Embed Size (px)
Citation preview
Bowel Preparation forColon Resection
Eric Klein, M.D.SUNY Downstate
Department of Surgery
www.downstatesurgery.org

www.downstatesurgery.org
Historical Perspective
• “During World War II, failure to treat penetrating colon injuries with diversion could result in court martial.”
Miller PR, Fabian TC, et al. Improving outcomes following penetrating colon wounds:application of a clinical pathway. Ann Surg. 2002 Jun;235(6):775-81.
www.downstatesurgery.org
Madden (1965)
• Primary resection and immediate anastomosis of perforated lesions of the colon– 85 cases from literature– 25 additional cases– 9.1% mortality
Madden JL. Primary resection and anastomosis in the treatment of perforated lesions of the colon. Amer Surg 31: 781, 1965.
www.downstatesurgery.org
Case Series (1987)
• In a series of 72 consecutive elective and emergency colectomies with primary anastomosis, all pre- and perioperative mechanical preparation of the bowel was omitted and the patient covered only by a single peroperative intravenous dose of cefuroxime and metronidazole. No anastomotic dehiscence was clinically apparent and wound infection was noted in only 8.3 per cent of patients.
Irving AD, Scrimgeour D. Mechanical bowel preparation for colonic resection and anastomosis. Br J Surg 1987; 74: 580-1.
www.downstatesurgery.org

Editorial
• “The paper which challenges accepted surgical practice, is a veritable little bomb of a paper, brief, iconoclastic, and disrespectful of hallowed tradition in colorectal surgery.”
www.downstatesurgery.org
Is Mechanical Bowel Preparation Mandatory for Elective Colon
Surgery?Ram E, Sherman Y, Weil R, Vishne T,
Kravarusic D, Dreznik Z.Arch Surg. 2005 Mar;140(3):285-8.
Israel
www.downstatesurgery.org
Colon Resections
• Excluded low LAR and surgery for polypoid lesions
• Prophylactic antibiotics (1 hour preop, 48 hours post-op)– Ceftriaxone 1g– Metronidazole 500mg
• Group 1 – Soffodex• Group 2 – No bowel prep
www.downstatesurgery.org
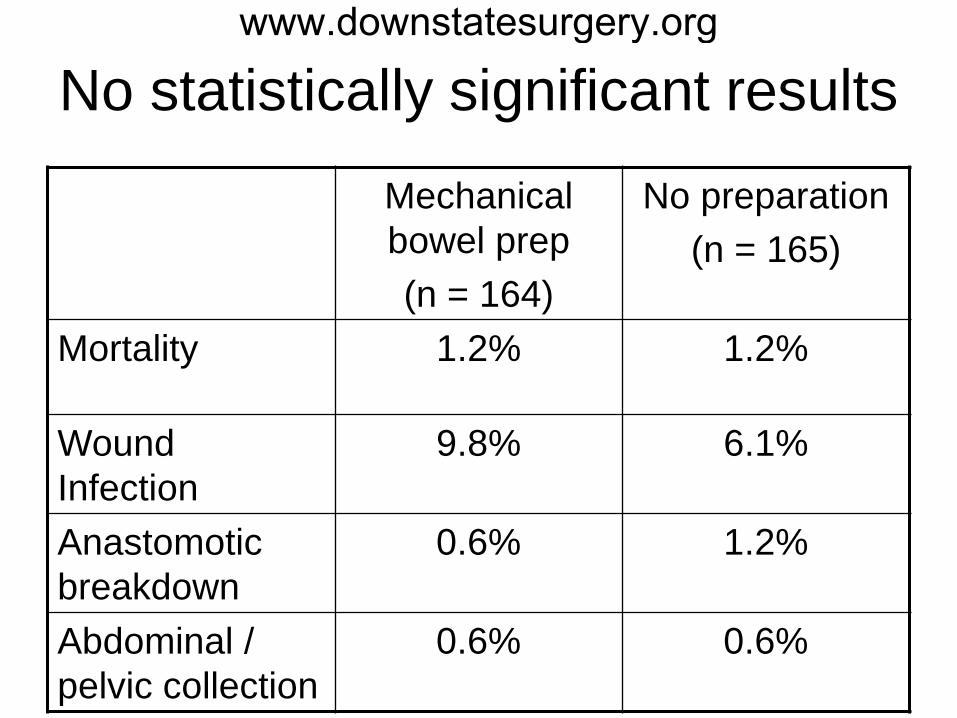
No statistically significant results
Mechanical bowel prep(n = 164)
No preparation(n = 165)
Mortality 1.2% 1.2%
Wound Infection
9.8% 6.1%
Anastomotic breakdown
0.6% 1.2%
Abdominal / pelvic collection
0.6% 0.6%
www.downstatesurgery.org
Randomized clinical trial of mechanical bowel preparation versus no preparation before elective left-sided colorectal
surgery.Bucher P, Gervaz P, Soravia C, Mermillod B, Erne M, Morel P.
Br J Surg. 2005 Apr;92(4):409-14.
Switzerland
www.downstatesurgery.org
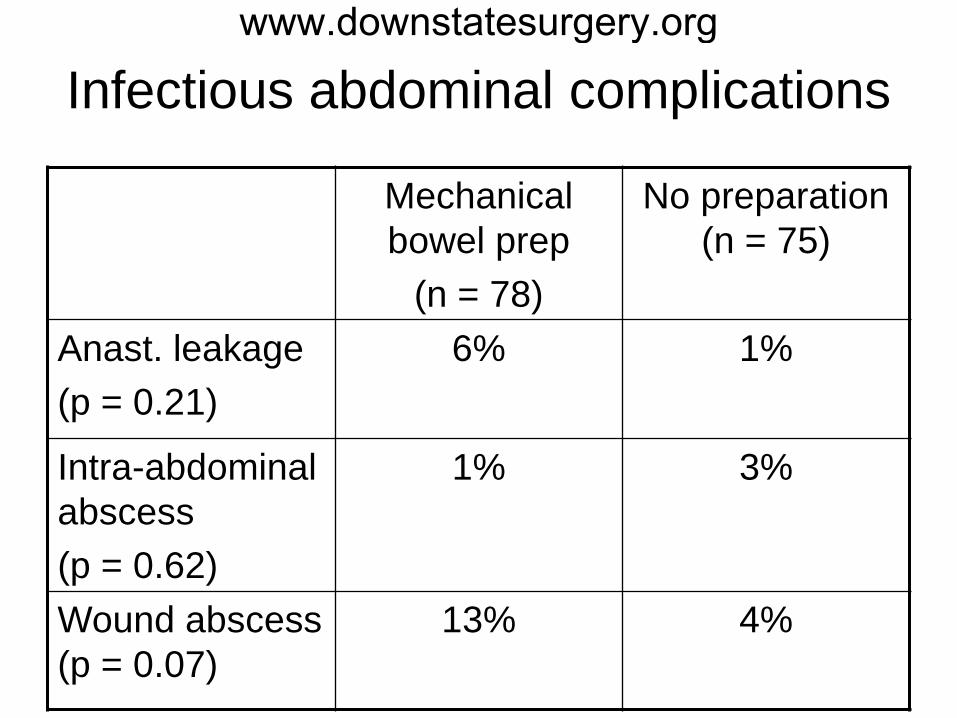
Infectious abdominal complications
Mechanical bowel prep
(n = 78)
No preparation (n = 75)
Anast. leakage(p = 0.21)
6% 1%
Intra-abdominal abscess(p = 0.62)
1% 3%
Wound abscess (p = 0.07)
13% 4%
www.downstatesurgery.org
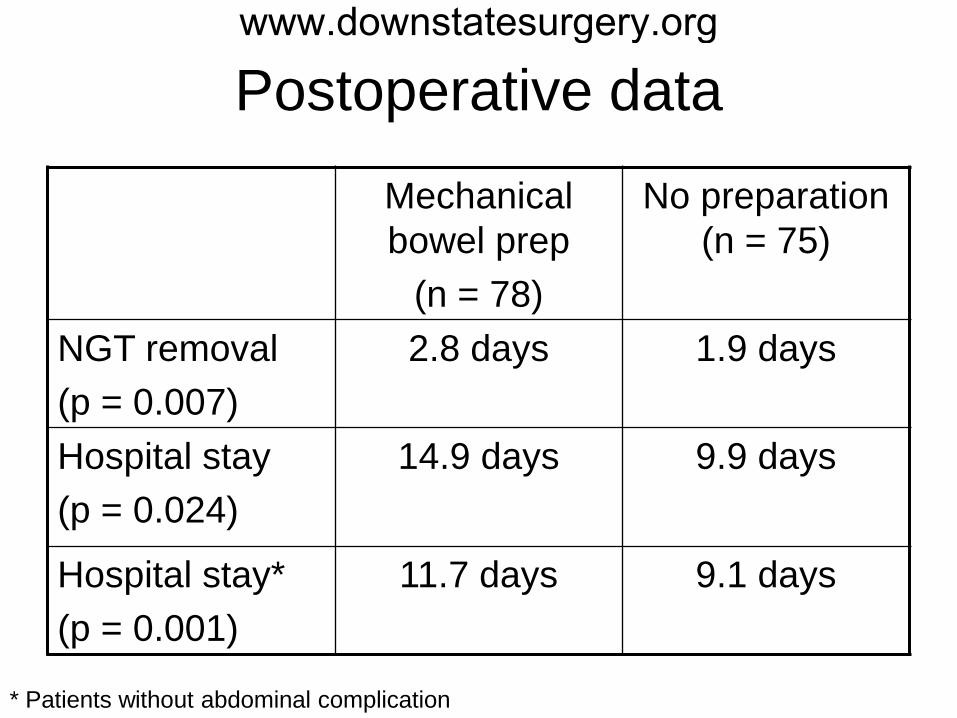
Postoperative data
Mechanical bowel prep
(n = 78)
No preparation (n = 75)
NGT removal(p = 0.007)
2.8 days 1.9 days
Hospital stay(p = 0.024)
14.9 days 9.9 days
Hospital stay* (p = 0.001)
11.7 days 9.1 days
* Patients without abdominal complication
www.downstatesurgery.org
Pre-operative mechanical bowel cleansing or not? An updated
meta-analysisWille-Jørgensen P, Guenaga KF,
Matos D, Castro AA.Colorectal Dis. 2005 Jul;7(4):304-10.
www.downstatesurgery.org
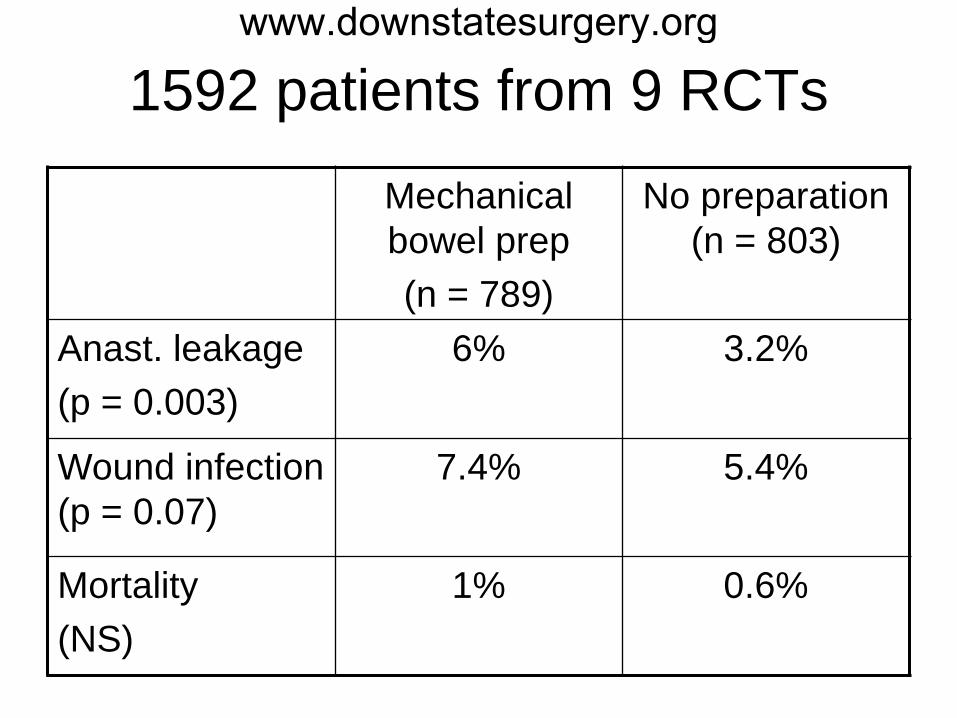
1592 patients from 9 RCTs
Mechanical bowel prep(n = 789)
No preparation (n = 803)
Anast. leakage(p = 0.003)
6% 3.2%
Wound infection (p = 0.07)
7.4% 5.4%
Mortality(NS)
1% 0.6%
www.downstatesurgery.org
Multicentre randomized clinical trial of mechanical bowel
preparation in elective colonic resection
Jung B, Påhlman L, Nyström PO, Nilsson E.
Br J Surg. 2007 Jun;94(6):689-95.
www.downstatesurgery.org
1505 patients randomized
• 1 German and 20 Swedish hospitals• Cancer, adenoma, diverticular disease• All patients had an anastomosis• All patients receieved oral or IV
prophylactic antibiotics• Bowel preparations
– Oral (polyethylene glycol or sodium phosphate)
– Some patients had a rectal enema
www.downstatesurgery.org
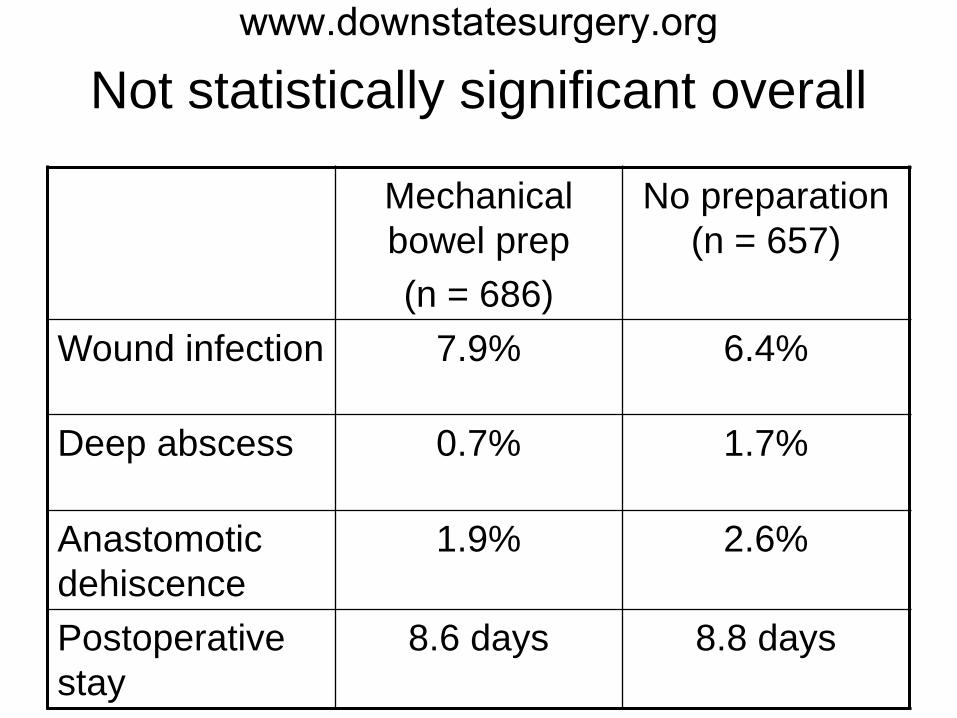
Not statistically significant overall
Mechanical bowel prep(n = 686)
No preparation (n = 657)
Wound infection 7.9% 6.4%
Deep abscess 0.7% 1.7%
Anastomotic dehiscence
1.9% 2.6%
Postoperative stay
8.6 days 8.8 days
www.downstatesurgery.org
Preoperative Oral Antibiotics in Colorectal Surgery Increases the Rate of Clostridium difficile Colitis
Wren SM, Ahmed N, Jamal A, Safadi BY.
Arch Surg. 2005 Aug;140(8):752-6.
www.downstatesurgery.org
Retrospective case-controlled
• Elective operations– Resections with or without anastomosis– Colostomy formation– Colostomy takedown
• Exclusions– C. diff within 30 days prior to surgery– bowel obstruction– < 30 day follow-up (or survival)
www.downstatesurgery.org
Bowel Preparation
• All patients received mechanical bowel preparation
• All patients received prophylactic IV antibiotics
www.downstatesurgery.org
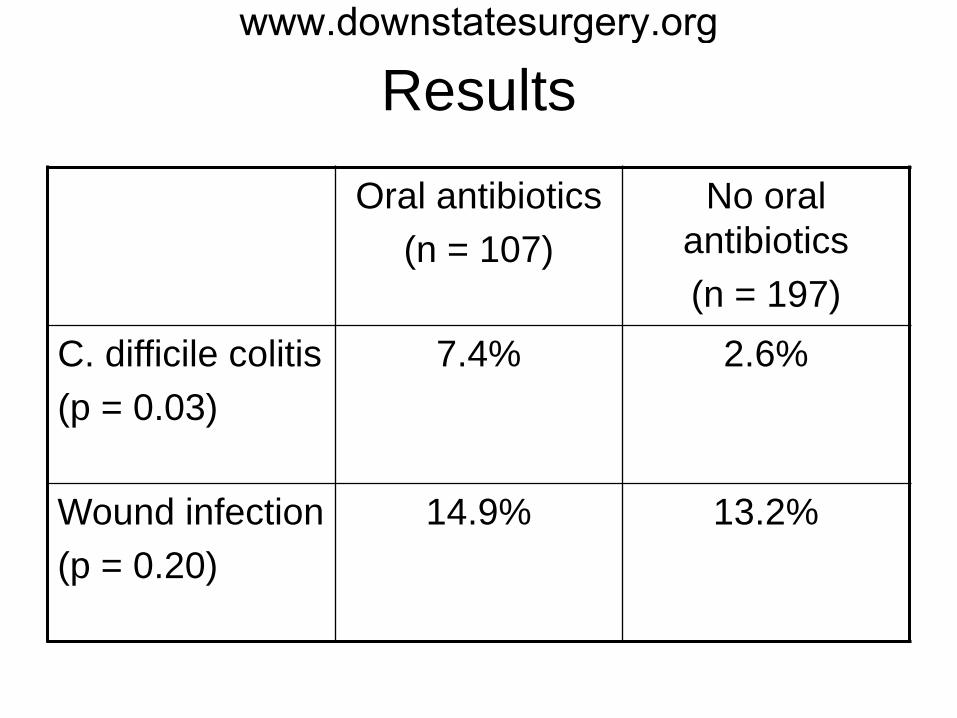
Results
Oral antibiotics(n = 107)
No oral antibiotics(n = 197)
C. difficile colitis(p = 0.03)
7.4% 2.6%
Wound infection(p = 0.20)
14.9% 13.2%
www.downstatesurgery.org
Reasons to continue mechanical bowel preparation
• Need to palpate small tumors• Need for intraoperative colonoscopy• Easier to handle lightweight bowel
laparoscopically• Low pelvic anastomosis
www.downstatesurgery.org
Reasons NOT to continue mechanical bowel preparation
• Significant patient discomfort• Causes electrolyte abnormalities• Causes hypovolemia• Associated with bacterial translocation
through the bowel wall• A poorly prepped bowel will allow easier
spillage of stool than an unprepped bowel
www.downstatesurgery.org
The Association of Coloproctology of Great Britain and Ireland
• Guidelines for the Management of Colorectal Cancer (2007)
• “Bowel preparation should not be used routinely before colorectal cancer resection.” (Recommendation grade B)
http://www.acpgbi.org.uk/assets/documents/COLO_guides.pdf
www.downstatesurgery.org
Australian Cancer Network
• Colorectal Cancer GuidelinesRevision Committee (2005)
• “Mechanical bowel preparation is not indicated in elective colorectal operations unless there are anticipated problems with faecal loading that might create technical difficulties with the procedure, e.g. laparoscopic surgery, low rectal cancers.”
http://www.nhmrc.gov.au/_files_nhmrc/file/nics/material_resources/epgr_review_chapter_9.pdf
www.downstatesurgery.org
American Society of Colon and Rectal Surgeons
www.downstatesurgery.org
Werner Forßmannwww.downstatesurgery.org
Ignaz Semmelweiswww.downstatesurgery.org