The MRSA Superbug
The MRSA SuperbugBrad M. Wright, PharmD, BCPSAssistant Clinical
ProfessorAuburn University Harrison School of PharmacyAdjunct
Assistant ProfessorUniversity of South Alabama College of
MedicineDisclosureProgramming offered by Auburn University Harrison
School of Pharmacy shall exhibit balance, providing the audience
information of different perspectives from which to develop an
informed professional opinion.
I, Brad Wright, have the following to disclose:Grant Funding
Novartis PharmaceuticalsObjectives1.Describe Methicillin-resistant
Staphylococcus aureus (MRSA) and the impact associated with
infection
2.Explain the differences between hospital and
community-associated MRSA
3.Discuss appropriate treatment options for MRSA infection
In the HospitalStaph often adds danger, days to a patient stay
Portland Tribune
Drug-resistant staph lurks in many places USA Today
Staph Superbug May Be Infecting Patients- ABC news
Problem of Hospital Acquired Infections, Antibiotic Resistance
is Growing Homeland SecurityCommunityMRSA Hospitalizations Surge,
as Drug Resistant Superbug Moves Outside Hospital Settings
MRSA "Superbug" Claims Life Of Another Texas Teen CBS
Schools On Alert For 'Superbug' Staph Infections CBS
Bacteria that killed Virginia teen found in other schools -
CNN
Headlines
What is MRSA?Methicillin-resistant Staphylococcus aureus
Leading cause of infections in both the hospital and the
community
Commonly found on the skin and in the nose of the general
population
Causes multiple types of infectionsInvasive Bloodstream,
pneumonia, etcNon-invasive Skin
Associated with a high risk of morbidity and mortality and
increased health care costs85% of all invasive MRSA infections
asociated with health care settings.
8What MRSA is notA death sentence
A new, never seen before type of infection or bug
Untreatable by current antibiotics
Only associated with dirty hospitals
A reason patients should not be around others or stay at
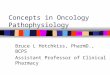
home9Burden of MRSA1999 295,000 hospitalization due to S. aureus Of
these an estimated 127,000 (43%) were due to MRSA
2005 478,000 hospitalizations due to S. aureusOf these, an
estimatetd 278,000 (58%) were due to MRSA
Hospitalizations associated with S. aureus infection increased
62% or ~ 8.4% per yearMRSA infections increased 119% or ~14% per
year.
Dramatic increase in skin infectionsEmerg Infect Dis
2007;13:1840-6, www.cdc.govBurden of MRSA
Emerg Infect Dis 2007;13:1840-6, How did we get here?1928
Penicillin discovered1941 Penicillin available in US 1940s
Resistance emerges 1958 Vancomycin introduced1959 Methicillin
introduced1961 First cases of MRSA1968 First hospital outbreak
followed by an increase in prevelance in hospitals1980s - 90s First
community outbreaks
12Where is MRSA?Initially MRSA was endemic to US hospitals and
long-term care facilitiesIll and elderly
patientsHealthcare-associated MRSA (HA-MRSA)
MRSA is no longer limited to just hospitalized patients1980s -
IV drug users in the community1990s - US Children
Outbreaks in communities worldwideCommunity-acquired MRSA
(CA-MRSA)13Where is MRSA In HospitalsThe proportion of
healthcare-associated staphylococcal infections that are due to
MRSA has been increasing 2% in 1974 64% in 2004More recent data
describes a stabilization or decrease in this trend56% of
device-associated infections with S. aureus reported as MRSA in
2006-2007 Most recent estimates show decreases in these infections
in the U.S.MRSA bloodstream infections demonstrated a 34% decrease
in incidence between 2005 and 2008Clin Infect Dis 2006;42:389-91,
www.cdc.gov, Infect Control Hosp Epidemiol 2008;29:996-1011 Most
common infections in the hospital14Where is MRSA - CommunityMost
Community-acquired MRSA presents as SSTI
In 2005, approximately14 million outpatient healthcare visits
were made for suspected S. aureus skin and soft tissue
infections
In 2004 >75% of SSTIs presenting to ED were S. aureus~60% -
MRSA
Most common CA-MRSA InfectionsN Engl J Med 2005;
352:1436-144416HA-MRSA vs CA-MRSAHA-MRSA infections occur in
patients who are in or recently have been in hospitals or other
health-care settingsOften are related to surgery or medical devices
Often found in the blood, tissues, lungs, heart valvesResistant to
many different drugs
CA-MRSA infections are found in patients in the communityUsually
limited to skin infectionsMay be susceptible to more types of
antibioticsDefinition of CA-MRSACDC definition:
Diagnosis of MRSA in the outpatient setting or positive culture
within 48 hours of hospital admissionNo history in the past year
of:HospitalizationAdmission to nursing home, skilled nursing
facility, or hospiceDialysisSurgeryNo permanent indwelling
catheters or medical deviceswww.cdc.govCA-MRSANot spill over of
HA-MRSA to the community
Separate and distinct clones of MRSAUSA 300
Panton-Valentine leukocidin (PVL) gene Virulence factor found in
almost all strains of CA-MRSACauses necrosis and
inflamationCommonly found in CA-MRSA not in HA-MRSA
Most common presentation is minor skin and soft tissue
infectionsSpider bitesSkin and Soft-tissue
InfectionsImpetigoSecondary infection - skin
lesionsAbscessFuruncleCarbunclePurulunt cellulitisNonpurulent
cellulitisComplicatetd SSTINonpurulent cellulitis often caused by
strep, not staph20Who is at Risk CA-MRSA?Factors associated with
increased risk:Close contactCuts/abrasions openings in the
skinContaminated items and surfacesCrowded living conditionsPoor
hygiene
These factors are common in: DormsAthletic facilitiesMilitary
barracks PrisonsDaycaresHA-MRSA vs CA-MRSACA MSAHA-MRSATime of
culture after hospital admission 48hrsCloneUSA 300USA 100Presence
of PVL toxinCommonRareRisk factorsUsually none; Close physical
contact, activities associated with poor communal hygieneRecent
hospitalization, surgery, prior antibioticsTypical patientYoung,
healthyChronically ill, hospitalizedType of infectionSkin abscesses
and cellulitisPneumonia, bloodstream, cSSIResistanceBeta-lactams;
typically resistant to fewer agentsMultiple-drug resistantTreatment
of CA-MRSA SSTIPrimary - Incision and drainageWith or without
antibiotic therapy
No further benefit associated with antibiotic therapy for simple
abscessesStudies have shown high cure rates whether or not an
antibiotic is usedTrials comparing TMP/SMX with placebo show no
difference in cure rateAntibiotic may prevent development of new
lesionsRetrospective trials suggest improved cure rates with
antibioticsClin Infect Dis 2011;52:1-38Treatment of CA-MRSA
SSTIAntibiotic therapy is recommended for abscesses associated
with:Severe or extensive diseaseRapid progressionSigns and symptoms
of systemic illnesAssociated comorbidities or
immunosuppresionExtremes of ageAbscess in an area difficult to
drainAssociated septic phlebitisLack of response to incision and
drainage
24Treatment of CA-MRSA SSTIOutpatients with purulent
cellulitisEmpirical antibiotic therapy for CA-MRSA5-10 days of
therapy
Outpatients with nonpurulent cellulitisEmpirical antibiotic
therapy for infection due to beta-hemolytic streptococci5-10 days
of therapyCA-MRSA coverage for those who do not respond to
beta-lactam therapy
If you suspect Staph, treat for MRSA25Treatment of CA-MRSA
SSTIOral antibiotic options for outpatients with
SSTIClindamycinTMP-SMXTetracyclinesLinezolid
Coverage for streptococci Clindamycin aloneTMP-SMX or
tetracycline + beta-lactamLinezolid alone
ClindamycinFDA approved to treat serious infections caused by
Staphylococcus aureus (not MRSA)
Mechanism of action: Inhibits protein synthesis
Typical Adult Dose: 300-450 mg PO TID600mg PO/IV TID (cSSTI)
ADRs: Diarrhea, GI upsetClostridium difficile associated
disease
Pregnancy cateory BBacteriostatic not recommended for
endovascular infection (infective endocardidtis or septic
thrombophlebitis)Excellent tissue penetration, particularly in bone
and abscessesSusceptibility to clindamycin are higher among CA-MRSA
than HA-MRSADiarrhea most common adverse effect and occurs in up to
20% of pts.C. DiffOral suspension not well tolerated in
childrenPregnancy category B27ClindamycinClindamycin ResistanceIn
Vitro susceptibility higher for CA-MRSA than HA-MRSAInducible
resistanceD-TestErythromycin disk is placed near clindamycin
diskEvaluate for D zone of inhibition
Clin Infect Dis. 2005;40(2):280-285. Detection of inducible
clindamycin resistance in erythromycin-resistant,
clinda-susceptible isolates28Trimethoprim - SulfamethoxazoleNo
FDA-labeled indication for Staphylococcal infection
Mechanism of Action - TMP and SMX each block folate synthesis at
a different step in the pathway which synergistically results in a
bactericidal effect
Dose: 1-2 double-strength (DS) tabs BID
Almost 100% of CA-MRSA strains are susceptible in
vitro29Trimethoprim-SulfamethoxazoleAdverse Reactions:Common: Rash,
Nausea, Vomiting, HyperkalemiaSevere: Cytopenias, Stevens-Johnson
syndrome, Nephritis
Drug interactions: Increased levels of warfarin, methotrexate,
phenytoinACEi
Caution in elderly, especially those with kidney disease
Pregnancy category C/DNot recommended in 3rd trimester
30TetracyclinesDoxycycline is FDA-approved for the treatment of
SSTI due to S. aureus.Not FDA approved for MRSA
Tetracycline, Doxycycline, and Minocycline
Mechanism of action: Inhibition of bacterial protein
synthesis
Doses:Minocycline - 200mg x1, then 100mg po BIDDoxycycline -
100mg po BIDEffective for treatment of SSTI, but data are lacking
to support their use in more-invasive infectionsMinocycline is
available IV and oralTigecycline bacteriostatic againstt MRSA,
caution should be used in treating patients with
bacteremia31TetracyclinesContraindications: Children < 8 years
of age Pregnancy
ADRs:Photosensitivity, N/V
Drug Interactions:Decreased absorption with food,dairy, or
antacids
Studies show tetracyclines are well tolerated with success of
95-100% in CA-MRSA SSTITet(k) confers resistance to tetracycline
and inducible resistance to doxy therefore minocycline may be most
preferredPregnancy category D No children under 8
Results of Antimicrob Agents and Chemother, Sept 2007, p.
3298-3303More patients in the beta-lactam group were likely to have
a surgical service to the I and d.
Treatment success was seen in 96% of the doxycycline group vs.
88% of the beta-lactam group
12% of the beta-lactam group changed therapy at day 4 to an
active agent
The only predictor of clinical failure in a bivariate analyses
was beta lactam therapyItems that were not predictors included:
severity of underlying illness, presense of SIRS (17% of each
group), or demographics
In a subgroup analyses of patients who only received I&D:
betalactam therapy was associated with a negative outcome (n=225;
adjust OR 3.39; 95% CI (1.07 10.75, p = 0.04)
Conclusion:
Probably the largest study to date (published in september 2007)
evaluating the use of tetracyclines/doxycycline in CA-MRSA SSTI.
Therapy was well tolerated and had a success rate of 96%. At
present, most laboratories are not testing mino or doxy versus s
aureus. Until they do, you should assume that tetracycline
resistance confers resistance to the class. May be useful in
patients with sulfa allergy. This study emphasizes the importance
of surgical drainage as primary therapy.
The limitations to this study: retrospective, no randomization,
patients excluded/did not follow up could have altered results
32LinezolidFDA approvedTreatment of SSTI and nosocomial
pneumonia due to MRSA
MOA: Inhibits protein synthesisInhibits PVL
Dose: 600mg BID (IV or PO)High bioavailability
Used for hospital-acquired and community-associated
infections
More expensive than other alternatives
Only orally available agent for which efficacy against MRSA
infection has been demonstrated in controlled trialsGreat activity
vs Group A strep
Has in vitro activity vs VISA and VRSA100% bioavalability only
give IV if GI absorption problem or pt cant take oralResistance is
rare.33Linezolid - ADRsMyelosuppression:Associated with long term
therapy (>2 weeks)S/Sx: thrombocytopenia, anemia,
pancytopenia
Serotonin SyndromeLinezolid = Mild MAO InhibitorConcomitant use
with SSRIs and SNRIs can lead to increase levels of
serotoninConcomitant use should be avoidedUse caution and monitor
for s/sx if used together
Pharmacotherapy. 2007 Aug;27(8):1189-97Long-term use is limited
by hematologic toxicity, with thrombocytopenia occuring more
frequently than anemia and neutropenia, peripheran and optic
neuropathy, and lactic acidosis. Weak, nonselective, reversible
inhibitor of MAO and has been associated with serotonin syndrome in
pts taking concurrent SSRIsLess bone marrow suppression in children
than adultsMost commor ADRs diarrhea, vomiting, loose stools,
anauseaPregnancy - C34Topical TreatmentsNeosporin/Polysporin
Mupirocin (Bactroban)
Retapamulin (Altabax)Recurrent MRSA SSTIsDefinition - 2 or more
discrete SSTI episodes at different sites over a 6-month period
Multidimensional approachEngage the patient in personal and
environmental hygiene measuresPreventive education on personal
hygiene and wound careCover infected skin and draining
woundsMaintain good personal hygieneAvoid sharing personal itemsUse
cleaners or detergents to clean surfacesClin Infect Dis
2011;52:1-38; www.cdc.gov/mrsa/enfironment/index.htmlRecurrent MRSA
SSTIs -DecolonizationEliminate S. aureus carriage
May be considered for patients with:Multiple recurrent SSTI
despite hygiene measuresOngoing transmission in a well-defined,
closely associated cohort
Should be offered in conjunction with ongoing reinforcement of
hygeiene measures
www.cdc.gov/ncidod/dhqp/ar_mrsa_ca.html; Clin Infect Dis;52:1-38
Given the potential role of colonization in the pathogenesis of
recurrent SSTI, prevention strategies have also focused on
decolonization, the use of antimicrobial or antiseptic agents to
suppress or eliminate S. Aureus carriage as a means of preventing
auto-infection or transmission
No published datta to support its efficacy in patients with
recurrent MRSA SSTI optimal regimen, frequency of application, and
duration of therapy are unclear. Unknown whether it will select for
or result in replacement with more resistant or more-virulent
strains37Recurrent MRSA SSTIsDecolonization strategiesNasal
mupirocin 5 day courseMupirocin + topical antiseptic
(chlorhexidine)Oral antibioticsRifampin + TMP-SMX/doxycycline5-10
daysCombine with hygiene measures and /or topic antiseptic
If household transmission is suspected:Personal and
environmental hygiene measuresEvaluation and treatment of
symptomatic contacts
Am J Infect Control 2007;35:16-14; Clin Infect Dis
2007;44:178-85; Clin Infect Dis;52:1-38 38Treatment of Complicated
SSTIComplicated SSTI (cSSTI) is defined as:Deeper soft-tissue
infectionsSurgical/traumatic wound infectionMajor
abscessesCellulitisInfected ulcers and burns
Also patients with systemic toxicity and/or rapidly progressing
or worsening infection
Inpatient management with surgical debridement and
broad-spectrum antibiotics
Clin Infect Dis;2011;52:1-38Treatment of Complicatted
SSTIEmpirical therapy for MRSA should be considered pending culture
data
Options for hospitalized patients
include:VancomycinLinezolidDaptomycinTelavancinClindamycin
CeftarolineBeta-lactam may be considered with nonpurulent
cellutis
7-14 days of therapy is recommended
Clin Infect Dis 2011;52:1-38VANC:Mainstay of parenteral therapy
for MRSA infectionsPreferred option in hospitalized
patients15-20mg/kg/dose IV every 8-12 hoursEfficacy has come into
question, with concerns over its slow bactericidal activity, the
emergence of resistant strains, and possible MIC Creep among
susceptible strainsInferior to beta-lactams for MSSA bacteremia and
infective endocarditisTissue penetration is highly variable and
depends upon the degree of inflamationLimited penetration into
bone, lung epithelial lining fluid and CSFPregnancy category
CDAPTOMYCIN:4mg/kg/dose IV dailyLess likely to develop
resistanceCan not be used for pneumoniaCEFTAROLINE:4mg/kg/dose IV
dailyLess likely to develop resistanceCan not be used for
pneumonia
40MRSA PneumoniaCA - MRSA has emerged as a cause of
community-acquired pneumonia (CAP)Secondary to influenza
infection
Empirical therapy for MRSA should be considered in patients with
severe CAP defined by any of the following:ICU admissionNecrotizing
or cavitary infiltratesEmpyema
Chest 2010;138:130-6; Clin Infect Dis 2011;52:1-38Discontinue if
blood or sputum cultures do not grow Staph41MRSA PneumoniaFor
HA-MRSA or CA-MRSA consider the following treatment options:IV
vancomycinLinezolid IV/POClindamycin IV/PO TID
Recommended length of therapy 7-21 days
Empyema Antibiotics in conjunction with drainageClin Infect Dis
2011;52:1-38MRSA osteomyelitisMRSA bone infections result
from:Hematogenous seedingContiguous focus of infectionDirect
inoculation from trauma or medical procedure
Surgical debridement of necrotic bone and drainage of adjacent
abscessMainstay of therapyCombine with antibiotics
MRSA Osteomyelitis Antibiotic TherapyOptimal route of
administration has not been established
Parenteral antibiotics include:VancomycinDaptomycin
6mg/kg/doseTMP-SMX 4mg/kg/dose BID w/ RifampinLinezolid
PO/IVClindamycin IV/PO
Optimal duration of therapy is unknown but a minimum of 8 weeks
is recommended
Parenteral, oral, or initial parenteral followed by oral therapy
may be usedDepends on individual patient circumstances44SummaryMRSA
is no longer confined to the hospital
CA MRSA often presents as a skin infectionTreatment usually
consists of TMP/SMX, clindamycin, tetracyclines, or linezolidMore
severe infections treated with IV antibiotics
Treatment should also consist of hygiene counseling
ReferencesCenters for disease control and prevention. MRSA
infections. http://www.cdc.gov/mrsa.html (Accessed 9/28/11)Liu C,
Bayer A, Cosgrove SE, et al. Clinical Practice Guidelines by the
Infectious Deseases Society of America for the Treatment of
Methiciliin-Resistant Staphylococcus Aureus Infections in Adults
and Children. Clin Infect Dis. (2005) 40 (2): 280-285. Klein E,
Smith DL, Laxminarayan R. Hospitalizations and Deaths Caused by
Methicillin-Resistant Staphylococcus aureus, United States,
19992005 Emerg Infect Dis 2007;13:1840-6.Klevens RM, Edwards JR,
Tenover FC, et al. Changes in the epidemiology of
methicillin-resistant Staphylococcus aureus in intensive care units
in US hospitals, 19922003. Clin Infect Dis 2006;42:389-91.Hidron
AI, Edwards JR, Patel J, et al, National Healthcare Safety Network
Team; Participating National Healthcare Safety Network Facilities:
Antimicrobial-resistant pathogens associated with
healthcare-associated infections: Annual summary of data reported
to the Natioanl Healthcare Safety Network at the Centes for Disease
Control and Prevention, 2006-2007. Infect Control Hosp Epidmiol
2008, 29:996-1011.Fridkin SK, Hageman JC, Morrison M, et al.
Methicillin-Resistant Staphylococcus aureus Disease in Three
Communities. N Engl J Med 2005; 352:1436-1444.Lewis JS, Jorgensen
JH. Inducible Clindamycin Resistance in Staphylococci: Should
Clinicians and Microbiologists be Concerned? Clin Infect Dis.
2005;40(2):280-285.Narita M, Tsuji BT, Yu VL. Linezolid-associated
peripheral and optic neuropathy, lactic acidosis, and serotonin
syndrome. Pharmacotherapy. 2007 Aug;27(8):1189-97Simor AE, Phillips
E, McGeer A, et al. Randomized controlled trial of chlorhexidine
gluconate for washing, intranasal mupirocin, and rifampin and
doxycycline versus no treatment for the eradication of
methicillin-resistant Staphylococcus aureus colonization. Clin
Infect Dis 2007;44:178-85.Lobo LJ, Reed KD, Wunderink RG. Expanded
clinical presentation of community-acquired methicillin-resistant
Staphylococcus aureus pneumonia. Chest 2010;138:130-6.
The MRSA SuperbugBrad M. Wright, PharmD, BCPSAssistant Clinical
ProfessorAuburn University Harrison School of PharmacyAdjunct
Assistant ProfessorUniversity of South Alabama College of
Medicine