Embed Size (px)
Citation preview
Highlights of Dr. Rory Houghtalen’s Grand Rounds Presentation on 9/09/2014
Compiled and Presented by Dave Porter

Presentation Outline
1. Introduction
2. Background
3. Indications
4. Adverse Effects Comparison to SSRIs
5. Tolerance, Abuse and Dose Tapering
6. Conclusions
7. Q&A Session

Introduction• Before the advent of benzodiazepines (benzos),
barbiturates were used to treat anxiety– Higher rates of withdrawal and dependence– Less safe in overdose, more drug-drug interactions
• Librium® (chlordiazepoxide) was the first benzo approved by the FDA– Marketed as a drug to “make patients more accessible
during psychological therapy”• Valium® (diazepam) approved next• High hopes for the future of these drugs
– Reports of overdose and dependence began the ongoing controversy

Clinical Controversies and Stigma• Some physicians are reluctant to prescribe benzos out
of fear they will be labeled as “problem prescribers” if their patients develop tolerance or drug-seeking behavior– Tolerance, dependence, abuse and withdrawal
• Benzos in pregnancy (www.motherisk.org/drugs.jsp) – Conflicting evidence regarding 1st trimester use
• Possibility of cleft palate, urogenital and neurological deformities– Post-partum complications
• “Floppy baby” and neonatal withdrawal syndromes– Recommended to avoid benzos in pregnancy if possible,
and to taper dose down before delivery• Patient perceptions of addiction and dependence
– Potential self-worth problems, even if best-practice use• Long term use vs. approved therapy duration
Mechanism of Action
• Benzos act on the GABA receptor complex– They do not bind directly to the GABA site, rather at a site
on the α-subunit– They are “positive allosteric modulators”
• They do not enact a response simply by binding to the α-subunit, but they promote GABA binding to the receptor
– Barbiturates also inhibit the AMPA receptor• ↑GABA, ↓glutamate…• More dangerous in overdose, due to the greater net NT inhibition
– “Z-drugs” (zaleplon, zolpidem and eszopiclone), propofol, etomidate, barbiturates, ethanol and gabapentin also bind to the GABA receptor complex at different sites

GABA Receptor Complex
Multiple Effects of Benzodiazepines
• Benzodiazepines have multiple effects– Anxiolytic– Amnesic– Antiseizure– Anesthetic– Sedative– Muscle relaxant
Indications• Acute Insomnia
– Benzos can reset biological clock with 7-10 days use– Risk of parasomnia and amnesia less than with the Z-drugs
• Chronic Insomnia– Can destabilize many diseases– Often have impairment of driving already– Clonazepam is the drug of choice for REM Behavioral
Disorder and Restless Leg Syndrome• Generalized Anxiety Disorder (GAD)
– Constant worrying about everything (kids, MVAs, Hell, etc)– Use SSRIs with benzos for breakthrough anxiety
• Acute Agitation– Lorazepam can be used with haloperidol as an IM injection
Indications• Social Anxiety Disorder
– Fear of rejection, social interactions, crowds– Longer acting benzos are more effective
• Panic Disorder– Feeling of impending doom during non-threatening events– Benzo efficacy comparable to SSRIs, SNRIs and TCAs
• Akithisia and tremor– Side effects of some medications– If removing the offending agent doesn’t help, add a
lipophilic BB (1st line) or benzo (2nd line, added to BB)• SOB in COPD
– Longer acting benzos can help control• Alcohol Withdrawal

Onset, Half-Life and Equivalent Dose
Bostwick JR, et al. Benzodiazepines: A versatile clinical tool. Evidence supports their use for alcohol withdrawal, insomnia, anxiety disorders, and other conditions. Current Psychiatry. April 2012. 11(4), 54-64.

Onset, Half-Life and Equivalent Dose
Bostwick JR, et al. Benzodiazepines: A versatile clinical tool. Evidence supports their use for alcohol withdrawal, insomnia, anxiety disorders, and other conditions. Current Psychiatry. April 2012. 11(4), 54-64.

Dosing Pearls
• Avoid using PRN dosing schedules as the primary dosing plan– Find lowest effective dose and maintain consistent dosing
intervals (i.e. alprazolam 0.5mg po T.I.D.)
• Pulse dosing may actually worsen anxiety
• Short acting benzos have higher Cmax
– Can be problematic for some patients

Benzodiazepines in the Elderly• Patients over 65 will gradually develop problems
metabolizing drugs– Use the LOT group of benzos in the elderly
• Lorazepam, oxazepam and temazepam
• Interestingly, long-term exposure may often lead to lessened ADRs– Elderly are more prone to confusion and paradoxical
agitation with acute exposure to benzos– Still recommended to gradually taper doses in the elderly
• Might run into resistance from patients• A patient with a 20 year history of panic disorder may be reluctant
to discontinue an effective treatment• No significant rush to decrease doses, if no ADRs present

Benzodiazepines and Beers Criteria
• The Beers Criteria was developed in 1991 to assist healthcare providers in improving medication safety in older adults
• Beers Criteria states that MDs should not give benzodiazepines to the elderly– Increased risk of falls, delirium, and MVAs
• However, long-acting benzos are preferred agents in the elderly– This is a loophole in the Beers Criteria

Benzodiazepines and SSRIs• Guidelines advocate for SSRIs to be used first line in
anxiety disorders (evidence is good but not great)– Some SSRIs are preferred depending on disorder– This doesn’t mean benzos should not be considered as a
concomitant option• Use benzos in the initiation phase of SSRIs
– SSRIs take 4-6 weeks for full effect, with an onset in approximately 2-3 weeks.
– Benzos have an onset in a few minutes, with full effects within 15-60 minutes
– Let patients know that the use of benzos will be temporary and a dose taper will occur
• Patient may be reluctant to stop the benzo due to the welcome and rapid relief of symptoms

Adverse Reaction Comparison
• Benzodiazepines– Greater impairment of
driving– Dizziness– More tolerance– Abuse risk– Potential pregnancy
concerns
• SSRIs/SNRIs– Weight gain– Sexual dysfunction– Suicidal thoughts– Increased lipids– Increased BGLs– Sleep disturbances– Hyponatremia

Benzodiazepine Tolerance
• Tolerance will develop in most patients after a month with a moderate to high dose
• Tolerance to acute dose sedation and memory impairment do occur– Patients will adapted to chronic use of benzos have lower
rates of sedation despite having higher blood levels– Using benzos for over a year retained sleep quality,
lower prevalence of confusion

Benzodiazepine Addiction and Abuse• Less than 1% of benzo users ever show and evidence of
abuse– Patients tend to independently decrease dose!– Benzos are most often abused when the drug-of-choice for
abuse is unavailable• Binge drinker can’t find alcohol, so they abuse benzos• Some cocaine users use benzos to quell cocaine ADRs
• Increased incidence of benzo abuse in opioid patients– Be judicious, but don’t shun benzos in these patients
• Some patients with social anxiety will abuse alcohol to decrease their symptoms– Is this more desirable than giving them a benzo?– Still the potential for abuse… but which is worse?
• Some physicians still will not prescribe a benzo in this situation

Benzodiazepine Overdose and Withdrawal
• Fatal overdose is rare, but benzos aren’t recommended for patients with a history of substance abuse
• Most overdoses are due to non-medical, recreational use
• Benzo withdrawal symptoms occur more frequently with options with shorter half-lives and faster onsets– Rebound anxiety and insomnia, worse than baseline levels– Frequent requestions for new prescriptions, MD shopping,
acquiring tablets from friends
Benzodiazepine Overdose and Withdrawal
• Fatal overdose is rare, but benzos aren’t recommended for patients with a history of substance abuse
• Most overdoses are due to non-medical, recreational use
• Benzo withdrawal symptoms occur more frequently with options with shorter half-lives and faster onsets– Rebound anxiety and insomnia, worse than baseline levels– Frequent requests for new prescriptions, MD shopping,
acquiring tablets from friends

Dose Tapering• Challenging for both short- and long-acting
– Abrupt withdrawal can precipitate panic, psychosis– If problems arise, decrease rate of tapering
• Do not increase the dose though!
• Time consuming!– Low dose benzos may require a taper of 4-6 weeks– High dose benzos may require a taper of greater than 6 months
• Give patient some autonomy in controlling their taper schedule– Proceed at the patient’s pace, but steadily
• Rapid detox centers not recommended– Patient would have no way to build up alternative living skills
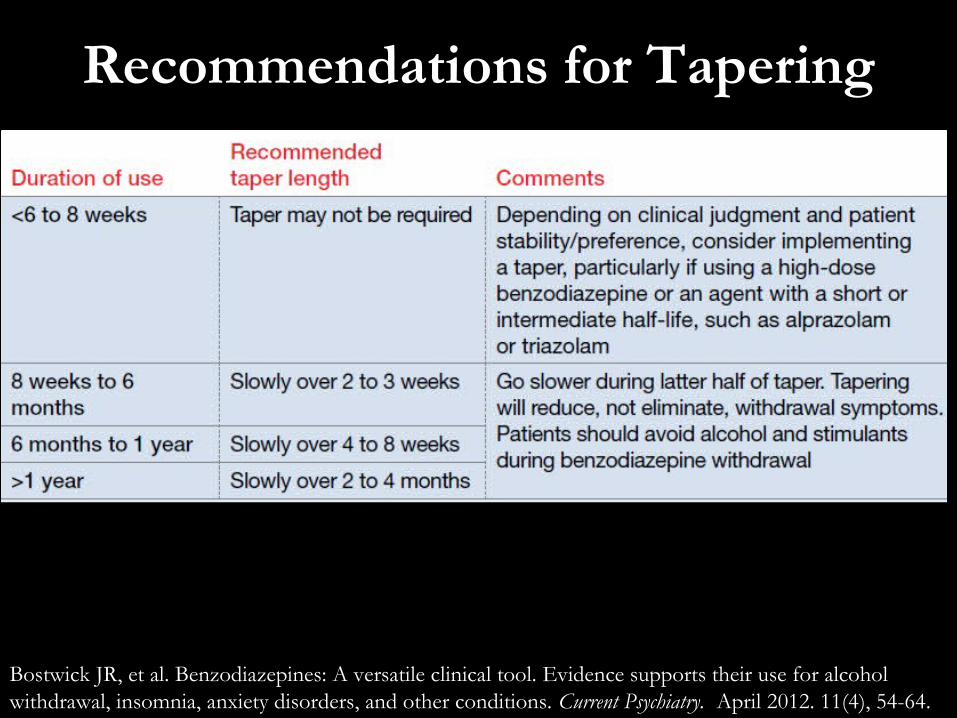
Recommendations for Tapering
Bostwick JR, et al. Benzodiazepines: A versatile clinical tool. Evidence supports their use for alcohol withdrawal, insomnia, anxiety disorders, and other conditions. Current Psychiatry. April 2012. 11(4), 54-64.

References
1. Bostwick JR, et al. Benzodiazepines: A versatile clinical tool. Evidence supports their use for alcohol withdrawal, insomnia, anxiety disorders, and other conditions. Current Psychiatry. April 2012. 11(4), 54-64.
2. Cloos, JM. Benzodiazepines and Addiction: Myths and Realities. Psychiatric Times. July 2010. pp.26-29.
3. Houghtalen R. Unity Hospital Grand Rounds. Sept 9, 2014.

Thanks for Listening!







![CaseReport Habit Breaking Appliance for Multiple Corrections · Habit Breaking Appliance for Multiple Corrections ... removable habit breaking appliances [15, 16]. Hence, habit breaking](https://img.pdfslide.us/doc/110x75/5f15893424a8522d646af1b7/casereport-habit-breaking-appliance-for-multiple-corrections-habit-breaking-appliance.jpg)



















![[Lean 101] Costs & Revenues - Breaking even or Breaking bad???](https://img.pdfslide.us/doc/110x75/58777a001a28ab5b568b76c5/lean-101-costs-revenues-breaking-even-or-breaking-bad.jpg)
