-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
1/67
BRAIN IMAGING
Interpretation of Brain CT and MRI
Angela Nelson, MSN, RN, CCRN,ACNP-BC
Department of Neurosurgery
I have no current affiliation or financial arrangement with
any grantor or commercial interest that might have direct
interest in the subject matter of this CE Program
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
2/67
Objectives
Identification of normal brain anatomy on
both CT and MRI imaging
Identification of common CNSabnormalities on both CT and MRI
imaging
Identification of appropriate radiographic
studies to be obtained for the more
common suspected CNS abnormalities
Brain Anatomy
Layers covering the Brain
SkinPeriosteumBone Cranium epidural
space is between dura mater andthe bone. Superior Sagittal
Sinuslies here
Dura Mater hard mother(leather like)
Subdural space lies between duraand arachnoid
Arachnoid Membranespider (spider web)
Subarachnoid spaces liesbetween the arachnoid and pia
Pia Gentle Mother (thinlayer adhering closely to brain)
Cerebrum
4 Lobes: Frontal, Temporal, Parietal andOccipital
Falx Cerebri Separates the 2 hemispheres
Tentorium Cerebelli Separates the cerebellumfrom the
Cerebrum
Gyri Rounded ridges on surface of brain
Sulci Shallow groves separating the gyri
Fissure Deeper groves
Gray Matter Unmylinated Nerve Fibers
White Matter Mylinated Nerve Fibers
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
3/67
Review of Lobes
Frontal-Personality, judgment, abstractreasoning, social
behavior, language
expression and movement Temporal-Hearing, language
expression,
storage and recall of memory
Parietal-Interprets and Integratessensations including pain,
temperature,touch, size, shape, distance and texture
Occipital-Interprets visual stimuli
Right and Left-Cerebral Hemispheres
connected by Corpus Collosum
RightEmotion
Prosopagnosia
Music
Spatial Relationship
Left
Logic Brain
Speech
Math
Science
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
4/67
Falx Cerebri
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
5/67
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
6/67
Basal Ganglia
Corpus Striatum Caudate Nucleus
Lentiform Nucleus Putamen and Globus
Pallidus
Interconnected nuclear masses deep
within cerebral hemispheres involved in
the initiation of voluntary movements,
controls of postural adjustments
associated with voluntary movements
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
7/67
White/Gray Matter
White Matter
Consists mostly ofmyelinated axons(surrounded by a fattysheath
containingmyelin) that connectvarious gray areas ofthe brain to
eachother
Gray MatterContains cell bodies aswell as fibers of
unmylinated neurons
Gray matter includes thebasal ganglia (caudatenucleus,
putamine,globus pallidus),thalmus, hypothalmus,subthalmus,
andcerebellar nuclei
Cerebellum
Maintains muscle tone, coordinate muscle
movement and controls balance
A disorder of this area may causedizziness, nausea, balance
and
coordination problems
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
8/67
Cerebellum
Brain Stem
Composed of Medulla Oblongato, Pons, andMidbrainMedullaAutonomic
Function (HR, RR, BP)
PonsArousal
Respiratory
Midbrain Controls sensory response
Produces autonomic behavior necessary forsurvival
Pathways for nerve fibers between higher andlower neural
centers
Origin for 10 of 12 pairs of cranial nerves
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
9/67
Medulla
Pons
Ventricular System
Contains the CSF
Composed of lateral ventricles, foramina
of Monro, the third ventricle, aqueduct ofSylvius, and the forth
ventricle
Choroid Plexus located throughout thesystem makes the CSF
CSF leaves the ventricles through theforamina of Magendie and
Lushka toreach the subarachnoid space
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
10/67
Lateral Ventricles
Foramen of Monroe
Third Ventricle
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
11/67
Aquaduct of Sylvius
4th Ventricle
Cerebral Circulation
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
12/67
Cerebral Circulation
MR Angiography
Internal Carotid Artery
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
13/67
Middle Cerebral Artery
Anterior Cerebral Artery
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
14/67
Venous Drainage
Venous Sinus Drainage
MR Venography
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
15/67
Computed Tomography
Nobel Prize Winner Sir Godfrey Hounsfielddeveloped CT for
clinical use in 1972-1973
The first company to introduce the CTscanner was EMI (English
MusicalInstruments)-the same company thatdistributed the Beatles on
the Apple label
Grossman, R.I. and Yousem, D.M. The Requistes. Neuroradiology.
Second Edition. Philadelphia, PA,2003
Computed Tomography Physics
Uses a highly collimated x-ray beam
Photons that pass through the patient are
collected by CT detectors which show a
differential rate of intensity on a gray scale
The beam is rotated across the patient at many
angles so as to get a differential rate of
absorption
Grossman, R.I. and Yousen, D.M. The Requistes. Neuroradiology.
Second Edition, Philadelphia, PA, 2003
Indications of Use of CT
First line in evaluation of a change in mental status
Test of choice for those with implantable devices
Shows acute and sub acute blood (ICH/SAH, SDH)
Bony abnormalities, i.e. Trauma or fracture
Edema/Mass effect
Abnormalities in size and shape of structures
i.e. brain tissue atrophy, gyri effacement with swelling
Hydrocephalus
Hemorrhagic stroke
Add contrast if looking for tumor, abscess, or cerebralarteries
and veins
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
16/67
Disadvantages of Computer Tomography
Poor imaging for demyelinating disease
Poor resolution in the posterior fossa of
the brain primarily due to streak artifactfrom the bones
Density gradients on CT
Bone
Calcification
Contrast material
Clotted blood
Some tumors with densely packed cells
Grey matter
White matter
Edema
Pus
Necrotic Cavities
CSF
Fat Air
How things appear on a CT?
Acute Blood/Calcifications-White
Chronic Blood Collection-Low density black to
gray as increasing density CSF/Air-Black
White Matter-Less dense than gray matter and
therefore will be darker
Ischemia-Lower density and therefore will be
darker and may not appear for 12 hours
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
17/67
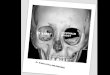
Radiographic Images
What is on the left
side of the picture
represents the rightside of the patients
brain
Axial-top to bottom or
bottom to top
Radiographic Images
Sagittal-Side to side
T1
Radiographic Imaging
Coronal-Front to back
or back to front
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
18/67
Orbit
Spenoid
Temporal
Mastoid Air
Auditory
Cerebellum
Frontal Lobe
Sylvian Fissure
Temporal Lobe
Supracellar Cistern
Midbrain
4th Ventricle
Cerebellum
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
19/67
Falx Cerebri
Frontal Lobe
Anterior Horn
3rd Ventricle
Quadrigeminal Cistern
Cerebellum
Radiology Atlas.exe
Caudate
Ant Horn Lat Ventricle
Internal Capsule
Putamen/Globus Pallidus
3rd Ventricle
Quadrigeminal Cistern
Vermis
Occipital Lobe
Falx Cerebri
Frontal Lobe
Body of Lateral Ventricles
Corpus Callosum
Parietal Lobe
Occipital Lobe
Superior Sagittal Sinus
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
20/67
Falx Cerebri
Superior Sagittal Sinus
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
21/67
How to Approach a Read
View the Subdural windows for bony
defects, fractures
Are the sinuses opacified
Bony Windows
Soft Tissues (brain window)
View the lateral, 3rd and 4th ventricles
Are they enlarged, compressed, distorted,
diplaced
Is there anything in them other than
choroid plexus
Look for blood or debris especially in the
dependent portions
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
22/67
Brain Window
Is there a focal density abnormality in the
brain?
Is there something that is notsymmetrical?
Is it mass producing or volume losing?
Are midline structures midline?
Are the sulci symmetrical or effaced?
Are the lateral ventricles symmetrical?
Brain Window
Is the gray/white junction seen around
both cerebral hemispheres?
Is the insular ribbon seen?
Are the basal ganglia distinct from the
internal and external capsule?
Spinal Cord
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
23/67
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
24/67
Sinuses
Orbits
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
25/67
ExternalAuditoryCanal Mastoid
Air Cells
Medulla
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
26/67
Cerebellum
TemporalLobe
4thVentricle
4th
Ventricle
Basilar Artery
Pons
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
27/67
Basilar Artery
Supracellar CisternSylvian Fiisure
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
28/67
Frontal Lobe
Parietal Lobe
QuadgeminalCistern
Anterior HornLateral Ventricle
Third Ventricle
Vermis ofCerebellum
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
29/67
OccipitalHorns
Occipital Horns
Caudate Head
Choroid Plexus
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
30/67
Body of Lateral Ventricles
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
31/67
White Matter
Faux Cerebri
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
32/67
Central Sulcus
Pre Central Gyrus
Post Central Gyrus
Intraparietal Sulcus
Cental Sulcus
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
33/67
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
34/67
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
35/67
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
36/67
Meningioma/CT
Epidural Hematoma/CT
Glioblastoma/CT
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
37/67
Hypertensive Cerebellar Bleed/CT
Coagulopathic Bleed/CT
Chronic Subdural Hematoma/CT
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
38/67
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
39/67
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
40/67
Diffusion MRI
Diffusion Weighted Imaging (DWI)
Determines the ease of water diffusion
Can determine cerebral ischemia within minutes
of irreversible damage Most sensitive way of determining an
acute
infarction
Good in differentiating vasogenic edema
(generally tracks along white matter and spares
the gray matter)
Appears as dark CSF, bright Fat and Lesions
DWI
Apparent Diffusion Coefficient (ADC)
Measures the brownian motion of protons
High ADC will be seen in CSF where there
protons can freely move
Low ADC will be found with new strokes
and tumors where they are more tightly
packed together
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
41/67
T1 Pre and Post contrast
CSF appears black
Subcutaneous tissue
(beneath the skull)appears white
Blood appears white
White matter brighterthan gray matter
Lesion will appear dark
Shows blood clearer
*Note-T1 post-sinus/nasal terbinates,choroid plexus bright
T2 MRI
CSF appears white
Subcutaneous tissueappears black
Blood appear white
White matter darker thangray matter
Shows older changes andmicrovascular
More accurate for brainpathology
Flair/Echo Gradient
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
42/67
Tonsils
Vertebral Artery
Falx Cerebelli
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
43/67
Vermis
Medulla, Verebral Artery, 4 th ventricle
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
44/67
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
45/67
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
46/67
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
47/67
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
48/67
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
49/67
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
50/67
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
51/67
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
52/67
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
53/67
Diffuse Axonal Injury
Frequent result of traumatic deceleration injuriesresulting in
shearing of axons and small bloodvessels
Frequent cause of persistent vegetative state
Usually occur at gray/white matter junction
DAI suggestive in any pt who demonstratesclinical symptoms
disproportionate to imagingfindings
Up to 90% of these patients remain in apersistent vegetative
state, rarely die
DAI/Diffusion
Glioblastoma
Average age of diagnosis 50-70
Occur more commonly in men
Most patients die within 8-18 months
Clinical presentation depends on location
of the tumor; stroke like symptoms, focal
neurological deficits, headache, change in
behavior, seizure
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
54/67
GBM/T1/T2
Meniogioma
15% of all brain tumors
More common in women
Usually occur in 3rd to 6th decade of life
Discrete well defined dural masses
Can remain clinically asymptomatic for years as
they grow slow
Common symptoms include focal defecits,
seizures, headaches and psycho organic
syndrome
Meningioma/T1/T2
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
55/67
STROKE
CT is preferred for intracranial
hemmorhage
For non hemorrhagic stroke a CT can benegative for 24-36
hours
Flair/T2 MRI can detect in 6-12 hours
Diffusion MRI can detect within minutes
STROKE/Ct/T1
T1
T2
FlairDWI
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
56/67
Metastatic Tumor
66 year old right
handed female with
PMH mestatic lungcancer, s/p Right
Lobectomy with
radiation and Right
masectomy
1-2 months of slurred
speech, word finding
difficulty and lethargy
Exam:
Mild right upper
extremity drift, mildright dysmetria
Found to have left
temporal lesions
Patient started on
Anti-convulsants and
lesion resected
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
57/67
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
58/67
Presumed Metastatic Lesions
72 year old right handed malewith Prior history of CABG,AAA,
Cardiac Stent, andrecently MylodysplasticSyndrome with a 4 day
historyof dizziness and headaches,now with confusion andreceptive
and expressivedysphagia
Exam significant for right sidedweakness, right drift,
rightfacial droop, inability to followcommands
Anticonvulsants and IVsteroids initiated
Platelet count 6
Hematology consult-found tohave high grade Mylodysplasia
Transfused multiple units ofplatelets in an attempt to
>150before OR
Patient developed AspirationPneumonia and surgery wasdelayed
Continued to deteriorate
CT Hemmorhagic Lesion
Large Left MCA Infarction
58 year old man withhistory of tobaccouse, HTN, BPH whowas in
process orbeing worked up for atransient decreasedsensation in
right arm
At work with suddenright sided weakness,right facial droop
andaphasia
Found to haveocculsion of the leftinternal carotid arteryand M1
segment leftMCA thrombus
Given TPA withoutimprovement
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
59/67
Pituitary Macroadenoma
39 year old righthanded male with noPMH.
Developed fatigue 3years ago, treated fordepression, startedon
Lexapro
Past 2 years noted adecrease in theamount of facial and
leg hair
Low testostone, LowLH
Visual fields normal
2.2 cm tumor
UnderwentEndoscopic TSSHapproach Resectionof Mass
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
60/67
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
61/67
Mystery Lesions
49 year old right handed
male with PMH of HIV,
AIDS, and Stoke presents
with a 3 week history of
headaches particularly
severe for the last 3 days
Exam significant for
dysarthric speech,
bilateral dysmetria, left
foot drop
Patient underwent
craniotomy with
pathology sent however
no cultures were sent.
Path inconclusive
Pathology inconclusive
Lesions/Old Infarctions
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
62/67
Arteriovenous Malformation
21 year old right handed malepresents with an acute onseton BLE
numbness
Had a warm sensation
throughout his body, felt dizzyand faint with a headachewhich
progressed to completeleft sided weakness
Exam significant for left sidedweakness although A/O x3
Angiogram Right frontal AVM
Underwent pre opAngio/Embolization of Lesion
AVM resected with post opAngio done
POD # 6 developedheadaches and CT revealedright frontal epidural
hematomaand pt emergently taken to OR
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
63/67
Acute Cerebral Infarction of Pre-Central
Gyrus
63 year old right
handed, male with
sudden onset oftingling in right check,
inability to speak and
could not properly use
right hand
T2 Acute Infarction
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
64/67
Communicating Hydrocephalus
CSF circulation
blocked at level of
arachnoidgranulations
Multiple Sclerosis/Flair
Age of onset 10-59, withpeak between 20-40
Demyelinating disease ofwhite matter affecting thecerebrum,
optic nervesand spinal cord
Typically hasexacerbations andremissions
Common symptomsvisual disturbances,spastic paraparesis
andbladder dysturbances
Infarction with Hemicraniectomy
Pre op Post op
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
65/67
TraumaSubdural
IntraparenchymalSAH
Epidural
Cerebellar Hemangioblastoma
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
66/67
DWI
Infarction
ADC
Melonoma with hemmorhage
XXXXXXXXXX
9.4.79
-
8/12/2019 Brain Understanding Interpretation of Ct and Mri
67/67