Embed Size (px)
Citation preview

Cancer Stem Cells in Brain Tumor Biology
Jeremy N. Rich and Christine E. EylerDepartment of Stem Cell Biology and Regenerative Medicine, Cleveland Clinic, Cleveland, OH44195 USA. Departments of Medicine, Surgery, Pharmacology and Cancer Biology; Preston RobertTisch Brain Tumor Center; Duke University Medical Center, Durham, NC 27710
AbstractTumors are aberrant organ systems containing a complex interplay between the neoplasticcompartment and recruited vascular, inflammatory, and stromal elements. Further, most cancersdisplay a hierarchy of differentiation states within the tumor cell population. Molecular signals thatdrive tumor formation and maintenance commonly overlap with those involved in normaldevelopment and wound responses – two processes in which normal stem cells function. It is thereforenot surprising that cancers invoke stem cell programs that promote tumor malignancy. Stem cell-likecancer cells (or cancer stem cells) need not be derived from normal stem cells but may be subjectedto evolutionary pressures that select for the capacity to self renew extensively or differentiatedepending on conditions. Current cancer model systems may not fully recapitulate the cellularcomplexity of cancers, perhaps partially explaining the lack of power of these models in predictingclinical outcomes. New methods are enabling researchers to identify and characterize cancer stemcells. Our laboratory focuses on the roles of brain tumor stem cells in clinically relevant tumorbiology, including therapeutic resistance, angiogenesis, and invasion/metastasis. We hope that thesestudies will translate into improved diagnostic, prognostic, and therapeutic approaches for these lethalcancers.
INTRODUCTIONPrimary brain tumors comprise a large family of cancers (>160 types according to the WorldHealth Organization (WHO)) (Furnari et al. 2007). The most common primary intrinsic braintumors are the gliomas for adults and medulloblastomas for children. Gliomas are defined bytheir morphologic and marker similarities to the glia, or supporting cells of the brain, thatinclude astrocytes and oligodendrocytes, and are named astrocytomas or oligodendrogliomas(N.B. ependymomas may be included as a glial tumor but display very different biologicalbehavior so are commonly considered separately). Gliomas are graded by histologic criteriathat include the presence of mitoses, aberrant nuclear or cytoplasmic morphology, glomeruloidangiogenesis, and necrosis according to a WHO system from grades I to IV with increasingmalignancy. Grade III gliomas (anaplastic astrocytoma or anaplastic astrocyoma) and gradeIV gliomas (glioblastoma multiforme) are the most common and lethal of the gliomas and aretreated in a similar manner. Standard of care for malignant gliomas (grade III and IV gliomas)consists of maximal surgical resection followed by external beam radiation with concurrentchemotherapy (the oral methylator temozolomide) then adjuvant temozolomide chemotherapy(Stupp et al. 2005). Unfortunately, tumor recurrence is essentially universal and no therapieshave clear benefit in improving the survival of patients experiencing tumor recurrence orprogression. The median survival for glioblastoma patients remains only 15 months. Theoutcome for children diagnosed with medulloblastoma is relatively better than for adults withglioblastoma but even long term survivors commonly suffer long term disability, including
Correspondence to Jeremy N. Rich, [email protected], Tel: 216-636-0790, Fax: 216-636-5454.
NIH Public AccessAuthor ManuscriptCold Spring Harb Symp Quant Biol. Author manuscript; available in PMC 2010 March 27.
Published in final edited form as:Cold Spring Harb Symp Quant Biol. 2008 ; 73: 411. doi:10.1101/sqb.2008.73.060.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

decreased intelligence. In fact, since the recent improvements in treating childhood leukemias,brain tumors are now the most common cause of pediatric cancer deaths. Thus, brain tumorspresent a severe clinical challenge with the overall survival of patients changing little in 30years.
This paper will serve to highlight the work of the Rich laboratory within the context of thefield. As a number of laboratories share a similar research focus, this discussion representsonly a small fraction of the work in the field and contains opinions of the author that may differfrom other researchers.
Cancer Stem Cells in Brain TumorsCancers are not simple collections of homogeneous neoplastic cells. Instead, a tumor is anorgan system comprised of a neoplastic compartment with associated vasculature,inflammatory cells, and reactive cellular and extracellular components (Reya et al. 2001).Bailey and Cushing long ago recognized that brain cancers display striking morphologicvariation, as evidenced by the term glioblastoma multiforme. Glial tumors often contain mixedsubpopulations that morphologically resemble astrocytes and oligodendrocytes, leading to anintermediate diagnosis of oligoastrocytomas in the WHO classification system. Geneticanalysis has additionally demonstrated that chromosomal aberrations and gene expression varyregionally within the tumor (Fulci et al. 2002). Regional variance is also evident in thecommonly observed mixed clinical responses detected for specific therapies in which part ofthe tumor may be responsive to a therapy whereas other areas fail to respond (Pope et al.2006). Differentiation markers have been assessed in human brain tumors and demonstrate thataberrant and multiple states of differentiation may be present in the same tumor. Ourunderstanding of the normal development of the nervous system has dramatically increased inrecent years. The nervous system has a complex differentiation hierarchy ranging from a neuralstem cell that can give rise to all of the major lineages in the brain parenchyma (primarilyneurons, astrocytes, and oligodendrocytes) to lineage committed progenitors that have a morerestricted differentiation potential to terminally differentiated cells (Uchida et al. 2000; Rietzeet al. 2001; Sanai et al. 2004) (Figure 1). The recognition of the importance of differentiationstate and the role of neural stem cells in development and wound responses (two processes thatare recapitulated in carcinogenesis) has prompted the application of neural stem cell biologyto neuro-oncology. Stem cell concepts can influence the understanding of brain cancer in twoprominent areas: tumor origin and maintenance. The cell-of-origin for brain tumors isunresolved with genetic models supporting either a stem cell origin or a dedifferentiatedcommitted cell of origin with even more recent evidence suggesting a potential dual originwith a common final morphology (reviewed in Furnari et al. 2007). No less controversial, thecancer stem cell hypothesis proposes that established tumors consist of a cellular hierarchywith a subpopulation of tumor cells able to maintain and propagate the tumor. Two competingmodels have been proposed: a stochastic model in which any cell within the tumor has an equalchance of growth based on the genetic phenotype of the cell, and the hierarchical model inwhich a subset of the neoplastic cells can maintain tumor growth indefinitely (Reya et al.2001). The initial identification of a cancer stem cell occurred in leukemia (Lapidot et al.1994; Bonnet and Dick 1997) but similar identifications in multiple systemic cancer types havefollowed (Al-Hajj et al. 2003; Hope et al. 2004; Li et al. 2007; O’Brien et al. 2007; Ricci-Vitiani et al. 2007; Dalerba et al. 2007). Cancer stem cells displaying these properties havebeen isolated from the major types of brain tumor including gliomas, medulloblastomas, andependymomas (Ignatova et al. 2002; Hemmati et al. 2003; Singh et al. 2003; Galli et al.2004; Singh et al. 2004; Yuan et al. 2004; Taylor et al. 2005) (Figure 2). Several issues havecontributed to the controversies surrounding the cancer stem cell hypothesis. These include:1) evidence that some cancers or some tumor models do not display a recognizable hierarchy(Quintana et al. 2008), 2) lack of universal markers that identify cancer stem cells and 3)
Rich and Eyler Page 2
Cold Spring Harb Symp Quant Biol. Author manuscript; available in PMC 2010 March 27.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

confusion over the implications of the cancer stem cell hypothesis in terms of the rarity ofcancer stem cells (Kelly et al. 2008) and implications as to the cell-of-origin. The cancer stemcell hypothesis does not require a rare cancer stem cell nor does it require a stem cell originfor tumors (Clarke et al. 2006). It is unlikely that stem cell biology will explain the entirety ofbrain tumor biology, but it is increasingly evident that stem cell signal transduction pathwaysare commonly dysregulated in brain tumors and that a tumor population can be commonlyderived from human brain tumor surgical specimens that exhibit characteristics similar tonormal stem cells. The acceptance of a cancer stem cell model is not mutually exclusive witha stochastic model of tumor initiation and maintenance that has been the leading paradigm incancer biology for years but it appears probable that these systems may be used in complementto inform research.
Defining Brain Tumor Stem CellsThere is no current agreement as to the definition of a normal stem cell beyond long termrenewal and differentiation potential so it is of little surprise that there is limited consensusregarding the defining characteristics of cancer stem cells. The current definition of a cancerstem cell requires self renewal, sustained proliferation, and tumor initiation/propagation(Clarke et al. 2006). As the stem cell-like populations are defined in functional assays, someinvestigators have selected a nomenclature to represent the ability to propagate tumors butthese terms fail to communicate that core characteristics may be shared between these tumorcells and normal stem cells (markers, signal transduction pathways, self renewal capacity, etc.).
Normal stem cells commonly express specific antigens that permit prospective enrichment ofcells that fulfill stem cell criteria, but no antigenic profile (the immunophenotype) is absolutelyrepresentative of a stem cell. Thus, we lack the ability to directly assess the creation of a perfectcopy of a cell in real time. Rather, stem cell assays validate that a cell capable of self renewalmust have been present at an earlier step. Stem cells have developmentally regulated replicationthat can be either symmetric (yielding two identical cells – either two stem or two differentiateddaughter cells) or asymmetric (giving rise to one differentiated and one undifferentiateddaughter cell) in response to cell state and external cues. Measuring the differentiation statusof a cell in a single division presents significant challenges to score a division as symmetric orasymmetric. To date, the current techniques have included the measurement of polarizedproteins, including Notch (Wu et al. 2007), but current techniques cannot verify in real timethat a daughter cell has not undergone differentiation. The gold standard for defining an adultstem cell remains the generation of the full cellular constituents of the relevant organ from asingle stem cell. For the nervous system, the ability to form neurons, astrocytes, andoligodendrocytes is required of normal neural stem cells. The differentiation cascade for thehematopoietic system is by far the best characterized but the nervous system is increasinglywell modeled. In cell culture systems without serum, neural progenitors may form threedimensional structures that do not adhere to the culture surface, called neurospheres. Thesecomplex structures tend to have the least differentiated cellular populations located on thesurface of the sphere with expression of differentiation markers more commonly occurring oncells in the interior. Complex neuronal processes may be formed in these structures, and somecorrelation of similar structures in the breast (mammospheres) has permitted an assessment ofself renewal through the serial passage of the spheres from single cells and proliferation fromthe size of the generated spheres. However, caution must be exercised in interpreting thesignificance of neurosphere generation (Singec et al. 2006). First, spheres may be generatedfrom cells that were incompletely disaggregated with residual cohesive cells. Second, spheresmay form and “grow” through the fusion of smaller structures that may be present at highercellular densities. In addition, neurospheres are cell culture artifacts that do not have in vivocorrelates. Finally, not all cells within a neurosphere have an undifferentiated state (in fact,stem-like cells are often a small minority) and even committed progenitors may be able to form
Rich and Eyler Page 3
Cold Spring Harb Symp Quant Biol. Author manuscript; available in PMC 2010 March 27.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

a neurosphere. Thus, the presence of a neurosphere does not prove the presence of a stem cellin normal physiology.
Within the field of cancer stem cell biology, the current state of understanding has led to highvariability in the rigor with which validation of the stem cell nature of a cellular population isapproached. Many groups have simply used the presence of a stem cell marker or neurospheregeneration as an indication of a cancer stem cell. This is inadequate and these studies maycreate difficulty in a field already confusing and controversial. The requirements andchallenges in the identification of a cancer stem cell are similar to those of normal stem cells.Two main approaches have been employed to date. In the first, tumors are disaggregated andcultured in serum free media until tumor spheres form (Ignatova et al. 2002; Hemmati et al.2003; Galli et al. 2004; Yuan et al. 2004). These spheres are sequentially passaged to confirmsustained self renewal. The advantage of this system is that it includes an important (ifchallenging) functional assay at the initial characterization. There are weaknesses, however,as the neurospheres are still mixed populations that represent only a small fraction of theoriginal tumor. The underlying heterogeneity will, by definition, be lost. While neurospherescan be subjected to differentiation conditions, it is unclear if these conditions are fullyrepresentative of the diversity of cellular populations in the original tumor. In addition, serialneurosphere passage requires extended periods of cell culture which can rapidly (even inminutes) induce significant alterations in cellular biology and gene expression. Therefore, therehas been a strong effort to identify cell surface antigens that can be used to prospectively enrichcancer stem cells from tumor populations immediately upon surgical resection (Singh et al.2003; Singh et al. 2004). Although several markers may be informative in brain tumor stemcell identification (e.g. Prominin-1 (CD133), CD15 (SSEA-1, Lewis × structure (Lex)), A2B5,BMI1, Nestin, Sox2, Musashi1), there are significant deficiencies with the current availablemarkers. In our own studies, markers are only reliably useful in segregating tumor initiationpotential after immediate derivation from an in vivo environment suggesting that markerexpression in cancer stem cells requires interactions with the micronenvironment. In summary,the current methods for enrichment for cancer stem cells remain imperfect and will requireimprovements.
The gold standard for cancer stem cells remains tumor propagation. The current preferred assayis the in vivo limiting dilution assay in which progressively smaller numbers of tumor cells areimplanted in an orthotopic location to demonstrate the minimal number of cells required toform tumors (Singh et al. 2004). Presumably, the number of cells represents a surrogate for thefrequency of true cancer stem cells. However, it is possible that for solid cancers that sometumors will require more than one cell to initiate tumor growth of even pure cancer stem cellpopulations. An ideal result would be to have single tumor cells demonstrate the capacity toform a tumor and give rise to daughter cells that share this characteristic (Quintana et al.2008). To date, the brain tumor field has not seen reports of this efficiency but rather have acellular requirement of 100–1000 from human surgical biopsy specimens (Singh et al. 2004;Bao et al. 2006b). Regardless, the requirement for in vivo tumor propagation is absolute. Themany studies that assess solely tumor sphere formation or expression of a cancer stem cellmarker cannot be considered to have demonstrated the presence of cancer stem cells and maydetract from the field.
An unresolved question in the solid tumor cancer stem cell field revolves around theproliferative rate of cancer stem cells. Normal stem cells and leukemic stem cells share theability to proliferate over the long term but are quiescent in normal conditions. In ex vivostudies, brain tumor stem cells are apparently proliferative but this may represent a responseto culture conditions. Preliminary studies of brain tumor specimens have suggested that tumorscontain cells that co-express cancer stem cell and proliferative markers, but the ability to
Rich and Eyler Page 4
Cold Spring Harb Symp Quant Biol. Author manuscript; available in PMC 2010 March 27.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

differentiate a stem cell population from a transit amplifying/committed progenitor populationremains unreported.
The cancer stem cell hypothesis has engendered criticism due to the lack of clarity in theterminology. Many researchers and the lay public assume that a cancer stem cell is derivedfrom a normal stem cell. Conceptually, brain tumors may be derived from neural stem cells,transit amplifying cells, or terminally differentiated cells. A stem cell cell-of-origin is anattractive hypothesis since the long life of these cells would permit the accumulation of geneticand epigenetic alterations required for transformation. In addition, many characteristics ofnormal neural stem cells are similar to characteristics of cells in high grade brain tumors(including diversity of cell populations, high migratory potential, and sustained proliferation).Several genetically engineered brain tumor models suggest that neural stem cells may betransformed with restricted oncogenic stimuli (reviewed in Furnari et al. 2007). However, othermodels support a potential for dedifferentiation of more differentiated cells in tumororigination. Very recently, two groups in parallel have demonstrated that identical tumors(medulloblastomas) can be derived from different cells of origin with identical geneticalterations strongly supporting a model in which cancers that display similar morphologiesmay be derived from different starting points (Schüller et al. 2008; Yang et al. 2008a). It islikely that no single rule may be applied to the originating cell for a single cancer.
Derivation of Brain Tumor Stem CellsOur approach in cancer stem cell derivation has been built on the seminal studies by the Dirkslaboratory that were in turn based on protocols for neural stem cell derivation (Singh et al.2003; Singh et al. 2004). We have used tumor sources of human surgical biopsy specimensimmediately collected after resection and tumor xenografts maintained in an in vivoenvironment. We disaggregate these tumors and then prospectively sort for a single cell surfacemarker, Prominin-1 (Cluster of differentiation 133 (CD133)), which is the most developedbrain tumor stem cell marker. Prominin-1 is a pentaspan transmembrane glycoprotein locatedon cellular protrusions that was originally identified separately through the development ofantibodies against the mouse neuroepithelium (Weigmann et al. 1997) and CD34bright
hematopoietic stem and progenitor cells derived from human fetal liver and bone marrow andblood (Yin et al. 1997; Miraglia et al. 1997). The function of Prominin-1 is unknown butmutations in Prominin-1 are detected in patients with familiar macular degeneration and disruptphotoreceptor disk morphogenesis in a genetic mouse model (Yang et al. 2008b).
CD133 was first used to enrich tumor repopulating cells in leukemia (Horn et al. 1999; Bühringet al. 1999) and informed prognosis (Lee et al. 2001). Based on its expression on neural stem/progenitor cells, CD133 was investigated as a brain tumor stem cell marker. In seminal studiesfirst performed in vitro and then in vivo, brain tumor stem cells were exclusively detected inCD133+ cells from gliomas and medulloblastomas (Singh et al. 2003; Singh et al. 2004).Tumor-derived neurospheres from pediatric brain tumors also express CD133 and other stemcell markers (Sox2, Musashi-1, Bmi-1, maternal embryonic leucine zipper kinase, andphosphoserine phosphatase) (Hemmati et al. 2003). The CD133 marker is not absolute but hasproven useful for the majority of tumors in our hands. The primary advantage to this approachis that the cellular heterogeneity that is the core of the cancer stem cell hypothesis is maintained.The cells that are collected are then cultured in appropriate media – stem cell populations aregrown in defined media with growth factors (Lee et al. 2006) but without serum whereas non-stem cell populations are maintained in serum. Under these conditions, the cancer stem cellswill tend to form neurosphere-like structures while non-stem cells will grow as adherent cells.We have found that the cells in both populations rapidly accumulate changes in gene expressionand genetic markers when cultured suggesting that characterization of cancer stem cells andtheir matched non-stem cell brethren should be performed at low passage number. Even this
Rich and Eyler Page 5
Cold Spring Harb Symp Quant Biol. Author manuscript; available in PMC 2010 March 27.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

caveat is likely inadequate as phosphorylated proteins become altered within minutes afterculturing but our current technologies do not permit a perfect system to maintain the originalcellular phenotype. Even in the earliest reports using CD133, the investigators recognizedvariation between tumors in marker expression. CD133 is also informative in ependymomasin conjunction with other markers (Nestin and BLBP) (Taylor et al. 2005). Many reports haveconfirmed the utility of CD133 in prospective isolation of brain tumor stem cells (Bao et al.2006a; Bao et al. 2006b; Piccirillo et al. 2006; Calabrese et al. 2007; Bao et al. 2008) andCD133 has proven useful in a number of other solid cancers, including colorectal cancers(O’Brien et al. 2007; Ricci-Vitiani et al. 2007). However, challenges to the universal expressionof CD133 have been raised and some tumors have tumor propagating potential withoutsignificant numbers of CD133+ cells (Beier et al. 2007). Interestingly, primary glioblastomashave much higher levels of CD133+ cells than recurrent tumors. The difficulties with CD133are multiple. The AC133 reagents (monoclonal antibodies against the CD133 glycoprotein)are challenging to use (Bidlingmaier et al. 2008). In flow cytometry assays, CD133+ peaks arenot fully separated from isotype antibody control peaks in most tumor preparations. Withouta clear separation, CD133− and CD133+ populations cannot be clearly delineated and requirefunctional validation. The precise methodologies used to disaggregate tissues and purifycellular populations can have profound effects on CD133 fractions (Panchision et al. 2007).Cell culture conditions are important to maintain appropriate tumor stem cell populations (Leeet al. 2006) but direct transfer to an in vivo environment may be optimal to preservation of aCD133+ tumor cell fraction (Shu et al. 2008). CD133 is not a static gene product but is a targetof promoter methylation alterations in cancers (Tabu et al. 2008; Yi et al. 2008) and may beregulated during the cell cycle (Jaksch et al. 2008). The complexity of these conditions hastranslated into the common use of very small numbers of tumor specimens in even high impactreports. It is almost certainly the case, however, that morphologically identical brain tumorshave underlying complex cellular differences due to different cell-of-origin or oncogenicchanges that are represented with different brain tumor stem cells that may express differentmarker immunophenotypes.
The Significance of Brain Tumor Stem Cells in Neuro-oncologyThough it may appear that the cancer stem cell hypothesis is merely an academic exercise ora laboratory phenomenon, one cannot deny the near total failure in the development of therapiesto improve the outcomes of brain cancer patients using traditional laboratory investigativeapproaches. The use of temozolomide has been hailed as a tremendous advance in the treatmentof malignant gliomas, but the benefit has been limited to less than three months of improvedmedian survival for glioblastoma patients (Stupp et al. 2005). Not only has the geneticknowledge of brain tumor biology been inadequate to drive new effective therapies, but theadvanced imaging technologies still are unreliable in early tumor detection and prediction ofthe most important outcome, survival. The heterogeneity of brain cancers may be helpful inexplaining many of our failures. To date, no direct proof of a role for cancer stem cells in braintumor clinical trials has been reported but several studies have examined the expression ofcancer stem cell marker positive cells in clinical brain tumor biopsy specimens.
CD133 immunohistochemistry of brain tumor specimens has shown variability in utility, likelydue to the combination of tumor heterogeneity and reagent specificity. CD133+ cells reside ina perivascular niche of tumors (Bao et al. 2006a; Calabrese et al. 2007; Christensen et al.2008). Analysis of CD133 and proliferation has not demonstrated consistent relationships todate (Christensen et al. 2008; Ma et al. 2008), but CD133 may inform prognosis (Zeppernicket al. 2008; Beier et al. 2008; Thon et al. 2008; Howard and Boockvar 2008) although somestudies have failed to demonstrate a link (Christensen et al. 2008). One study (Liu et al.,2006) found that CD133 mRNA increased upon tumor recurrence. In summary, it is premature
Rich and Eyler Page 6
Cold Spring Harb Symp Quant Biol. Author manuscript; available in PMC 2010 March 27.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

to consider CD133 as a validated prognostic indicator. The validation of other potential markersremains less developed.
Brain Tumor Stem Cells in Therapeutic ResistanceUnfortunately, patients afflicted with malignant gliomas suffer nearly universal treatmentfailure and death. As described above, surgical resection and cytotoxic modalities (radiation,chemotherapy) remain the mainstay of brain tumor therapy [of note, anti-angiogenic therapyin the form of the humanized neutralizing antibody against vascular endothelial growth factor(VEGF) has shown initial promise]. The mechanisms through which brain tumors becomeresistance to conventional therapy are poorly understood and are likely multi-factorial. Weexamined a potential contribution of brain tumor stem cells to radiation resistance (Bao et al.2006b). We found that ionizing radiation increased the relative frequency of tumor cellsexpressing cancer stem cell markers in treated xenografts. The relative enrichment of thesecells was accompanied by maintained capacity for self renewal and tumor propagation whereasmatched non-stem cancer stem cells were more likely to die. Cancer stem cell enriched culturestreated with radiation demonstrate a lower apoptotic fraction than non-stem cells in the sameconditions allowing for the outgrowth of the cancer stem cells. To elucidate a potentialmechanism, we studied the DNA damage checkpoint response in which a cascade of proteinsintegrates signals from damage sensors to determine whether cells will initiate a cell cyclearrest with DNA repair or undergo apoptosis. Cancer stem cells treated with radiation or radio-mimetics displayed an increased activation of the DNA damage checkpoint response incomparison to matched non-stem cancer cells. Although the activated proteins showedvariability between samples, some proteins appeared to be activated at baseline (e.g. Rad17)as if the cancer stem cells were primed to respond to genotoxic stress, which may be an earlyevent in cancer initiation. The role of the DNA damage checkpoint response provedcontributory as a pharmacologic inhibitor of the checkpoint sensitized the cancer stem cells toradiation. These results were supported by studies in genetically engineered medulloblastomas(Hambardzumyan et al. 2008). Other researchers have also found that neurosphere formingbrain tumor cells are more resistant to chemotherapy than similar cells grown underdifferentiating conditions (Liu et al. 2006). In sum, though these studies suggest that cancerstem cells may contribute to the common therapeutic resistance of brain tumors and may betargetable with pharmacologic approaches, it also seems unlikely that the full extent ofresistance in brain tumors derives from cancer stem cells.
Brain tumor stem cells in angiogenesisMalignant gliomas are commonly angiogenic with vascular proliferation serving as aninformative histologic feature indicating a glioblastoma among the gliomas. Many growthfactors are secreted by malignant gliomas to stimulate and maintain neoangiogenic vasculature.Targeted therapies have been developed against some of these pathways (reviewed in Jain etal. 2007). Most clinical trials have demonstrated modest benefits to these agents, but a potentialclinical efficacy has been seen in several trials of bevacizumab (Avastin), a neutralizingantibody against VEGF (Vredenburgh et al. 2006; Vredenburgh et al. 2007). Interestingly, theactivity of low molecular weight inhibitors against the VEGF receptors have been more modestin clinical trial suggesting that the same molecular pathway may be targeted by different agentswith different outcomes. During our studies of brain tumor stem cells, we noted that cancerstem cells form highly angiogenic tumors in comparison to the uncommon tumors that wedetect in propagation studies with cancer stem cell depleted cultures (Bao et al. 2006a). Wefound that conditioned media from cancer stem cells strongly induced endothelial cellmigration, proliferation, and tube formation in contrast to non-stem cancer cell conditionedmedia. Characterization of angiogenic proteins in the conditioned media revealed a consistentupregulation of VEGF. We were able to specifically block the effects of cancer stem cell
Rich and Eyler Page 7
Cold Spring Harb Symp Quant Biol. Author manuscript; available in PMC 2010 March 27.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

conditioned media on endothelial cells using bevacizumab. In animal studies, bevacizumabstrongly reduced the growth of tumors derived from cancer stem cells to a size and paucity ofvascularity nearly identical to that of the uncommon tumors formed by non-stem cancer cells.As non-stem cancer cells can survive implantation but rarely form tumors, the angiogenic drivemay provide one explanation for the striking tumor propagation of cancer stem cells. Inaddition, cancer stem cells may provide an angiogenic drive to support the growth of non-stemcancer cells, suggesting that their effects in the tumor may not need to be limited solely to thedirect production of progeny. In our studies, we noted that the cancer stem cells appeared tobe located near the vasculature. These observations have been confirmed and extended in aseminal study that demonstrated that brain tumor stem cell growth is supported by endothelialcells and that tumor formation by the cancer stem cells requires support from a vascular niche(Calabrese et al. 2007). Additional studies further indicate the presence of cancer stem cellmarker positive cells located in the perivascular niche of patient specimens. In sum, thesestudies suggest that brain tumor stem cells have the ability to form their own tumormicroevironment through the elaboration of angiogenic factors but at the same time remaindependent on that niche (Gilbertson and Rich 2007). These results may partially explain boththe clinical activity of bevacizumab and the invasive phenotype in patients who suffer failureafter bevacizumab treatment, since cancer stem cells display an invasive phenotype.
Targeting brain tumor stem cellsThere have been numerous recent reports of molecular targets that may be useful in ablatingbrain tumor stem cells. Several of these reports have focused on core stem cell/differentiationpathways, including BMI1 (Bruggeman et al. 2007, Godlewski et al. 2008), bone morphogenicprotein (BMP) (Piccirillo et al. 2006), Sonic Hedgehog (Bar et al. 2007, Clement et al. 2007),Sox2 (Gangemi et al. 2008), Oct4 (Du et al. 2008) and Notch (Fan et al. 2006). Inhibitors ofgrowth factor pathways, including epidermal growth factor (EGF) (Soeda et al. 2008) andplatelet-derived growth factor (PDGF), may be also be useful against brain tumor stem cells.To discover new molecular targets, we have compared expression of gene products or activatedsignal transduction pathways between cancer stem cells and non-stem cancer cells. Therationale behind this approach is that previously unrecognized targets may be discovered inthe small fraction of cells that we have found to be cancer stem cells in brain tumors (it is againimportant to note that cancer stem cells may not necessarily be uncommon).
In one study, we found that the cell surface protein, L1 cell adhesion molecule (L1CAM,CD171), is preferentially expressed in brain tumor stem cell enriched cultures (Bao et al.2008). L1CAM co-segregates with CD133 in glioblastoma patient biopsy specimens and isexpressed at higher levels than in human neural progenitors. L1CAM contributes to brain tumorstem cell survival as targeting L1CAM expression through lentiviral short hairpin RNA(shRNA) specifically induced apoptosis in brain tumor stem cell cultures and ablatedneurosphere formation. We found that L1CAM mediates its effects on brain tumor stem cellsat least in part through the regulation of the transcriptional regulator, Olig2. Other studies havedemonstrated that the targeted disruption of Olig2 in genetically engineered brain tumor modelsblocks tumor initiation (Ligon et al. 2007). In our studies, targeting L1CAM decreased Olig2expression and increased the expression of the key Olig2 target, the p21CIP1/WAF1 cyclindependent kinase inhibitor, and overexpression of Olig2 rescued the effects of L1CAMtargeting. Most importantly, targeting L1CAM either prior to xenotransplantation or inestablished tumors reduced tumor growth and extended the lifespan of mice bearing tumorstem cell xenografts. These results demonstrated that analysis of brain tumor stem cells canidentify novel molecular targets that may useful for brain tumor therapy.
The phosphoinositide 3-kinase (PI3K) pathway is commonly dysregulated in malignantgliomas through mutations in either the subunits of PI3K or the PTEN tumor suppressor gene
Rich and Eyler Page 8
Cold Spring Harb Symp Quant Biol. Author manuscript; available in PMC 2010 March 27.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

(Cancer Genome Atlas Research Network 2008). PI3K functions in part through regulation ofthe AKT/protein kinase B (PKB) survival pathway. We therefore examined the activation stateof AKT in brain tumor stem cells in comparison to matched non-stem tumor cells (Eyler et al.2008). The level of activating phosphorylation of AKT was lower at baseline in brain tumorstem cell cultures but was also more sensitive to inhibitory effects of low molecular weightAKT inhibitors. Whereas AKT inhibition of non-stem tumor cells was largely cytostatic, tumorstem cells displayed an apoptotic response with AKT or PI3K inhibitors. AKT inhibitors alsoreduced neurosphere formation and invasion. Finally, tumor initiation was impaired by AKTinhibition. These results and those from other laboratories studying BMP, Notch, sonichedgehog (SHH) and EGFR (Piccirillo et al. 2006, Lee et al. 2008, Fan et al. 2006, Bar et al.2007, Clement et al. 2007, Soeda et al. 2008) suggest that brain tumor stem cells may beparticular sensitive to targeted therapies against signal transduction pathways.
The c-myc oncogene is commonly involved in cancer initiation and maintenance but the roleof c-myc in glioma biology is poorly understood. We examined the potential role of c-myc inbrain tumor stem cells due to the involvement of c-myc in normal stem cell biology (Wang etal. 2008). Glioma stem cells derived from human surgical biopsies consistently expressedhigher levels of c-myc mRNA and protein relative to the non-stem tumor cells. Targeting c-myc expression was cytostatic in non-stem tumor cells but potently induced apoptosis andblocked self renewal in the glioma stem cells. Most importantly, targeting c-myc expressioncompletely blocked tumor propagation in transplantation studies. These results are very similarto those from a genetically engineered glioma model in which p53 and Pten are disrupted(Zheng et al. 2008).
These and several other studies have laid the foundation for novel insights into brain tumorbiology through the analysis of molecular regulators of brain tumor stem cells. The extensionof these studies into combination regimens with other therapies and potential clinical trialapplication may offer improved clinical outcomes.
PerspectiveNeuro-oncology has witnessed some important therapeutic advances, particularly in thetreatment of pediatric brain tumors. Unfortunately the outcome for adult patients with the mostcommon intrinsic primary brain tumor, glioblastoma multiforme, continues to be extremelypoor with even the most exciting advances providing only minimal improvement in mediansurvival in clinical trials. Fundamental changes in our paradigm in the development ofprognostic markers, imaging, and therapy must occur for real change to come to patients. It ispotentially useful to take lessons from another area of medicine, infectious diseases.Mycobacterium tuberculosis (Mtb) is a major health burden in the developing world and inimmunocompromised hosts. Few new effective anti-tuberculosis agents have been developed.Recent studies suggest that traditional high-throughput Mtb drug development assays thatessentially non-specifically target proliferation may not be useful in improving patient outcomebecause the model does not recapitulate the in vivo conditions (Nathan et al. 2008). Rather,Mtb displays a cellular heterogeneity with a small fraction of the total population that is resistantto conventional therapies and is relatively quiescent. Nonreplicating bacteria may be criticalto the problem of persistent Mtb infection. The striking parallels to cancer stem cell biologycannot be ignored and is not surprising as nature tends to repeat patterns. It is probable that notall cancers display a clear cellular hierarchy of tumor growth but the heterogeneity of cancersis essential to incorporate in models. The concept of stem cell-like cells within brain tumors isnot new but recent technologies have improved the ability to prospectively enrich for cancerstem cells and the recent increase in genetic understanding of brain tumors has informed thedevelopment of genetic brain tumor models. Although it is unlikely that brain tumor stem cellswill inform all of brain tumor biology, our current failure in clinical Neuro-oncology demands
Rich and Eyler Page 9
Cold Spring Harb Symp Quant Biol. Author manuscript; available in PMC 2010 March 27.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

the aggressive investigation of new areas of research. Our studies and those of other laboratorieshave suggested that brain tumor stem cells contribute to therapeutic resistance, tumorangiogenesis, and invasion. Further characterization of this cellular fraction may guide thedevelopment of biomarkers, imaging modalities, and treatments that will hopefully be moreeffective. However, this field is immature and the progress forward will likely be made withstumbles and errors but will be a learning process. The current challenge in deriving andmaintaining brain tumor stem cells is a major limitation in the field as most laboratories do nothave access to viable clinical specimens and animal resources. However, it is important to findways to adapt these techniques for widespread use since there is currently insufficient evidencethat established cell lines maintained for long periods in serum are useful in cancer stem cellstudies. Cell culture – particularly long term cell culture in medium containing serum – is wellrecognized to induce genetic changes that were not present in the original tumor, limiting theutility of cell lines in modeling the original disease. The development of validated brain tumormodels that can be shared in the field would be an important step forward. In addition, thefunctional assays for all brain tumor stem cell studies must be standardized with current useof serial neurosphere formation as a surrogate for self renewal and tumor propagation.Available markers for brain tumor stem cells are imperfect and cannot be definitively linkedto a stem cell phenotype, supporting an urgent need for improved markers. As brain tumorsare likely heterogeneous diseases, universal marker immunophenotypes may not be identifiablebut markers may assist in subcategorizing tumors. Molecular regulators of brain tumor stemcells may provide biomarkers, imaging targets, and therapeutic targets but it is likely thatmolecules may be shared with normal somatic stem cells so their use may be complicated.Regardless of the outcome, the recognition of the potential importance of the cancer stem cellhypothesis has energized brain tumor research. The healthy debate between believers andskeptics will almost certainly lead to completely unforeseen directions in the field of braintumor research and therapeutic development. In the end, we all hope to help those patients andfamilies who are afflicted by brain tumors.
AcknowledgmentsFinancial support was provided by the Childhood Brain Tumor Foundation, the Pediatric Brain Tumor Foundation ofthe United States, Accelerate Brain Cancer Cure, Alexander and Margaret Stewart Trust, Brain Tumor Society,Goldhirsh Foundation, Duke Comprehensive Cancer Center Stem Cell Initiative Grant, NIH grants NS047409,NS054276, CA129958 and CA116659. J.R. is a Damon Runyon-Lilly Clinical Investigator supported by the DamonRunyon Cancer Research Foundation.
REFERENCESAl-Hajj M, Wicha MS, Benito-Hernandez A, Morrison SJ, Clarke MF. Prospective identification of
tumorigenic breast cancer cells. Proc. Natl. Acad. Sci. U.S.A 2003;100:3983–3988. [PubMed:12629218]
Bao S, Wu Q, Sathornsumetee S, Hao Y, Li Z, Hjelmeland AB, Shi Q, McLendon RE, Bigner DD, RichJN. Stem cell-like glioma cells promote tumor angiogenesis through vascular endothelial growthfactor. Cancer Res 2006a;66:7843–7848. [PubMed: 16912155]
Bao S, Wu Q, McLendon RE, Hao Y, Shi Q, Hjelmeland AB, Dewhirst MW, Bigner DD, Rich JN. Gliomastem cells promote radioresistance by preferential activation of the DNA damage response. Nature2006b;444:756–760. [PubMed: 17051156]
Bao S, Wu Q, Li Z, Sathornsumetee S, Wang H, McLendon RE, Hjelmeland AB, Rich JN. Targetingcancer stem cells through L1CAM suppresses glioma growth. Cancer Res 2008;68:6043–6048.[PubMed: 18676824]
Bar EE, Chaudhry A, Lin A, Fan X, Schreck K, Matsui W, Piccirillo S, Vescovi AL, DiMeco F, OliviA, Eberhart CG. Cyclopamine-mediated hedgehog pathway inhibition depletes stem-like cancer cellsin glioblastoma. Stem Cells 2007;25:2524–2533. [PubMed: 17628016]
Rich and Eyler Page 10
Cold Spring Harb Symp Quant Biol. Author manuscript; available in PMC 2010 March 27.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Beier D, Hau P, Proescholdt M, Lohmeier A, Wischhusen J, Oefner PJ, Aigner L, Brawanski A, BogdahnU, Beier CP. CD133(+) and CD133(−) glioblastoma-derived cancer stem cells show differentialgrowth characteristics and molecular profiles. Cancer Res 2007;67:4010–4015. [PubMed: 17483311]
Bidlingmaier S, Zhu X, Liu B. The utility and limitations of glycosylated human CD133 epitopes indefining cancer stem cells. J. Mol. Med 2008;86:1025–1032. [PubMed: 18535813]
Bonnet D, Dick JE. Human acute myeloid leukemia is organized as a hierarchy that originates from aprimitive hematopoietic cell. Nature Med 1997;3:730–737. [PubMed: 9212098]
Bruggeman SW, Hulsman D, Tanger E, Buckle T, Blom M, Zevenhoven J, van Tellingen O, van andLohuizen M. Bmi1 controls tumor development in an Ink4a/Arf-independent manner in a mouse modelfor glioma. Cancer Cell 2007;12:328–341. [PubMed: 17936558]
Bühring HJ, Seiffert M, Marxer A, Weiss B, Faul C, Kanz L, Brugger W. AC133 antigen expression isnot restricted to acute myeloid leukemia blasts but is also found on acute lymphoid leukemia blastsand on a subset of CD34+ B-cell precursors. Blood 1999;94:832–833. [PubMed: 10438201]
Calabrese C, Poppleton H, Kocak M, Hogg TL, Fuller C, Hamner B, Oh EY, Gaber MW, Finklestein D,Allen M, Frank A, Bayazitov IT, Zakharenko SS, Gajjar A, Davidoff A, Gilbertson RJ. A perivascularniche for brain tumor stem cells. Cancer Cell 2007;11:69–82. [PubMed: 17222791]
Christensen K, Schrøder HD, Kristensen BW. CD133 identifies perivascular niches in grade II–IVastrocytomas. J. Neurooncol 2008;90:157–170. [PubMed: 18612800]
Clarke MF, Dick JE, Dirks PB, Eaves CJ, Jamieson CH, Jones DL, Visvader J, Weissman IL, Wahl GM.Cancer stem cells--perspectives on current status and future directions: AACR Workshop on cancerstem cells. Cancer Res 2006;66:9339–9344. [PubMed: 16990346]
Clement V, Sanchez P, de Tribolet N, Radovanovic I, Ruiz i Altaba A. HEDGEHOG-GLI1 signalingregulates human glioma growth, cancer stem cell self-renewal, and tumorigenicity. Curr. Biol2007;17:165–172. [PubMed: 17196391]
Cancer Genome Atlas Research Network. Comprehensive genomic characterization defines humanglioblastoma genes and core pathways. Nature 2008;455:1061–1068. [PubMed: 18772890]
Dalerba P, Dylla SJ, Park IK, Liu R, Wang X, Cho RW, Hoey T, Gurney A, Huang EH, Simeone DM,Shelton AA, Parmiani G, Castelli C, Clarke MF. Phenotypic characterization of human colorectalcancer stem cells. Proc. Natl. Acad. Sci. U.S.A 2007;104:10158–10163. [PubMed: 17548814]
Du Z, Jia D, Liu S, Wang F, Li G, Zhang Y, Cao X, Ling EA, Hao A. Oct4 is expressed in human gliomasand promotes colony formation in glioma cells. Glia. 2008 [Epub ahead of print].
Eyler CE, Foo WC, Lafiura KM, McLendon RE, Hjelmeland AB, Rich JN. Brain Cancer Stem CellsDisplay Preferential Sensitivity to Akt Inhibition. Stem Cells. 2008 [Epub ahead of print].
Fan X, Matsui W, Khaki L, Stearns D, Chun J, Li YM, Eberhart CG. Notch pathway inhibition depletesstem-like cells and blocks engraftment in embryonal brain tumors. Cancer Res 2006;66:7445–7452.[PubMed: 16885340]
Fulci G, Ishii N, Maurici D, Gernert K, Hainaut P, Kaur B, Van Meir EG. Initiation of human astrocytomaby clonal evolution of cells with progressive loss of p53 functions in a patient with a 283H TP53germline mutation: evidence for a precursor lesion. Cancer Res 2002;62:2897–2906. [PubMed:12019170]
Furnari FB, Fenton T, Bachoo RM, Mukasa A, Stommel JM, Stegh A, Hahn WC, Ligon KL, Louis DN,Brennan C, Chin L, DePinho RA, Cavenee WK. Malignant astrocytic glioma: genetics, biology, andpaths to treatment. Genes Dev 2007;21:2683–2710. [PubMed: 17974913]
Galli R, Binda E, Orfanelli U, Cipelletti B, Gritti A, De Vitis S, Fiocco R, Foroni C, Dimeco F, VescoviA. Isolation and characterization of tumorigenic, stem-like neural precursors from humanglioblastoma. Cancer Res 2004;64:7011–7021. [PubMed: 15466194]
Gangemi RM, Griffero F, Marubbi D, Perera M, Capra MC, Malatesta P, Ravetti GL, Zona GL, DagaA, Corte G. SOX2 Silencing in Glioblastoma Tumor Initiating Cells Causes Stop of Proliferationand Loss of Tumorigenicity. Stem Cells. 2008 [Epub ahead of print].
Gilbertson RJ, Rich JN. Making a tumour's bed: glioblastoma stem cells and the vascular niche. Nat. Rev.Cancer 2007;10:733–736. [PubMed: 17882276]
Godlewski J, Nowicki MO, Bronisz A, Williams S, Otsuki A, Nuovo G, Raychaudhury A, Newton HB,Chiocca EA, Lawler S. Targeting of the Bmi-1 oncogene/stem cell renewal factor by microRNA-128
Rich and Eyler Page 11
Cold Spring Harb Symp Quant Biol. Author manuscript; available in PMC 2010 March 27.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

inhibits glioma proliferation and self-renewal. Cancer Res 2008;22:9125–9130. [PubMed:19010882]
Hambardzumyan D, Becher OJ, Rosenblum MK, Pandolfi PP, Manova-Todorova K, Holland EC. PI3Kpathway regulates survival of cancer stem cells residing in the perivascular niche following radiationin medulloblastoma in vivo. Genes Dev 2008;22:436–448. [PubMed: 18281460]
Hemmati HD, Nakano I, Lazareff JA, Masterman-Smith M, Geschwind DH, Bronner-Fraser M,Kornblum HI. Cancerous stem cells can arise from pediatric brain tumors. Proc. Natl. Acad. Sci.U.S.A 2003;100:15178–15183. [PubMed: 14645703]
Hope KJ, Jin L, Dick JE. Acute myeloid leukemia originates from a hierarchy of leukemic stem cellclasses that differ in self-renewal capacity. Nat. Immunol 2004;5:738–743. [PubMed: 15170211]
Horn PA, Tesch H, Staib P, Kube D, Diehl V, Voliotis D. Expression of AC133, a novel hematopoieticprecursor antigen, on acute myeloid leukemia cells. Blood 1999;93:1435–1437. [PubMed:10075457]
Howard BM, Boockvar JA. Stem Cell Marker CD133 Expression Predicts Outcome in Glioma Patients.Neurosurgery 2008;62:N8.
Ignatova TN, Kukekov VG, Laywell ED, Suslov ON, Vrionis FD, Steindler DA. Human cortical glialtumors contain neural stem-like cells expressing astroglial and neuronal markers in vitro. Glia2002;39:193–206. [PubMed: 12203386]
Jain RK, di Tomaso E, Duda DG, Loeffler JS, Sorensen AG, Batchelor TT. Angiogenesis in braintumours. Nat. Rev. Neurosci 2007;8:610–622. [PubMed: 17643088]
Jaksch M, Múnera J, Bajpai R, Terskikh A, Oshima RG. Cell cycle-dependent variation of a CD133epitope in human embryonic stem cell, colon cancer, and melanoma cell lines. Cancer Res2008;68:7882–7886. [PubMed: 18829544]
Kelly PN, Dakic A, Adams JM, Nutt SL, Strasser A. Tumor growth need not be driven by rare cancerstem cells. Science 2007;20:337. 317(5836). [PubMed: 17641192]
Lapidot T, Sirard C, Vormoor J, Murdoch B, Hoang T, Caceres-Cortes J, Minden M, Paterson B, CaligiuriMA, Dick JE. A cell initiating human acute myeloid leukaemia after transplantation into SCID mice.Nature 1994;367:645–648. [PubMed: 7509044]
Lee J, Kotliarova S, Kotliarov Y, Li A, Su Q, Donin NM, Pastorino S, Purow BW, Christopher N, ZhangW, Park JK, Fine HA. Tumor stem cells derived from glioblastomas cultured in bFGF and EGF moreclosely mirror the phenotype and genotype of primary tumors than do serum-cultured cell lines.Cancer Cell 2006;9:391–403. [PubMed: 16697959]
Lee J, Son MJ, Woolard K, Donin NM, Li A, Cheng CH, Kotliarova S, Kotliarov Y, Walling J, Ahn S,Kim M, Totonchy M, Cusack T, Ene C, Ma H, Su Q, Zenklusen JC, Zhang W, Maric D, Fine FA.Epigenetic-mediated dysfunction of the bone morphogenetic protein pathway inhibits differentiationof glioblastoma-initiating cells. Cancer Cell 2008;13:69–80. [PubMed: 18167341]
Lee ST, Jang JH, Min YH, Hahn JS, Ko YW. AC133 antigen as a prognostic factor in acute leukemia.Leuk. Res 2001;25:757–767. [PubMed: 11489469]
Li C, Heidt DG, Dalerba P, Burant CF, Zhang L, Adsay V, Wicha M, Clarke MF, Simeone DM.Identification of pancreatic cancer stem cells. Cancer Res 2007;67:1030–1037. [PubMed: 17283135]
Ligon KL, Huillard E, Mehta S, Kesari S, Liu H, Alberta JA, Bachoo RM, Kane M, Louis DN, DepinhoRA, Anderson DJ, Stiles CD, Rowitch DH. Olig2-regulated lineage-restricted pathway controlsreplication competence in neural stem cells and malignant glioma. Neuron 2007;53:503–517.[PubMed: 17296553]
Liu G, Yuan X, Zeng Z, Tunici P, Ng H, Abdulkadir IR, Lu L, Irvin D, Black KL, Yu JS. Analysis ofgene expression and chemoresistance of CD133+ cancer stem cells in glioblastoma. Mol. Cancer2006;5:67. [PubMed: 17140455]
Ma YH, Mentlein R, Knerlich F, Kruse ML, Mehdorn HM, Held-Feindt J. Expression of stem cell markersin human astrocytomas of different WHO grades. J. Neurooncol 2008;86:31–45. [PubMed:17611714]
Miraglia S, Godfrey W, Yin AH, Atkins K, Warnke R, Holden JT, Bray RA, Waller EK, Buck DW. Anovel five-transmembrane hematopoietic stem cell antigen: isolation, characterization, and molecularcloning. Blood 1997;90:5013–5021. [PubMed: 9389721]
Rich and Eyler Page 12
Cold Spring Harb Symp Quant Biol. Author manuscript; available in PMC 2010 March 27.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Nathan C, Gold B, Lin G, Stegman M, de Carvalho LP, Vandal O, Venugopal A, Bryk R. A philosophyof anti-infectives as a guide in the search for new drugs for tuberculosis. Tuberculosis (Edinb)2008;1:S25–S33. [PubMed: 18762150]
O'Brien CA, Pollett A, Gallinger S, Dick JE. A human colon cancer cell capable of initiating tumourgrowth in immunodeficient mice. Nature 2007;445:106–110. [PubMed: 17122772]
Panchision DM, Chen HL, Pistollato F, Papini D, Ni HT, Hawley TS. Optimized flow cytometric analysisof central nervous system tissue reveals novel functional relationships among cells expressingCD133, CD15, and CD24. Stem Cells 2007;25:1560–1570. [PubMed: 17332513]
Piccirillo SG, Reynolds BA, Zanetti N, Lamorte G, Binda E, Broggi G, Brem H, Olivi A, Dimeco F,Vescovi AL. Bone morphogenetic proteins inhibit the tumorigenic potential of human brain tumour-initiating cells. Nature 2006;444:761–765. [PubMed: 17151667]
Pope WB, Lai A, Nghiemphu P, Mischel P, Cloughesy TF. MRI in patients with high-grade gliomastreated with bevacizumab and chemotherapy. Neurology 2006;8:1258–1260. [PubMed: 16636248]
Quintana E, Shackleton M, Sabel MS, Fullen DR, Johnson TM, Morrison SJ. Efficient tumour formationby single human melanoma cells. Nature 2008;456:593–598. [PubMed: 19052619]
Reya T, Morrison SJ, Clarke MF, Weissman IL. Stem cells, cancer, and cancer stem cells. Nature2001;414:105–111. [PubMed: 11689955]
Ricci-Vitiani L, Lombardi DG, Pilozzi E, Biffoni M, Todaro M, Peschle C, De Maria R. Identificationand expansion of human colon-cancer initiating cells. Nature 2007;445:111–115. [PubMed:17122771]
Rietze RL, Valcanis H, Brooker GF, Thomas T, Voss AK, Bartlett PF. Purification of a pluripotent neuralstem cell from the adult mouse brain. Nature 2001;412:736–739. [PubMed: 11507641]
Sanai N, Tramontin AD, Quiñones-Hinojosa A, Barbaro NM, Gupta N, Kunwar S, Lawton MT,McDermott MW, Parsa AT, Manuel-García Verdugo J, Berger MS, Alvarez-Buylla A. Uniqueastrocyte ribbon in adult human brain contains neural stem cells but lacks chain migration. Nature2004;427:740–744. [PubMed: 14973487]
Schüller U, Heine VM, Mao J, Kho AT, Dillon AK, Han YG, Huillard E, Sun T, Ligon AH, Qian Y, MaQ, Alvarez-Buylla A, McMahon AP, Rowitch DH, Ligon KL. Acquisition of granule neuronprecursor identity is a critical determinant of progenitor cell competence to form Shh-inducedmedulloblastoma. Cancer Cell 2008;2:123–134.
Shu Q, Wong KK, Su JM, Adesina AM, Yu LT, Tsang YT, Antalffy BC, Baxter P, Perlaky L, Yang J,Dauser RC, Chintagumpala M, Blaney SM, Lau CC, Li XN. Direct orthotopic transplantation offresh surgical specimen preserves CD133+ tumor cells in clinically relevant mouse models ofmedulloblastoma and glioma. Stem Cells 2008;26:1414–1424. [PubMed: 18403755]
Singec I, Knoth R, Meyer RP, Maciaczyk J, Volk B, Nikkhah G, Frotscher M, Snyder EY. Defining theactual sensitivity and specificity of the neurosphere assay in stem cell biology. Nat. Methods2006;3:801–806. [PubMed: 16990812]
Singh SK, Clarke ID, Terasaki M, Bonn VE, Hawkins C, Squire J, Dirks PB. Identification of a cancerstem cell in human brain tumors. Cancer Res 2003;63:5821–5828. [PubMed: 14522905]
Singh SK, Hawkins C, Clarke ID, Squire JA, Bayani J, Hide T, Henkelman RM, Cusimano MD, DirksPB. Identification of human brain tumour initiating cells. Nature 2004;432:396–401. [PubMed:15549107]
Soeda A, Inagaki A, Oka N, Ikegame Y, Aoki H, Yoshimura S, Nakashima S, Kunisada T, Iwama T.Epidermal growth factor plays a crucial role in mitogenic regulation of human brain tumor stem cells.J. Biol. Chem 2008;283:10958–10966. [PubMed: 18292095]
Stupp R, Mason WP, van den Bent MJ, Weller M, Fisher B, Taphoorn MJ, Belanger K, Brandes AA,Marosi C, Bogdahn U, Curschmann J, Janzer RC, Ludwin SK, Gorlia T, Allgeier A, Lacombe D,Cairncross JG, Eisenhauer E, Mirimanoff RO. European Organisation for Research and Treatmentof Cancer Brain Tumor and Radiotherapy Groups; National Cancer Institute of Canada Clinical TrialsGroup. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N. Engl. J. Med2005;352:987–996. [PubMed: 15758009]
Tabu K, Sasai K, Kimura T, Wang L, Aoyanagi E, Kohsaka S, Tanino M, Nishihara H, Tanaka S. Promoterhypomethylation regulates CD133 expression in human gliomas. Cell Res 2008;18:1037–1046.[PubMed: 18679414]
Rich and Eyler Page 13
Cold Spring Harb Symp Quant Biol. Author manuscript; available in PMC 2010 March 27.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Taylor MD, Poppleton H, Fuller C, Su X, Liu Y, Jensen P, Magdaleno S, Dalton J, Calabrese C, BoardJ, Macdonald T, Rutka J, Guha A, Gajjar A, Curran T, Gilbertson RJ. Radial glia cells are candidatestem cells of ependymoma. Cancer Cell 2005;8:323–335. [PubMed: 16226707]
Thon N, Damianoff K, Hegermann J, Grau S, Krebs B, Schnell O, Tonn JC, Goldbrunner R. Presence ofpluripotent CD133(+) cells correlates with malignancy of gliomas. Mol. Cell. Neurosci. 2008 [Epubahead of print].
Uchida N, Buck DW, He D, Reitsma MJ, Masek M, Phan TV, Tsukamoto AS, Gage FH, Weissman IL.Direct isolation of human central nervous system stem cells. Proc. Natl. Acad. Sci. U.S.A2000;97:14720–14725. [PubMed: 11121071]
Vredenburgh JJ, Desjardins A, Herndon JE 2nd, Dowell JM, Reardon DA, Quinn JA, Rich JN,Sathornsumetee S, Gururangan S, Wagner M, Bigner DD, Friedman AH, Friedman HS. Phase II trialof bevacizumab and irinotecan in recurrent malignant glioma. Clin. Cancer Res 2007a;13:1253–1259.[PubMed: 17317837]
Vredenburgh JJ, Desjardins A, Herndon JE 2nd, Marcello J, Reardon DA, Quinn JA, Rich JN,Sathornsumetee S, Gururangan S, Sampson J, Wagner M, Bailey L, Bigner DD, Friedman AH,Friedman HS. Bevacizumab plus irinotecan in recurrent glioblastoma multiforme. J. Clin. Oncol2007;25:4722–4729. [PubMed: 17947719]
Wang J, Wang H, Li Z, Wu Q, Lathia JD, McLendon RE, Hjelmeland AB, Rich JN. c-Myc is requiredfor maintenance of glioma cancer stem cells. PLoS ONE 2008;11:e3769. [PubMed: 19020659]
Weigmann A, Corbeil D, Hellwig A, Huttner WB. Prominin, a novel microvilli-specific polytopicmembrane protein of the apical surface of epithelial cells, is targeted to plasmalemmal protrusionsof non-epithelial cells. Proc. Natl. Acad. Sci U.S.A 1997;94:12425–12430. [PubMed: 9356465]
Wu M, Kwon HY, Rattis F, Blum J, Zhao C, Ashkenazi R, Jackson TL, Gaiano N, Oliver T, Reya T.Imaging hematopoietic precursor division in real time. Cell Stem Cell 2007;5:541–554. [PubMed:18345353]
Yang ZJ, Ellis T, Markant SL, Read TA, Kessler JD, Bourboulas M, Schüller U, Machold R, Fishell G,Rowitch DH, Wainwright BJ, Wechsler-Reya RJ. Medulloblastoma can be initiated by deletion ofPatched in lineage-restricted progenitors or stem cells. Cancer Cell 2008b;2:135–145.
Yang Z, Chen Y, Lillo C, Chien J, Yu Z, Michaelides M, Klein M, Howes KA, Li Y, Kaminoh Y, ChenH, Zhao C, Chen Y, Al-Sheikh YT, Karan G, Corbeil D, Escher P, Kamaya S, Li C, Johnson S,Frederick JM, Zhao Y, Wang C, Cameron DJ, Huttner WB, Schorderet DF, Munier FL, Moore AT,Birch DG, Baehr W, Hunt DM, Williams DS, Zhang K. Mutant prominin 1 found in patients withmacular degeneration disrupts photoreceptor disk morphogenesis in mice. J. Clin. Invest 2008a;118:2908–2916. [PubMed: 18654668]
Yi JM, Tsai HC, Glöckner SC, Lin S, Ohm JE, Easwaran H, James CD, Costello JF, Riggins G, EberhartCG, Laterra J, Vescovi AL, Ahuja N, Herman JG, Schuebel KE, Baylin SB. Abnormal DNAmethylation of CD133 in colorectal and glioblastoma tumors. Cancer Res 2008;68:8094–8103.[PubMed: 18829568]
Yin AH, Miraglia S, Zanjani ED, Almeida-Porada G, Ogawa M, Leary AG, Olweus J, Kearney J, BuckDW. AC133, a novel marker for human hematopoietic stem and progenitor cells. Blood1997;90:5002–5012. [PubMed: 9389720]
Yuan X, Curtin J, Xiong Y, Liu G, Waschsmann-Hogiu S, Farkas DL, Black KL, Yu JS. Isolation ofcancer stem cells from adult glioblastoma multiforme. Oncogene 2004;23:9392–9400. [PubMed:15558011]
Zeppernick F, Ahmadi R, Campos B, Dictus C, Helmke BM, Becker N, Lichter P, Unterberg A,Radlwimmer B, Herold-Mende CC. Stem cell marker CD133 affects clinical outcome in gliomapatients. Clin. Cancer Res 2008;14:123–129. [PubMed: 18172261]
Zheng H, Ying H, Yan H, Kimmelman AC, Hiller DJ, Chen AJ, Perry SR, Tonon G, Chu GC, Ding Z,Stommel JM, Dunn KL, Wiedemeyer R, You MJ, Brennan C, Wang YA, Ligon KL, Wong WH,Chin L, DePinho RA. p53 and Pten control neural and glioma stem/progenitor cell renewal anddifferentiation. Nature 2008;7216:1129–1133. [PubMed: 18948956]
Rich and Eyler Page 14
Cold Spring Harb Symp Quant Biol. Author manuscript; available in PMC 2010 March 27.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

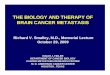
Figure 1.Brain tumors display a cellular hierarchy that resembles, but differs from, the normal neuralcell hierarchy. Normal neural stem cells have the ability to self-renew while also dividing togive rise to uncommitted progenitor cells which, in turn, give rise to lineage-restrictedcommitted progenitors and finally differentiated astrocytes, oligodendrocytes and neurons.Similarly, tumors appear to have a cellular hierarchy with self-renewing glioma stem cells ableto generate a variety of more differentiated progeny, though patterns of differentiation appearto be less discrete than in the normal brain and many of the cancer stem cell-derived progenydisplay aberrant differentiation patterns, expressing more than one type of differentiationmarker.
Rich and Eyler Page 15
Cold Spring Harb Symp Quant Biol. Author manuscript; available in PMC 2010 March 27.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

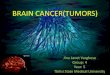
Figure 2.Cancer stem cells are defined by a capacity for sustained self-renewal, persistent proliferationand tumor initiation or propagation. Some characteristics that are often, but not necessarily,associated with brain tumor stem cells include rarity within a tumor, expression of stem cellmarkers, and a capacity for multi-lineage differentiation.
Rich and Eyler Page 16
Cold Spring Harb Symp Quant Biol. Author manuscript; available in PMC 2010 March 27.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript