Embed Size (px)
Citation preview
Brain Injury CourseBrain Injury Course
Emergency Department Approach to Emergency Department Approach to ComaComa
Andy Jagoda, MD, FACEPAndy Jagoda, MD, FACEP
Professor of Emergency MedicineProfessor of Emergency Medicine
Mount Sinai School of MedicineMount Sinai School of Medicine

ObjectivesObjectives
• Review the neurologic evaluation of Review the neurologic evaluation of the patient in comathe patient in coma
• Review the differential diagnosis of Review the differential diagnosis of comacoma
• Discuss the indications for Discuss the indications for diagnostic testing in the patient with diagnostic testing in the patient with coma of undetermined etiologycoma of undetermined etiology
DefinitionsDefinitions
• Lethargy – decreased responsiveness but Lethargy – decreased responsiveness but arousablearousable
• Stupor – diminished awareness, arousable Stupor – diminished awareness, arousable only with vigorous stimulation and patient only with vigorous stimulation and patient does not interact in a meaningful waydoes not interact in a meaningful way
• Coma – diminished awareness, patient Coma – diminished awareness, patient can not be aroused even with vigorous can not be aroused even with vigorous stimulation. Response to noxious stimulation. Response to noxious stimulation tends to be stereotyped or stimulation tends to be stereotyped or reflexivereflexive
Case Study: Patient in ComaCase Study: Patient in Coma
• 56 year old male found by family on couch 56 year old male found by family on couch unresponsive; last seen “normal” one half unresponsive; last seen “normal” one half hour earlier; 60 minutes prior to ED arrival.hour earlier; 60 minutes prior to ED arrival.
• Brought by EMS; intubated in the field Brought by EMS; intubated in the field without drugswithout drugs
• Past history: hypertension, diabetesPast history: hypertension, diabetes• No history of traumaNo history of trauma• Meds: atenolol, HCTZ, insulin,Meds: atenolol, HCTZ, insulin,• ROS: negativeROS: negative
Case Study: Coma cont’dCase Study: Coma cont’d
• 150/90, 16, 80, 37 R, BS 160, intubated 150/90, 16, 80, 37 R, BS 160, intubated 100% pulse ox100% pulse ox
• Head – atraumaticHead – atraumatic• No gag; no spontaneous swallowing No gag; no spontaneous swallowing • Neck – suppleNeck – supple• Cardiopulmonary – normalCardiopulmonary – normal• Abdomen – softAbdomen – soft• Skin – no rashes, warm and drySkin – no rashes, warm and dry
Case Study: Coma cont’dCase Study: Coma cont’d
• No distress; non verbalNo distress; non verbal• Eyes closedEyes closed• No posturing; no asymmetry of faceNo posturing; no asymmetry of face• Pupils 2 mm Pupils 2 mm • Decreased muscle tone, no rigidityDecreased muscle tone, no rigidity• No response to painful stimuliNo response to painful stimuli• DTRs absentDTRs absent• Toes – no extensor planter reflexToes – no extensor planter reflex• Rectal absentRectal absent

Key questions in comaKey questions in coma
• What is the differential diagnosisWhat is the differential diagnosis What are the diagnoses you might What are the diagnoses you might
not think of . . . But don’t want to not think of . . . But don’t want to missmiss
• Does the GCS score predict outcome Does the GCS score predict outcome in this patientin this patient
• What are the physical findings that What are the physical findings that help localize the lesion, identify the help localize the lesion, identify the etiology, direct managementetiology, direct management
The Exam in ComaThe Exam in Coma
• Assess ABC’s, pupils, and skin:Assess ABC’s, pupils, and skin: Toxic syndromesToxic syndromes
• Assess for responsiveness: AVPUAssess for responsiveness: AVPU• Assess GCS scoreAssess GCS score
Eye opening, verbal, Eye opening, verbal, motormotor• PosturingPosturing• AsymmetryAsymmetry• AutomatismsAutomatisms

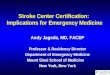
Decorticate posturing in comatose patient
Lesion above the red nucleus
Lower limbs extend, upper limbs flex following stimulus
Activity in the brainstem flexor center, the red nucleus
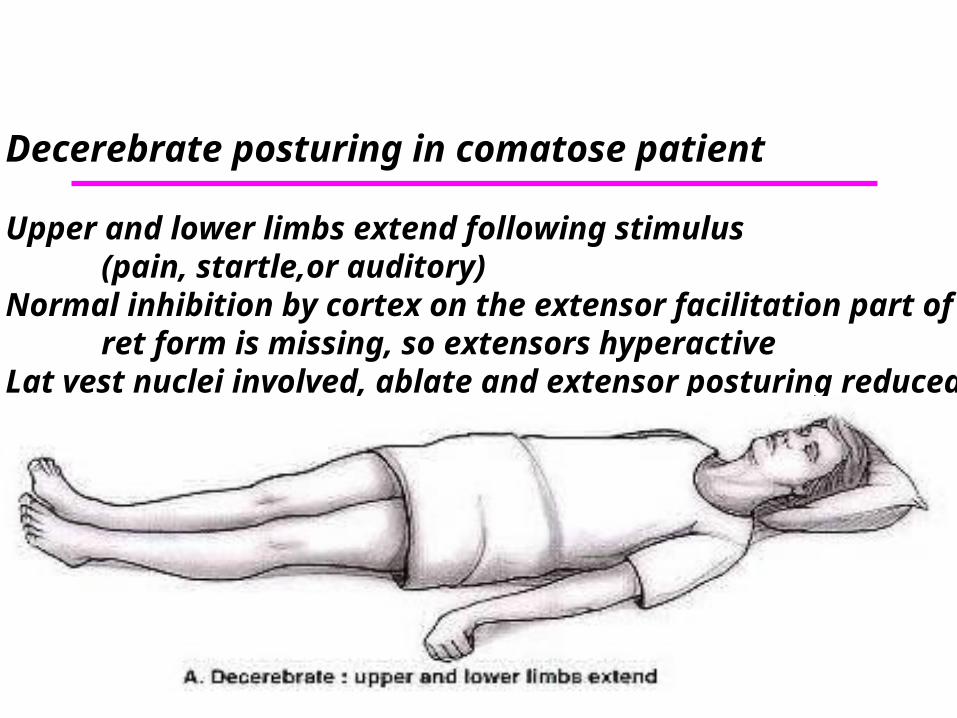
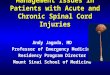
Decerebrate posturing in comatose patient
Upper and lower limbs extend following stimulus (pain, startle,or auditory)
Normal inhibition by cortex on the extensor facilitation part ofret form is missing, so extensors hyperactive
Lat vest nuclei involved, ablate and extensor posturing reduced
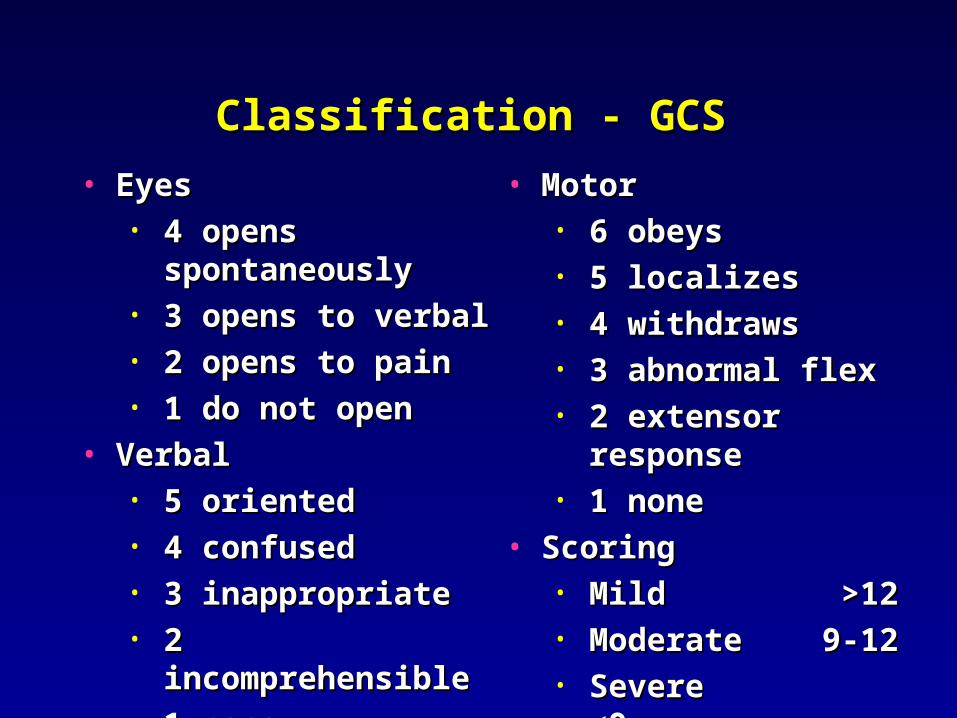
• EyesEyes• 4 opens 4 opens
spontaneouslyspontaneously• 3 opens to verbal3 opens to verbal• 2 opens to pain2 opens to pain• 1 do not open1 do not open
• VerbalVerbal• 5 oriented5 oriented• 4 confused4 confused• 3 inappropriate3 inappropriate• 2 incomprehensible2 incomprehensible• 1 none1 none
• MotorMotor• 6 obeys6 obeys• 5 localizes5 localizes• 4 withdraws4 withdraws• 3 abnormal flex3 abnormal flex• 2 extensor response2 extensor response• 1 none1 none
• ScoringScoring• MildMild >12 >12• ModerateModerate 9-12 9-12• Severe <9Severe <9
Classification - GCSClassification - GCS

• Developed for prognosis in severe TBIDeveloped for prognosis in severe TBI
• Timing of score is not standardizedTiming of score is not standardized
• One score not sufficient - perform One score not sufficient - perform
serial examsserial exams
Prognosis worse if score does not Prognosis worse if score does not
improve or it worsensimprove or it worsens
• Does not account for drugs, seizures, Does not account for drugs, seizures,
or metabolic problemsor metabolic problems
Classification - GCS - MortalityClassification - GCS - Mortality

The Eye Exam in ComaThe Eye Exam in Coma
• Pupils: size, reactivity, deviation, nystagmusPupils: size, reactivity, deviation, nystagmus Toward a cortical lesion; away from sz Toward a cortical lesion; away from sz
• Fundoscopic examFundoscopic exam Limited value in acute processesLimited value in acute processes
• Pupil asymmetry: < 1 mm normalPupil asymmetry: < 1 mm normal• Pupil asymmetry: > 1mm sens 40% spec 67% for Pupil asymmetry: > 1mm sens 40% spec 67% for
space occupying lesionsspace occupying lesions Anisocoria: ipsilateral in 21%,Anisocoria: ipsilateral in 21%, Of 51 patients with assym >3mm, 57% did not Of 51 patients with assym >3mm, 57% did not
have a mass lesionhave a mass lesion
Chestnut et al. Neurosurg 1994:34:840

The Eye Exam in ComaThe Eye Exam in Coma
• Pupils generally remain reactive in coma Pupils generally remain reactive in coma from metabolic or infectious etiologiesfrom metabolic or infectious etiologies Pin point pupil(s)Pin point pupil(s)
• opioid, alpha adrenergic, chol odopioid, alpha adrenergic, chol od• Carotid / vertebral artery dissectionCarotid / vertebral artery dissection• pontine infarctpontine infarct
locked in syndromelocked in syndrome Dilated pupil(s)Dilated pupil(s)
• anticholinergic, sympath odanticholinergic, sympath od• herniation herniation
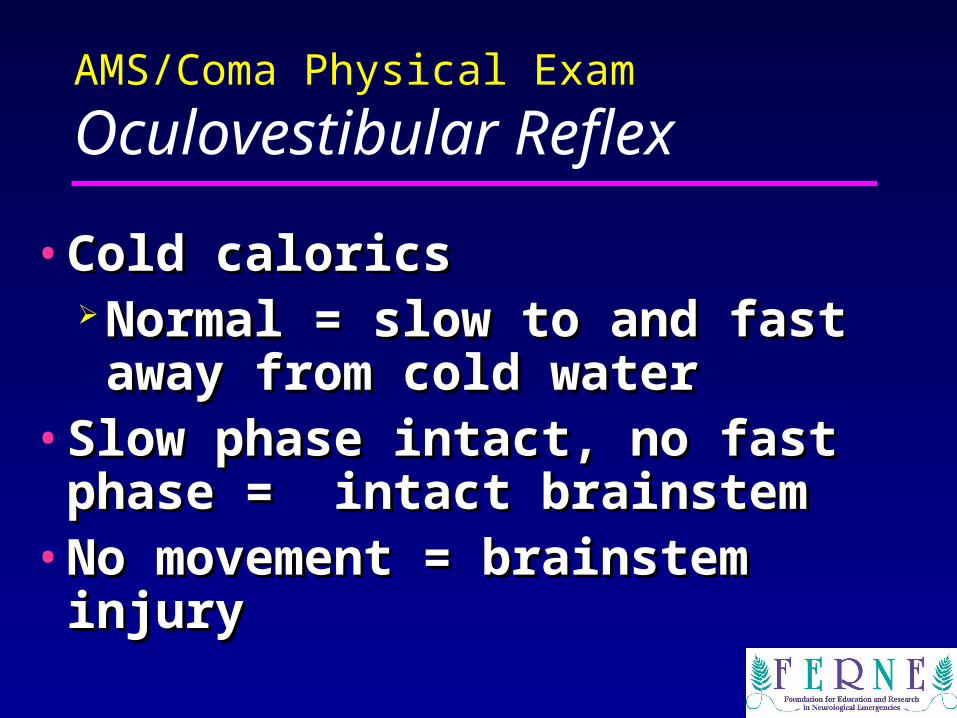
AMS/Coma Physical Exam
Oculovestibular Reflex
• Cold caloricsCold calorics Normal = slow to and fast away Normal = slow to and fast away
from cold waterfrom cold water• Slow phase intact, no fast phase = Slow phase intact, no fast phase =
intact brainstem intact brainstem• No movement = brainstem injuryNo movement = brainstem injury
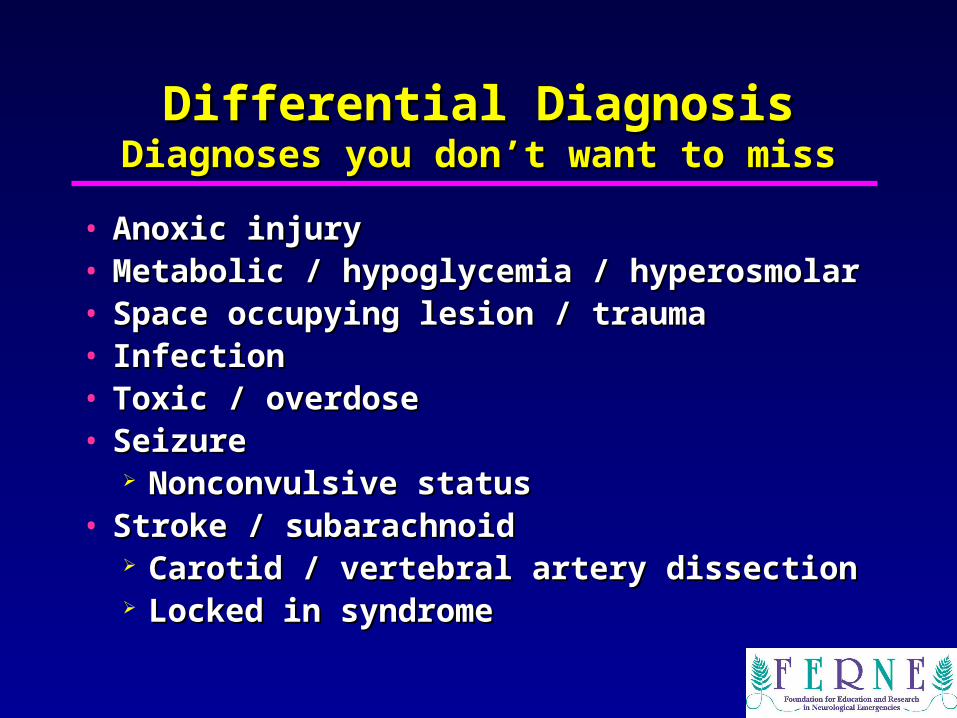
Differential DiagnosisDifferential DiagnosisDiagnoses you don’t want to missDiagnoses you don’t want to miss
• Anoxic injuryAnoxic injury• Metabolic / hypoglycemia / hyperosmolarMetabolic / hypoglycemia / hyperosmolar• Space occupying lesion / traumaSpace occupying lesion / trauma• InfectionInfection• Toxic / overdoseToxic / overdose• SeizureSeizure
Nonconvulsive statusNonconvulsive status• Stroke / subarachnoidStroke / subarachnoid
Carotid / vertebral artery dissectionCarotid / vertebral artery dissection Locked in syndromeLocked in syndrome

Diagnostic TestingDiagnostic Testing
• Metabolic profilesMetabolic profiles• NeuroimagingNeuroimaging
Non contrast head CTNon contrast head CT• Acute blood / mass lesionAcute blood / mass lesion
MRIMRI• Posterior fossa / Early infarctPosterior fossa / Early infarct
• LPLP Xanothochromia / InfectionXanothochromia / Infection
• EEGEEG

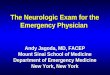
Case Study: CT ScanCase Study: CT Scan1
2
3
4
5
7
1. Frontal pole2. Lateral sulcus3. Third ventricle4. Mesencephalon5. Vermis of the
anterior lobe of the cerebellum
6. Anterior lobe of the cerebellum
7. Occipital lobe
6

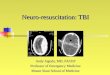
Baseline CT scanBaseline CT scan
1
2
34
1. Temporal lobe 3. Fourth ventricle
2. Pons 4. Post lobe cerebellum

The SubpoenaThe Subpoena
• All labs “normal”All labs “normal”
• CT done 4 hours after ED admissionCT done 4 hours after ED admission Read as “normal”Read as “normal”
• Admitted to MICUAdmitted to MICU
• Neurology consult finds:Neurology consult finds: Vertical gaze intact on commandVertical gaze intact on command Cold calorics: no movementCold calorics: no movement
Final Diagnosis:Final Diagnosis:Locked-In SyndromeLocked-In Syndrome
• Basilar artery occlusionBasilar artery occlusion• Bilateral lesions of the ventral ponsBilateral lesions of the ventral pons
Interrupts corticobulbar and Interrupts corticobulbar and corticospinal tractscorticospinal tracts
Awake, quadriplegia, bilateral facial and Awake, quadriplegia, bilateral facial and oropharyngeal palsy, preserved vertical oropharyngeal palsy, preserved vertical gazegaze
May present comatose if reticular May present comatose if reticular activating system is involvedactivating system is involved
The SubpoenaThe Subpoena
• ED physician accused of:ED physician accused of: Failure to do a proper examFailure to do a proper exam Failure to obtain a timely CTFailure to obtain a timely CT Failure to activate hospital’s stroke Failure to activate hospital’s stroke
teamteam Failure to administer t-PAFailure to administer t-PA Failure to provide appropriate care Failure to provide appropriate care
to prevent pain and sufferingto prevent pain and suffering

ConclusionsConclusions
• Approach to the patient in coma requires a Approach to the patient in coma requires a systematic exam that will then direct systematic exam that will then direct diagnostic testingdiagnostic testing
• The exam in coma should focus on pupils, The exam in coma should focus on pupils, GCS score with attention to motor GCS score with attention to motor posturing, asymmetry, and automatismsposturing, asymmetry, and automatisms
• Emergency physicians play a critical role Emergency physicians play a critical role in diagnosing and managing patients in in diagnosing and managing patients in coma; decision making in the ED has coma; decision making in the ED has significant impact on outcomes. significant impact on outcomes.