Embed Size (px)
Citation preview

Aug., 1910. DENGUE OR PHLEBOTOMUS FEVER. 281
(Drigimil Articles;.
DENGUE OR PHLEBOTOMUS FEVER? NOTES ON AN EPIDEMIC AT
NOWSHERA.
By C. N. C. WIMBERLEY, LIEUT.-COLONEL, I.M.S.
In the Indian Medical Gazette (for July 1908), Lfc.-Col. Fooks, i.M.s., described an
outbreak of " Dengue Fever ''
amongst the men of the 15th Lancers at Sialkot during the
months of October and November, 1907. Last autumn I had to deal with a very
similar epidemic of fever in the men of the loth Sikhs, stationed at Nowshera. In this
Regiment about 160 cases were met with
between the 4th October and the end of Nov-
ember. All the other troops in the Canton-
ment, British and Native, were also affected, but none so severely as the 15th Sikhs.
The epidemic wfis of such a natuie as to
form a well-marked clinical entity. From in-
fluenza it differed in so far that catarrhal res-
piratory symptoms were lately present, nor weie the symptoms of the piotean character that aie associated with influenza, but nearly always of one marked clinical type. Again, convalescence was usually rapid, and the marked asthenia which follows influenza was not apparent. From the clinical description of dengue given by Manson, and copied i?t0 all text-books on
tropical' medicine, it differed in so far that there was no sudden 'widespread onset?the cases
occurring irregularly during a period of some seven w?eeks.
?
Nor were the pains and aches complained of, though generally severe, of the
excruciating character which has given the
pseudonym of " Break-bone Fever
"
to dengue. Again the pains did not persist after the termin- ation of the fever, but only lasted for a couple of davs or so after the
onset.
The disease met with may shortly be des-
cribed as a sharp attack of pyrexia, lasting usually from three to
six days, accompanied by severe headache in the frontal or orbital regions, and by pains in the back
and thighs. In some
cases these pains were so severe as to cause the
patients very great suffering but m others
they were of a milder nature. But some
decree of pain was universally complained of.
They usually lasted for the first two days of the fever only, great relief being experienced in
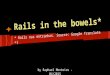
the third day. In a veiy large proportion of cases vomiting also occurred during the first dav or two The temperature generally rose to 103? or higher, reaching its maximum in the evening of tha second day, others commenced to fall" gradually by lysis ; but in many cases first before reaching normal there was a further sudden rise which persisted for some hours, after which the temperature fell rapidly to subnormal. This terminal fever was generally m'irked by severe constipation, the final fall beincr frequently coincident with the free evacuation of the bowels by a purgative. In not a few cases it was associated with epistaxis. Subnormal temperatures during the first few days of convalescence were universal. It was difficult to calculate the exact duration of the pyrexial attack, as some men did not report sick at onco and were indefinite as to how long they had been ill before coming to hospital but so far as I could elicit, the fever lasted?
3 days in 37 cases. 4 ? ?
5 ? ? ?
6 >. " 33 ?
7 )i " ? "
a ... 2 ..
NAME 46 78
19 0 9 DATE
Day of Dis. TIME
s RALlA SINGH
OCT
5 M.E
6 M.E
7 M E
8 M E
9 10 m.em.ei
105
_3?_
&
HEADACHE V0MITI NG PA INS
CASE.No.5

282 THE INDIAN MEDICAL GAZETTE. [Aug., 1910.
In about 8 per cent, of the cases a rash was
observed, appearing first on the forearms about the time of the terminal rise of temperature, and then spreading over the body, sometimes as a mere mottling of the skin, but in several
cases as a well marked macalo-papular rash. Then coming to hospital had a very heavy, almost drunken look, with congested faces, supposed conjunctiva), and white-coated tongues. This appearance with the complaint of frontal headache and lumbago-like pains was very characteristic. Recruits and young soldiers were especially affected ; and two officers and one officer's wife were amongst my patients. The disease was?distinctly infectious. Several
sick attendants contracted it in hospital. There were as a rule no complications. A few men have slight bronchial catarrh, and one weakly follower developed broncho-pneumonia, coma
vigil, and rapidly succumbed.
Convalescence was usually rapid, and few
sequelae were noticed. One man had musculo-
spiral paralysis and wrist drop which soon
passed off, and another presented slight maniacal symptoms for a few days. But the bulk
of the sufferers expressed themselves as quite well a couple of days after their temperature fell.
No true relapses occurred. As noticed by Colonel Fooks, I found the
pulse rate markedly diminished during the
latter part of the fever, and during early con- valescence. In several cases with a temperature of 102? the pulse was only 05, and with the
subnormal temperatures of convalescence the
pulse was usually not above 55. I append a few illustrative charts. The great point of interest in such epidemics
is their etiology.
The " Three-day Fever " of the Mediterranean
littoral has been proved by Doerr to be conveyed by the bite of a sandfly (Phlebotomus), and Lieutenant-Colonel Birt, R.A.M.C., in Malta has confirmed this.
Now the Phlebotomus is a very common insect in the Peshawar Valley, indeed all over the Pun- jab, causing a good deal of annoj^ance at any rate. But in most years I think
" sandflies " are most abundant in the early months of the hot weather, i.e., in April and May. During the very hot months their numbers diminish, but increase
again in the autumn. And it is in the autumn
only that these outbreaks of Dengue-like fever
occur, so far as my experience goes; I have
frequently, at the commencement of the hot
weather, met with irregular pyrexial attacks of short duration, somewhat resembling the cases
I have described above, but have never at that time of year seen anything of the nature of an epidemic. Whereas in the autumn
months I believe epidemics to be not un-
common.
The virus described by Doerr in the "Papa- tasi Fever," of Herzegovina, is ultra-microscopic, and able to pass through a Berkefelt filter. It can hardly then be of a protozoal nature.
Nor does quinine appear to have the slightest effect on fevers of this nature. When the late epidemic occurred in Nowshera, all the troops were saturated with quinine, which had, for several months, been issued as a prophylactic against malaria.
Such outbreaks as I have described above, appear to me to agree in all essential points with McCarrison's " three-day Fever of Chitral;
"
Dengue Fever as described by Ashburnham and Craig in the Phillipines; and "
Papatasi Fever" of the Mediterranean.





![Healthy Bowels Healthy YOU! [Read-Only] · Healthy Bowels, Healthy YOU! • You’ve been taught not to bring it up in polite conversation • Many people feel uncomfortable discussing](https://img.pdfslide.us/doc/110x75/60354af98095985cc16215e0/healthy-bowels-healthy-you-read-only-healthy-bowels-healthy-you-a-youave.jpg)