemotherapy resulted in superior outcomes compared to chemotherapy alone in all clinical endpoints, including overall survival [115].
More recently, three separate groups evaluated the use of trastuzumab in patients with early breast cancer [41-43]. Pooled results of all trials, which included nearly 10,000 patients, indicated a statistically significant improvement in DFS in favor of trastuzumab combined with adjuvant chemotherapy compared with chemotherapy alone (p < 0.0001). The HR of 0.62 [95% confidence interval (CI) 0.56 – 0.68] repre-sents a 38% lower relative risk for disease progression or death from any cause with the use of trastuzumab. These data, showing the largely indisputable benefits in DFS observed with trastuzumab treatment, could be expected to translate into a sustained long-term benefit in overall survival. This conclusion is supported by similar observations made by the Early Breast Cancer Trialists’ Collaborative Group (EBCTCG) overview [47].
Also evident from these trials was the statistically higher risk for developing class III/IV congestive heart failure when
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y SU
NY
Ups
tate
Med
ical
Uni
vers
ity o
n 08
/16/
14Fo
r pe
rson
al u
se o
nly.

Higa
ExpertOpin.Pharmacother.(2009) 10(15) 2489
trastuzumab was combined with chemotherapy, especially the anthracyclines [116-119]. Although the precise mechanism is not known, it has been speculated that contractile dysfunction may result from blocking a HER2 pathway that mediates growth and survival of cardiac smooth muscle cells [120,121]. Nevertheless, outcomes data strongly suggest that combining trastuzumab with or following chemotherapy in the adjuvant setting results in benefits unparalleled by most available thera-pies for solid tumors. Combination of trastuzumab with or following chemotherapy should be strongly considered for patients with HER2-positive early-stage breast cancer, especially those at low risk for cardiovascular morbidity.
Despite the encouraging results, it is important to emphasize that not all patients respond to trastuzumab and that meta-static disease eventually progresses despite early benefits. More-over, and except for a few retrospective reports of continued trastuzumab administration beyond first progression, no other HER2-directed therapeutic option had been available [122-125]. The effort to develop an agent that could be used in patients with disease refractory to trastuzumab depended on another unique characteristic of the target receptor. As HER2 appears to be the preferred dimeric partner of the three other members of the ErbB family, this feature may contribute to the observed receptor-associated virulence in breast tumors. The relevance of this bi-partisan coupling is two-fold. First, the function of the EGFR–HER2 heterodimers appears to be phenotypically distinct from each of their homodimers; and second, although ligand-less, the poor prognosis associated with tumors overexpressing HER2 may be due, in part, to transactivation of the intrinsically high tyrosine kinase activity of HER2 by the consorting partner.
4.2.2 LapatinibLapatinib (Tykerb®, GlaxoSmith Kline), a small molecule that functions as a competitive inhibitor of both EGFR and HER2 tyrosine kinases, has been shown to cause prolonged downregulation of tyrosine phosphorylation in tumor cells [126]. Clinical results of a pivotal Phase III trial in women with advanced, HER-positive breast cancer refractory to trastuzumab and chemotherapy showed that median time to progression (the primary study endpoint) was significantly longer in the group randomized to lapatinib plus capecitabine (a prodrug of 5-fluorouracil) than to capecitabine alone [127] Response rates were also higher in patients randomized to combination therapy. Because HER2 positivity confers a higher risk of developing brain metastasis, an equally noteworthy finding was the significantly lower incidence of disease progression in the CNS in women receiving lapatinib. A number of trials with lapatinib are currently in progress, including a ‘head-to-head’ comparison between lapatinib and trastuzumab in patients with HER2-positive, early breast cancer following completion of chemotherapy. Another interesting clinical trial may establish proof of principle regarding the ‘cross-talk’ that occurs between the estrogen receptor and HER2 [128]. Designed to test the hypothesis that estrogen deprivation
upregulates the HER2 signaling pathway, patients with ER-positive breast cancer will be randomized to receive an aromatase inhibitor with or without lapatinib.
Perhaps most intriguing are the mechanisms by which lapatinib is able to overcome trastuzumab resistance [129]. Although the answer may be partly explained by the pres-ence of EGFR, the author refers the reader to the referenced article for more details.
4.3 VascularendothelialgrowthfactorNeoplastic cells share two physiologic characteristics with normal cells: i) the absolute requirement for oxygen; and ii) the ability to adapt in response to hypoxia. The importance of oxygen in cell survival is supported not only by the develop-ment and conservation of complex respiratory and circulatory systems in all mammals, but also with the observation that no other substance, when withheld, causes death more rapidly than oxygen deprivation. Not unexpectedly, decreased cellular oxygen concentration is a potent stimulus of an adaptive response known as angiogenesis, a process characterized by new blood vessels ‘sprouting’ from existing vasculature [130].
Neovasculature formation, however, may not be solely reactive in nature, as several investigators have reported that induction of angiogenesis preceded the emergence of malig-nant tumors [131,132]. The fact that tumor dissemination, occult neoplastic deposition, and lethal cancer progression are also dependent on the formation of new blood vessels further suggests acquisition of the ability to activate angio-genesis is an inherent, and essential, part of the entire tumorigenic process.
The best characterized of the angiogenesis mediators is vascular endothelial growth factor-A or (VEGF), a pleotropic cytokine that promotes both physiologic and pathologic angiogenesis [133-135]. Of the four isoforms of the protein, VEGF121 and VEGF165 are believed to be the most important ligands for specific receptor tyrosine kinases (only VEG-FR-1/flt-1 and VEGFR-2/KDR/flk-1 are expressed preferen-tially on proliferating endothelial cells). Ligand–receptor interaction triggers a cascade of intracellular signals that affect endothelial cell proliferation, migration, permeability, and survival [136,137].
Targeting tumor vasculature is even more appealing because anti-angiogenesis therapies could overcome intrinsic tumor resistance, delay or circumvent acquired resistance to these agents, and possess broad-spectrum of anti-tumor activity. The mitogen or receptor can be pharmacologically targeted by numerous strategies. Monoclonal antibodies that recognize VEGF protein or the extracellular domain of VEGFR2 are potent suppressors of established tumor growth in preclinical models [138-140]. However, the finding that antibodies had no effect on the ex-vivo growth of breast cancer cells suggests that VEGF receptors are preferentially, although not exclu-sively, expressed on proliferating endothelial cells or a major part of the antibody’s anti-tumor effect is mediated by immune mechanisms.
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y SU
NY
Ups
tate
Med
ical
Uni
vers
ity o
n 08
/16/
14Fo
r pe
rson
al u
se o
nly.

Breastcancer:beyondthecuttingedge
2490 ExpertOpin.Pharmacother.(2009) 10(15)
4.3.1 BevacizumabBevacizumab (Avastin®, Genentec, Inc.) binds all isoforms of VEGF, preventing molecular interaction with its receptors. Based on the positive results of a Phase III study conducted in 722 patients with metastatic breast cancer, bevacizumab received accelerated approval (in combination with paclitaxel) for the treatment of patients with metastatic breast cancer [141]. In this study the risk of disease progression was decreased by 40% (HR 0.60; p < .0001) with the combination of bevaci-zumab plus paclitaxel compared to paclitaxel alone. It is empha-sized that while the median progression-free survival (PFS; the primary endpoint) was significantly longer (11.8 months) with the combination compared with paclitaxel alone (5.9 months), the secondary end point of OS did not reach statistical significance. On a cautionary note, administration of bevacizumab is associated with a higher incidence of adverse effects, some severe, including bowel perforation, delayed wound healing, hypertension, thrombosis, and bleeding.
Although other agents targeting the angiogenic pathway are currently begin tested, outcomes data suggest that efficacy in advanced breast cancer are likely to be modest, at best. It is uncertain, although possible, that inhibitors of angiogenesis may have a larger impact in breast cancer when used in the adjuvant setting.
4.4 MicrotubuleandothertargetsOur understanding of the tubulin multiplex continues to evolve, and a brief review of this critical regulatory pathway is warranted to better comprehend the purported mechanism of a number of agents used to treat breast cancer. Structurally, the basic units of the microtubule are α- and β-tubulin monomers, which heterodimerize and then elongate to form protofilaments. Interestingly, elongation of the tubulin dimers occurs along a single directional orientation with ‘negative’ α-subunits of one protofilament in contact with ‘positive’ β-subunits of another protofilament resulting in a ‘polar’ assemblage. Critical information that ensures molecular polarity is most likely inherent in the integrity of tubulin itself [142].
Perhaps one of the most striking characteristics of the microtubule are the random transitions between growth and shrinkage, a process referred to as ‘dynamic instability’. The fascinating process has a profound effect on cell morphology, motility, mitosis, and death. In contrast to the anti-microtubule effect of the vinca alkaloids, which appears to be mediated by inhibiting polymerization, in-vitro studies show that the anti-tumor activity of the taxanes and ixabepilone occurs primarily by blocking disassembly, thus kinetically ‘stabilizing’ the microtubule structure. This rather demure effect, however, is misleading because critical cellular processes are dependent on the unfettered process of microtubule dynamics.
The anti-tumor effects of the microtubule stabilizing agents appear to follow molecular ordering of two major events. First, hindrance of the transition between metaphase and anaphase by β-tubulin-bound drug creates havoc with spindle formation, resulting in mitotic arrest. Interference with mitotic
spindle function then (somehow) engages the mitochondrial apoptotic pathway, resulting in activation of multiple cell-death mechanisms [143-145].
Other ‘targets’ of cytotoxic agents frequently used in the treatment of breast cancer include topoisomerase IIα (anthracy-clines), thymidylate synthase (5-fluorouracil, capecitabine), and dihydrofolate reductase (methotrexate). Although inhibition of these enzymes appears to be the primary anti-tumor mecha-nism, it is highly conceivable that the lethal event occurs further downstream, by disrupting the balance of critical pro-teins that regulate tumor-cell survival, including members of the bcl-2 family, p53 and PTEN, or APO-1/Fas. The apparent targets are by no means trivial as the listed cytotoxic agents when used either alone or more often, in combination, are highly effective in the treatment of breast cancer.
In addition to ER and HER2, overexpression of topoi-somerase IIα might also have predictive value. Whereas ear-lier adjuvant studies showed the superiority of anthracycline-based therapy compared with CMF (cyclophosphamide, metho-trexate, and fluorouracil) in decreasing local recurrence and death, emerging data suggest that non-anthracycline, taxane-containing regimens are equally, if not more, effective. The implications of these newer findings are potentially substantial in that anthracycline therapy could be ‘tailored’ to patients with tumors that co-express HER2 and topoisomerase IIα, a subset that appears to accrue the most benefit but comprises less than 10% of all breast cancers. In addition, the applica-tion of non-anthracycline-based therapy obviates long-term toxicities to the heart and bone marrow.
5. Conclusions
Careful assessment of tumor characteristics has been instru-mental in the management of the disease. However, it is clear that cure has not been achieved in all patients with early breast cancer. Equally important, although perhaps less appreciated, is the psychological toll the disease exacts on the patient.
Society today is much more conscious about breast cancer diagnosis than it was 30 years ago. It is perhaps chilling to realize that, prior to around 1980, most patients were not told their diagnosis because of the emotional response it was thought would be evoked [146]. Women with breast cancer now have the opportunity to be intimately involved in treat-ment decisions, and they have espoused a need for ensuring that their psychosocial well-being is cared for. Commonplace fears, once fueled by the mutilating surgery and its subsequent assault on femininity and sexuality, are still present and manifested in similar ways [147,148]. In addition to the broad range of affective disorders associated with the diagnosis and surgery, cognitive deficits experienced by patients may also be caused by chemotherapy and hormonal therapy [149].
One component of the management of patients with breast cancer that impacts both physical and psychosocial outcomes is supportive care. Advances in supportive care are, at least partly, responsible for improving both types of outcome;
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y SU
NY
Ups
tate
Med
ical
Uni
vers
ity o
n 08
/16/
14Fo
r pe
rson
al u
se o
nly.

Higa
ExpertOpin.Pharmacother.(2009) 10(15) 2491
however, more efficacious anti-tumor strategies might be accompanied by additional stressors and burdens in terms of side effects and duration of therapy. A prime example relates to women with early, hormone-receptor-positive breast cancer, who are likely to receive adjuvant endocrine therapy for 5 – 10 years, of which 3 – 8 years might be with an aromatase inhibitor (AI); the negative impact of AIs on bone mineral-ization can be prevented or attenuated by adjunctive bispho-sphonate therapy [150]. More intriguing were the results from a clinical trial that adding a bisphosphonate to endocrine ther-apy significantly prolonged disease-free and relapse-free survival compared with endocrine therapy alone [151]. Although provoca-tive, these findings do not change the current standard of care as the results must be confirmed by a larger clinical trial.
6. Expertopinion
The ‘cutting edge’ in breast cancer refers to more than the minimal surgical intervention required to achieve an optimal outcome; today, the margins encompass a better understanding of the disease, which has intensified the search for features unique to individual tumors and patients. As such, the heavy investment in basic research must continue to enhance the probability that novel principles will translate into clinical benefit much like therapies aimed at blocking estrogen-, HER2-, and angiogenesis-mediated tumor growth. What appear to be at the forefront of new targets for breast cancer are agents that inhibit poly (ADP-ribose) polymerase-1 or PARP-1. Recently reported, a Phase II randomized trial indicated that patients receiving gemcitabine, carboplatin, plus a PARP-1 inhibitor as 2nd- or 3rd-line therapy for advanced triple-negative breast cancer had significantly better median PFS and OS, as well as clinical benefit rate (complete and partial responses, as well as stable disease lasting > 6 months) compared to patients treated with the chemotherapy doublet alone [152].
Other potential tumor targets that are especially promising include insulin growth factor receptor-1 (IGF-1), Src, the aurora kinases, platelet-derived growth factor (PDGF), Ras, and B-raf.
Equally important as the search for new targets, breast-cancer treatment could improve substantially by elucidating the mechanisms of resistance to drug therapy. For example, SERM resistance develops after approximately 1 year of therapy in both preclinical animal models and patients with metastatic breast cancer [153]. Besides resistance that might be mediated by ErbB receptors, an intriguing laboratory finding is that tamoxifen-resistant tumor cells apparently are ‘re-wired’ such that estrogens transduce apoptotic rather than survival signals [154]. That low-dose estrogen could actually be used to treat breast cancers that have become refractory to estrogen-deprivation strategies is counterintuitive, yet truly remarkable.
Development of drug resistance is also observed in nearly all patients with HER2-positive metastatic breast cancer who appear to become refractory within 12 months after initially
responding to trastuzumab [122]. Equally discouraging is the development of recurrent disease following adjuvant treatment with the antibody [41,42]. Determining the mechanism of resistance to anti-HER2 therapy would be beneficial in two ways: i) the development of effective alternative agents; and ii) the introduction of strategies that could prevent (or at least delay) the development of such resistance.
Although the precise explanation is not known, part of the explanation for HER2-resistance may be related to other HER family members. Thus, the consequences of receptor dimerization may be of immense oncogenic significance. Although formation of ligand-bound complexes induces receptor dimerization, heterodimers – especially HER2-containing complexes – appear to confer a more aggressive phenotype. This conclusion is supported by the coupling of HER2 with HER3. Whereas neither monomeric HER2 nor HER3 can support linear signaling alone, it is fascinating that this heterodimer has been shown to possess the most potent mitogenic and transforming properties [155]. Similarly, signaling through the EGFR–HER2 complex is more potent than either homodimer alone [156]. The latter statement is supported by the very modest clinical responses observed in breast cancer with anti-EGFR therapies, a finding that may be due to the relatively small degree of tumor dependence on EGFR alone [157-159]. However, oncogenic signaling through the functional interaction between EGFR and HER2 may be totally different. This is aptly shown in mice bearing a breast cancer xenograft that co-expressed EGFR and HER2 and the abundant heterodimers that were formed [160]. Inter-estingly, phosphorylation of two key downstream proteins can be inhibited when both receptor kinases are blocked. In addition, inhibition of EGFR with gefitinib represses heterodi-meric transactivation of HER2 in cells that also co-express both receptors [161]. Finally, inhibition of EGFR/HER2 cross-talk by targeting the EGFR kinase alone results in uncoupling of HER2/HER3 heterodimers [161]. These findings provide possible explanations for the efficacy of lapatinib in a tumor where trastuzumab had little effect.
Tumor and patient heterogeneity have resulted in improved clinical outcomes (i.e., increased antitumor effect and decreased toxicity) by personalizing cancer care. Also inherent in this evolutionary concept is the unique opportunity to improve the economic consequences associated with the management of patients with breast cancer. This, however, will require: i) identification of predictive biomarkers to guide the appli-cation of targeted agents as well as traditional chemo-therapy (of note, although the ER and HER2 are predictive of response, not all patients respond to therapies directed at these receptors and even less is known about chemotherapy; moreover, no predictive biomarker has been identified for anti-angiogenic therapy); ii) determination of the optimal biologic dose that results in complete and selective target inhibition; iii) recognition of appropriate clinical trial endpoints that reflect drug efficacy; and iv) conservation of objective perspectives because targeting the obvious, the
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y SU
NY
Ups
tate
Med
ical
Uni
vers
ity o
n 08
/16/
14Fo
r pe
rson
al u
se o
nly.

Breastcancer:beyondthecuttingedge
2492 ExpertOpin.Pharmacother.(2009) 10(15)
aberrant molecules, may be a masterful diversion of tumor cells (i.e., this notion is exemplified by the anti-tumor effect achieved by inhibiting the 26S proteasome, an essential component of cell metabolism that retards tumor progression by interfering with the orderly degradation of normal, key regulatory molecules).
The oncology community awaits another wave of conceptual discoveries that could translate into ground-breaking clinical
trials and new treatment paradigms. The mantra in breast cancer will remain a cure; and instead of genes and dreams, perhaps one day it will be a certain reality.
Declarationofinterest
The author states no conflict of interest and has received no payment in preparation of this manuscript.
BibliographyPapers of special note have been highlighted as either of interest (•) or of considerable interest (••) to readers.
1. Deapen D, Liu L, Perkins C, et al. Rapidly rising breast cancer incidence rates among Asian-American women. Int J Cancer 2002;99:747-50
2. Lee J, Demissie K, Lu SE, Rhoads GG. Cancer incidence among Korean-American immigrants in the United States and native Koreans in South Korea. Cancer Control 2007;14:78-85
3. Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2008. CA Cancer J Clin 2008;58:71-96
4. Vogel VG. Epidemiology of breast cancer. In: Winchester DJ, Winchester DP, Hudis CA, Northon L, editors, Breast Cancer, 2nd edition. Hamilton, Ontario, BC Decker, 2006. p. 47-60
5. Collaborative Group on Hormonal Factors in Breast Cancer. Familial breast cancer: collaborative reanalysis of individual data from 52 epidemiological studies including 58,209 women with breast cancer and 101,986 women without the disease. Lancet 2001;358:1389-99
6. Edwards BK, Brown ML, Wingo PA, et al. Annual report to the nation on the status of cancer, 1975-2002, featuring population-based trends in cancer treatment. J Natl Cancer Inst 2005;97:1407-27
7. Ries LAG, Kosary CL, Hankey BF, et al. SEER Cancer Statistics Review, 1973-1996. Bethesda, MD: National Cancer Institute, 1999
8. Podhajcer OL, Bravo AI, Dain L, et al. In vitro analysis of the cellular proliferative response to 17-beta-estradiol of human breast cancer. Cancer 1988;61:1807-12
9. Phipps AI, Malone KE, Porter PL, et al. Reproductive and hormonal risk factors for postmenopausal luminal,
HER-2-overexpressing, and triple-negative breast cancer. Cancer 2008;113:1521-626
10. Friebel TM, Domchek SM, Neuhausen SL, et al. Bilateral prophylactic oophorectomy and bilateral prophylactic mastectomy in a prospective cohort of unaffected BRCA1 and BRCA2 mutation carriers. Clin Breast Cancer 2007;7:875-82
11. Gotlieb WH, Barchana M, Ben-Baruch G, Friedman E. Malignancies following bilateral salpingo-oophorectomy (BSO). Eur J Surg Oncol 2006;32:1231-4
12. Kauff ND, Domchek SM, Friebel TM, et al. Risk-reduction salpingo-oophorectomy for the prevention of BRCA1- and BRCA2-associated breast and gynecologic cancer: a multicenter, prospective study. J Clin Oncol 2008;26:1331-7
13. Jordan C. Historical perspective on hormonal therapy of advanced breast cancer. Clin Ther 2002;24(Suppl A):3-16
• Succinctpaperwrittenbypre-eminentscientist.
14. Easton DF, Bishop DT, Ford D, Crockford GP. Genetic linkage analysis in familial breast and ovarian cancer: results from 214 families. The Breast Cancer Linkage Consortium. Am J Hum Genet 1993;52:678-701
15. Wooster R, Neuhausen SL, Mangion J, et al. Localization of a breast cancer susceptibility gene, BRCA2, to chromosome 13q12-13. Science 1994;265:2088-90
16. Easton DF. How many more breast cancer predisposition genes are there? Breast Cancer Res 1999;1:14-7
17. Easton DF, Poole KA, Dunning AM, et al. Genome-wide association study identifies novel breast cancer susceptibility loci. Nature 2007;447:1087-93
18. Hunter DJ, Draft P, Jacobs KB, et al. A genome-wide association study identifies alleles in FGFR2 associated with risk of sporadic postmenopausal breast cancer. Nat Genet 2007;39:870-4
19. Stacey SN, Manolescu A, Sulem P, et al. Common variants on chromosomes 2q35 and 16q12 confer susceptibility to estrogen receptor-positive breast cancer. Nat Genet 2007;39:865-9
20. Madigan MP, Ziegler RG, Benichou J, et al. Proportion of breast cancer cases in the United States explained by well-established risk factors. J Natl Cancer Inst 1995;87:1681-5
21. Olsen O, Gotzsche PC. Cochrane review on screening for breast cancer with mammography. Lancet 2001;358:1340-2
• Provocativepaperprovidinginsightsintothevalueofmammography.
22. U.S. Preventive Services Task Force Genetic risk assessment and BRCA mutation testing for breast and ovarian cancer susceptibility: recommendation statement. Ann Intern Med 2005;143:355-61
23. Fletcher SW, Black W, Harris R, et al. Report of the international workshop on screening for breast cancer. J Natl Cancer Inst 1993;85:1644-56
24. Fisher B, Redmond C, Fisher ER, et al. Ten-year results of a randomized clinical trial comparing radical mastectomy and total mastectomy with or without radiation. N Engl J Med 1985;312:674-81
• Groundbreakingclinicaltrialthatchangedatreatmentstrategy.
25. Fisher B, Anderson S, Redmond CK, et al. Re-analysis and results after 12 years of follow-up in a randomized clinical trial comparing total mastectomy with lumpectomy with or without irradiation in the treatment of breast cancer. N Engl J Med 1995;333:1456-61
• Follow-uppaperconfirmingtheclinicalapplicationoflessaggressivesurgery.
26. Jacobson JA, Danforth DN, Cowan KH, et al. Ten-year results of a comparison of conservation with mastectomy in the treatment of stage I and II breast cancer. N Engl J Med 1995;332:907-11
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y SU
NY
Ups
tate
Med
ical
Uni
vers
ity o
n 08
/16/
14Fo
r pe
rson
al u
se o
nly.

Higa
ExpertOpin.Pharmacother.(2009) 10(15) 2493
27. Veronesi U, Salvadori B, Luini A, et al. Breast conservation is a safe method in patients with small cancer of the breast. Long-term results of three randomized trials on 1,973 patients. Eur J Cancer 1995;31A:1574-9
28. Beatson GT. On the treatment of inoperable cases of carcinoma of the mamma: suggestions for a new method of treatment with illustrative cases. Lancet 1896;2:104-7
29. Diab SG, Elledge RM, Clark GM. Tumor characteristics and clinical outcome of elderly women with breast cancer. J Natl Cancer Inst 2000;92:550-6
30. Axwlsson C, Mouridsen H, Sedeler K, et al. Axillary dissection of level I and II lymph nodes is important in breast cancer classification. Eur J Cancer 1992;28A:1415-8
31. Krag D, Weaver D, Ashikaga T, et al. The sentinel node in breast cancer: a multicenter validation study. N Engl J Med 1998;337:941-6
• Sentinelpaperthatsupportingachange inmanagementstrategy.
32. Veronesi U, Paganelli G, Vitale G, et al. Sentinel lymph node biopsy and axillary dissection for breast cancer: results in a large series. J Natl Cancer Inst 1999;91:368-73
33. Early Breast Cancer Trialists’ Collaborative Group. Effects of radiotherapy and surgery in early breast cancer: an overview of the randomized trials. N Engl J Med 1995;333:1444-55
34. Fisher B, Brown AM, Dimitrov NV, et al. Two months of doxorubicin-cyclophosphamide with and without interval reinduction therapy compared with 6 months of cyclophosphamide, methotrexate, and fluorouracil in positive-node breast cancer patients with tamoxifen-nonresponsive tumors: results from the national surgical adjuvant breast and bowel project B-15. J Clin Oncol 1990;8:1483-96
35. Fisher B, Redmond C, Dimitrov NV, et al. A randomized clinical trial evaluating sequential methotrexate and fluorouracil in the treatment of patients with node-negative breast cancer who have estrogen receptor-negative tumors. N Engl J Med 1989;320:479-84
36. Mansour EG, Gray R, Shatila AH, et al. Efficacy of adjuvant chemotherapy in high-risk node-negative breast cancer.
An intergroup study. N Engl J Med 1989;320:485-90
37. Early Breast Cancer Trialists’ Collaborative Group (EBCTCG). Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet 2005;365:1687-717
38. Henderson IC, Berry DA, Demetri GD, et al. Improved outcomes from adding sequential paclitaxel but not from escalating doxorubicin dose in an adjuvant chemotherapy regimen for patients with node-positive primary breast cancer. J Clin Oncol 2003;21:976-83
39. Mamaounas EP, Bryant J, Lembersky B, et al. Paclitaxel after doxorubicin plus cyclophosphamide as adjuvant chemotherapy for node-positive breast cancer. Results from NSABP B-28. J Clin Oncol 2005;23:3686-96
40. Winer E, Hudis C, Burstein H, et al. American Society of Clinical Oncology technology assessment on the use of aromatase inhibitors as adjuvant therapy for postmenopausal women with hormone receptor-positive breast cancer: status report 2004. J Clin Oncol 2005;23:619-29
41. Romond EH, Perez EA, Bryant J, et al. Trastuzumab plus adjuvant chemotherapy for operable HER2-positive breast cancer. N Engl J Med 2005;353:1673-84
• Historicclinicaltrialthatchangedachangeintreatmentstandard.
42. Piccart-Gebhart MJ, Procter M, Leyland-Jones B, et al. Trastuzumab after adjuvant chemotherapy in HER2-positive breast cancer. N Engl J Med 2005;353:1659-72
• Historicclinicaltrialthatchangedachangeintreatmentstandard.
43. Slamon D, Eiermann W, Robert NJ, et al. BCIRG 006: 2nd interim analysis phase III randomized trial comparing doxorubicin and cyclophosphamide followed by docetaxel with doxorubicin and cyclophosphamide followed by docetaxel and trastuzumab with docetaxel, carboplatin and trastuzumab in Her2/neu-positive early breast cancer patients. Presented at the 2006 San Antonio Breast Cancer Symposium; December 14–17, 2006; San Antonio, Texas
44. Buzdar AU, Ibrahim NK, Francis D, et al. Significantly higher pathologic complete
remission rate after neoadjuvant therapy with trastuzumab, paclitaxel, and epirubicin chemotherapy: results of a randomized trial in human epidermal growth factor receptor 2-positive operable breast cancer. J Clin Oncol 2005;23:3676-85
45. Coudert BP, Arnould L, Moreau L, et al. Pre-operative systemic (neo-adjuvant therapy with trastuzumab and docetaxel for HER2-overexpressing stage II or III breast cancer: results of a multicenter phase II trial. Ann Oncol 2006;17:409-14
46. Gianni L, Eiermann W, Semiglazov V, et al. Neoadjuvant trastuzumab in patients with HER2-positive locally advanced breast cancer: primary efficacy analysis of the NOAH trial. Presented at 31st annual San Antonio breast cancer symposium: abstract 31, December 12, 2008
47. Early Breast Cancer Trialists’ Collaborative Group. Tamoxifen for early breast cancer: an overview of the randomised trials. Lancet 1998;351:1451-67
• Meta-analysiswithprofounddatabaseandimplications.
48. Early Breast Cancer Trialists’ Collaborative Group. Polychemotherapy for early breast cancer: an overview of the randomised trials. Lancet 1998;352:930-42
49. Ravdin PM, Siminoff IA, Harvey JA. Survey of breast cancer patients concerning their knowledge and expectations of adjuvant therapy. J Clin Oncol 1998;16:515-21
50. Lindley C, Vasa S, Sawyer WT, Winer EP. Quality of life and preferences for treatment following systemic adjuvant therapy for early stage breast cancer. J Clin Oncol 1998;16:380-7
51. van de vijver MJ, He YD, van’t Veer L, et al. A gene-expression signature as a predictor of survival in breast cancer. N Engl J Med 2002;347:1999-2009
52. Sotiriou C, Neo S, McShane L, et al. Breast cancer classification and prognosis based on gene expression profiles from a population based study. Proc Natl Acad Sci USA 2003;100:10393-8
53. Perou C, Sorlie T, Eisin M, et al. Molecular portraits of human breast tumours. Nature 2000;406:747-52
54. Sorlie T, Perou C. Tibshirani R, et al. Gene expression patterns of breast carcinomas distinguish tumor subclasses with clinical implications. Proc Natl Acad Sci USA 2001;98:10869-74
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y SU
NY
Ups
tate
Med
ical
Uni
vers
ity o
n 08
/16/
14Fo
r pe
rson
al u
se o
nly.

Breastcancer:beyondthecuttingedge
2494 ExpertOpin.Pharmacother.(2009) 10(15)
55. Paik S, Tang G, Shak S, et al. Gene expression and benefit of chemotherapy in women with node-negative, estrogen receptor-positive breast cancer. J Clin Oncol 2006;24:3726-34
• Novelfindingswithsignificantclinicalimplications.
56. Albain K, Barlow W, Shak S, et al. Prognostic and predictive value of the 21-gene recurrence score assay in postmenopausal, node-positive, ER-positive breast cancer (S8814, INT0100) (abstr 10). Program and abstracts of the 30th annual San Antonio breast cancer symposium, Dec 13 – 16, 2007
57. Burstein HJ, Harris LN, Gleman R, et al. Preoperative therapy with trastuzumab and paclitaxel followed by sequential adjuvant doxorubicin/cyclophosphamide for HER2- overexpressing stage II or III breast cancer: a pilot study. J Clin Oncol 2003;21:46-53
58. Arnould L, Arveux P, Couturier J, et al. Pathological complete response to trastuzumab-based neoadjuvant therapy is related to the level of HER-2 amplification. Clin Cancer Res 2007;13:6404-9
59. Yagata H, Nakamura S, Toi M, et al. Evaluation of circulating tumor cells in patients with breast cancer: multi-institutional clinical trial in Japan. Int J Clin Oncol 2008;13:252-6
60. May FEB, Westley BR. Characterization of sequences related to the mouse mammary tumor virus that are specific to MCF-7 breast cancer cells. Cancer Res 1989;49:3879-83
61. Labrecque LG, Barnes DM, Fentiman IS, Griffin BE. Epstein-Barr virus in epithelial cell tumors: a breast cancer study. Cancer Res 1995;55:39-45
62. Chang S, Parker SL, Pham T, et al. Inflammatory breast carcinoma incidence and survival: the surveillance, epidemiology, and end results program of the National Cancer Institute, 1975-1992. Cancer 1998;82:2366-72
63. Ueno NT, Buzdar AU, Singletary SE, et al. Combined-modality treatment of inflammatory breast carcinoma: twenty years of experience at M.D. Anderson cancer center. Cancer Chemother Pharmacol 1997;40:321-9
64. Fisher B, Brown A, Mamounas E, et al. Effect of preoperative chemotherapy on local-regional disease in women with
operable breast cancer: findings from national surgical adjuvant breast and bowel project B-18. J Clin Oncol 1997;15:2483-93
65. Fisher B, Bryant J, Wolmark N, et al. Effect of preoperative chemotherapy on the outcome of women with operable breast cancer. J Clin Oncol 1998;16:2672-85
66. Rastogi P, Anderson SJ, Bear HD, et al. Preoperative chemotherapy: updates of national surgical adjuvant breast and bowel project protocols B-18 and B-27. J Clin Oncol 2008;26:778-85
67. Moulder S, Hortobagyi GN. Advances in the treatment of breast cancer. Clin Pharmacol Ther 2008;83:26-36
68. Osborne CK. Tamoxifen in the treatment of breast cancer. N Engl J Med 1998;339:1609-18
69. Sledge GW, Neuberg D, Bernardo P, et al. Phase III trial of doxorubicin, paclitaxel, and the combination of doxorubicin and paclitaxel as front-line chemotherapy for metastatic breast cancer; an intergroup trial (E1193). J Clin Oncol 2003;21:588-92
70. O’Shaughnessy J, Miles D, Vukelja S, et al. Superior survival with capecitabine plus docetaxel combination therapy in anthracycline-pretreated patients with advanced breast cancer: phase III trial results. J Clin Oncol 2002;20:2812-23
71. Albain KS, Nag SM, Calderillo-Ruiz G, et al. Gemcitabine plus paclitaxel versus paclitaxel monotherapy in patients with metastatic breast cancer and prior anthracycline treatment. J Clin Oncol 2008;26:3950-7
72. Kauff ND, Domchek SM, Friebel TM, et al. Risk-reduction salpingo-oophorectomy for the prevention of BRCA1- and BRCA2-associated breast and gynecologic cancer: a multicenter, prospective study. J Clin Oncol 2008;26:1331-7
73. Friebel TM, Domchek SM, Neuhausen SL, et al. Bilateral prophylactic oophorectomy and bilateral prophylactic mastectomy in a prospective cohort of unaffected BRCA1 and BRCA2 mutation carriers. Clin Breast Cancer 2007;7:875-82
74. Hartmann LC, Sellers TA, Schaid DJ, et al. Efficacy of bilateral prophylactic mastectomy in BRCA1 and BRCA2 gene mutation carriers. J Natl Cancer Inst 2001;93:1633-7
75. Meijers-Heijboer H, van Geel B, van Putten WLJ, et al. Breast cancer
after prophylactic bilateral mastectomy in women with a BRCA1 or BRCA2 mutation. N Engl J Med 2001;345:159-64
76. Fisher B, Costantino JP, Wickerham DL, et al. Tamoxifen for prevention of breast cancer: report of the National Surgical Adjuvant Breast and Bowel Project P-1 Study. J Natl Cancer Inst 1998;90:1371-88
• Historicclinicaltrialwithsignificantclinicalimplications.
77. Vogel GV, Costantino JP, Wickerham DL, et al. Effects of tamoxifen vs. raloxifene on the risk of developing invasive breast cancer and other disease outcomes: the NSABP study of tamoxifen and raloxifene (STAR) P-2 trial. JAMA 2006;295:2727-41
• Historicclinicaltrialwithsignificantclinicalimplications.
78. Cuzick J, Forbes J, Edwards R, et al. First results from the International Breast Cancer Intervention Study (IBIS-1): a randomised prevention trial. Lancet 2002;360:817-24
79. Cuzick J, Forbes J, Sestak I, et al. Long-term results of tamoxifen prophylaxis for breast cancer-96 month follow-up of the randomised IBIS-I study. J Natl Cancer Inst 2007;99:272-82
80. Lim H-S, Lee HJ, Lee ES, et al. Clinical implications of CYP2D6 genotypes predictive of tamoxifen pharmacokinetics in metastatic breast cancer. J Clin Oncol 2007;25:3837-45
81. Bonanni B, Macis D, Maisonneuve P, et al. Polymorphism in the CYP2D6 tamoxifen-metabolizing gene influences clinical effect but not hot flashes. Data from the Italian tamoxifen trial. J Clin Oncol 2006;24:3708-9
82. Goetz MP, Rae JM, Suman VJ, et al. Pharmacogenetics of tamoxifen biotransformation is associated with clinical outcomes of efficacy and hot flashes. J Clin Oncol 2005;23:9312-8
83. Kato S, Endoh H, Masuhiro Y, et al. Activation of the estrogen receptor through phosphorylation by mitogen-activated protein kinase. Science 1995;270:1491-4
84. McInerney EM, Tsai MJ, O’Malley BW, Katzenellenbogen BS. Analysis of estrogen receptor transcriptional enhancement by a nuclear hormone receptor coactivator. Proc Natl Acad Sci USA 1996;93:10069-73
85. Kushner PJ, Agard DA, Greene GL, et al. Estrogen receptor pathways to AP-1. J Steroid Biochem Mol Biol 2000;74:311-7
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y SU
NY
Ups
tate
Med
ical
Uni
vers
ity o
n 08
/16/
14Fo
r pe
rson
al u
se o
nly.

Higa
ExpertOpin.Pharmacother.(2009) 10(15) 2495
86. Lippman ME, Dickson RB. Growth control of normal and malignant breast epithelium. Prog Clin Biol Res 1990;354:147-78
87. Sachse C, Brockmoller J, Bauer S, Roots I. Cytochrome P450 2D6 variants in a Caucasian population: allele frequencies and phenotypic consequence. Am J Hum Genet 1997;60:284-95
88. Stearns V, Johnson MD, Rae JM, et al. Active tamoxifen metabolite plasma concentrations after co-administration of tamoxifen and the selective serotonin reuptake inhibitor paroxetine. J Natl Cancer Inst 2003;95:1758-64
89. Jin Y, Desta Z, Stearns V, et al. CYP2D6 genotype, antidepressant use, and tamoxifen metabolism during adjuvant breast cancer treatment. J Natl Cancer Inst 2005;97:30-9
90. Guiterrez MC, Detre S, Johnston S, et al. Molecular changes in tamoxifen-resistant breast cancer: relationship between estrogen receptor, HER-2 and p38 mitogen-activated protein kinase. J Clin Oncol 2005;23:2469-76
91. Kurebayashi J, Okubo S, Yamamoto Y, et al. Inhibition of HER1 signaling pathway enhances antitumor effect of endocrine therapy in breast cancer. Breast Cancer 2004;11:38-41
92. Pietras RJ, Arboleda J, Reese DM, et al. HER-2 tyrosine kinase pathway targets estrogen receptor and promotes hormone-independent growth in human breast cancer cells. Oncogene 1995;10:2435-46
93. Bulun SE, Simpson E. Regulation of aromatase expression in human tissues. Breast Cancer Res Treat 1994;30:19-29
94. Wander HE, Blossey HC, Nagel GA. Aminoglutethimide in the treatment of premenopausal patients with metastatic breast cancer. Eur J Clin Oncol 1986;22:1371-4
95. Kramer S, Leeker M, Jager W. Gonadotropin levels in ovarian cyst fluids: a predictor of malignancy? Int J Biol Markers 1998;13:165-8
96. Bines J, Oleske DM, Cobleigh MA. Ovarian function in premenopausal women treated with adjuvant chemotherapy for breast cancer. J Clin Oncol 1996;14:1718-29
97. Smith IE, Dowsett M, Yap Y-S, et al. Adjuvant aromatase inhibitors for early breast cancer after chemotherapy-induced
amenorrhaea: caution and suggested guidelines. J Clin Oncol 2006;16:2444-7
98. Forward DP, Cheung KL, Jackson L, Robertson JFR. Clinical and endocrine data for goserelin plus anastrozole as second-line endocrine therapy for premenopausal advanced breast cancer. Br J Cancer 2004;90:590-4
99. Stein RC, Dowsett M, Hedley A, et al. The clinical and endocrine effects of 4-hydroxyandrostenedione alone and in combination with goserelin in premenopausal women with advanced breast cancer. Br J Cancer 1990;62:679-83
100. Celio L, Martinetti A, Ferrari L. Premenopausal breast cancer patients treated with a gonadrotropin-releasing hormone analog alone or in combination with an aromatase inhibitor: a comparative endocrine study. Anticancer Res 1999;19:2261-8
101. Mauri D, Pavlidis N, Polyzos NP, et al. Survival with aromatase inhibitors and inactivators versus standard hormonal therapy in advanced breast cancer: meta-analysis. J Natl Cancer Inst 2006;98:1285-91
102. Jonat W, Gnant M, Boccardo F, et al. Effectiveness of switching from adjuvant tamoxifen to anastrozole in postmenopausal women with hormone-sensitive early-stage breast cancer: a meta-analysis. Lancet Oncol 2006;7:991-6
103. The Breast International Group (BIG) I-98 Collaborative Group. A comparison of letrozole and tamoxifen in postmenopausal women with early breast cancer. N Engl J Med 2005;353:2747-57
• Historicclinicaltrialthatchangedsupportedachangeintreatmentstandard.
104. Goss PE, Ingle JN, Martino S, et al. Randomized trial of letrozole following tamoxifen as extended adjuvant therapy in receptor-positive breast cancer: updated findings from NCIC CTG MA.17. J Natl Cancer Inst 2005;97:1262-71
• Historicclinicaltrialthatchangedsupportedachangeintreatmentstandard.
105. Coombes RC, Hall E, Gibson LJ, et al. A randomized trial of exemestane after two to three years of tamoxifen therapy in postmenopausal women with primary breast cancer. N Engl J Med 2004;350:1081-92
106. Jones FE, Stern DF. Expression of dominant-negative ErbB2 in the
mammary gland of transgenic mice reveals a role in lobuloalveolar development and lactation. Oncogene 1999;18:3481-90
107. Jones FE, Welte T, Fu XY, Stern DF. ErbB4 signaling in the mammary gland is required for lobuloalveolar development and Stat5 activation during lactation. J Cell Biol 1999;147:77-87
108. Harris AL, Nicholson S, Sainsbury R, et al. Epidermal growth factor receptor and other oncogenes as prognostic markers. Natl Cancer Inst Monogr 1992;11:181-7
109. Di Marco E, Pierce JH, Fleming TP, et al. Autocrine interaction between TGF alpha and the EGF-receptor: quantitative requirements for induction of the malignant phenotype. Oncogene 1989;4:831-8
110. Press MF, Bernstein L, Thomas PA, et al. HER-2/neu gene amplification characterized by fluorescence in situ hybridization: poor prognosis in node-negative breast carcinomas. J Clin Oncol 1997;15:2894-904
111. Slamon DJ, Clark GM, Wong SG, et al. Human breast cancer: correlation of relapse and survival with amplification of the HER-2/neu oncogene. Science 1987;235:177-82
112. Seshadri R, Firgaira FA, Horsfall DJ, et al. Clinical significance of HER-2/neu oncogene amplification in primary breast cancer. The South Australian Breast Cancer Study Group. J Clin Oncol 1993;11:1936-42
113. Vogel CL, Cobleigh MA, Tripathy D, et al. Efficacy and safety of trastuzumab as a single agent in first-line treatment of HER2-overexpressing metastatic breast cancer. J Clin Oncol 2002;20:719-26
114. Burstein HJ, Harris LN, Marcom PK, et al. Trastuzumab and vinorelbine as first-line therapy for HER2-overexpressing metastatic breast cancer: multicenter phase II trial with clinical outcomes, analysis of serum tumor markers as predictive factors, and cardiac surveillance algorithm. J Clin Oncol 2003;21:2889-95
115. Slamon DJ, Leyland-Jones B, Shak S, et al. Use of chemotherapy plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2. N Engl J Med 2001;344:783-92
• Historicclinicaltrialprovidingproof ofconcept.
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y SU
NY
Ups
tate
Med
ical
Uni
vers
ity o
n 08
/16/
14Fo
r pe
rson
al u
se o
nly.

Breastcancer:beyondthecuttingedge
2496 ExpertOpin.Pharmacother.(2009) 10(15)
116. Hind D, Pilgrim H, Ward S. Questions about adjuvant trastuzumab still remain. Lancet 2007;369:3-5
117. Perez EA, Suman VJ, Davidson NE, et al. Interim cardiac safety analysis of NCCTG N9831 Intergroup adjuvant trastuzumab trial. J Clin Oncol 2005;23:abstract 556
118. Tan-Chiu E, Yothers G, Romond E, et al. Assessment of cardiac dysfunction in a randomized trial comparing doxorubicin and cyclophosphamide followed by paclitaxel, with or without trastuzumab as adjuvant therapy in node-positive, human epidermal growth factor receptor 2-overexpressing breast cancer: NSABP B-31. J Clin Oncol 2005;23:7811-9
119. Geyer CE Jr, Bryant JL, Romond EH, et al. Update of cardiac dysfunction on NSABP B-31, a randomized trial of sequential doxorubicin/cyclophosphamide (AC) paclitaxel (T) vs. AC T with trastuzumab (H). J Clin Oncol 2006;24:abstract 581
120. Zhao Y, Sawyer DR, Baliga RR, et al. Neuregulins promote survival and growth of cardiac myocytes. J Biol Chem 1998;273:10261-9
121. Sawyer DB, Zuppinger C, Miller TA, et al. Modulation of anthracycline-induced myofibrillar disarray in rat ventricular myocytes by neuregulin-1β and anti-erbB2: potential mechanism for trastuzumab-induced cardiotoxicity. Circulation 2002;105:1551-4
122. Montemurro F, Donadio M, Clavarezza M, et al. Outcome of patients with HER2-positive advanced breast cancer progressing during trastuzumab-based therapy. Oncologist 2006;11:318-24
123. Bartsch R, Wenzel C, Hussian D, et al. Analysis of trastuzumab and chemotherapy in advanced breast cancer after the failure of at least one earlier combination: an observational study. BMC Cancer 2006;6:63-8
124. Garcia-Saenz JA, Martin M, Puente J, et al. Trastuzumab associated with successive cytotoxic therapies beyond disease progression in metastatic breast cancer. Clin Breast Cancer 2005;6:325-9
125. Gelmon KA, Mackey J, Verma S, et al. Use of trastuzumab beyond disease progression: observations from a retrospective review of case histories. Clin Breast Cancer 2004;5:52-8
126. Wood ER, Truesdale AT, McDonald OB, et al. A unique structure for epidermal
growth factor receptor bound to GW572016 (lapatinib): relationships among protein conformation, inhibitor off-rate, and receptor activity in tumor cells. Cancer Res 2004;64:6652-9
127. Geyer CE, Forster J, Lindquist D, et al. Lapatinib plus capecitabine for HER2-positive advanced breast cancer. N Engl J Med 2006;355:2733-43
128. Shou J, Massarweh S, Osborne CK, et al. Mechanisms of tamoxifen resistance: increased estrogen receptor-HER2/neu crosstalk in ER/HER2-posivitive breast cancer. J Natl Cancer Inst 2004;96:926-35
129. Higa GM, Abraham J. Lapatinib in the treatment of breast cancer. Expert Rev Anticancer Ther 2007;7:1183-92
130. Gimbrone MA, Leapman SB, Cotran RS, Folkman J. Tumor dormancy in vivo by prevention of neovascularization. J Exp Med 1972;136:261-76
131. Skobe M, Rockwell P, Goldstein N, et al. Halting angiogenesis suppresses carcinoma cell invasion. Nat Med 1997;3:1222-7
132. Christofori G, Hanahan D. Molecular dissection of multistage tumorigenesis in transgenic mice. Semin Cancer Biol 1994;5:3-21
133. Rak J, Mitsuhashi Y, Sheehan C, et al. Oncogenes and tumor angiogenesis: differential modes of vascular endothelial growth factor upregulation in ras-transformed epithelial cells and fibroblasts. Cancer Res 2000;60:490-8
134. Viloria Petit AM, Rak J, Hung M-C, et al. Neutralizing antibodies against epidermal growth factor and erbB-2/neu receptor tyrosine kinases down-regulate vascular endothelial growth factor production by tumor cells in vitro and in vivo. Am J Pathol 1997;151:1523-30
135. Wang D, Su Huang H-J, Kazlauskas A, Cavenee WK. Induction of vascular endothelial growth factor expression in endothelial cells by platelet-derived growth factor through the activation of phosphatidylinositol 3-kinase. Cancer Res 1999;59:1464-72
136. Pidgeon GP, Barr MP, Harmey JH, et al. Vascular endothelial growth factor (VEGF) upregulates bcl-2 and inhibits apoptosis in human and murine mammary adenocarcinoma cells. Br J Cancer 2001;85:273-8
137. Katoh O, Takahashi T, Oguri T, et al. Vascular endothelial growth factor inhibits
apoptotic death in hematopoietic cells after exposure to chemotherapeutic drugs by inducing MCL1 acting as an antiapoptotic factor. Cancer Res 1998;58:5565-9
138. Yokota A, Asano M, Okamoto T, et al. Suppression of ascites formation and re-accumulation associated with human ovarian cancer by anti-VPF monoclonal antibody in vivo. Anti Cancer Res 2000;20:155-60
139. Fong TA, Shawver LK, Sun L, et al. SU5416 is a potent and selective inhibitor of the vascular endothelial growth factor receptor (flk/kdr) that inhibits tyrosine kinase catalysis, tumour vascularisation and growth of multiple tumour types. Cancer Res 1999;59:99-106
140. Prewett M, Huber J, Li Y, et al. Antivascular endothelial growth factor receptor (fetal liver kinase 1) monoclonal antibody inhibits tumour angiogenesis and growth of several mouse and human tumors. Cancer Res 1999;59:5209-18
141. Miller K, Wang M, Gralow J, et al. Paclitaxel plus bevacizumab versus paclitaxel alone for metastatic breast cancer. N Engl J Med 2007;357:2666-76
142. McIntosh JR. The role of microtubules in chromosome movement. In: Hyams JS, Lloyd CW, editors, Microtubules, Wiley-Liss, Inc., New York, USA, 1994. p. 413-434
143. Wang TH, Wang HS, Soong YK. Paclitaxel-induced cell death: where the cell cycle and apoptosis come together. Cancer 2000;88:2619-28
144. Donaldson KL, Goolsby G, Kiener PA, Wahl AF. Activation of p34cdc2 coincident with taxol-induced apoptosis. Cell Growth Diff 1994;5:1041-50
155. Shaulsky G, Goldfinger N, Tosky MS, et al. Nuclear localization is essential for the activity of p53 protein. Oncogene 1991;6:2055-65
146. Meyerowitz BE. Psychosocial correlates of breast cancer and its treatments. Psychol Bull 1980;87:108-31
147. van Gestel YR, Voogd AC, Vingerhoets AJ, et al. A comparison of quality of life, disease impact and risk perception in women with invasive breast cancer and ductal carcinoma in situ. Eur J Cancer 2007;43:549-56
148. Rakovitch E, Franssen E, Kim J, et al. A comparison of risk perception and psychological morbidity in women with ductal carcinoma in situ and early invasive
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y SU
NY
Ups
tate
Med
ical
Uni
vers
ity o
n 08
/16/
14Fo
r pe
rson
al u
se o
nly.

Higa
ExpertOpin.Pharmacother.(2009) 10(15) 2497
breast cancer. Breast Cancer Res Treat 2003;77:285-93
149. Abraham J, Haut MW, Moran MT, et al. Adjuvant chemotherapy for breast cancer: effects on cerebral white matter seen in diffusion tensor imaging. Clin Breast Cancer 2008;8:88-91
150. Hershman DL, McMahon DJ, Crew KD, et al. Zoledronic acid prevents bone loss in premenopausal women undergoing adjuvant chemotherapy for early-stage breast cancer. J Clin Oncol 2008;26:4739-45
151. Gnant M, Mlineritsch B, Schippinger W, et al. Adjuvant ovarian suppression combined with tamoxifen or anastrozole, alone or in combination with zoledronic acid, in premenopausal women with endocrine-responsive, stage I and II breast cancer: first efficacy results from ABCSG-12 [abstract LBA4]. Proc Am Soc Clin Oncol 2008;26:18S
152. O’Shaughnessy C, Osborne J, Pippen M, et al. Efficacy of BSI-201, a poly (ADP-ribose) polymerase-1 (PARP-1) inhibitor, in combination gemcitabine/carboplatin (G/C) in patients with metastatic triple-negative breast cancer (TNBC): results of a randomized phase II trial [abstract 3]. J Clin Oncol 2009;27(18S):793s
153. Gottardis MM, Jordan VC. Development of tamoxifen-stimulated growth of MCF-7 tumors in athymic mice after long-term antiestrogen administration. Cancer Res 1988;48:5183-7
154. Lewis JS, Meeke K, Osipio C, et al. Intrinsic mechanism of estradiol-induced apoptosis in breast cancer cells resistant to estrogen deprivation. J Natl Cancer Inst 2005;97:1746-59
155. Alimandi M, Romano A, Curia MC, et al. Cooperative signaling of erbB3 and erbB2 in neoplastic transformation and human mammary carcinomas. Oncogene 1995;10:1813-21
156. Kokai Y, Myers JN, Wada T, et al. Synergistic interaction of p185c-neu and the EGF receptor leads to transformation of rodent fibroblasts. Cell 1989;58:287-92
157. Baselga J, Albanell J, Ruiz A, et al. Phase II and tumor pharmacodynamic study of gefitinib in patients with advanced breast cancer. J Clin Oncol 2005;23:5323-233
158. von Minckwitz G, Jonat W, Fasching P, et al. A multicentre phase II study
on geftinib in taxane- and anthracycline-pretreated metastatic breast cancer. Breast Cancer Res Treat 2005;89:165-72
159. Modi S, D’Andrea G, Norton L, et al. A phase I study of cetuximab/paclitaxel in patients with advanced-stage breast cancer. Clin Breast Cancer 2006;7:270-7
160. Xia W, Liu L-H, Ho P, Spector NL. Truncated ErbB2 receptor (p95ErbB2) is regulated by heregulin through heterodimer formation with ErbB3 yet remains sensitive to the dual EGFR/ErbB2 kinase inhibitor GW72016. Oncogene 2004;23:646-53
161. Moulder SL, Yakes FM, Muthuswamy SK, et al. Epidermal growth factor receptor (HER1) tyrosine kinase inhibitor ZD1839 (Iressa) inhibits HER2/neu (erbB2)-overexpressing breast cancer cells in vitro and in vivo. Cancer Res 2001;61:8887-95
162. Goss PE, Ingle JN, Martino S, et al. A randomized trial of letrozole in postmenopausal women after five years of tamoxifen therapy for early-stage breast cancer. N Engl J Med 2003;349:1793-802
163. Boer K, Lang I, Huhos E, et al. Hungarian experience with docetaxel combination (TAC) in the adjuvant treatment of breast cancer. Results of BCIRG 001 randomized, multicentric, phase III trial. Magy Onkol 2003;47:141-8
164. Perez EA, Romond EH, Suman VJ, et al. Updated results of the combined analysis of NCCTG N9831 and NSABP B-31 adjuvant chemotherapy with/without trastuzumab in patients with HER2-positive breast cancer. J Clin Oncol 2007;25:abstract 512
165. National Surgical Adjuvant Breast and Bowel Project (NSABP) Phase III randomized, double-blind trial examining oral administration of exemestane (Aromasin) versus placebo for 2 years in postmenopausal women who have completed 5 years of adjuvant tamoxifen therapy. NSABP B-33. Available from: www.nsabp.pitt.edu/B33-Information.html [Accessed 22 September 2006]
166. Baum M, Budzar AU, Cuzick J, et al. Anastrozole alone or in combination with tamoxifen versus tamoxifen alone for adjuvant treatment of postmenopausal women with early breast cancer: first results of the ATAC randomised trial. Lancet 2002;359:2131-9
167. Thurlimann B, Keshaviah A, Coates AS, et al. A comparison of letrozole and tamoxifen in postmenopausal women with early breast cancer. N Engl J Med 2005;353:2747-57
168. Coombes RC, Hall E, Gibson LJ, et al. A randomized trial of exemestane after two to three years of tamoxifen therapy in postmenopausal women with primary breast cancer. N Engl J Med 2004;350:1081-92
169. Slamon D, Eiermann W, Robert N, et al. Phase III randomized trial comparing doxorubicin and cyclophosphamide followed by docetaxel (AC T) with doxorubicin and cyclophosphamide followed by docetaxel and trastuzumab (AC TH) with docetaxel, carboplatin and trastuzumab (TCH) in HER2 positive early breast cancer patients: BCIRG 006 study [abstract 1]. Breast Cancer Res Treat 2005;94(Suppl 1):S5
170. Sunderland MC, Osborne CK. Tamoxifen in premenopausal patients with metastatic breast cancer. J Clin Oncol 1991;9:1283-97
171. Blamey RW, Jonat W, Kaufmann M, et al. Goserelin depot in the treatment of premenopausal advanced breast cancer. Eur J Cancer 1992;28A:810-4
172. Jonat W, Howell A. Blomqvist C, et al. A randomized trial comparing two doses of the new selective aromatase inhibitor anastrozole (Arimidex) with megestrol acetate in postmenopausal patients with advanced breast cancer. Eur J Cancer 1996;32A:404-12
173. Dombernowsky P, Smith I, Falkson G, et al. Letrozole, a new oral aromatase inhibitor for advanced breast cancer: double-blind randomized trial showing a dose effect and improved efficacy and tolerability compared with megestrol acetate. J Clin Oncol 1998;16:453-61
174. Smith RE, Brown AM, Mamounas EP, et al. Randomized trial of 3-hour versus 24-hour infusion of high-dose paclitaxel in patients with metastatic or locally advanced breast cancer: national surgical adjuvant breast and bowel project B-26. J Clin Oncol 1999;17:3403-11
175. Perez EA, Vogel CL, Irwin DH, et al. Multicenter phase II trial of weekly paclitaxel in women with metastatic breast cancer. J Clin Oncol 2001;19:4216-23
176. Nabholtz JM, Senn HJ, Bezwoda WR, et al. Prospective randomized trial of
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y SU
NY
Ups
tate
Med
ical
Uni
vers
ity o
n 08
/16/
14Fo
r pe
rson
al u
se o
nly.

Breastcancer:beyondthecuttingedge
2498 ExpertOpin.Pharmacother.(2009) 10(15)
docetaxel versus mitomycin plus vinblastine in patients with metastatic breast cancer progressing despite previous anthracycline-containing chemotherapy. 304 Study Group. J Clin Oncol 1999;17:1413-24
177. Hoff PM, Ansari R, Batist G, et al. Comparison of oral capecitabine versus intravenous fluorouracil plus leucovorin as first-line treatment in 605 patients with metastatic colorectal cancer: results of a randomized phase III study. J Clin Oncol 2001;19;2282-92
178. Gradishar WJ, Tjulandin S, Davidson N, et al. Phase III trial of nanoparticle albumin-bound paclitaxel compared with polyethylated castor oil-based paclitaxel in women with breast cancer. J Clin Oncol 2005;23:7794-803
179. Fisher B, Anderson S, Wickerham DL, et al. Increased intensification and total dose of cyclophosphamide in a doxorubicin-cyclophosphamide regimen for the treatment of primary breast cancer: findings from national surgical adjuvant breast and bowel project B-22. J Clin Oncol 1997;15:1858-69
180. Biganzoli L, Cufer T, Brunign P, et al. Doxorubicin and paclitaxel versus doxorubicin and cyclophosphamide as first-line chemotherapy in metastatic breast cancer: The European Organization for Research and Treatment of Cancer 10961 Multicenter Phase III Trial. J Clin Oncol 2002;20:3114-21
181. Nabholtz JM, Falkson C, Campos D, et al. Docetaxel and doxorubicin compared with doxorubicin and cyclophosphamide as first-line chemotherapy for metastatic breast cancer: results of a randomized, multicenter, phase III trial. J Clin Oncol 2003;21:968-75
182. Albain K, Nag S, Calderillo-Ruiz G, et al. Global phase III study of gemcitabine plus paclitaxel (GT) versus paclitaxel (T) as front-line therapy for metastatic breast cancer (MBC): First report of overall survival [abstract 510]. Proc Am Soc Clin Oncol 2004;22:52
183. O’Shaughnessy J, Miles D, Vukelja S, et al. Superior survival with capecitabine plus docetaxel combination therapy in anthracycline-pretreated patients with advanced breast cancer: Phase III trial results. J Clin Oncol 2002;20:2812-23
184. Thomas ES, Gomez HL, Li RK, et al. Ixabepilone plus capecitabine for metastatic breast cancer progressing after anthracycline and taxane treatment. J Clin Oncol 2007;25:5210-7
185. Miller K, Wang M, Gralow J, et al. A randomized phase II trial of paclitaxel versus paclitaxel plus bevacizumab as first-line therapy for locally recurrent or metastatic breast cancer: a trial coordinated by the Eastern Cooperative Oncology Group (E2100) [abstract 3]. Breast Cancer Res Treat 2005;95(Suppl 1):S6
186. Geyer CE, Forster J, Lindquist D, et al. Lapatinib plus capecitabine for
HER2-positive advanced breast cancer. N Engl J Med 2006;255:2733-43
187. Fountzilas G, Dafni U, Dimopoulos MA, et al. A randomized phase III study comparing three anthracycline-free taxane-based regimens, as first-line chemotherapy, in metastatic breast cancer: a Hellenic Cooperative Oncology Group study. Breast Cancer Res Treat 2009;115:87-9
188. Burstein HJ, Kuter I, Campos SM, et al. Clinical activity of trastuzumab and vinorelbine in women with HER2-overexpressing metastatic breast cancer. J Clin Oncol 2001;19:2722-30
189. Esteva FJ, Valero V, Booser D, et al. Phase II study of weekly docetaxel and trastuzumab for patients with HER2-overexpressing metastatic breast cancer. J Clin Oncol 2002;20:1800-8
190. Osako T, Ito Y, Takahashi S, et al. Efficacy and safety of trastuzumab plus capecitabine in heavily pretreated patients with HER2-postive metastatic breast cancer. Cancer Chemother Pharmacol 2008;62:159-64
AffiliationGerald M Higa PharmDAssociate Professor, West Virginia University, Mary Babb Randolph Cancer Center, Schools of Pharmacy and Medicine, Morgantown, WV 26506-9520, USA Tel: +1 304 293 1461; Fax: +1 304 293 7672; E-mail: [email protected]
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y SU
NY
Ups
tate
Med
ical
Uni
vers
ity o
n 08
/16/
14Fo
r pe
rson
al u
se o
nly.