-
ANOMALOUS DEVELOPMENT OF BRAIN STRUCTUREAND FUNCTION IN SPINA
BIFIDA
MYELOMENINGOCELE
Jenifer Juranek1* and Michael S. Salman21Department of
Pediatrics, Childrens Learning Institute, University of Texas
Health Science Center at Houston, Houston, Texas2Section of
Pediatric Neurology, Faculty of Medicine, Childrens Hospital,
University of Manitoba, Winnipeg, Manitoba, Canada
Spina bifida myelomeningocele (SBM) is a specific type of
neuraltube defect whereby the open neural tube at the level of the
spinal cordalters brain development during early stages of
gestation. Some struc-tural anomalies are virtually unique to
individuals with SBM, including acomplex pattern of cerebellar
dysplasia known as the Chiari II malforma-tion. Other structural
anomalies are not necessarily unique to SBM,including altered
development of the corpus callosum and posteriorfossa. Within SBM,
tremendous heterogeneity is reflected in the degreeto which brain
structures are atypical in qualitative appearance andquantitative
measures of morphometry. Hallmark structural features ofSBM include
overall reductions in posterior fossa and cerebellum size
andvolume. Studies of the corpus callosum have shown complex
patterns ofagenesis or hypoplasia along its rostral-caudal axis,
with rostrum andsplenium regions particularly susceptible to
agenesis. Studies of corticalregions have demonstrated complex
patterns of thickening, thinning,and gyrification. Diffusion tensor
imaging studies have reported compro-mised integrity of some
specific white matter pathways. Given equallycomplex ocular motor,
motor, and cognitive phenotypes consisting of rela-tive strengths
and weaknesses that seem to align with altered
structuraldevelopment, studies of SBM provide new insights to our
current under-standing of brain structurefunction associations. '
2010 Wiley-Liss, Inc.Dev Disabil Res Rev 2010;16:2330.
Key Words: Chiari II malformation; cerebellum; neuroimaging;
structure;function; cortex; corpus callosum
Spina bifida myelomeningocele (SBM) is a special type ofneural
tube defect whereby a failure in programmed fetaldevelopment (e.g.,
neural tube closure) at the level ofthe spine translates into
substantially altered brain develop-ment, in both structural and
functional domains. Both qualita-tive and quantitative studies have
documented a remarkabledegree of heterogeneity among individuals
with SBM in termsof size, shape, and appearance of the cerebellum,
corpus cal-losum, and cerebral cortex. Similarly, a wide range of
cogni-tive strengths and relative weaknesses among individuals
withSBM are also documented in the published literature. As
high-lighted below in the present paper, qualitative and
quantitativeinvestigations of brain regions hypothesized to be
associatedwith cognitive strengths and weaknesses in individuals
withSBM provide new insights into current models of brain-behavior
associations in general. Although hydrocephalus
commonly occurs in individuals with SBM, it will not be
dis-cussed in detail here, and readers are referred to [Del
Bigio,2010].
OVERVIEW OF STRUCTURAL FEATURESASSOCIATEDWITH SBM
Common structural characteristics associated with SBMinclude
anomalous development of the skull, as well as infra-and
supra-tentorial regions of the brain [McLone and Dias,2003]. Chiari
II malformation (CII) is a complex congenitalanomaly that involves
the midbrain, hindbrain (i.e., pons, me-dulla, and cerebellum) and
cervical spinal cord [Harding andCopp, 2002; Barkovich, 2005],
which occurs universally andexclusively in SBM [Wagner et al.,
2002]. Prominent featuresof CII include a significantly smaller
posterior fossa with itscontents crowded and distorted in
appearance [Barkovich,2005]. Additional features of SBM can include
tectal beaking,hydrocephalus, and corpus callosum hypoplasia and
dysgenesis,but these features are variable. Although less studied,
anenlarged massa intermedia and gyral malformations of theneocortex
also occur commonly in SBM with CII.
The main features of CII are based on qualitative
andquantitative descriptions of gross anomalies (Table 1),
particu-larly midline brain structures [McLone and Dias, 2003].
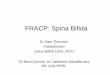
Themesencephalic tectum is often distorted and stretched
posteri-orly and inferiorly (see Fig. 1), which is frequently
describedon magnetic resonance imaging (MRI) scans as beaking ofthe
tectum. Tectal beaking is reported to occur in 75% of CIIcases,
being particularly prominent in older patients with anextensive
myelomeningocele [Fletcher et al., 2005]. Typicallyin CII, the
brainstem is stretched down to the level of the fo-ramen magnum or
cervical spine with narrowing in its anteri-
Grant sponsor: Eunice Kennedy Shriver National Institute of
Child Health andHuman Development (NICHD) or the National
Institutes of Health; Grantnumbers: P01-HD35946, R01
HD046609.*Correspondence to: Jenifer Juranek, Department of
Pediatrics, University of TexasHealth Science Center at Houston,
Childrens Learning Institute, 7000 Fannin Ste.2411, Houston, TX
77030. E-mail: [email protected] 10 January 2010;
Accepted 1 March 2010Published online in Wiley InterScience
(www.interscience.wiley.com).DOI: 10.1002/ddrr.88
DEVELOPMENTAL DISABILITIESRESEARCH REVIEWS 16: 23 30 (2010)
' 2010Wiley -Liss, Inc.
-
orposterior diameter. A cervico-med-ullary kink may be seen at
the junctionbetween the cervical spinal cord and themedulla
oblongata [Barkovich, 2005],which may lead to symptoms of
spinalcord compression [Oaks and Gaskill,1992]. Although the
inferior vermis fre-quently herniates down to the upper cer-vical
vertebrae (C), at C2 or C4 level,the superior part of the
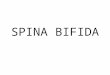
cerebellar vermisherniates upward (Fig. 1). As describedby
Barkovich [2005] and shown in Fig-ure 2, the cerebellum wraps
around thebrainstem. In some cases, low insertionof the tentorium
cerebelli, cerebellardysplasia, agenesis, or hypoplasia of
thelateral cerebellar hemispheres also occurs[Gilbert et al., 1986;
Harding and Copp,2002; Barkovich, 2005].
Morphology of the corpus cal-losum (CC) is also compromised
duringearly embryogenesis in SBM [Barko-vich, 2005] as the CC
programmed pat-tern of development usually occurs inutero between 7
and 20 weeks of gesta-tion [Barkovich and Norman, 1988].Complex
patterns of CC dysmorphol-ogy occur along its rostro-caudal axis
inSBM [Hannay et al., 2009]. Althoughpartial agenesis or dysgenesis
and hypo-plasia (e.g., underdevelopment) are de-scriptive terms
frequently used to com-municate type of dysmorphology, thegenu,
body, splenium, and rostrum aresubdivisions of the CC used to
commu-nicate where the dysmorphology hasoccurred [Fletcher et al.,
2005; Milleret al., 2008]. An association has beenreported between
spatial location of CC
agenesis and level of the vertebral col-umn where the
myelomeningoceleoccurs (e.g., thoracic versus lumbar/sac-ral), with
thoracic lesions being twice aslikely to have agenesis of the
spleniumas lumbar/sacral level lesions [Hannayet al., 2009]. Thin
regions of the CCare generally thought to develop sec-ondary to
increased intracranial pressureand hydrocephalus, which develop
in8090% of children born with SBM[Reigel and Rotenstein, 1994].
Theories and Mechanisms of ChiariType II Malformation
Over the years, several theorieshave been proposed to explain
CII.Although no single theory fullyaccounts for all features of CII
[Steven-son, 2004; Tubbs et al., 2008], the cur-rently most widely
accepted theory isthe unified theory [McLone andKnepper, 1989].
According to thistheory, cerebrospinal fluid (CSF) leaksthrough the
spinal defect into the intra-uterine environment. Failure of
neuraltube closure hinders normal distensionof the embryonic
ventricular systemthrough the pressure generated fromCSF buildup
during the temporary pe-riod of spinal neurocele occlusion
[Des-mond, 1982]. Lack of ventricular dis-tension in utero limits
the normalgrowth of the bony elements of theposterior fossa, which
significantlyreduces posterior fossa size [McLoneand Knepper, 1989;
McLone and Dias,2003]. The contents of the posteriorfossa, which
proliferate rapidly later[Griffiths et al., 2004], are
constrainedby a smaller than normal posterior fossa,thereby lending
the cerebellum tocompression and subsequent volumetricreduction as
well as displacement and
herniation along its vertical and anteri-orposterior axes.
In light of the unified theory, severaltestable hypotheses to
prevent CII fromdeveloping have emerged. The basic ra-tionale is
that preventing CII will also pre-vent downstream consequences of
CII[Walsh et al., 2001]. Specifically, one mightpredict that fetal
surgical techniquesdesigned to repair the spinal defect in
uterowould stop CSF leakage through the me-ningomyelocele, thereby
preserving nor-mal distension of the ventricular system,and thus
facilitating normal bone growth[see Bowman and McLone, 2010].
Re-ports of reduced or prenatal resolution ofhindbrain herniation
following surgicalrepair of spinal meningomyelocele in bothanimal
model systems [Meuli et al., 1995]and human patients [Adzick et
al., 1998;Bruner et al., 1999; Sutton et al., 1999;Tulipan et al.,
1999] are consistent withthe unified theory. Additionally,
infantswith SBM who had fetal surgery to closetheir spinal defect
have decreased symp-toms and signs of brainstem compression[Danzer
et al., 2008]. Currently, an NIH-funded multicenter study is
conducting aprospective randomized clinical trial (e.g.,Management
of MyelomeningoceleStudy) to compare efficacy of prenatal
fetalsurgery with standard postnatal repair onimproving
neurological outcome andreducing anomalous brain development inSBM
[Mitchell et al., 2004; Sutton andAdzick, 2004; Bowman et al.,
2009; Bow-man and McLone, 2010].
Additional theories proposed toexplain CII that have not been
widelysupported include: hindbrain dysgenesistheory, which
postulated that the hind-
Table 1. Structural ChangesWithin the Posterior Fossain Chiari
II Malformation
Small posterior fossaSmall cerebellar volume (especiallythe
cerebellar hemispheres)
Reduced cerebellar weightDysplastic looking cerebellumExpanded
midsagittal vermis areaVermis (6tonsils) herniation belowforamen
magnum
Upward herniation of the superior vermisWrapping of the
cerebellar hemispheresaround the brainstem
Enlarged tentorium incisuraDysplastic tentorium cerebelli
withabnormally low insertion
Inferior displacement of thelower brainstem
Tectal beakingMedullary-cervical kinkAqueduct stenosisSmall and
inferiorly displaced fourthventricle
Enlarged foramen magnum
Fig. 1. T1-weighted midsagittal MRI in achild with Chiari type
II malformationillustrating herniation of the inferior cere-bellar
vermis (horizontal arrow) and tectalbeaking (vertical arrow). The
fourth ven-tricle is small in size. Fig. 2. T1-weighted axial MRI
at the
level of the pons in a child with ChiariType II malformation
illustrating wrappingof the cerebellar hemispheres around
thebrainstem (arrow).
24 Dev Disabil Res Rev Development of BRAIN Structure and
Function JUranek And SALMAN
-
brain was underdeveloped in SBM; thetraction theory in which
downwardtraction of the lower spinal cord wasthought to pull down
the hindbraininto the spinal canal; the overgrowththeory, which
suggested there is over-growth of the neural tissue prior to
clo-sure of the neural tube; and the hydro-dynamic theory in which
there isdownward herniation of the hindbraincaused by the raised
intracranial pressurefrom the hydrocephalus [Gardner et al.,1975;
Gilbert et al., 1986; McLone andKnepper, 1989; Harding and
Copp,2002].
Recent investigations have triedto bridge both ends of the
myelome-ningocele problem: the open neuraltube defect in the spinal
cord andreduced posterior fossa size in the cra-nium. As suggested
by Williams [2008],both genetic and environmental factorsare likely
to have key roles in the etiol-ogy of posterior fossa hypoplasia in
CII,which together with low-spinal pres-sure, contribute to the
development ofCII [Williams, 2008]. In Sarnats molec-ular genetic
explanation for CII abnor-malities, he suggested that
abnormalrhombomere formation and ectopicexpression of homeobox
genes of therostrocaudal axis of the neural tube mayexplain CII
features [Sarnat, 2000].Clearly, additional research is needed
toclarify the mechanism(s) mediating therobust association between
the forma-tion of the myelomeningocele in thespine and the CII in
the cranium.
As enthusiasm for genotypephe-notype studies focused on the
cerebel-lum continues to spread, our knowledgeof molecular cascades
underlying neuraltube closure and posterior fossa devel-opment will
expand accordingly [seeAu et al., 2010]. Recent reports suggesta
transcription factor expressed in thehead mesenchyme, FOXC1, is
requiredfor normal skull development [Riceet al., 2003] and normal
cerebellar de-velopment [Aldinger et al., 2009b]. Var-iations in
the amino acid sequence ofFOXC1 can result in a spectrum
ofphenotypes in cerebellar morphologyvia defective mesenchymal
signaling[Aldinger et al., 2009a]. FOXC1 is areasonable candidate
for further study asit is expressed near the time of neuraltube
closure and is localized to the mes-enchyme where skull
development,brainstem, and cerebellar developmentcould all be
influenced by variability inits expression levels [Aldinger et
al.,2009b]. However, definitive mecha-nisms underlying CII
development stillremain to be elucidated.
The Cerebellum: QuantitativeStudies
Studies of the cerebellum haveconsistently reported reduced
cerebellarsize in SBM, which is even evidentearly in fetal
development. In a 16-week-old fetus with SBM, the neuraltissue in
the posterior fossa was foundto be half the size of the neural
tissue inthe posterior fossa in a control fetus[Brocklehurst,
1969]. In young neo-nates, significant reduction in
cerebellarweight was found in 100 children withSBM, who died within
4 weeks ofbirth, in comparison with cerebellarweight of 60 children
with normal ver-mis who died from other causes [Var-iend and Emery,
1973]. Subsequentdegeneration of the cerebellum in CII,also
referred to as vanishing cerebel-lum, in CII has also been
reported(e.g., in Seners [1995] study of fourchildren, age 1 month
to 4.5 years,using magnetic resonance imaging(MRI) of the brain).
Microscopic stud-ies have described reduced cell numbersand DNA
content, particularly in theinternal granular layer of the
inferiorvermis, in 100 children with SBMcompared with 120 controls
[Emeryand Gadsdon, 1975]. More recently, mi-croscopic analyses of
herniated cerebel-lar tissue have documented granule andPurkinje
cell loss, reduction and gliosisof the folia, and myelin depletion
[Har-ding and Copp, 2002].
Distance measurements, planime-try (e.g., area measurements),
and bio-metric (e.g., shape) analyses of the pos-terior fossa and
its contents have beenperformed in MRI studies of individu-als with
SBM to quantify abnormalities,document variability, and predict
func-tion or prognosis. In SBM, the longesttransverse and
longitudinal distancesacross the midsagittal vermis
indicatedexpansion, not reduction, relative toage-matched controls
[Salman et al.,2006a]. In the same study, mean areameasurements of
the midsagittal vermis(anterior, posterior, and inferior
subdi-visions) were significantly increased by25% in SBM compared
to normal con-trols despite a 9% reduction in posteriorfossa area
measurements in SBM[Salman et al., 2006a]. Using shapeanalyses,
Tsai et al. [2002] quantitativelydocumented the tremendous
variabilityacross individuals with SBM in thedegree to which the
hindbrain is mal-formed. According to their findings,shape changes
in bone and vermiandescent co-occur in a relational
fashion.However, herniation of the cervico-medullary junction
appears to be inde-
pendent of vermian herniation, therebysuggesting different
etiologies for her-niation of the vermis and herniation ofthe
cervico-medullary junction.
Early volumetric studies of thecerebellum in a group of
individualswith SBM used noninvasive MRImethods to quantitatively
assess groupdifferences between 52 children withSBM and 16
age-matched controls[Dennis et al., 2004]. Although thisstudy found
significantly reduced cere-bellar volumes in the SBM group, italso
described a significant effect oflesion level on cerebellar gray
matter(GM) and white matter (WM) volumes.Consistent with
neurological outcomes,where individuals with lower level spi-nal
lesions are less impaired than thosewith thoracic level lesions,
higher spinallesion levels exhibited greater reductionsin
cerebellar volumes of GM and WM(37%) than those with lower
levellesions (22%) [Dennis et al., 2004].Another study of children
with SBM[Fletcher et al., 2005] reported reducedcerebrum and
cerebellar volumes inchildren with upper (n 5 25) in com-parison
with lower (n 5 61) spinallesion levels. Together, these
studiesdemonstrate that upper level spinallesions in SBM are a
marker of moresevere brain dysmorphology and areassociated with
poorer cognitive andbehavioral outcomes [Dennis et al.,2004;
Fletcher et al., 2005].
A recent volumetric MRI studyused a simple approach for
parcellatingthe cerebellum into meaningful subu-nits: the corpus
medullare, the anteriorlobe, and the posteriorsuperior
andposteriorinferior subdivisions [Juraneket al., in press].
Despite the overallreduction in cerebellar volume in theSBM group,
absolute and relative vol-ume of the anterior lobe was
signifi-cantly increased relative to a typicallydeveloping
comparison group. Althoughthe absolute volume of the
corpusmedullare was significantly reduced inthe SBM group, the
relative volume ofthe corpus medullare was not signifi-cantly
different from the typically devel-oping group when corrected for
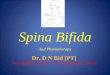
totalcerebellar volume. As shown in Figure3, the smaller cerebellum
observed inindividuals with SBM is not simply, lin-early reduced
equally across all regions,but rather disproportionately enlarged
inthe anterior lobe, reduced in the poste-riorinferior subdivision,
and not signif-icantly different in the corpus medullareor the
posteriorsuperior subdivision.
The functional significance ofregionally specific patterns of
volumet-
Dev Disabil Res Rev Development of BRAIN Structure and Function
JUranek And SALMAN 25
-
ric enlargement and reduction in cere-bellar subdivisions
remains to be estab-lished. Although the anterior lobe isgenerally
associated with motor func-tion, it is not yet clear whether a
largeranterior lobe confers advantages or dis-advantages in the
motor function do-main. Individuals with SBM demon-strate a wide
range of deficits in motorskills requiring strength or
speed[Hetherington and Dennis, 1999] ordynamic regulatory control
[Sandleret al., 1993; Jewell et al., 2009]. In con-trast, they
perform pretty well on motorskills requiring learning and
adaptation[Colvin et al., 2003; Edelstein et al.,2004; Dennis et
al., 2006a]. Thus,ongoing studies investigating these typesof brain
structurefunction associationsare ideally suited to provide
newknowledge and insight for continuedprogress in hypothesis-driven
research.
Consequences of Chiari Type IIMalformation on Hindbrain Motorand
Visceral Functions
Intrinsic brainstem abnormalitiesand pressure on the brainstem
from acrowded posterior fossa and hydroceph-alus give rise to a
diverse range ofsymptoms such as headaches, apnea,
bradycardia, dysphagia, torticollis, spas-ticity, and impaired
auditory evokedpotentials [Wagner et al., 2002; Henri-ques Filho
and Pratesi, 2006; Bowmanand McLone, 2010]. Brainstem com-pression
occurs in a third of patientswith CII and may be fatal in about
athird of these patients [Stevenson,2004]. Surgical decompression
of theposterior fossa for symptomatic CII isrequired in 817% of
subjects withSBM [Wagner et al., 2002] and usuallyleads to clinical
improvement. Maternalfetal surgery for SBM may also reducethe
incidence and severity of brainstemdysfunction [Danzer et al.,
2008].
Several eye movement abnormal-ities occur in CII including
impairedsmooth ocular pursuit, saccadic (i.e., fasteye movements)
dysmetria, impairedperformance of the vestibular-ocularreflex,
various forms of pathologicalnystagmus (abnormal ocular
oscilla-tions), strabismus, and internuclear oph-thalmoplegia (a
type of gaze palsy thatcauses double vision) [Leigh and Zee,2006].
Recording different classes ofeye movements in CII has shed
newlight on motor function of the hind-brain in CII in relation to
the anatomi-cal changes in this malformation. Mid-
sagittal vermis expansion, including thesignificant expansion of
vermis lobulesVI-VII area and preserved medial cere-bellar volume
corresponded to sparingof eye movements processed by the ver-mis,
despite the overall reduction incerebellar size that accompanies
the de-formity of CII [Salman et al., 2009].These eye movement
systems includesaccadic accuracy, saccadic adaptation (aform of
ocular motor learning), andsmooth ocular pursuit [Salman et
al.,2005, 2006b, 2007] In contrast, CIIpatients with abnormal
ocular motorfunctions did not have a significantlyexpanded
midsagittal vermis area. Fur-thermore, their midsagittal vermis
areaoccupied a smaller midsagittal posteriorfossa area, and their
cerebellar volumeswere smaller than in patients with CII,who had
normal eye movements[Salman et al., 2009].
Therefore, the overall reductionin posterior fossa and
cerebellar sizes inCII does not affect cerebellar structuresor
functions uniformly, because there isevidence for functional ocular
motorcircuits within the deformed hindbrainstructures in many
patients with CII. Inaddition, saccadic adaptation stilloccurred in
CII despite the small anddysplastic cerebellum and was evidenteven
in patients with eye movementabnormalities [Salman et al.,
2006b,2009]. Other types of motor learninghave also been reported
to be preservedin patients with CII including adapta-tion on
reaching or ballistic movements,mirror drawing performance,
andweight judgments [Colvin et al., 2003;Edelstein et al., 2004;
Dennis et al.,2006a].
The Corpus CallosumEven before sophisticated imaging
methods became available for quantita-tive analyses of WM in
SBM, aberrantdevelopment of the corpus callosum in7090% of SBM
cases [Barkovich,2005] made it a key focus of early qual-itative
imaging investigations. Dysgene-sis of the CC is not a unique
feature toSBM, as it also occurs in other neuro-genetic syndromes
[Ettlinger, 1977].Yet, along with hydrocephalus, CC dys-morphology
was one of the earliest visi-ble signs that incomplete neural
tubeclosure at the level of the spinal cordhad serious consequences
extendingbeyond the tentorium.
As reported in qualitative studiesof the CC, morphological
variabilityis remarkable across individuals withSBM [Reigel and
Rotenstein, 1994].Although some of this variability may
Fig. 3. The cerebellum has been parcellated into three primarily
gray matter compartmentsas shown in sagittal (left panels) and
coronal (right panels) views. Boundary demarcationsbetween
compartments are indicated by bright white lines (anterior lobe,
superior-posterior,and inferior-posterior subdivisions) in three
representative subjects (A, B). A: Typically develop-ing child with
cerebellar subdivisions numbered as: 1, anterior lobe; 2,
superiorposterior; and3, inferiorposterior. B: Child with SBM. The
central corpus medullare was also parceled sepa-rate from the other
three parcels for quantitative analyses. The smaller cerebellum
observed inindividuals with SBM is not simply linearly reduced
equally across all regions, but rather dispro-portionately enlarged
in the anterior lobe, reduced in the posteriorinferior subdivision,
andnot significantly different in the corpus medullare or the
posteriorsuperior subdivision.
26 Dev Disabil Res Rev Development of BRAIN Structure and
Function JUranek And SALMAN
-
be related to lesion level, lesion leveldoes not account for all
of the hetero-geneity [Fletcher et al., 2005]. Recently,26 regional
patterns of CC morphologyhave been carefully documented in asample
of 193 children with SBM basedon qualitative assessment of CC
appear-ance across four subdivisions: rostrum,genu, body, and
splenium [Hannayet al., 2009]. Whereas more than 50%of the study
sample exhibited partialdysgenesis in either the rostrum (21%)or
splenium (10%) or both regions(22%), only 4% of the study samplehad
normal-appearing CC morphologyacross all four subdivisions. The
remain-der of the study sample did not exhibitany dysgenesis, but
rather displayed var-ious regional patterns of hypoplastic
andnormal appearing subdivisions of theCC.
In early quantitative MRI investi-gations of the corpus callosum
in SBM,cross sectional area measurements wereobtained from a single
mid-sagittal slicein each participant [Fletcher et al.,1992, 1996;
Hommet et al., 2002;Kawamura et al., 2002]. On average,the area
measurement of the CC was
small in children with SBM comparedwith controls. In all these
studies, adiverse spectrum of CC morphologyacross SBM cases was
reported; a mi-nority of cases appearing to have nor-mal CC size
and morphology, and themajority of cases appearing abnormalwith
either hypoplastic features and/orpartial agenesis. Consistent with
a ros-tral-caudal developmental course of theCC [Barkovich and
Norman, 1988],the genu was reported to be relativelywell preserved
in individuals with SBM,with hypoplastic features occurring inthe
body, and agenesis most prominentin the isthmus/splenium
subregion[Kawamura et al., 2002].
Given the high incidence of pos-terior CC dysmorphology in
individualswith SBM, it is not too surprising thatsignificant
deficits commonly occur inperformance of cognitive tasks
requiringrecruitment of posterior networks,interhemispheric
transfer, and transfer oflanguage information [Huber-Okrainecet
al., 2005; Dennis et al., 2006b; Han-nay et al., 2008]. Thus,
processing ofsemantic information is performed rela-tively easily,
presumably due to a well-
preserved genu as suggested by resultsof split-brain surgical
patient studies[Sidtis et al., 1981]. However, idiomcomprehension
is negatively impactedby hypoplastic CC morphology[Huber-Okrainec
et al., 2005]. Eveninterhemispheric processing of simpleauditory
signals, as used in a dichoticlistening task, is influenced by
spleniumdysgenesis, but not CC hypoplasia[Hannay et al., 2008].
The CortexOriginally described nearly 20
years ago using pneumoencephalogra-phy and cerebral tomography
imaging,posterior thinning of the cortical mantlein SBM was an
important discovery thatseemed to explain behavioral deficits
inposterior network function [Denniset al., 1981]. Using en bloc
regionaldefinitions in their volumetric analysesof structural MRIs,
Fletcher et al.[2005] described significant reductionsin both GM
and WM volumes poste-rior to the genu of the corpus callosumin SBM.
More recently, high-resolutionsurface-based cortical
reconstructionanalysis methods developed by Fischland Dale [2000]
have been used. Thisstudy reported significantly reducedcortical
thickness in posterior regionsand significantly increased
corticalthickness in frontal regions based ongroup comparisons
between an SBMgroup and healthy controls matched onage and gender
[Juranek et al., 2008].These findings of altered spatial patternsof
cortical thickening and thinning sug-gest a potential structural
correlates ofcognitive strengths and weaknesses gen-erally
exhibited by individuals withSBM.
Additional morphometry measuresderived from surface-based
analyses of theneocortex in individuals with SBM haveincluded
cortical GM volume and corticalcomplexity (e.g., gyrification).
Using a3D local gyrification index (LGI) measureof cortical
complexity developed bySchaer et al. [2008], spatial patterns
ofcortical gyrification have been contrastedwith patterns of
cortical thicknessbetween a group of individuals with SBM(n 5 74)
and a comparison group of typi-cally developing study participants
(n 531). As shown in Figures 4 and 5, inferiorparietal and
posterior temporal areasexhibiting cortical thinning are also
char-acterized by increased cortical complexity.In frontal regions,
SBM exhibits increasedcortical thickness bilaterally in the
follow-ing regions: inferior frontal, middle fron-tal, medial
orbitofrontal, rostral anterior
Fig. 4. Significant group differences in cortical thickness
between individuals with SBM (n 574) and a comparison group of
typically developing (TD) study participants (n 5 31). Hotcolors
indicate cortical thickness is greater in the SBM group relative to
the TD group; coldcolors indicate cortical thickness is reduced in
the SBM group relative to the TD group. Colorscale bar indicates
significance values (corrected for multiple comparisons) ranging
from P