Embed Size (px)
Citation preview

MAGMA (2005) 18: 316–331DOI 10.1007/s10334-005-0020-0 RESEARCH ARTICLE
Miguel Martın-LandroveFinita MayobreIgor BautistaRaul Villalta
Brain tumor evaluation and segmentation byin vivo proton spectroscopy and relaxometry
Received: 25 April 2005Accepted: 23 November 2005Published online: 30 December 2005© ESMRMB 2005
Brain tumor evaluation and segmentationby 1HMRS and relaxometry
M. Martın-Landrove · F. MayobreDepartamento de Espectroscopıa yDesarrollo de Aplicaciones,Instituto de Resonancia Magnetica,La Florida, San Roman
M. Martın-Landrove (B) · I. BautistaR. VillaltaUniversidad Central de Venezuela,Facultad de Ciencias, Escuela de Fısica,Centro de Resonancia Magnetica,Grupo de Fısica Molecular,A.P. 47586, Caracas 1041-A, VenezuelaE-mail: [email protected].: +58-212-6051194Fax: +58-212-6051516, +58-212-9928903
Abstract A new methodology hasbeen developed for the evaluationand segmentation of brain tumorsusing information obtained bydifferent magnetic resonancetechniques such as in vivo protonmagnetic resonance spectroscopy(1HMRS) and relaxometry. In vivo1HMRS may be used as apreoperative technique that allowsnoninvasive monitoring ofmetabolites to identify the differenttissue types present in the lesion(active tumor, necrotic tissue, edema,and normal or non-affected tissue).Spatial resolution for treatmentconsideration may be improved byusing 1HMRS combined or fusedwith images obtained by relaxometrywhich exhibit excellent spatialresolution. Some segmentationschemes are presented and discussed.The results show that segmentation
performed in this way efficientlydetermines the spatial localization ofthe tumor both qualitatively andquantitatively. It providesappropriate information for therapyplanning and application oftherapies such as radiosurgery orradiotherapy and future control ofpatient evolution.
Keywords Relaxation · in vivoSpectroscopy · Assessment ·Segmentation
Introduction
Evaluation and segmentation of brain tumors can beassessed by proton magnetic resonance spectroscopy(1HMRS) and relaxometry, two magnetic resonance tech-niques. 1HMRS determines metabolic tissue informationby analyzing the composition and spatial distributionof cellular metabolites [1]. 1HMRS distinguishes malig-nant tumors from normal brain tissue due to signifi-cant spectral differences reported between tumor, necrosisand normal brain tissue. Recent in vivo 1HMRS stud-ies have been used to grade brain tumors [2–6]. Themetabolites involved in the differentiation of neoplasticand non-neoplastic tumors are: N-acetyl aspartate (NAA)
considered a neuronal marker, choline (Cho) a markerof membrane turnover or higher cellular density, creatine(Cre) a metabolite involved in cell energy metabolism, lac-tate (Lac) a marker of anaerobic glycolysis and mobilelipids (Lip) visible after membrane breakdown. NAA andCre decrease and Cho increases in the presence of highgrade tumors.
1HMRS spectra are mainly interpreted on the basis ofthe relative amplitudes of the above metabolites [1]. Nor-fray et al. [6] found significant differences in Cho/Cre ratiobetween tumor and normal brain regions. Vigneron et al.[7] and Nelson et al. [8] reported Cho/NAA ratios greaterthan 1.3 in spectra of histologically confirmed tumors, themean value for all tumor types being 3.91 ± 1.52. Other

317
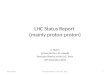
Fig. 1 1H SVS obtained from a patient with histological provenfibrillary astrocytoma grade III (patient 3). Spectrum from the tu-mor on the right and from the contralateral normal tissue on the left;TE = 30 ms, TR = 1,500 ms, 256 averages
authors reported similar values for high grade tumors [9–11]. Adamson et al. [12] reported Cho/NAA ratio lowerthan the reported above (over 1 for confirmed neoplastictumors). Presence of Lac or Lip with elevated Cho is evi-dence of relatively high grade tumors [12]. Low levels ofCho, Cre, and NAA correspond to necrosis.
Relaxation studies were used in the past for the local-ization and evaluation of tumors, being the T2-map of atissue often used as a basis for interpreting clinical im-ages [13]. Studies of multiexponential T2 decay have pre-viously been performed in both non living material [14–16]and biological systems [17–19]. Among the different imag-ing techniques that generates T2-weighted images are spinecho, fast spin-echo, and GRASE (gradient spin echo),being the first two the most accurate for anatomical detailand relaxation time determination [20]. Sometimes spin-echo techniques are combined with the application of con-trast agents [21,22] to evaluate perfusion.
Regardless of its diagnostic power, in vivo 1HMRScould be benefit by being combined with images of appro-priate spatial resolution in order to obtain improved infor-mation for treatment considerations. Some approaches forthe solution to this problem have been proposed introduc-ing the concept of nosologic image, i.e., an image wherethe pixels are classified according to the presence of disease[23]. The image is obtained either with spectroscopic infor-mation alone or combining it with T1- and T2-weighted
images [24,25]. Unfortunately, nosologic images obtainedin this way still lack of appropriate spatial resolution usu-ally limited to the spectroscopic voxel size. The aim of thiswork is to combine or fuse in vivo 1HMRS informationwith images obtained by MR relaxometry and to obtainnosologic maps of appropriate spatial resolution for theevaluation and segmentation of brain tumors.
Methods
Ten patients with different brain tumor types were analyzed inthe present work. Data obtained from measurements on twohealthy volunteers served as controls. All the patients and vol-unteers were informed about the experimental procedures to beperformed and signed informed consent forms in compliancewith ethical guidelines. All the measurements were carried outin a Siemens Magnetom Sonata, with a magnetic field strengthof 1.5 T. MR images were obtained before 1HMRS for voxellocalization. 1HMRS studies were assessed by single voxel spec-troscopy (SVS) or by chemical shift imaging (CSI) techniques.
Single voxel spectroscopy was performed by a PRESS se-quence with CHESS for water suppression, TR of 1,500 ms, 256averages and TE = 30 ms. Voxel sizes covered a range between 4.1and 5.4 cm3 and a reference voxel was used for control (Fig. 1).In some cases, when contrast with Gd-DTPA was necessary,unimportant changes in the spectrum were observed.
Chemical shift imaging provides a spectral array which mapstumor heterogeneity and determines the spatial extent of themetabolite abnormality. CSI was performed with a PRESS se-quence to obtain spatial distributions of metabolite relative con-centration across the lesion, using a TE = 135 ms, TR = 1,500 ms,

318
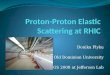
Fig. 2 Some of the CSI gridsused in this work; the red coloredinsert correspond to thosevoxels where the spectroscopicevaluation was performed
and VOI of 96 cm3 (80×80×15 mm). At TE = 135 ms, Lac sig-nal appears as an inverted doublet in the spectrum which allowsthe differentiation from the Lip signal. No lipid saturation pulseswere used. The CSI grids included the region of the lesion as wellas neighboring tissues as depicted in Fig. 2. VOI consisted of an8 × 8 cm region placed within a 16 × 16 cm field of view on a1.5–2 cm transverse section. A 16 × 16 phase-encoding matrixwas used to obtain an 8×8 array for spectra in the VOI, with anin-plane resolution of 1×1 cm and a voxel size of 1×1×1 cm3.The spectroscopy data analysis was performed only in voxelswithin an 8×8 matrix centered on the lesion, avoiding those onnon neurological structures and discarding others on the basisof poor spectral quality, i.e., low signal to noise ratio or badphase and base line adjustment. The quantification of the spec-troscopic information was based on relative values: each spec-trum was fitted for NAA at 2.02 ppm, Cre at 3.04 ppm, Cho at3.21 ppm, Lac at 1.3 ppm and Lip at 0.9 and 1.4 ppm using thefitting software in the equipment. Peak integrals and integralratios were calculated for the metabolite markers Cho, Cre, andNAA. Cho/NAA ratio was used as the main criterion in thisstudy and the Cho/Cre ratio as a secondary criterion. The crite-rion for malignancy in any voxel was a Cho/NAA ratio over 1.3.This value was used for both SVS and CSI. The voxel was con-sidered atypical if the Cho/NAA ratio had a value between 0.9and 1.29. No quantification of other metabolites was performed.
Relaxometry studies were performed after the 1HMRS stud-ies and prior to additional 1HMRS studies performed with Gd-DTPA when they were necessary to fully assess the tumoral le-sion. A standard multiecho sequence (CPMG) was used with 16echoes, at echo times given by a base TE = 22 ms and eight 5 mmthick planes centered on the tumor. The slice parameters werethe same for those used for the CSI grids. This procedure allowedfor the inclusion of two relaxometry planes in the same spatialregion of the CSI grid, facilitating the information matching be-tween the two types of measurements. The multiecho sequence
Fig. 3 Flux diagram of the segmentation procedure
was preferred to other sequences, (T2-weighted), because it pro-vides a set of images from which the relaxation rates or therelaxation rate distributions could be appropriately and quan-titatively evaluated. An image processing algorithm was devel-oped to extract the magnetization decays for different ROIs orrelaxometry voxels which come from a specific voxel from theCSI grid, providing the relaxation data. Within each ROI orrelaxometry voxel, the relaxation data were processed by an in-verse laplace transform (ILT) algorithm to obtain the relaxationrate distributions involved. The application of such algorithm

319
Fig. 4 Performance of the ILTalgorithm on a Pentium 4Workstation, 2.27 GHz. a Theprocessing time depends on thenumber of replicas and exhibitsa linear behavior, with anaverage time of 3.29 s perreplica. b Spectrum comingfrom a single relaxation voxel asa function of the number ofreplicas used to define it. Noticethat for as much as 50 replicas,i.e., about 164 s in processingtime, the relaxation spectrumremains stable in its structure
is fully justified since there is a partial volume problem [26–28],i.e., the voxel size is usually big enough to contain several tis-sue types, and it is expected that the relaxation spectrum shouldexhibit some structure depending on the proportion on whichany of the different tissue types are present in the voxel. Usually,segmentation methods based on T2-weighted images determinethe relaxation rate distribution by calculating the relaxation ratepixel by pixel using a small number of echoes (2 or 4), assuminga single exponential decay. This brings as a consequence that thecalculated relaxation rate is some kind of average of the relax-ation rates present in the pixel distorting the actual relaxationrate distribution in any selected ROI. The ILT algorithm will be
discussed in detail in the next section. The relaxation spectra ob-tained in this way were classified according to the spectroscopicinformation thereby determining the relaxation rates associatedto the different tissue types present in the lesion for a partic-ular patient, (i.e., those relaxation spectra coming from a CSIvoxel are all associated to the type of tissue present in that vo-xel as established by the spectroscopic result, which depends onthe metabolic ratios). Once the relaxation spectra were obtainedand classified, the relaxation rates for the different tissues weredetermined, and their values were used for the segmentation pro-cedure. The segmentation was made on a pixel by pixel basis by alinear regression algorithm to determine the proportion in which

320
Table 1 Proton magnetic resonance spectroscopy (1HMRS) and histopathological results of ten patients with brain tumor
Patient number Age 1H MRS (Cho/NAA) 1H MRS (Cho/Cre) 1H MRS (NAA/Cre) Biopsy
1 50 15.75 6.10 0.39 Glioblastoma multiforme2 46 X X X Glioblastoma multiforme3 19 3.18 3.46 1.09 Fibrillary astrocytoma grade III4 16 2.66 1.64 0.62 Oligodendroglioma grade II5 37 1.79 1.22 0.68 Fibrillary astrocytoma grade II6 28 3.13 1.89 0.60 Fibrillary astrocytoma grade II7 37 1.10 1.42 1.30 Non-Hodgkin’s lymphoma8 7 0.26 1.83 6.99 Not performed9 37 1.88 1.72 0.92 Meningioma
10 10 0.85 1.33 1.57 Meningioma
Cho/NAA, Cho/Cre, and NAA/Cre ratios are calculated from single voxel spectroscopy (1H SVS) spectra. NAA signal was notdetected in tumor no. 2 spectrum; for this reason ratios were not calculated (X)
Table 2 Chemical shift imaging (CSI) results of the ten brain tumors studied. number of voxels analyzed, number and percentage of spectrasuggesting malignancy (Cho/NAA = 1.3 or over) and number and percentage of atypical spectra (Cho/NAA between 0.9 and 1.29)
Tumor number Number of voxels analyzed Malignant spectra number (%) Atypical spectra number (%)
1 26 20 (77%) 4 (5%)2 6 5 (83%) 1 (17%)3 20 7 (35%) 6 (30%)4 Not performed – –5 10 3 (30%) 2 (20%)6 6 5 (83%) 07 10 2 (20%) 1 (10%)8 Not performed – –9 6 3 (50%) (*) 2 (33%)
10 6 2 (33%) (*) 0
In the case of meningiomas (*), it was obtained a high Cho/NAA ratio, not necessarily associated to malignancy
the different tissue types are present in the pixel. The completesegmentation procedure can be seen as a flux diagram in Fig. 3.Control slices, i.e., those not affected by the lesion in the samepatient, and control cases were used to test the segmentationprocedures.
The ILT algorithm
There are a wide variety of different approaches [29,30] tosolve numerically the ILT problem, and some of them areof standard use in many laboratories around the world.Such is the case with the DISCRETE and CONTIN pro-grams [29], which are applicable in many situations. Mostof these approaches make use of assumptions about themathematical properties of the function to be obtainedby the inversion procedure and rely on these propertiesin the general development of the algorithm, while oth-ers introduce regularization parameters or a fixed numberof components in the relaxation spectrum. The algorithm
developed for this and other investigations [31,32] wasshown to be adequate for precise line shape determina-tion. Nevertheless, there are always some drawbacks: along processing time due to the optimization procedurebased on simulated annealing as well as the requirementsof appropriate and complete data acquisition; i.e., im-proper sampling of the decay introduces artifacts in therelaxation rate spectrum, which sometimes may be easilydetected and eliminated from the relaxation spectrum.
The ILT algorithm used in this work is described below.Since the signal is known in a finite number of points onthe real axis, the numerical solution of the problem cor-responds to a very ill-posed first-kind Fredholm integralequation of the form
M(t)=∞∫
0
dλ e−λt P (λ), (1)
where M(t) corresponds to the transversal magnetization,and λ is the relaxation rate. Equation (1) represents a very

321
Fig. 5 Average probability distribution function or relaxation ratespectra for different malignant lesions, a, b correspond to gliobas-toma multiforme, d corresponds to an oligodendroglioma grade IIand c–f correspond to fibrillary astrocytomas
general way of expressing the transversal relaxation decaydepending on the particular relaxation rate distributionP(λ) [31–33]. This distribution can be represented by ahistogram or collection of bars of variable width, which isgiven by
P(λ)=N∑
k=1
Pk(λ), (2)
where N is the number of components, and Pk(λ) is thekth elementary component given by
Pk(λ)=Pk �(λ−λk)�(λk +�λk −λ). (3)
This representation can be used for the description ofdiscrete and continuous distributions as well. In the par-ticular case of a discrete distribution, a set of very local-ized functions with a small width can be obtained, andit is indistinguishable from a very narrow and continuousdistribution. This width is a function of relevant physicaleffects, noise, and loss of information due to the use of anumber of finite points. In practice it is very difficult toseparate each contribution, although in the case of noise,previous filtering procedures can be considered.

322
Table 3 Relaxation rates, 1/T2 (s−1), for edema or necrosis, tumor, and normal gray/white matter in the different pathologies studied in thiswork
Tumor type 1/T2 (s−1) Edema or Necrosis 1/T2 (s−1) Tumor 1/T2 (s−1) Gray/white Matter
Glioblastoma multiforme 1.88 6.61 11.02Glioblastoma multiforme 2.22 6.69 11.47Fibrillary astrocytoma grade III 1.74 6.26 9.34Oligodendroglioma grade II 2.67 5.52 8.67Fibrillary astrocytoma grade II 1.89 7.43 14.48Fibrillary astrocytoma grade II 3.43 5.05 11.91Non-Hodgkin’s lymphoma 2.20 5.18 12.52Craniopharyngioma 2.12 6.67 9.80Meningioma 0.65 6.67 25.26Meningioma 1.77 7.47 13.70
The rates were obtained by analysis of the relaxation spectra shown in Fig. 5
The problem to be solved can be stated as an optimi-zation procedure where a set of distribution components,which provide the best fit for the M(t) function, has to befound. For this purpose simulated annealing and Metrop-olis algorithms [34–37] were used. The configuration tobe tested in each Metropolis algorithm cycle is given by afinite number of elementary components that are sampledin the relaxation rate position λk and width �λk for thekth element. At the same time, the total number of com-ponents N for the configuration is also changed, which isa new feature in an optimization procedure of this kind.This sampling in the total number of components is per-formed by considering two options with the same proba-bility within the Metropolis algorithm cycle:
(1) The total number of components N is unchanged, andin this case one component is taken with equal proba-bility from the current configuration set to change thenumerical value of the relaxation rate position andits width. This change is achieved first by adding anincrement with uniform probability within the interval[−ε,+ε] and taking the absolute value of the result forthe energy position; then the same process is repeatedfor the corresponding width. The value ε=1 was takenarbitrarily. The time scale is set by assuming that themaximum measurement time is equal to 1.
(2) A new component is created and added to the existingconfiguration. The creation of this component impliesthe generation of a relaxation rate position and its cor-responding width by means of the following steps: (a)A choice with equal probability is made in order todecide whether the new relaxation rate is going to bewithin the existing set or, on the contrary, happensto be the maximum of the new configuration set. (b)In the former case the new relaxation rate is placedwith equal probability in between two other relaxa-tion rates of the old configuration, while in the lattercase, the new relaxation rate is chosen with a non uni-
form probability distribution. This probability distri-bution provides a practical boundary for the domainto be sampled, and it should vanish for large relaxationrates. The simplest choice corresponds to an exponen-tial distribution, but other distributions can be con-sidered as well. In the present implementation of thealgorithm, the exponential distribution was chosen.The cost function was chosen from results of robuststatistics to noise filtering, and it is known in the lit-erature as the least absolute deviation (LAD) optimi-zation (38). For nP , points it is given by
�= 1nP
nP∑i=1
∣∣Mexp(ti)−Mop(ti)∣∣∣∣Mexp(ti)
∣∣ (4)
and it can be seen as an average relative error. In thepresence of information loss the absolute value pro-vides better noise filtering than the usual quadraticvalue since the median is much less sensitive than themean to the presence of fluctuations of any size. Thequantity Mexp(t) corresponds to the measured signaland Mop(t) is the optimized signal given by
Mop(t)=∑
k
∞∫
0
dλ e−λtPk(λ). (5)
In this work a fast simulated annealing approach isused (Cauchy machine) [39], which mean that the tem-perature parameter is proportional to the inverse ofthe Monte Carlo iteration number. Up to 300 parallelsimulations with different initial conditions were per-formed in order to avoid the problem of the appear-ance of metastable states [37–39] which are intrinsic tothe metropolis algorithm. For each simulation, 10,000Monte carlo steps were performed during an anneal-ing cycle. Stability is assumed when there is no changeof the parameters during a complete annealing cycle.Once stability is reached, it may be supposed that the

323
Fig. 6 Variation of the imagesegmentation according to thesquared correlation coefficientvalue in the range from 0.91(top left) to 0.99 (bottom right).Only pixels shown in colorsatisfied the correlationcoefficient criterion
lowest minimum was obtained in every simulation.The final histogram is taken by averaging the totalset of individual histograms, each one of them cor-responding to different initial conditions. This pro-cedure is performed in order to avoid the increasein condition number for the matrix used in the leastsquare procedure when the number of components isalso increased. The total processing time depends onthe number of relaxation voxels, the number of datapoints for each relaxation data (eight in the presentcase) and the number of parallel simulations or rep-licas. In the present work a Pentium 4 Workstationworking at 2.27 GHz was used for the calculations.The average processing time for a complete simula-tion was of 3.29 s, usually comprising two or more
annealing cycles in the optimization procedure. Theaverage time needed for the evaluation of the histo-gram in a relaxation voxel was of 999.13 ± 195.74 s,for 300 simulations or replicas. Some results of theperformance of the ILT algorithm are shown in Fig. 4.By inspection of the figure, it can be seen that the totalprocessing time can be shortened considerably usinga smaller number of simulations (instead of 300) andby an appropriate selection of the relaxation voxelsin order to reduce its number. Further reduction ofthe processing time up to a limit close to the process-ing time per simulation or replica can be achieved byparallel computing. In its present form, the ILT algo-rithm can be used as a tool to determine precisely therelaxation spectrum within a region of interest but it

324
is impractical for the analysis of relaxation data on apixel by pixel basis.
Results and discussion
The histological tumor type found in the patientbrains were glioblastoma multiforme(GM) (two patients),fibrillary astrocitoma grade III (one patient), fibrillaryastrocytoma grade II (two patients), oligodendrogliomagrade II (one patient), non-Hodgkin’s lymphoma (one pa-tient) and meningioma (two patients). No biopsy was ob-tained from tumor of patient no.8 but MRI suggesteda germinoma o craniopharyngioma. This patient didnot return to the hospital after the MRI, 1HMRS, andrelaxometry studies.
1HMRS ratios from control subjects were similar topublished normal ratios [1]. 1HMRS and histopatholog-ical results of ten brain tumors are presented in Table 1.All tumors exhibited different MR imaging and 1HMRSresults are expressed as Cho/NAA value. Cho/NAA ra-tio was used to distinguish between normal, atypical andprobably malignant tissue. Vigneron et al. [7] and Nelsonet al. [8] found significant Cho levels and a Cho/NAA ratioabove 1.3 in patients with histologically confirmed tumorsand 1.73 for confirmed cancer. Even though references [16]and [17] represent studies that were performed at long echotimes, it can be expected that the threshold ratio Cho/NAAfor pathology can be also assumed for short echo times,since the transversal relaxation times for Cho and NAAare very similar [37–42]. For this reason, in the presentwork any voxel, SVS or CSI, with a ratio Cho/NAA above1.3 was considered suggestive of malignancy. This assump-tion turned out to be in good agreement with the histo-pathological results. Eight patients presented Cho/NAAratios over 1.3. 1HMRS results were confirmed later byhistological analysis. Low and high grade tumors (gradeII, III, and IV astrocytomas as well as non-Hodgkin lym-phoma) presented Cho/NAA ratios over 1.3. Meningio-mas presented Col/NAA ratios over 1.3. This result agreeswith the literature were high Cho signal in meningiomashas been reported [2,42,43]. No alanine was detected.Benign tumor presented a Cho/NAA below 1.3 (patientno. 8).
SVS results are showed in Table 1. The highestCho/NAA and Cho/Cre values were obtained in patientno.1 who presented a GM. No NAA and high Cho sig-nals were detected in patient no.2 who also presented aGM. patient no. 3 who had a grade III astrocytoma pre-sented Cho/NAA and Cho/Cre values slightly elevatedif compared with grade II astrocytomas. Even in thesmall number of patients studied in this work, the 1HSVS results agree with those of the literature where thehigher ratio values correspond to higher tumor grades
Fig. 7 Contour plot for a glioblastoma multiforme. Color scale isrelated to the value of the AR coefficient: red color indicates maxi-mum value and blue indicates minimum value
Table 4 Values of p,<p >,v, and ρ for patients and controls
Patient number p 〈p〉 v ρ
1 0.8415 8155 85.522 0.9059 16030 137.653 0.7152 4394 53.354 0.7838 1947 69.425 0.6873 6046 79.256 0.7937 0.5819±0.0749 3095 86.877 0.8393 2849 100.418 0.6688 7793 32.889 0.8436 5954 133.3510 0.7586 9914 72.82C1 0.6191 489 51.45C2 0.5927 714 37.31C3 0.6149 316 26.04C4 0.5653 0.7838±0.0766 57 21.95C5 0.5507 23 20.31C6 0.6863 878 49.48C7 0.4444 4 37.89
Controls C3–C7 correspond to planes unaffected by the lesion.All the quantities represent averages over the complete set ofplanes (eight in total) except for controls C3–C7. All quantitiesare adimensional

325
Fig. 8 Segmented images: a andb for glioblastoma multiforme,c and d for meningiomas. Left:segmentation using RGBpalette, middle: segmentationwith gray palette and right:T2W image for TE = 22 ms
[4,44–46]. NAA/Cre ratios did not discriminate betweenpossibly malignant and normal tissue.
The number and percentage of CSI voxels withCho/NAA above 1.3 (malignant) and between 0.8 and 1.29
(atypical) from the total voxels analyzed are presentedin Table 2. Different numbers of voxels were analyzedfrom each patient. All patients with low and high gradetumors (II, III and IV astrocytoma and non-Hodgkin’s

326
Fig. 9 Segmented image. a forfibrillary astrocytoma grade III,b and c, for fibrillaryastrocytomas grade II, c foroligodendroglioma grade II.Left: segmentation using RGBpalette, middle: segmentationwith gray palette and right:T2W image for TE = 22 ms
lymphoma) presented atypical and possible malignantvoxels. Meningiomas also presented voxels with a highCho/NAA ratio [2,42,43].
For each voxel in the relaxometry grid of a partic-ular case, the relaxation rate spectrum was determined
using the ILT algorithm discussed in the previous section.Each relaxation rate spectrum obtained was correlatedwith SVS and CSI results and compared with histopa-thology. This was made taking into account not only thespectroscopic data for that voxel but also the data coming

327
Fig. 10 Segmented images forthe control cases using the RGBpalette. C1 and C2 correspondto healthy volunteers, while C3through C7 correspond tounaffected slices in patients.Relaxation rates used for thesegmentation in control casesC3 through C7 are thoseobtained from the analysis ofthe lesions and depicted inTable 3
from other voxels for which single relaxation spectra andinterpretable spectroscopic data were available. Once theassignment of relaxation rates to pathology was estab-lished, an average relaxation spectrum over the lesion canbe obtained to further determine the typical relaxationrates. The average relaxation spectra are shown in Fig. 5and the results are summarized in Table 3.
Inspection of Table 3 and Fig. 5 demonstrate that is notpossible to obtain a typical relaxation spectrum or valuesof the relaxation rate for a particular type of tumor andthat it is patient dependent. This is due to the fact that thelesions are of different dimensions and exhibit different
tissue heterogeneity, but nevertheless, a certain range canbe establish for each kind of tissue present in the image:from 0.65 to 3.43 s−1 for edema or necrosis, from 5.05 to7.47 s−1 for tumor and from 8.67 to 25.26 s−1 for normalor unaffected tissue. In order to obtain a segmentation ofthe lesion, we have selected a color code to indicate theexistence of pathology: R (red) corresponds to tumor, G
(green) to normal or unaffected tissue and B (blue) thatcorresponds to edema or necrosis, or in general, to thepresence of liquid in the lesion. Instead of using the ILTalgorithm for the determination of the relaxation rate orrelaxation rate distribution pixel by pixel, i.e., a procedure

328
Fig. 11 Average probability distribution function or relaxation spectrum for a lesion (continuous line) and for non affected tissue (dottedline). Relaxation spectra were determined for the same patient. On the left are shown the relaxometry grids used to calculate the relaxationspectrum
Fig. 12 Single voxel spectrum and segmented images for possible craniopharyngioma
which is time consuming and sensitive to small signal tonoise ratios, each pixel was analyzed assuming that it wascomposed at least of one of the tissue categories givenin Table 3. This is equivalent to assuming that the imageintensity in each pixel (in a set of multiecho images) is a lin-ear superposition of three different decaying exponentialfunctions, each one of them characterized by a relaxationrate and corresponding to a tissue category
I (t)=bl +ARXR(t)+AGXG(t)+ABXB(t), (6)
where
Xi(t)= exp(−λit) (7)
with i = R,G or B, λi is the relaxation rate determinedby assignment of pathology from the average relaxationspectrum, bl is a parameter introduced to take into ac-count corrections in the baseline of the image intensity(also applied to the ILT algorithm) and the coefficientsAi , which are positive, determine the proportion of eachrelaxation decay in the image. Particular attention waspaid to the correlation coefficient in the linear regressionanalysis, and in the present work, the coefficients Ai wereonly accepted for those fittings with a squared correlationcoefficient higher than 0.99. This step is necessary becausethe exponential functions are correlated. For example, two

329
exponential functions with relatively different decay expo-nents could have a squared correlation coefficient close to1. Figure 6 shows how the image segmentation changesdepending on the value of the squared correlation coeffi-cient.
Once the Ais are determined the image can be seg-mented separately to show edema or necrosis, tumoral,and normal or unaffected tissue. In particular, for ther-apy purposes, it is important to isolate tumoral tissue anddetermine contour plots that describe the distribution oftumoral activity in the lesion. This information is depictedin Fig. 7. To further assess the segmentation procedure itis necessary to eliminate false “tumor positive” pixels dueto the fact that the exponential functions are correlated. A“tumor density probability”, p, is defined in the followingway: for only those pixels with an AR coefficient differentfrom zero, an average is taken over its neighboring pixelsincluding the pixel itself, assigning the value of 1 if thepixel has an AR �= 0 and a value of 0 if AR = 0. The aver-age obtained in this way represents the value of p and itsmaximum value is 1, a situation that occurs if and onlyif, the central pixel and all the pixels around it have anAR �=0. The pixel is accepted as a true “tumor positive” ifand only if p, is greater than 1/3. With this filtering processa more compact segmentation of the tumor is obtained asit eliminates isolated low density pixels and pixel clusters.The segmentation procedure outlined before depends onthe particular set of relaxation rates. The combination ofthe ILT algorithm and the spectroscopic data provides notonly the mean relaxation rates but also their dispersions.In order to fully assess the segmentation of the image sev-eral set of relaxation rates were used, constructed in thefollowing way: for each relaxation rate value, i.e., the meanvalue in the relaxation rate spectrum for a particular tis-sue type, a set of three values are generated, one is themean value itself and the other two are obtained by addingor subtracting its standard deviation; all 27 combinationswere considered in an optimization procedure to maximizethe parameter p. Typical values of p covered a range of0.67–0.96. Control values of p ranged from 0.44 to 0.69.For the calculation of the control parameters not onlyimages obtained from control volunteers were used, butalso those planes in patients that were clearly unaffectedby the lesion. This is shown in Table 4. Other quantities canbe defined to evaluate the tumor, such as the “volume”,v, defined as the number of positive voxels in a particularimage, and the “mean tumor image intensity”, ρ, which isthe local average image intensity for positive pixels. Theseadditional parameters are also shown in Table 4.
Instead of using color code, a gray palette can be usedto map the RGB code on a gray scale as follows: AR in206–255 (light gray), AG in 51–205 (gray), and AB in 0–50 (dark gray). This procedure is useful when no colordisplay is available, and in general is more familiar to theradiologist, who is trained in analyzing images based on
a gray scale and the particular mapping selected closelyresembles gadolinium contrasted images. Additionally, itpreserves anatomical details of the image, which are of rel-evance for image registration or fusion procedures, com-monly used in therapy planning. The comparison betweencolor RGB code segmentation and gray scale mapping canbe seen in Figs. 8 and 9. Analysis of Figs. 8 and 9 dem-onstrate that in most cases a segmentation of the lesioncan be done. In particular, in Fig. 8a, b and 9a throughc, correspond to glioblastoma multiformes and fibrillaryastrocytomas, respectively. It is possible to separate theactive region of the tumor from its necrotic center and alsoto quantify the proportion of necrosis to active tumor, arelation that could be very useful in the evaluation of atumor under therapy. In the case of more benign tumors,such as oligodendrogliomas, Fig. 9d and meningiomas,Fig. 8c, d, it is also possible to define a good segmentationof the lesion and to establish a follow up under therapy.In Fig. 10, the segmented images corresponding to con-trol cases are shown. For control cases C1 and C2, theimages were segmented using the relaxation rates com-ing from the ILT procedure applied to their own set ofslices and also using the average relaxation rates obtainedfrom the patients, i.e., these relaxation rates include thosecorresponding to malignant tissue. For control cases C3through C7, the relaxation rates used in the segmentationwere those obtained by the ILT procedure on the slices thatexhibited the pathology. This assumption is justified sincethe relaxation spectrum within the lesion differs notice-ably from the relaxation spectrum obtained from regionsof unaffected issue, as depicted in Fig. 11. In either case,the segmentation obtained for control cases did not revealany significant manifestation of pathology as can be seenin Fig. 10.
Finally, in the case of patient no.8, a possible cra-niopharyngioma, the resulting segmentation is shown inFig. 12, together with the SVS spectrum. The segmentedimage is consistent with the 1HMRS evaluation in thesense that the lesion is not malignant. Nevertheless, sinceno CSI could be performed on this patient, the segmenta-tion was performed by analyzing the relaxation data andassuming that the relaxation associated with malignantactivity was located in the same range as in the other casesstudied. This procedure could account for some of the redcoloring that is observed on the left of the image.
Conclusions
This study combines two non invasive methods 1HMRSand Relaxation studies, in order to utilize them ascomplementary methodologies in the assessment of braintumors. The methodology devloped in this work mixessuccessfully data coming from 1HMRS and relaxometry

330
to produce appropriate segmentation of tumor imageswith enough spatial resolution to be used for tumor evalu-ation and therapy planning. The methodology uses a newalgorithm (ILT) to perform the analysis of the relaxationdata without making initial assumptions about the char-acteristics of the tissue. This makes it a powerful tool forthe determination of the actual relaxation rate distribu-tions, which is the key factor necessary for the correct seg-mentation and assessment of the tumor image. This factopens the possibility to use the relaxation spectra on thesame foot as 1HMRS spectra to determine nosologic im-ages [23–25] with higher spatial resolution, improving thedetermination of the gross tumor volume (GTV), neces-sary for treatment planning. Segmentation methodologiesand strategies taken from the analysis of nosologic imagesderived from 1HMRS spectra alone could also be appliedor extended to these new combined images. Also, if a cor-relation between relaxation rate and spectroscopic datacan be established, a task that will be undertaken in the
future, the methodology developed in this work could beused as a tool to improve the spatial resolution of CSImaps by acting in a retrograde manner: the spectroscopicinformation obtained in a not well defined CSI voxel, (avoxel with atypical metabolite ratios), will be decomposedaccording to the proportion of its relaxation components,each one associated to each tissue. This will lead to a met-abolic map with a higher spatial resolution than the oneobtained with the standard CSI sequence. The methodol-ogy may also be associated with other imaging techniques,like diffusion or perfusion to further assess the localiza-tion of the tumor. Its application can be extended to otherorgans like breast or prostate.
Acknowledgements The authors would like to thank the MRI radiol-ogists and technologists from the Instituto de Resonancia MagneticaLa Florida-San Roman, Caracas, Venezuela who helped in this pro-ject. This work was financially supported by Centro de DiagnosticoBiomagnetic, C.A.
References
1. Danielsen ER, Ross B (1999) Magneticresonance spectroscopy of neurologicaldiseases. Marcel Decker, New York
2. Castillo M, Kwock L (1998) ProtonMR spectroscopy of common braintumors. Neuroimag Clin North Am4:733–752
3. Howe FA, Barton SJ, Cudlip SA,Stubbs M, Saunders DE, Murphy M,Wilking P. Opstad KS et al (2003)Metabolic profiles of human braintumors using quantitative in vivo 1Hmagnetic resonance spectroscopy.Magn Reson Med 49:223–232
4. Nelson SJ (2003) Multivoxel magneticresonance spectroscopy of braintumors. Mol Cancer Ther 2:497–507
5. Barton SJ, Howe FA, Tomlins AM,Cudlip SA, Nicholson JK, Bell BA,Griffiths JR (1999) Comparison of invivo 1H MRS of human brain tumourswith 1H HR-MAS spectroscopy ofintact biopsy samples in vitro. Magma8:121–128
6. Norfray JF, Tomita T, Byrd SE, RossBD, Berger PA, Miller RS(1999)Clinical impact of MR spectroscopywhen MR imaging is indeterminate forpediatric brain tumors. AJR Am JRoentgenol. 173:119–125
7. Vigneron DB, Dowling C, Day M et al(1997) Determination of metabolitelevels in necrosis/astrogliosis and viablecancer in brain tumor masses using 3DH MR spectroscopy imaging. In:Proceedings 5th ISMRM, New York, p1146
8. Nelson S, Vigneron D, Dillon W (1999)Serial evaluation of patients with brain
tumors using volume MRI and 3D 1HMRSI. NMR Biomed 12:123–138
9. Negendank WG, Sauter R, Brown TRet al (1996) Proton MagneticResonance Spectroscopy in patientswith glial tumor: a multicenter study.J Neurosurg 84:440–458
10. Sijens PE, Kopp MV, Brunetti A et al(1995) 1H MR spectroscopy in patientswith metastatic brain tumors: amulticenter study. Magn Reson Med33:818–826
11. Shimizu H, Kumabe T, Tominaga T,Kayama T, Hara K, Ono Y, Sato K,Arai N, Fujiwara S, Yoshimoto T(1996) Non-invasive evaluation ofmalignancy of brain tumors withproton MR spectroscopy. Am JNeuroradiol 17:737–747
12. Adamson AJ, Rand SD, Prost RW,Kim TA, Schultz C, Haughton VM(1998) Focal brain lesions: effect ofsingle-voxel proton MR spectroscopicfindings on treatment decisions,Radiology 209:73–78
13. Chee Z-H, Jones JP, Singh M(1993)Foundations of medical imaging.Wiley, New York
14. Watanabe T, Murase N, Staemmler M,Gersonde K (1992) Multiexponentialproton relaxation processes ofcompartmentalized water in gels. MagnReson Med 27:118–134
15. Kuhn W, Barth P, Denner P, Muller R,Characterization of elastomericmaterials by NMR microscopy. Sol StNMR 6:295–308
16. Luciani AM, Capua SD, Guidoni L,Ragona R, Rosi A, Viti V (1996)
Multiexponential T2 relaxation inFricke agarose gels: implications forNMR dosimetry. Phys Med Biol41:509–521
17. Cheng KH (1994) In vivo tissuecharacterization of human brain bychi-squared parameter maps:multiparameter proton T2 relaxationanalysis. Magn Reson Med12:1099–1109
18. Does MD, Sayder J, MultiexponentialT2 relaxation in degeneratingperipheral nerve. Magn Reson Med35:207–213
19. Thomsen C (1996) Quantitativemagnetic resonance methods for invivo investigation of the human liverand spleen. Technical aspects andpreliminary clinical results. ActaRadiol Suppl 401:1–34
20. Fellner F, Fellner C, Held P, Schmitt R(1997) Comparison of spin-echo MRpulse sequences for imaging of thebrain. Am J Neuroradiol 18:1617–1625
21. Knopp EA, Cha S, Johnson G,Mazumdar A, Golfinos JG, Zagzag D,Miller DC, Kelly PJ, Kricheff II (1999)Glial neoplasms: dynamiccontrast-enhanced T2*-weighted MRimaging. Radiology 211:791–798
22. Cha S, Knopp EA, Johnson G, Litt A.Glass J, Gruber ML, Lu S, Zagzag D(2000) Dynamic contrast-enhancedT2*-weighted MR imaging of recurrentmalignant gliomas treated withthalidomine and carboplatin. AmJ Neuroradiol 21:881–890

331
23. Szabo de Edelenyi F. Rubin C, EsteveF, Grand S, Decorps M, Lefournier V,Le Bas J-F, Remy C (2000) A newapproach for analyzing protonmagnetic resonance spectroscopicimages of brain tumors:nosologicimages. Nat Med 6:1287–1289
24. Simonetti AW, Meissen WJ, van derGraff M, Postma GJ, Heerschap A,Buydens LMC (2003) A chemometricapproach for brain tumor classificationusing magnetic resonance imaging andspectroscopy. Anal Chem 75:5352–5361
25. Simonetti AW, Meissen WJ, Szabo deEdelenyi F, van Asten JJA, HeerschapA, Buydens LMC (2005) Combinationof feature-reduced MR spectroscopicand MR imaging data for improvedbrain tumor classification. NMRBiomed 18:34–43
26. Pokric M, Thacker N, Scott MLJ,Jackson A (2001) The importance ofpartial voluming in multi-dimensionalmedical image segmentation.In: WNiessen, M Viergever (eds) MICCAI2001, LNCS 2208. Springer-Verlag,Berlin Heidelberg, Newyork
27. Shattuck DW, Sandor-Leahy SR,Schaper KA, Rottenberg DA, LeahyRM (2001) Magnetic resonance imagetissue classification using a partialvolume model. NeuroImage13:856–876
28. Van Leemput K, Maes F,Vandermeulen D, Suetens P (2003) Aunifying framework for partial volumesegmentation of brain MR images.IEEE Trans Med Imaging 22:105–119
29. Provencher SW (1982) A constrainedregularization method for invertingdata represented by linear algebraic orintegral equations. Comput PhysCommun 27:213–227 and Contin: Ageneral purpose constrainedregularization program for inverting
noise linear and integral equations.Comput Phys Commun 27:229–242
30. Butler JP, Reeds JA, Dawson SV (1981)Estimating solutions of the first kindintegral equations with nonnegativityconstraints and optimal smoothing.SIAM J Numer Anal 18:381–397
31. Martın-Landrove M, Martın R,Benavides A (1995) Transversalrelaxation rate distribution analysis inporous media, Proceedings of theinternational society of magneticresonance XIIth meeting part I. BullMagn Reson 17:73–78
32. Bonalde I, Martın-Landrove M,Benavides A, Martın R, Espidel J(1995) Nuclear magnetic resonancerelaxation study of wettability ofporous rocks at different magneticfields. J Appl Phys 78:6033–6038
33. Martın R, Martın-Landrove M (1998)A novel algorithm for tumorcharacterization by analysis oftransversal relaxation rate distributionsin MRI.In: Spatially resolved magneticresonance. Wiley-VCH, New York,Chap 11, pp 133–138
34. Bhanot G (1988) The metropolisalgorithm. Rep Prog Phys 51:429–457
35. Kirkpatrick S, Gellatt CD, Vecchi MP(1983) Optimization by simulatedannealing. Science 220:671–680
36. Kirkpatrick S (1984) Optimization bysimulated annealing: quantitativestudies. J Stat Phys 34:975–986
37. Bonomi E, Lutton JL (1984) TheN-city traveling salesman problem andthe Metropolis algorithm. SIAM Rev26:551–568
38. Scales JA, Gersztenkorn A (1988)Robust methods in inverse theory.Inverse Probl 4:1071–1091
39. Szu H, Hartley R (1987) Fast simulatedannealing. Phys Lett A 122:157–162
40. Rutgers DR, van der Grond J (2002)Relaxation times of choline, creatine,and N-acetyl aspartate in humancerebral white matter at 1.5 T. NMRBiomed 15:215–221
41. Rutgers DR, Kingsley PB, van derGrond J (2003) Saturation-corrected T1and T2 relaxation times of choline,creatine, and N-acetyl aspartate inhuman cerebral white matter at 1.5 T.NMR Biomed 16:286–288
42. Castillo M, Smith JK, Kwock L (2002)Correlation of Myo-inositol levels andgrading of cerebral astrocytomas. AmJ Neuroradiol 21:1621–1645
43. Opstad KS, Provencher SW, Bell BA,Griffiths JR, Howe FA (2003)Detection of elevated glutathione inmeningiomas by quantitative in vivo1H MRS. Magn Reson Med49:632–637
44. Law M, Cha S, Knop EA, JohnsonJ, Litt A (2002) High-grade gliomasand solitary metastases: differentiationby using perfusion and protonspectroscopy MR imaging. Radiology3:715–721
45. Tate AR, Griffiths JR, Martınez-PerezI, Moreno A, Barba I, Cabanas ME,Watson D, Alonso J, Bartumeus F,Isamet F, Ferrer I, Vila F, Ferrer E,Capdevila A, Arus C (1998) Towards amethod for automated classification of1H MRS spectra from brain tumors.NMR Biomed 11:117–191
46. Vuori K, Kankaanranta L, HakkinenAM, Gaily E, Valanne L, GranstronML et al (2004) Low-grade gliomasand focal cortical developmentalmalformations: differentiation withproton MR spectroscopy. Radiology230(3):703–708