Embed Size (px)
DESCRIPTION
book of pain version 1
Citation preview

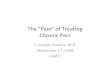
Highland Book of PainTake control of acute pain in the
emergency department
Table of Contents
1. Regional block by location and injury. 22. Drug guide for acute pain: ..................43. Pharmacological options for sedation .54. Local Anesthetics.................................65. Local anesthetic toxicity .....................66. Nerve anatomy ....................................78. Nerve injury: ......................................77. Cutaneous innervation......................8-98. Nerve blocks used in the ED..............109. Setting up for a successful block.......1010. Block Technique: ............................1111. Specific blocks ….......................12-53
DRAFT DO NOT COPY DO NOT DISTRIBUTE
1

1. Regional block by location and injuryCondition / injury / area Block Comments Pg
headache Greater occipital
Trun
cal Fractured ribs Intercostal > 4 or bilateral
need epidural 24
Hernia Illioinguinal-Illiohypogastric 26Abdominal wall injury
Transversus Abdomius Plane 26
Buttock injury “Butt block” 32
Upp
er e
xtre
mity
Humerus or forearm
SupraclavicularInterscalene
14, 12
Acute or chronic Shoulder Suprascapular 34
Shoulder dislocation
Suprascapular plus intraarticular 34
Clavicle Superficial cervical plexus 52
Isolated hand FUN block 18
Boxer's fracture Ulnar block 18
Low
er E
xtre
mity
Lateral thigh Lateral femoral cutaneous Femoral neck or hip fracture “3 in 1” or “3 in 3” block
16,18,20Femoral shaft or
capitellum Femoral block
Complex knee fracture Femoral + subgluteal sciatic 16,
Tibial or tib / fibAnkle Popliteal block
* Hypothetical risk of missing a compartment syndrome.
28
Foot
A. Popiliteal blockB. Saphenous for medial cutaneous forelegC. Ankle block for selective anesthesia of foot
* Ankle block can be tailored for smaller injureis
28,30
2

Condition / injury / area Block Comments Pg
Nec
k an
d Fa
ce
Upper lip Infraorbital 38Lower lip Mental 40Chin Extended mental 40Forehead supraorbital 42Tip of nose Dorsal nasal 44Scalp over ear zygoma-temporal 46Mid Cheek zygoma-facial 48Inferior ear Greater auricular 50Lateral neck
Superficial cervical plexus52
clavicle
3

2. Drug guide for acute pain:
Acute Equianalgesic DosingAge IV Morphine (mg) IV Dilaudid (mg) Fentanyl (mcg)*20-39 7.5-12.540-59 5.0-10.0 0.75 – 1.5 50-10060-69 2.5-7.570-85 2.5-5.0>85 2.0-3.0*Outpatient use of vicodin counts toward 5d opiate use requirement needed to start a patch.
Undifferentiated pain: Start w/ an NSAID- Tylenol 650-1000mg or Ibuprofen 400-800mg or Vicodin 2 tabs [=1gm tylenol + 10 oxycodone (3 IV morphine equivalents] Consider Toradol- 15 – 30 IV (kidney stones, ortho injury). Escalate with opiates. Fentanyl causes less hypotension but is short acting.
Trauma:Toradol 30 mg IV, then Ibuprofen 800mg PO TID + gabapentin 100 TID, Vicodin 2 tabs Q 6hrs ATC, dilaudid 1-2 mg IV Q2hrs PRN breakthrough.
Undifferentiated severe headache:Toradol 15-30 IV, compazine, triptan(know the contraindications), greater occipital nerve block (avoid opiates)
Neuropathic pain Gabapentin 100mg PO TID increasing to 300-900 TID Amytriptiline start at 25mg PO QD increase to 50 after 1wkEffexor 37.5 PO QD increasing to 75 after 5-7d
4

3. Pharmacological options for sedation Overview: Propofol has replaced versed + fentanyl as 1st linefor longer procedures such as abscess drainage. Methohexital is a great option for reductions because it produces muscle relaxation.Propofol. Ultrashort acting sedative-hypnotic. Dose dependent sedation. Start 1.0mg/kg IV bolus over 1-2 minutes then 0.5mg/kg boluses as needed. Problems-respiratory depression, hypotension, pain on injection. Be prepared with BVM as needed. No analgesiaKetamine: Much increased interest recently. NMDA inhibitor that produces strong analgesia and dissociative sedation. Start 1.5-2.0 mg/kg IV over 2 minutes then 0.5mg/kg boluses as needed. Also may use 4-5mg/kg IM x 1. Problems-Salivary secretions, emesis, increased HR, inotropy, and HTN. Laryngospasm. Muscle rigidity and twitching. Emergence phenomenon. “Ketofol”: Unclear benefit to mixture. Hypothesis is that ketamine provides analgesia and cardiovascular stimulation counteracting the depressive effects of propofol. Start 1:1 mix at 0.75 mg/kg IV.Etomidate. Gaba agonist. No advantage over propofol. Start 0.1 mg/kg IV bolus over 2 minutes then 0.05 to 0.1 mg/kg boluses as needed. Problems-20-40% incidence of myoclonus. Respiratory depression, hypotension, pain on injection. Be prepared with BVM.Fentanyl plus Versed:Midazolam. Sedation, muscle relaxation, amnesia. Rapid onset in 1-3 minutes, duration of 30 minutes. Start 1-2 mg IV over 1 minute then 1 mg IV every 2-3 minutes titrating to effect. Problems-respiratory depression, hypotension, pain on injection. Be prepared with BVM.Fentanyl. Rapid acting opiate with duration of 30-40 minutes. Start 1-1.5 mcg/kg IV then 50 mcg IV every 2-3 minutes titrating to effect. Problems-same as VersedAdministration strategy: Start with 1-1.5 mcg/kg IV fentanyl and observe then give 1-2 mg IV Versed. Go up with 50mcg fentanyl + 1 mg Versed IV I q 2-3 minutes intervals.Methohexital. Ultrashort acting. Rapid onset. Best for orthopedic procedures and imaging sedation. Most patients wake up within 10 minutes. Start 0.75-1.0 mg/kg IV over 1 minute then 0.5 mg/kg IV as needed. Problems-respiratory depression, hypotension, no analgesia.
5

4. Local Anesthetics
5. Local anesthetic toxicity CNS- Early or mild toxicity: light-headedness, dizziness, tinnitus, circumoral numbness, abnormal taste, confusion and drowsiness. Throughout the injection talk to the patient asking them how they feel. Any suggestion of confusion should alert you to the possibility of toxicity and you should stop any further injection. Severe toxicity: tonic-clonic convulsion leading to progressive loss of consciousness, coma, respiratory depression, and respiratory arrest.CV- Bradycardia, hypotension-> CV collapse. Usually about 4 - 7 times the convulsant dose needs to be injected before cardiovascular collapse occurs due two direct action on myocardium. Bupivacaine requires ressucitation with lipid emulsion. Intralipid rescue of an adult weighing 70 kg: Use a 500-mL bag of fat emulsion (Intralipid 20%) and a 50-mL syringe.->Draw up 50 mL and give it stat intravenously, and then draw up and give another 20 mL.-> Repeat up to twice more as the epinephrine is given as needed. Then give intrailip bag IV over the next 15 minutes.
6
Onset Duration Duration Rec. Rec.(%) (min) Plain With Max imum Max imum
Solution Single Dose Single Dose(minutes) (minutes) (mg/kg) (mg)
0.5-1.5 < 2 to 30 60-120 120-240 500 + epinephrine
0.25-0.5 2-30 180-360 240-720 225-250
local anesth. Conc.
Epi
Lidocaine 4.5 ( 7 w / epi)900 + epi for brachial plex us block or femoral/sciatic block
* Rapid onset and moderate duration of action. Absorption and plasma lev el w ill v ary by site of administration. Max imum single dose should not ex ceed 4.5 mg/kg or 300 mg (7 mg/kg or 500 mg w ith epinephrine) for infiltration and peripheral blocks. Bupivacaine 2.5 (3 w /epi)
*Has inherent v asoconstrictiv e activ ity and the addition of epinephrine does not significantly alter the onset or duration of action. Max imum single dose should not ex ceed 2.5 mg/kg or 250 mg.

6. Nerve anatomy
8. Nerve injury: Mechanisms are unclearLargest series->Incidence of persistent injury = 2.4 /10,000 blocks (blind technique). Smaller studies show incidence of parasthesis to be about 0.2% which is the same rate of incidence of brachial plexus injury after HIP surgery due to patient positioning. Ultrasound guided blocks in awake patients in the ED are likely to have a lower risk of injury. Note: 15% have parasthesias in the first 3-4 days • Avoid high pressure injections. Animal data suggests high
injection pressure leads to nerve injury. No human data.• Avoid patients with already damaged nerves. Patients with
diseased or injured nerves from DM, chemotherapy, PVD, MS, or other condition may be at higher risk for injury.
• Avoid painful injections. Pain iindicates perneurial puncture and you should reposition your needle, if it still hurts abort the block.
• Avoid heavily sedated patients and patients with altered mental status. Pt must be able to communicate.
REF: ASRA Practice Advisory on Neuological Complications in Regional Anesthesia. Reg Anesth Pain Med 2008;33(5).
7

7. Cutaneous innervation
8

9

8. Peripheral nerve blocks used in the EDUpper extremity:
● Greater occipital nerve● Superficial cervical plexus ● Suprascapular ● Interscalene ● Supraclavicular ● FUN block
Trunk:● Intercostal nerve block● Illioinguinal-illiohyogastric ● Genitofemoral nerve block● transversus abdominus plane● Butt block
Lower extremity:● Sciatic nerve block: posterior ● 3 in 1 Femoral nerve block● 3 and 3 Femoral nerve block● Popliteal block: all approaches● Saphenous nerve block● Ankle blocks
Other:● Greater occipital nerve block● Other scalp blocks● Ankle blocks● Dental blocks
9. Setting up for a successful block• Consent must include risk of parasthesias, hematoma formation,
intavascular injury, and block failure. • Premedication with a low dose benzodiazapine is great. • Clarify timing and expectations with patient and all participating
providers including consultants. ◦Blocks need a minimum of 20minutes to 40 minutes to take
effect. Consultants should not begin until you give the OK.◦Blocks should be used in conjunction with sedation and not as
a substitute. For very painful procedures, be ready to titrate sedation to depth of block. (see section on sedation)
◦Partial or failed blocks may need to be repeated. This is OK. Wait at least 45 minutes if using large volumes.
• Gather syringes (control allow for aspiration), 22 gauge spinal needles(1.5 or 3.5in as needed), 4x4 gauze, chlorhexadine, and a marking pen.
• Either load up syringe directly with your local or use larger syringe (30cc) with 3-way stop cock
• Mark anatomy with pen and position patient as needed
10

10. Block Technique: The goal is to steer the needle away from high risk structures such as vessels and pleura and to confirm spread of local anesthetic within the correct fascial compartments and around the target nerves.1. Find landmark vascular structure (possibly assisted by color Doppler), bone, or muscle2. Find nerve or plexus on short-axis imaging (transverse scan)3. Adjust depth to 1cm below target; adjust gain as necessary4. Use the “PART” maneuvers to optimize image quality
a. Pressure: varying degrees of transducer pressure on skinb. Alignment: sliding movement of the transducer to definethe lengthwise course of the nervec. Rotation: the transducer is turned in either a clockwise orcounterclockwise direction to optimize the imaged. Tilting: the transducer is tilted in both directions to maximize the angle of incidence of the ultrasound beam with the target nerve
5. Scan anticipated needle trajectory with color Doppler to identify any unsuspected vessels. 6. Use small test doses to help locate needle tip. 7. Look for “dough nut” sign of circumferential hypoechoic spread.8. Follow spread longitudinally distal and proximal along nerve to confirm anesthetic presence in the correct fascial compartment.
11
1. In-plane
2. out-of-plane

11. Interscalene blockThis block is block approaches the brachial plexus at the level of the roots and covers the from the clavicle to the hand but often misses the ulnar distribution of the hand. Ideal for deltiod abscesses. Keep in mind that you virtually always inadvertently block the phrenic nerve thereby paralyzing that hemidiaphram. The advantage is that the block is very superficial and the risk of pneumothorax is very low. Procedure1. Have the patient turn their head to the contralateral side and find the cricoid cartilage. 2. Scan laterally from the trachea at this level identifying the thyroid gland, internal jugular vein and carotid artery. 3. Keep scaning laterally as the belly of the sternocleidomastoid thins out. On its lateral border the anterior (medial) and median(lateral) scalene muscles will come into view just deep to the sternocleidomastoid. 4. Use in plane technique with a lateral approach and a 1.5 inch needle.5. Pass through the median scalene and get in between the hypoechoic nerve roots. As always inject slowly and gently. Use 10-20 mL
12

Shallow, lateral, in plane approach through the middle scalene
13

12. Supraclavicular block: “The spinal of the arm” Used for mid-humerus down, including the hand. Due to the tight compartmentalization of the brachial plexus as it passes deep to the clavicle, this block has a high success rate with a dense anesthesia. The big draw back is the risk of pneumothorax due to the proximity of the superior pole of the lung. This risk is increased in tall, thin patients and on the right side. As a result, this is a block where you need to clearly visualize the subclavian artery, the first rib, the pleura, and your block needle as you advance to the plexus. The subclavian comes off the brachiocephalic trunk on the right and the aortic arch on the left then runs over the first rib and under the clavicle becoming the axillary artery. Just deep to the first rib is the lung.
1. Have patient turn their head 45º contralaterally2. The plexus lies immediate posterior and lateral to the lateral border
of the clavicular head of the sternocleidomastoid laterally adjacent to the pulsing subclavian artery.
3. Start scanning with your probe parallel to the clavicle at its lateral upper border and slide medially into the supraclavicular fossa until the pulsing subclavian artery comes into view.
4. Just superior and lateral to the subclavian artery the plexus appears as cluster of hypoechoic grapelike structures. The plexus should be 1-2cm deep.
5. Note the depth of the pleura and the first rib.6. Insert your 22 g 1.5 inch needle laterally and in-plane. Visualize
the pleura, first rib, sublacavian artery and your needle as you slowly advance medially.
14

Guide your needle in-plane with the subclavian artery, 1st rib, and pleura in view. The spread of local should lift the plexus off the 1st rib.
15

13. Medial and Lateral antebrachial cutaneous blocks: The lateral antebrachial nerve is blocked by palpating the distal insertion of the biceps tendon in the AC then injecting 5mL just lateral and deep to the tendon. Next make a subcutaneous wheal extending laterally about 5cm across the flexor surface of the AC. Block the medial antebrachial nerve with a C shaped half-ring of subcutaneous wheal about ½ of the way up from the elbow on the medial arm.
16

17

14. The fascia illica (Femoral nerve) block: The most technically uncomplicated block we use. Standard of care for hip and femur fractures with few draw backs. The crucial move is piercing the fascia iliaca. This block incompletely covers the femur and anterior thigh to the tibial insertion of the patellar tendon. It is part of the leg block that involves the femoral, lateral femoral cutaneous and obturator nerves.1. Supine position with a small degree of external rotation as needed.2. Find ingiunal crease that lies 3-6cm distal to the ligament itself3. Look for the femoral artery starting about 1/3 of the way lateral from
midline along the inguinal crease. 4. Scan laterally inplane with the inguinal crease.5. Identify the femoral vein, femoral artery and finally the femoral nerve
just lateral to the artery.6. About 4 cm distal to the inguinal crease you may see the profunda
femoris artery branch off. This helps if the inguinal crease is not anatomically clear. Your block site is 1-3cm proximal to this point.
7. With the artery in short axis view use color Doppler to confirm arterial flow. The nerve should be 2-4cm deep to the skin.
8. Use in-plane technique with a 22g 3.5 inch needle advance lateral to medial and pass through the fasica iliaca just lateral to the nerve. Withdraw slowly giving small test doses and visualize local anesthetic spread displacing and surrounding the nerve when you are in the correct fascial plane.
LATERAL
FI: fascia iliaca; FL-fascia lata; F-femoral ; IPM-iliopsoas muscle; PECT-pectineous
18

The key is penetrate the fascia iliaca that surrounds the iliacus muscle and visualize the spread of local displacing the nerve off the artery and anteriorly off the iliacus muscle.
LATERAL
19

15. Continuous catheter placement. This technique has been shown to have the same safety profile as a single shot block with the added benefit of allowing for superior long term analgesia using infusion pumps. The prep is similar to that of LP with a sterile field, gloves, and probe cover. An epidural kit has everything you need including 17g Tuohy needle, epidural catheter, steri-strips, tegaderm, drape, anaseptic cleanser. Approach: same as fasica illiaca block but with larger needle preanesthesia with sin weal is advisable. In-plane or out of plane approach works. The key with both is to get underneath the fascia illiaca. Preload the needle with your catheter and note the mark level as it exits the back end of the needle. Once in the perineural space inject 10mL after aspiration and watch for LA spread. When covinced that you are in the right place advance the catheter 5-7cm. Find it with ultrasound and inject another 5-10 mL to confirm LA spread. You can tunnel it or simply coil it on the skin and tape it down with steri-strips then cover with a big tegaderm.
20

21

16. Obturator: this is a challenging block due to the depth of the target and its location deep in the groin. The reason to attempt this block is that the obturator nerve is frequently not blocked by the fascia illica block and often provides significant innervation to the femur itself. The injection point is just medial to the femoral artery about 4cm deep.Using a 2.5 22g spinal you should just be able to reach it. Have the patient gentle externally rotate the hip as possible then get the femoral artery and vein in transverse view, slide just medial to the vien and rotate 90° to position the superior pubic ramus(SPR) cephalad in your field. Enter relatively steep in plane targeting a hyperechoic triangle at the base of the SPR. YOU MUST ASPIRATE BEFORE INJECTION. THE OBTURATOR VEIN LIVES HERE! BE SURE YOU USE LA WITH EPI AS AN INDICATOR OF INTRAVASCULAR INJECTION AND THAT YOU OBSERVE LA SPREAD IN REAL TIME.
22

23

17. FUN block (forearm ultrasound guided nerve block)The initial description of the this block in the ED was done here at highland, as was the supraclavicular block. This block is very low risk and relatively non-invasive, however the nerves are small and a full block of the hand requires three separate injections. It is very effective for hand injuries, but tends to be incomplete for wrist fractures.
24

Ulnar, median, and radial nerves. Arrow=nerve;Arrowhead=artery
25
Ulnar nerve: Scan the volar mid forearm beginning at the ulnar side and find ulnar artery just ulnar to the artery lies the nerve. Inject with in-plane technique with 3-5 mL for all forearm blocks.
Median nerve: The median nerve lies between the palmaris longus and flexor carpi ulnaris tendons. Start scanning at the wrist and move proximally for optimal view.
Radial nerve:Radial nerve lies on the radial side of the radial artery and can be blocked at the forearm (shown) or at the AC fossa.

Transversus abdominis plane block (TAP)This block covers the anterior abdominal wall from the level of the umbilicus to the inguinal region innervated by the illiohypogastric and illioinguinal nerves. Palpate the lower costal margin and the illiac crest at the anterior axillary line. Scan with ta linear probe in transverse orientation in this region obtain a clear view of the hyperechoic external oblique, internal oblique, and transversalis fascial planes. Note the depth of the peritoneum. Insert the needle 2cm from the probe in plane, moving laterally and posteriorly until the tip is at the fascial plane between the internal oblique and transversalis muscles. Aspirate then deliver 15-20mL of local anesthetic.
26

27

Intercostal Nerve Block: This block provides dense anesthesia for rib fractures and chest wall procedures such as thoracostomy tubes. Postion the patient sitting up if possible; lateral decubitus and prone also works. Take the time to identify C7 and the inferior border of the scapula and quickly mark each vertebral prominence. Place your probe in transverse position relative to the rib. The best view is found 4-7 lateral to the midline on the border of the paraspinus muscles. Direct your needle in-plane toward the middle of the inferior border of the rib. You must always keep the pleura and your needle tip clearly in view. Never injection without aspiration first. This is a highly vascular area. Ptx is a real risk. Block a minimum of 3 levels, with 5 being optimal. Use maximum of 30ml of 1:1 1%lidocaine + 0.5% bupivacaine.
28

29

Popliteal block. This blocks the entire leg from just below the knee down excluding the saphenous distribution of the medial foreleg
30

31

Saphenous block. In conjunction with the popliteal block this a complete block of the forleg and foot. The nerve runs in the fascia between the sartorious and the vastus medialis. In some it is adajcent to the saphenous vein. Approach the nerve from the antero-medial aspect of the thigh just above the knee. Use an inplane approach moving down the fascia over the vastus medialis. The nerve is surrounded by lots of fascia and not very sharply defined. Use a 3.5 needle and 10 ml of local.
32

33

Butt block. Born at Highland. This a field block over posterior illiac crest centered 7 to 8 cms lateral to the midline. The nerves run right over the illiac crest in small tunnels. The key is getting a layer of anesthetic right over the bone. Palpate or use ultrasound to locate the crest 7 cm from midline. Perpandicular to the skin direc the needle and hit bone. Remember the nerves go over the top of the crest, be sure you are not inferior to the crest on the illiac wing. This is large volume block, if you are planning on other blocks I would use 20-30 cc of a mix of 3:1 0.5% bupivacaine and normal saline. This gives you an additional 20cc of 0.25% bupivacaine for rescue local. This block misses the cleft area of the medial buttock and the inferior buttock. You may try a subcutaneous field block extending from the PSIS to the sacrum. Finally, the Inferior cluneals come off the posterior femoral cutaneous nerve that can be seen with ultrasound just medial to the sciatiac nerve beneath the gluteus maximus. It can be blocked directly with uls guidance or a field block along inferior edge of the gluteus maximus.
34

35

suprascapular. Alleviates chronic shoulder pain from arthritis, cacilfic tendonitis, and adhesive capsulitis. Use a linear probe parallel to the scapular spine to visualize the suprascapular notch. You should clearly see the bony outline of the coracoid laterally with the pulsing suprascapular artery just lateral to the hyperechpoic nerve. The key is getting underneath the suprascapular ligament. Be aware extending anteriorly could result in pleural puncture. Aspirate to avoid arterial injection. Inject 20mg triamcinolone and 5-10 mL bupivacaine.
36

Suprascapular
37

Face Blocks. Note: V3 is a deep block that will not be covered. The greater auricular block is part of the superficial cervical plexus block.
38

39

Infaorbital.
This block is for upper lip lacerations primarily, but much of the nasal side wall, part of the cheek and eyelid are also numbed. The infraorbital nerve exists through the infraorbital foramen. The foramen is located on a line dropped from the medial edge (limbus) of the iris. If the patient stares straight ahead, the infraorbital foramen is located 4 to 7 mm below the orbital rim on that line .
The injection point for the infraorbital nerve is in the center of the small triangle lateral to the alar rim and medial to the nasolabial fold
With your left index finger on the infraorbital rim, ask the patient to look straight ahead. Holding the syringe like a pen, you advance the needle to bone toward the designated point about 4 to 7 mm down from the rim. Often, the needle tip goes directly into the foramen itself. Inject 1 to 2 cc.
40

41

Mental block. This blocks the lower lip and chin.
The mental nerve usually exits from its foramen below the apex of the second bicuspid. In some people stretching out the lip actually makes this nerve visible.
Place the needle tip in the buccal sulcus near the base of the tooth and inject a small amount under the mucosa.
To block the chin, an end branch of the mental nerve and the terminal branches of the mylohyoid need to be blocked. These can be done immediately after the mental block by an anterior premandibular injection anterior to the vestibule in front of the anterior teeth. You must change your position to behind the patient, turn the syringe more vertically, and inject in the supraperiosteal plane with at least a 1.5-inch needle. Inject anterior to and beyond the lower border of the mandible but not quite out of the skin.
42

43

Supraorbital/Supratrochlear/Infratrochlear. This blocks the forehead, medial upper eye lid, and the bridge of the nose.
Inject along the supraorbital rim from lateral to medial by stretching out the eyebrow laterally and piercing the lateral part of the middle third of the eyebrow. Aim the needle at the supraorbital notch, which is palpable. Keep your other hand on the rim. After injecting 1 to 2 cc prior to the notch under the muscle, the needle moves medially a few millimeters along the rim, and another cc is deposited. Finally, another 1 cc is deposited as the needle advances toward and touches the nasal bones.
44

Dorsal Nasal Block. This blocks the tip of the nose and the cartilaginous dorsum.
The external or dorsal nasal nerve emerges at the lower border of the nasal bone .5 to 1 cm off the midline from a small groove in the distal nasal bones and passes under the nasalis transversis muscle to supply some of the skin of the ala, vestibule, and lip.
Palpate the nasal midline and feel the end of the nasal bones using the thumb on one side and the index finger on the other. The nerve exits about 6 to 10 mm from the midline of the nasal bones. Inject 1-2 ml.
45

Zygomaticotemporal From above the patient, inject behind the lateral orbital rim with needle insertion at about 10 to 12 mm behind and just below the zygomaticofrontal suture (palpable). By sliding the 1.5-inch needle along the mid-posterior bony wall toward a point about 1 cm below the canthal level, one can block easily during the pullout . This injection blocks a sideward, fan-shaped area about a quarter of a circle that abuts the area numbed by the supraorbital block.
46

Zygomaticofacial Nerve. The zygomaticofacial block is always done right after the zygomaticotemporal block. With the patient's head slightly turned inject anesthetic into a dime-sized area just lateral to the junction of the lateral and inferior orbital rim.
Numb area. The zygomaticofacial nerve provides sensation to an area at the cheek prominence and below. See diagram.
47

Superficial cervical plexus – Covers neck and clavicle. Superficial fan block along posterior border of the SCM. Palpate the mastoid process then at the level of the cricoid palpate the C6 transverse process. The center of the fan is at the midpoint of this line. This is often about 6.5cm inferior to the external acoustic meatus. Blocks the lower 1/3 of the ear and surrounding skin.
48

49

50

![Edited by - Dubravka · PDF fileMinistry of Pain' - or so Croatian Dubravka Ugresic tells us iu the opening pages of her 2005 book The Mi»is[i~~ of Pain [Ministarstvo boli].~ Tlie](https://img.pdfslide.us/doc/110x75/5a8625e07f8b9a14748c985a/edited-by-dubravka-of-pain-or-so-croatian-dubravka-ugresic-tells-us-iu-the.jpg)