Embed Size (px)
Citation preview

Brachial Plexus and Nerves about the ShoulderCarlo Martinoli, M.D.,1 Nicola Gandolfo, M.D.,2 Maribel Miguel Perez, M.D.,3
Andrea Klauser, M.D.,4 Federigo Palmieri, M.D.,1 Luca Padua, M.D.,5,6
and Alberto Tagliafico, M.D.1
ABSTRACT
Ultrasound (US) and MR imaging have been shown able to detect in-depthfeatures of brachial plexus anatomy and to localize pathological lesions in disorders whereelectrophysiology and physical findings are nonspecific or nonlocalizing. High-endgradient technology, phased array coils, and selection of an appropriate protocol of pulsesequences are the main requirements to evaluate the brachial plexus nerves with MRimaging and to distinguish between intrinsic and extrinsic pathological changes. A carefulscanning technique based on anatomical landmarks is required to image the brachial plexusnerves with US. In traumatic injuries, MR imaging and myelographic techniques canexclude nerve lesions at the level of neural foramina and at intradural location. Outside thespinal canal, US is an excellent alternative to MR imaging to determine the presence of alesion, to establish the site and the level of nerve involvement, as well as to confirm orexclude major nerve injuries.
In addition to brachial plexus injuries, MR imaging and US can be contributory ina variety of nontraumatic brachial plexopathies of a compressive, neoplastic, and inflam-matory nature. In the thoracic outlet syndrome, imaging performed in association withpostural maneuvers can help diagnose dynamic compressions. MR imaging and US are alsoeffective to recognize neuropathies about the shoulder girdle involving the suprascapular,axillary, long thoracic, and spinal accessory nerves that may mimic brachial plexopathy. Inthis article, the clinical entities just listed are discussed independently, providing anoverview of the current status of knowledge regarding imaging assessment.
KEYWORDS: Brachial plexus, Parsonage-Turner syndrome, brachial plexopathies,thoracic outlet syndrome, magnetic resonance imaging, ultrasound, MR myelography
Evaluation of the brachial plexus represents agreat challenge to the clinician and the radiologist,posing difficulties in patient management, the timingand range of investigation, as well as the indication forsurgery.1 In the diagnostic workup for brachial plexuspathology, a preliminary meticulous physical examina-
tion is essential to understand which part or parts of theplexus are involved.2,3 Electrophysiology, includingnerve conduction studies and electromyography(EMG), may serve to confirm and extend clinical in-formation, to assess whether a lesion is pre- or post-ganglionic based on the pattern of involvement.2,3
1Cattedra di Radiologia–DISC, Universita di Genova, Genova, Italy;2IM2S–Institut Monegasque de Medecine and chirurgie Sportive,Montecarlo, Monaco; 3Unit of Human Anatomy and Embryology,Department of Pathology and Experimental Therapy, Faculty ofMedicine (C Bellvitge), University of Barcelona, Barcelona, Spain;4Department of Diagnostic Radiology, Medical University Innsbruck,Innsbruck, Austria; 5Fondazione Don Gnocchi Onlus; 6Department ofNeurology, Policlinico ‘‘A. Gemelli,’’ Universita Cattolica del SacroCuore, Rome, Italy.
Address for correspondence and reprint requests: Carlo Martinoli,
M.D., Cattedra di Radiologia–DISC, Universita di Genova, LargoRosanna Benzi 8, I-16132 Genova, Italy (e-mail: [email protected]).
Imaging of the Peripheral Nerves; Guest Editor, Carlo Martinoli,M.D.
Semin Musculoskelet Radiol 2010;14:523–546. Copyright # 2010Thieme Medical Publishers, Inc., 333 Seventh Avenue, New York, NY10001, USA. Tel: + 1(212) 584-4662.DOI: http://dx.doi.org/10.1055/s-0030-1268072.ISSN 1089-7860.
523
Dow
nloa
ded
by: R
utge
rs U
nive
rsity
. Cop
yrig
hted
mat
eria
l.

However, functional studies are often nonspecific ornonlocalizing, especially at the early stage of somebrachial plexopathies or in cases of mild abnormalities.4
Imaging modalities, therefore, are a necessary comple-ment to conclude the diagnostic assessment of mostbrachial plexus disorders. Imaging is currently based onmagnetic resonance (MR) imaging, computed tomog-raphy (CT), ultrasound (US), myelographic techniques,and radiography.5–7 Although MR imaging is widelyregarded as the method of choice in the workup ofmany brachial plexus disorders, this technique hasinherent limitations in specific clinical settings andcan be variably supported by other modalities depend-ing on the underlying clinical problem but also on theequipment used and the management policy of periph-eral nerve surgeons.
In the last decade, the diagnostic workup forevaluation of brachial plexus pathology has been con-tinually reviewed with technological refinements inprogress and the introduction of novel cutting-edgeimaging algorithms.1,8 Light must be shed, therefore,on where imaging is going to draw the current optimalimaging strategy for any indication, thereby avoidingunderutilization or inappropriate use of the availableimaging techniques. In this article, we discuss andillustrate the imaging appearance of a wide spectrum of
brachial plexus pathologies, including traumatic injuries,entrapment syndrome at the thoracic outlet, Parsonage-Turner syndrome, secondary and primary tumors, andradiation therapy. In addition to the plexus, somefrequently missed uncommon neuropathies about theshoulder girdle affecting the suprascapular, the axillary,the long thoracic and the spinal accessory nerves arediscussed.9,10
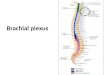
NORMAL ANATOMYThe brachial plexus has a complex anatomy with manynerves involved that interconnect.11 At each vertebrallevel, anterior (motor) and posterior (sensory) nerverootlets exit the spinal cord and merge at the dorsalroot ganglion at the level of the neural foramina. There-after, each ganglion gives off a large ventral and a smalldorsal branch, each including motor and sensory fibers.The dorsal branch provides nerve supply to the para-spinal muscles but does not take part in the brachialplexus (Fig. 1A). Instead, the plexus is formed by thecontribution of the ventral branches coming from thefour cervical (C5, C6, C7, and C8) and the first thoracic(T1) level (Fig. 1B). These branches are referred to as theproper ‘‘nerve roots’’ and extend from the neural fora-mina to the interscalene triangle.
Figure 1 Brachial plexus anatomy. (A) Schematic drawing of a cross-sectional view of the fifth cervical vertebra showing thespinal cord (black arrow). The spinal nerve arises from the spinal cord by dorsal (outlined arrowhead) and ventral (black arrowhead)rootlets. The spinal ganglion (G) is located on the dorsal root within the intervertebral foramen. The dorsal and ventral rootlets joinat about the level of the intervertebral foramen to form a spinal nerve. Just outside the foramen, the spinal nerve divides intoventral (1) and dorsal (2) branches. The ventral branches participate in the brachial plexus, the dorsal ones direct posteriorly tosupply the paraspinal muscles, including the multifidus (MF), the semispinalis cervicis (SS), the semispinalis capitis (SC), and thelongus colli (LC). The spinal cord, the rootlets, the ganglion, and the spinal nerve are invested by the arachnoid and dura mater(white arrow). a, vertebral artery. Note that the sixth cervical nerve leaves the intervertebral foramen superior to the transverseprocess of C6. (B) Schematic drawing of the general structure of the brachial plexus. C5, fifth nerve root; C6, sixth nerve root; C7,seventh nerve root; C8, eighth nerve root; T1, first thoracic nerve root. Moving away from the spine, C5 and C6 join to form theupper trunk, C7 continues as the middle trunk, and C8 and T1 constitute the lower trunk. Each of the trunks splits into anterior andposterior divisions that further anastomose to give origin to the lateral, medial, and posterior cords. The level of origin of the longthoracic, suprascapular, musculocutaneous, axillary, radial, ulnar, and median nerves is shown.
524 SEMINARS IN MUSCULOSKELETAL RADIOLOGY/VOLUME 14, NUMBER 5 2010
Dow
nloa
ded
by: R
utge
rs U
nive
rsity
. Cop
yrig
hted
mat
eria
l.

At the external border of the interscalene triangle,the roots unite to form three trunks: The roots of C5 andC6 join together to form the upper trunk, the root of C7continues as the middle trunk, and, in the lower neck,the roots of C8 and T1 form the lower trunk of thebrachial plexus. More distally, in the supraclavicularregion, each trunk gives off two divisional branches,named anterior and posterior divisions, which innervatethe flexor and extensor muscles of the upper extremity,respectively. In the axilla, these divisions join in variouscombinations to form the cords of the brachial plexus.The lateral cord is formed by the anterior division of theupper and middle trunks, the medial cord by the anteriordivision of the lower trunk, and the posterior cord by theposterior divisions of all the trunks. Distal to the
pectoralis minor muscle, the cords continue as the fiveperipheral nerves of the upper limb. The axillary andradial nerves originate from the posterior cord, themusculocutaneous and part of the median nerve arisefrom the lateral cord, whereas the other contributions offibers to the median nerve and the ulnar nerve originatefrom the medial cord.
Clinically relevant spaces along the course ofbrachial plexus nerves are (1) the interscalene triangle,(2) the costoclavicular space, and (3) the retropectoralisminor space (subcoracoid tunnel).12 The interscalenetriangle is bordered by the anterior and middle scalenemuscles on each side and the first rib inferiorly(Figs. 2A, B). The subclavian artery travels throughthe lower part of this space, and the lower trunk of the
Figure 2 Brachial plexus anatomy: interscalene triangle. (A) Schematic drawing illustrates the trunks as they exit theinterscalene space, a passageway delimited by the anterior scalene (AS), the middle scalene (MS), and the first rib. The trunksare located superior to the subclavian artery (white arrow). Note the phrenic nerve (arrowhead) as it winds through the anteriorscalene muscle. The posterior scalene muscle (PS) is also demonstrated in close proximity to the middle scalene. Black arrow,subclavian vein. (B) Cadaveric view shows the brachial plexus trunks passing through the interscalene triangle. The phrenic(arrowheads) and the suprascapular nerves are demonstrated in relationship to the nerve trunks. (C) Sagittal turbo spin-echo T1-weighted image of the interscalene space reveals the roots from C5 through T1 as aligned hypoechoic dots passing deep to theanterior scalene muscle and posterior to the subclavian artery (SA). (D) Oblique transverse ultrasound image demonstrates thebrachial plexus nerves as hypoechoic dots embedded in the hyperechoic fatty space lying between the scalene muscles. Themore external the nerve bundles, the higher the level of the plexus. SCM, sternocleidomastoid muscle.
BRACHIAL PLEXUS AND NERVES ABOUT THE SHOULDER/MARTINOLI ET AL 525
Dow
nloa
ded
by: R
utge
rs U
nive
rsity
. Cop
yrig
hted
mat
eria
l.

plexus crosses the inferior part of the triangle behindthe subclavian artery. This space may be responsible forupper extremity neurovascular compression. A narrowtriangle may often be due to anatomical variants ofsize, shape, and attachment of the scalene muscles onthe first rib, and they can cause a scissoring effect onthe plexus nerves and the vessels.12,13 Distal to theinterscalene triangle, the costoclavicular space is atriangular space bounded anteriorly by the inner halfof the clavicle, underlying the subclavius muscle andthe costoclavicular ligament, and posteromedially bythe first rib and insertion of the anterior and themiddle scalene muscles (Figs. 3A, B). In this space,neurovascular compression may occur as a result ofcongenital or acquired changes in the clavicle and first
rib, structural changes in the subclavius muscle, changein shoulder position, and trauma.12,13 Crossing downthe clavicle, the nerve cords enter the retropectoralisminor space (Figs. 4A, B). During upper limb eleva-tion, the cords may lean tightly against the posteriorside of the pectoralis minor, which may be predispos-ing to compression, especially in short, stocky muscularyoung men, leading to numbness and tingling in thehands and weakness in the arms during hyperabduc-tion. The most common anatomical variants of bra-chial plexus nerves are the passage of the C5 rootcompletely in front of (3%) or piercing (13%) theanterior scalene muscle and the course of the C8 andT1 roots behind the middle scalene muscle rather thanpassing anterior to it.14,15
Figure 3 Brachial plexus anatomy: costoclavicular space. (A) Schematic drawing illustrates the relevant anatomical structuresof the costoclavicular space, a rectangular passageway delimited by the clavicle (1) and the first rib (2). Note the insertion of theanterior (4) and middle (3) scalene muscles on the first rib, the transversely oriented subclavius muscle (5), and, in a more medialposition, the costoclavicular ligament (6), also known as the rhomboid ligament. The fascicles of the different nerve cords(arrow) and the subclavian artery (A) cross this space passing between the scalene muscles and underneath the subclavius. Thesubclavian vein (V) runs more anteriorly. (B) Cadaveric slice in the short axis of the costoclavicular space with (C), correspondingT1-weighted turbo spin-echo magnetic resonance image demonstrates the nerve cords (arrows), the subclavian artery (A) andvein (V) between the clavicle and the first rib. Note the subclavius (5) and the pectoralis major (PMj).
526 SEMINARS IN MUSCULOSKELETAL RADIOLOGY/VOLUME 14, NUMBER 5 2010
Dow
nloa
ded
by: R
utge
rs U
nive
rsity
. Cop
yrig
hted
mat
eria
l.

MAGNETIC RESONANCE IMAGINGTECHNIQUEMR imaging of the brachial plexus is best performed byusing a multielement phased-array radiofrequency re-ceiver coil to span the neck-to-shoulder area with theaim of imaging either the right or the left plexus at highspatial resolution, rather than a bilateral examinationwith lower resolution.16 For imaging the preganglionicsegment of brachial plexus nerves, gadolinium (Gd)-enhanced MR imaging and three-dimensional (3D)heavily T2-weighted MR imaging with fat- and flowsuppression (MR myelography) are the most valuabletechniques for identifying root avulsions and pseudome-ningoceles.17 Concerning the rootlets, the ganglionicarea and initial segment of the roots, MR myelographyhas become the reference modality in the last few years,limiting the use of CT myelography to patients with
contraindications to MR imaging or whenever MRimaging provides insufficient preoperative data.1
Compared with CT myelography, MR myelog-raphy is noninvasive, does not use ionizing radiation, andis superior to depict pseudomeningoceles because someof them do not communicate with the dural sac andcannot be filled in with contrast medium.6 For theexamination of the postganglionic plexus, a comprehen-sive MR imaging examination should extend from thecervical spine to the cords in the axilla, just distal to thepectoralis minor muscle16 (Fig. 5). At field strengthsfrom 1T to 3T, the brachial plexus can be evaluatedbased on its appearance on T1- and T2-weighted imageswith flow compensation.
Concerning sequence protocols, standard 2Dturbo spin-echo (TSE) sequences are valuable to gen-erate images with T1 contrast. These images display
Figure 4 Brachial plexus anatomy: retropectoralis minor space and axillary region. (A) Schematic drawing with (B), anatomiccorrelation, illustrates the arrangement of the lateral (LC), medial (MC), and posterior (PC) cords of the plexus relative to theaxillary artery (A), the coracobrachialis (CoB), and the pectoralis minor (Pmin) muscle. Note the origin of the axillary,musculocutaneous, radial, medial (MN), and ulnar (UN) nerves. (C) Oblique sagittal T1-weighted turbo spin-echo magneticresonance image of the retropectoralis minor space. Deep to the pectoralis major (PMj) and minor (Pmin) muscles, the positionof the LC, MC, and PC cords of the plexus relative to the axillary artery (A) and vein (V) is shown. (D) Corresponding ultrasoundimage depicts the hypoechoic fascicles of the different nerve cords distributed around the axillary artery.
BRACHIAL PLEXUS AND NERVES ABOUT THE SHOULDER/MARTINOLI ET AL 527
Dow
nloa
ded
by: R
utge
rs U
nive
rsity
. Cop
yrig
hted
mat
eria
l.

nerves as linear low signal intensity structures outlinedby surrounding fat and allow assessment of their rela-tionship with relevant regional structures, includingbones, muscles, and blood vessels18 (Figs. 2C, 3C, 4C,and 5). Fluid-sensitive sequences with T2 contrastincluding fat-suppressed T2-weighted TSE or shorttau inversion recovery (STIR) sequences are then ob-tained to detect pathological changes within plexuscomponents. Although STIR sequences are able togive more uniform and consistent suppression of fatsignal across the field of view (FOV), they have lowersignal-to-noise ratio, are more sensitive to blood flowartifacts, and allow acquisition of a lower number ofslices rather than TSE T2-weighted sequences.18 Onfat-suppressed TSE T2-weighted images, shimming ofthe magnetic field over the volume encompassing theregion of interest may be helpful to reduce areas ofincomplete suppression of fat signal or with watersaturation rather than fat saturation. Placing a bagcontaining clay suspensions against the ipsilateral neckand suprascapular region has also been proposed toreduce magnetic susceptibility effects. MR imagingtypically includes true coronal planes over the neck-to-shoulder area using a wide FOV and double oblique(oblique-sagittal oblique-coronal) planes oriented in thetrue short-axis of brachial plexus nerves.11 These latterplanes are acquired with a smaller FOV. Instead of truesagittal images, double oblique planes can better approx-imate the real cross-section of brachial plexus fascicles,offering a better display of subtle nerve abnormalities.
On T2-weighted images, obliquely oriented saturationbands over the heart and thoracic aorta may contribute tofurther improve MR image quality by arterial flowsaturation. 3D acquisitions have recently been imple-mented to image the plexus, including CISS 3D, truefast imaging with steady-state precession 3D, and 3DSTIR sequences.19–22
As technology advances, these sequences and newones in progress are increasingly gaining ground toprovide a more flexible delineation of the out-of-planecourse of brachial plexus nerves. The image data set ofthese sequences, with <1 mm isotropic resolution, canbe reformatted in any plane, regardless of the prescribedplane during the image acquisition, thus allowing visual-ization of long nerve segments in a single image andgiving better depiction of diffuse pathological processesaffecting them. In specific clinical settings (e.g., sus-pected tumors, radiation injury, neuritis, or after regionalsurgery), Gd-enhanced fat-suppressed TSE T1-weighted sequences can be used.18,23
Diffusion tensor imaging (DTI) with tractogra-phy has recently been proven to provide indirect 3Dimages of nerves.24 However, the application of DTI toget reproducible tracking of brachial plexus fibers ap-pears to be technically challenging due to the small sizeof nerves, the changing orientation of the fibers, thepeculiar location of the plexus between the neck and theshoulder, where relevant geometric distortion and arti-fact may occur, as well as the intrinsic low signal-to-noise ratio of echo-planar imaging technique.24 In addi-tion, current reconstruction algorithms are time con-suming and have poor reproducibility.
Concerning image parameters, an in-plane reso-lution of 2 mm2 with 3-mm slice thickness providessufficient signal-to-noise ratio for brachial plexus trac-tography. In perspective, DTI is the only method that canoffer an indirect view of the nerve microstructure inaddition to the information on fibers trajectory. WithDTI, nerves are depicted because water diffusion pref-erably follows the long axis of the fibers and is restrictedtransversely (inherent anisotropic diffusion). Similar toother nerves, the representation of brachial plexus nerveswith this technique reflects lines of fast water diffusionthat probably give a representation of the axonal archi-tecture and transport25 (Fig. 6). Tractography is a prom-ising method to visualize the 3D course of brachial plexusnerves and provide important information about the siteof swelling and loss of water due to nerve abnormalities orentrapment.26 Further experience is needed, however, tosolve technical challenges and evaluate the ultimate roleof this technique for brachial plexus imaging.
ULTRASOUND SCANNING TECHNIQUEUS has recently proved to be an effective means todepict normal brachial plexus anatomy at several levels,
Figure 5 Normal brachial plexus. Coronal T1-weightedturbo spin-echo magnetic resonance image of a normalbrachial plexus (outlined arrows) using a wide field of viewand phased array coil. The numbers indicate the approximatesagittal locations for the roots (1), trunks (2), divisions (3),cords (4), and peripheral nerves (5). The divisions and cordsrun alongside the subclavian/axillary artery (a).
528 SEMINARS IN MUSCULOSKELETAL RADIOLOGY/VOLUME 14, NUMBER 5 2010
Dow
nloa
ded
by: R
utge
rs U
nive
rsity
. Cop
yrig
hted
mat
eria
l.

including the paravertebral area, the interscalene tri-angle, the supraclavicular region, and the retropector-alis minor space.11,27–32 The US examination ofbrachial plexus nerves is based on detection of someanatomical landmarks in the neck, including bones(roots), muscles (trunks), and vessels (divisions andcords). As the roots exit the neural foramina, they slidebetween two apophyses of the transverse processes ofthe cervical vertebrae, the anterior and posterior tu-bercles (Fig. 7). Each root emerges from the foramen asa monofascicular hypoechoic structure, an appearancequite different from that of nerves in the extremitiesthat is made of clusters of hypoechoic fascicles.27,31
Imaging based on scanning planes is ideal todepict the relationship of the roots with the transverseprocesses at any given level. Based on the peculiarappearance of the transverse process of C7, in whichthe posterior tubercle is absent, US is able to establishthe level of nerve roots.31 The scanning technique must
be systematic and should reveal the C7 vertebra as thefirst landmark. The C7 root is detected on the sameplane of the C7 vertebra because it is bordered bythe posterior tubercle only. Given that, the probe maymove either up or down on axial planes depending on theroot the examiner wants to image.31 Shifting the probeupward, the C6 vertebra is recognized due to thepresence of prominent anterior and posterior tubercles:The C6 root appears as a hypoechoic structure held inbetween them. The transverse processes of C5 havebasically the same shape of C6 and can be identified asthe successive step cranial to the C6 level by taking intoaccount the number of transverse processes encounteredwhile sweeping the transducer cranially from C7. As arule, the higher the level, the closer the space interveningbetween the tubercles. Shifting the probe downwardfrom C7, the lateral aspect of the T1 vertebra appearsflat without any tubercle; at this level, the C8 root can beappreciated while exiting the foramen. More caudally,visualization of the T1 root is unfeasible with US due toa problem of access related to a too deep location of theintervertebral foramen between the T1 and T2 vertebraand the interposition of the first rib. In the paravertebralarea, coronal planes are able to depict the nerve rootsusing the same scanning planes for the study of vertebralvessels. On these planes, the picture of vertebral vessels isobscured at regular intervals by the acoustic shadowingfrom the anterior tubercles of the transverse processes.Moving the transducer slightly on the back, the vesselsdisappear and the roots appear as curved elongatedhypoechoic images exiting the neural foramina anddescending the lateral neck spaces. At the level of theinterscalene triangle, the roots appear as aligned hypo-echoic dots passing between the anterior and middlescalene muscles (Fig. 2D). In this space, the mostsuperficial fascicles belong to C5 and the deepest to C8.
The ability of US to recognize the exact level ofthe roots in the paravertebral area also leads to a con-fident identification of the trunks by simply followingthe nerve bundles from where they arise. Between theinterscalene triangle and the costoclavicular space, thedivisions and the initial part of the cords are visualized asa cluster of hypoechoic rounded images, most of whichrunning alongside the posterior aspect of the subclavianartery, just over the first rib and the apical pleura. Thedorsal scapular artery, a small vessel arising from thesubclavian artery, may be seen encroaching the nervedivisions and cords in the supraclavicular region. Thisvessel may pass posterior to or among the fascicles, inthis latter case forming a cleavage plane that is frequentlylocated between the middle and the lower plexus com-ponents. More distally, the costoclavicular space is blindto US examination due to the interposition of theclavicle and the lack of an acoustic window. The inabilityto image this important space represents one of the mainlimitations of a US approach. Crossing down the
Figure 6 New magnetic resonance imaging techniques.(A) Coronal reformatted diffusion-weighted image showsnerves of the brachial plexus. On either side, the nerve roots(arrowheads) are depicted as individual structures. Dorsalganglia (arrow) are also seen as a series of paraforaminalnodular swellings. (B) Coronal view of the spine and brachialplexus nerves imaged with diffusion tensor imaging tracto-graphy in a volunteer showing the three-dimensional courseof the brachial plexus nerves from the C5 through C8 level.
BRACHIAL PLEXUS AND NERVES ABOUT THE SHOULDER/MARTINOLI ET AL 529
Dow
nloa
ded
by: R
utge
rs U
nive
rsity
. Cop
yrig
hted
mat
eria
l.

clavicle, in the retropectoralis minor space, the nervecords continue their course around the axillary artery.11
The fascicles belonging to the posterior cord coursebehind the artery; the lateral cord runs external and themedial cord internal to it (Fig. 4D). On short-axisplanes, the axillary artery is the main landmark toidentify the nerves in this area. This arrangement ismaintained across these spaces like a ‘‘three-point’’ starwith the artery centered in the middle.
Finally, the examination of the most distal part ofbrachial plexus nerves is completed using an axillaryapproach as these nerves assume a deeper course. Espe-cially in overweight people or patients with hypertro-phied regional musculature, the nerves in the axillaryarea may be too deep and undefined using an anteriorapproach. With an axillary approach, nerves appear moresuperficial in this area and can be accurately evaluated.US scanning should first start at the proximal arm toidentify the median, ulnar, and radial nerves as theysurround the brachial artery. Then the probe is swept upalong the short axis of the nerves to reach the distal partof the cords.
TRAUMATIC PLEXOPATHIESClosed brachial plexus injuries are relatively infrequent,affecting!1% of all multitrauma patients and approach-ing 5% in high-velocity motor vehicle accidents, primar-ily motorcycle accidents, but result in debilitatingconsequences in a patient group that is relatively
young.1,33 After traffic accidents, the second most com-mon cause is obstetric trauma that may occur frommechanical injury involving shoulder dystocia duringdifficult childbirth.34 Brachial plexus injuries are typi-cally related to a violent excessive nerve stretching as itoccurs during simultaneous traction of the arm andthrowing of the head to the opposite shoulder.33 De-pending on trauma characteristics, brachial plexus le-sions can be divided into complete (when C5 through T1components are involved) and incomplete injuries.
Incomplete injuries can be further subdivided intotwo types: upper and lower brachial plexus lesions.Upper lesions involve damage of C5 and C6 roots andlead to Erb’s palsy, producing the so-called waiter’s tipdeformity, due to loss of the external rotators of theshoulder (suprascapular, axillary), arm flexors (musculo-cutaneous), and hand extensors (radial); lower lesionsinvolve C8 and T1 either before or after they have joinedto form the lower trunk. This latter condition, known asKlumpke’s palsy, is less frequent and mainly affects theintrinsic muscles of the hand and the flexors of the wristand fingers (ulnar, median). An early assessment of theextent and severity of the injury is essential for decidingtreatment strategies.1,4
Several types of injury may occur at the brachialplexus level, including nerve stretching (neurapraxia),the most common and least severe form, rootlets avul-sion (preganglionic separation from the spinal cord),pseudomeningocele (tear in the meningeal sheatharound the nerve roots with leakage of cerebrospinal
Figure 7 Normal brachial plexus. (A) Transverse ultrasound image over the left anterolateral neck demonstrates the mainlandmarks for identification of the nerve roots. Note the position of the left lobe of the thyroid (Thy) and the common carotidartery (CA) located between the superficial sternocleidomastoid (scm) and the deep longus colli (lc) muscles. Deep to thesestructures, the lateral aspect of the C6 vertebra shows a wavy hyperechoic contour that delineates the vertebral body (1), thepedicle (2), and the transverse process (3), which exhibits in turn two prominent anterior (4) and posterior (5) tubercles. The C6root (arrow) appears as a hypoechoic image lying in between these tubercles. (B) Cadaveric slice shows the relevant anatomicalstructures depicted in (A) including the common carotid artery, the longus colli muscle, and the transverse process of the C6vertebra, characterized by anterior and posterior tubercles. Note the nerve root (arrow) located in between the tubercles, thesuperficial internal jugular vein (IJV) and the vertebral artery (VA) in a deeper position.
530 SEMINARS IN MUSCULOSKELETAL RADIOLOGY/VOLUME 14, NUMBER 5 2010
Dow
nloa
ded
by: R
utge
rs U
nive
rsity
. Cop
yrig
hted
mat
eria
l.

fluid), and postganglionic injury (discontinuity of thebrachial plexus nerves distal to the ganglion). Differ-entiation between intraspinal nerve root avulsion, theso-called preganglionic injuries, from extraforaminallesions, or postganglionic injuries is aided by electro-physiological studies based on detection of abnormalitiesin the paraspinal muscles, and especially the multifidus,in injuries located proximal to the brachial plexus.35 Asubstantial number of root avulsions occur, however,without denervation signs in the paraspinal musclesdue to the multisegmental level of innervation of thesemuscles. Somatosensory evoked potentials can be used todiagnose intraforaminal nerve injuries, but because thesedo not enable physicians to discriminate between in-complete avulsions and intact roots or between intra-foraminal root avulsion and rootlet avulsion from thespinal cord, conventional MR imaging and myelo-graphic techniques based on CT/MR imaging play animportant role in the diagnostic workup.1,4
The first task of imaging is distinguishing intra-spinal nerve root avulsion, the so-called preganglionicinjuries, from extraforaminal lesions, or postganglionicinjuries because the surgical treatment differs in eachcase.4,36 In preganglionic injuries, the lesion is intra-dural and located proximal to the dorsal root ganglion.Despite some attempts to subdivide these lesions intocentral and peripheral, in most cases they are notconsidered amenable to direct repair and the prognosisis unfavorable.37 Nerve transfers are usually performedto restore function, using intercostal transfer to themusculocutaneous to regain elbow function or spinalaccessory to suprascapular to reestablish flexion. Incervical nerve root avulsion, the finding of a traumaticpseudomeningocele indicates an extradural collectionof cerebrospinal fluid due to laceration of the duralsleeve17 (Fig. 8). This is the main landmark thatindicates a preganglionic injury is present, althoughpseudomeningocele may occur without nerve root
Figure 8 Pseudomeningocele. (A, B) Twenty-six-year-old man with a traumatic pseudomeningocele after a motorcycleaccident. (A) Axial turbo spin-echo (TSE) T2-weighted magnetic resonance (MR) image shows the retracted right C7 nerve root(outlined arrow) and the leakage of cerebral spinal fluid (arrowheads). Note mild denervation signs (white arrow) in the rightmultifidus and semispinalis capitis muscles. (B) Coronal short tau inversion recovery MR image of the distal plexus revealsa wavy appearance of the retracted nerve cords (outlined arrows). (C) Transverse TSE T1-weighted MR image and(D) corresponding three-dimensional MR myelogram in a 17-year-old young man with chronic root avulsion demonstrate aprominent pseudomeningocele (outlined arrowheads) extending laterally to form a sac (asterisk) in the postscalenic area.Observe the normal contralateral root (black arrowhead, C) at the same vertebral level.
BRACHIAL PLEXUS AND NERVES ABOUT THE SHOULDER/MARTINOLI ET AL 531
Dow
nloa
ded
by: R
utge
rs U
nive
rsity
. Cop
yrig
hted
mat
eria
l.

avulsion (!15% of cases) and, conversely, avulsion mayoccur without meningocele (20% of cases).38–40
Other signs of preganglionic injury include Gdenhancement of intradural roots, intramedullary edema(T2-weighted sequences), lateral displacement of thespinal cord, intracanal hematoma, and secondary dener-vation signs.4,41,42 These signs are found in !20% ofcases.38 Comparing the results of CT myelography andMR myelography, current literature reports that bothimaging modalities have similar sensitivity for detectingintraspinal nerve injuries.17
After excluding preganglionic injuries, an earlyassessment of the extent and severity of the injuryoutside the spine is essential for determining treatment.In contrast to preganglionic injuries, postganglioniclesions with defects in nerve continuity can be repairedwith nerve grafting that involves excision of the dam-aged segment and autograft between two nerve ends, orneurolysis to remove perineural scar and adhesions.4 Ifnerve fascicles are intact, spontaneous recovery is usu-ally expected. In postganglionic injuries, lesions mustbe further subdivided in supraclavicular and infracla-vicular based on their location.4 Preoperative electro-physiological studies are routinely performed to assessthe status of brachial plexus nerves outside the spine butoften yield ambiguous findings.2,43 Because patientssuffering from major postganglionic nerve injuries areknown to recover better if operated on early (within3 months after injury), diagnostic imaging with US andMR imaging has critical value for assessing the status ofnerves outside the neural foramina.1,4,17,43 In patientswith severe extraspinal injuries, signs of nerve disconti-nuity are most often observed (1) at the interscalenetriangle, as a result of the tethering effect exerted bythe scalene muscles on the stretched nerves; and, moredistally, (2) at the costoclavicular space, especially inpatients with clavicular fracture when bony fragmentsdirectly impinge the underlying cords. Diagnosticimaging may provide an early categorization of extra-spinal plexus pathology and define surgical candidatesby identifying the exact site of the injury, how many andwhich are the nerves involved, the severity of involve-ment, and the position of the retracted wavy nerve endsin cases of neurotmesis.
In the acute phase, the information provided byUS seems even more detailed than the one provided byMR imaging to distinguish the interrupted nerves fromthe adjacent deranged soft tissue with hemorrhage andedema.43–45 However, the interpretation of imagingfindings becomes more accurate and informative aftera few weeks when hematomas or areas of subcutaneousemphysema are reabsorbed and stump neuromas aredeveloping at the nerve ends (Fig. 9). In chronicinjuries, fibrous scar arising from damaged fasciclesmay also be seen encasing normal fascicles and causinglate worsening of symptoms (Fig. 10). At the different
levels, US and MR imaging can assess the relationshipof fibrotic areas with brachial plexus nerves. When thetraction injury is not strong enough to determinecomplete interruption of nerve bundles, segmental fusi-form thickening of the involved nerves reflecting aspindle neuroma may occur as a result of tractiontrauma (Fig. 11). Spindle traction neuromas usually
Figure 9 Acute brachial plexus injury in a 25-year-oldmotorcyclist with total plexus palsy following a traffic acci-dent. The examination was performed 1 week after trauma.(A) Long-axis ultrasound (US) image over the C5 (whitearrowheads) and C6 (outlined arrowheads) components ofthe upper trunk of the right brachial plexus. Both nerves aretransected and exhibit a wavy course. At their end, bulbousneuromas (asterisks) are starting to develop. (B) Three-dimensional gradient-recalled echo MR imaging acquisitionwith multiplanar reconstruction obtained along the axis of theright roots demonstrates discontinuity (outlined arrows) ofC5 through C8 roots. Distal to the transection level, hetero-geneous signal in the soft tissues (asterisk) of the supracla-vicular area is seen. When compared with the left side, notethe swollen appearance and more vertical course of theaffected right roots.
532 SEMINARS IN MUSCULOSKELETAL RADIOLOGY/VOLUME 14, NUMBER 5 2010
Dow
nloa
ded
by: R
utge
rs U
nive
rsity
. Cop
yrig
hted
mat
eria
l.

develop at the interscalene triangle and in the spaceintervening between it and the costoclavicular space.Depending on the severity of traction injury, a faintfascicular pattern with swollen fascicles can be stillvisible within the neuroma or a homogeneous fusiformhypoechoic mass is found in continuity with thenerve.46 In injuries associated with clavicle fracture,the involvement of the nerve cords typically occur at thecostoclavicular space (Fig. 12). Following open surgeryaround the shoulder or glenohumeral joint dislocation,the involvement of the nerve cords is found moredistally, at the level of the retropectoralis minor space.
For the diagnostic workup, a combined approachwith MR imaging and US can be used to evaluate thetraumatized patient, the first technique to evaluate thespine and the foraminal region, the second to assessthe nerves outside the spine.43 Detection of extraspinalnerve abnormalities with US may have important clinicalimplications. It may give an early assessment of the statusof the plexus in the immediate phases after the traumawhen clinical findings are not yet conclusive on whethera brachial plexus damage will require surgery. US seemsto be particularly effective in patients with supraclavic-ular postganglionic injuries, a difficult-to-explore areawith MR imaging.
NEUROGENIC THORACIC OUTLETSYNDROMEThoracic outlet syndrome is a range of disorders arisingfrom the passage of the subclavian artery and vein andbrachial plexus nerves through the three anatomicalspaces of the thoracic outlet: the interscalene triangle,the costoclavicular space, and the retropectoralis minorspace, the narrowing of which can variably lead toarterial, venous, or nervous compression.12,38,47,48 Apure neurogenic syndrome is disputed in the literature
Figure 10 Chronic brachial plexus injury in a 47-year-oldman with median nerve palsy following a closed trauma1 year before. In the last 3 months, the patient presentedprogressive worsening of pain and neurogenic symptoms inthe territory of ulnar nerve distribution. (A) Oblique sagittalturbo spin-echo T2-weighted magnetic resonance image ofthe supraclavicular space demonstrates swollen hyperin-tense cords of the plexus (white arrowhead) grouped to-gether and encased by a peripheral fibrous scar (arrows).Outlined arrowhead, subclavian vessels. (B) Correspondingshort-axis ultrasound image confirms the presence of scartissue (arrows) derived from a previous nerve injury. Withinthe scar, intact hyperechoic fascicles (arrowheads) withpreserved fascicular echotexture are seen. Cl, clavicle; sa,subclavian artery.
Figure 11 Brachial plexus injury in a 25-year-old manfollowing a motorcycle accident. (A) Long-axis ultrasoundimage of the C5 (outlined arrowheads) and C6 (white arrow-heads) roots in the paravertebral region reveals nerve ab-normalities related to a stretching injury (axonotmesis). Bothnerve roots are continuous but have wavy and irregularcontours and less defined fascicular echotexture. (B) Normalcontralateral side for comparison.
BRACHIAL PLEXUS AND NERVES ABOUT THE SHOULDER/MARTINOLI ET AL 533
Dow
nloa
ded
by: R
utge
rs U
nive
rsity
. Cop
yrig
hted
mat
eria
l.

and seems to occur more frequently at the interscalenetriangle and the costoclavicular space rather than at thelevel of the retropectoralis minor space.47,49 In manycases, the nerve involvement is not isolated but associ-ated with arterial disease, as a possible result of commonneurovascular compression and/or arterial disease caus-ing secondary disturbances in the intranervous micro-vasculature.12
The clinical diagnosis is difficult because symp-toms are vague and nonspecific. In upper plexus involve-ment, pain typically radiates in the ipsilateral neck up tothe occipital region, and it may involve the rhomboidarea, the upper pectoralis area, and the deltoid andtrapezius down to the external aspect of the arm. Lowerplexus pain distributes around the shoulder and radiatesdown the medial arm and the medial forearm, with anulnar nerve distribution.12,49 Detection of nerve com-pression is very difficult to detect with imaging modal-ities both in its isolated form or in association withvascular disease. In fact, US is unable to evaluate nervechanges about the costoclavicular space due to problemsof access of the US beam. Similarly, direct visualizationof focal swelling and signal intensity changes in the
affected nerves at the costoclavicular space is exceptionalwith MR imaging.
Some authors found good correlation betweendistortion of brachial plexus nerves seen on MR imagingand clinical symptoms.50 Using multiplanar reformattingof 3D gradient-recalled echo MR acquisitions or volu-metric CT scan with planes reconstructed in the shortaxis of the interscalene and costoclavicular spaces, imag-ing is able to directly measure the size of these spaceswith the arm alongside the body or during a posturalmaneuver, such as holding the arm 130 degrees abductedand rotated externally (Wright’s test).51,52 Patients withthoracic outlet syndrome showed a significantly smallercostoclavicular distance and a wider retropectoralis mi-nor space after arm abduction (Fig. 13A). In addition,they exhibited a thicker subclavius muscle at rest andduring postural maneuver than did normal volunteers.51
MR imaging may occasionally depict fibrous bandscausing nerve distortion.50 A hypertrophied anteriorscalene muscle, possibly accompanied by or fused witha hypertrophied middle scalene compressing the plexusagainst the first rib (scalenus anticus syndrome), can alsobe depicted on MR imaging and multislice CT.16,53 In
Figure 12 Brachial plexus injury in a 51-year-old woman who had a right clavicular fracture following a car accident andsubsequent motor and sensory disturbances in the territory of radial nerve distribution. (A) Radiograph shows right clavicularfracture with detachment of some pointed fragments (arrowheads). (B, C) Short-axis ultrasound (US) image of thesupraclavicular space obtained in (B) neutral position and (C) during external rotation of the right arm. In (B), US demonstratesthe subclavian artery (sa) and some apparently normal nerve cords (arrow). In (C), the external rotation of the arm makes theposterior cord (arrowheads) visible by displacing it from underneath the clavicle. Note the swollen and hypoechoic appearanceof this cord, partially damaged by the pointed fracture fragments. (D) Sagittal turbo spin-echo T1-weighted magnetic resonance(MR) image obtained at the fracture level reveals heterogeneous hypointense tissue (arrow) located deep to the clavicle andposterior to the subclavian artery (outlined arrowhead) and vein (white arrowhead). Coexisting deltoid (asterisk) injury is alsodepicted.
534 SEMINARS IN MUSCULOSKELETAL RADIOLOGY/VOLUME 14, NUMBER 5 2010
Dow
nloa
ded
by: R
utge
rs U
nive
rsity
. Cop
yrig
hted
mat
eria
l.

some instances, compression may be related to theanomalous insertion of the middle scalene into almostthe entire length of the first rib, thus overlapping theanterior scalene and creating a very narrow window forthe neurovascular bundle.12 In this compression, theAdson’s test is positive when the patient’s head is turnedoutward. Finally, care should be taken not to miss acervical rib or an elongated transverse process of the C7vertebra. Both structures are often associated with fi-brous bands.7,12,54 For this purpose, a plain film shouldbe always obtained before other imaging studies.
Supernumerary cervical ribs account for !0.5 to0.6% of normal people, and in more than half of the casesthey are bilateral. Conventionally, cervical ribs can begrouped into four types: type I, <2.5 cm in length; typeII, >2.5 cm with free tip; type III, full-size cervical ribwith fibrous connection to the first rib; and type IV, full-size cervical rib with a chondral attachment to the firstrib.55 Depending on the rib size, symptoms are presentalong the C7-T1 distribution with a positive Adson’stest when the patient’s head is rotated inward. In thesepatients, dynamic US may reveal a tight contact andimpingement of the nerve divisions with the tip of thecervical rib while performing the postural maneuver(Fig. 14). US has proved to be a useful tool to demon-strate cervical ribs in children, thus avoiding ionizingradiation.56
PARSONAGE-TURNER SYNDROMEParsonage-Turner syndrome, also known as ‘‘acute bra-chial plexus neuritis’’ or ‘‘neuralgic amyotrophy,’’ is a self-limiting clinical entity consisting of a sudden onset of
severe shoulder burning pain followed shortly by pro-found muscle weakness and flaccid paralysis of at leastone of the shoulder girdle muscles.57 Typically, there isno loss of sensation associated with the weakness. Thisuncommon but not rare disorder (incidence rate:1.64" 105 people) has a peak incidence between the3rd and the 5th decades and male predominance (male-to-female ratio ranges from 2:1 to 11.5:1), is oftenbilateral (a third of cases), and may mimic other morecommon pathological conditions (e.g., cervical radicul-opathy, shoulder impingement syndrome, nerve entrap-ment due to local mass effect, and rotator cuff tear).58
Although different factors, including viral infec-tion, trauma, surgery, and autoimmunity have beenimplicated to play a causative role, the precise etiologyof Parsonage-Turner syndrome still remains controver-sial.58 Electrodiagnostic studies may demonstratechanges related to acute denervation in the brachialplexus distribution, especially in the C5 and C6 terri-tory.59 The suprascapular nerve (supplying the supra-spinatus and the infraspinatus) is the most commonlyinvolved. Among other nerves of the shoulder girdle, theaxillary (deltoid and teres minor), long thoracic (serratusanterior), and musculocutaneous (coracobrachialis, bi-ceps brachii and brachialis) may be affected individuallyor in combination. Imaging studies may help confirm thediagnosis.59–61
Although US is able to suggest denervation byshowing loss in bulk and hyperechoic appearance of theaffected muscles in the absence of tendon tears, MRimaging seems more reliable and gives a comprehensiveview of the complex pattern of muscle involvement thatcharacterizes the Parsonage-Turner syndrome. It may
Figure 13 Thoracic outlet syndrome in a 24-year-old woman with neurovascular symptoms. (A) Sagittal turbo spin-echo (TSE)T1-weighted image of the costoclavicular space obtained in the short axis with arm hyperabduction reveals a reduced distancebetween the clavicle (1) and the first rib (2) with compacted neurovascular structures (outlined arrow). a, subclavian artery. (B)Magnetic resonance angiography image obtained with maximum-intensity projection reconstruction algorithm while keepingthe patient’s arm hyperabducted demonstrates flow signal in the right brachiocephalic vein (outlined arrow) but not in the rightsubclavian (arrowheads).
BRACHIAL PLEXUS AND NERVES ABOUT THE SHOULDER/MARTINOLI ET AL 535
Dow
nloa
ded
by: R
utge
rs U
nive
rsity
. Cop
yrig
hted
mat
eria
l.

also rule out cervical radiculopathy. Early MR imagingstudies demonstrate intramuscular increased T2 signalintensity as a possible result of the increased extracellularwater content and/or increased intramuscular capillaryblood volume that occur during partial denervation60,61
(Fig. 15). Later on, intramuscular fatty infiltration anddecrease in muscle bulk can be observed. In mostinstances, brachial plexus nerves retain normal size,appearance, and signal intensity. Focal areas of increasedGd enhancement and higher T2 signal intensity mayseldom be seen in the nerves supplying denervatedmuscles as a nonspecific sign of inflammation (neuritis).Prognosis is generally benign, with !75% recoverywithin 2 years, and treatment is symptomatic (analgesicdrug and physical therapy).
TUMORS AND POSTRADIATION IMAGINGBrachial plexus tumors include two main classes ofdisorder: metastatic disease and neurogenic primary
tumors.47 Concerning metastatic disease, a wide varietyof histotypes have been reported to involve the brachialplexus secondarily. Among them, breast cancer is morecommon by far, accounting for approximately <1 to1.8% of patients because one of the most relevantlymphatic drainage paths of the breast passes throughthe axillary region.62 The onset of metastatic plexusdisease varies widely with a mean of 5.5 years. MRimaging demonstrates metastases as definite space-oc-cupying lesions along the course of brachial plexusnerves, characterized by low intensity signal onT1-weighted images, increased signal intensity (higherthan that of muscle) on T2-weighted images and Gdenhancement; however, the signal intensity may vary54
(Fig. 16). Pleural and vertebral involvement can be alsoassessed with this technique. US may reveal a well-defined solid mass with irregular margins and hypoechoicechotexture encasing nerves with an abrupt nerve-to-tumor interface.44 Alternatively, the neoplasm maycause segmental thickening and hypoechoic appearance
Figure 14 Thoracic outlet syndrome in a 66-year-old woman with a cervical rib and sensory disturbances in the area of themedian nerve. (A) Schematic drawing simulates the position of a type 4 supernumerary rib (arrows). Note the interscalenetriangle delimited by the anterior scalene muscle (1), the middle scalene muscle (2), and the first rib (5). The distal tip (blackarrow) of the cervical rib protrudes within the triangle thus narrowing its space and possibly impinging the nerve roots(arrowhead). Other relevant regional structures are the posterior scalene (3), the clavicle (4), and the second rib (6). C7 and T1indicate the vertebral levels. (B) Plain film demonstrates the supernumerary rib (white arrow) joining a prominent accessoryprocess (outlined arrow) of the first rib by a synchondrosis (outlined arrowhead). (C) Cranial and (D) caudal short-axis ultrasoundimages obtained over the supernumerary rib (asterisk) demonstrate the C7 root (arrow) snapping over the bone.
536 SEMINARS IN MUSCULOSKELETAL RADIOLOGY/VOLUME 14, NUMBER 5 2010
Dow
nloa
ded
by: R
utge
rs U
nive
rsity
. Cop
yrig
hted
mat
eria
l.

of the involved nerves without causing a clear masseffect.44 Satellite lymph nodes are often associated.
Distinguishing between metastatic plexopathy andradiation injury is critical to determine both prognosis andtreatment, but the distinction is not easy to make, andboth electrophysiology and imaging studies have met withlimited success.7 The incidence of radiation-inducedbrachial plexopathy is significantly higher when the axil-lary dose of radiation therapy is >60 Gy.62 The dosealone, however, does not determine whether a givenpatient will develop radiation damage: the treatmenttechnique and the concomitant use of chemotherapyseem also to play a role. Sensory symptoms, such asnumbness and paresthesias (55%) along with swellingand weakness of the arm (45%), are the initial symptomsin patients with radiation plexopathy. In contrast, pain is
the presenting symptom in 98% of patients with meta-static plexopathy.62,63 Based on location, the upper plexus(C5-C6) seems more frequently involved in radiationinjury, the lower trunk (C8-T1) in metastatic disease.62
Horner’s syndrome is also more likely found in metastaticplexopathy rather than in radiation disease. In radiationplexopathy, MR imaging reveals diffuse thickening of theinvolved nerves without a focal mass and soft tissuechanges with low signal intensity on both T1- and T2-weighted sequences.16,47,64 Gd does not help differentiatebetween tumor and radiation fibrosis because both con-ditions show some degree of enhancement.54 US demon-strates diffuse thickening of nerve fascicles in the absenceof a focal mass. Different from neoplastic infiltration, thenerve thickening is more uniform, and some faint fasci-cular pattern is preserved in radiation fibrosis.44 However,
Figure 15 Parsonage-Turner syndrome in a 40-year-old patient. (A) Photograph from above shows obvious atrophy of theright supraspinatus (1) and infraspinatus (2) muscles and winged scapula (curved arrow). The patient also had weakness of thetrapezius. (B, C) Corresponding axial fat-suppressed turbo spin-echo (TSE) T2-weighted magnetic resonance (MR) imagesreveal reduced volume and hyperintense appearance of the supraspinatus (outlined arrows) and the infraspinatus (outlinedarrowheads). (D) Oblique sagittal short tau inversion recovery MR image shows hyperintense appearance of the trapezius,supraspinatus (SS), infraspinatus (IS) relative to the subscapularis (SubS) and the teres minor (Tm).
BRACHIAL PLEXUS AND NERVES ABOUT THE SHOULDER/MARTINOLI ET AL 537
Dow
nloa
ded
by: R
utge
rs U
nive
rsity
. Cop
yrig
hted
mat
eria
l.

this finding is far from being specific to the diagnosis, andsuch a differentiation remains problematic with bothmodalities. 18F-fluorodeoxyglucose positron emission to-mography (FDG-PET) and 18FDG-CT-PET have beenused for this purpose.65,66 The results seem promising,particularly if other imaging studies are indeterminatedespite clear clinical evidence of brachial plexopathy andfor depicting metastases outside the axilla.16,65,66
Among other malignant histotypes, Pancoast’stumor (superior sulcus tumor) characteristically presentswith a syndrome of pain around the shoulder and in thearm derived from involvement of the C8, T1, and T2root distribution.54 The main features associated withthis syndrome are Horner’s syndrome (i.e., ptosis of theupper eyelid, miosis, anhydrosis, enophthalmos, and lossof ciliospinal reflex), muscle atrophy in the territory ofulnar nerve distribution, radiographic detection of anopacity at the lung apex with first rib destruction, and,
often, vertebral body involvement. 3D MR imaging andmultislice CT have markedly improved the visualizationof this tumor and its relationship with brachial plexusnerves and the subclavian vessels. Primary neurogenictumors of the brachial plexus, including neurofibromasand schwannomas, are far less common than metastaticdisorders. The MR imaging and US characteristics ofthese tumors are equal to those already described in otherlocations47 (Fig. 17). The feature of value in distinguish-ing these tumors from other soft tissue masses—andespecially from enlarged supraclavicular lymph nodes—is demonstration of the continuity between the tumorand the nerve of origin.
NERVES AROUND THE SHOULDERIn some clinical settings, other neuropathies around theshoulder may be added to the differential diagnosis list
Figure 16 Brachial plexus metastasis from breast cancer in a 65-year-old woman. (A) Oblique sagittal turbo spin-echo (TSE)T1-weighted and (B) fat-suppressed TSE T2-weighted magnetic resonance images of the infraclavicular region show aninfiltrating mass (white arrows) encasing the subclavian artery (arrowhead) and brachial plexus nerves (outlined arrow). (C)Long-axis ultrasound image demonstrates markedly swollen and hypoechoic appearance of the nerve cords (arrows) as a resultof the infiltrative spreading of cancer. Some nerve fascicles (arrowheads) are preserved and retain a normal appearance.Asterisk, subclavius muscle; cl, clavicle.
538 SEMINARS IN MUSCULOSKELETAL RADIOLOGY/VOLUME 14, NUMBER 5 2010
Dow
nloa
ded
by: R
utge
rs U
nive
rsity
. Cop
yrig
hted
mat
eria
l.

for a suspected brachial plexus disorder. A brief focus onthese frequently missed conditions affecting the supra-scapular, axillary, long thoracic, and spinal accessorynerves is therefore needed to remind the radiologist ofthese problems when evaluating patients with suspectedbrachial plexus pathology that does not fit typical diag-noses.
Suprascapular NeuropathyFrom an anatomical point of view, the suprascapular is apurely motor nerve that takes its origin from the uppertrunk (C5 and C6) of the plexus.9 It descends the neckwith an oblique lateral course passing beneath thetrapezius and the omohyoideus and enters the supra-spinous fossa through the suprascapular notch(Fig. 18A). This notch has variable shape and is roofedby the transverse scapular ligament. After crossing thisligament, the suprascapular nerve gives off motorbranches to the supraspinatus muscle. The nerve thentravels obliquely along the floor of the supraspinousfossa, deep to the supraspinatus, until !2 cm from theglenoid rim, and curves around the lateral margin of thebase of the scapular spine, an area also referred to as thespinoglenoid notch, to enter the infraspinous fossa9
(Fig. 18A). At the spinoglenoid notch, the nerve maybe roofed by the inferior transverse scapular ligament.Along its course, the suprascapular nerve is accompaniedby the suprascapular vessels.
Due to its relatively fixed position combinedwith its lying under the rotator cuff muscles, the supra-scapular nerve is particularly susceptible to compres-sion. The suprascapular notch and the spinoglenoidnotch are the most frequent sites of nerve entrapment.A narrow suprascapular notch, an abnormal transversescapular ligament, mechanical stretching of the nerveby repeated overhead activities, spinoglenoid varicos-
ities, even relatively small space-occupying lesions likeparalabral ganglion cysts, and brachial plexus disorders(Parsonage-Turner syndrome) have been reported aspotential causes of suprascapular neuropathy.9 Regard-less of the cause, if the nerve is entrapped at thesupraspinous notch, the supraspinatus and the infra-spinatus muscles undergo denervation changes. Bycontrast, if the nerve is compressed more distally, atthe spinoglenoid notch, denervation is limited to theinfraspinatus or part of it, whereas the supraspinatusremains spared. Symptoms are insidious at onset unlessthere is a history of acute trauma and may mimicglenohumeral instability. Late in the process, wastingor atrophy of the involved muscles become more easilymanifest. In many instances, however, the patient doesnot complain of weakness because of compensation ofthe posterior deltoid and teres minor.
The diagnosis of suprascapular neuropathy isessentially based on a careful and thorough history andphysical examination. Neurophysiology, includingEMG and nerve conduction studies, may help confirmthe diagnosis, but there are false negatives and it may notalways define the nature of the abnormal findings andlocalize the site of compression.67 Imaging may be usefulto evaluate patients with suprascapular neuropathy, es-pecially to determine the presence of paralabral cystscompressing the nerve and to assess the rotator cuffmuscles for atrophy.68 Paralabral cysts are usually asso-ciated with tears of the superior and posterior glenoidlabrum (from 8- to 11-o’clock positions), related to thepassage of joint fluid into the cyst through a thinpedicle.61,69,70 During their growth, paralabral cystsmay spread into the spinoglenoid notch, the suprascap-ular notch, or both, possibly causing nerve entrapmentand muscle denervation.69 US and MR imaging canidentify the cyst and recognize secondary changes ofnerve damage, including loss in bulk and echotextural/
Figure 17 Schwannoma of the brachial plexus. (A) Short-axis ultrasound (US) image over the brachial plexus in a patientpresenting with a palpable mass in the supraclavicular region. Note a solid hypoechoic mass (asterisk) located posterior to theaxillary artery (ax). The mass is surrounded by intact nerve fascicles (arrowheads) and, on long-axis planes (not shown), was incontinuity with one of them. (B) Correlative turbo spin-echo (TSE) T1-weighted and (C) fat-suppressed TSE T2-weighted imagesshow the mass (asterisk) in close relationship with the axillary artery (arrow).
BRACHIAL PLEXUS AND NERVES ABOUT THE SHOULDER/MARTINOLI ET AL 539
Dow
nloa
ded
by: R
utge
rs U
nive
rsity
. Cop
yrig
hted
mat
eria
l.

signal intensity changes in the innervated muscles due toedema and fatty replacement54 (Fig. 18B). The continu-ity of the cyst with a defect in the labrum can be revealedwith these techniques as well. A direct correlation hasbeen found between the size of paralabral cysts and the
onset of denervation symptoms, with an average volumeof the cysts causing muscle denervation significantlygreater (6.0 cm3 versus 2.2 cm3 of all other paralabralcysts).69 Due to their deep location, depiction of parala-bral cysts requires a careful scanning technique withUS.71 Varicose veins in the spinoglenoid notch is themain differential diagnosis. Although enlarged spino-glenoid notch veins look like a cyst because they appearas fluid-filled images, they change their shape, collapsingin internal rotation of the arm and dilating maximally inexternal rotation.
Some relationship between spinoglenoid varicos-ities and suprascapular neuropathy has been sug-gested.61,68,72 It is unclear, however, if these twoentities are separate expression of a narrow suprascapulartunnel or if the varicosities may actually lead to nerveimpingement. Percutaneous needle aspiration of the cystcontent can be attempted under US guidance to treatsuprascapular nerve compression.73,74 For this purpose,repeated ‘‘to-and-fro’’ passage movements of the needletip are helpful to avoid recurrence. This procedure hasreported to lead to marked relief of symptoms in >86%of patients.74
Axillary NeuropathyThe axillary nerve arises from the posterior cord of thebrachial plexus receiving fibers from C5 and C6 levels.9
It travels below the coracoid process and then along theinferolateral border of the subscapularis to curve inferiorto the glenohumeral joint and pass through the quadri-lateral space, a squared passageway bounded by the longhead of the triceps medially, the surgical neck of thehumerus laterally, the teres minor cranially and the teresmajor and latissimus dorsi caudally. After crossing thisspace, the axillary nerve enters the posterior aspect of theshoulder and divides into two terminal branches: ante-rior and posterior. The anterior branch supplies theanterior and middle deltoid muscle and overlying skin;the posterior branch innervates the teres minor and theposterior deltoid muscle and distributes to the skinoverlying the distal deltoid and the proximal triceps9
(Figs. 19A, B). Along its course, the nerve is accom-panied by the posterior circumflex artery. The axillaryneuropathy may be secondary to stretching injures orextrinsic compression in the quadrilateral space causedby humeral fractures, improper use of crutches, casts,fibrous bands, space-occupying masses, and inferiorparaglenoid cysts (from the 9- to 7-o’clock positions).9,61
Iatrogenic nerve damage during arthroscopic proceduresaround the coracoid or by posterior surgical arthroscopicportals has been reported.9 When entrapment of theaxillary nerve occurs in the quadrilateral space, there isselective denervation of the teres minor muscle becausethe anterior branch of the nerve (supplying the deltoid) isspared.
Figure 18 Suprascapular nerve. (A) Schematic drawingillustrates the anatomy of the suprascapular nerve as seenfrom the posterior aspect of the shoulder. Note the nerve(arrowheads) traveling under the transverse scapular liga-ment (1) at the supraspinous notch and then under thespinoglenoid ligament (2) at the spinoglenoid notch. Thenerve gives off branches for the supraspinatus (a) in thesupraspinous fossa and for the infraspinatus (b) in the infra-spinous fossa. Along its course, the nerve is accompanied bythe suprascapular artery (arrows). (B) Axial fat-suppressedturbo spin-echo T2-weighted magnetic resonance image ofthe shoulder in a 43-year-old manual worker with chronicshoulder pain. A ganglion cyst (asterisk) is shown in thespinoglenoid notch causing selective denervation of theinfraspinatus muscle (arrows).
540 SEMINARS IN MUSCULOSKELETAL RADIOLOGY/VOLUME 14, NUMBER 5 2010
Dow
nloa
ded
by: R
utge
rs U
nive
rsity
. Cop
yrig
hted
mat
eria
l.

The axillary neuropathy may be discovered inci-dentally during routine examination of the shoulderbecause the action of the teres minor cannot be clearlyseparated from the contribution of the infraspinatus.This would suggest that the disease may exist in asubclinical form. When symptomatic, the axillary neuro-pathy presents with vague, often nonspecific, posteriorshoulder pain, sensory disturbances over the externalaspect of the shoulder, and weakness exacerbated byoverhead activity and heavy lifting. Even without anydetectable soft tissue abnormality along the nerve course,the imaging diagnosis of axillary neuropathy is based onthe evidence of volume loss and echotextural/signal
changes of the involved muscles in the absence of atendon tear (Figs. 19C, D). MR imaging is superior toUS to depict any space-occupying lesion in the quadri-lateral space, such as paralabral cysts extending off theinferior aspect of the glenoid in association with a tear ofthe inferior labrum.71,75,76
Long Thoracic NeuropathyFrom an anatomical point of view, the long thoracicnerve takes its origin from C5 through C7 and occa-sionally (8%) C8.10 After traveling anteriorly to theposterior scalene muscle, it traverses distally and laterally
Figure 19 Axillary nerve. Schematic drawings illustrate the anatomy of the axillary nerve in relation to some relevant musclesof the shoulder girdle and the quadrilateral space as seen from (A) the anterior and (B) the posterior aspect of the shoulder. Afterarising from the posterior cord of the brachial plexus, the axillary nerve (arrow) traverses the inferior border of the subscapularismuscle (2) and then passes through the quadrilateral space, a narrow passageway delimited by the humerus, the teres major(3), the long head of the triceps (4), and the teres minor (5) muscles to enter the posterior aspect of the shoulder. The axillarynerve splits into an anterior branch (black arrowhead) that provides motor supply to the anterior and middle parts of the deltoid(1), and a posterior branch (outlined arrowhead) that supplies the teres minor and the posterior part of the deltoid continuingdown as the superior lateral cutaneous nerve of the arm. Along its course, the nerve is accompanied by the posterior circumflexartery. (C) Sagittal ultrasound image over the infraspinous fossa in a 35-year-old professional volleyball player with axillaryneuropathy. Note the atrophy of the deltoid and teres minor compared with the infraspinatus. The teres minor appearshyperechoic as a result of fatty replacement. (D) Oblique sagittal short tau inversion recovery magnetic resonance imagereveals intramuscular edema with increased signal intensity in the deltoid (1) and teres minor (5).
BRACHIAL PLEXUS AND NERVES ABOUT THE SHOULDER/MARTINOLI ET AL 541
Dow
nloa
ded
by: R
utge
rs U
nive
rsity
. Cop
yrig
hted
mat
eria
l.

to pass below the clavicle and under the first and thesecond rib. More distally, the long thoracic nerve de-scends along the chest wall in the midaxillary line to theouter border of the serratus anterior, sending branches toeach of the digitations of this muscle10 (Fig. 20A). Theserratus anterior, which forms the medial wall of theaxilla, originates from the first through ninth ribs andinserts into the costomedial border of the scapula. It actsas a stabilizer of the scapula during the initial stages ofabduction (Fig. 20B).
Long thoracic neuropathy most often derivesfrom repeated microtrauma as a result of a stretching
injury. This typically occurs in athletes (e.g., throwingsports like baseball, javelin, or when spiking or serving avolleyball or a tennis ball) when the head is tilted androtated laterally away from the affected extremity andthe arm is raised overhead.10 Direct trauma over theupper anterior chest and whiplash injury may also causenerve compression.77 Nontraumatic causes include com-pression by distended bursae, such as the subcoracoidbursa or the subscapularis recess. Regardless of thepathomechanism, it is still unclear where the injuryoccurs along the course of the nerve. Physical examina-tion reveals a distinct clinical picture with scapular
Figure 20 Long thoracic nerve. (A) Schematic drawing illustrates the anatomy of the long thoracic nerve. After branching offbefore the brachial plexus, note the long thoracic nerve (arrows) piercing the middle scalene muscle (MS) and then becomingsubcutaneous about the level of the first or second rib and sending off branches to the different digitations (asterisks) of theserratus anterior muscle. AS, anterior scalene muscle; I–IV, rib levels. (B) Schematic drawing shows the action of the serratusanterior in stabilizing the scapula against the chest wall. Arrows, vector forces during serratus anterior muscle contraction. (C)Winged scapula in a 24-year-old woman with long thoracic nerve palsy following a car accident. Winging (arrows) involves theentire medial border of the left scapula. (D) Axial fat-suppressed turbo spin-echo T2-weighted image of the posterior chest wallobtained in the same patient shown in (B). Note increased intensity signal in the left serratus anterior muscle (white arrow)compared with the right one (outlined arrow).
542 SEMINARS IN MUSCULOSKELETAL RADIOLOGY/VOLUME 14, NUMBER 5 2010
Dow
nloa
ded
by: R
utge
rs U
nive
rsity
. Cop
yrig
hted
mat
eria
l.

winging, particularly when the patient extends his or herarms and pushes against a wall78 (Fig. 20C). Directevaluation of the long thoracic nerve is feasible only inpart and for limited segments with US. The diagnosisbasically relies on detection of denervation signs in theserratus anterior muscle. MR imaging is superior to USto recognize these signs (Fig. 20D).
Spinal Accessory NeuropathyAlthough not a true peripheral nerve, the spinal acces-sory nerve (CN XI) can be acceptably included in the listof nerves around the shoulder because it supplies thetrapezius and sternocleidomastoid. After exiting theskull through the jugular foramen, the spinal accessorynerve divides into two branches. The internal one joins
with the vagus; the external is mainly a motor nervecontaining some sensory fibers coming from C1 throughC3.10 This latter branch courses underneath the digastricand the sternocleidomastoid and, more distally, crossesin diagonal the posterior cervical triangle bordered by thesternocleidomastoid anteriorly, the trapezius posteriorly,and the clavicle caudally (Fig. 21A). In this area, thespinal accessory nerve has a superficial course beneaththe superficial cervical fascia and passes adjacent tolymph nodes. Thus it is vulnerable to blunt trauma,traction, and penetrating wounds or surgical procedures,such as radical neck dissection for neoplasm, carotidendarterectomy, and cervical lymph node biopsy.
Spinal accessory palsy causes a clinically distinctpicture resulting from the paralysis of the trapezius, withdrooping shoulder, asymmetry of the neckline, weakness
Figure 21 Spinal accessory nerve. (A) Schematic drawing shows the pertinent anatomy of the spinal accessory nerve(arrowhead) that emerges underneath the sternocleidomastoid muscle (1), becomes superficial at the posterior cervical triangle(2), and then enters and supplies the trapezius muscle (3). (B) Winged scapula in a 27-year-old woman with spinal accessorynerve palsy after cervical lymph node biopsy. Winging (arrow) involves the superomedial scapula. (C) Longitudinal ultrasoundimage obtained over the left cervical region in the same patient shown in (B). The spinal accessory nerve (outlined arrows) isseen crossing the sternocleidomastoid muscle and ending in a small fusiform neuroma (white arrow) suggesting completenerve transection.
BRACHIAL PLEXUS AND NERVES ABOUT THE SHOULDER/MARTINOLI ET AL 543
Dow
nloa
ded
by: R
utge
rs U
nive
rsity
. Cop
yrig
hted
mat
eria
l.

of forward elevation, and abduction of the arm andwinging of the scapula. Concerning this latter sign andunlike winging as seen with serratus palsy, only theinferior tip of the scapula is prominent. EMG and nerveconduction studies are helpful to diagnose accessorynerve palsy and locate the level of injury.79 US cancomplement functional studies to depict the spinalaccessory nerve through the posterior cervical triangleand is able to reveal, in pathological cases, stump neuro-mas or scarring tissue encasing it80 (Fig. 21B). For thisevaluation, US seems more accurate than MR imagingowing to a higher spatial and contrast resolution.
REFERENCES
1. Abul-Kasim K, Backman C, Bjorkman A, Dahlin LB.Advanced radiological work-up as an adjunct to decision inearly reconstructive surgery in brachial plexus injuries.J Brachial Plex Peripher Nerve Inj 2010;5:14
2. Swash M. Diagnosis of brachial root and plexus lesions.J Neurol 1986;233(3):131–135
3. Brunelli GA, Brunelli GR. Preoperative assessment of theadult plexus patient. Microsurgery 1995;16(1):17–21
4. Tavakkolizadeh A, Saifuddin A, Birch R. Imaging of adultbrachial plexus traction injuries. J Hand Surg [Br] 2001;26(3):183–191
5. van Es HW. MRI of the brachial plexus. Eur Radiol 2001;11(2):325–336
6. Yoshikawa T, Hayashi N, Yamamoto S, et al. Brachial plexusinjury: clinical manifestations, conventional imaging findings,and the latest imaging techniques. Radiographics 2006;26(Suppl 1):S133–S143
7. Demondion X, Herbinet P, Van Sint Jan S, Boutry N,Chantelot C, Cotten A. Imaging assessment of thoracicoutlet syndrome. Radiographics 2006;26(6):1735–1750
8. Vargas MI, Viallon M, Nguyen D, Beaulieu JY, Delavelle J,Becker M. New approaches in imaging of the brachial plexus.Eur J Radiol 2010;74(2):403–410
9. Safran MR. Nerve injury about the shoulder in athletes, part1: suprascapular nerve and axillary nerve. Am J Sports Med2004;32(3):803–819
10. Safran MR. Nerve injury about the shoulder in athletes, part2: long thoracic nerve, spinal accessory nerve, burners/stingers, thoracic outlet syndrome. Am J Sports Med 2004;32(4):1063–1076
11. Demondion X, Herbinet P, Boutry N, Fontaine C, FranckeJP, Cotten A. Sonographic mapping of the normal brachialplexus. AJNR Am J Neuroradiol 2003;24(7):1303–1309
12. Atasoy E. Thoracic outlet compression syndrome. OrthopClin North Am 1996;27(2):265–303
13. Demondion X, Boutry N, Drizenko A, Paul C, Francke JP,Cotten A. Thoracic outlet: anatomic correlation with MRimaging. AJR Am J Roentgenol 2000;175(2):417–422
14. Harry WG, Bennett JD, Guha SC. Scalene muscles and thebrachial plexus: anatomical variations and their clinicalsignificance. Clin Anat 1997;10(4):250–252
15. Kocabiyik N, Yalcin B, Kilic C, Ozan H. Multiple anomaliesof the brachial plexus: a case report. Neuroanatomy 2007;8:21–23
16. Bowen BC, Pattany PM, Saraf-Lavi E, Maravilla KR. Thebrachial plexus: normal anatomy, pathology, and MR
imaging. Neuroimaging Clin N Am 2004;14(1):59–85, vii–viii
17. Gasparotti R, Ferraresi S, Pinelli L, et al. Three-dimensionalMR myelography of traumatic injuries of the brachial plexus.AJNR Am J Neuroradiol 1997;18(9):1733–1742
18. Posniak HV, Olson MC, Dudiak CM, Wisniewski R,O’Malley CO. MR imaging of the brachial plexus. AJR Am JRoentgenol 1993;161(2):373–379
19. Viallon M, Vargas MI, Jlassi H, Lovblad KO, Delavelle J.High-resolution and functional magnetic resonance imagingof the brachial plexus using an isotropic 3D T2 STIR (shortterm inversion recovery) SPACE sequence and diffusiontensor imaging. Eur Radiol 2008;18(5):1018–1023
20. Stevens KJ, Busse RF, Han E, et al. Ankle: isotropic MRimaging with 3D-FSE-cube—initial experience in healthyvolunteers. Radiology 2008;249(3):1026–1033
21. Chagla GH, Busse RF, Sydnor R, Rowley HA, Turski PA.Three-dimensional fluid attenuated inversion recovery imag-ing with isotropic resolution and nonselective adiabaticinversion provides improved three-dimensional visualizationand cerebrospinal fluid suppression compared to two-dimen-sional flair at 3 Tesla. Invest Radiol 2008;43(8):547–551
22. Van Es HW, Witkamp TD, Ramos LM, et al. MR imagingof the brachial plexus using a T1-weighted three-dimensionalvolume acquisition. Int J Neuroradiol 1996;2:264–273
23. Hayashi N, Yamamoto S, Okubo T, et al. Avulsion injury ofcervical nerve roots: enhanced intradural nerve roots at MRimaging. Radiology 1998;206(3):817–822
24. Takahara T, Hendrikse J, Yamashita T, et al. Diffusion-weighted MR neurography of the brachial plexus: feasibilitystudy. Radiology 2008;249(2):653–660
25. Jones DK, Horsfield MA, Simmons A. Optimal strategiesfor measuring diffusion in anisotropic systems by magneticresonance imaging. Magn Reson Med 1999;42(3):515–525
26. Jambawalikar S, Baum J, Button T, Li H, Geronimo V,Gould ES. Diffusion tensor imaging of peripheral nerves.Skeletal Radiol 2010;39(11):1073–1079
27. Sheppard DG, Iyer RB, Fenstermacher MJ. Brachial plexus:demonstration at US. Radiology 1998;208(2):402–406
28. Yang WT, Chui PT, Metreweli C. Anatomy of the normalbrachial plexus revealed by sonography and the role ofsonographic guidance in anesthesia of the brachial plexus.AJR Am J Roentgenol 1998;171(6):1631–1636
29. Retzl G, Kapral S, Greher M, Mauritz W. Ultrasonographicfindings of the axillary part of the brachial plexus. AnesthAnalg 2001;92(5):1271–1275
30. Apan A, Baydar S, Yilmaz S, et al. Surface landmarks ofbrachial plexus: ultrasound and magnetic resonance imagingfor supraclavicular approach with anatomical correlation. EurJ Ultrasound 2001;13(3):191–196
31. Martinoli C, Bianchi S, Santacroce E, Pugliese F, Graif M,Derchi LE. Brachial plexus sonography: a technique forassessing the root level. AJR Am J Roentgenol 2002;179(3):699–702
32. Cash CJC, Sardesai AM, Berman LH, et al. Spatial mappingof the brachial plexus using three-dimensional ultrasound. BrJ Radiol 2005;78(936):1086–1094
33. Songcharoen P. Management of brachial plexus injury inadults. Scand J Surg 2008;97(4):317–323
34. Miller SF, Glasier CM, Griebel ML, Boop FA. Brachialplexopathy in infants after traumatic delivery: evaluation withMR imaging. Radiology 1993;189(2):481–484
544 SEMINARS IN MUSCULOSKELETAL RADIOLOGY/VOLUME 14, NUMBER 5 2010
Dow
nloa
ded
by: R
utge
rs U
nive
rsity
. Cop
yrig
hted
mat
eria
l.

35. Hayashi N, Masumoto T, Abe O, Aoki S, Ohtomo K, TajiriY. Accuracy of abnormal paraspinal muscle findings oncontrast-enhanced MR images as indirect signs of unilateralcervical root-avulsion injury. Radiology 2002;223(2):397–402
36. Birch R. Brachial plexus injuries. Curr Orthop 1987;1:316–323
37. Schenker M, Birch R. Diagnosis of the level of intraduralrupture of the rootlets in traction lesions of the brachialplexus. J Bone Joint Surg [Br] 2001;83:916–920
38. Aralasmak A, Karaali K, Cevikol C, Uysal H, Senol U. MRimaging findings in brachial plexopathy with thoracic outletsyndrome. AJNR Am J Neuroradiol 2010;31(3):410–417
39. Carvalho GA, Nikkhah G, Matthies C, Penkert G, Samii M.Diagnosis of root avulsions in traumatic brachial plexusinjuries: value of computerized tomography myelography andmagnetic resonance imaging. J Neurosurg 1997;86(1):69–76
40. Hashimoto T, Mitomo M, Hirabuki N, et al. Nerve rootavulsion of birth palsy: comparison of myelography with CTmyelography and somatosensory evoked potential. Radiology1991;178(3):841–845
41. Hems TE, Birch R, Carlstedt T. The role of magneticresonance imaging in the management of traction injuriesto the adult brachial plexus. J Hand Surg [Br] 1999;24(5):550–555
42. Nakamura T, Yabe Y, Horiuchi Y, Takayama S. Magneticresonance myelography in brachial plexus injury. J Bone JointSurg Br 1997;79(5):764–769
43. Gruber H, Glodny B, Galiano K, et al. High-resolutionultrasound of the supraclavicular brachial plexus—can itimprove therapeutic decisions in patients with plexus trauma?Eur Radiol 2007;17(6):1611–1620
44. Graif M, Martinoli C, Rochkind S, et al. Sonographicevaluation of brachial plexus pathology. Eur Radiol 2004;14(2):193–200
45. Haber HP, Sinis N, Haerle M, Schaller HE. Sonography ofbrachial plexus traction injuries. AJR Am J Roentgenol2006;186(6):1787–1791
46. Shafighi M, Gurunluoglu R, Ninkovic M, Mallouhi A,Bodner G. Ultrasonography for depiction of brachial plexusinjury. J Ultrasound Med 2003;22(6):631–634
47. Wittenberg KH, Adkins MC. MR imaging of nontraumaticbrachial plexopathies: frequency and spectrum of findings.Radiographics 2000;20(4):1023–1032
48. Brantigan CO, Roos DB. Etiology of neurogenic thoracicoutlet syndrome. Hand Clin 2004;20(1):17–22
49. Brantigan CO, Roos DB. Diagnosing thoracic outletsyndrome. Hand Clin 2004;20(1):27–36
50. Panegyres PK, Moore N, Gibson R, Rushworth G, DonaghyM. Thoracic outlet syndromes and magnetic resonanceimaging. Brain 1993;116(Pt 4):823–841
51. Demondion X, Bacqueville E, Paul C, Duquesnoy B,Hachulla E, Cotten A. Thoracic outlet: assessment withMR imaging in asymptomatic and symptomatic populations.Radiology 2003;227(2):461–468
52. Remy-Jardin M, Remy J, Masson P, et al. Helical CTangiography of thoracic outlet syndrome: functional anatomy.AJR Am J Roentgenol 2000;174(6):1667–1674
53. Collins JD, Shaver ML, Disher AC, Miller TQ. Compro-mising abnormalities of the brachial plexus as displayed bymagnetic resonance imaging. Clin Anat 1995;8(1):1–16
54. van Es HW. MRI of the brachial plexus. Eur Radiol2001;11(2):325–336
55. Gruber W. Ueber die halstrippen des menschen mitvergleichend-anatomischen. St. Petersburg, Russia: Bemer-kungen; 1869
56. Mangrulkar VH, Cohen HL, Dougherty D. Sonography fordiagnosis of cervical ribs in children. J Ultrasound Med2008;27(7):1083–1086
57. Parsonage MJA, Turner JW. Neuralgic amyotrophy; theshoulder-girdle syndrome. Lancet 1948;1(6513):973–978
58. Tsairis P, Dyck PJ, Mulder DW. Natural history of brachialplexus neuropathy. Report on 99 patients. Arch Neurol1972;27(2):109–117
59. Scalf RE, Wenger DE, Frick MA, Mandrekar JN, AdkinsMC. MRI findings of 26 patients with Parsonage-Turnersyndrome. AJR Am J Roentgenol 2007;189(1):W39–44
60. Gaskin CM, Helms CA. Parsonage-Turner syndrome: MRimaging findings and clinical information of 27 patients.Radiology 2006;240(2):501–507
61. Bredella MA, Tirman PFJ, Fritz RC, Wischer TK, Stork A,Genant HK. Denervation syndromes of the shoulder girdle:MR imaging with electrophysiologic correlation. SkeletalRadiol 1999;28(10):567–572
62. Kori SH, Foley KM, Posner JB. Brachial plexus lesions inpatients with cancer: 100 cases. Neurology 1981;31(1):45–50
63. Lederman RJ, Wilbourn AJ. Brachial plexopathy: recurrentcancer or radiation? Neurology 1984;34(10):1331–1335
64. Bowen BC, Verma A, Brandon AH, Fiedler JA. Radiation-induced brachial plexopathy: MR and clinical findings. AJNRAm J Neuroradiol 1996;17(10):1932–1936
65. Ahmad A, Barrington S, Maisey M, Rubens RD. Use ofpositron emission tomography in evaluation of brachialplexopathy in breast cancer patients. Br J Cancer 1999;79(3–4):478–482
66. Luthra K, Shah S, Purandare N, Medhi S, Rangarajan V,Samuel AM. F-18 FDG PET-CT appearance of metastaticbrachial plexopathy in a case of carcinoma of the breast. ClinNucl Med 2006;31(7):432–434
67. Padua L, LoMonaco M, Padua R, Gregori B, Valente EM,Tonali P. Suprascapular nerve entrapment. Neurophysiolog-ical localization in 6 cases. Acta Orthop Scand 1996;67(5):482–484
68. Ludig T, Walter F, Chapuis D, Mole D, Roland J, Blum A.MR imaging evaluation of suprascapular nerve entrapment.Eur Radiol 2001;11(11):2161–2169
69. Tung GA, Entzian D, Stern JB, Green A. MR imaging andMR arthrography of paraglenoid labral cysts. AJR Am JRoentgenol 2000;174(6):1707–1715
70. O’Connor EE, Dixon LB, Peabody T, Stacy GS. MRI ofcystic and soft-tissue masses of the shoulder joint. AJR Am JRoentgenol 2004;183(1):39–47
71. Martinoli C, Bianchi S, Pugliese F, et al. Sonography ofentrapment neuropathies in the upper limb (wrist excluded). JClin Ultrasound 2004;32(9):438–450
72. Carroll KW, Helms CA, Otte MT, Moellken SM, Fritz R.Enlarged spinoglenoid notch veins causing suprascapularnerve compression. Skeletal Radiol 2003;32(2):72–77
73. Hashimoto BE, Hayes AS, Ager JD. Sonographic diagnosisand treatment of ganglion cysts causing suprascapular nerveentrapment. J Ultrasound Med 1994;13(9):671–674
74. Chiou HJ, Chou YH, Wu JJ, et al. Alternative andeffective treatment of shoulder ganglion cyst: ultrasono-graphically guided aspiration. J Ultrasound Med 1999;18(8):531–535
BRACHIAL PLEXUS AND NERVES ABOUT THE SHOULDER/MARTINOLI ET AL 545
Dow
nloa
ded
by: R
utge
rs U
nive
rsity
. Cop
yrig
hted
mat
eria
l.

75. Cothran RL Jr, Helms C. Quadrilateral space syndrome:incidence of imaging findings in a population referred for MRIof the shoulder. AJR Am J Roentgenol 2005;184(3):989–992
76. Sofka CM, Lin J, Feinberg J, Potter HG. Teres minordenervation on routine magnetic resonance imaging of theshoulder. Skeletal Radiol 2004;33(9):514–518
77. Omar N, Alvi F, Srinivasan MS. An unusual presentation ofwhiplash injury: long thoracic and spinal accessory nerveinjury. Eur Spine J 2007;16(Suppl 3):275–277
78. Wiater JM, Flatow EL. Long thoracic nerve injury. ClinOrthop Relat Res 1999;368(368):17–27
79. Massey EW. Spinal accessory nerve lesions. Semin Neurol2009;29(1):82–84
80. Bodner G, Harpf C, Gardetto A, et al. Ultrasonography ofthe accessory nerve: normal and pathologic findings incadavers and patients with iatrogenic accessory nerve palsy.J Ultrasound Med 2002;21(10):1159–1163
546 SEMINARS IN MUSCULOSKELETAL RADIOLOGY/VOLUME 14, NUMBER 5 2010
Dow
nloa
ded
by: R
utge
rs U
nive
rsity
. Cop
yrig
hted
mat
eria
l.