Embed Size (px)
Citation preview

Determination of death according to neurological criteria has far-reaching implications.Heart-beating, brain-dead donors provide the majority of organs for transplant.1 Extendedtimes between terminal brain stem herniation, declaration of brain death, and organ recovery
risk loss of organs because of refractory cardiopulmonary instability.2-5 A second implication is the costof intensive care, potentially exceeding $5000 daily.5-7 Recognizing terminal brain stem herniation andearlier declaration of brain death may help avoid costs associated with futile care. Last, patients whohave had terminal brain stem herniation and who are medically unsuitable for organ donation may nolonger benefit from intensive care.5 Delay in determining brain death may add to the stress a patient’sfamily experiences in keeping a vigil for a loved one without a chance of recovery.8 From brain injurythrough progression of intracranial pathophysiological changes, promoting recovery is the goal. Withrefractory injury and final brain stem herniation, a brain death protocol is appropriate.
The concept of brain death dates to 1959 with the introduction of “coma dépassé,” a state beyondcoma indicating loss of life functions such as reflexes, consciousness, and mobility. In 1968 the Harvard
Brain Death:Assessment, Controversy,and Confounding FactorsRICHARD B. ARBOUR, RN, MSN, CCRN, CNRN, CCNS
©2013 American Association of Critical-Care Nurses doi: http://dx.doi.org/10.4037/ccn2013215
Feature
When brain injury is refractory to aggressive management and is considered nonsurvivable, with loss of con-sciousness and brain stem reflexes, a brain death protocol may be initiated to determine death according toneurological criteria. Clinical evaluation typically entails 2 consecutive formal neurological examinations todocument total loss of consciousness and absence of brain stem reflexes and then apnea testing to evaluatecarbon dioxide unresponsiveness within the brain stem. Confounding factors such as use of therapeutic hypother-mia, high-dose metabolic suppression, and movements associated with complex spinal reflexes, fasciculations,or cardiogenic ventilator autotriggering may delay initiation or completion of brain death protocols. Neuro -diagnostic studies such as 4-vessel cerebral angiography can rapidly document absence of blood flow to thebrain and decrease intervals between onset of terminal brain stem herniation and formal declaration of deathby neurological criteria. Intracranial pathophysiology leading to brain death must be considered along with clin-ical assessment, patterns of vital signs, and relevant diagnostic studies. (Critical Care Nurse. 2013;33[6]:27-48)
www.ccnonline.org CriticalCareNurse Vol 33, No. 6, DECEMBER 2013 27
This article has been designated for CNE credit. A closed-book, multiple-choice examination follows this article,which tests your knowledge of the following objectives:
1. Describe the pathophysiology of brain injury2. Identify criteria for determining brain death3. Discuss nursing care of patients with brain injury
CNE Continuing Nursing Education

committee on brain death described “irreversible coma”(what is now described as brain death), incorporatingmost of the current clinical evaluation techniques. TheHarvard criteria have become the basis for much of cur-rent brain death protocols.9
Optimal care requires rapid recognition of progressionof a brain injury, such as worsening findings on neuro-logical examination and decreases in brain stem function.Missed opportunities for intervention may occur duringinjury progression, recognition, and management anddetermination of brain death. Nurses are integral inquickly recognizing progressive injury and terminal
brain stemherniation,providingaggressivecare, and
decreasing the number of silent brain deaths.10 Theseactions can improve donor recognition, optimize resourceutilization in the intensive care unit (ICU), increase avail-ability of potentially transplantable organs,11 and enableearly initiation of goal-directed therapy,12 improvingphysiological stability and organ function.
In this article, I review cerebral pathophysiology andterminal brain stem herniation, identify and illustratecriteria for determining brain death, and detail confound-ing factors in brain death.
Pathophysiology of Brain InjuryTerminal brain stem herniation is often the final stage
in refractory brain injury caused by trauma, ischemia orinfarction, hemorrhage, intracranial tumors, and infec-tious processes such as encephalitis and meningitis.Anoxic or ischemic injury after cardiopulmonary arrestcan initiate neuronal death and lead to terminal brainstem dysfunction.13-16
Progression of injury and neurological decline afternonsurvivable traumatic brain injury or catastrophicbrain hemorrhage generally follows a rostral to caudal
path over various intervals but has the same final desti-nation. In patients with rapid progression of brain edemaand corresponding elevations in intracranial pressure(ICP), the cerebral cortex is compressed against the innersurface of the skull. The result is compromised microvas-cular blood flow in higher brain centers and consequentdysfunction as evidenced by progressive loss of conscious-ness. Further progression of injury may lead to patholog-ical posturing and/or seizure activity. Continued increasesin pressure then may lead to transtentorial (central) her-niation syndromes with distortion of the posterior fossaand brain stem displacement through the foramen mag-num.13,17-20 The Cushing response, due to pressure orischemia on the pons, is considered a reflex response tomaintain brain perfusion in patients with elevated ICPsand is characterized by hypertension, bradycardia, andwidened pulse pressure.20 Progression of ischemia or dis-tortion of the medulla oblongata and hypothalamusresults in additional sympathetic outflow as endogenouscatecholamine stores are released, causing hypertension,tachycardia, and vasoconstriction in an effort to main-tain cerebral perfusion pressure.13,14,17,18,20,21
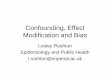
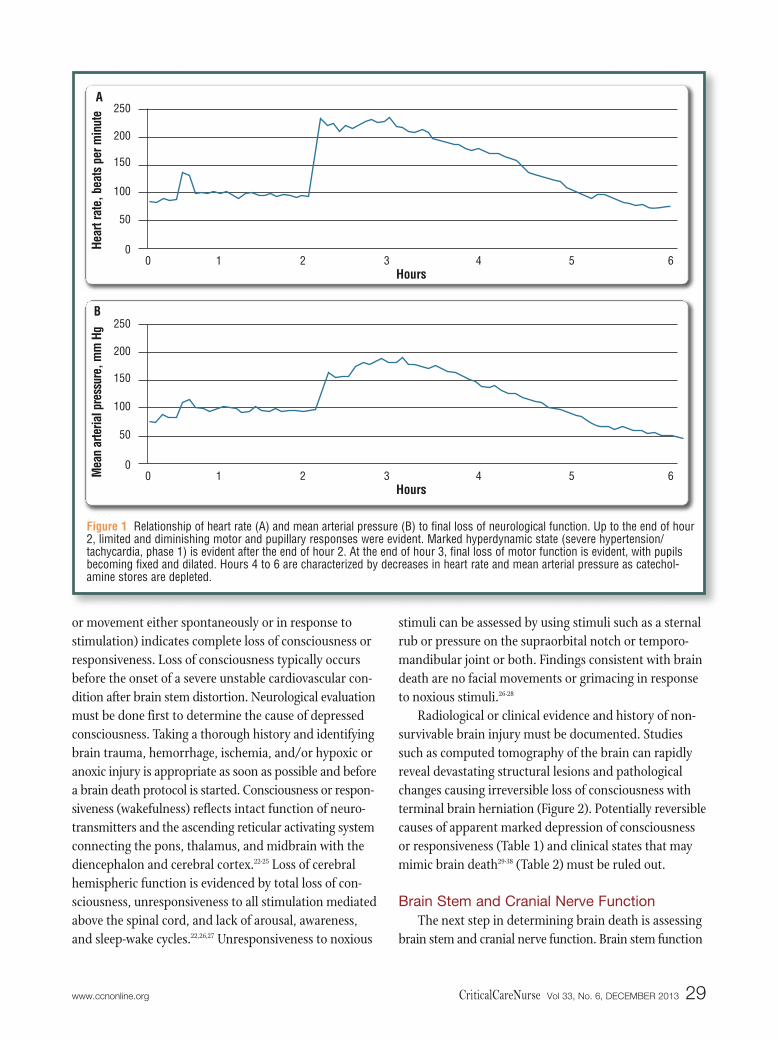
Initially brain stem distortion results in a hyperten-sive state as a reflex response, an attempt to maintainbrain perfusion. Final brain stem dysfunction or hernia-tion, with total loss of catecholamine regulation, causestotal loss of sympathetic control and typically occurs in2 phases. Phase 1 is due to massive catecholamine releaseand total loss of regulation in the sympathetic nervoussystem and is associated with pronounced vasoconstric-tion. Phase 2 occurs after catecholamine depletion andproduces hypotension and loss of vasomotor tone. Eval-uation of changes in vital signs after brain stem distortionor herniation can be part of the neurological assessmentbecause of the relationship between patterns of vitalsigns and severity of brain stem dysfunction (Figure 1).A hypertensive or hyperdynamic state may be evidentimmediately before terminal brain stem dysfunction.
Neurological Assessment and Determination of Brain DeathLevel of Consciousness
Lack of consciousness and unresponsiveness to nox-ious stimuli reflect severe brain dysfunction above thebrain stem. Assessment of consciousness or responsive-ness may be done initially by using the Glasgow ComaScale (GCS). A score of 3 (no eye opening, verbal response,
28 CriticalCareNurse Vol 33, No. 6, DECEMBER 2013 www.ccnonline.org
Richard B. Arbour is a liver transplant coordinator at ThomasJefferson University Hospital in Philadelphia, Pennsylvania.Corresponding author: Richard B. Arbour, RN, MSN, CCRN, CNRN, CCNS, FAAN,5928 N 11th St, Philadelphia, PA 19141 (e-mail: [email protected]).
To purchase electronic or print reprints, contact the American Association of Critical-Care Nurses, 101 Columbia, Aliso Viejo, CA 92656. Phone, (800) 899-1712 or (949)362-2050 (ext 532); fax, (949) 362-2049; e-mail, [email protected].
Author
Optimal care following severe brain injuryincludes surveillance, rapid recognition ofinjury progression and aggressive inter-vention, maximizing chance of recovery.
or movement either spontaneously or in response tostimulation) indicates complete loss of consciousness orresponsiveness. Loss of consciousness typically occursbefore the onset of a severe unstable cardiovascular con-dition after brain stem distortion. Neurological evaluationmust be done first to determine the cause of depressedconsciousness. Taking a thorough history and identifyingbrain trauma, hemorrhage, ischemia, and/or hypoxic oranoxic injury is appropriate as soon as possible and beforea brain death protocol is started. Consciousness or respon-siveness (wakefulness) reflects intact function of neuro-transmitters and the ascending reticular activating systemconnecting the pons, thalamus, and midbrain with thediencephalon and cerebral cortex.22-25 Loss of cerebralhemispheric function is evidenced by total loss of con-sciousness, unresponsiveness to all stimulation mediatedabove the spinal cord, and lack of arousal, awareness,and sleep-wake cycles.22,26,27 Unresponsiveness to noxious
stimuli can be assessed by using stimuli such as a sternalrub or pressure on the supraorbital notch or temporo-mandibular joint or both. Findings consistent with braindeath are no facial movements or grimacing in responseto noxious stimuli.26-28
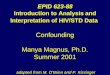
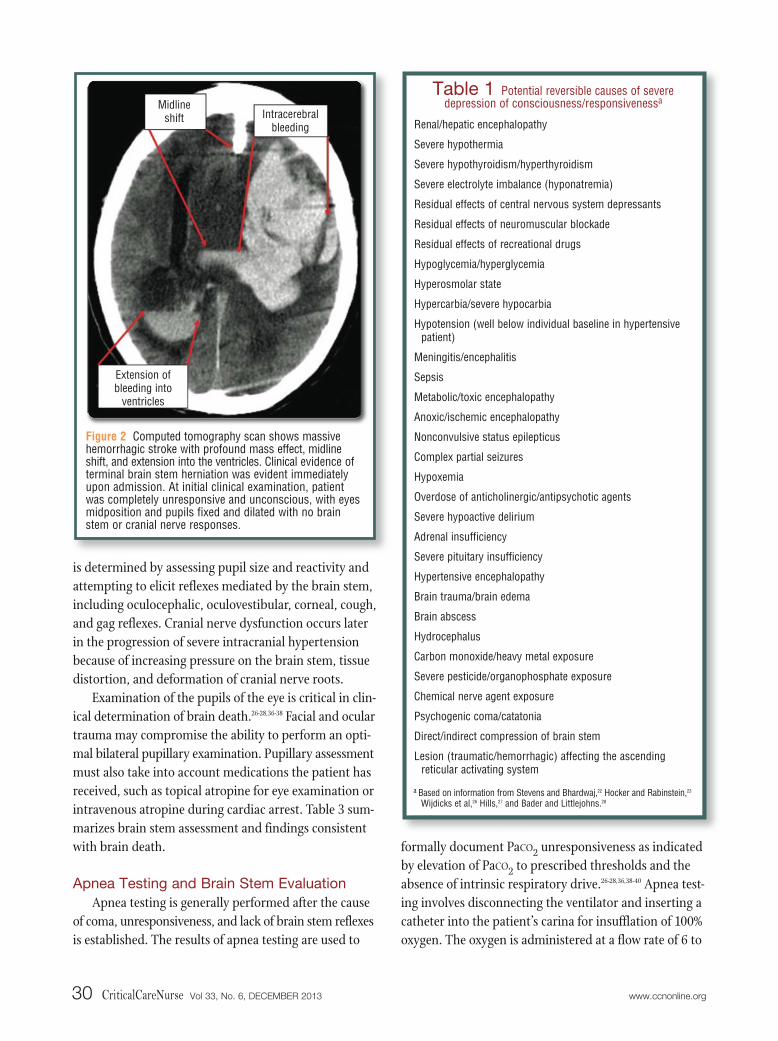
Radiological or clinical evidence and history of non-survivable brain injury must be documented. Studiessuch as computed tomography of the brain can rapidlyreveal devastating structural lesions and pathologicalchanges causing irreversible loss of consciousness withterminal brain herniation (Figure 2). Potentially reversiblecauses of apparent marked depression of consciousnessor responsiveness (Table 1) and clinical states that maymimic brain death29-38 (Table 2) must be ruled out.
Brain Stem and Cranial Nerve FunctionThe next step in determining brain death is assessing
brain stem and cranial nerve function. Brain stem function
www.ccnonline.org CriticalCareNurse Vol 33, No. 6, DECEMBER 2013 29
Figure 1 Relationship of heart rate (A) and mean arterial pressure (B) to final loss of neurological function. Up to the end of hour2, limited and diminishing motor and pupillary responses were evident. Marked hyperdynamic state (severe hypertension/tachycardia, phase 1) is evident after the end of hour 2. At the end of hour 3, final loss of motor function is evident, with pupilsbecoming fixed and dilated. Hours 4 to 6 are characterized by decreases in heart rate and mean arterial pressure as catechol -amine stores are depleted.
Hear
t rat
e, b
eats
per
min
ute
Hours
A250
200
150
100
50
00 1 2 3 4 5 6
Mea
n ar
teria
l pre
ssur
e, m
m H
g
Hours
B250
200
150
100
50
00 1 2 3 4 5 6
is determined by assessing pupil size and reactivity andattempting to elicit reflexes mediated by the brain stem,including oculocephalic, oculovestibular, corneal, cough,and gag reflexes. Cranial nerve dysfunction occurs laterin the progression of severe intracranial hypertensionbecause of increasing pressure on the brain stem, tissuedistortion, and deformation of cranial nerve roots.
Examination of the pupils of the eye is critical in clin-ical determination of brain death.26-28,36-38 Facial and oculartrauma may compromise the ability to perform an opti-mal bilateral pupillary examination. Pupillary assessmentmust also take into account medications the patient hasreceived, such as topical atropine for eye examination orintravenous atropine during cardiac arrest. Table 3 sum-marizes brain stem assessment and findings consistentwith brain death.
Apnea Testing and Brain Stem EvaluationApnea testing is generally performed after the cause
of coma, unresponsiveness, and lack of brain stem reflexesis established. The results of apnea testing are used to
formally document PaCO2 unresponsiveness as indicatedby elevation of PaCO2 to prescribed thresholds and theabsence of intrinsic respiratory drive.26-28,36,38-40 Apnea test-ing involves disconnecting the ventilator and inserting acatheter into the patient’s carina for insufflation of 100%oxygen. The oxygen is administered at a flow rate of 6 to
30 CriticalCareNurse Vol 33, No. 6, DECEMBER 2013 www.ccnonline.org
Figure 2 Computed tomography scan shows massivehemorrhagic stroke with profound mass effect, midlineshift, and extension into the ventricles. Clinical evidence ofterminal brain stem herniation was evident immediatelyupon admission. At initial clinical examination, patientwas completely unresponsive and unconscious, with eyesmidposition and pupils fixed and dilated with no brainstem or cranial nerve responses.
Midlineshift Intracerebral
bleeding
Extension of bleeding into
ventricles
Table 1 Potential reversible causes of severedepression of consciousness/responsivenessa
Renal/hepatic encephalopathy
Severe hypothermia
Severe hypothyroidism/hyperthyroidism
Severe electrolyte imbalance (hyponatremia)
Residual effects of central nervous system depressants
Residual effects of neuromuscular blockade
Residual effects of recreational drugs
Hypoglycemia/hyperglycemia
Hyperosmolar state
Hypercarbia/severe hypocarbia
Hypotension (well below individual baseline in hypertensivepatient)
Meningitis/encephalitis
Sepsis
Metabolic/toxic encephalopathy
Anoxic/ischemic encephalopathy
Nonconvulsive status epilepticus
Complex partial seizures
Hypoxemia
Overdose of anticholinergic/antipsychotic agents
Severe hypoactive delirium
Adrenal insufficiency
Severe pituitary insufficiency
Hypertensive encephalopathy
Brain trauma/brain edema
Brain abscess
Hydrocephalus
Carbon monoxide/heavy metal exposure
Severe pesticide/organophosphate exposure
Chemical nerve agent exposure
Psychogenic coma/catatonia
Direct/indirect compression of brain stem
Lesion (traumatic/hemorrhagic) affecting the ascendingreticular activating system
a Based on information from Stevens and Bhardwaj,22 Hocker and Rabinstein,23
Wijdicks et al,26 Hills,27 and Bader and Littlejohns.28

10 L/min to maintain oxygenation by convection anddiffusion across the alveolar-capillary interface. Thediameter of the insufflation catheter should be approxi-mately 14F to 16F or slightly larger and should notocclude the airway.26-28,36,38 If the insufflation catheter istoo large, high-flow oxygen cannot escape the lungs andmay lead to barotrauma, pneumothorax, or subcutaneousemphysema. The elevation in PaCO2 is generally biphasic,with the more significant and rapid increase within the
initial 1 to 4 minutes. The initial rapid increase is dueto equilibration of arterial and mixed central venouscarbon dioxide followed by a slower increase in arterialcarbon dioxide in response to a basal metabolic state.26
Other techniques used to assess carbon dioxide unre-sponsiveness at the brain stem include controlled hypoven-tilation (minute ventilation, 0.5-2.0 L/min) with frequentmonitoring of PCO2 or continuous positive airway pres-sure, which maintains oxygen flow and stable intra -thoracic pressure.41
Apnea testing, the most critical phase of brain deathtesting, may result in further cardiopulmonary instabil-ity. For maximum safety, apnea testing is done as a col-laborative and multidisciplinary effort. Careful assessmentand monitoring are essential to avoid further instabilityafter terminal brain stem herniation and to identify falseindications of intrinsic respiratory drive. Several stepsshould be undertaken to minimize risk during apneatesting (Table 4).
With close monitoring of the stability of the patient’scardiovascular status, available physiological parameters,and assessment of the chest and/or abdominal wall for
www.ccnonline.org CriticalCareNurse Vol 33, No. 6, DECEMBER 2013 31
Table 2 Factors that may mimic brain death
Locked-in syndrome
Fulminant Guillain-Barré syndrome
Severe hypothermia
Post–cardiac arrest syndrome
Massive baclofen/anticholinergic overdose
Severe overdose of central nervous system depressants
Massive overdose of valproic acid
Massive overdose of tricyclic antidepressants
Severe snake envenomation
Brain stem reflex
Oculocephalic
Oculovestibular (coldcalorics)
Corneal
Cough/gag
Pupillary light
Cranial nerve(s), brain areas tested
III, oculomotorIV, trochlearVIII, vestibulocochlearPons and midbrain
III, oculomotorIV, trochlearVI, abducensVIII, vestibulocochlear Pons and midbrain
III, oculomotorV, trigeminalVII, facialPons
IX, glossopharyngealX, vagusMedulla
II, opticIII, oculomotorMidbrain
Examination technique
After spinal cord injury, other contraindicationsruled out: rapidly rotate patient’s head to eitherside and observe for eye movement relative toorbit
After tympanic membrane rupture, other con-traindications, and cerumen deposits ruled out:elevate head of bed to 30º (if no contraindicationsto doing so), irrigate each ear canal in turn with50 mL of ice water, observe for eye movement/deviation
Lightly brush cornea with sterile cotton swab
Gag reflex: stimulate deep posterior pharynx(oral/pharyngeal suction device)
Cough reflex: use deep endotracheal suctioning todepth of carina (2 passes with suction catheter)
Assess pupillary size and shape in slightly dark-ened room; shine a bright light into each eyeand assess reaction (or not) in each eye
Findings consistent with brain death
No apparent eye movementwithin the orbit
No eye movement for 1 minute after irrigationof each ear canal
No eye blink in response tocorneal stimulation
No response to either stimulation
Pupils dilated to a possiblerange of 4-9 mm diameter,nonreactive to bright light,and midposition withinthe orbit
Table 3 Brain stem assessment during determination of brain deatha
a Based on information from Wijdicks et al,26 Hills,27 Bader and Littlejohns,28 Morenski et al,36 Henneman and Karras,37 and Wijdicks.38

indications of intrinsic respiratory drive, apnea testingcontinues for 8 to 10 minutes if tolerated. Indications foraborting apnea testing include marked oxygen desatura-tion (<85% for >30 seconds) and/or unstable bloodpressure (<90 mm Hg systolic and unresponsive to drugtherapy) and/or unstable cardiac rhythm (bradycardia,ventricular ectopy).26-28,38,39 If aborted, apnea testing can betried again by using a secondary technique with T-piece,continuous positive airway pressure at 10 cm H2O, and100% oxygen at 12 L/min.26,40 This approach is not aswidely used as supporting oxygenation with an insuffla-tion catheter for high-flow oxygen but may be an alter-native. With no intrinsic respiratory drive, samples forarterial blood gas analysis are obtained after 8 to 10minutes. Results of apnea testing consistent with braindeath include no movement of the chest and abdominalwalls (a finding consistent with no intrinsic respiratorydrive) and PaCO2 elevations 20 mm Hg or greater frombaseline or reaching a threshold of 60 mm Hg.26-28,36,38-41
If results are inconclusive after 10 minutes, with norespiratory drive, and the patient’s condition is stable,
apnea testing can be repeated for a longer interval (10-15 minutes) after appropriate preparation.26,27 If thepatient’s cardiopulmonary status is severely unstableand apnea testing is not tolerated, documentation andpossibly adjunctive testing are required.28
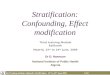
Assessment during apnea testing includes assessingfor movement of the chest and/or abdominal wall anddifferentiating between movements associated with res-piratory effort, such as retraction of the chest or abdomi-nal wall, use of intercostal muscles, and nasal flaring ormouth movements, and movements produced in phasewith the cardiac cycle. The cardiovascular state associatedwith terminal brain stem dysfunction can produce a highcardiac output and stroke volume and potentially causemovements of the chest or abdominal wall in phase withthe cardiac cycle; this condition is termed hyperdynamicprecordium.5,13,42 Any members of the health care teaminvolved in apnea testing should be aware of how quicklya patient’s cardiovascular status can become unstable.Blood pressure may decrease from baseline to criticallylow levels within seconds (Figure 3).
32 CriticalCareNurse Vol 33, No. 6, DECEMBER 2013 www.ccnonline.org
Steps
Stabilize systolic blood pressure ≥100 mm Hg
Stabilize body temperature ≥36.5ºC (preferred)(Apnea testing can be done at lower tempera-tures, but additional time required for increasein CO2, risking cardiovascular instability)
Normalize PaCO2 to range of 35-45 mm Hg
Maintain adequate circulating blood volume
Administer 100% oxygen for ≥10 minutes toPaO2 ≥200 mm Hg
Method
Appropriate titration of inotropicand/or vasoactive agents
Use of heating blankets, infusion ofwarmed intravenous fluids, heatlamps
Downward titration of controlled ven-tilation (tidal volume/ventilator setrate) unless contraindicated to attainnormocarbia/baseline PaCO2
Appropriate administration of crystal-loid, colloid, and/or blood productsto replace volume losses and correctabsolute/relative hypovolemia
Fraction of inspired oxygen 1.0 withpositive end-expiratory pressure at 5 cm H2O
When pulse oximetry indicates stableoxygen saturation, assay arterial bloodgases to document baseline level
Rationale
Optimizes cardiovascular stability, tissueperfusion, and physiological reserve
Necessary because of loss of vasomotortone
Hypothermia suppresses neuronal activityincluding at brain stem level and prolongsduration of action for central nervoussystem depressants and neuromuscularblockers
Baseline arterial CO2 level establishes astarting point for CO2 measurement atintervals
Beginning with hypocarbic state willrequire additional time for CO2 increaseand increase risk for cardiovascularinstability
Stabilizes cardiovascular/blood pressureduring stress of apnea testing
Facilitates oxygenation, eliminates nitrogenstores, and avoids oxygen desaturationand cardiovascular consequences
Table 4 Preparatory steps before apnea testinga
a Based on information from Wijdicks et al,26 Hills,27 Bader and Littlejohns,28 Wijdicks,38 Scott et al,39 and Wijdicks et al.40

Adjunctive Neurodiagnostic TestingIf apnea testing is not tolerated by the patient, the
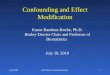
results are inconclusive, or shorter intervals are requiredbetween initiation and completion of a brain death pro-tocol, ancillary neurodiagnostic testing26-28,36,38,43-56 (Table 5)may be appropriate. Early use of adjunctive testing maydecrease intervals between terminal brain stem hernia-tion, declaration of brain death, and organ recovery fortransplant, facilitating earlier hormonal resuscitationprotocols and earlier organ recovery. Neurodiagnosticoptions include 4-vessel cerebral angiography (Figure 4),radionuclide cerebral perfusion scan (Figure 5), and electroencephalography26-28,36,38,43 (Figure 6), as well astranscranial Doppler ultrasound and computed tomo-graphic angiography. Potential limitations are associatedwith adjunctive testing, and in some instances, theresults may be equivocal. Use of neurodiagnostic testingsuch as 4-vessel angiography and radionuclide flowstudy to expedite determination of brain death may beindicated in clinical situations such as concurrent use ofhigh-dose barbiturates and therapeutic hypothermia forintracranial hypertension that progressed to terminalherniation.
Adjunctive neurodiagnostic testing is contradicted inany patient whose cardiopulmonary status is so unstablethat it precludes transporting the patient out of the ICU
a long distance for radiological studies. Brain death (aclinical diagnosis) can occur with preservation of cere-bral blood flow if ICP is insufficient to eliminate all cere-bral bloodflow.47 If theresults ofadjunctivetesting areinconclu-sive, optionsmay include repeating the examination later or waitingfor drug clearance (central nervous system depressants),thereby enabling optimal clinical neurological assessment.47
Confounding Factors in Brain DeathAfter an irreversible cause of unconsciousness is
identified, determination of brain death is based primarilyon clinical findings, including results of clinical neurolog-ical examination, papillary examination, and brain stemand apnea testing.26-28,36-38 Patients’ movements in braindeath may also be confounding factors in clinical evalua-tion. Possible confounding factors include spinal cordinjury, movements in brain death (complex spinal reflexes,muscle fasciculations, ventilator autotriggering), thera-peutic hypothermia, and transient brain stem depressionafter cardiopulmonary arrest5,13,32,34,38,42,45,57-86 (Table 6).
Clinically appropriate use of adjunctive neurodiagnostic testing, with good selectionof patients, may decrease intervals betweenterminal brain stem herniation and declarationof death by neurologic criteria.
www.ccnonline.org CriticalCareNurse Vol 33, No. 6, DECEMBER 2013 33
Figure 3 Illustration of rapid cardiovascular compromise upon initiation of apnea testing. Apnea testing was initiated at 15:29:13with systolic blood pressure of 140 mm Hg. By 15:29:26, systolic blood pressure was 70 mm Hg. By the time ventilation wasrestored at 15:29:37, systolic blood pressure was 45 to 50 mm Hg. The patient’s blood pressure recovered quickly when con-trolled ventilation was restarted with no additional complications. Tracing sweep speed is 25 mm/s.
15:29:13
Bloo
d pr
essu
re, m
m H
g
15:29:26
15:29:37
160
120
80
40
0
160
120
80
40
0 25 mm/s

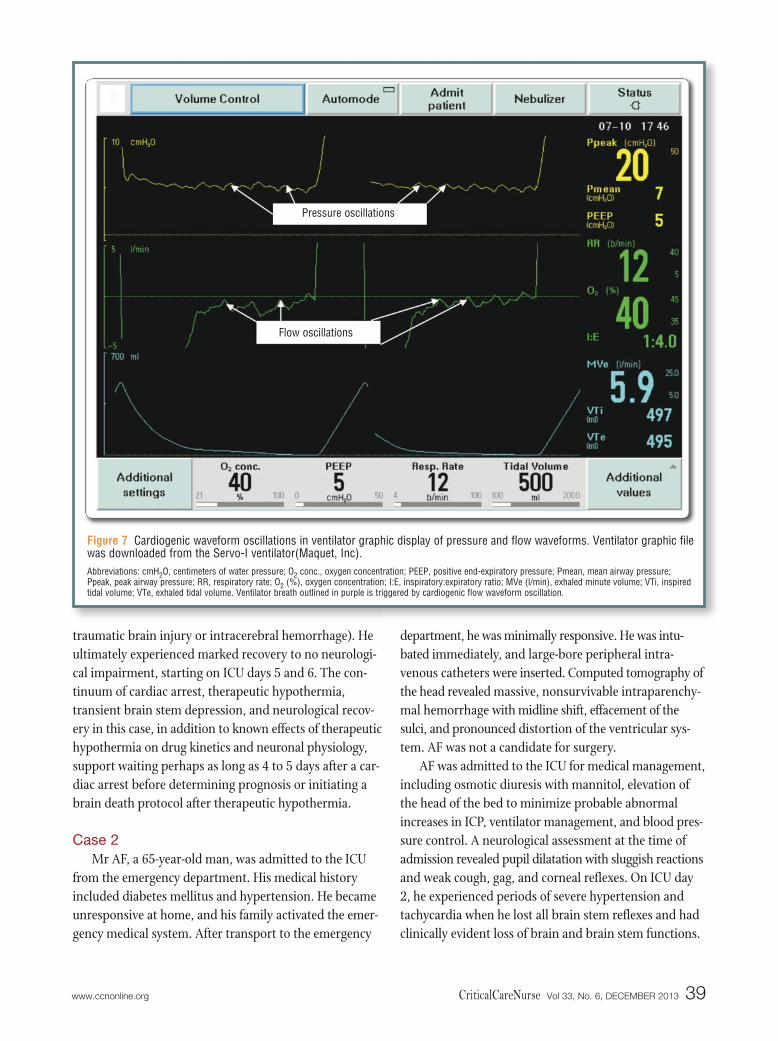
Several well-written references5,13,42,64,65,67 provide a morecomplete analysis of risk factors, physiology, recognition,and clinical management of ventilator autotriggering.Figure 7 illustrates cardiogenic waveform oscillations inpressure and flow waveforms.
Case StudiesThe following 2 case studies illustrate clinical issues
and confounding factors encountered with neurologicalevaluation to determine brain death. Patient 1 had severeanoxic-ischemic brain injury following resuscitationfrom cardiopulmonary arrest after which he was treatedwith therapeutic hypothermia. Results of a neurologicalexamination indicated terminal brain stem dysfunction.
Patient 2 had a nonsurvivable intracerebral hemorrhageand had clinically evident catastrophic cerebral andbrain stem dysfunction. In this case, a formal braindeath protocol was initiated but was interrupted becausethe patient was breathing faster than the rate set for theventilator, falsely indicating intrinsic respiratory drive.
Case 1SB, a 52-year-old man with no history of cardiovas-
cular disease, experienced cardiopulmonary arrest dueto ventricular fibrillation. A total of 6 minutes elapsedbefore he received cardiopulmonary resuscitation. Hisfamily activated the emergency medical system and begancardiopulmonary resuscitation; he also received Advanced
34 CriticalCareNurse Vol 33, No. 6, DECEMBER 2013 www.ccnonline.org
Test
4-Vessel cerebral angiography
Radionuclide cerebral perfusion scanning
Diagnostic electroencephalography (EEG)
Emerging techniques
Transcranial Doppler ultrasound
Computed tomographic angiography
Description
Injection of radiopaque contrast material intocarotid/vertebrobasilar systems throughcatheter inserted via femoral artery and positioned radiographically
Injection of radioisotope tracer such as technetium-99m, serial anteroposterior and lateral skull imaging (30, 60, 120 minutes)
Full diagnostic EEG with array of scalp electrodesDevice sensitivity ≥2 μV and tracing ≥30 minutesTracing evaluated in response to visual/auditory
stimulation
Placement of transducer over insonation windows (temporal and occipital) and determination of blood flow state
Injection of contrast material during image acquisition of brain
Advantages
Short time to obtain results, easy to interpret,and when consistent with brain death,definitive
Less invasive than other methods, rapidinterpretation, no contrast load on kidneys
Easy access to perform at bedside, noninvasive, and data available quickly
Can be performed at bedside and rapidly inter-preted with appropriately trained personnel
Validated to measure cerebral blood flow statein vasospasm, cerebral autoregulatory state,and perfusion
Strong positive correlation with results of 4-vessel angiography
Useful for determining timing of 4-vesselangiography
Less invasive than 4-vessel angiography,rapid image acquisition, ability for brainevaluation in presence of central nervoussystem depressants, and widely available
Strong correlation with results of 4-vesselangiography
Table 5 Adjunctive/confirmatory testing used in brain death determination

Life Support therapy. Time to return of spontaneous cir-culation was approximately 25 minutes. The patient wasintubated, received controlled ventilatory support, andwas transported immediately to the emergency depart-ment. He was comatose and unresponsive with dilatedand minimally responsive pupils. Therapeutic hypother-mia was started within approximately 3 hours of returnof spontaneous circulation. His core body temperaturedecreased from 36.5ºC to 32.3ºC during an interval of 2.5hours. He received midazolam, fentanyl, and vecuroniuminfusions concurrently for sedation, analgesia, and neu-romuscular blockade/shivering management, respectively.
Neurological evaluation and prognostication duringthe maintenance phase of therapeutic hypothermia were
not possible because of the use of neruomuscular block-ers and central nervous system depressants and the con-current effects of hypothermia on pharmacokinetics andneuronal physiology. After the patient had been in thetarget temperature range of 32ºC to 34ºC for 27 hours,the rewarming phase of therapeutic hypothermia wasstarted; 5 hours later his baseline temperature was 36.5ºC.On ICU day 3 (after rewarming and discontinuation orrecovery from neuromuscular blockers and centralnervous system depressants) his GCS score was 3: nocough or gag reflexes; dilated, nonreactive pupils; unre-sponsiveness to noxious stimuli; and no clinically evidentbrain or brain stem function. His neurological prognosison ICU day 4 was considered abysmal, and withdrawal
www.ccnonline.org CriticalCareNurse Vol 33, No. 6, DECEMBER 2013 35
Limitations
Invasive, requires transport to angiography suite of patientwho may be in unstable condition
Administering contrast material may compromise kidney functionIf brain death not associated with current elevation of intracra-
nial pressure (hypoxic injury, craniectomy), flow may be pre-served in clinical examination, consistent with brain death
Requires extended transport of patient who may be in unsta-ble condition
May yield radiographic evidence of flow in clinical examinationconsistent with brain death (craniotomy defect, absence ofsignificant elevation of intracranial pressure)
Electrical interference in intensive care unit (intravenous pumps,beds, ventilators, personnel) may be reflected in EEG and bedifficult to prove to patient’s family that findings do not indicateactivity in the patient’s brain
Cardiac artifact may give false hope to family looking for “flat”EEG to mean brain death
EEG does not reflect activity in deep structures such as brainstem and can be affected by clinical states such as hypother-mia, residual central nervous system depressant effects, andtransient neuronal dysfunction after cardiac arrest
Can be technically difficult to find insonation windowsSignal can be compromised by skull thicknessLarge cranial defect can yield evidence of cerebral blood flow
with isoelectric EEG and findings on clinical examinationconsistent with brain death
Cerebral flow may be evident with low intracranial pressureand/or large craniotomy defect in patient meeting clinical criteria for brain death
More study required for further validation in United States
Normal findings
Net forward blood flow fromcarotid/vertebrobasilar systeminto brain, filling larger vessels(Figure 4A)
Uptake of isotope in distributionof cerebral vessels (Figure 5A)
Generally high-frequency andlow-amplitude waveforms onEEG tracing
EEG also variable in response totactile, somatosensory, audi-tory, and/or visual stimulation(Figure 6A)
Net forward flow of blood visualized through occipital/temporal windows
Flow preservation (opacificationof vessels) within cerebralvasculature
Findings in brain death
Lack of cerebral vessel filling aboveskull entry points for carotid and vertebrobasilar circulation (Figure 4B)
No uptake of isotope in distribution ofcerebral vessels (Figure 5B)
Lack of cerebral electrical activity andinvariant in response to tactile,somatosensory, auditory, and visualstimulation (Figure 6B)
Brief systolic forward flow or systolicspikes and diastolic reverse flow
Brief systolic forward flow or systolicspikes and no diastolic flow
No demonstrable flow in a patient inwhom flow was previously evident onDoppler images
No flow of contrast material within middle cerebral artery, cerebral venoussystems, and vertebrobasilar system

of aggressive support was considered. On ICU days 5and 6, his neurological status improved, beginning withrecovery of cough and gag reflexes and then full pupilreactivity. By ICU day 7, SB was awake and followingcommands. He required close supervision pending fullcognitive recovery for much of the remainder of hisinpatient stay. When discharged from the hospital, hewas fully ambulatory, interacted with others, and hadno neurological impairment.
At one stage after rewarming (day 3 after the cardiacarrest), SB met clinical criteria of brain death to thepoint that a formal brain death protocol might havebeen considered in other circumstances (eg, massive
36 CriticalCareNurse Vol 33, No. 6, DECEMBER 2013 www.ccnonline.org
Figure 4 Cerebral angiograms show normal blood flowto brain (A) and lack of blood flow to brain consistentwith death according to neurological criteria (B).
A
B
Figure 5 Radionuclide flow study shows normal uptake ofisotope into cerebral tissue (A) consistent with stable brainmetabolism and blood flow, inconsistent with death accord-ing to neurological criteria. Anteroposterior (B) and lateral(C) views illustrate “hollow skull” phenomenon consistentwith lack of radioisotope uptake into the brain and lack ofbrain perfusion. This finding in context with neurologicalexamination findings of no brain/brain stem function; pupilsfixed, dilated, and midposition; and apnea test indicating totalunresponsiveness to carbon dioxide and no intrinsic respi-ratory drive within formal brain death evaluation supports adetermination of death according to neurological criteria.
Figure 5A adapted from Arbour,13 with permission from Lippincott Williamsand Wilkins/Wolters Kluwer Health.
A
B
C

www.ccnonline.org CriticalCareNurse Vol 33, No. 6, DECEMBER 2013 37
Figure 6 Electroencephalography (EEG) tracings of a patient who is responsive and interactive with the environment (A) and apatient with brain death (B). Each tracing encompasses a 20-second interval of EEG data collection. Electrocardiographic (EKG)artifact is prominent in B.
Fp1-F7
A
B
F7-T3T3-T5T5-O1
Fp2-F8F8-T4T4-T6T6-O2
Fp1-F3F3-C3C3-P3P3-O1
Fp2-F4F4-C4C4-P4P4-O2Fz-CzCz-PzA1-CzCz-A2*EKG
Fp1-A1F7-A1T3-A1T5-A1O1-A1
Fp2-A2F8-A2T4-A2T6-A2O2-A2F3-A1C3-A1P3-A1F4-A2C4-A2P4-A2Fz-CzCz-PzA1-CzCz-A2*EKG

Confounding factor
High cervical spinalcord injury
Complex spinal reflexmovements
Muscle fasciculations
Ventilator autotriggering
Cardiac autotriggeringand context of braindeath physiology
Interventions for suspected cardiogenic ventilator autotriggering
Therapeutic hypothermia
Neurological evaluationafter a cardiac arrest
Implications in brain death determination
Cough/gag reflexes, motor responses to noxious stimulation, intrinsic respiratory drive, and valid apnea testingrequire intact spinal cord function
High spinal cord injury can result in no responses to brain stem testing with preserved brain/brain stem function
Movements including arm adduction/elbow flexion may resemble purposeful localizing to the airwayMuscle stretch reflexes, abdominal muscle movements, facial twitching, persistent positive Babinski reflexes,
and toe flexion from plantar stimulation may be elicited by mechanical stimulation of the spinal cord/sensorynerve roots or during transcranial Doppler ultrasound
“Lazarus sign” (shoulder adduction, elbow flexion, arm lifting, possible crossing of hands) may also occurThese possibly frequent (~43% occurrence) movements in brain-dead patients may falsely suggest that brain
death has not occurred
Fasciculations affecting extremities, chest, and abdomen may occur, beginning shortly after terminal brainstem herniation and persist up to 2-3 days
Fasciculations may falsely suggest presence of brain/brain stem function
Intrinsic and extrinsic causes of ventilator autotriggering may falsely suggest residual brain stem function andpreservation of intrinsic respiratory drive
Extrinsic causes include airway cuff leak, bronchopleural fistula, and chest tube leakIntrinsic causes include mechanical circulatory supports such as intra-aortic balloon pump, cardiogenic
autotriggering, and total artificial heartIntrinsic and/or extrinsic causes may affect intrathoracic pressure dynamics, altering ventilator airway
pressure and bias flow, and may trigger a ventilator breathThis factor may delay or result in abortion of formal brain death protocol(s)
Phase 1 (hypertensive) after brain stem herniation produces higher stroke volume due to increased catecholamine level and inotropic state
Phase 2 (hypotensive) with higher stroke volume is due to decreased vascular tone and cardiac workCyclical volume displacement in thorax is due to expansion/contraction of cardiac size and forward blood flow
from cardiac cycleStroke volume may be normal (60-100 mL), change in cardiac volume at systole (61 ± 2 mL or -8.2% ± 0.8%)Net intrathoracic volume change with cardiac cycle may exceed 120-160 mLCyclical variation in pulmonary blood flow with cardiac cycle occursCorrelation between pulmonary blood flow/cardiac oscillation in airway pressure/flow waveforms is positiveCyclical blood flow/cardiac size changes may displace compliant lung tissue, causing gas displacement in
patient-ventilator system and oscillations in pressure and/or flow waveformsIf cardiac oscillations exceed ventilator trigger threshold, breath may be delivered
Analyze ventilator flow and pressure waveforms concurrently with clinical evaluation; include decreasing waveform scales, increasing detail available to review
Match precordial motion with cardiac cycle, pulse palpation, auditory tone (beep), and QRS on bedside monitor as well as corresponding oscillations on ventilator flow and pressure waveforms
Identify or rule out indications of intrinsic respiratory drive on clinical evaluation and ventilator waveform analysisIf cardiogenic oscillations are present and exceed ventilator trigger threshold, increase trigger threshold
beyond their amplitudeChanging from flow to pressure triggering such as -2 cm H2O may be sufficient to eliminate autotriggering
Treatment is increasingly used after cardiac arrest, as an option for hepatic encephalopathy/brain edema as abridge to liver transplant, case-by-case basis for elevation of intracranial pressure after traumatic brain injuryand research for therapy after stroke
Anoxic-ischemic brain injury can progress to neuronal death/brain deathTemperature-dependent slowing of neuronal impulse generation and conductionPharmacokinetic changes prolong duration of action of central nervous system depressants and neuromuscular
blockadeAll evaluations (electroencephalography, evoked potentials, pupillary light response, and brain stem reflexes)
are alteredLack of motor/papillary light responses 72 hours after cardiac arrest not universally reliable outcome
predictorsWaiting 72 hours after rewarming (4-5 days after cardiac arrest) may be appropriate to account for
pharmacokinetic changes/central nervous system depressants/neuromuscular blocking agents
Delayed neurological recovery may be associated with transient brain/brain stem depression due tohypoxic/anoxic injury
Unexpected recovery after cardiac arrest and therapeutic hypothermia have occurredNeurological evaluation/prognosis should be done cautiously, possibly >72 hours
Table 6 Confounding factors and related clinical implications in determination of brain deatha
a All patients reported as having muscle movement related to complex spinal reflexes or fasciculations met formal criteria for brain death.
38 CriticalCareNurse Vol 33, No. 6, DECEMBER 2013 www.ccnonline.org
traumatic brain injury or intracerebral hemorrhage). Heultimately experienced marked recovery to no neurologi-cal impairment, starting on ICU days 5 and 6. The con-tinuum of cardiac arrest, therapeutic hypothermia,transient brain stem depression, and neurological recov-ery in this case, in addition to known effects of therapeutichypothermia on drug kinetics and neuronal physiology,support waiting perhaps as long as 4 to 5 days after a car-diac arrest before determining prognosis or initiating abrain death protocol after therapeutic hypothermia.
Case 2Mr AF, a 65-year-old man, was admitted to the ICU
from the emergency department. His medical historyincluded diabetes mellitus and hypertension. He becameunresponsive at home, and his family activated the emer-gency medical system. After transport to the emergency
department, he was minimally responsive. He was intu-bated immediately, and large-bore peripheral intra-venous catheters were inserted. Computed tomography ofthe head revealed massive, nonsurvivable intraparenchy-mal hemorrhage with midline shift, effacement of thesulci, and pronounced distortion of the ventricular sys-tem. AF was not a candidate for surgery.
AF was admitted to the ICU for medical management,including osmotic diuresis with mannitol, elevation ofthe head of the bed to minimize probable abnormalincreases in ICP, ventilator management, and blood pres-sure control. A neurological assessment at the time ofadmission revealed pupil dilatation with sluggish reactionsand weak cough, gag, and corneal reflexes. On ICU day2, he experienced periods of severe hypertension andtachycardia when he lost all brain stem reflexes and hadclinically evident loss of brain and brain stem functions.
www.ccnonline.org CriticalCareNurse Vol 33, No. 6, DECEMBER 2013 39
Figure 7 Cardiogenic waveform oscillations in ventilator graphic display of pressure and flow waveforms. Ventilator graphic filewas downloaded from the Servo-I ventilator(Maquet, Inc). Abbreviations: cmH2O, centimeters of water pressure; O2 conc., oxygen concentration; PEEP, positive end-expiratory pressure; Pmean, mean airway pressure;Ppeak, peak airway pressure; RR, respiratory rate; O2 (%), oxygen concentration; I:E, inspiratory:expiratory ratio; MVe (l/min), exhaled minute volume; VTi, inspiredtidal volume; VTe, exhaled tidal volume. Ventilator breath outlined in purple is triggered by cardiogenic flow waveform oscillation.
Pressure oscillations
Flow oscillations

His GCS score was 3: pupils fixed, dilated, and midposi-tion. After his condition was stabilized, a brain deathprotocol was initiated. Per policy, the first of 2 formalneurological examinations was completed, documentingtotal loss of consciousness or responsiveness; no cough,gag, or corneal reflexes; no oculocephalic or oculovestibu-lar reflexes; and no respiratory drive—all findings con-sistent with brain death. The second examination wasscheduled for 6 hours later.
Approximately 3 hours after the initial examination,AF was breathing faster than the rate set on the ventila-tor, an action potentially inconsistent with brain death.His neurological assessment was unchanged as com-pared with the initial formal examination, which showedfindings consistent with death by neurological criteria.Cardiopulmonary assessment revealed hyperdynamicprecordium with chest wall movements in exact phasewith the cardiac cycle, matching pulse palpation, andQRS tone shown on the bedside monitor. In addition,
examinationof the patient-ventilator sys-tem indicatedregular oscilla-tions in venti-lator pressure
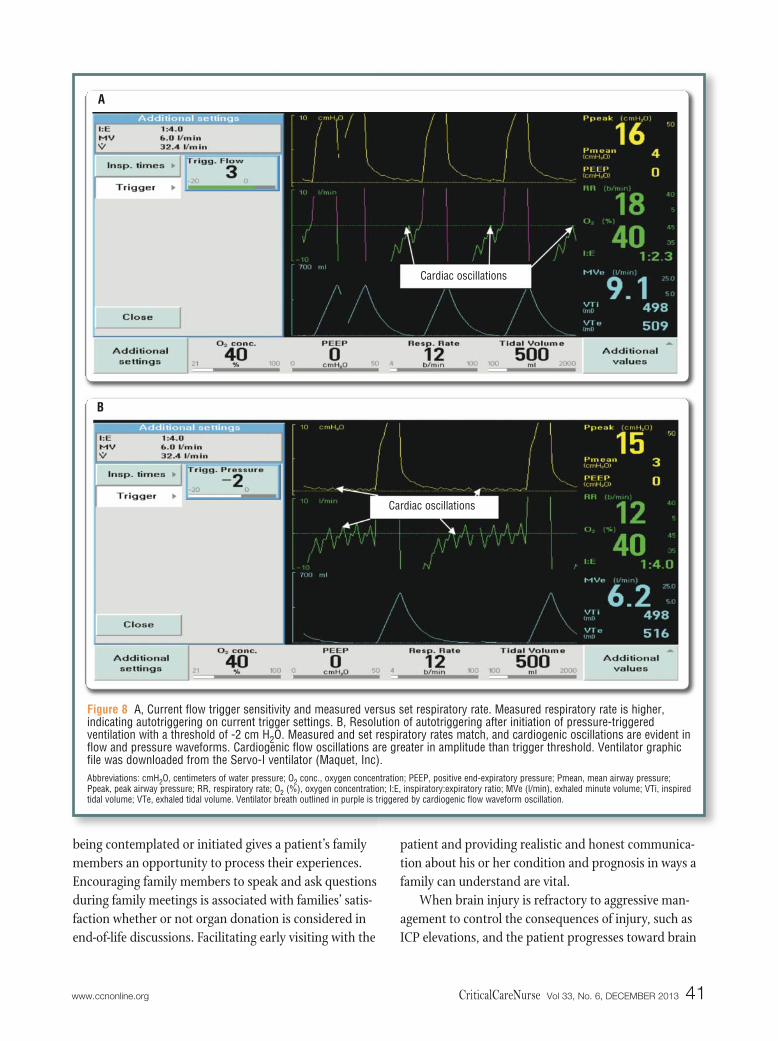
and flow waveforms in exact phase with pulse palpation,QRS tone, and precordial movements. Waveform scaleswere decreased to increase detail available on waveformanalysis. Flow triggering with a threshold of 2 L/minwas being used. Flow waveform oscillations exceededthe sensitivity of the flow trigger. The sensitivity wasincreased to 3 L/min with the patient still breathingfaster than the rate set for the ventilator (Figure 8A).Pressure triggering was initiated with a threshold of -2 cm H2O. This change eliminated autotriggering with aresulting match between set and measured respiratoryrate on the ventilator. There were also no indications ofintrinsic respiratory drive as determined by close clinicalevaluation and ventilator waveform analysis (Figure 8B).With the problem of autotriggering resolved, the secondneurological examination was performed, and apneatesting indicated total loss of carbon dioxide reactivitymediated by the brain stem. The results were consistentwith brain death, and the patient was declared deadaccording to neurological criteria. AF was medicallysuitable for organ donation, and consent was obtained
for organ recovery. After optimization of cardiopulmonarystatus and organ function, his liver and kidneys wererecovered and transplanted.
The care of AF illustrates multidisciplinary evaluationamong nurses, respiratory therapists, and physicians inidentifying and managing cardiac autotriggering thatmight have delayed completion of a brain death protocolor caused confusion about neurological status or both.With rapid identification and clinical management ofautotriggering, the problem was resolved and braindeath was pronounced, facilitating organ recovery.
Nursing ConsiderationsNursing considerations in brain death are not lim-
ited to clinical management after declaration of deathaccording to neurological criteria. Nursing considera-tions begin when a patient is admitted to the ICU, wellbefore initiation of a brain death protocol.
Montoring, Interventions, and Family CareGoals of frequent, dynamic neurological assessments
of patients with brain injury include identifying injuryprogression, detecting stabilized neurological status orresponse to therapy, and rapidly determining and actingon opportunities for intervention before brain herniationsyndromes occur. Patient advocacy and vigilance are vitalto identify and aggressively treat consequences of injuryto other body systems at the earliest opportunity. Whenevolving consequences of brain injury are identified,patient advocacy may take the form of prioritizing aggres-sive, mechanism-based care in treating intracranialpathophysiology. Advocacy, honesty, and the develop-ment of trust between a patient’s family and personnelon the health care team markedly promote communica-tion and rapport during a stressful and difficult time forthe family. Family members of a patient with a devastat-ing brain injury are under stress8 and need empathy,teaching, and an environment of trust. Nurses are pivotalto establish trust and help the family understand the tor-rent of information from multiple health care providers.Taking time and building on the trust established uponICU admission can help the family understand braininjury, progression of the injury, and what brain deathmeans. All these considerations are vital with or withoutorgan recovery and transplantation as possible end points.
Allowing time and resources, including spiritual sup-port or chaplains, when formal brain death protocols are
40 CriticalCareNurse Vol 33, No. 6, DECEMBER 2013 www.ccnonline.org
A patient who has had terminal brain stemherniation and a clinical examination consistent with brain death may still experience spinal reflex movements or cardiac ventilator autotriggering as possibleconfounding factors.
being contemplated or initiated gives a patient’s familymembers an opportunity to process their experiences.Encouraging family members to speak and ask questionsduring family meetings is associated with families’ satis-faction whether or not organ donation is considered inend-of-life discussions. Facilitating early visiting with the
patient and providing realistic and honest communica-tion about his or her condition and prognosis in ways afamily can understand are vital.
When brain injury is refractory to aggressive man-agement to control the consequences of injury, such asICP elevations, and the patient progresses toward brain
www.ccnonline.org CriticalCareNurse Vol 33, No. 6, DECEMBER 2013 41
Figure 8 A, Current flow trigger sensitivity and measured versus set respiratory rate. Measured respiratory rate is higher, indicating autotriggering on current trigger settings. B, Resolution of autotriggering after initiation of pressure-triggered ventilation with a threshold of -2 cm H2O. Measured and set respiratory rates match, and cardiogenic oscillations are evident inflow and pressure waveforms. Cardiogenic flow oscillations are greater in amplitude than trigger threshold. Ventilator graphicfile was downloaded from the Servo-I ventilator (Maquet, Inc). Abbreviations: cmH2O, centimeters of water pressure; O2 conc., oxygen concentration; PEEP, positive end-expiratory pressure; Pmean, mean airway pressure;Ppeak, peak airway pressure; RR, respiratory rate; O2 (%), oxygen concentration; I:E, inspiratory:expiratory ratio; MVe (l/min), exhaled minute volume; VTi, inspiredtidal volume; VTe, exhaled tidal volume. Ventilator breath outlined in purple is triggered by cardiogenic flow waveform oscillation.
Cardiac oscillations
A
B
Cardiac oscillations

death, empathy and honesty are important in commu-nicating this decline to the patient’s family members.Critical care nurses are often the first care providers torecognize a patient’s worsening neurological status andinitiate formal neurological evaluation for brain death.87
At this stage, with a worsening neurological status, spe-cific clinical triggers may be met to initiate referral of apotential donor to the organ procurement organization.The triggers may include a decrease in the GCS score orloss of one or more brain stem reflexes or both. The rep-resentative of the procurement organization has nodirect involvement in clinical management of the patientuntil brain death is formally declared and consent hasbeen obtained for organ donation. Direct involvementin clinical management by an organ procurement organ-
ization beforedeclarationof braindeath is apotentialconflict of
interest.88 Any family discussion should start with athorough explanation of the patient’s grave conditionand should include definition of terms. Providing a cleardefinition of brain death and ensuring the family’sunderstanding before organ donation is discussed arevital to avoid later misunderstanding.89 Communicationwith family members after completion of a brain deathprotocol needs to be unequivocal that brain dead is dead.89
The dead-donor rule requiring declaration of deathbefore organ recovery for transplant can then apply.90
Bedside clinicians must maintain frequent monitor-ing, begin preparatory steps for clinical examinationscalled for in a brain death protocol, and facilitate safetransport for neurodiagnostic studies as appropriate.Preparation for clinical examinations may consist ofpositioning and monitoring the patient, optimizing astable cardiopulmonary status for apnea testing, andpositioning the patient for assessment of brain stemreflexes. Ruling out cervical spine injury before assess-ment of oculocephalic reflexes and rupture of the tym-panic membrane before assessment of oculovestibularreflexes are appropriate. Obtaining sterile cotton swabsfor assessing corneal reflexes and ice water and syringesfor caloric stimulation of the ear is appropriate.
Any discussions with a patient’s family should takeinto account cultural and religious perspectives and how
family members define death. Brain death may havevariable meanings for individuals. One meaning may besevere brain injury. Another may be unawareness of sur-roundings. Establishing how family members perceivedeath is an optimal starting point for exploring organdonation.91 Religious issues are of utmost importance indiscussing brain death. Most religions, including Islam,Christianity, Judaism, and Hinduism, support organdonation as a charitable and helping act. Understandingthe religious perspectives of the family of a potentialdonor can better prepare health care providers for dis-cussions about brain death.92,93 The need for carefulchoice of words and use of the same terminology by allmembers of the health care team in discussing braindeath with patients’ families cannot be overstated.94
Care must also be taken to address nursing concernsregarding brain death. One potential barrier perceivedby nurses is lack of confidence in brain death evaluation.95
Role of Advanced Practice NursesThe role of an advanced practice nurse (APN) may
start with patient rounds, identifying patients at highrisk for brain stem herniation. Before terminal herniationsyndromes occur, an APN may expedite aggressive careto control ICP elevations and may coordinate additionaltherapeutic interventions and neurodiagnostics. An APNmay use these clinical events as teaching moments to illus-trate clinical findings and aggressive, mechanism-basedcare in controlling ICP elevations. An APN may educateand support bedside clinicians throughout a patient’scare and may facilitate preparation and provide supportduring formal brain death protocols. Coordinating andassisting with clinical examinations and neurodiagnosticstudies and facilitating appropriate clinical documenta-tion of brain death protocols as needed may also be rolesof an APN. Table 7 provides a sample checklist of com-ponents of a brain death protocol.13,22,24,26-28,36-39,42,43,46,95
APNs may also be integral to identifying and resolv-ing potential confounding factors in brain death, such asmovements associated with complex spinal reflexes orcardiogenic ventilator autotriggering. Movements inbrain death or ventilator autotriggering may initially beconsidered inconsistent with brain death. An APN mayeducate clinicians and patients’ family members that apatient with documented clinical examinations, resultsof apnea testing, and neurodiagnostic findings consistentwith brain death can experience spinal reflex movements.
42 CriticalCareNurse Vol 33, No. 6, DECEMBER 2013 www.ccnonline.org
Providing clear, consistent terminology anddefinitions and ensuring family members’understanding of brain death is paramountbefore discussing organ donation and toavoid later misunderstanding.

The nurse can point out, in real time, that these move-ments can still occur after brain death and do not
contradict a determination of death according to neurological criteria. APNs are well positioned for
www.ccnonline.org CriticalCareNurse Vol 33, No. 6, DECEMBER 2013 43
Date:
Time:
Examiner:
Confounding factors eliminated:
Body temperature (>36.0ºC-36.5ºC)
Central nervous system depressants
Severe shock state
Reversible encephalopathy
Neuromuscular blockade
Reversible severe electrolyte imbalance
Loss of consciousness/responsiveness (score of 3 on Glasgow Coma Scale)
Absent response to noxious stimuli
Absent muscle movements
Loss of brain stem reflexes
Pupils fixed, dilated, midposition
No corneal reflexes
No oculocephalic reflexes
No oculovestibular reflexes
No gag reflex
No cough reflex
Apnea test (date/results): _______________________________________________________________________________________
Initial PaCO2: ______________
Final PaCO2: ______________
Adjunctive neurodiagnostic testing:
Test: ____________________________________________
Result: ____________________________________________
Declaration of death by neurologic criteria:
Date: ______________
Time: ______________
___________________________________________________________________________________________________________Physician signature (examination 1) Date/time:
___________________________________________________________________________________________________________Physician signature (examination 2) Date/time:
Exam 1 Exam 2
Table 7 Sample checklist illustrating components of a brain death protocol

multidisciplinary collaboration with other members ofthe health care team, such as respiratory therapists, tojointly analyze ventilator waveform data and identifyand resolve cardiogenic oscillation as a cause of ventila-tor autotriggering in a brain-dead patient.
APNs are pivotal in identifying and facilitating thechanging priorities of care during and after determina-tion of brain death. Before brain death is determined,the priority is optimal neurological recovery via meas-ures such as metabolic suppression, osmotic dieresis,and judicious fluid management. After brain death hasbeen declared, if organ donation becomes the focus ofcare, an APN may facilitate care to optimize end-organperfusion, initiate hormonal resuscitation protocols,promote aggressive cardiopulmonary management, andprovide goal-directed therapy. Goal-directed therapymay include initiation of hormonal resuscitation proto-cols even before completion of brain death protocols tomanage multisystem consequences of terminal brain stemdysfunction. Hormonal resuscitation refers to adminis-tration of thyroid hormone replacement, vasopressin,and steroids to treat loss of thyroid hormone bioavail-ability, loss of antidiuretic hormone, and decreased levelsof stress hormones such as cortisol associated with ter-minal brain stem dysfunction.20
Collaboration between bedside clinicians and APNscannot be overstated. One example of collaboration isdeveloping optimal clinical surveillance of patients afterbrain injury. The bedside clinician can communicatewith the APN about patients with refractory ICP eleva-tions, and together the nurses can use critical thinkingskills to revise and implement an updated plan of care.A second example is presenting a unified approach inlanguage, message, and terminology to a patient’s familymembers. This approach will help ensure developmentof trust and therapeutic relationships between the patient’sfamily members and members of the health care team.A third example is working together to ensure that apatient’s family members understand brain death beforeorgan donation is suggested. As a result of the collabora-tion, both bedside nurses and APNs can advocate forthe needs of a patient’s family, helping ensure that allthe family members’ questions are answered and thatthe members have optimal opportunity to talk and askquestions during family meetings.
Teaching moments are a fourth example of collabo-ration between APNs and bedside clinicians. These
moments can be used to share knowledge of injury pro-gression and to establish a time line, defining the pointat which terminal brain stem herniation occurs. This col-laboration is helpful in quality management, decreasingintervals between terminal brain stem herniation andinitiation of brain death protocols and preparing staff toact as preceptors for new nurses as the nurses experiencecaring for patients with progression from brain injury toterminal herniation syndromes.
A fifth example is debriefing; that is, discussing feel-ings and clinical issues after the often intense experienceof caring for a brain-dead patient (and the patient’s fam-ily). The debriefing allows APNs and bedside cliniciansto process feelings about a particular case and to collab-orate on ways to improve future clinical managementand family care.
SummaryFuture directions in practice and research related to
brain death are multiple. One direction is toward moreuniform national or international standards for deter-mining brain death.95 Practices vary widely within coun-tries, states, and institutions, even with intervals betweenclinical examinations. In many states, a single formalneurological examination with apnea testing is sufficientfor declaration of brain death after an observation period(several hours for example) after the brain injury.26 Clearstandards would facilitate uniform protocols, includinguniform intervals for examination for determination ofdeath. Longer intervals between consecutive examinationsmay risk organ recovery because of a patient’s unstablecardiopulmonary status. Aggressive surveillance, patientadvocacy, and collaboration during all phases of care areimperative. Close attention to the needs of patients’ familymembers remains important as part of optimal caring,best practices, and empathy. CCN
Financial DisclosuresNone reported.
44 CriticalCareNurse Vol 33, No. 6, DECEMBER 2013 www.ccnonline.org
Now that you’ve read the article, create or contribute to an online discussionabout this topic using eLetters. Just visit www.ccnonline.org and select the articleyou want to comment on. In the full-text or PDF view of the article, click“Responses” in the middle column and then “Submit a response.”
To learn more about brain death in the critical care setting, read“Awakening (Mis)conceptions About Brain Death” by Savel andMunro in the American Journal of Critical Care, November2012;21:377-379. Available at www.ajcconline.org.

References1. United Network of Organ Sharing. 2012 data: spring regional meetings.
http://www.unos.org/donation/index.php?topic=data_resources.Accessed September 4, 2013.
2. Murugan R, Venkataraman R, Wahed AS, et al. Preload responsivenessis associated with increased interleukin-6 and lower organ yield frombrain-dead donors. Crit Care Med. 2009;37(8):2387-2393.
3. McKeown DW, Bonser RS, Kellum JA. Management of the heartbeatingbrain-dead organ donor. Br J Anaesth. 2012;108(suppl 1):i96-i107.
4. Salim A, Velmahos GC, Brown C, Belzberg H, Demetriades D. Aggressiveorgan donor management significantly increases the number of organsavailable for transplantation. J Trauma. 2005;58(5):991-994.
5. Arbour R. Confounding factors in brain death: cardiogenic ventilatorautotriggering and implications for organ transplantation. Intensive CritCare Nurs. 2012;28(6):321-328. doi:10.1016/j.iccn.2012.03.003.
6. Dasta JF, McLaughlin TP, Mody SH, Piech CT. Daily cost of an intensivecare unit day: the contribution of mechanical ventilation. Crit Care Med.2005;33(6):1266-1271.
7. Curtis JR, Engelberg RA, Bensink ME, Ramsay SD. End-of-life care in theICU: can we simultaneously increase quality and reduce costs? Am J RespirCrit Care Med. 2012;186(7):587-592.
8. McAdam JL, Puntillo K. Symptoms experiences by family members ofpatients in intensive care units. Am J Crit Care. 2009;18(3):200-210.
9. Matis GK, Chrysou OI, Silva D, Birblis TA. Brain death: history, updatedguidelines and unanswered questions. Inter J Neurosurg. 2012;8(1). doi:10.5580/2b52. http://archive.ispub.com/journal/the-internet-journal-of-neurosurgery/volume-8-number-1/brain-death-history-updated-guidelines-and-unanswered-questions.html#sthash.7cEf8mMN.dpbs.Accessed September 4, 2013.
10. Saviozzi A. The role of nurses in the risk management of organ and tis-sue donation. Transplant Proc. 2010;42(6):2200-2201.
11. Procaccio F, Rizzato L, Ricci A, Venettoni S, Nanni Costa A. Do “silent”brain deaths affect potential organ donation? Transplant Proc. 2010;42(6):2190-2191.
12. Hagan ME, McClean D, Falcone CA, Arrington J, Matthews D, Summe C.Attaining specific donor management goals increases number of organstransplanted per donor: a quality improvement project. Prog Transplant.2009;19(3):227-231.
13. Arbour R. Clinical management of the organ donor. AACN Clin Issues.2005;16(4):551-580.
14. Westendorp WH, Leuvenink HG, Ploeg RJ. Brain death induced renalinjury. Curr Opin Organ Transplant. 2011;16(2):151-156.
15. Harukuni I, Bhardwaj A. Mechanisms of brain injury after global cerebralischemia. Neurol Clin. 2006;24:1-21.
16. Busl KM, Greer DM. Hypoxic-ischemic brain injury: pathophysiology,neuropathology and mechanisms. NeuroRehabilitation. 2010;26(1):5-13.
17. Bugge JF. Brain death and its implications for management of thepotential organ donor. Acta Anaesthesiol Scand. 2009;53:1239-1250.
18. Shah VR. Aggressive management of multiorgan donor. Transplant Proc.2008;40:1087-1090.
19. Ullah S, Zabala L, Watkins B, Schmitz ML. Cardiac organ donor manage-ment. Perfusion. 2006;21:93-98.
20. Arbour R. Early metabolic/cellular-level resuscitation following terminalbrain stem herniation: implications for organ transplantation. AACNAdv Crit Care. 2013;24(1):59-78.
21. Naik PM, Angel LH. Special issues in the management and selection ofthe donor for lung transplantation. Semin Immunopathol. 2011;33:201-210.
22. Stevens RD, Bhardwaj A. Approach to the comatose patient. Crit CareMed. 2006;34(1):31-41.
23. Hocker S, Rabinstein AA. A clinical and investigative approach to thepatient with diminished responsiveness. Neurol Clin. 2011;29(4):739-747.
24. Young GB. Impaired consciousness and herniation syndromes. NeurolClin. 2011;29(4):765-772.
25. De Ribaupierre S. Trauma and impaired consciousness. Neurol Clin. 2011;29(4):883-902.
26. Wijdicks EFM, Varelas PN, Gronseth GS, Greer DM. Evidence-basedguideline update: determining brain death in adults. Neurology. 2010;74:1911-1918.
27. Hills TE. Brain death: a review of evidence-based guidelines. Nursing.2010;40(12):34-40.
28. Bader MK, Littlejohns LR, eds. AANN Core Curriculum for NeuroscienceNursing. 5th ed. Glenview, IL: American Association of NeuroscienceNurses; 2010.
29. Sullivan R, Hodgman MJ, Kao L, Tormoehlen LM. Baclofen overdosemimicking brain death. Clin Toxicol. 2012;50(2):141-144.
30. Auinger K, Müller V, Rudiger A, Maggiorini M. Valproic acid intoxicationimitating brain death. Am J Emerg Med. 2009;27(9):1177.e5-1177.e6.
31. John J, Gane BD, Plakkal N, Aghoram R, Sampath S. Snake bite mimick-ing brain death. Cases J. 2008;12;1(1):16.
32. Samaniego EA, Mylnash M, Caulfield AF, Eyngorn I, Wijman CA. Sedationconfounds outcome prediction in cardiac arrest survivors treated withhypothermia. Neurocrit Care. 2011;15(1):113-119.
33. Bernard V, Van Pesch V, Hantson P. Guillain-Barré syndrome mimickingbrain death pattern: a poorly reversible condition. Acta Neurol Belg.2010;110(1):93-96.
34. Yannopoulos D, Kotsifas K, Aufderheide TP, Lurie KG. Cardiac arrest,mild therapeutic hypothermia and unanticipated cerebral recovery. Neu-rologist. 2007;13(6):369-375.
35. Webb AC, Samuels OB. Reversible brain death after cardiopulmonaryarrest and induced hypothermia. Crit Care Med. 2011;39(6):1538-1542.
36. Morenski JD, Oro JJ, Tobias JD, Singh A. Determination of death by neu-rological criteria. J Intensive Care Med. 2003;18(4):211-221.
37. Henneman EA, Karras GE. Determining brain death in adults: a guide-line for use in critical care. Crit Care Nurse. 2004;24(5):50-56.
38. Wijdicks EFM. The diagnosis of brain death. N Engl J Med. 2001;344(16):1215-1221.
39. Scott JB, Gentile MA, Bennett SN, Couture M, Macintyre NR. Apnea test-ing during brain death assessment: a review of clinical practice and pub-lished literature. Respir Care. 2013;58(3):532-538.
40. Wijdicks EF, Rabinstein AA, Manno EM, Atkinson JD. Pronouncing braindeath: contemporary practice and safety of the apnea test. Neurology.2008;71(16):1240-1244.
41. Lang CJG, Heckmann JG. Apnea testing for the diagnosis of brain death.Acta Neurol Scand. 2005;112:358-369
42. Arbour R. Cardiogenic oscillation and ventilator autotriggering in brain-dead patients: a case series. Am J Crit Care. 2009;18(5):496, 488-495.
43. Heran MK, Heran NS, Shemie SD. A review of ancillary tests in evaluat-ing brain death. Can J Neurol Sci. 2008;35(4):409-419.
44. Zuckier LS, Kolano J. Radionuclide studies in the determination of brain death:criteria, concepts and controversies. Semin Nucl Med. 2008;38(4): 262-273.
45. Sinha P, Conrad GR. Scintigraphic confirmation of brain death. SeminNucl Med. 2012;42(1):27-32.
46. Baron L, Shemie SD, Teitelbaum J, Doig CJ. Brief review: history, conceptand controversies in the neurological determination of death. Can J Anaesth.2006;53(6):602-608.
47. Flowers WM, Patel BR. Persistence of cerebral blood flow after brain death.South Med J. 2000;93(4):364-367.
48. Saqqur M, Zygun D, Demchuk A. Role of transcranial Doppler in neuro-critical care. Crit Care Med. 2007;35(5):S216-S223.
49. Dosemeci L, Dora B, Yilmaz M, et al. Utility of transcranial Dopplerultrasonography for confirmatory diagnosis of brain death: two sides ofthe coin. Transplantation. 2004;77(1):71-75.
50. Poularas J, Karakitsos D, Kouraklis G, et al. Comparison between tran-scranial color Doppler ultrasonography and angiography in the confir-mation of brain death. Transplant Proc. 2006;38:1213-1217.
51. Monteiro LM, Bollen CW, van Huffelen AC, Ackerstaff RG, Jansen NJ,van Vught AJ. Transcranial Doppler ultrasonography to confirm braindeath: a meta-analysis. Intensive Care Med. 2006;32:1937-1944.
52. Vincenzini E, Pro S, Randi F. Transcranial Doppler for brain death afterdecompressive craniectomy: persistence of cerebral blood flow with flatEEG. Intensive Care Med. 2010;36:2163-2164.
53. Frampas E, Videcoq M, de Kerviler E, et al. CT angiography for braindeath diagnosis. AJNR Am J Neuroradiol. 2009;30(8):1566-1570.
54. Combes JC, Chomel A, Ricolfi F, d’Athis P, Freysz M. Reliability of com-puted tomographic angiography in the diagnosis of brain death. Trans-plant Proc. 2007;39:16-20.
55. Berenguer CM, Davis FE, Howington JU. Brain death confirmation: com-parison of computed tomographic angiography with nuclear medicineperfusion scan. J Trauma. 2010;68(3):553-559.
56. Greer DM, Strozyk D, Schwamm LH. False-positive CT angiography inbrain death. Neurocrit Care. 2009;11:272-275.
57. Joffe AR, Anton N, Blacvkwood J. Brain death and the cervical spinal cord: aconfounding factor in the clinical examination. Spinal Cord. 2010;48:2-9.
58. Saposnik G, Bueri JA, Maurino J, Saizar R, Garretto NS. Spontaneousand reflex movements in brain death. Neurology. 2000;54:221-223.
59. Saposnik G, Maurino J, Saizar R, Bueri JA. Undulating toe movements inbrain death. Eur J Neurol. 2004;11:723-727.
60. Jain S, DeGeorgia M. Brain death-associated reflexes and automatisms.Neurocrit Care. 2005;3:122-126.
61. De Freitas GR, Lima MASD, André C. Complex spinal reflexes duringtranscranial Doppler ultrasound examination for the confirmation ofbrain death. Acta Neurol Scand. 2003;108:170-173.
62. Saposnik G, Basile VS, Young GB. Movements in brain death: a systematicreview. Can J Neurol Sci. 2009;36:154-160.
www.ccnonline.org CriticalCareNurse Vol 33, No. 6, DECEMBER 2013 45

63. Beckmann YY, Ciftci Y, Secil Y, Eren S. Fasciculations in brain death.Crit Care Med. 2010;38(12):2377-2378.
64. Dodd-Sullivan R, Quirin J, Newhart J. Ventilator autotriggering: a cautionin brain death diagnosis. Prog Transplant. 2011;21:152-155.
65. Shoham AB, Patel B, Arabia FA, Murray MJ. Mechanical ventilation andthe total artificial heart: optimal ventilator trigger to avoid post-operativeautocycling—a case series and literature review. J Cardiothorac Surg. 2010;5:39. http://www.cardiothoracicsurgery.org/content/5/1/39. AccessedSeptember 5, 2013.
66. Gupta D, Duke JC, Rubens A, Orlewicz M. Intra-aortic balloon pumpdeflation generated suction-like forward aortic blood flow and auto-triggering of a flow-triggered mechanical ventilator. WebmedCentralCritical Care. 2012;3(1):WMC002854. http://www.webmedcentral.com/article_view/2854. Accessed September 5, 2013.
67. Imanaka H, Nishimura M, Takeuchi M, Kimball WR, Yahagi N, Kumon K.Autotriggering caused by cardiogenic oscillation during flow-triggeredmechanical ventilation. Crit Care Med. 2000;28(2):402-407.
68. Edwards Lifesciences. Normal hemodynamic parameters and labora-tory values: stroke volume. http://ht.edwards.com/scin/edwards/sitecollectionimages/edwards/products/presep/ar05688_parameters.pdf.
69. Carlsson M, Cain P, Holmqvist C, Stahlberg F, Lundback S, Arheden H.Total heart volume variation throughout the cardiac cycle. Am J PhysiolHeart Circ Physiol. 2004;287(1):H243-H250.
70. Ugander M, Jense E, Arheden H. Pulmonary intravascular blood volumechanges through the cardiac cycle in healthy volunteers studied by car-diovascular magnetic resonance measurements of arterial and venousflow. J Cardiovasc Magn Reson. 2009;11:42. http://www.jcmr-online.com/content/11/1/42. Accessed September 5, 2013.
71. Tusman G, Suarez-Sipman F, Peces-Barba G, Climente C, Areta MA.Pulmonary blood flow generates cardiogenic oscillations. Respir PhysiolNeurobiol. 2009;167(3):247-254.
72. Holzer M. Targeted temperature management for comatose survivorsof cardiac arrest. N Engl J Med. 2010;363:1256-1264.
73. Hypothermia After Cardiac Arrest Study Group. Mild therapeutic hypother-mia to improve the neurologic outcome after cardiac arrest [publishedcorrection appears in N Engl J Med. 2002;346(22):1756]. N Engl J Med.2002;346(8):549-556.
74. Bernard SA, Gray TW, Buist MD, et al. Treatment of comatose survivorsof out-of-hospital cardiac arrest with induced hypothermia. N Engl J Med.2002;346(8):557-563.
75. Lee WM, Stravitz RT, Larson AM. Introduction to the revised AmericanAssociation for the Study of Liver Diseases position paper on acute liverfailure 2011. Hepatology. 2012;55(3):965-967.
76. Mpabanzi L, Jalan R. Neurological complications of acute liver failure:pathophysiological basis of current management and emerging therapies.Neurochem Int. 2012;60(7):736-742.
77. Pathikonda M, Munoz SJ. Concise review: acute liver failure. Ann Hepatol.2010;9(1):7-14.
78. Kramer C, Freeman WD, Larson JS, et al. Therapeutic hypothermia forsevere traumatic brain injury: a critically appraised topic. Neurologist.2012;18(3):173-177.
79. Sadaka F, Veremakis C. Therapeutic hypothermia for the managementof intracranial hypertension in severe traumatic brain injury: a system-atic review. Brain Inj. 2012;26(7-8):899-908.
80. Jiang J. Clinical study of mild hypothermia treatment for severe traumaticbrain injury. J Neurotrauma. 2009;26:399-406.
81. Meyer MJ, Megyesi J, Meythaler J, et al. Acute management of acquiredbrain injury, I: an evidence-based review of non-pharmacological inter-ventions. Brain Inj. 2010;24(5):694-705.
82. Faridar A, Bershad EM, Emiru T, Iaizzo PA, Suarez JI, Divani AA. Ther-apeutic hypothermia in stroke and traumatic brain injury. Front Neurol.2011;2:80. doi:10.3389/fneur.2011.00080.
83. Blondin NA, Greer DM. Neurologic prognosis in cardiac arrest patientstreated with therapeutic hypothermia. Neurologist. 2011;17:241-248.
84. Bouwes A, Binnekade JM, Kuiper MA, et al. Prognosis of coma aftertherapeutic hypothermia: a prospective cohort study. Ann Neurol. 2012;7(2):206-212.
85. Perman SM, Kirkpatrick JN, Reitsma AM, et al. Timing of neuroprog-nostication in postcardiac arrest therapeutic hypothermia. Crit Care Med.2012;40(3):719-724.
86. Rossetti AO, Oddo M, Logroscino G, Kaplan PW. Prognostication aftercardiac arrest and hypothermia: a prospective study. Ann Neurol. 2010;67:301-307.
87. Ashwal S, Serna-Fonseca T. Brain death in infants and children. Crit CareNurse. 2006;26(2):117-128.
88. Verheijde JL, Rady MY, McGregor JL. Growing concerns about braindeath and organ donation. Indian Pediatr. 2008;45(11):883-888.
89. Murthy TVSP. Organ donation: intensive care issues in managing braindead. Med J Armed Forces India. 2009;65(2):155-160.
90. Truog RD, Robinson WM. Role of brain death and the dead-donor rule inthe ethics of organ transplantation. Crit Care Med. 2003;31(9):2391-2396.
91. Long T, Sque M, Addington-Hall J. What does a diagnosis of brain deathmean to family members approached about organ donation? A reviewof the literature. Prog Transplant. 2008;18(2):118-126.
92. Oliver M, Woywodt A, Ahmed A, Saif I. Organ donation, transplantationand religion. Nephrol Dial Transplant. 2011;26:437-444.
93. Arbour R. Al Ghamdi HMS, Peters L. Islam, brain death and transplan-tation: culture, faith and jurisprudence. AACN Adv Crit Care. 2012;23(4):381-394.
94. Savel RH, Munro CL. Awakening (mis)conceptions about brain death.Am J Crit Care. 2012;21(6):377-379.
95. Floden A, Persson LO, Rizell M, Sanner M, Forsberg A. Attitudes to organdonation among Swedish ICU nurses. J Clin Nurs. 2011;20(21-22):3183-3195.
96. Scripko PD, Greer DM. An update on brain death criteria a simplealgorithm with complex questions. Neurologist. 2011;17:237-240.
46 CriticalCareNurse Vol 33, No. 6, DECEMBER 2013 www.ccnonline.org

CCN Fast FactsBrain Death: Assessment, Controversy,
and Confounding Factors
CriticalCareNurseThe journal for high acuity, progressive, and critical care nursing
Table Factors that may mimic brain death
Locked-in syndrome
Fulminant Guillain-Barré syndrome
Severe hypothermia
Post–cardiac arrest syndrome
Massive baclofen/anticholinergic overdose
Severe overdose of central nervous system depressants
Massive overdose of valproic acid
Massive overdose of tricyclic antidepressants
Severe snake envenomation
www.ccnonline.org CriticalCareNurse Vol 33, No. 6, DECEMBER 2013 47
Arbour RB. Brain Death: Assessment, Controversy, and Confounding Factors. Critical Care Nurse. 2013;33(6):27-48.
• If apnea testing is not tolerated by the patient, theresults are inconclusive, or shorter intervals are requiredbetween initiation and completion of a brain death proto-col, ancillary neurodiagnostic may be appropriate, includ-ing 4-vessel cerebral angiography, radionuclide cerebralperfusion scan, and electroencephalography as well as tran-scranial Doppler ultrasound and computed tomographicangiography.
• Patients’ movements in brain death may be confound-ing factors in clinical evaluation. Possible confounding fac-tors include spinal cord injury, movements in brain death(complex spinal reflexes, ventilator autotriggering), thera-peutic hypothermia, and transient brain stem depressionafter cardiopulmonary arrest.
• Goals of frequent neurological assessments of patientswith brain injury include identifying injury progression,detecting stabilized neurological status or response to ther-apy, and rapidly determining and acting on opportunitiesfor intervention before brain herniation syndromes occur.
• Allowing time and resources, including spiritual sup-port or chaplains, when formal brain death protocols arebeing initiated gives a patient’s family members an opportu-nity to process their experiences.
• When brain injury is refractory to aggressive manage-ment to control the consequences of injury and the patientprogresses toward brain death, empathy and honesty areimportant in communicating this decline to the patient’sfamily members.
• Bedside clinicians must maintain frequent monitor-ing, begin preparatory steps for clinical examinations calledfor in a brain death protocol, and facilitate safe transportfor neurodiagnostic studies as appropriate.
• Future directions in practice and research related tobrain death are multiple. One direction is toward more uni-form national or international standards for determiningbrain death. Clear standards would facilitate uniform proto-cols, including uniform intervals for examination for deter-mination of death. Longer intervals between consecutiveexaminations may risk organ recovery because of a patient’sunstable cardiopulmonary status. CCN
Facts• Lack of consciousness and unresponsiveness to nox-
ious stimuli reflect severe brain dysfunction above thebrain stem. Assessment of consciousness may be doneinitially by using the Glasgow Coma Scale. A score of 3(no eye opening, verbal response, or movement eitherspontaneously or in response to stimulation) indicatescomplete loss of consciousness or responsiveness.
• Radiological or clinical evidence of nonsurvivablebrain injury must be documented. Potentially reversiblecauses of apparent marked depression of consciousnessor responsiveness and clinical states that may mimicbrain death (see Table) must be ruled out.
• Brain stem function is determined by assessingpupil size and reactivity and reflexes mediated by thebrain stem, including oculocephalic, oculovestibular,corneal, cough, and gag reflexes.
• Apnea testing is performed after the cause of coma,unresponsiveness, and lack of brain stem reflexes is estab-lished. The results of apnea testing are used to formallydocument PaCO2 unresponsiveness as indicated by eleva-tion of PaCO2 to prescribed thresholds and the absence ofintrinsic respiratory drive.
• Apnea testing involves disconnecting the ventilatorand inserting a catheter into the patient’s carina for insuf-flation of 100% oxygen.