Embed Size (px)
Citation preview
AnalysisBreast
Program and
Client: MD
Duck
Department
liffe
D 2000
TABLE OF CONTENTS
Executive Summary 1Introduction 3Background 3Approach and Methodology 5Findings 5Alternatives and/or Hypotheses Considered 11Conclusions 12Recommendations 13Action Plan 14Definitions 15
Appendices (A thru KK)
11
Executive Summary
The student team was asked to determine causes of low patient satisfaction forwait times in the Breast Care Center (BCC). According to a November 1999survey, 10% of the patients rated their wait time in the clinic as “Excellent”. TheCancer Center has a patient satisfaction goal of 50% “Excellent”.
The team observed 81 patients in the BCC over the course of 6 weeks, collectingboth qualitative and quantitative data regarding patient stays and staff utilization.Time studies were conducted to gather information on the current state of thesystem. Patient and staff interviews were conducted to gather a betterunderstanding of how the clinic works, including staff roles and patient flowthroughout the clinic.
Each patient was placed into one of three groups: new undiagnosed, return visit,or new cancer. Because the clinics all operate on Monday, the data wereanalyzed together. However, since different patient types require differentservices, the data were also analyzed separately during scheduling analysis.
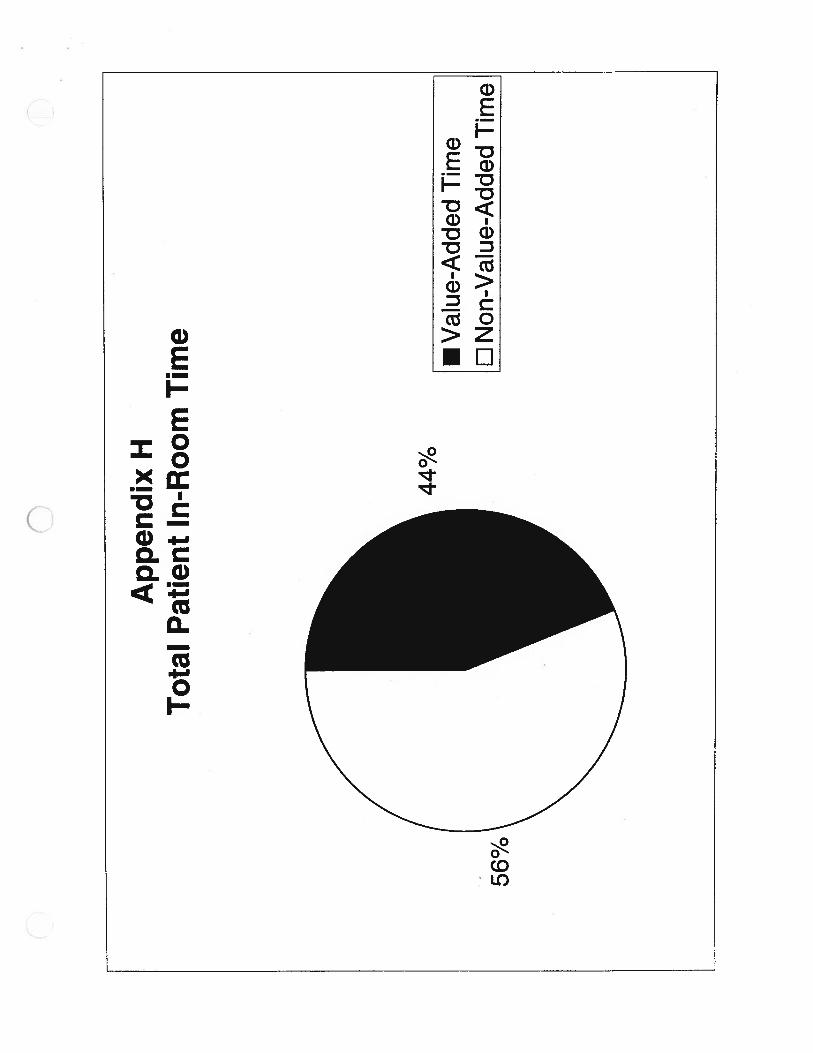
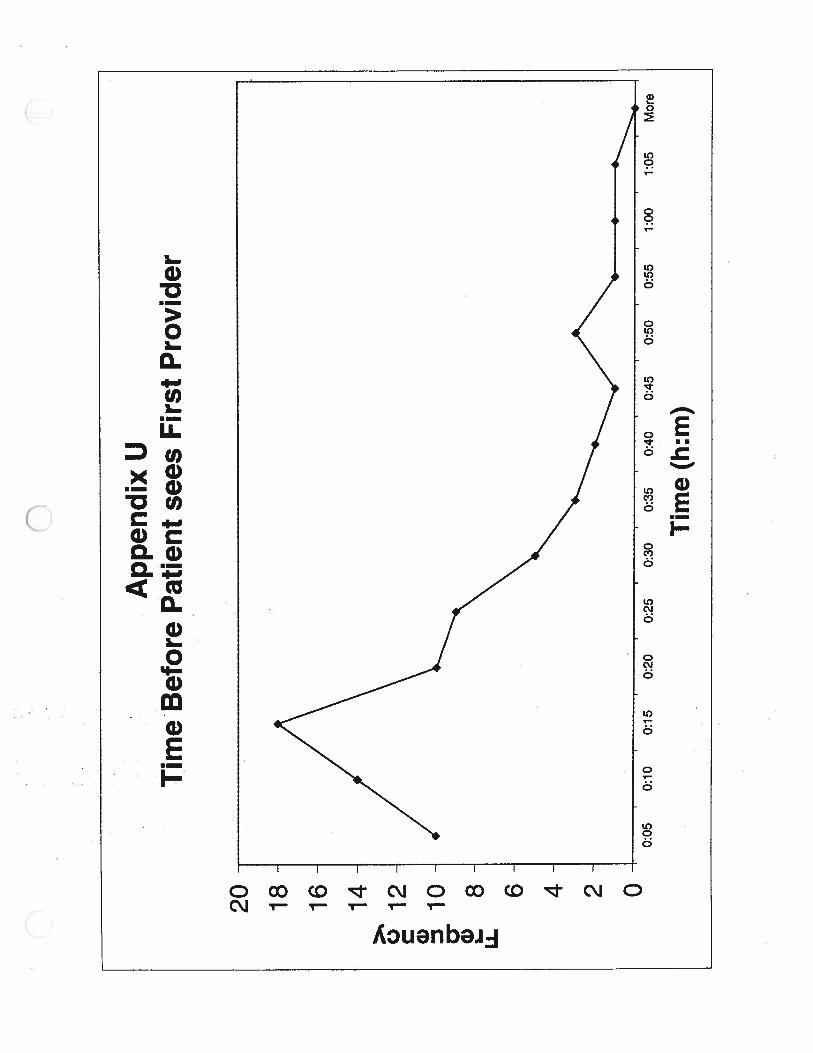
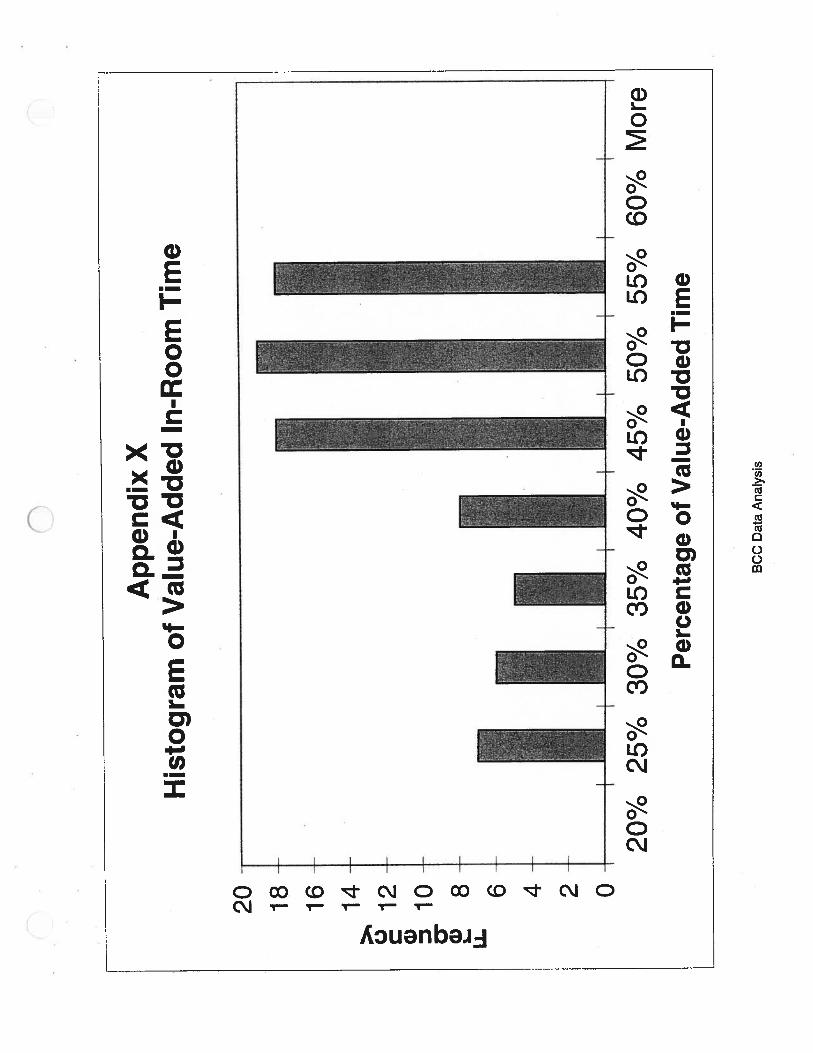
Patients spent an average of 55 minutes in the exam room. 30 of those minuteswere spent waiting for a provider (non-value-added time), and 25 minutes werespent with the provider (value-added time), so that 44% of the time in the examroom patients were with a provider, and 55% of the time was spent waiting. Onaverage, a patient waited in an exam room for 17 minutes before being seen bythe provider.
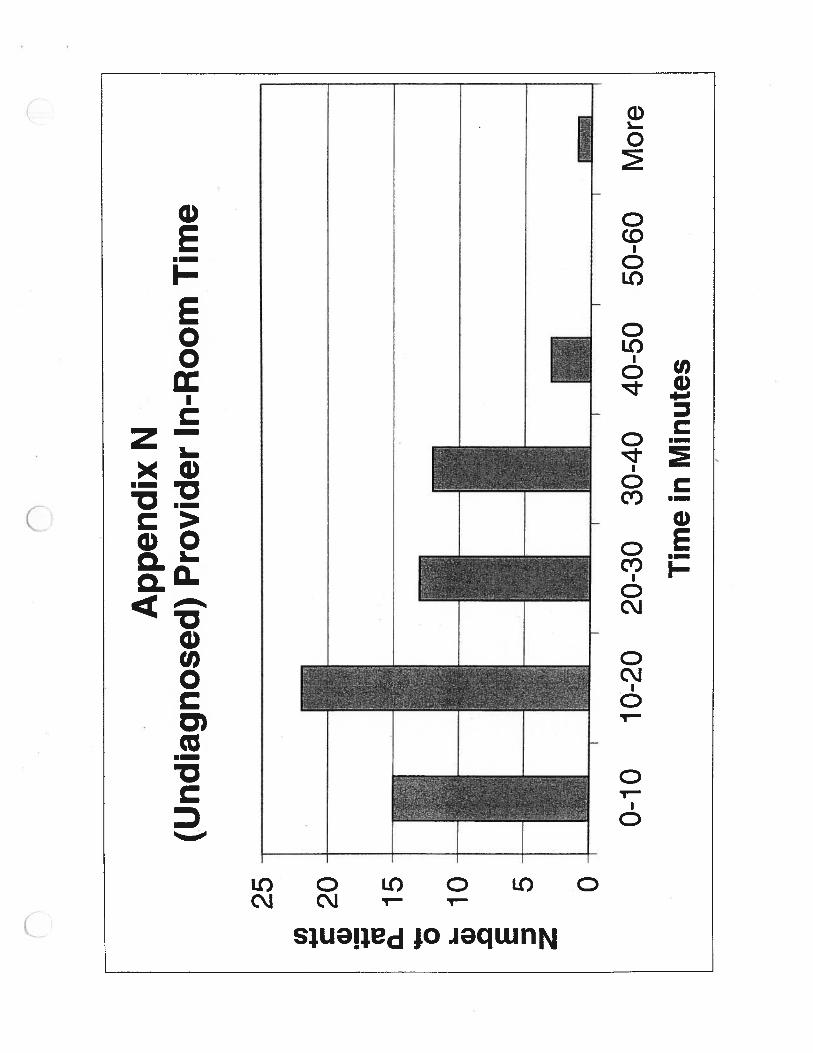
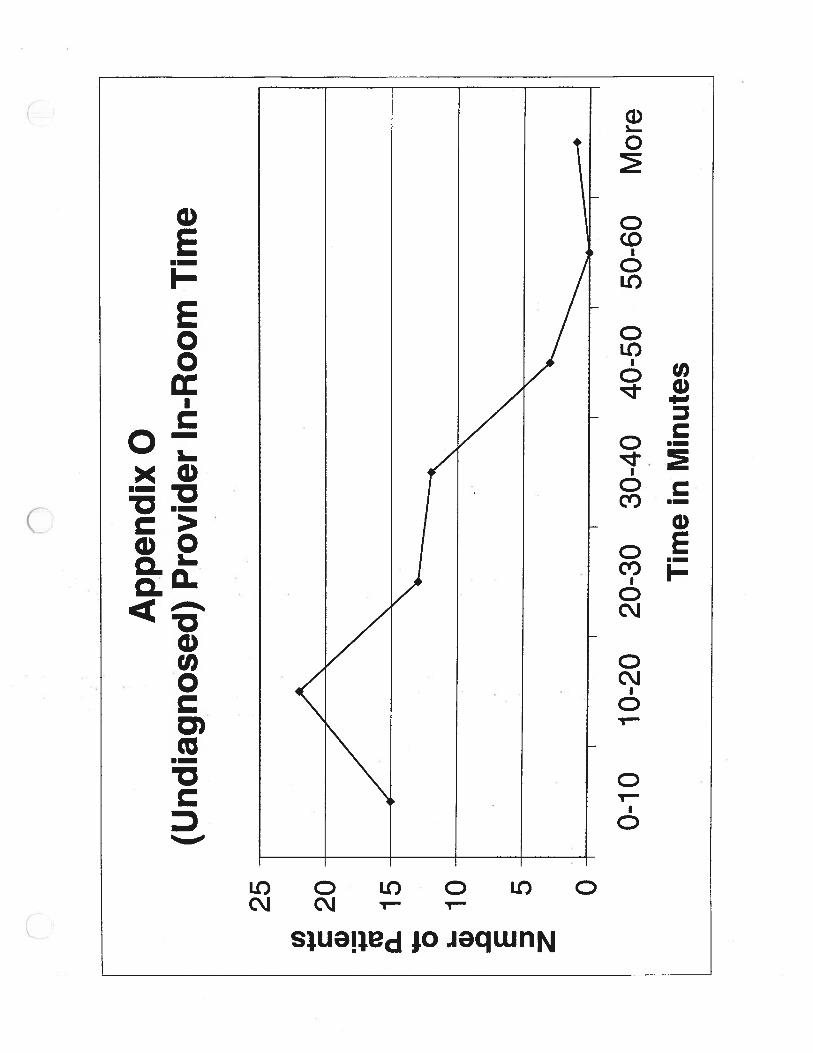
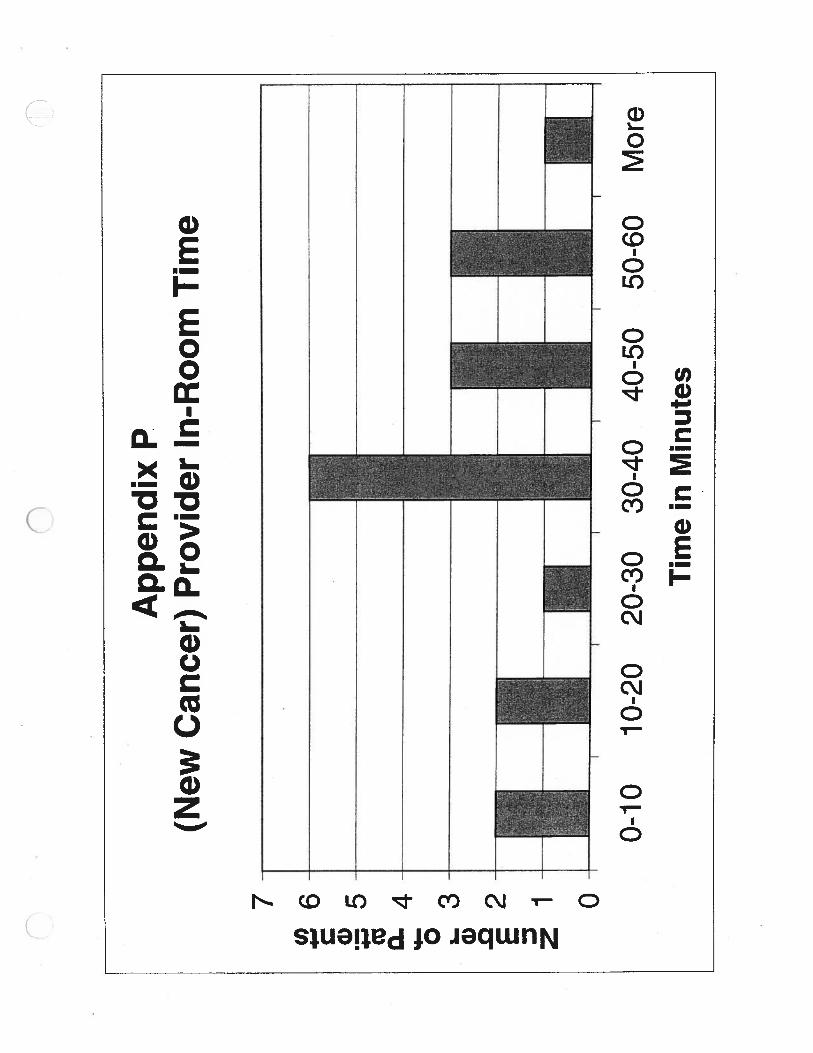
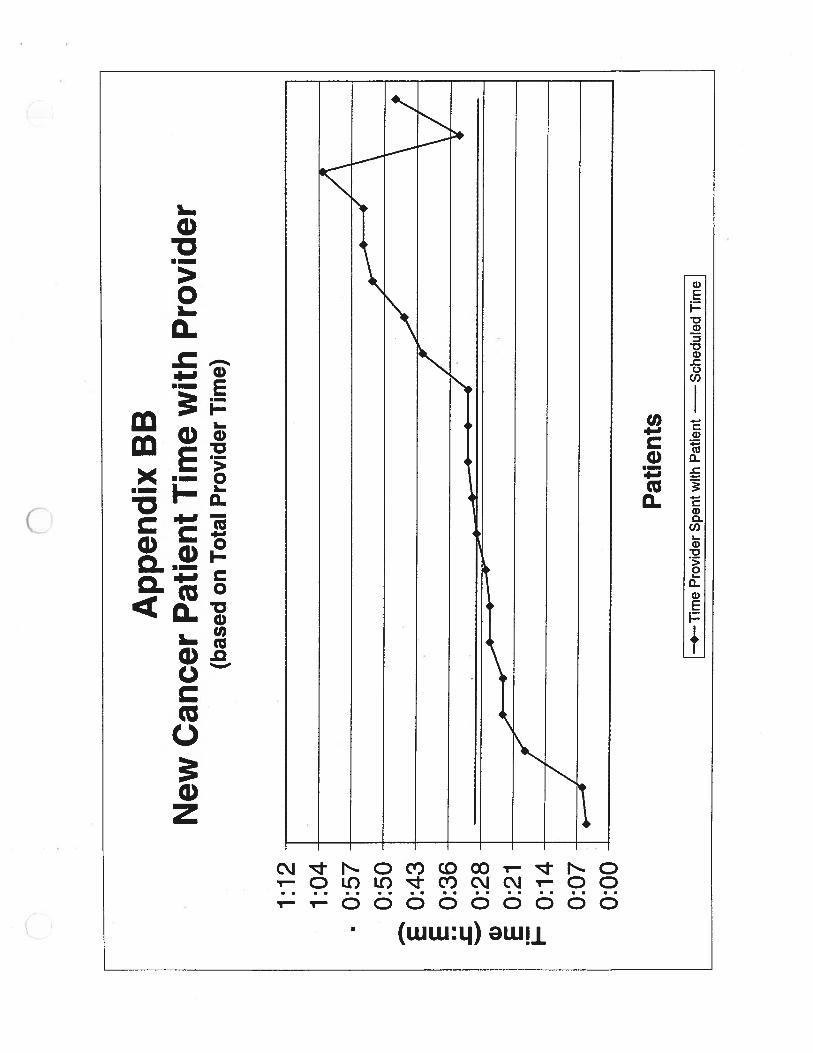
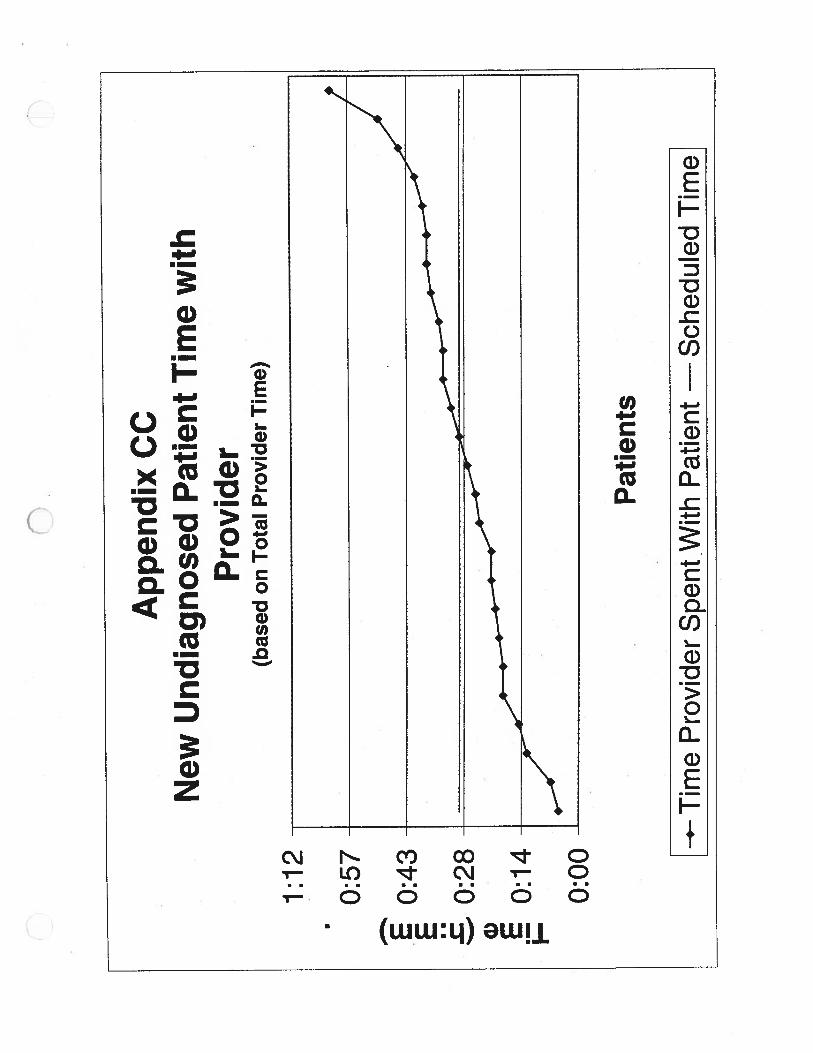
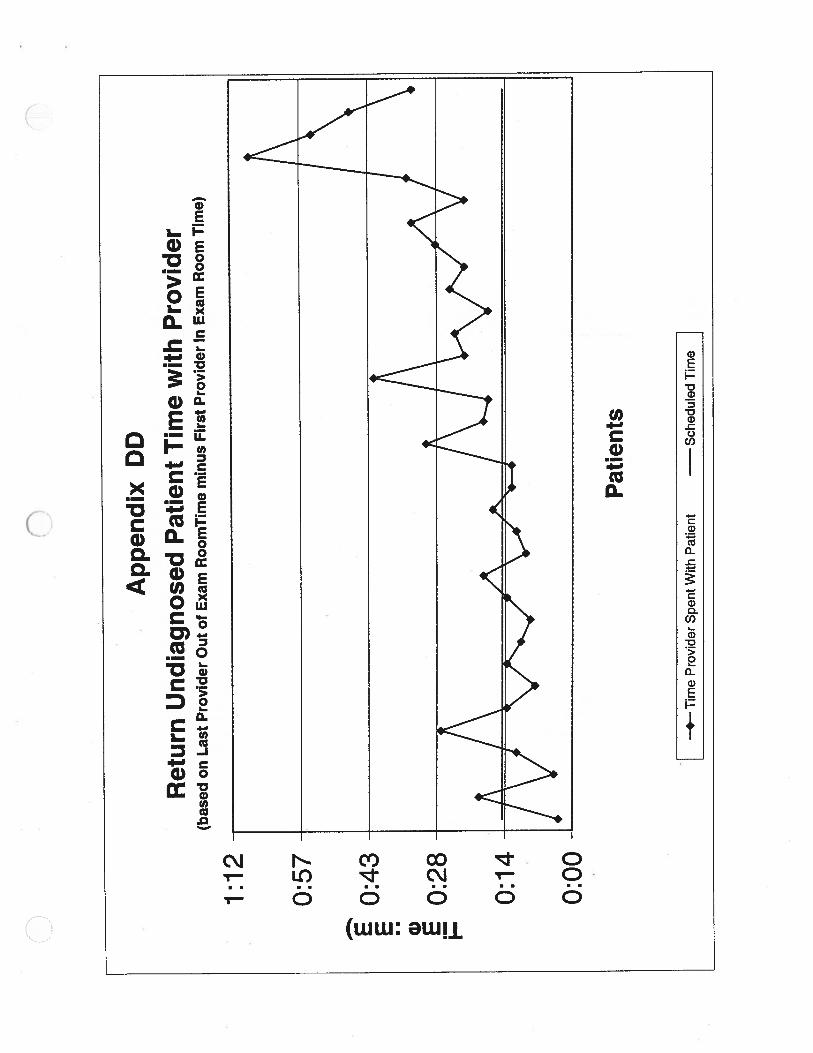
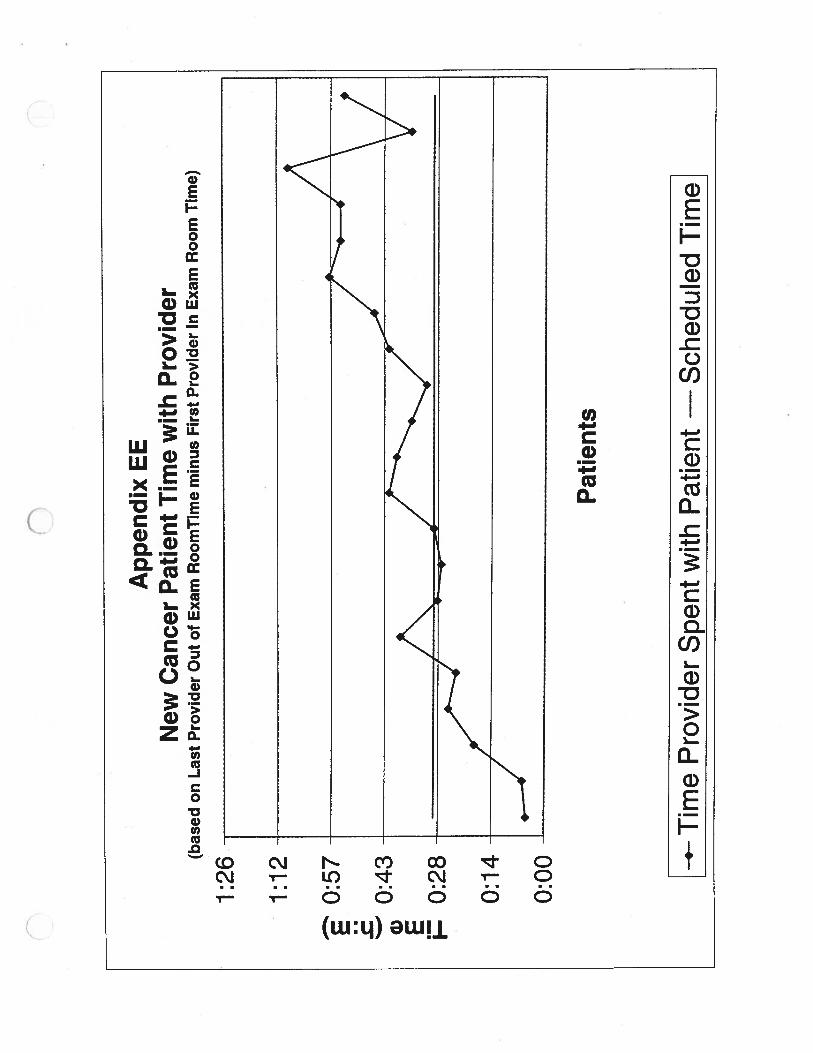
New undiagnosed patients are scheduled for 30-minute appointments. Studiesshowed that average total provider time for these patients were 43 minutes.Return undiagnosed patients are scheduled for 15-minute appointments, andtotal provider time for them averaged 23 minutes per patient. New cancerpatients are scheduled for 30-minute appointments, and total provider time forthem averaged 36 minutes. Because patients are being scheduled for less timethan they are actually seen, they are experiencing long wait times in the waitingrooms and in the exam rooms.
Through qualitative data collection it was found that much of the patientdissatisfaction comes from a lack of personalization to their visit. Occasionally, apatient would be placed in an exam room and left, sometimes for over an hour,without being seen by anyone. It was observed in the Melanoma Clinic thatwhen patients experience long waits, a staff member would notify the patient thatthe provider was running late and give an estimate of when the provider would beready. This type of patient personalization should be implemented in the BCCsince long wait times will occur once in a while.
1
It was also observed that staff members to not use the lighting system 100% ofthe time. The lighting system is designed to allow staff members to determinethe current state of any exam room, so that if a room is available for a patient, anMA can take a patient into the room. Since the lighting system is not being usedeffectively, MA’s must check each room before taking a patient into it. If all staffmembers used the lighting system 100% if the time, MA’s would not need tocheck the room before taking in a patient.
Because new cancer patients spend around 8 hours in the clinic, it should befurther explored to split the multidisciplinary clinic (for new cancer patients) into 2clinics operating on different days, one for the new patients and one for theirfollow-up visits. This would possibly simplify scheduling since currently,afternoon scheduling is not done until the tumor board meets at 1:30.
2
Introduction
The Breast Care Clinic (BCC) at the University of Michigan Hospital requested astudy to be conducted to determine patient flow and patient satisfaction. OurIndustrial and Operations 481 team, a group of three student consultants, hasbeen asked to provide a patient flow analysis in the BCC. The Industrial andOperations 481 team analyzed BCC exam room utilization, and patient waittimes. The main goal of this project is to investigate the satisfaction rate ofpatients waiting for services in the Breast Care Clinic and give recommendationsto remedy this problem.
Background
In a November 1999 survey, results showed that 10% of patients seen in theBreast Care Clinic described their wait time at the clinic as “excellent.” This isthe lowest percentage across all clinics in the University of MichiganComprehensive Cancer Center. The institutional goal is 50%. The team ofstudent consultants observed qualitatively and quantitatively the two main areasof the clinic including the 1) waiting room/check-in area, and 2) examinationrooms. By making recommendations as to how to decrease wait time, thestudent team will increase the percentage of patients who describe their waittimes as “excellent”. This will be done by exploring new ways to educate andservice patients at the clinic.
The Breast Care Cancer Clinic currently operates on Mondays and Thursdays.The Monday Breast Care Clinic consists of three clinics, two undiagnosed breastproblem clinics and one multidisciplinary clinic for newly diagnosed breast cancerpatients. The Undiagnosed Breast Care Clinic — Surgery, is a morning clinic.This clinic spans from 7:45AM until 12:30PM and is staffed by one surgeon(Oncology) and residents. The patient population consists of people with one ormore of the following:
• Benign, undiagnosed breast problems.• Mammographic abnormalities.• Abnormal breast exams.• Breast imaging referrals.• Breast problems requiring a fine needle aspiration (FNA), surgical biopsy,
or suspicious for malignancy.
A second clinic is the Undiagnosed Breast Care Clinic — Gynecology, which isanother morning clinic and spans from 8:00AM until 12:00PM. A gynecologistand a resident staff this clinic. The patient population consists of people with oneor more of the following:
• Benign, undiagnosed breast problems.• Breast problems of women who are pregnant or postpartum.
3

• Mammographic abnormalities.• Abnormal breast exams.• Breast problems requiring FNA, surgical biopsy, or not suspicious for
malignancy.
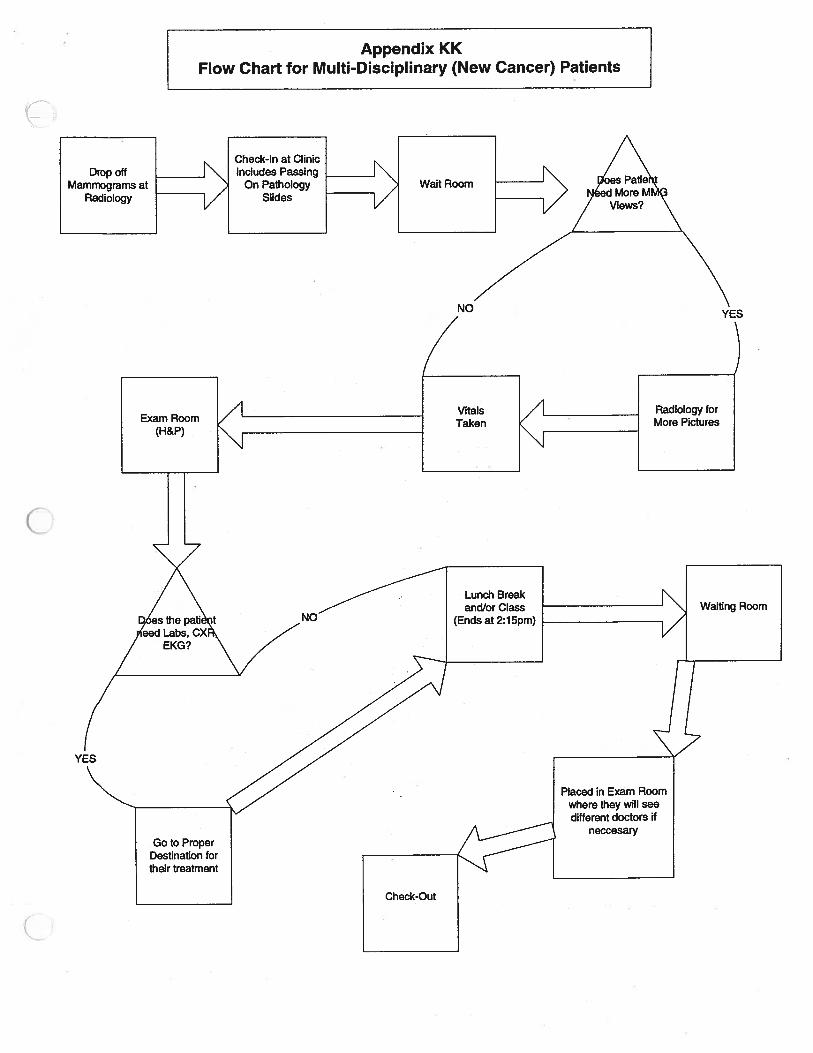
The third clinic is the Multidisciplinary Breast Cancer Clinic. Surgeons and amultidisciplinary team consisting of Radiology Oncology, Medical Oncology,Plastic Surgery, and social work staff this clinic. The clinic can accept up to 8new patients per week. In the Multidisciplinary Breast Cancer Clinic, the 8 newpatients are brought in during the morning and spoken to by a nurse practitioner.The nurse practitioner performs a history and physical (intake process) on thepatients. Concurrently with the intake process, the pathologists and theradiologists read the patient’s pathology slides and mammograms, respectively.If additional mammogram views are needed or additional ultrasound views areneeded the nurse practitioner will take the patient to have them performed. Inthe afternoon, the doctors, nurses, and specialists decide which patient will seewhich medical physician. On average, 26 patients are seen in the morningthroughout the 3 clinics. When a new cancer patient requests an appointment,the wait may currently be one to two weeks.
In this clinic, once a new patient gets an appointment, they receive aninformation packet sent via Federal Express. This packet includes an itinerary ofwhat the patient should expect during their visit and directions for the patientupon arriving to the clinic. They are instructed to drop off their Mammograms atthe Radiology Department at 9:00AM and then proceed to the Breast Care Clinicand drop off their pathology slides at check-in. When they arrive, they will wait tobe seen by a nurse practitioner. The nurse practitioner will educate the newclients about both the procedure of the options they have as well as the cancerand will let them know if they need any other Mammogram views. If other viewsare needed, the patient will be sent back to the Radiology Department. Theresults of the mammogram, the pathology, and the meeting with the nursepractitioner will be discussed among the doctors at the Tumor Board from 1:00-2:30PM every Monday. The results of this meeting will determine their treatmentrecommendations and which disciplines will need to be involved. The returnpatients just need to arrive for their appointment times.
In response to the BCC’s goals for decreased wait times and increased patientsatisfaction, the student team analyzed the clinics’ performance in order torecommend actions to:
• Decrease patient visit time, especially through reducing non-value addedtime.
• Decrease barriers to staff efficiency throughout patients’ visit.• Increase effectiveness of educational material available for patients.• Increase examination room utilization.
4

Approach and Methodology
The approach the student team used to assess the BCC is classified into fourphases.
• Observe the BCC.• Collect data (both time studies of patient flow and interviewing).• Analyze data.• Make recommendations.
To address the patient flow issues at the clinic, the student team documented thecurrent system, took extensive time studies on the patient flow, and interviewedpatients and personnel regarding their interactions. The student team thenanalyzed the results from each individual part (Check-In/Waiting Area, ExamRoom) to detect barriers to efficiency problems.
The student team also examined the educational material available to thepatients before they visit the clinic. This allowed the team to have a morethorough understanding of the mindset of the patients when they arrive at theclinic.
Based on survey results, the Melanoma Clinic currently has the highest customersatisfaction regarding wait to see a doctor. The team toured the clinic and tookqualitative and quantitative observations of how their patient flow differs from thatin the Breast Care Clinic. We used this information to compare (benchmark) theclinics.
Some limitations that were faced were that there are limitations to any samplingcollection method. The clinics schedule data was used to confirm andsupplement collected data. The student team asked the patients to fill out datacollection forms. The limitations that were associated with this samplingcollection method included:
• Not all patients wanted to fill out the form.• Multiple forms were incomplete, missing key information such as
accurate times, or providers.
Findings
A. Data
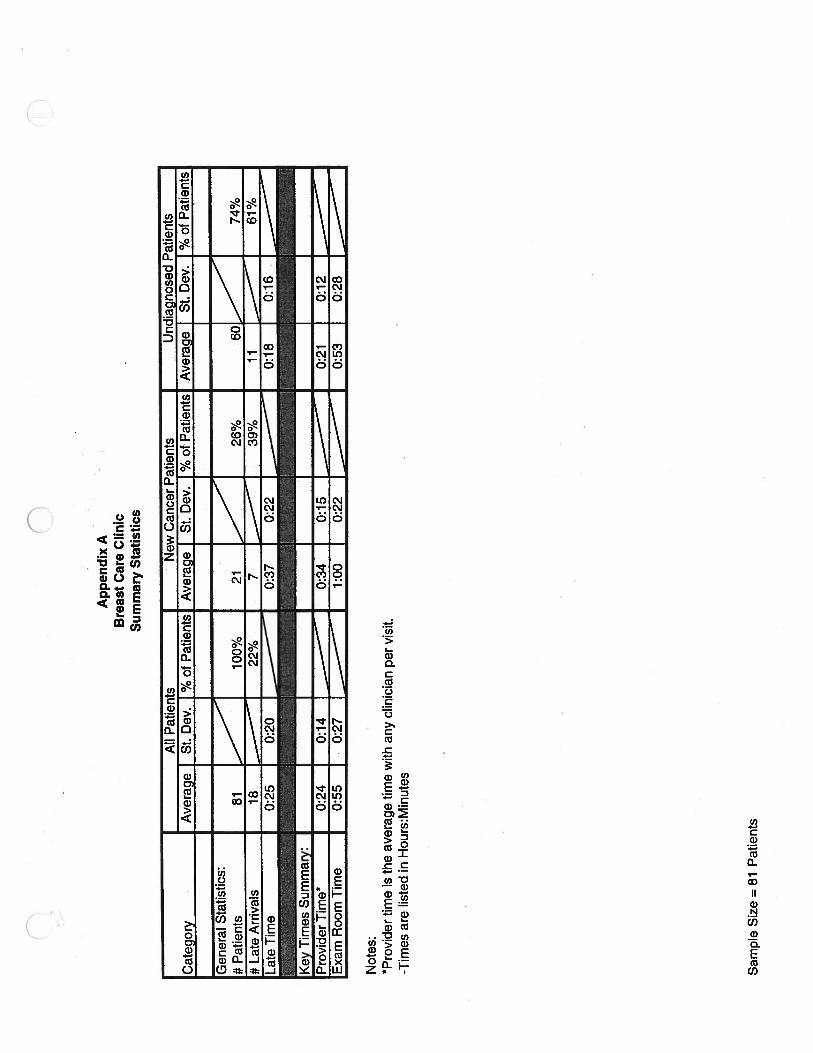
The following table shows the summary statistics of the BCC. The sample sizeconsisted of 81 Breast Care Clinic patients.
5
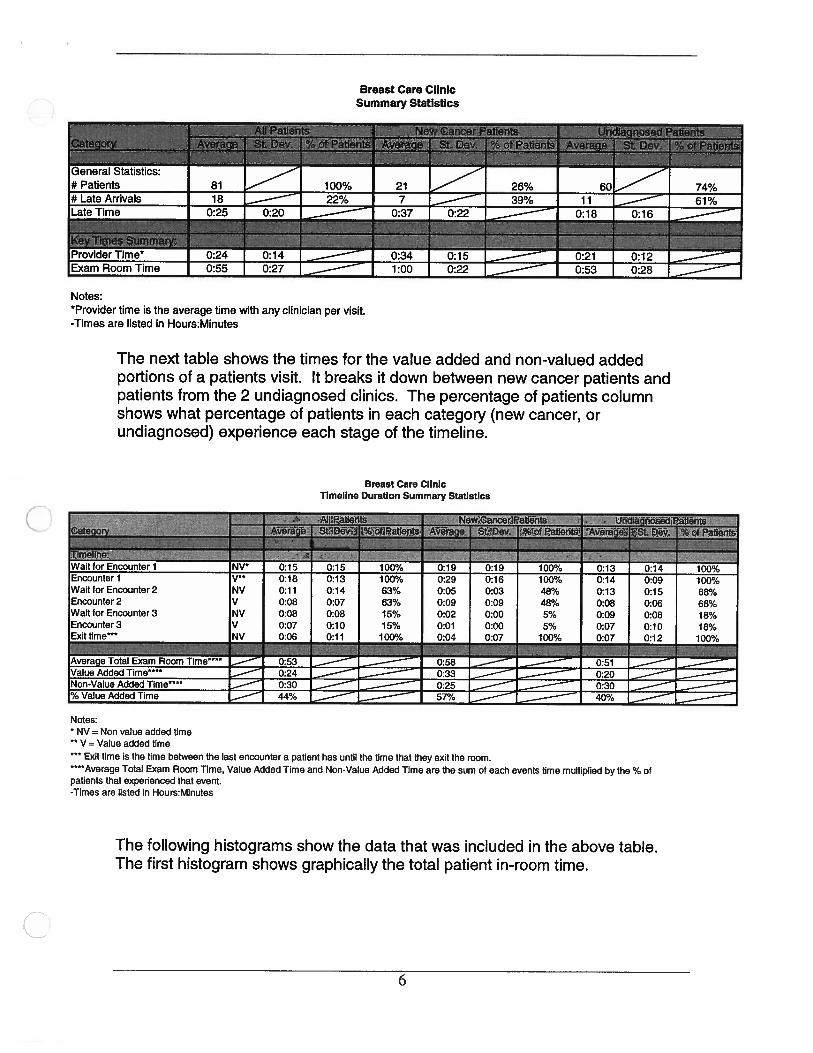
Breast Care ClinicSummary Statistics
Pat1tit*IL
______
-; Wa StDev %ofPàti ‘
General Statistics:
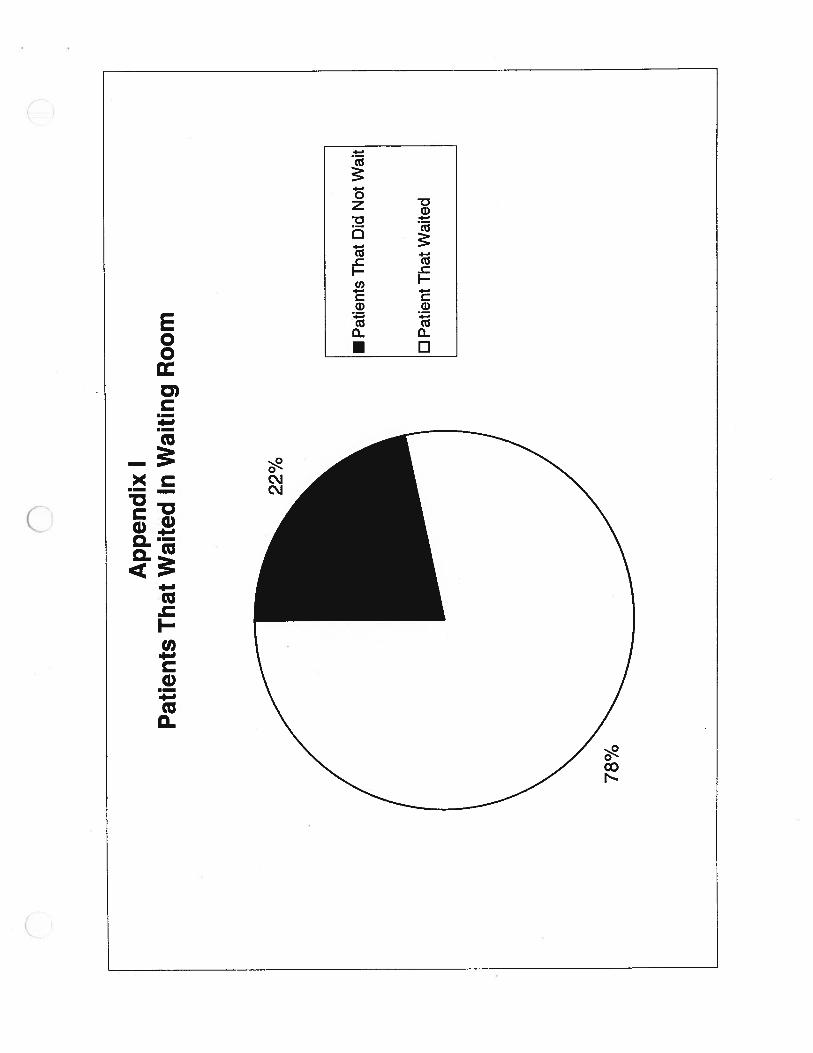
# Patients 81 100% 21 26% 60[__— 74%#LateArrivals 18 22% 7 39% I 11 L— 61%Late Time 0:25 0:20 0:37 0:22 __—j 0:18 0:18
Provider Time* 0:24 0:14 ___ 0:34 0:15 __— 0:21 0:121Exam Room Time 0:55 0:27 __.__— 1:00 0:22 ___— 0:53 0:28 ___—
Notes:*provider time is the average time with any clinician per visit.-Times are listed in Hours:Minutes
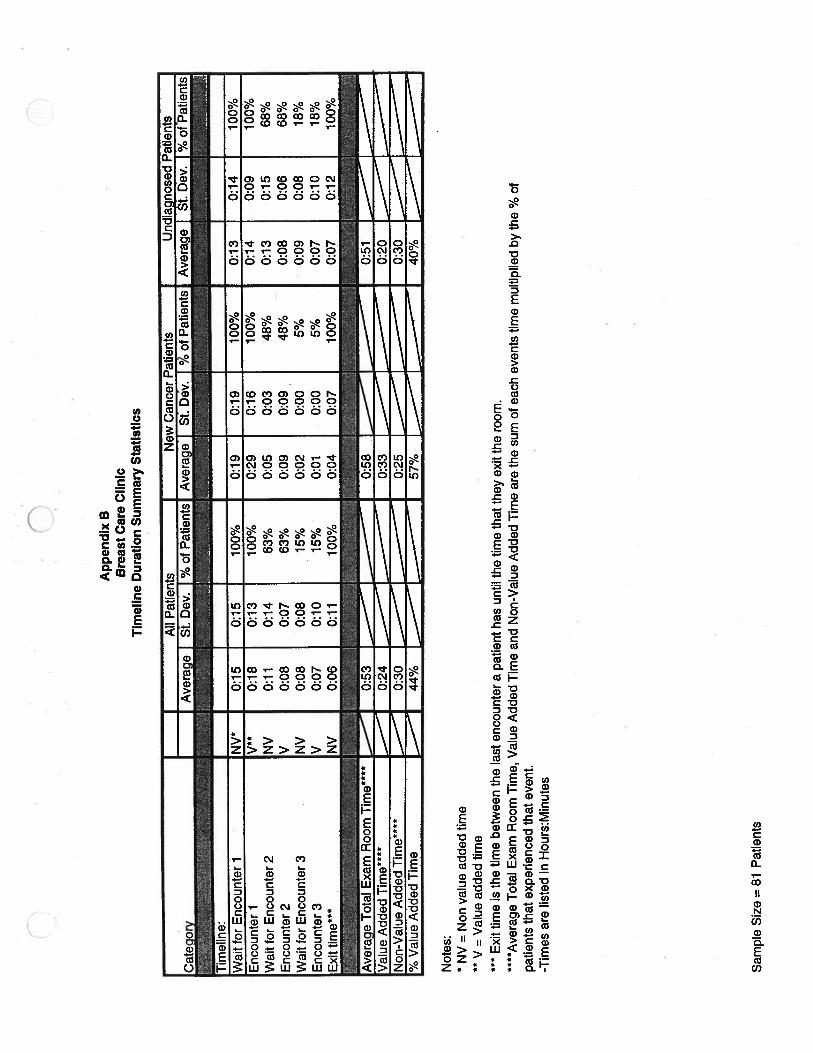
The next table shows the times for the value added and non-valued addedportions of a patients visit. It breaks it down between new cancer patients andpatients from the 2 undiagnosed clinics. The percentage of patients columnshows what percentage of patients in each category (new cancer, orundiagnosed) experience each stage of the timeline.
Breast Care ClinicTimeline Duration Summary Statistics
ZZaverage Total Exam Room Time**** — 0:53 — 0:58 0:51value Added Time****
— 0:24 0:33 0:20‘lon-Value Added Time****
.— 0:30 0:25 0:303 Value Added Time ..— 44% 57% 40%
Notes:* NV = Non value added time** V = Value added time
Exit time is the time between the last encounter a patient has until the time that they exit the room.****Average Total Exam Room Time, Value Added Time and Non-Value Added Time are the sum of each events time multiplied by the % ofpatients that experienced that event.-Times are listed in Hours:Minutes
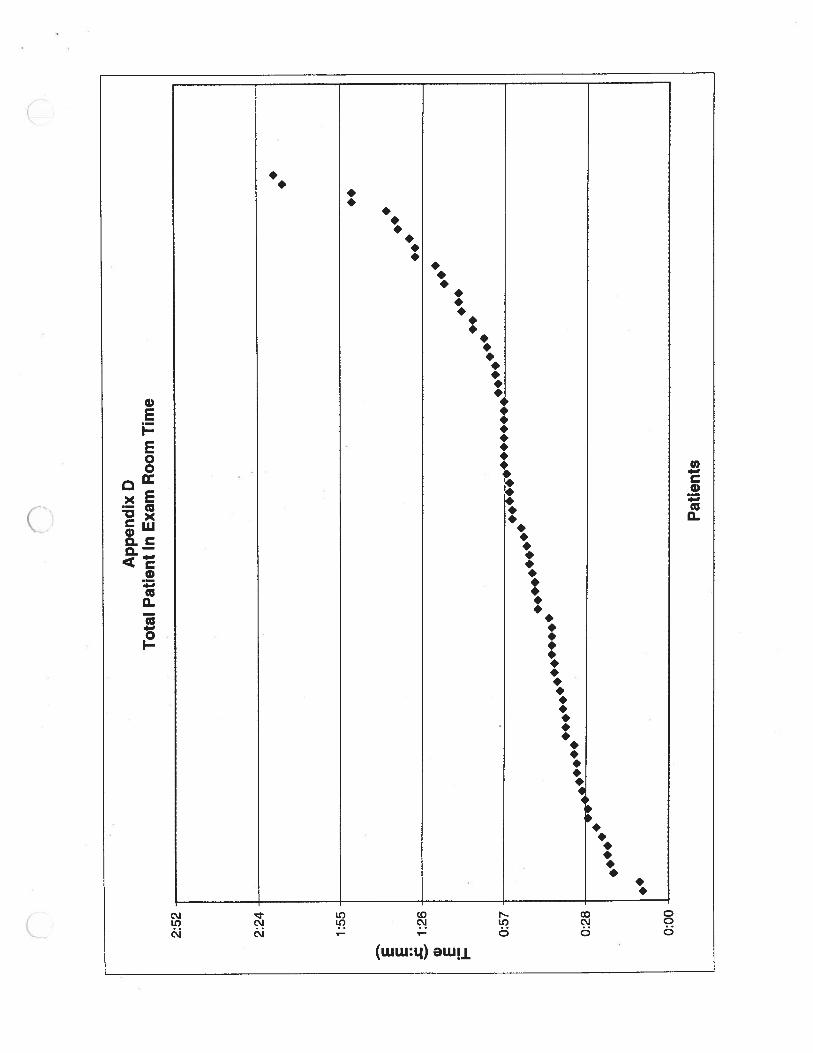
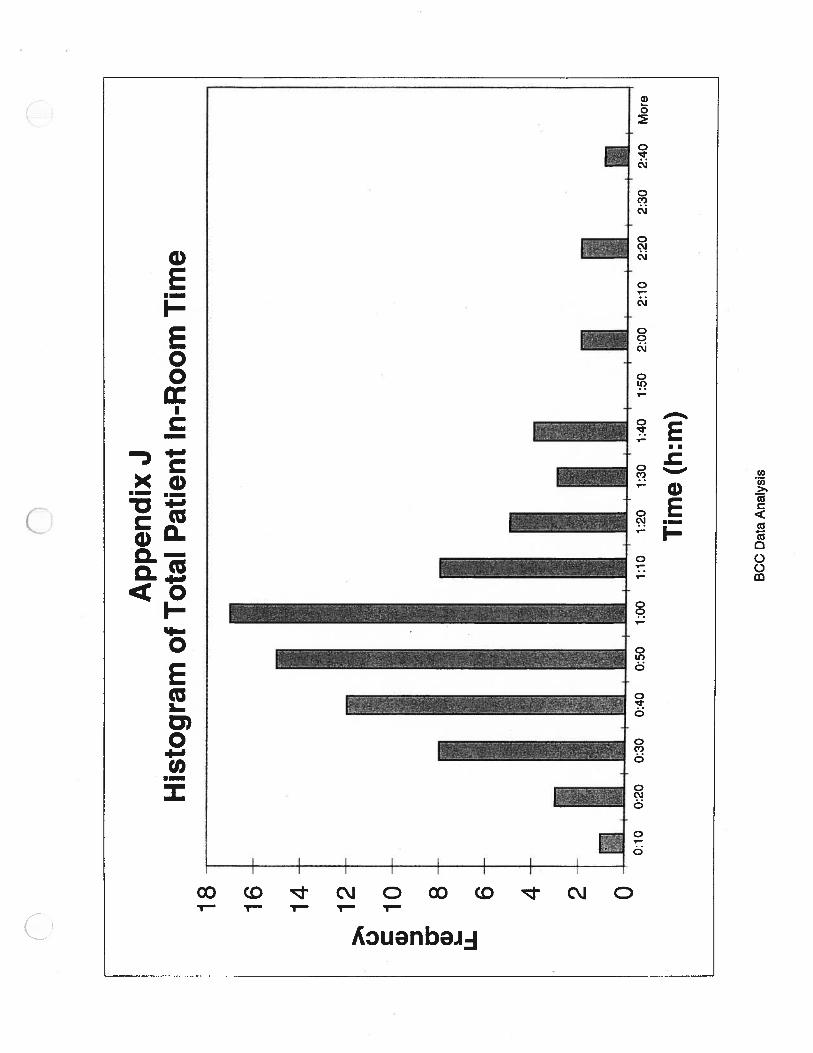
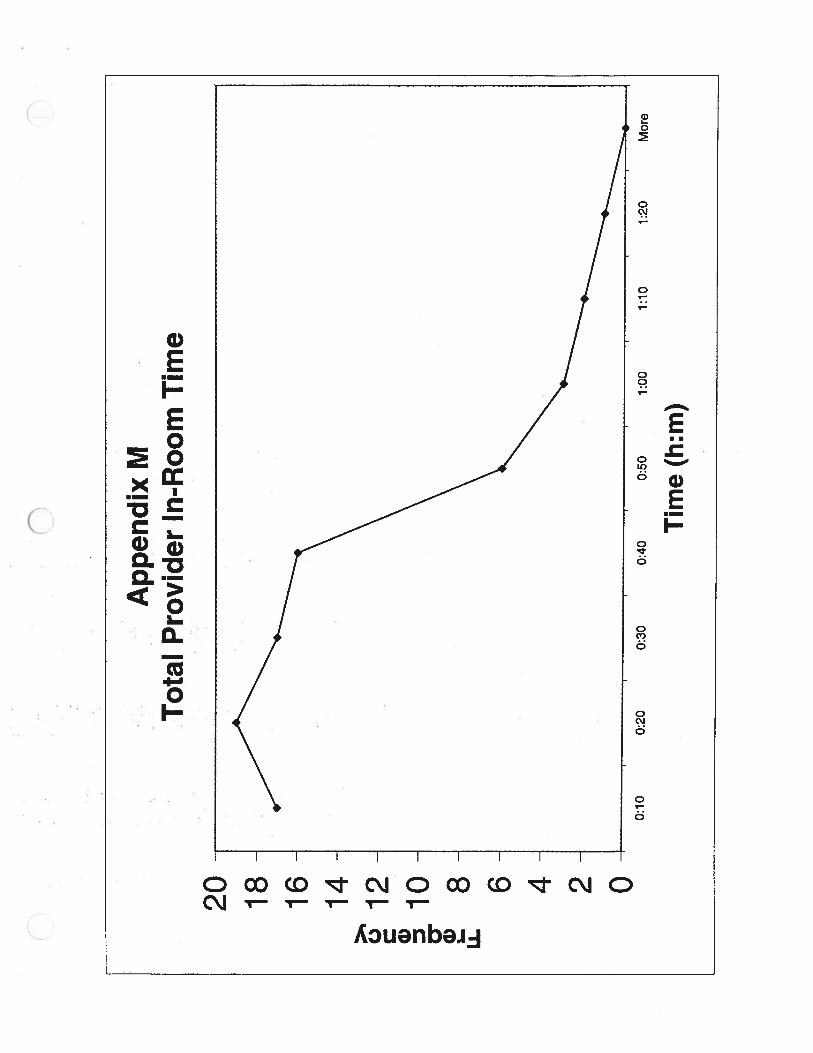
The following histograms show the data that was included in the above table.The first histogram shows graphically the total patient in-room time.
Wait for Encounter 2Encounter 2Wait for Encounter 3Encounter 3Exit time***
NVI)
NV
NV
0:180:110:080:080:070:06
0:130:140:070:080:100:11
100%63%63%15%15%
100%
0:290:050:090:020:010:04
0:160:030:090:000:000:07
48%48%5%5%
100%
0:140:130:080:090:070:07
0:090:150:060:080:100:12
68%68%18%18%
100%
6
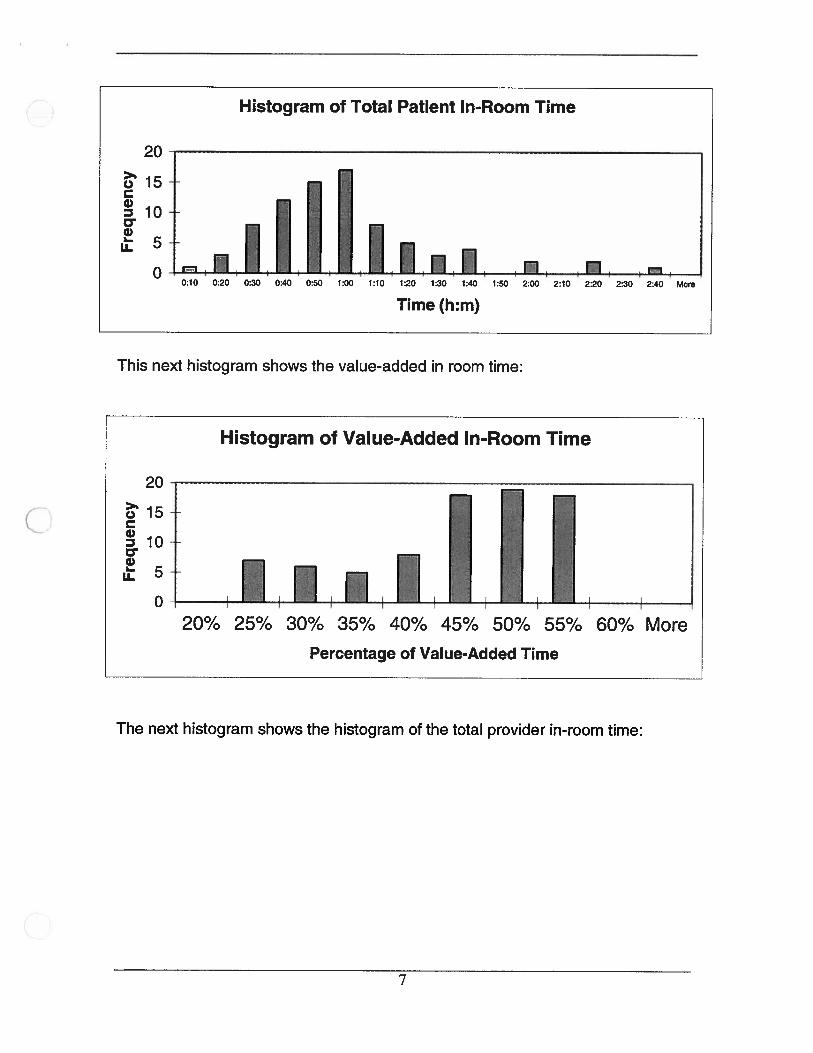
Histogram of Total Patient In-Room Time
This next histogram shows the value-added in room time:
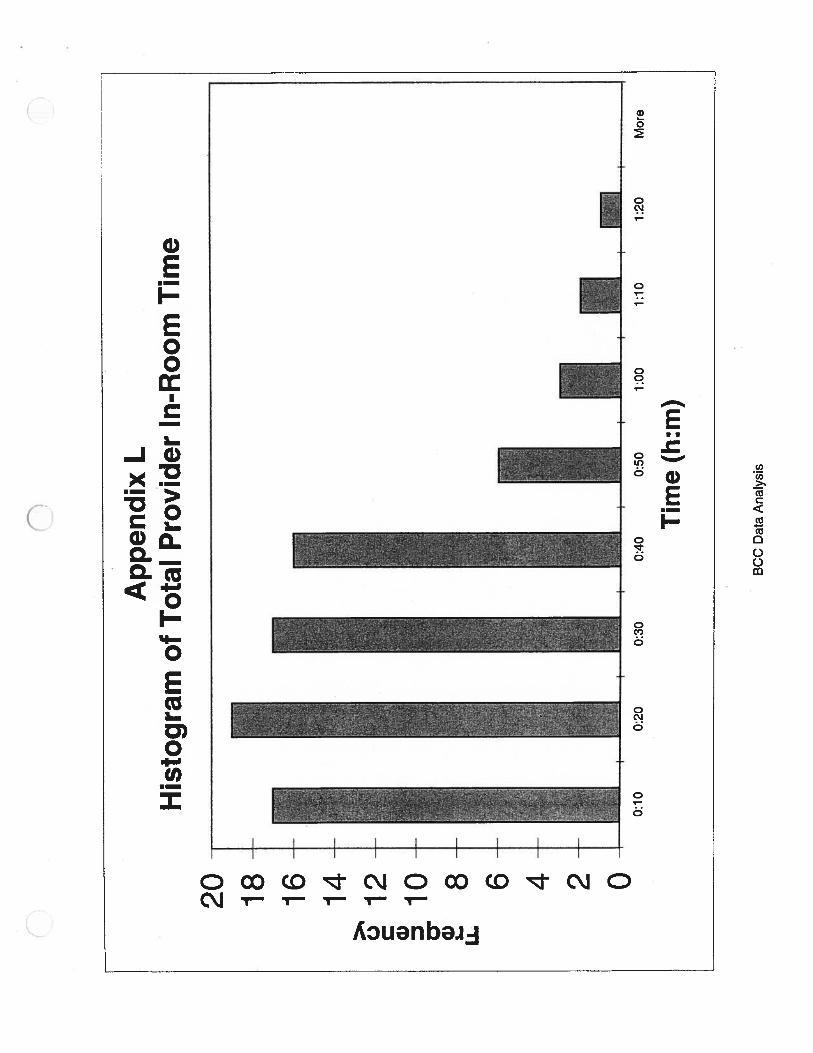
The next histogram shows the histogram of the total provider in-room time:
20
015a)
100•I
LI.
0
Time(h:m)
Histogram of Value-Added In-Room Time
C)Ca)D 10
....•,. I20% 25% 30% 35% 40% 45% 50% 55% 60% More
Percentage of Value-Added Time
7
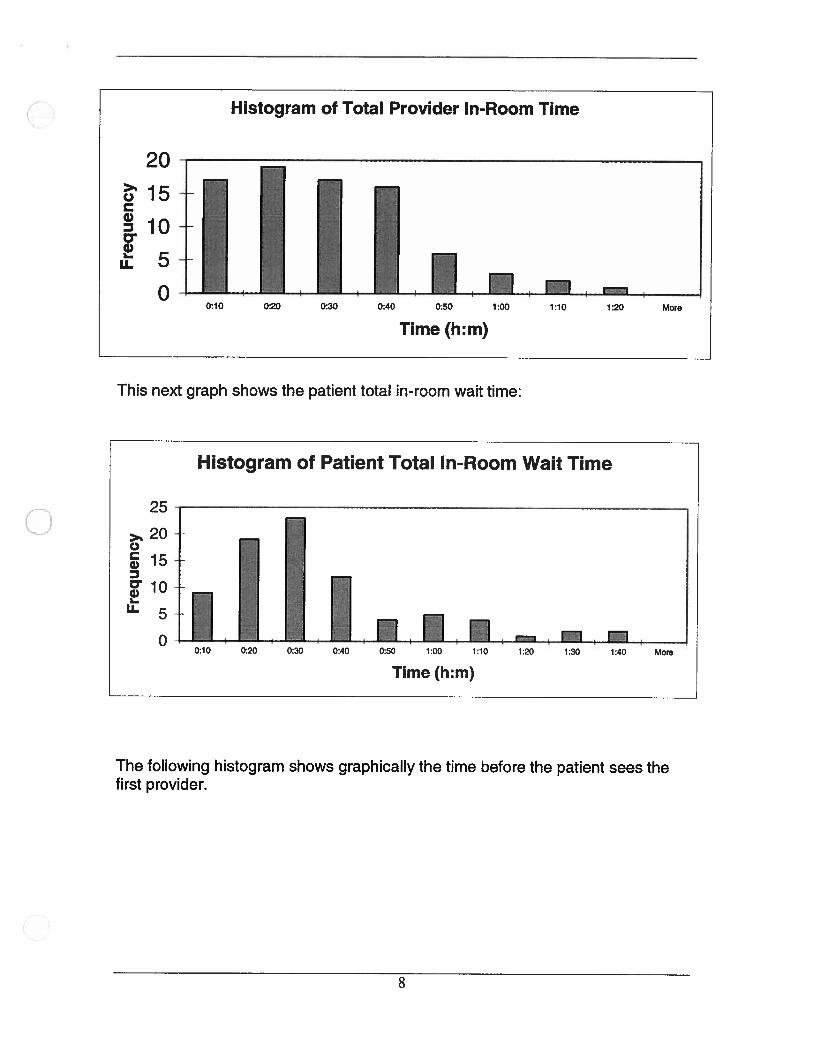
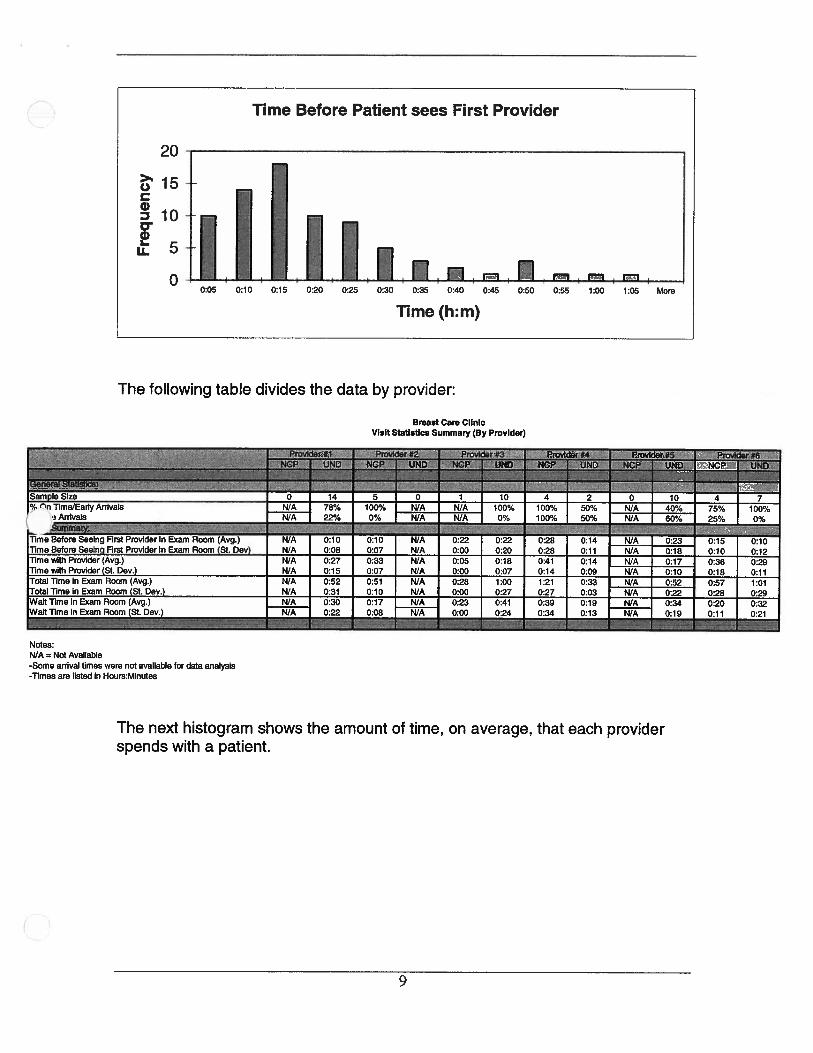
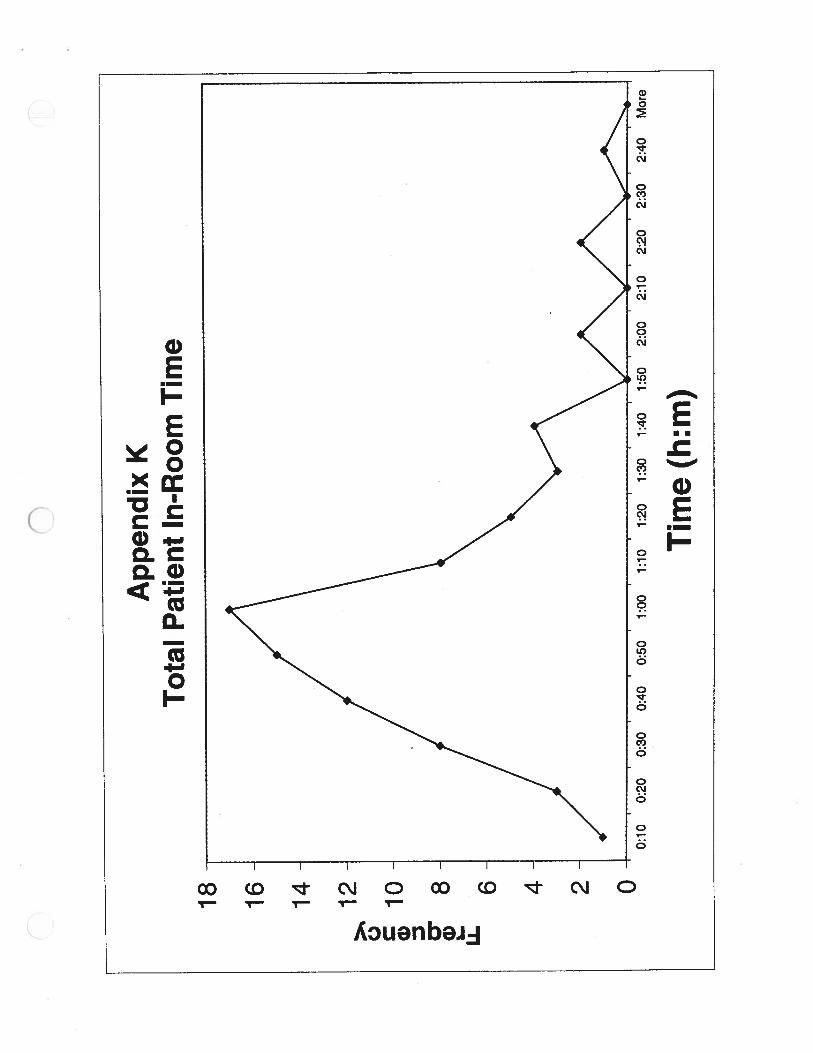
This next graph shows the patient total in-room wait time:
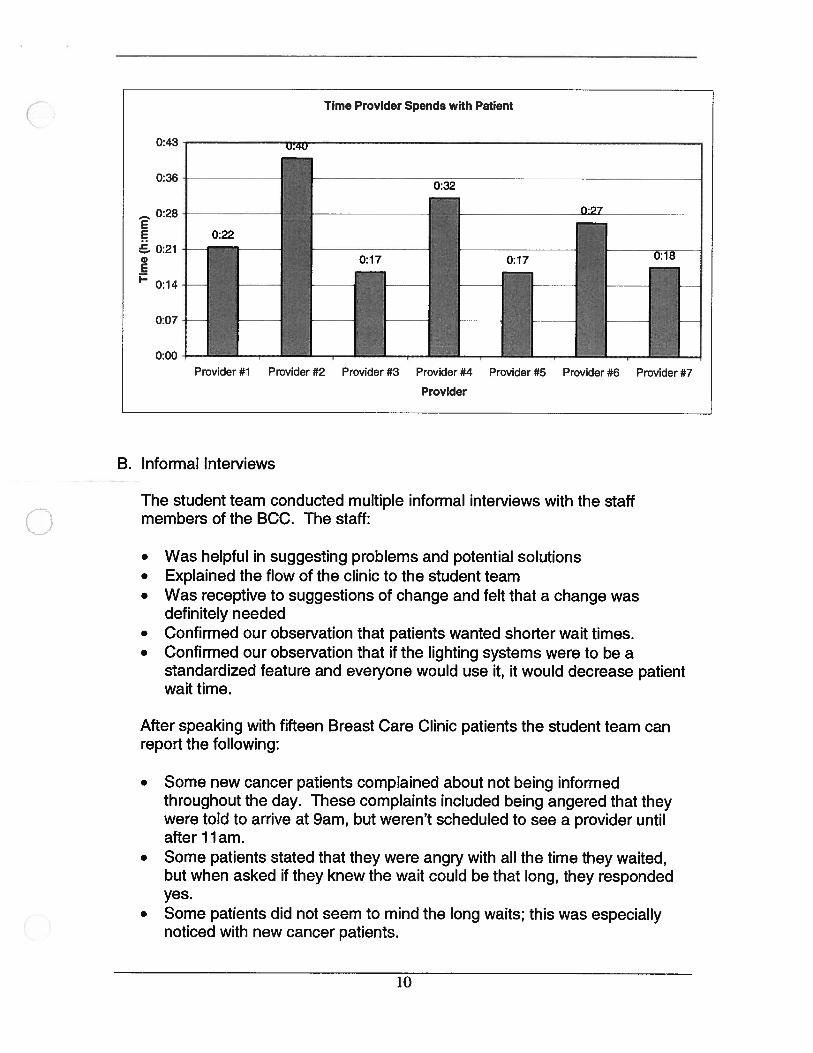
The following histogram shows graphically the time before the patient sees thefirst provider.
20
Histogram of Total Provider In-Room Time
15C.)
0
d)Li.
10
5
00:10 0:20 0:30 0:40 0:50 1:00 1:10 1:20 More
Time (h:m)
Histogram of Patient Total In-Room Wait Time
25
>. 20C.)
.1oLi.5
0
Time (h:m)
8
The following table divides the data by provider:
Notes:N/A = Not Available-Some arrival times were not available for data analysis-Times are listed in Hours:Minutes
N/A 78% 100% N/A N/AN/A 22% 0% N/A N/A
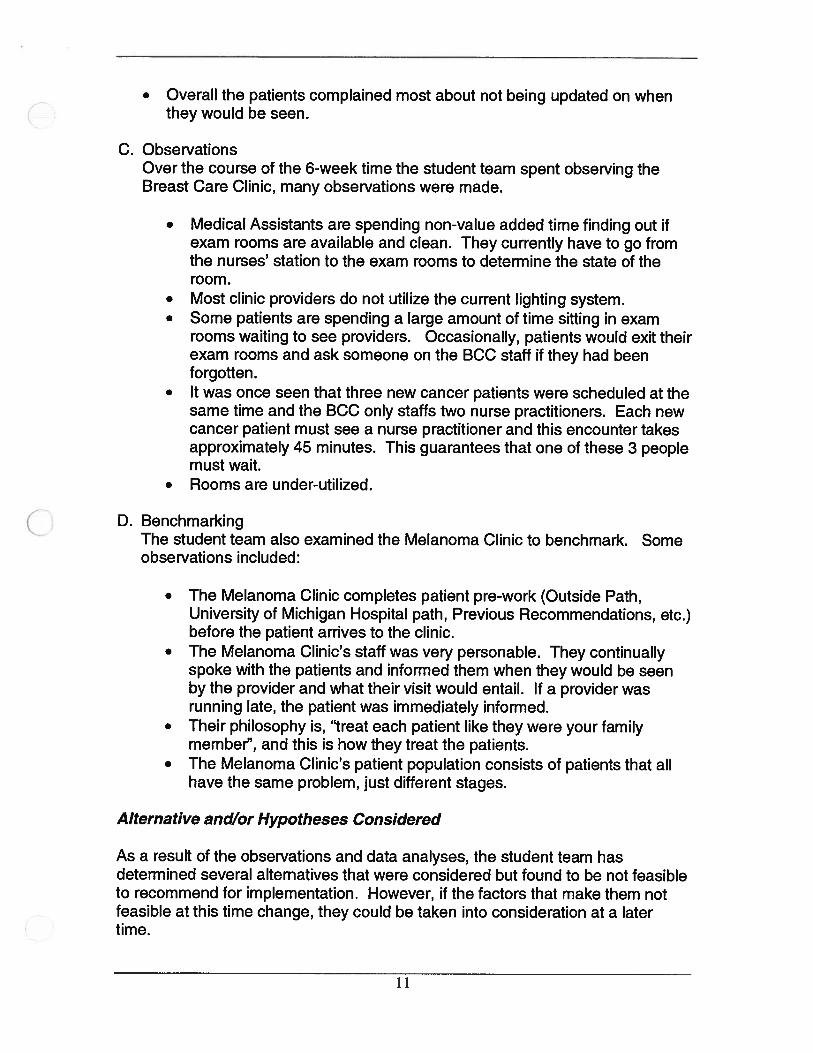
The next histogram shows the amount of time, on average, that each providerspends with a patient.
Breast Care ClinicVisit Statistics Summary (By Provider)
100%0%
100%100%
50%50%
i.-...Time Before Seeing First Provider in Exam Room (Avg.) N/A 0:10 0:10 N/A 0:22 0:22 0:28 0:14 N/A 0:23 0:15 0:10Time Before Seeinci First Provider in Exam Room (St. 0ev) N/A 0:08 0:07 N/A 0:00 0:20 0:28 0:11 N/A 0:18 0:10 0:12Time with Provider (Avg.) N/A 0:27 0:33 N/A 0:05 0:18 0:41 0:14 N/A 0:17 0:36 0:29TimewilhProvider(St.Dev.) N/A 0:15 0:07 N/A 0:00 0:07 0:14 0:09 N/A 0:10 0:18 0:11Total Time in Exam Room (Avg.) N/A 0:52 0:51 N/A 0:28 1:00 1:21 0:33 N/A 0:52 0:57 1:01Total Time in Exam Room (St. 0ev.) N/A 0:31 0:10 N/A 0:00 0:27 0:27 0:03 N/A 0:22 0:28 0:29Wait Time in Exam Room (Avg.) N/A 0:30 0:17 N/A 0:23 0:41 0:39 0:19 N/A 0:34 0:20 0:32Wait Time in Exam Room (St. 0ev.) N/A 0:22 0:08 N/A 0:00 0:24 0:34 0:13 N/A 0:19 0:11 0:21
--
N/A 40%N/A 60%
75%25%
100%0%
9
Time Provider Spends with Patient
B. Informal Interviews
The student team conducted multiple informal interviews with the staffmembers of the BCC. The staff:
• Was helpful in suggesting problems and potential solutions• Explained the flow of the clinic to the student team• Was receptive to suggestions of change and felt that a change was
definitely needed• Confirmed our observation that patients wanted shorter wait times.• Confirmed our observation that if the lighting systems were to be a
standardized feature and everyone would use it, it would decrease patientwait time.
After speaking with fifteen Breast Care Clinic patients the student team canreport the following:
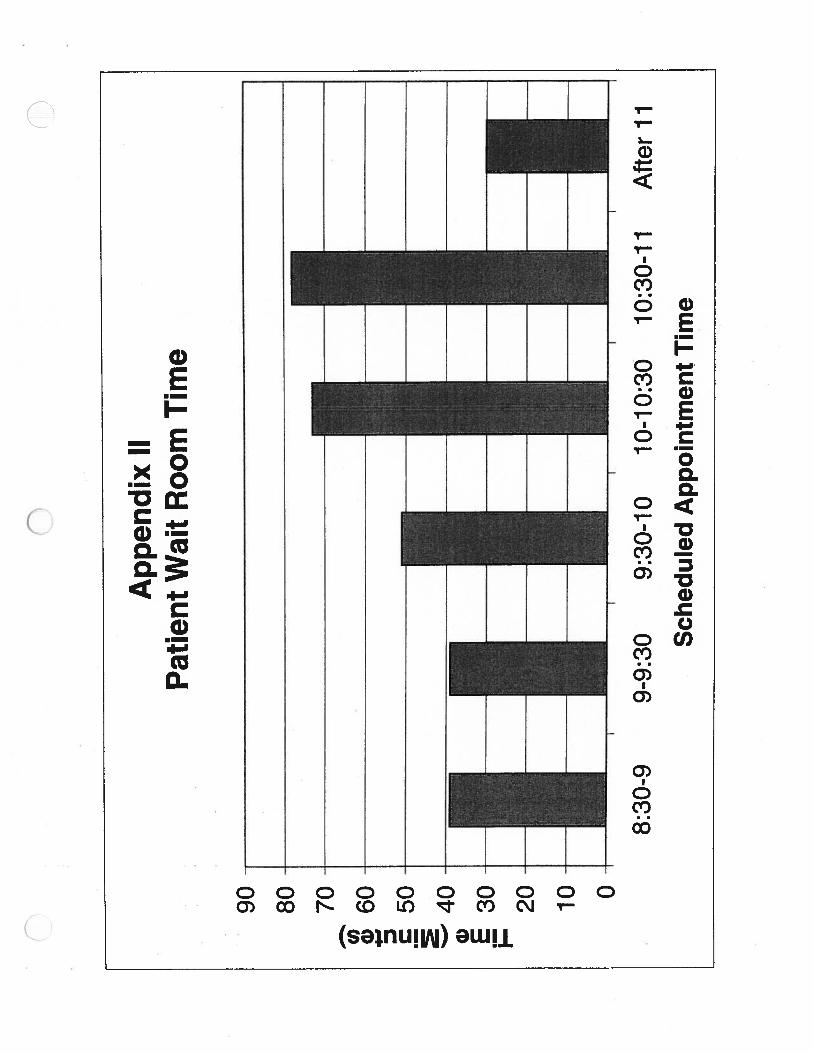
• Some new cancer patients complained about not being informedthroughout the day. These complaints included being angered that theywere told to arrive at 9am, but weren’t scheduled to see a provider untilafter 11am.
• Some patients stated that they were angry with all the time they waited,but when asked if they knew the wait could be that long, they respondedyes.
• Some patients did not seem to mind the long waits; this was especiallynoticed with new cancer patients.
0:43
0:36
__
0:28EEG 0:21
0:14
0:07
0:00
Provider #1 Provider #2 Provider #3 Provider #4 Provider #5 Provider #6 Provider #7
Provider
10
• Overall the patients complained most about not being updated on whenthey would be seen.
C. ObservationsOver the course of the 6-week time the student team spent observing theBreast Care Clinic, many observations were made.
• Medical Assistants are spending non-value added time finding out ifexam rooms are available and clean. They currently have to go fromthe nurses’ station to the exam rooms to determine the state of theroom.
• Most clinic providers do not utilize the current lighting system.• Some patients are spending a large amount of time sitting in exam
rooms waiting to see providers. Occasionally, patients would exit theirexam rooms and ask someone on the BCC staff if they had beenforgotten.
• It was once seen that three new cancer patients were scheduled at thesame time and the BCC only staffs two nurse practitioners. Each newcancer patient must see a nurse practitioner and this encounter takesapproximately 45 minutes. This guarantees that one of these 3 peoplemust wait.
• Rooms are under-utilized.
D. BenchmarkingThe student team also examined the Melanoma Clinic to benchmark. Someobservations included:
• The Melanoma Clinic completes patient pre-work (Outside Path,University of Michigan Hospital path, Previous Recommendations, etc.)before the patient arrives to the clinic.
• The Melanoma Clinic’s staff was very personable. They continuallyspoke with the patients and informed them when they would be seenby the provider and what their visit would entail. If a provider wasrunning late, the patient was immediately informed.
• Their philosophy is, “treat each patient like they were your familymember”, and this is how they treat the patients.
• The Melanoma Clinic’s patient population consists of patients that allhave the same problem, just different stages.
Alternative and/or Hypotheses Considered
As a result of the observations and data analyses, the student team hasdetermined several alternatives that were considered but found to be not feasibleto recommend for implementation. However, if the factors that make them notfeasible at this time change, they could be taken into consideration at a latertime.
11
A. Drop off of Mammograms
The student team considered having patients drop off their mammogramsbefore their Monday clinic appointment. This would allow additionalmammogram views to be taken before the Monday clinic; thus allowingpatients to arrive at their scheduled appointment time, not all at 9:00AM. Thiswould considerably reduce their wait time. This is not feasible at this timebecause some patients live too far away to come in twice, they just want tocome in for one day and have everything done. Another reason is because itrequires rework by radiology. The radiologists would have to read thepatients mammograms before their appointment and then reread themammograms on the day of the patient’s appointment.
B. Ship Mammograms
The student team also considered having the patient’s ship theirmammograms to the BCC before their Monday clinic appointment. Thiswould allow the patient to schedule an appointment with the radiologydepartment in order to have additional views taken. This would lead toimproved patient scheduling in the BCC because then the patients who didnot need additional views could just come at their appointment time and thepatients who did need additional view could come in at their scheduledradiology appointment. The current system of hand carrying themammograms has been determined to be the most efficient making this notreasonable. There is also an excessive cost of reading outsidemammograms with little reimbursement and many people do not show lead tonot implementing this consideration.
Conclusions
• Patients are experiencing added wait time in the waiting room because theBCC staff is not utilizing the lighting system. If all BCC staff used thelighting system then the MA’s would not have to spend time walking to theexam rooms to see if the rooms are available to put patients in. This timeis added time that the patient has to wait in the wait room.
• Many patients are spending more time with their provider than is allocatedfor them in the clinic schedule.
• Patients are uninformed about when they will see their provider and howtheir visit schedule will proceed.
• Patients are experiencing long wait times in exam rooms.• Breast Care Clinic is over scheduling.
12
Recommendations
• Further explore splitting the multidisciplinary clinic into 2 clinics, one fornew cancer patients and one for follow up visits (post-surgery). Patientsare dissatisfied with long waits that occur. The clinic could be split into 2half days, one to see the nurse practitioner (for the new cancer patients),and one for the second half of the new cancer patients treatment and forthe follow up visits. This would still require only one tumor board thatwould take place at the second clinic. All patients would still have thebenefits of the multidisciplinary clinic; they would just not have to stay inthe clinic for an entire day. Patients who are traveling a long distancewould have the option of either coming for an entire day, or utilizing theprospective new system of the split clinic.
• Further explore splitting the clinics into 2 separate days, one for theundiagnosed clinics and one for the multidisciplinary clinic. This wouldallow the clinic to utilize all their doctors for each clinic, each week.
• Standardize usage of lighting system. Not all providers are currently usingthe lighting system. This is causing the MA’s to spend time checkingrooms to make sure they are available before taking a patient back to theexam room. MA’s are then unable to complete other tasks, such asinforming patients when doctors are late. With standardized usage of thelighting system by all clinic staff, MA’s would not need to check the roomsbefore taking a patient back. MA’s could simply look at the light board todetermine available rooms. It must be stressed, however, that all staffmust use the system or it will not be fully effective.
• Make patient visits more personal. Since nobody visits the patients oncethey enter an exam room until the provider comes, some patients feel thatthey have been forgotten. By having an MA or available staff person gointo exam rooms with patients waiting, the patients feel like they are beingattended to. This does not significantly decrease overall wait time, butbecause the patients are constantly being attended to, they do not feel asdissatisfied with their wait. Also, if the lighting system is used effectively,MA’s will have time available so that they can speak with the patientswhen doctors are running late.
• Look further into changing patient duration scheduling. Because patientsare being scheduled for times shorter than their actual provider times,doctors get overloaded and cannot see patients at their scheduled times,This causes the patients to wait longer in the exam room to see theprovider. By scheduling for longer appointment duration times, patientswill have less wait time in the exam room.
13

• Perform pre-work for patients, similar to the pre-work done for the patientsin the Melanoma clinic, before the patient comes in for their appointment.Include data such as who the patient was referred by, their path outside ofthe University of Michigan health system, their University of Michiganhealth system path so far, and recommendations up to this point.
Action Plan
A. Lighting System
To implement the lighting system, all clinic staff needs to be trained on theusage of the lighting system. It should be known clinic wide that the lightingsystem is an essential way to keep the clinic running efficiently. This shouldbe implemented immediately. The lighting system is already in place so therewould be no extra cost involved with this recommendation. The providersneed to be taught how the system works and they need to use it every time.A Breast Care Clinic supervisor should implement this.
B. Personalization
Hold an informational seminar, available to all clinic staff, on customer serviceto aid in personalizing service. This can be implemented whenever a seminarcan be scheduled. A Breast Care Clinic supervisor should implement this.
C. Splitting Clinics
Explore options of having undiagnosed and diagnosed clinics on separatedays. This would require extensive financial and scheduling analysis todetermine feasibility. A Breast Care Clinic supervisor should implement this.
14
Definitions
The following definitions are needed in order to understand report content:
Early arrival Patient arrives before their scheduledappointment time.
Encounters When a patient is being seen by anycombination of providers.
FNA A fine needle aspiration.
NP A new patient.
Non-value-added time Any time the patient is not with any type ofprovider (waiting time).
Provider/Clinician A faculty or staff member, including Physicians,Residents, Fellows, Medical Assistants,Physician’s Assistants, Nurses, NursePractitioners, or Clerks.
RV A return visit.
Room utilization The percentage of time a patient is in theexamination room.
Time with provider The time a patient is with a provider.
Value-added time The time spent with a provider.
Visit duration The total amount of time the patient spends in the clinic.
15
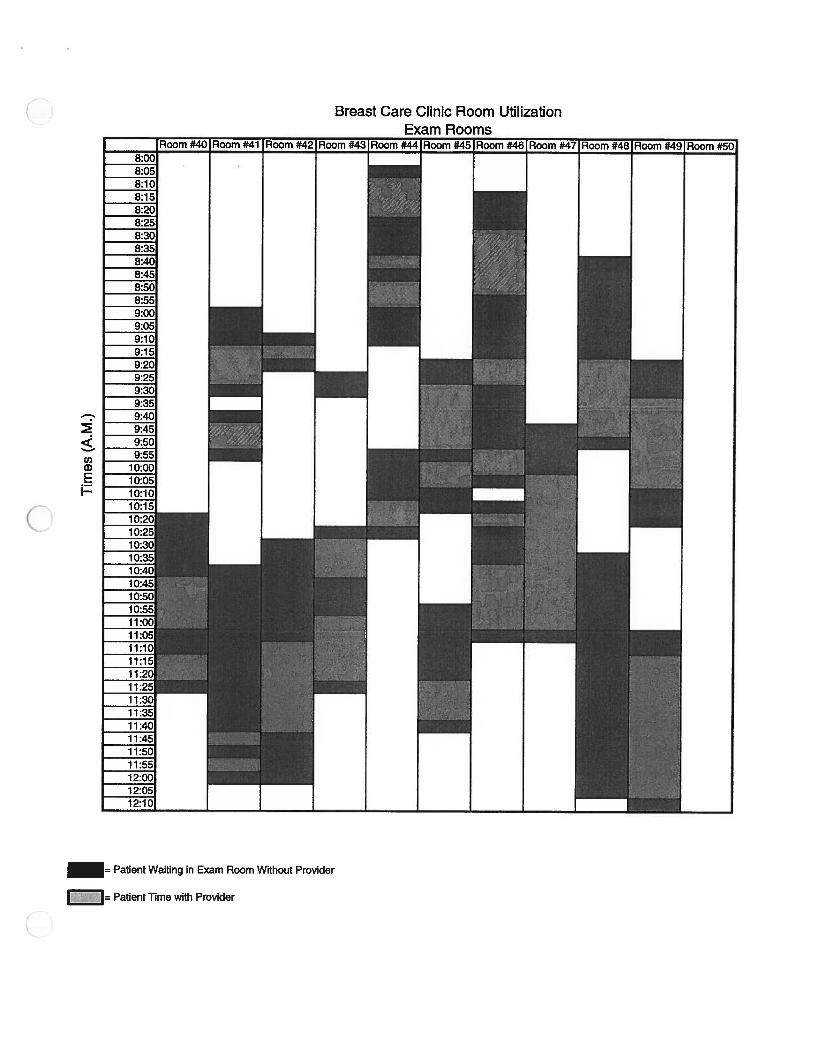
Cl)a)BI-
= Patient Waiting in Exam Room Without Provider
Patient Time with Provider
Breast Care Clinic Room Utilization
App
endi
xA
Bre
ast
Car
eC
lini
cS
umm
ary
Sta
tist
ics
All
Pat
ient
sN
ewC
ance
rP
atie
nts
Und
iagn
osed
Pat
ient
s
Cat
egor
yA
vera
geSt
.D
ev.
%of
Pat
ient
sA
vera
geSt
.D
ev.
%of
Pat
ient
sA
vera
geSt
.D
ev.
%of
Pat
ient
s
Gen
eral
Sta
tist
ics:
100%
2126
%60
74%
#P
atie
nts
81#
Lat
eA
rriv
als
1822
%7
39%
1161
%L
ate
Tim
e0:
250:
200:
370:
220:
180:
16
Key
Tim
esS
umm
ary:
Pro
vide
rTim
e*0:
240:
140:
340:
150:
210:
12E
xam
Roo
mT
ime
0:55
0:27
1:00
0:22
0:53
0:28
Not
es:
*pro
vide
rtim
eis
the
aver
age
tim
ew
ithan
ycl
inic
ian
per
visi
t.-T
imes
are
liste
din
Hou
rs:M
inut
es
Sam
ple
Siz
e=
81P
atie
nts
Appen
dix
BB
reas
tC
are
Cli
nic
Tim
elin
eD
urat
ion
Sum
mar
yS
tati
stic
s
________
All
Pat
ient
sN
ewC
ance
rP
atie
nts
Und
iagn
osed
_Pat
ents
Cat
eqor
yA
vera
geSt
.D
ev.
%of
Pat
ient
sA
vera
geSt
.D
év.
%of
Pat
ient
sA
vera
geSt
.D
ev.
%of
Pat
ient
s
zz
zzT
imel
ine:
Wai
tfo
rE
ncou
nter
1N
V*
0:15
0:15
100%
0:19
0:19
100%
0:13
0:14
100%
Enc
ount
er1
V**
0:18
0:13
100%
0:29
0:16
100%
0:14
0:09
100%
Wai
tfo
rE
ncou
nter
2N
V0:
110:
1463
%0:
050:
0348
%0:
130:
1568
%
Enc
ount
er2
V0:
080:
0763
%0:
090:
0948
%0:
080:
0668
%
Wai
tfo
rE
ncou
nter
3N
V0:
080:
0815
%0:
020:
005%
0:09
0:08
18%
Enc
ount
er3
V0:
070:
1015
%0:
010:
005%
0:07
0:10
18%
Exi
ttim
e***
NV
0:06
0:11
100%
0:04
0:07
100%
0:07
0:12
100%
—__
EE
ZA
vera
geT
otal
Exa
mR
oom
Tim
e***
*0:
530:
580:
51V
alue
Add
edTi
me*
***
—0:
240:
330:
20N
on-V
alue
Add
edTi
me*
***
—0:
300:
250:
30%
Val
ueA
dded
Tim
e—
44%
57%
40%
Not
es:
*N
V=
Non
valu
ead
ded
tim
e**
V=
Val
uead
ded
tim
eE
xit
tim
eis
the
tim
ebe
twee
nth
ela
sten
coun
ter
apa
tien
tha
sun
tilth
eti
me
that
they
exit
the
room
.**
**A
vera
geT
otal
Exa
mR
oom
Tim
e,V
alue
Add
edT
ime
and
Non
-Val
ueA
dded
Tim
ear
eth
esu
mof
each
even
tsti
me
mul
tiplie
dby
the
%of
pati
ents
that
expe
rien
ced
that
even
t.-T
imes
are
list
edin
Hou
rs:M
inut
es
Sam
ple
Siz
e=
81P
atie
nts

App
endi
xC
Bre
ast
Car
eC
lini
cV
isit
Sta
tist
ics
Sum
mar
y(B
yP
rovi
der)
Prov
ider
#1Pr
ovid
er#2
Prov
ider
#3Pr
ovid
er#4
Prov
ider
#5Pr
ovid
er#6
Prov
ider
#7N
CP
UN
DN
CP
UN
DN
CP
UN
DN
CP
UN
DN
CP
UN
DN
CP
UN
DN
CP
UN
D
tatistcs:
Sam
ple
Siz
e0
145
01
104
2-
010
47
613
%O
nT
im&
Ear
lyA
rriv
als
N/A
78%
100%
N/A
N/A
100%
100%
50%
N/A
40%
75%
100%
N/A
71%
%L
ate
Arr
ival
sN
/A22
%0%
N/A
WA
0%10
0%50
%N
/A60
%25
%0%
N/A
29%
Tim
eSu
mm
ary:
Tim
eB
efor
eS
eein
gFi
rst
Pro
vide
rin
Exa
mR
oom
(Avg
.)N
/A0:
100:
10W
A0:
220:
220:
280:
14N
/A0:
230:
150:
100:
210:
09
Tim
eB
efor
eS
eein
gFi
rst
Pro
vide
rin
Exa
mR
oom
(St.
Dev
)N
/A0:
080:
07N
/A0:
000:
200:
280:
11N
/A0:
180:
100:
120:
170:
06
Tim
ew
ithP
rovi
der(
Avg
.)N
/A0:
270:
33N
/A0:
050:
180:
410:
14N
/A0:
170:
360:
290:
290:
13T
ime
with
Pro
vide
r(S
t.D
ay.)
N/A
0:15
0:07
N/A
0:00
0:07
0:14
0:09
N/A
0:10
0:18
0:11
0:17
0:09
Tot
alT
ime
inE
xam
Roo
m(A
vg.)
N/A
0:52
0:51
N/A
0:28
1:00
1:21
0:33
N/A
0:52
0:57
1:01
1:01
0:40
Tot
alT
ime
inE
xam
Roo
m(S
t.D
ev.
N/A
0:31
0:10
N/A
0:00
0:27
0:27
0:03
N/A
0:22
0:28
0:29
0:19
0:20
Wai
tT
ime
inE
xam
Roo
m(A
vg.)
N/A
0:30
0:17
N/A
0:23
0:41
0:39
0:19
N/A
0:34
0:20
0:32
0:31
0:27
Wai
tT
ime
inE
xam
Roo
m(S
t.D
ev.)
N/A
0:22
0:08
N/A
0:00
0:24
0:34
0:13
N/A
0:19
0:11
0:21
0:19
0:19
Not
es:
N/A
=N
olA
vaila
ble
5om
ear
riva
ltim
esw
ere
not
avai
labl
efo
rda
taan
alys
is-T
imes
are
liste
din
Hou
rs:M
irru
tes
Sam
ple
Size
=76
Pat
ient
s
nC)
App
endi
xD
Tot
alP
atie
ntIn
Exa
mR
oom
Tim
e
2:52
2:24
1:55
E &1:
26a) E iz
0:57
0:28
0:00
Pat
ien
ts

\.I
Ap
pen
dix
ET
otal
Pat
ient
In-R
oom
Wai
tT
ime
1:40
-
1:26
-
1:12
-
£O
:57
C) p043
+•
+
0:28
-
0:14
0:00
Pat
ient
s

1:04
0:57
0:50
0:43
0:36
0:28
0:21
0:14
0:07
0:00
n
App
endi
xF
Wai
tT
ime
InE
xam
Roo
mB
efor
eP
atie
nt
See
sF
irst
Pro
vid
er
E G) E iz
Pat
ients

0.
App
endi
xG
Tot
alP
rovi
der
InE
xam
Roo
mT
ime
1:12
1:04
0:57
0:50
__
0:43
E £0:
36a) .
0:28
0:21
0:14
0:07
0:00
Pat
ien
ts
•V
alue
-Add
edT
ime
LJN
on-V
alue
-Add
edT
ime
n
Ap
pen
dix
HT
otal
Pat
ient
In-R
oom
Tim
e
44%
56%
00
App
endi
xI
Pat
ients
Tha
tW
aite
dIn
Wai
ting
Roo
m
•P
atie
nts
Tha
tD
idN
otW
ait
DP
atie
ntT
hat
Wai
ted
>1
0 C 0•
G) L1
App
endi
xJ
His
togr
amof
Tot
alP
atie
ntIn
-Roo
mT
ime
18 16 14 12 10 8 6 4 2 00:
100:
200:
300:
400:
501:
001:
101:
201:
301:
401:
502:
002:
102:
202:
302:
40M
ore
Tim
e(h
:m)
BC
CD
ata
Ana
lysi
s
>1
0 0 a) LL.
2 0
App
endi
xK
Tot
alP
atie
ntIn
-Roo
mT
ime
0:10
0:20
0:30
0:40
0:50
1:00
1:10
1:20
1:30
1:40
1:50
2:00
2:10
2:20
2:30
2:40
Mor
e
Tim
e(h
:m)
n
18 16 14 12 10 8 6 4
20 18 16 14 12 10 8 6 4 2 0
App
endi
xL
His
togr
amof
Tot
alP
rovi
der
In-R
oom
Tim
e
C.) C G) z a) LI
0:10
0:20
0:30
0:40
0:50
1:00
1:10
1:20
Tim
e(h
:m)
Mor
e
BC
CD
ata
Ana
lysi
s
0 C z 0• a) LL
App
endi
xM
Tot
alP
rovi
der
In-R
oom
Tim
e
Tim
e(h
:m)
20 18 16 14 12 10 8 6 4 2 00:
100:
200:
300:
400:
501:
001:
101:
20M
ore
Cl)
4-’ C .! 4-’ 0 II 0 -o E z
Appen
dix
N(U
nd
iag
no
sed
)P
rovid
erIn
-Roo
mT
ime
25 20 15 10 5 0
0-10
10-2
020
-30
30-4
040
-50
50-6
0M
ore
Tim
ein
Min
utes
NumberofPatients-LL
C01001001
N2: \co
o/CD
/0.
7II —.
CA)I cpCDX—.CJ—
/C
/01/o 0/
301/-‘C—.
0CD
0-‘CD
Cl)
C .! II 0 II 0 G) . E z
0-10
10-2
020
-30
30-4
040
-50
Tim
ein
Min
utes
50-6
0M
ore
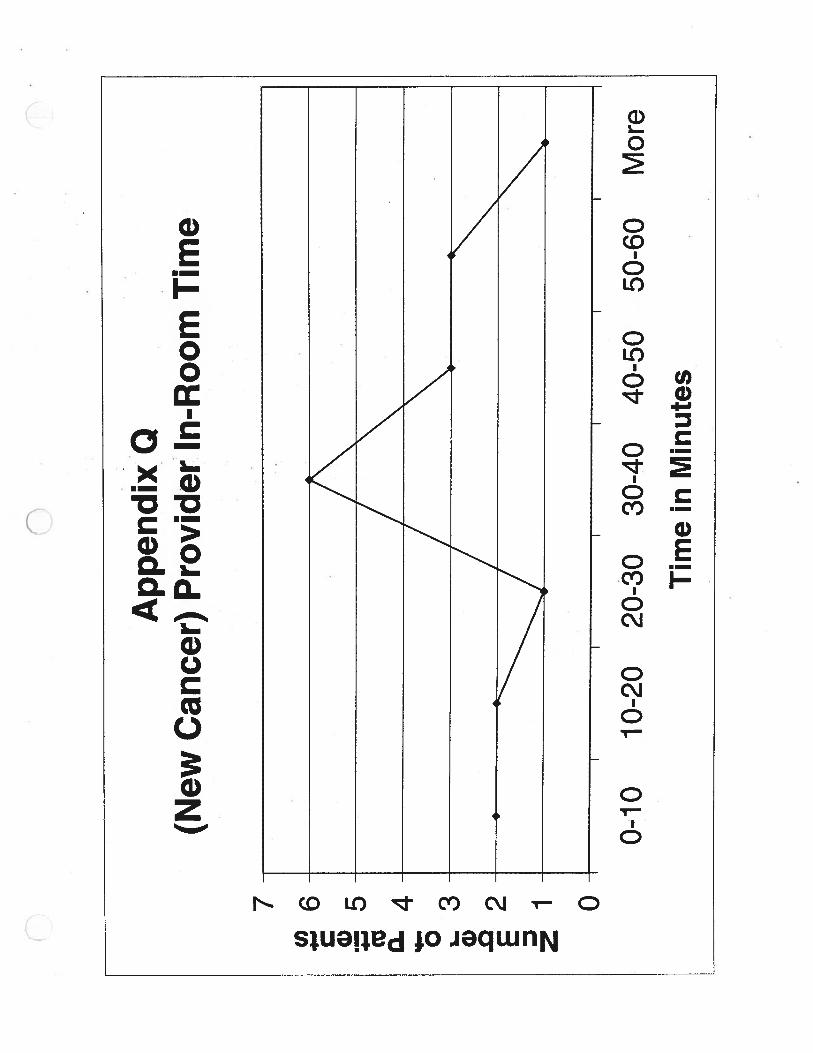
App
endi
xP
(New
Can
cer)
Pro
vid
erIn
-Roo
mT
ime
7 6 5 4 3 2 1 0
Cl)
(U 0 0 a) E 3 z
App
endi
x0
(New
Can
cer)
Pro
vide
rIn
-Roo
mT
ime
7 6 5 4 3 2 1 0
10-2
00-
1020
-30
30-4
040
-50
50-6
0M
ore
Tim
ein
Min
utes
0 a) z 0 a) U-
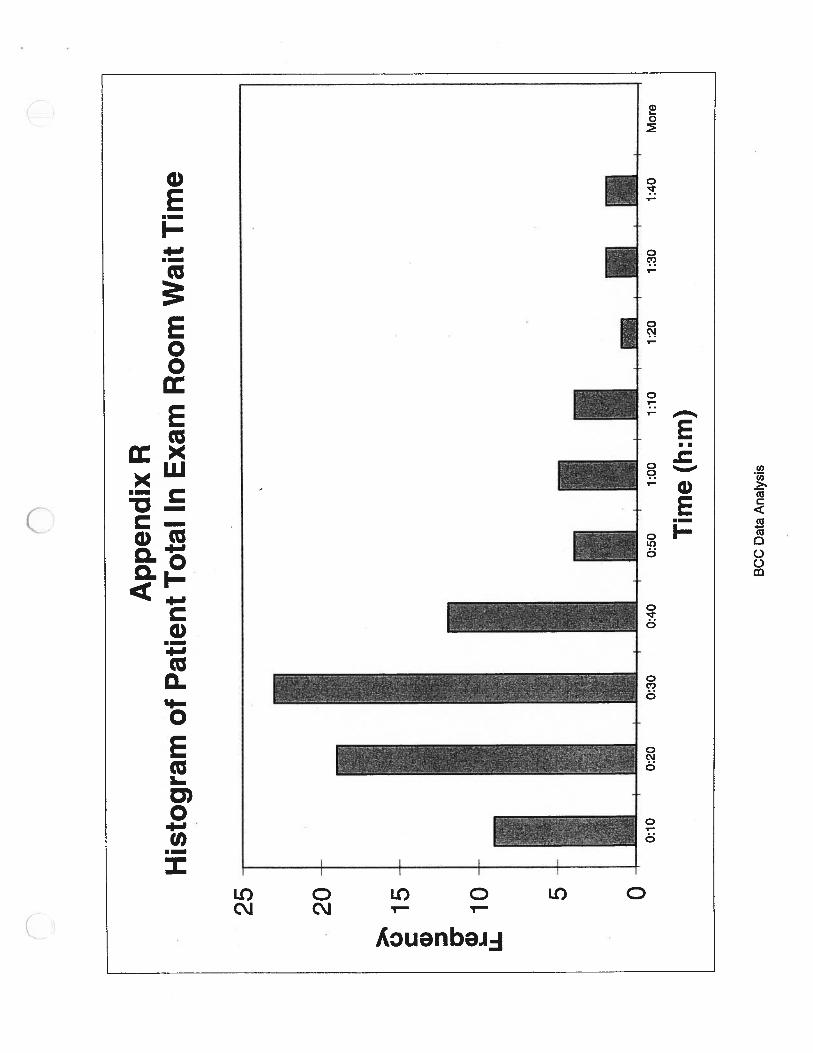
25
App
endi
xR
His
tog
ram
ofP
atie
nt
Tot
alIn
Exa
mR
oom
Wai
tT
ime
20 15 10 5 0
Tim
e(h
:m)
BC
CD
ata
Ana
lysi
s
C.)
0•
I U-
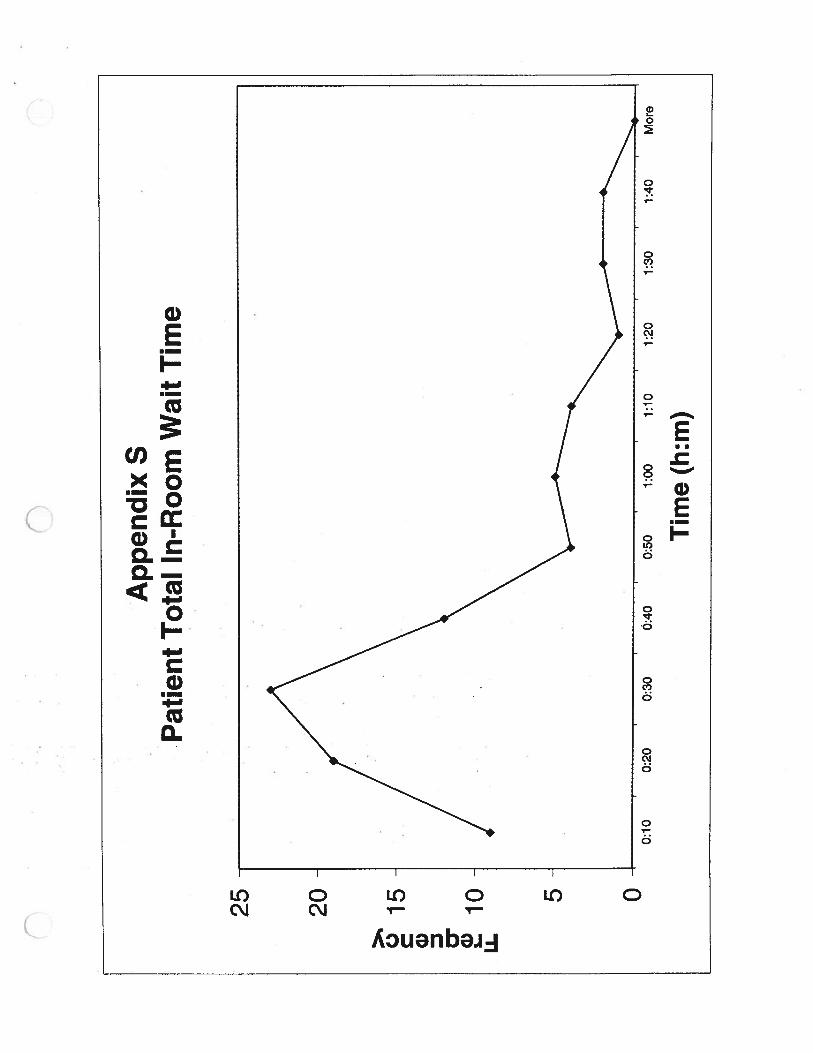
Appen
dix
SP
atie
nt
Tot
alIn
-Roo
mW
ait
Tim
e
nC
25 20 15 10 5 00:
100:
200:
300:
400:
501:
001:
101:
201:
301:
40M
ore
Tim
e(h
:m)
0 z 0•
G) U-
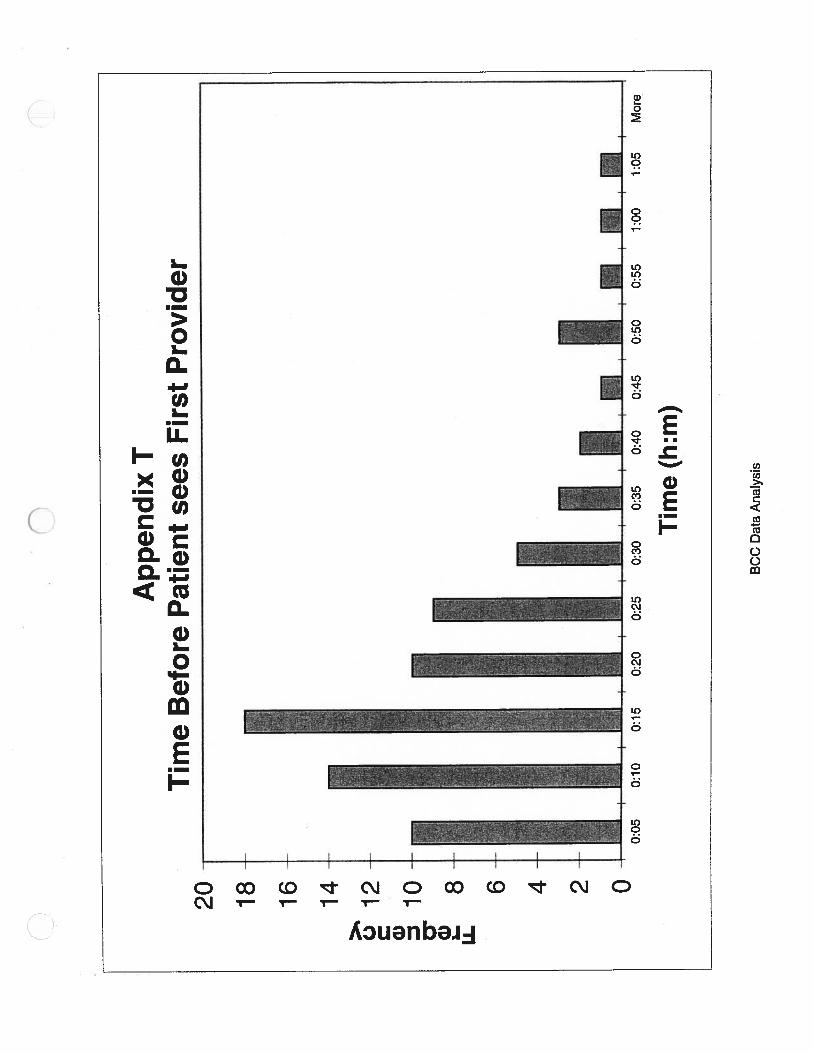
Appen
dix
TT
ime
Bef
ore
Pat
ient
sees
Fir
stP
rovid
er20 18 16 14 12 10 8 6 4 2 0
0:05
0:10
0:15
0:20
0:25
0:30
0:35
0:40
0:45
0:50
0:55
1:00
1:05
Mor
e
Tim
e(h
:m)
BC
CD
ata
Ana
lysi
s
:fl
fl
Ap
pen
dix
UT
imeB
efore
Pat
ien
tse
es
Fir
stP
rov
ider
20 18 16 14
01
2
10
0 a) U6 4 2 0
0:05
0:10
0:15
0:20
0:25
0:30
0:35
0:40
0:45
0:50
0:55
1:00
1:05
Mor
e
Tim
e(h
:m)

fl
C.) a) LL
App
endi
xV
His
togr
amof
Appontm
ents
Sta
rtin
gA
fter
Sch
edule
dT
ime
25 20 15 10 5 00:
100:
200:
30
11 1:00
1:10
1:20
Tim
e(h
:m)
1:30
1:40
1:50
2:00
Mor
e
BC
CD
ata
Ana
lysi
s
Ap
pen
dix
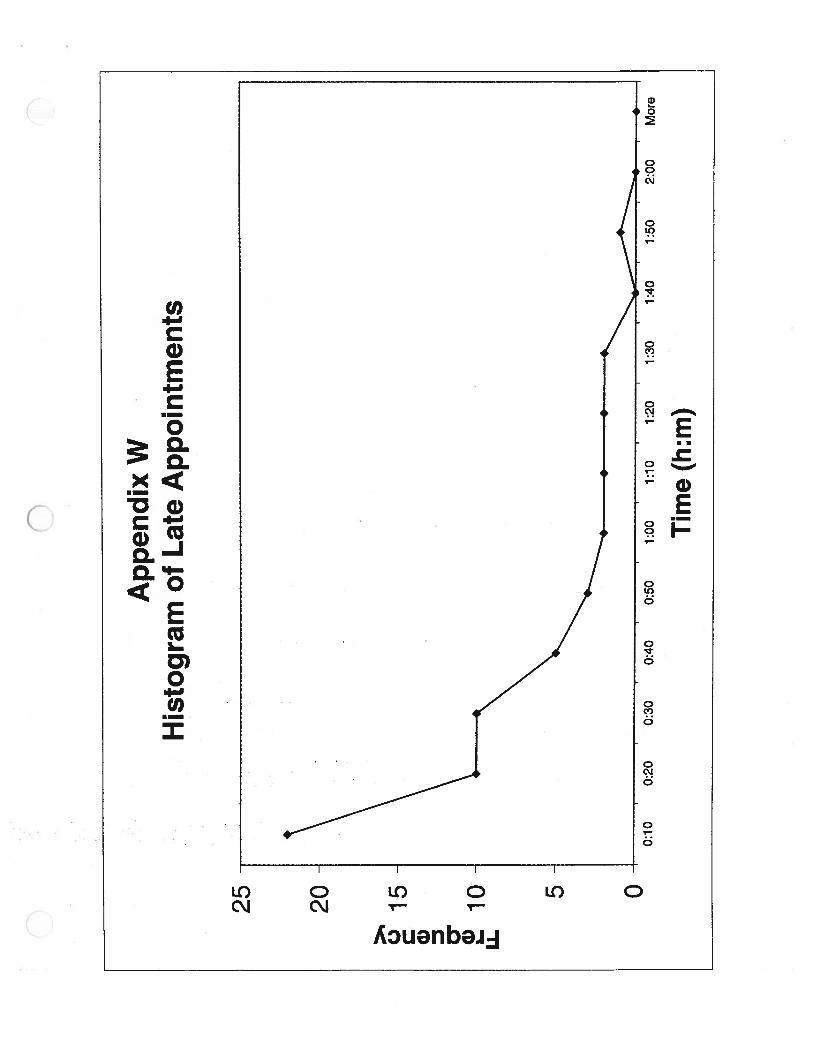
WH
isto
gra
mof
Lat
eA
pp
oin
tmen
ts
25-
20
>1 01
5
0• 1o
LL
5 0-
II
0:10
0:20
0:30
0:40
0:50
1:00
1:10
1:20
1:30
1:40
1:50
2:00
Mor
e
Tim
e(h
:m)
C.)
C G) 0 LL.
App
endi
xX
His
togr
amof
Val
ue-A
dded
In-R
oom
Tim
e
20 18 16 14 12
10 8 6 4 2-
0-
II
20%
25
%30
%35
%40
%45
%50
%55
%60
%M
ore
Per
centa
ge
ofV
alue
-Add
edT
ime
BC
CD
ata
Ana
lysi
s
>% 0 C G) I-
Li.
Tim
e(m
m)
70M
ore
App
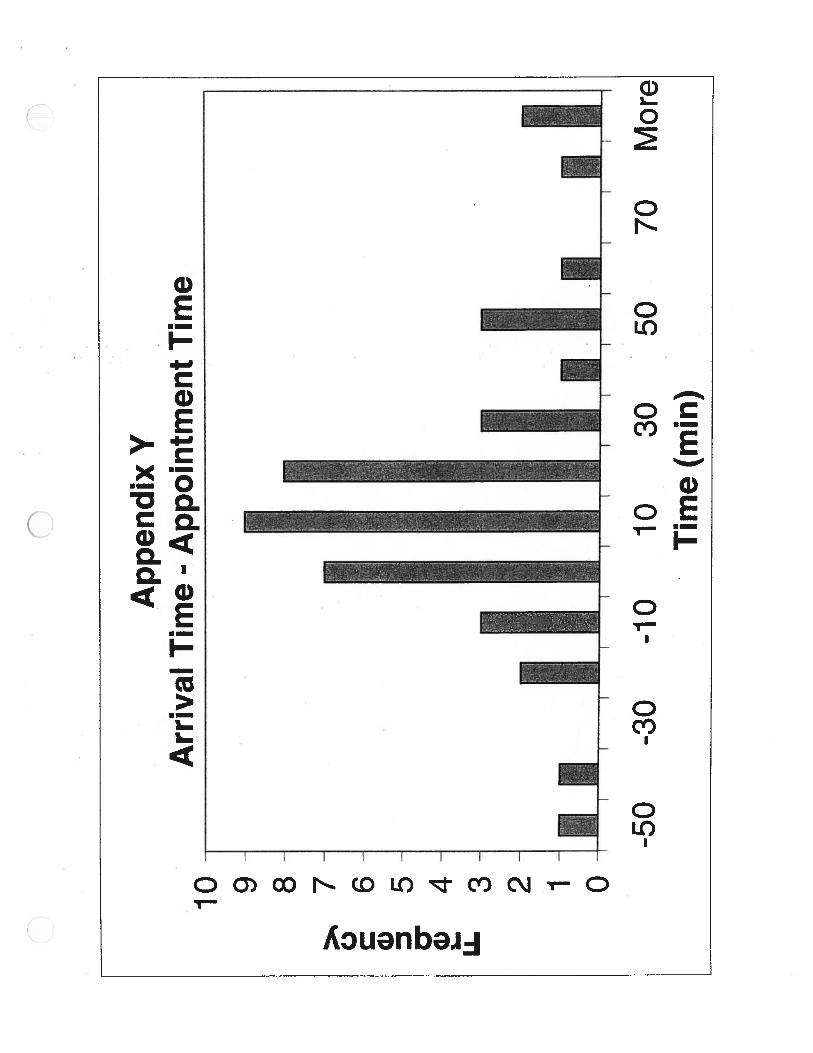
endi
xY
Arr
ival
Tim
e-
Appoin
tmen
tT
ime
10 9 8 7 6 5 4 3 2 1 0
-50
-30
-10
1030
50
C L.
LL
n
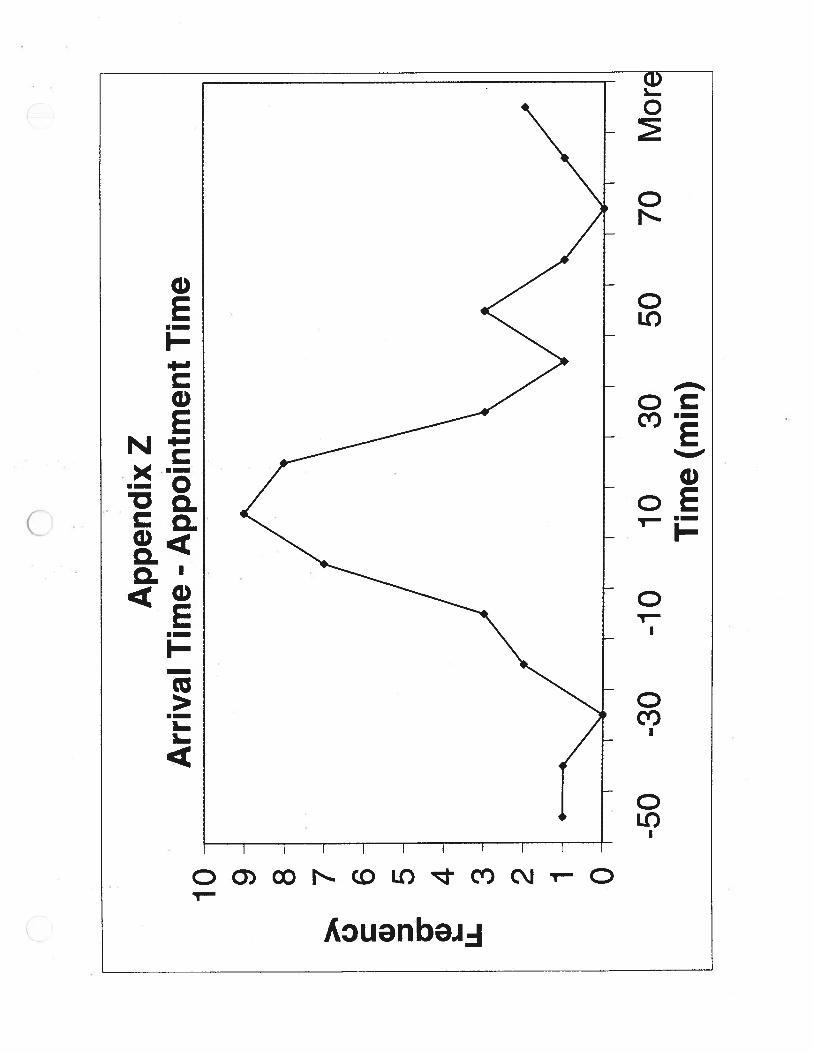
Appen
dix
ZA
rriv
alT
ime
-A
pp
oin
tmen
tT
ime
10 9 8 7 6 5 4 3 2 1 0
-50
-30
-10
1030
50T
ime
(mm
)70
Mor
E

L.C)V>o -
I— Eiz
. -g•1-’ -
0U)
E IU)
cC)
Cu
a)(I)0.
,l 0 a)
5— 0• • U)w
a)2
CD.—
V
D
I
C)
CD CC) C’.J C C
C C C C C
- (ww:q)ewij
V• —
oO a)
-3
-G)
-
-— a)—
X.—o• I..
yb
C’)
O-.—I— >0
D0a)2
-
CCu
C-)
zODT-C
(ww:q)aw
C.)C.)x
04)0.
a)EizC
•1-CD0.Va)C’)0Ca)Cu
CD
a)z
a)EI
a)
0
G)CoCu
Cl)
0
ci)EF-c,a)D
ci)-
0Co
Cci)
0
‘IC’4j
LC)
aC’)
0
Co
a 0
000
(ww:q) awii
0n
App
endi
xD
D
Ret
urn
Undia
gnose
dP
atie
nt
Tim
ew
ith
Pro
vide
r(b
ased
onL
ast
Pro
vide
rO
utof
Exa
mR
oom
Tim
em
inus
Fir
stP
rovi
der
InE
xam
Roo
mT
ime)
1:12
-
0:57
-
0:4
3-
.0:
28I-
0:14
0:00
Pat
ient
s
—+—
Tim
eP
rovi
der
Spe
ntW
ithP
atie
nt—
Schedule
dT
ime
n•0
App
endi
xE
EN
ewC
ance
rP
atie
nt
Tim
ew
ith
Pro
vid
er(b
ased
on
Las
tP
rovid
erO
utof
Exa
mR
oom
Tim
em
inu
sF
irst
Pro
vid
erIn
Exa
mR
oom
Tim
e)
1:26
1:12
i—0:
28
0:14
0:00
Pat
ients
Tim
eP
rovi
der
Spe
ntw
ithP
atie
nt—
Sch
edul
edT
ime
C)
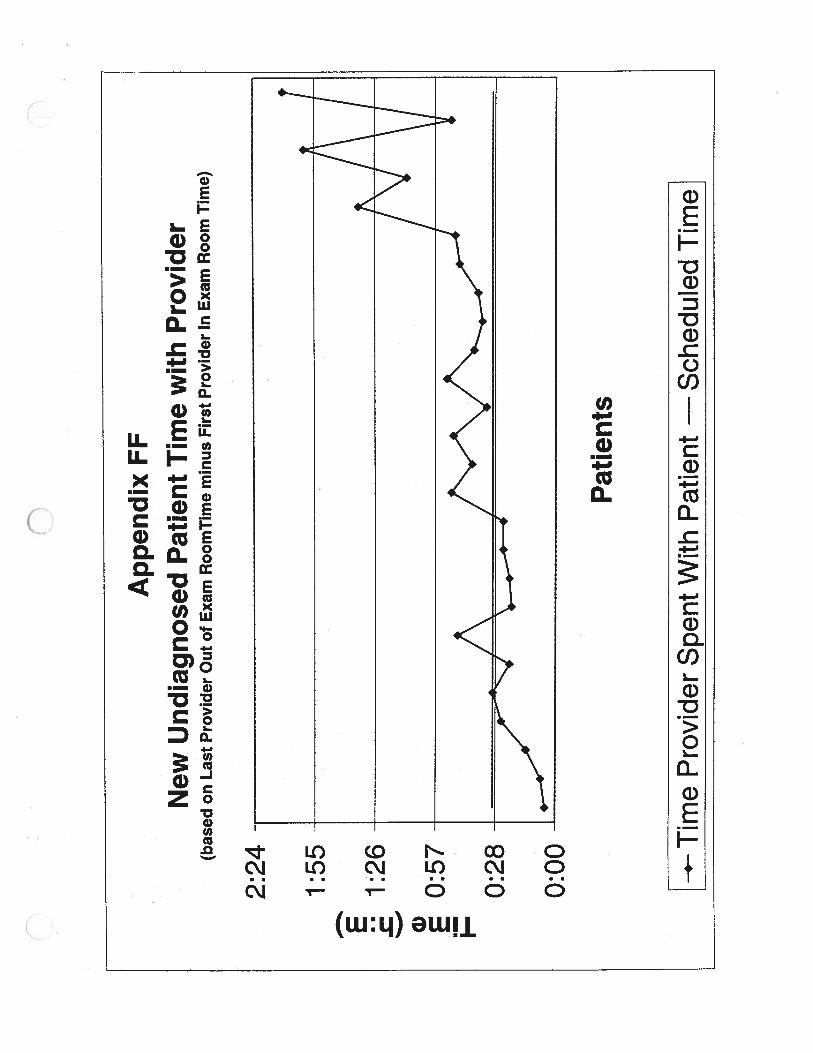
VA
ppen
dix
FF
New
Undia
gnose
dP
atie
nt
Tim
ew
ith
Pro
vid
er(b
ased
onL
ast
Pro
vide
rO
utof
Exa
mR
oom
Tim
em
inus
Fir
stP
rovi
der
InE
xam
Roo
mT
ime)
2:24
-
1:55
-
1:26
0:5
7-
Pat
ients
—.-T
ime
Pro
vide
rS
pent
With
Pat
ient
*S
ched
uled
Tim
e
E -C a) E I-
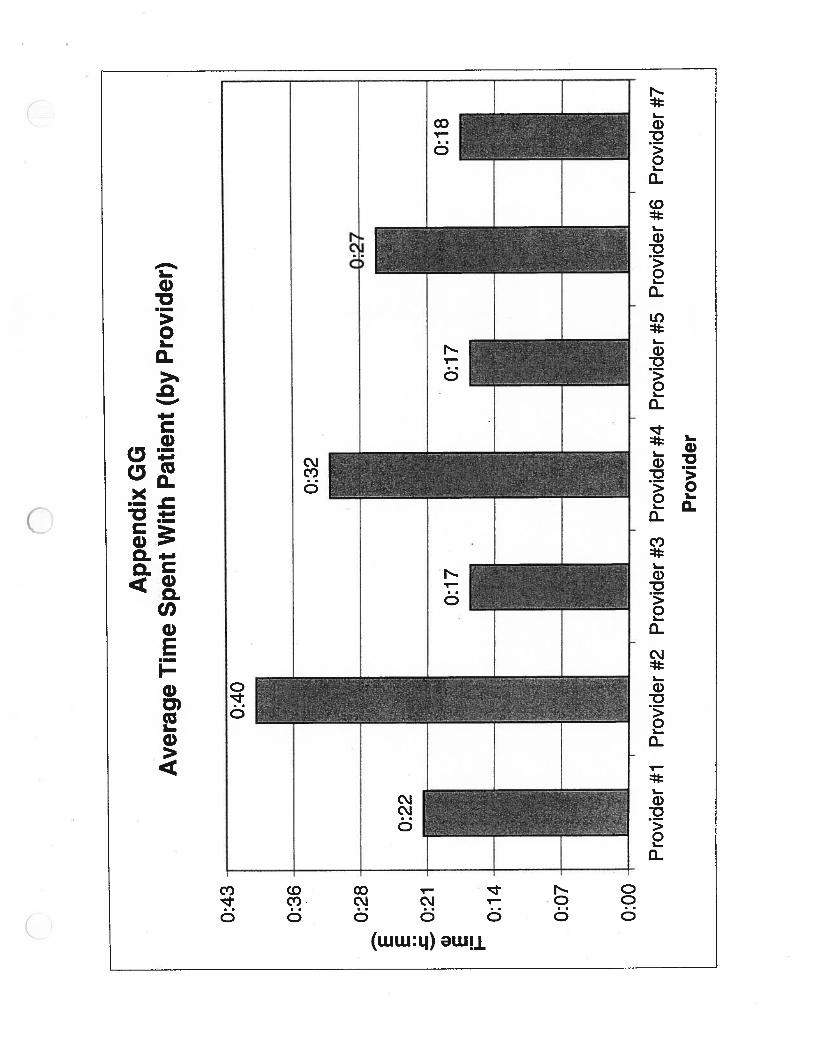
App
endi
xG
GA
ver
age
Tim
eS
pen
tW
ith
Pat
ient
(by
Pro
vide
r)
0:32
0:43
0:36
0:28
0:21
0:14
0:07
0:00
0:17
0:17
I•
I•
II
Pro
vide
r#1
Pro
vide
r#2
Pro
vide
r#3
Pro
vide
r#4
Pro
vide
r#5
Pro
vide
r#6
Pro
vide
r#7
Pro
vid
er
Cl)
G)
C WE jz
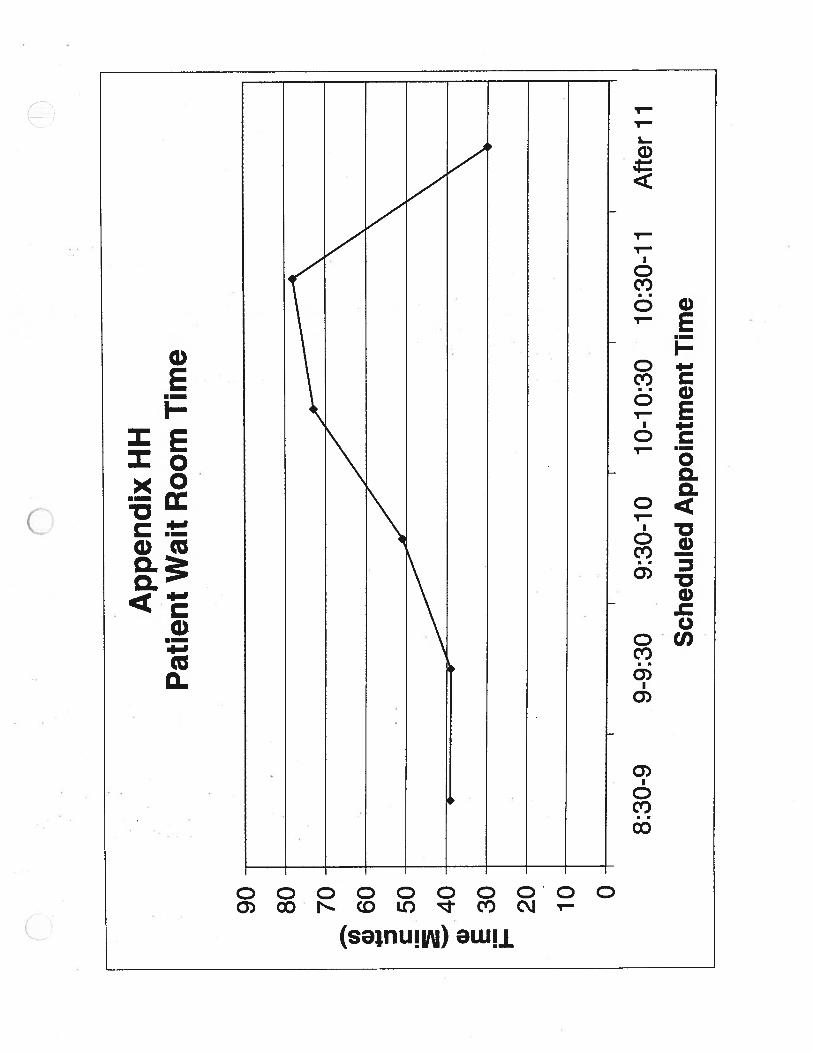
Ap
pen
dix
HH
Pat
ient
Wai
tR
oom
Tim
e
8:30
-910
:30-
11A
fter
11Th
90 80 70 60 50 40 30 20 10 0
9-9:
309:
30-1
010
-10:
30
Sch
edu
led
Appoin
tmen
tT
ime
90 80 70 60 50 40 30 20 10
Ap
pen
dix
IIP
atie
nt
Wai
tR
oom
Tim
e
Cl) a) z C I:
0
8:30
-99-
9:30
9:30
-10
10-1
0:30
10:3
0-11
Sch
edule
dA
ppoin
tmen
tT
ime
Aft
er11
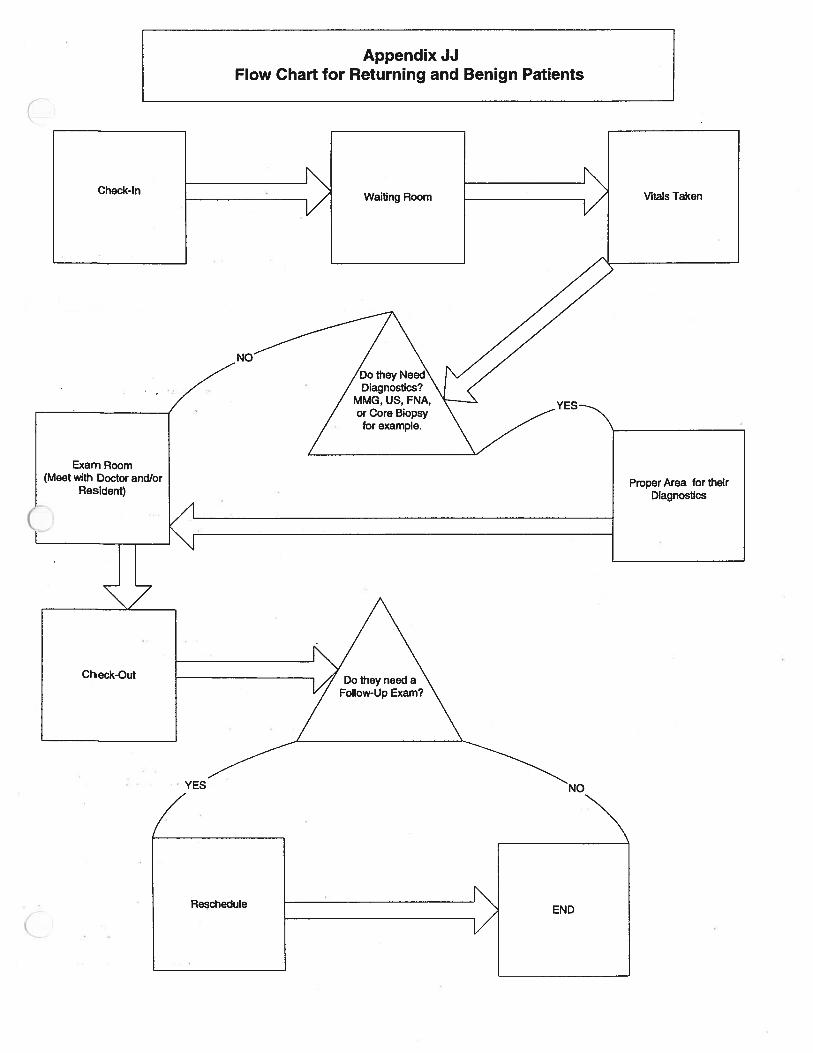
Appendix JJFlow Chart for Returning and Benign Patients
Check-InWaiting Room Vitals Taken
Exam Room
Resident)Proper Area for their
Diagnostics
ACheck-Out
Reschedule
C
Appendix KKFlow Chart for Multi-Disciplinary (New Cancer) Patients
Check-In at ClinicIncludes Passing
On PathologySlides
Radiology forMore Pictures
Waiting Room
Go to ProperDestination fortheir treatment
Placed in Exam Roomwhere they will seedifferent doctors if
neccesary
Drop offMammograms at
RadiologyWait Room



















![Untitled-2 [regtigblessed.co.za]regtigblessed.co.za/Floral_Fabric_Catalogue.pdf · F0002 Pattern Repeat Size: 50cm . F0003 Pattern Repeat Size: 50cm . F0004 Pattern Repeat Size: 50cm](https://img.pdfslide.us/doc/110x75/5f2be74d8f69417fe634bdb6/untitled-2-f0002-pattern-repeat-size-50cm-f0003-pattern-repeat-size-50cm.jpg)