Embed Size (px)
Citation preview
BRd 3(1)
28-1June 2016 Version 1
CHAPTER 28
MEDICAL AND DENTAL CARE
CONTENTS
Para2801. Introduction2802. Medical Force Generation2803. References2804. Naval Service Medical Board of Survey and Naval Service Medical Employability
Board2805. Provision of Medical Care2806. Provision of Dental Care2807. Medical Information - Disclosure to Command2808. Adventurous Training and Sports2809. Reserves2810. Medical Welfare2811. Dangerously Ill Forwarding of Relatives (DILFOR)2812. Long Term Sickness2813. Referral to Defence Mental Health Services2814. HIV Positive Individuals - Employment at Sea
ANNEXES
Annex 28A Documentation for Referral to a Department of Community Mental HealthAnnex 28B Guidance for Primary Care Medica Officers on Confidentiality and Consent for
Requests for F Med 1041Annex 28C Guidance on the Completion of an F Med 1041
UN
CO
NTR
OLL
ED
WH
EN
PR
INTE
D
BRd 3(1)
28-2June 2016 Version 1
CHAPTER 28
MEDICAL AND DENTAL CARE
2801. IntroductionThe Defence Medical Services (DMS)1 will provide healthcare, medical operational
capability and health advice to maximise the fighting power of the Armed Forces. The missionflows directly from the Defence Plan through to the Service Personnel Plan. The DMSStrategic Plan includes performance indicators such as the numbers of service personnelmedically and dentally fit for deployment and for the provision and/or delivery of primary,intermediate and secondary healthcare appropriate to the environment where personnel areserving.
2802. Medical Force GenerationThe RN Medical Services are directed (under PFS) to ensure that the maximum
numbers of personnel are fit for task. Joint Medical Employment Standards (JMES) codes areused to define the medical employment standard appropriate to an individual's medical fitnessand enable the communication of the necessary information to the employer (CareerManagers, Chain of Command) without any breach of medical confidentiality. They ensurethat the individual is appropriately employed without unnecessarily endangering their ownhealth or that of others2. To allow appropriate assigning, Career Managers are provided withan individual serviceperson's JMES through JPA.
2803. References
a. BR1991 (Instructions for the Royal Naval Medical Service) and BR 1750A(Handbook of Naval Medical Standards) are the primary references for Naval policyand organisation of Medical and Dental Care. They also contain the procedures andstandards for the provision of medical and dental care to entitled personnel.
b. Maritime Reserves. See BR 3(2) Annex 3B for medical administration ofMaritime Reserves.
2804. Naval Service Medical Board of Survey and Naval Service Medical Employability Board
Whilst short term changes to medical grading and work limitations are made at Unitlevel the assessment of long-term fitness for further service and long term restrictions on workability is conducted in a 2 stage process. This involves referral to the Naval Service MedicalBoard of Survey which gives a medical recommendation on fitness. This recommendation isthen considered by the Naval Service Medical Employability Board, on behalf of the NavalService as the employer, and a decision taken as to whether the Service person can besuccessfully employed within the proposed restrictions. Details of the function and processesof the Boards are in BR 1991 Chapter 8.
1. Defence Medical Services Strategic Plan 2010/20142. 2009DIN01-183
UN
CO
NTR
OLL
ED
WH
EN
PR
INTE
D
BRd 3(1)
28-3June 2016 Version 1
2805. Provision of Medical CareIn partnership with others3 the RNMS will provide high quality healthcare to support
force generation and maintain the health of the Naval Service.
a. Primary healthcare (General Practice, Mental Health, Occupational Health andDefence Rehabilitation) is provided to entitled personnel, in the firm base, by DefencePrimary Health Care (DPHC) to a standard at least as good as, and relevant to, UKcivilian best practice. The RNMS retains responsibility for provision of primaryhealthcare and occupational health to deployed Naval Service, RFA and Royal NavalReserve personnel.
b. Access to timely Secondary Healthcare in the UK at least equivalent to thatprovided by the National Health Service1.
c. All Naval personnel are directed to carry a valid European Health Insurance Card(EHIC)4 and strongly advised to hold appropriate travel insurance when travellinganywhere at their own expense or for non-Service reasons.
d. The management of some chronic conditions could be compromised by anassignment overseas. Before deploying overseas, the assigned serviceperson is tomake a declaration concerning the health of their dependants. All long term medicalconditions are to be declared in accordance with single Service procedures in order toallow the receiving theatre to make an informed decision as to whether a chroniccondition can be appropriately managed. Where a condition cannot be managed, adecision then has to be made, by the assigning authority, as to whether theassignment can go ahead.
2806. Provision of Dental CareDental Care is provided by the Defence Dental Service (DDS) to entitled personnel to
a level at least equvalent to the NHS.
2807. Medical Information - Disclosure to Command
a. All health or other personal information received by Service and civilian medicalpersonnel acting in that capacity from, or in relation to, a patient is confidential, andmedical personnel have a legal5 as well as an ethical duty to keep that informationconfidential. The duty of confidentiality is described in detail in guidance from therelevant professional bodies (e.g. GMC, GDC, NMC, HPC). This guidance is to befollowed by Service and civilian medical personnel at all times.
b. Except in limited circunstances, disclosure of personal medical information iscontrary to the law and to the public interest. Loss of confidence by personnel in theconfidentiality of their healthcare may result in medical conditions being concealed,with consequent risks to Unit safety and operational effectiveness.
c. Personal medical information may only be disclosed:
3. Defence Primary Healthcare (DPHC), NHS, Private Providers, third sector, coalition partners4. 2010DIN01-1105. Data Protection Act 1998
UN
CO
NTR
OLL
ED
WH
EN
PR
INTE
D
BRd 3(1)
28-4June 2016 Version 1
(1) With the individual's valid consent;
(2) Where required under the law6;
(3) Where substantial public interest demands disclosure without consent,particularly protection of:
(a) The operational capability (OC) of the Unit;
(b) Safety of other Unit personnel.
d. Disclosures made for OC or safety reasons must only be made directly to theCommanding Officer.
e. Information disclosed to the Commanding Officer is to be limited to that which isrequired for the protection of OC or the safety of Unit personnel.
f. The Commanding Officer must respect the confidential nature of all informationdisclosed, and must only communicate as much detail to other personnel as requiredto deliver essential purposes of protecting OC or the safety of Unit personnel.
g. The individual must be informed of the content of all disclosures of their personalmedical information to Command, preferably prior to disclosure but in any event at theearliest reasonable opportunity.
h. Private medical information is not to be used to instigate disciplinary proceedingsother than in exceptional circumstances with the advice of Navy HQ Legal.
i. Specific Instances
(1) Drug and Alcohol Misuse. When drug or alcohol misuse is disclosedduring a clinical consultation, this information must only be disclosed to Commandif the nature of the misuse threatens harm to other members of the Unit or to OC.An example of such a threat would be a pilot who proposed to fly aircraft whileintoxicated. Medical personnel must report drug and alcohol misuse when theybecome aware of such misuse outside of their medical capacity.
(2) Post-Coital Contraception. Requests by personnel for post-coitalcontraception must not be disclosed outside the consultation without the consentof the individual.
6. http://www.gmc-uk.org/guidance/ethical_guidance/confidentiality.asp - Paras 35 and 36 and supplementary guid-ance
UN
CO
NTR
OLL
ED
WH
EN
PR
INTE
D
BRd 3(1)
28-5June 2016 Version 1
2808. Adventurous Training and SportsMilitary personnel undertaking correctly staffed and officially sanctioned adventure
training and sports are entitled to medical care at public expense. However, in some countrieswhere such activities take place, the civil health infrastructure cannot provide a suitable levelof care. Private medical facilities that can provide the required level of care might be availablebut proof of ability to pay is often required before treatment commences. Military teamsventuring overseas are strongly advised to take out private medical insurance. Refer to themost current DIN - Insurance for Adventurous Training Activities.
2809. ReservesFor members of the Reserve component of the Armed Forces undertaking officially
sanctioned military activity, be it sporting, adventurous training or military training, medicalsupport is provided at public expense up to the point where the individual is fit to be dischargedhome to the care of their own GP. However, long term health care is not provided by MoD tomanage the consequences of injury or illness sustained by members of the Reservecomponent unless sustained whilst mobilised for operations: that responsibility lies with theNHS. Refer to JSP 753 (Tri Service Regulations for the Mobilisation of Reserves).
2810. Medical WelfareService personnel admitted to hospital may require welfare support. The Defence
Medical Welfare Services (DMWS) are currently contracted to provide welfare services toService patients both on operations and in some peacetime locations on a constant basis.DMWS support is provided under the following categories:
a. Welfare needs assessment;
b. Response to requests for welfare support;
c. Emotional and practical support;
d. Liaison and referral to other agencies as appropriate.
Although DMWS provide a hospital welfare service, the patient’s chain of command isexpected to remain fully engaged in the needs of the Service person undergoing hospital care.Arrangements are in place (Liaison Officers) for linkage between DMWS and single ServiceWelfare organisations (RNRMW, AWA and SSAFA) (see Chapter 24).
2811. Dangerously Ill Forwarding of Relatives (DILFOR)DILFOR is an allowance designed to help ease the emotional and financial burden of
close family members of a serviceperson who is unexpectedly admitted to hospital. DILFORis available to provide travel and subsistence to enable family members to visit the Serviceperson. Details of DILFOR are contained in Chapter 7 of JSP 751 (Joint Casualty andCompassionate Policy and Procedures). To be entitled to DILFOR the patient must have arecommendation from the medical authority concerned that states that a visit from close familymembers would be in the best interest of the patient's recovery.
UN
CO
NTR
OLL
ED
WH
EN
PR
INTE
D
BRd 3(1)
28-6June 2016 Version 1
2812. Long Term SicknessEach Service has in place comprehensive long term sickness management policies
that ensure that Service personnel who are long term sick are properly tracked managed andsupported. Further information relating to Long Term Sickness can be found at Chapter 33(Recovery Pathway).
2813. Referral to Defence Mental Health Services
a. Service personnel may be referred to the Defence Mental Health Services(DMHS) for a number of reasons, either because of obvious psychiatric illness,behavioural problems, alcohol problems or merely for assessment prior to disciplinaryaction.
b. DPHC Departments of Community Mental Health (DCMH) are based at HMNaval Base Portsmouth, HMS DRAKE and HMS NEPTUNE. Regular peripateticclinics are also held in a number of other Royal Naval Shore Establishments and, ifappropriate to the needs of the Fleet, visits can be made to HM Ships. There aretwelve other DCMHs in the UK operated by the DPHC; all DCMHs see patients fromall three Services.
c. Even when family informants are available, mental health professionals areheavily dependent on the information about behaviour obtained from Service sources;such information should be contained in the referring Medical Report and appropriateExecutive Reports. Recent information is provided by means of the F Med 1041which should be completed by the Commanding or Divisional Officer. In the event ofa possible recommendation for Discharge SHORE on the grounds of TemperamentalUnsuitability, the F Med 1041 must be signed by the person's Commanding Officer.SJARs completed by the Divisional Officer give a longitudinal picture, which is ofparticular advantage in cases of possible temperamental unsuitability for Service lifeor in cases of chronic alcohol abuse.
d. It may also be appropriate for the Service mental health professional to speakdirectly with a person's Divisional Officer, Head of Department, Commanding Officeror career manager in order to complete a mental health assessment and makeappropriate recommendations.
e. The acquisition of information from the Executive should be dealt with appropriatesensitivity. The fact of referral itself may be considered sensitive information. Theattitude of a person to referral must be sensitively enquired about by the referringmedical officer. Concerns about confidentiality are to be taken seriously.Nevertheless, occupational risks are often only quantifiable with good informationabout the serviceperson's performance both recently and during their career.Referring medical officers should seek the person's consent to request an F Med 1041(and Service Documents) using the procedure on the form itself. Should a patientrefuse consent, this should be recorded in the referring F Med 7 and the referral notdelayed. Personnel should be made aware that the mental health assessment maybe incomplete if such documentation is not available.
UN
CO
NTR
OLL
ED
WH
EN
PR
INTE
D
BRd 3(1)
28-7June 2016 Version 1
f. Details of the required documentation for psychiatric referrals and contact detailsof port area DCMH are at Annex 28A. Annex 28B and Annex 28C provide guidanceto Medical personnel and the Chain of Command on requesting and providing anFMed 1041.
2814. HIV Positive Individuals - Employment at Sea
a. References
(1) HIV/AIDS in the Armed Forces - Guidance for Service Healthcare Workers.
(2) JSP 950 Vol 6 Chap 7 Leaflet 6-7-5.
(3) BRd 9467 (FLAGOs) Articles 1915 and 1916.
b. It is Government policy not to allow discrimination against personnel on thegrounds of HIV status. Personnel who are HIV positive will at all times be dealt within accordance with the principles of medical confidentiality (Reference (1)). OnlyMedical Branch staff and, where appropriate, the Commanding Officer, will be madeaware of the status of such individuals.
c. Personnel becoming HIV positive in service will be medically graded by a NavalService Medical Board of Survey (NSMBOS) in accordance with the provisions ofReference (2). Subsequent assigning decisions will be made on the basis of thismedical employment standard by a Naval Service Medical Employment Board(NSMEB). Such decisions will take account of the individual merits of each case, andwill incorporate guidance upon the duties to which these personnel may be allocated.
d. Specific information on the risks of cross infection will be found in Reference (3).
UN
CO
NTR
OLL
ED
WH
EN
PR
INTE
D
BRd 3(1)
28A-1June 2016 Version 1
ANNEX 28A
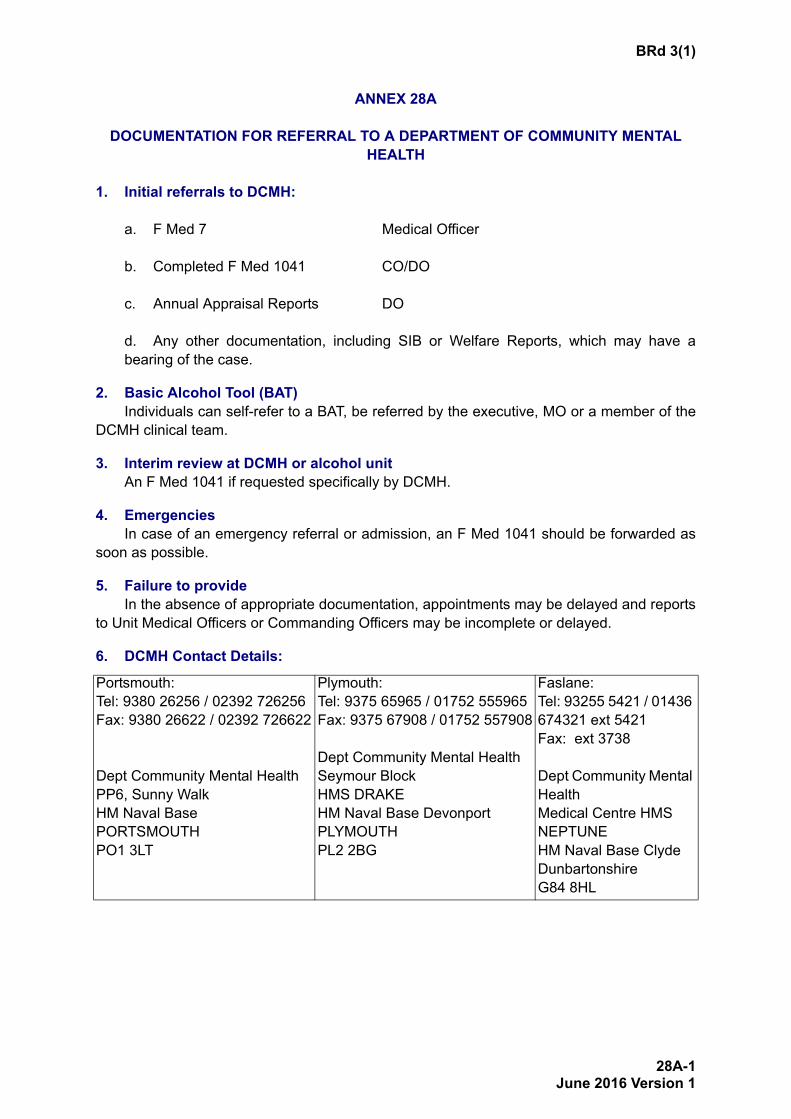
DOCUMENTATION FOR REFERRAL TO A DEPARTMENT OF COMMUNITY MENTAL HEALTH
1. Initial referrals to DCMH:
a. F Med 7 Medical Officer
b. Completed F Med 1041 CO/DO
c. Annual Appraisal Reports DO
d. Any other documentation, including SIB or Welfare Reports, which may have abearing of the case.
2. Basic Alcohol Tool (BAT)Individuals can self-refer to a BAT, be referred by the executive, MO or a member of the
DCMH clinical team.
3. Interim review at DCMH or alcohol unitAn F Med 1041 if requested specifically by DCMH.
4. EmergenciesIn case of an emergency referral or admission, an F Med 1041 should be forwarded as
soon as possible.
5. Failure to provideIn the absence of appropriate documentation, appointments may be delayed and reports
to Unit Medical Officers or Commanding Officers may be incomplete or delayed.
6. DCMH Contact Details:
Portsmouth:Tel: 9380 26256 / 02392 726256Fax: 9380 26622 / 02392 726622
Dept Community Mental HealthPP6, Sunny WalkHM Naval BasePORTSMOUTHPO1 3LT
Plymouth:Tel: 9375 65965 / 01752 555965Fax: 9375 67908 / 01752 557908
Dept Community Mental HealthSeymour BlockHMS DRAKEHM Naval Base DevonportPLYMOUTHPL2 2BG
Faslane:Tel: 93255 5421 / 01436 674321 ext 5421Fax: ext 3738
Dept Community Mental HealthMedical Centre HMS NEPTUNEHM Naval Base ClydeDunbartonshireG84 8HL
UN
CO
NTR
OLL
ED
WH
EN
PR
INTE
D
BRd 3(1)
28B-1June 2016 Version 1
ANNEX 28B
GUIDANCE FOR PRIMARY CARE MEDICAL OFFICERS ON CONFIDENTIALITY AND CONSENT FOR REQUESTS FOR F MED 1041
1. BackgroundThe General Medical Council (GMC) gives guidance on disclosure of medical information
to employers1. The guidance refers, in the main, to reports from health professionals toemployers. F Med 1041 is a report in the opposite direction, but the act of requesting thisdocument is a disclosure in itself and generally relates to alerting the Executive to that personseeing a mental health professional. The GMC guidance advises:
a. Patients must be informed about disclosures they would not reasonably expect
b. Patients’ consent must be sought before disclosing identifiable information (in thiscase the fact that the person is being referred to a mental health professional).
c. Informing the patient means appraising the patient of the scope, purpose and likelyconsequences of the disclosure.
d. Obtaining or seeing written consent to the disclosure and that that consent is obtainedfrom an appropriate authority. JSP 950 Vol 1 Chap 2 Leaflet 1-2-4 outlines the consentprocess for requesting the F Med 1041 and has a consent form as part of the documentitself, which primary care medical officers should use.
2. Guidance
a. This Annex gives guidance to primary care medical officers on the informationrequirements for gaining fully valid consent.
b. Scope. The F Med 1041 is a performance report and its aim is provide a specialisthealthcare professional with information and opinion from the person’s employer -essentially their line manager or Divisional Officer. The report should, in cases wheretemperamental unsuitability is being assessed, be signed by the person’s commandingofficer.
c. Purpose
(1) A full mental health assessment usually requires third party information. Thiswill come from people who know the person well and over a period of time. It isespecially useful if those people have known the person before their problems began.When decisions about occupational fitness need addressing, such third partyinformation as can be gained from employers is invaluable.
1. GMC “Confidentiality” and “Confidentiality: Supplementary Guidance” 2009
UN
CO
NTR
OLL
ED
WH
EN
PR
INTE
D
BRd 3(1)
28B-2June 2016 Version 1
(2) An F Med 1041 will describe the usual duties of the person, conditions of work– both physical and mental demands, ability perform present duties, any barriers tosatisfactory performance (e.g. dexterity, mobility, co-ordination, lifting & carryingability, memory, concentration, judgement, impulsivity, ability to form relationships,speech or hearing impairment), efficiency and response to training, opinion on likelycareer progression, recent and past operational experience, comments on motivationmorale and personal habits (smoking, alcohol use and appearance) and how thesemay have changed, comment on social and welfare circumstances, any equality anddiversity issues, finances, legal and family problems, and an opinion on retention intheir current assignment and / or the Service and any alteration in employment orworking hours.
d. Likely Consequences
(1) If Command are already aware of the referral there will no be no likely additionalconsequences.
(2) If the report request alerts Command to the referral, this should encourageCommand to engage positively with the referred person and their welfare.
(3) There may be concern on part of the referred person about the effect referralwill have on their career and the on the attitude of Command and other colleaguestowards them. These concerns should be discussed. In particular it should be drawnto the patient's attention that mental health difficulties often cause occupationalproblems in themselves which can impair their career progression whereas anyintervention by a DCMH will be aimed at returning an individual to full fitness in atimely fashion. Ultimately, if the person does not consent to the request, then thatposition should be accepted and the lack of F Med 1041 and reason for this shouldbe noted in the referring F Med 7. In discussing the request the following can benoted:
(a) More than half all those referred2 to MH services return to full fitness (P2).
(b) All leadership courses from CO designate Course to LRCC havepresentations on stress management, which aim to ensure that leaders areinformed about causes and effects of stressors and strain, provide simplemeasures to manage stress and sources of support and develop theirknowledge to help counter stigmatising beliefs about stress.
(4) The consequence of not having an F Med 1041 raised is that the mental healthprofessional may not be able to form an adequate opinion about their occupationalfitness and thus provide advice on an appropriate medical category or decide ontreatment options.
2. In a limited study of 12 months of referrals to a DCMH in 2007 68% of the referrals returned to full fitness.
UN
CO
NTR
OLL
ED
WH
EN
PR
INTE
D
BRd 3(1)
28C-1June 2016 Version 1
ANNEX 28C
GUIDANCE ON THE COMPLETION OF AN F MED 1041
1. IntroductionThe F Med 1041 replaced the F Med 8. However the principles in completion of the form
remained much the same. The form can be used for any specialist medical opinion, not justpsychiatric cases. Initiation of production is by the unit Medical Officer, who will gain theconsent of the individual about whom the report is to be made. Because of the associationwith specialist medical opinion many people assume that some form of specialist knowledgeis required. In fact the F Med 1041 is a relatively simple form which can be extremely helpfulfor a healthcare professional seeing the patient. In cases where the person is to be seen bypsychiatric services, the aim is to give the mental health professional a picture of his/hernormal behaviour pattern and whether there have been any marked recent changes. Thenotes that are attached are intended to assist by indicating some of the categories ofinformation which may be useful in helping the health professional to disentangle cause andeffect in a patient’s symptoms and distinguish illness from a normal reaction to stresses ofliving. The form itself has different sections which have notes on what information is required.They and those below should not be regarded as comprehensive, or allowed to restrictcommunication of information thought by the compiler to be important. Much of the informationmay not be relevant to the patient’s illness but it is not possible to predict in advance what isand what is not important. The request for F Med 1041 may come “out of the blue” andtherefore raise, for the first time, the question of the Serviceperson’s fitness for their job. Oftena psychiatric assessment is a screening process aimed at the prevention of occupational orhealth problems. Thus, a request for a F Med 1041 should not be taken to indicate that thesubject may have become unreliable in their job, a security risk or dangerous, or changed intheir ability to discharge their Service responsibilities.
2. Completion
a. The F Med 1041 should be signed by the Commanding Officer, but the preparation isoften devolved onto a Section Commander or Head of Department. It is appropriate anduseful to consult Junior Officers and Senior Non Commissioned Officers to gain a morerounded impression of the person.
b. The fact that a Serviceperson has only just arrived at a unit does not mean that auseful F Med 1041 cannot be completed. First impressions, however brief, may providemore useful information than Confidential Reports, (which should be photocopied andforwarded with the F Med 1041).
c. If the person is potentially temperamentally unsuitable the compiler would be welladvised to look at Para 5443 to familiarise themselves with what that term means.
UN
CO
NTR
OLL
ED
WH
EN
PR
INTE
D
BRd 3(1)
28C-2June 2016 Version 1
3. Additional Information This can be obtained from:
a. JSP 950 Vol 1 Chap 2 Leaflet 1-2-4.
b. The Unit Medical Officer.
c. Base-port Department of Community Mental Health.
4. Individual Sections of the F MED 1041
a. Section 1. Description of Present Duties: Give details of all their duties and theirworking environment, especially if it is hazardous, noisy, cramped, long hours, extremesof temperature or of any other difficult condition. Give some indication of how stressful,demanding or menial the job is.
b. Section 2. Ability to Perform Present Duties: If emotional distress has beenobserved then this should be noted and what reasons might be relevant. This may ariseas a result of retrospective analysis when F Med 1041 is requested. Issues may bephysical or psychological. This section gives information on factors contributing to theirstate just before or at the time medical help is sought.
c. Section 3. Identifiable barriers to satisfactory performance of essential tasks:Consider capacities relevant to duties of trade / branch. Examples include: manualdexterity, mobility, physical coordination, ability to lift, move or carry objects, memory,concentration, judgement, impulsivity, difficulties with relationships, speech or hearingimpairment.
d. Section 4. Efficiency and response to enhanced professional / trade training:
(1) Is he/she good at his/her trade?
(2) Does he/she require constant supervision?
(3) Does he/she learn by his/her mistakes?
(4) What his/her attitude when confronted by his/her mistakes?
(5) Is he/she keen to learn or to accept additional tasks or is he/she usually missingwhen extra work occurs?
(6) Have there been any recent significant changes in his/her efficiency orresponse?
(7) Does he/she show potential for further promotion?
e. Section 5. Likely career progression in terms of activity based on standard careerpathway irrespective of performance to date.
f. Section 6. Recent and past operational experience.
UN
CO
NTR
OLL
ED
WH
EN
PR
INTE
D
BRd 3(1)
28C-3June 2016 Version 1
g. Section 7. Comments on motivation, morale and personal habits and how thesehave changed (smoking, alcohol intake, appearance, disciplinary issues and attitude toService. Include:
(1) Is he/she usually punctual?
(2) Do other Sections or Units ever praise or criticise him/her for any reason.
(3) What seems to have been his/her general attitude towards Service life anddiscipline?
(4) Does he/she involve himself/herself in unit social activities? If he/she does notspontaneously participate how does he/she respond to invitations to take part?
(5) Have there been any recent and significant changes in his/her behaviour.
(6) Are there any outstanding charges against him/her? If so, is this a commonfeature or is the conduct previously acceptable?
(7) Is he/she friendly and outgoing or is he/she solitary and withdrawn?
(8) Does he/she seem to have many friends and what is his/her apparentrelationship with his/her Seniors/Subordinates/Colleagues?
(9) Is he/she normally cheerful or morose? Does he/she fluctuate between the twoextremes?
(10) Is he/she constantly criticising or complaining without good cause? How doothers react to him/her?
(11) What is his/her standard of personal appearance? If criticised, how does he/she respond?
(12) What are his/her leisure activities?
(13) Does he/she drink alcohol in significant amounts? If so is this in a crowd or ishe/she a solitary drinker. Does he/she ever drink during the day, and if so to whatextent does it affect his/her work.
(14) Have there been any recent significant changes in his/her outlook or personalhabits, particularly anything you believe may indicate use of non-prescribed drugs.
h. Section 8. Other relevant information including workplace, social and welfarecircumstances, E&D issues, financial, legal & family problems.
UN
CO
NTR
OLL
ED
WH
EN
PR
INTE
D
BRd 3(1)
28C-4June 2016 Version 1
i. Section 9. Executive/Management comments on advisability of retention in currentassignment, in current trade / branch and in the Service (suggest an appropriatealternative employment or alternative hours of duty where appropriate). If disciplinarymatters are outstanding, a comment on advisability on pursuing these matters in the eventof a recommendation to discharge the person would be helpful. Whilst the mental healthassessment may well be addressing issues of retention it is vital to have the unit’s opinionon this. Reports ending with “Please assess this person’s suitability for continued service”are not very helpful.
j. Section 10. Executive/Management Comments on Advisability of Retention inPresent Posting/Assignment/Appointment, in Present Employment or in the Service:Comments in this section relate to your opinion generated from the facts that you haveprovided in the above sections. They should cover the issue of retention in the Serviceand/or alternative employment in another part of the Service. It would also be appropriateto express an opinion on the Service interest in retention, for example, if there areoutstanding disciplinary matters.
5. AccessA completed F Med 1041 when held in the patient’s health records is subject to the normal
rights of access by the patient under the Access to Heath Records Act 1990. Under theprovisions of the Act, however, the Health Professional holding the FMed 1041 has discretionto withhold access to that part of the record which they consider would be harmful were thatpart of the record shown to them. With the current consent procedure, the whole process ofraising the F Med 1041 should be very open, and it is good practice to show the individual whathas been written, in the same way as an Appraisal report.
UN
CO
NTR
OLL
ED
WH
EN
PR
INTE
D