Embed Size (px)
Citation preview
ISBN
BOOK OF ABSTRACTS BOOK OF ABSTRACTS BOOK OF ABSTRACTS BOOK OF ABSTRACTS FINAL PROGRAMMEFINAL PROGRAMMEFINAL PROGRAMMEFINAL PROGRAMME
7777thththth Croatian Congress on Regional AnaesthesiaCroatian Congress on Regional AnaesthesiaCroatian Congress on Regional AnaesthesiaCroatian Congress on Regional Anaesthesia and Analgesia with International Participationand Analgesia with International Participationand Analgesia with International Participationand Analgesia with International Participation
School of Medicine, University of Zagreb June 14–15, 2019.
Šalata 3, Zagreb, Croatia

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 2
Editors: Kata Šakić (Zagreb, Croatia) Livija Šakić (Zagreb, Croatia)
Reviewers: Eleonora Goluža (Zagreb, Croatia)
Neven Elezović (Split, Croatia) Livija Šakić (Zagreb, Croatia)
Ivana Bičanić (Zagreb, Croatia) Dinko Bagatin(Croatia
Language editor
Tihana Ptičar
ORGANIZERS CROATIAN MEDICAL ASSOCIATION
CROATION SOCIETY OF REGIONAL ANAESTHESIA AND ANALGESIA EUROPEAN SOCIETY OF REGIONAL ANAESTHESIA &PAIN THERAPY
School of Medicine University of Zagreb Chair of Anaesthesiology and Reanimathology
Under the Auspices of
DEPARTMENT OF MEDICAL SCIENCES
CROATIAN ACADEMY OF SCIENCES AND ARTS
7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 3
Organizers: Croatian Society of Regional Anaesthesia and Analgesia - Croatian Medical Association (CSRAA-CroMA) http://hdraa.com.hr member of European Society of Regional Anaesthesia & Pain Therapy (ESRA) http://www.esraeurope.org Co-organizers: School of medicine University of Zagreb Dept.of Anaesthesiology and reanimathology Zagreb. Organizing committee: Predsident: Kata Šakić (Croatia), Vice president: Slobodan Mihaljević (Zagreb) Secretaries: Ivan Šklebar (Zagreb), Livija Šakić (Zagreb) Members: Dinko Bagatin (Zagreb), Daniela Bandić-Pavlović (Zagreb), Ivana Bičanić(Zagreb), Luka Djulabić (Zagreb), Neven Elezović (Split), Vjekoslav Jeleč (Zagreb), Krešimir Oremuš (Zagreb), Šimun Šakić (Zagreb), Tatjana Šimurina (Zadar), Miroslav Župčić (Rijeka) Scientific committee: Alain Delbos (France), Vesna Novak Jankovič (Slovenia), Slobodan Mihaljević (Croatia), Narinder Rawal (Sweden), Krešimir Rotim (Croatia), Ismet Suljević (Bosnia and Herzegovina), Kata Šakić (Croatia), Marc Van De Velde (Belgium) Invited speakers: Alain Delbos (France), Mano Doraiswami (UK), Viktor ðuzel (UK), Slobodan Gligorijevic (Switzerland), Vesna Novak Jankovič (Slovenia), Narinder Rawal (Sweden), Ismet Suljević (BIH), Marc Van De Velde (Belgium) Invited speakers (Croatia): Tomislav Badel (Zagreb), Daniela Bandić Pavlović (Zagreb), Ivan Bohaček (Zagreb), Dubravko Habek (Zagreb), Slobodan Mihaljević (Zagreb), Krešimir Oremuš (Zagreb), Jasminka Peršec (Zagreb), Zdravko Petanjek (Zagreb), Ivan Radoš (Osijek), Kata Šakić (Zagreb), Livija Šakić (Zagreb), Tatjana Šimurina (Zadar) Ivan Šklebar (Zagreb), Dinko Tonković (Zagreb), Branko Tripković (Zagreb), Branko Vitale (Zagreb), Miroslav Župčić (Rijeka) CSRAA programme topics: The CSRAA programme focuses on clinical research, education and clinical application in anaesthesia and acute and chronic pain management. Programme is comprised of: Central Nerve Blocks, Peripheral Nerve Blocks, Regional Anaesthesia and analgesia in Paediatrics and Obstetrics, Ultrasonography, Postoperative pain management, Chronic Pain Management, Ethics and education, Free topics. Invited speakers:
1. Alain Delbos - Professor of Anesthesiology
7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 4
President of European Society of Regional anaesthesia &Pain Therapy, France email: [email protected]
2. Narinder Rawal, MD, Ph.D., FRCA (Hon),
EDRA Professor of Anaesthesiology Department of Anaesthesiology and Intensive Care Örebro University 701 85 Örebro, Sweden email: [email protected] Past secretary of European Society of Regional anaesthesia &Pain Therapy
3. Marc Van De Velde - Professor of
Anesthesiology University Hospitals Leuven, Katholieke Universiteit Leuven, Belgium email: [email protected] Past President of European Society of Regional anaesthesia &Pain Therapy
4. Prof. Slobodan. Gligorijevic MD
Dept of Anaesthesiology &Intensive Medicine Clinic Hirslanden, Zürich, Switzerland
email: [email protected] Past President of European Society of Regional anaesthesia &Pain Therapy
cinu i liječen 5. Prof. Vesna Novak Jankovič , MD, PhD
Department of anesthesiology, reanimathology and intensive care University hospital Centar Ljubljana, Ljubljana, Slovenia email: [email protected]
6. Assoc. prof, Ismet Suljević MD PhD
Clinical Department of Anaesthesiology and Intensive Therapy, University Medical Centre Sarajevo, Bosnia-Herzegovina
email: [email protected]
7. Mano Doraiswami, MD Barking, Havering and Redbridge University Hospitals NHS Trust, Head of Department of Anaesthesia, London, United Kingdom
8. Viktor ðuzel, MD PhD Barking, Havering and Redbridge University Hospitals NHS Trust, Department of Anaesthesia, London, United Kingdom
email: [email protected]
, Speakers of Croatia
9. Prof. Kata Šakić, MD, PhD, DEAA- Professor of Anesthesiology, School of Medicine University of Zagreb, retired. General, Plastic, Reconsctructive and Aesthetic Surgery Polyclinic „ Bagatin“, Zagreb, Croatia Faculty of dental medicine and health Osijek, J.J. Strossmayer University of Osijek, Osijek, Croatia Catholic University of Croatia, Zagreb, Croatia email: [email protected]
10. Prof. Slobodan Mihaljević, MD, PhD, University of Zagreb School of Medicine Department of anaesthesiology, reanimatology and intensive medicine, KBC-Zagreb, Zagreb Croatia email: [email protected]
11. Prof. Dinko Tonković, MD, PhD,
University of Zagreb School of Medicine Department of anaesthesiology, reanimatology and intensive medicine, KBC-Zagreb, Zagreb Croatia email: [email protected]
12. Associate Prof.Daniela Bandić-Pavlović, MD,
PhD, University of Zagreb School of Medicine Department of anaesthesiology,reanimatology and intensive medicine, KBC-Zagreb, Zagreb Croatia email: [email protected]
13. Prof. Branko Tripković, MD, PhD, University of Zagreb School of Medicine Department of anaesthesiology,reanimatology and intensive medicine, KBC-Zagreb, Zagreb Croatia email: [email protected]
14. Associate Prof. Ivan Šklebar, MD, PhD,
Department of anaesthesiology in ginecology and obstetrics, University Hospital „Sveti Duh“ Zagreb, Croatia Catholic University of Croatia, Zagreb, Croatia email: [email protected]
15. Associate Prof. Tatjana Šimurina, MD, PhD, Department of anaesthesiology Genral Hospital Zadar, University of Zadar Zadar, Croatia
email: [email protected]
16. Assistant professor Ivan Rados, MD PhD, anesthesiologist Department of Anesthesiology and ICU; Clinical Hospital Centar, Osijek; School of Medicine, University JJ Strossmayer, Osijek, Osijek, Croatia email: [email protected]
17. Assistant professor Miroslav Župčić, MD PhD, anesthesiologist

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 5
Department of Anesthesiology and ICU; Clinical Hospital Centar, Rijeka; School of Medicine, University of Rijeka, Rijeka, Croatia email: [email protected]
18. Neven Elezovic, MD, anesthesiologist, Department of Anesthesiology and ICU Clinical Hospital Split, Croatia; email: [email protected]
19. Prof. Dubravko Habek, MD, PhD,
Catholic University of Croatia Hospital Sveti Duh Zagreb Department of ginekology and obstetrics Zagreb, Croatia email: [email protected]
20. Prof. Zdravko Petanjek, MD, PhD,
University of Zagreb School of Medicine Chair of anatomy Zagreb , Croatia email: [email protected]
21. Ivan Bohaček MD, PhD, University of Zagreb School of Medicine Dept. of anatomy and orthopaedic surgery Zagreb, Croatia email: [email protected]
22. Prof. Tomislav Badel, MD, PhD, University of Zagreb Fakulty of Dental Medicine Zagreb, Croatia email: [email protected]
23. Prof. Branko Vitale, MD, PhD, Academy of Medical Sciences of Croatia, Zagreb, Croatia email: [email protected]
24. Livija Šakić, MD, PhD Department of anaesthesiology,reanimatology and intensive medicine University Hospital „Sveti Duh“ Zagreb, Croatia email: [email protected]

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 6
Dear ColleaDear ColleaDear ColleaDear Colleagues, Guests and Friends,gues, Guests and Friends,gues, Guests and Friends,gues, Guests and Friends, On behalf of Croatian Society of Regional Anaesthesia and Analgesia, Croatian Medical Association (CSRAA-CroMA) and European Society of Regional Anaesthesia and Pain Therapy (ESRA) it is our great pleasure and honour to welcome you to the 7th Croatian Congress of Regional Anaesthesia and Analgesia with International participation, School of medicine University of Zagreb, in Zagreb, Croatia, June 14 -15, 2019. The scientific programme is designed for anaesthesiologists and other physicians interested in regional anaesthesia for surgical procedures, as well as in acute and chronic pain management. Paper of invited speaker are published in issue of the Acta Clinica Croatia had been prepared for oral presentations at the 7th Croatian Congress of Regional Anaesthesia and Analgesia with international participation, held on June 14-15, 2019 in Zagreb, Croatia. The Congress was organized by the Croatian Society of Regional Anaesthesia and Analgesia in collaboration with the European Society of Regional Anaesthesia & Pain Therapy and School of Medicine, University of Zagreb under the auspices of the Croatian Academy of Science and Arts. Prior to acceptance and publication, all articles had undergone double review process, CrossRef similarity check and language editing. Regional anaesthesia specialists and enthusiasts have a mission to improve the current state-of-the-art of regional anaesthesia in orthopaedics, obstetrics and day surgery as well as to advance the therapy of postsurgical pain, pains in adults and in children, and of any kind of severe pain that can be helped by sensible administration of drugs and other pain therapies. In addition to education on current pain research and therapy through conferences and publications, we must promote education on the management of pain for both medical students and health professionals. By recognizing the dominant role of the brain, which generates our subjective experiences and activates our defense systems, we are now able to get a bit closer to the interlinked relationship between pain and stress. These relationships among stress, gender, the immune system, and chronic pain syndromes reveal the need to study pain in a biological context far broader than a pain pathway. Postoperative pain has been poorly managed for decades. Regional anaesthetic techniques are the most effective methods to treat postoperative pain. The role of acute pain services to improve pain management and outcome is well accepted but implementation seems challenging. The industrial exhibition is an opportunity for you to network and to keep up-to-date with the latest pharmacological and technological developments. Each company is a supporter of the Congress and we would like to thank them all for their commitment and contribution by visiting the exhibition.
We sincerely hope that you will enjoy both, the educational value of the programme and the unique
atmosphere of charming City of Zagreb. We are looking forward to greeting you personally in Zagreb.
Professor Kata Šakić, MD, PhD President of Croatian Society of Regional Anaesthesia and Analgesia, Croatian Medical Association, Zagreb, Croatia
Professor Slobodan Mihaljević, MD, PhD Head Chair of Anaesthesiology School of Medicine, University of Zagreb, Croatia


7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 8
General informationGeneral informationGeneral informationGeneral information The Symposium will be organised in a form of oral presentations, video projections, workshops and poster presentations
Presentations (apart from invited speakers) will not be allowed without payed registration fee.
Papers of invited speakers are reviewed and published in Journal “Acta Clinica Croatica” 2019″ indexed in SCI and MEDLINE database; Acta Clin Croat, Vol. 58, (Suppl. 1) 2019 (for more info see:http://actaclinicacroatica.hr) Certificate Congress participation will be evaluated on the basis of rule of professional improving and verification of qualification for physicians by the Croatian Medical Chamber. The Participation Certificate will be handed to all participants with regulated registration fee.
Congress Venue "Medicinski fakultet", Šalata 3, 10 000 Zagreb, Croatia
Official Symposium languages English and Croatian (simultaneous translation will not be provided)
Presentations Oral presentations can be in Croatian or English. All presenting materials must be in English. Official emblems All registrated participants and accompanying persons will receive official congress emblem. Social program and program for accompanying persons Cultural and social events are planned for the Congress participants.
• Welcome reception (Friday, June 14th, 2019, 08:00 pm) • Gala dinner (Saturday, June 15th, 2019, 08:00 pm)
Congress service (registration fee and hotel) Iva Posavec mag.oec. Congress department O-Tours PCO d.o.o. Gajeva 6 / 1 st floor HR-10000 Zagreb Croatia
7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 9
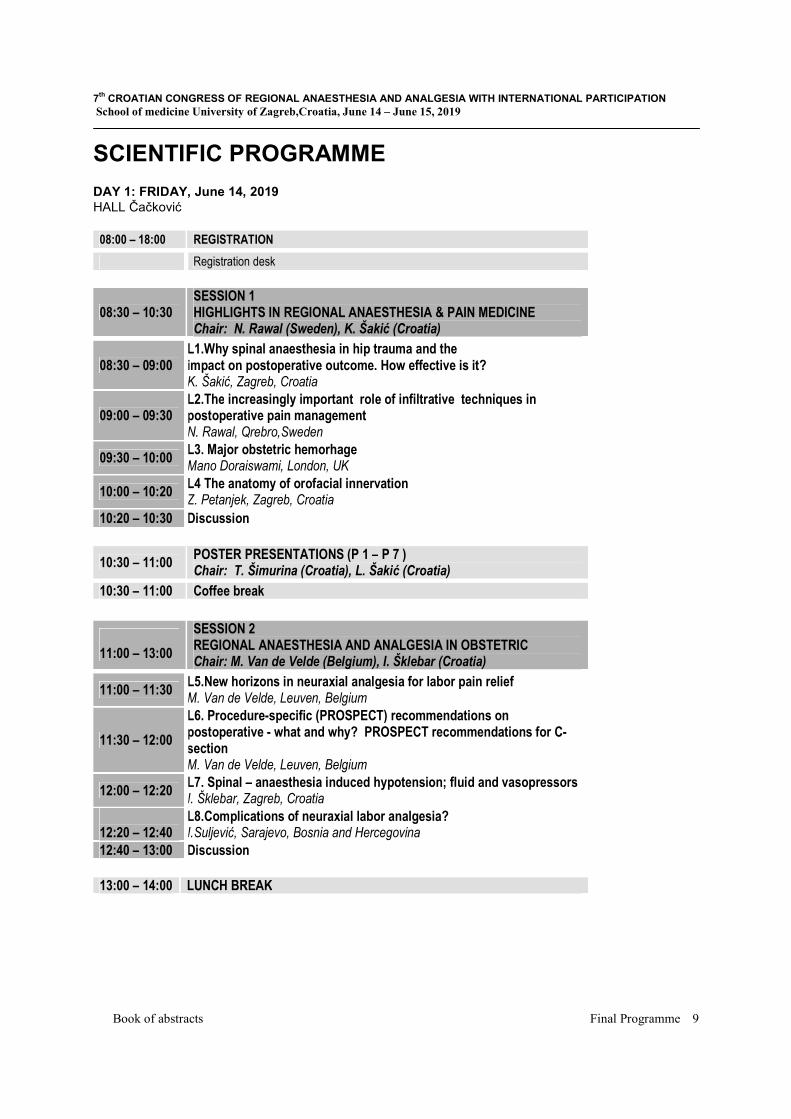
SCIENTIFIC PROGRAMME DAY 1: FRIDAY, June 14, 2019
HALL Čačković 08:00 – 18:00 REGISTRATION
Registration desk
08:30 – 10:30 SESSION 1 HIGHLIGHTS IN REGIONAL ANAESTHESIA & PAIN MEDICINE Chair: N. Rawal (Sweden), K. Šakić (Croatia)
08:30 – 09:00 L1.Why spinal anaesthesia in hip trauma and the impact on postoperative outcome. How effective is it? K. Šakić, Zagreb, Croatia
09:00 – 09:30 L2.The increasingly important role of infiltrative techniques in postoperative pain management N. Rawal, Qrebro,Sweden
09:30 – 10:00 L3. Major obstetric hemorhage Mano Doraiswami, London, UK
10:00 – 10:20 L4 The anatomy of orofacial innervation Z. Petanjek, Zagreb, Croatia
10:20 – 10:30 Discussion
10:30 – 11:00 POSTER PRESENTATIONS (P 1 – P 7 ) Chair: T. Šimurina (Croatia), L. Šakić (Croatia)
10:30 – 11:00 Coffee break
11:00 – 13:00
SESSION 2 REGIONAL ANAESTHESIA AND ANALGESIA IN OBSTETRIC Chair: M. Van de Velde (Belgium), I. Šklebar (Croatia)
11:00 – 11:30 L5.New horizons in neuraxial analgesia for labor pain relief M. Van de Velde, Leuven, Belgium
11:30 – 12:00
L6. Procedure-specific (PROSPECT) recommendations on postoperative - what and why? PROSPECT recommendations for C- section M. Van de Velde, Leuven, Belgium
12:00 – 12:20 L7. Spinal – anaesthesia induced hypotension; fluid and vasopressors I. Šklebar, Zagreb, Croatia
12:20 – 12:40
L8.Complications of neuraxial labor analgesia? I.Suljević, Sarajevo, Bosnia and Hercegovina
12:40 – 13:00 Discussion
13:00 – 14:00 LUNCH BREAK

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 10
14:00 – 16:00 SESSION 3 REGIONAL ANAESTHESIA & PAIN MEDICINE IN ELDERLY Chair: B. Tripković (Croatia), S. Gligorijevic (Switzerland)
14:00 – 14:30 L9. Holistic approach to the immunobiology of aging (view on the turn of millenium) B. Vitale, Zagreb, Croatia
14:30 – 15:00 L10. New horizons in Neuraxial Anesthesia in high risk orthopaedic patients B. Tripković, Zagreb, Croatia
15:00 – 15:30 L11 Inervation of the hip joint and applications of fascia iliaca block, critical evaluation of quadrates lumborum block I. Bohaček, Zagreb, Croatia
15:30 – 15:50 L12. Maternal mortality and role of the anaesthetist S. Mihaljević, Zagreb, Croatia
15:50 – 16:00 Discussion
16:00 – 16:30 POSTER PRESENTATIONS (P 8 – P15) Chair: D. Bandić Pavlović (Zagreb), I. Bičanić (Zagreb)
16:00 – 16:30 Coffee break
16:30 – 18:30 SESSION 4 PERIOPERATIVE PAIN MANAGEMENT-LIA Chair: N. Rawal (Sweden), M. Župčić (Croatia)
16:30 – 17:00
L13. Procedure-Specific Pain Management (PROSPECT) - An update. N.Rawal, Qrebro,Sweeden
17:00 – 17:20 L14.Regional blocks for postoperative pain management - an update" S. Gligorijevic, Zuerich, Switzerland
17:20 – 17:40 L15.Postoperative objective assessment and functional recovery nerve blocks Paravertebral block in plastic surgery M. Župčić, Zagreb, Croatia
17:40 – 18:00 L16.Local anaesthetics and steroids; Contraindications and complications T. Simurina, Zadar, Croatia
18:00 – 18:20 L17.Assesing the block for different pain-an evidenced based approach D. Bandić Pavlović, Zagreb, Croatia
18:20 – 18:30 Discussion
20:00 – 22:00 WELCOME RECEPTION, “Dverce”, Gornji Grad, Zagreb
CSRAA 2019 Best Poster Award Musical act: “Lege Artis Choir “( Music art band of School of Medicine Zagreb, Zagreb)

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 11
DAY 2: SATURDAY, June 15, 2019 HALL Čačković
08:30 – 10:30 SESSION 5 REFRESHER KNOWLEDGE Chair: A. Delbos, France, V.Novak Jankovič, Slovenia
08:30 – 09:00
L18.Blocks for foot and ankle surgery A. Delbos, Paris, France
09:00 – 09:20
L19. RA in Thoracic and Abdominal surgery V. Novak Janković, Ljubljana, Slovenia
09:20 – 09:40
L20.Enhached recovery in caesarean section V. ðuzel, London, UK
09:40 – 10:00
L21. Blocks for lower limb and abdominal surgery J. Peršec, Zagreb, Croatia
10:00 – 10:20 L22.US skills Beyond RA in lower limb traumatology and orthopaedics K. Oremuš, Zagreb, Croatia
10:20 – 10:30 Disccusion
10:30 – 11:00 POSTER PRESENTATIONS (P 16– P 24 ) Chair: M.Žura, (Zagreb), N. Elezović (Split)
10:30 – 11:00 Coffee break
11:00 – 13:00
SESSION 6 REFRESHER KNOWLEDGE Chair: D. Tonković (Croatia), I.Radoš (Croatia)
11:00 – 11:30 L23. Regional anaesthesia in neurosurgery D. Tonković, Zagreb, Croatia
11:30 – 12:00 L24. Invasive procedures for chronic pain I. Radoš, Osijek, Croatia
12:00 – 12:20 L25.Orofacial pain – diagnostic and therapeutic challenges T. Badel, Zagreb, Croatia
12:20 – 12:40
L25. Dexamethasone - intrathecal minimiser of simple haemathologic stress biomarkers in hip fracture L. Šakić, Zagreb, Croatia
12:40 – 13:00 L26. Medico - legal responsibility in management of acute and chronic pain in obestrics D. Habek, Zagreb, Croatia
13:00 – 13:10 Discussion
13:00 – 14:30 LUNCH BREAK
7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 12
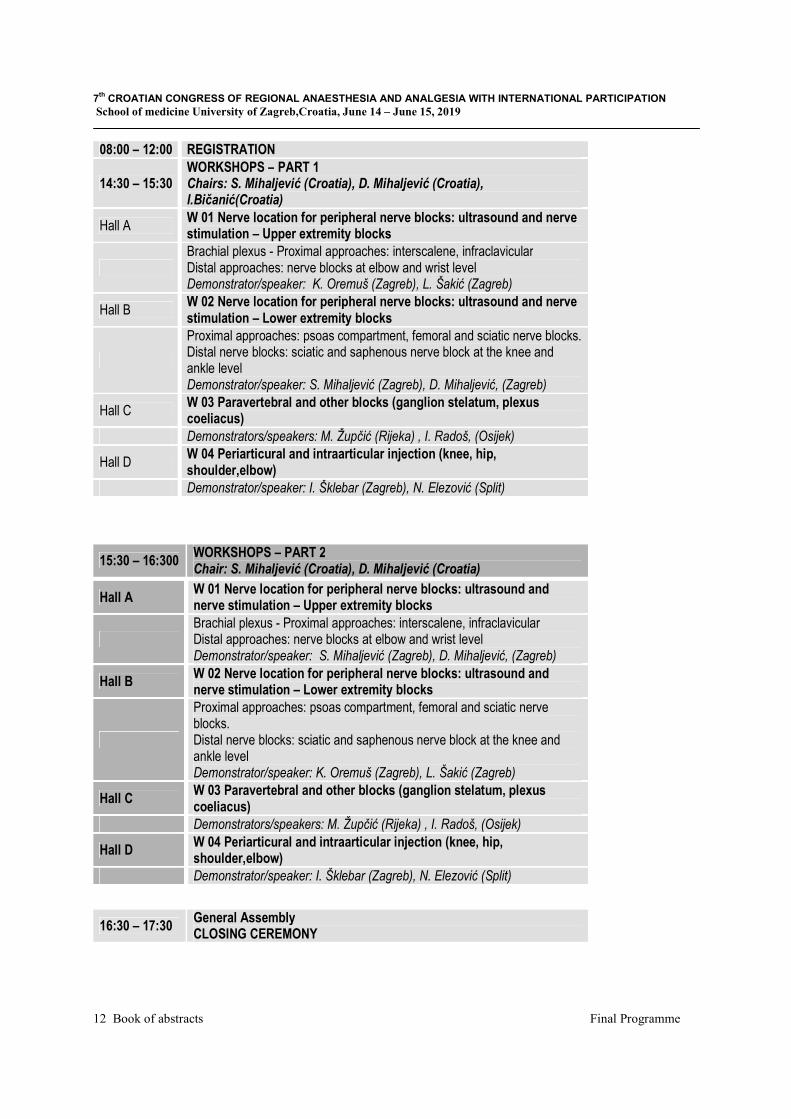
08:00 – 12:00 REGISTRATION
14:30 – 15:30 WORKSHOPS – PART 1 Chairs: S. Mihaljević (Croatia), D. Mihaljević (Croatia), I.Bičanić(Croatia)
Hall A W 01 Nerve location for peripheral nerve blocks: ultrasound and nerve stimulation – Upper extremity blocks
Brachial plexus - Proximal approaches: interscalene, infraclavicular Distal approaches: nerve blocks at elbow and wrist level Demonstrator/speaker: K. Oremuš (Zagreb), L. Šakić (Zagreb)
Hall B W 02 Nerve location for peripheral nerve blocks: ultrasound and nerve stimulation – Lower extremity blocks
Proximal approaches: psoas compartment, femoral and sciatic nerve blocks. Distal nerve blocks: sciatic and saphenous nerve block at the knee and ankle level Demonstrator/speaker: S. Mihaljević (Zagreb), D. Mihaljević, (Zagreb)
Hall C W 03 Paravertebral and other blocks (ganglion stelatum, plexus coeliacus)
Demonstrators/speakers: M. Župčić (Rijeka) , I. Radoš, (Osijek)
Hall D W 04 Periarticural and intraarticular injection (knee, hip, shoulder,elbow)
Demonstrator/speaker: I. Šklebar (Zagreb), N. Elezović (Split)
15:30 – 16:300 WORKSHOPS – PART 2 Chair: S. Mihaljević (Croatia), D. Mihaljević (Croatia)
Hall A W 01 Nerve location for peripheral nerve blocks: ultrasound and nerve stimulation – Upper extremity blocks
Brachial plexus - Proximal approaches: interscalene, infraclavicular Distal approaches: nerve blocks at elbow and wrist level Demonstrator/speaker: S. Mihaljević (Zagreb), D. Mihaljević, (Zagreb)
Hall B W 02 Nerve location for peripheral nerve blocks: ultrasound and nerve stimulation – Lower extremity blocks
Proximal approaches: psoas compartment, femoral and sciatic nerve blocks. Distal nerve blocks: sciatic and saphenous nerve block at the knee and ankle level Demonstrator/speaker: K. Oremuš (Zagreb), L. Šakić (Zagreb)
Hall C W 03 Paravertebral and other blocks (ganglion stelatum, plexus coeliacus)
Demonstrators/speakers: M. Župčić (Rijeka) , I. Radoš, (Osijek)
Hall D W 04 Periarticural and intraarticular injection (knee, hip, shoulder,elbow)
Demonstrator/speaker: I. Šklebar (Zagreb), N. Elezović (Split)
16:30 – 17:30 General Assembly CLOSING CEREMONY

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 13
Poster presentations:
10:30 – 11:00 Friday 14
POSTER PRESENTATIONS (P 1 – P 7 ) Chair: T. Šimurina (Croatia), L. Šakić (Croatia)
P1. Effect of lidocaine on perioperative proinflammatory cytokine levels in blood and cerebrospinal fluid in cerebral aneurysm patients – study concept MARIJANA MATAS, ANTE SEKULIĆ,VLATKA SOTOŠEK TOKMADŽIĆ, ROBERT LIKIĆ,ANA KOZMAR, IVANA BUREŠ, MARTIN LACKOVIĆ
P2. Postpuncture headache risk using ocular ultrasound MAŠA KONTIC, DINKO TONKOVIĆ,SANDA ROŽANKOVIĆ P3. Anesthesia and analgesia for French Ambulatory Extraperitoneal Cesarean Section technique of extraabdominal cesarean section IVAN IVANOVSKI, KATARINA KLIČAN JAIĆ, MAJA PEŠIĆ, ŽELJKO IVANEC, MARINKO VUČIĆ, KRUNOSLAV KUNA
P4. Trend and development of epidural analgesia and anesthesia in the maternity ward of Sestre Milosrdnice University Hosptal Center over the past ten years (2008-2018) KATARINA KLIČAN JAIĆ, MAJA PEŠIĆ, IVAN IVANOVSKI , IVONA BANOŽIĆ , KRUNOSLAV KUNA, MARINKO VUČIĆ P5. Is regional anaesthesia superior regarding to POCD? MARIJANA ŽURA, ANDREA PERŠIN BERAKOVIĆ, IVA BAČAK KOCMAN, DUBRAVKA BARTOLEK HAMP, SLOBODAN MIHALJEVIĆ P6. The most common complications of spinal anaesthesia for caesarean section TONKA BUJAS, TEA MEDVED, KRISTINA NJERŠ, IVAN ŠKLEBAR,
P7. Fascia iliaca compartment block for hip fractures TEA FABIJANIĆ, DANIELA BANDIĆ PAVLOVIĆ
16:00 – 16:30 Friday 14
POSTER PRESENTATIONS (P 8 – P15) Chair: D. Bandić Pavlović (Zagreb), I. Bičanić (Zagreb)
P8. QUADRATUS LUMBORUM BLOCK- better immediate patient outcome in abdominal surgery KARMELIĆ DORA, BUDIĆ NEDILJKA, PETROVIĆ IGOR, HABIJANEC BORNA, MIHALJEVIĆ SLOBODAN P9. intermediate cervical plexus block in cervical spine surgery patients ANITA MISIR, DANIELA BANDIĆ PAVLOVIĆ, NATAŠA KOVAČ, MARTINA MIKLIĆ BUBLIĆ, DINKO TONKOVIĆ, SLOBODAN MIHALJEVIĆ
P10. Interscalene block after left upper lobectomy: A case study
AGATA ŠKUNCA , ALENKA CAR ŠOŠTARIĆ, MARIO MANDUŠIĆ, MIRELA DOBRIĆ
P11. Femoral block 3 in 1 and auriculopuncture in the treatment of postoperative pain- case report ZRINKA OREŠKOVIĆ, BRANKO TRIPKOVIĆ, IVANA STIPČIĆ, KATICA KODŽOMAN P12. Ultrasound-guided rectus sheet block; intraoperative and postoperative analgesic technique for umbilical hernia repair surgery in a 5 year old child ANA FUĆAK PRIMC1,SLOBODAN MIĆIĆ,1 GORAN PAVELIĆ1,MIROSLAV ŽUPČIĆ1,2,3
P13. Plasma levels of interleukin-6 in response to two different techniques of postoperative analgesia GORDANA KRISTEK, IVAN RADOŠ, DALIBOR KRISTEK, SONJA ŠKILJIĆ, NENAD NEŠKOVIĆ, HRVOJE VINKOVIĆ, IVANA HARŠANJI-DRENJANČEVIĆ,

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 14
P14. Regional anaesthesia: everyday practice on Department of Traumatology in first quarter of 2019 ANA MILETIĆ, I. ROSO, T. BEKER, M. DOBRIĆ P15. Enhanced multimodal analgesia controlled by staff „truth about opioids“ MARINA BARKOVIĆ, MIRO ŽUPČIĆ 10:30 – 11:00 Saturday 15
POSTER PRESENTATIONS (P 16– P 21 ) Chair: E.Goluža, (Zagreb), N. Elezović (Split)
P16. Fluoroscopic-guided sacroiliac joint injections for relieving chronic axial low back pain in a tertiary Hospital in Croatia: a preliminary study KALAGAC FABRIS LADA, ZANGHIRELLA-MARETIC SAMANTHA, BIBERIĆ MAŠA, ZRNA SINIŠA, KOŠETO ALEKSANDAR, RADOLOVIĆ KREŠIMIR
P17. IVRA and its adjuvants in limb surgery FILIP MEDIĆ, FILIP MUSTAČ, MAŠA ALFIREVIĆ, INGA MLADIĆ BATINICA
P18. Approaches and Management in Abdominoplasty surgery with von Willebrand Disease in an Ambulatory Setting JUDITH ADRIANNE DEUTSCH ,. DINKO BAGATIN ,JOHANN NEMRAVA, KATA ŠAKIĆ, TOMICA BAGATIN P19. Local infiltration analgesia for reduction of postoperative pain following general anaesthesia for mammoplasty in day surgery JOHANN NEMRAVA ., DINKO BAGATIN ., KATA ŠAKIĆ ., TOMICA BAGATIN .,JUDITH ADRIANNE DEUTSCH
P20. Trends in the administration of local anaesthesia for dental procedures IVANA SPLIVALO , TOMISLAV ŠKLEBAR , IVAN ŠKLEBAR
P21 Performance, tolerance and safety of Spinal Anaesthesia for ureterorenoscopy (URS) and in situ lithotripsy (Review) SANDRA NENADIĆ ŠPRAJC1, ELEONORA GOLUŽA1, IGOR VLATKOVIĆ1, MARJAN MARIĆ2, ŽELJKO KAŠTELAN2, SLOBODAN MIHALJEVIĆ1 P22 Scalp block as safe method for emergency operation in paediatric neurosurgery LUK A VRDOLJAK ,MAŠA DELIĆ, ŽELJKA ZADRO, BARBARA BORAS, MARKO BOŠNJAK, IVANA BULIĆ, MARIJA BOŠNJAK, JOSIP PALADINO, VASILIJE STAMBOLIJA
23. P Bilateral intermediate cervical block with general anesthesia for right sided thyroid lobectomy, a case report DANIJEL KNEŽEVIĆ1, EMANUEL BOROVIĆ1, BERISLAV BARBALIĆ1 24. P. Effect of superficial cervical block on early postoperative recovery and reduction of analgesia in patients following anterior approach cervical spine surgery
JOSIP KOVAČEVIĆ, VASILIJE STAMBOLIJA, MIROSLAV VUKIĆ,MARIN LOZIĆ, IVAN DOMAZET, MARTINA MIKLIĆ BUBLIĆ, LUKA VRDOLJAK, DUJE ŠTAMBUK
7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 15
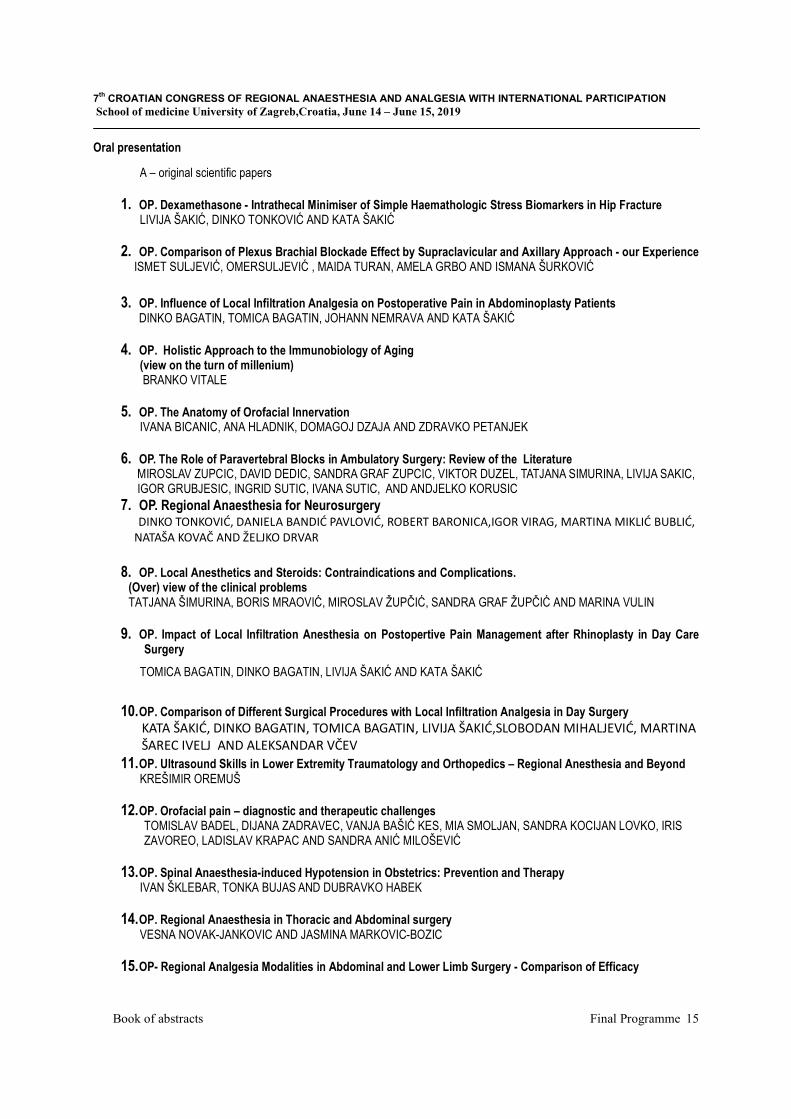
Oral presentation
A – original scientific papers
1. OP. Dexamethasone - Intrathecal Minimiser of Simple Haemathologic Stress Biomarkers in Hip Fracture LIVIJA ŠAKIĆ, DINKO TONKOVIĆ AND KATA ŠAKIĆ
2. OP. Comparison of Plexus Brachial Blockade Effect by Supraclavicular and Axillary Approach - our Experience ISMET SULJEVIĆ, OMERSULJEVIĆ , MAIDA TURAN, AMELA GRBO AND ISMANA ŠURKOVIĆ
3. OP. Influence of Local Infiltration Analgesia on Postoperative Pain in Abdominoplasty Patients DINKO BAGATIN, TOMICA BAGATIN, JOHANN NEMRAVA AND KATA ŠAKIĆ
4. OP. Holistic Approach to the Immunobiology of Aging (view on the turn of millenium) BRANKO VITALE
5. OP. The Anatomy of Orofacial Innervation IVANA BICANIC, ANA HLADNIK, DOMAGOJ DZAJA AND ZDRAVKO PETANJEK
6. OP. The Role of Paravertebral Blocks in Ambulatory Surgery: Review of the Literature MIROSLAV ZUPCIC, DAVID DEDIC, SANDRA GRAF ZUPCIC, VIKTOR DUZEL, TATJANA SIMURINA, LIVIJA SAKIC, IGOR GRUBJESIC, INGRID SUTIC, IVANA SUTIC, AND ANDJELKO KORUSIC
7. OP. Regional Anaesthesia for Neurosurgery DINKO TONKOVIĆ, DANIELA BANDIĆ PAVLOVIĆ, ROBERT BARONICA,IGOR VIRAG, MARTINA MIKLIĆ BUBLIĆ, NATAŠA KOVAČ AND ŽELJKO DRVAR
8. OP. Local Anesthetics and Steroids: Contraindications and Complications. (Over) view of the clinical problems TATJANA ŠIMURINA, BORIS MRAOVIĆ, MIROSLAV ŽUPČIĆ, SANDRA GRAF ŽUPČIĆ AND MARINA VULIN
9. OP. Impact of Local Infiltration Anesthesia on Postopertive Pain Management after Rhinoplasty in Day Care Surgery
TOMICA BAGATIN, DINKO BAGATIN, LIVIJA ŠAKIĆ AND KATA ŠAKIĆ
10. OP. Comparison of Different Surgical Procedures with Local Infiltration Analgesia in Day Surgery KATA ŠAKIĆ, DINKO BAGATIN, TOMICA BAGATIN, LIVIJA ŠAKIĆ,SLOBODAN MIHALJEVIĆ, MARTINA ŠAREC IVELJ AND ALEKSANDAR VČEV
11. OP. Ultrasound Skills in Lower Extremity Traumatology and Orthopedics – Regional Anesthesia and Beyond KREŠIMIR OREMUŠ
12. OP. Orofacial pain – diagnostic and therapeutic challenges
TOMISLAV BADEL, DIJANA ZADRAVEC, VANJA BAŠIĆ KES, MIA SMOLJAN, SANDRA KOCIJAN LOVKO, IRIS ZAVOREO, LADISLAV KRAPAC AND SANDRA ANIĆ MILOŠEVIĆ
13. OP. Spinal Anaesthesia-induced Hypotension in Obstetrics: Prevention and Therapy
IVAN ŠKLEBAR, TONKA BUJAS AND DUBRAVKO HABEK
14. OP. Regional Anaesthesia in Thoracic and Abdominal surgery VESNA NOVAK-JANKOVIC AND JASMINA MARKOVIC-BOZIC
15. OP- Regional Analgesia Modalities in Abdominal and Lower Limb Surgery - Comparison of Efficacy

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 16
JASMINKA PERŠEC AND MONIKA ŠERIĆ
16. OP. Applications and Critical Evaluation of Fascia Iliaca Compartment Block and Quadratus Lumborum Block for Orthopaedic Procedures IVAN BOHAČEK, MIHOVIL PLEČKO, BRANKO TRIPKOVIĆ, MISLAV ČIMIĆ, MISLAV JELIĆ AND DOMAGOJ DELIMAR
17. OP- Medico- Legal Responsibility in Management of Acute and Chronic Pain in Obstetric DUBRAVKO HABEK AND IVAN ŠKLEBAR
18. OP Epidural Analgesia in Multipy Injured Patients with Severe Chest Trauma: Two Case Reports and Literature Review
NINA SULEN, TATJANA ŠIMURINA. EDI KARUC AND ANELA TOLIĆ
19. OP Major obstetric haemorhage MANO DORAISWAMI 20.OP Enhanced recovery in caesarean section VIKTOR DUZEL
21.OP Minimally invasive treatments for chronic pain
IVAN RADOS

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 17
Poster presentation
01 P. Effect of lidocaine on perioperative proinflammatory cytokine levels in blood and cerebrospinal fluid in cerebral aneurysm patients – study concept
MATAS MARIJANA1, SEKULIĆ ANTE1,2, SOTOŠEK TOKMADŽIĆ VLATKA3, ROBERT LIKIĆ2, KOZMAR ANA4, BUREŠ IVANA1, LACKOVIĆ MARTIN1
1University Hospital Center Zagreb, Department of anesthesiology, reanimatology and intensive care, Zagreb, Croatia
2University of Zagreb, School of Medicine, Zagreb, Croatia
3University of Rijeka, Faculty of Medicine, Rijeka, Croatia
4University Hospital Center Zagreb, Department of laboratory diagnostics, Zagreb, Croatia E-mail:[email protected]
Background and purpose: Cerebral aneurysm surgery has significant mortality and morbidity rate. Inflammation plays a key role in the pathogenesis of intracranial aneurysms, their rupture, subarachnoid haemorrhage and neurologic complications. Primary neurosurgical brain injury activates immune cells and triggers cytokine release. Proinflammatory cytokine level in blood and cerebrospinal fluid is an indicator of inflammatory response. Cytokines contribute to secondary brain injury and can worsen the outcome of the treatment. Preventing secondary brain injury by modulating inflammatory response represents a therapeutic target in neuroanesthesiology.
Lidocaine is local anesthetic that can be applied in neurosurgery as regional anesthesia of the scalp and as topical anesthesia of the throat prior to direct laryngoscopy and endotracheal intubation. Except analgetic, lidocaine has systemic anti-inflammatory and neuroprotective effect. It acts through several mechanisms on various types of immune cells producing immunosuppressing effect. Lidocaine passes through blood-brain barrier and can act on activated microglia within central nervous system causing attenuation of immune response.
Primary aim of this prospective randomized trial is to determine influence of lidocaine administration on inflammatory cytokine levels in serum and cerebrospinal fluid during cerebral aneurysm surgery.
We hypothesized that lidocaine administration during cerebral aneurysm surgery would significantly change levels of pro-inflammatory cytokines in cerebrospinal fluid and serum. Lower concentrations of pro-inflammatory cytokines can possibly contribute to better outcome and significantly lower incidence of postoperative complications.
Materials and methods: Enzyme-immunochemical analysis will be used to measure levels of cytokines interleukin-1β, interleukin-6 and tumor necrosis factor-α in cerebrospinal fluid and serum in two groups of patients. Investigation group will have, during cerebrovascular surgery under general anesthesia, regional anesthesia of the scalp and topical anesthesia of the throat

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 18
prior to laryngoscopy, all done with lidocaine. Control group will have general anesthesia without lidocaine administration.
02 P. Postpuncture headache risk using ocular ultrasound
MAŠA KONTIC1, DINKO TONKOVIĆ2,SANDA ROŽANKOVIĆ3
1Department ofanaesthesiology, reanimatologyandintensivetreatmentGeneral Hospital SisakJ.J. Strossmayera 59, Sisak, Croatia 2Department of anaesthesiology, reanimatology and intensive medicine, Neurosurgical, otorhinolaringology and oculistic department, Clinical Hospital Centre Zagreb, Zagreb, Croatia 3Department of ofthalmology,General Hospital Sisak , Sisak, Croatia E-mail:[email protected]
POSTPUNCTURE HEADACHE RISK USING OCULAR ULTRASOUND
Maša Kontic1,Dinko Tonković2,Sanda Rožanković3
1Department ofanaesthesiology, reanimatologyandintensivetreatmentGeneral Hospital SisakJ.J. Strossmayera 59, Sisak, Croatia 2Clinic for anaesthesiology, reanimatologyandintensivetreatmentNeurosurgical, otorhinolaringologyandoculisticdepartment, ClinicalHospital Centre Zagreb, Zagreb, Croatia 3Oculistic department General Hospital Sisak, Sisak, Croatia
E-mail; [email protected]
BACKGROUND AND PURPOSE: This study reveals that postpunctural headache has a notable effect on quality of life in postpartal period. It is of clinical interest if the implementation of ocular ultrasound as diagnostic tool will affect the manifestation of postpuncture headache, following blood pressure and opticus diameter MATERIAL AND METHODS:Cross-sectional study carried on19 healthy pregnant women betweeen 19 and 34 years of age, provided written informed consent to participate in this trial.The study was conducted through a three-month period .There is no previous data about headaches. Hemodynamic and optical nerve measurements were assessed both preoperatively and at 12 hours after anaesthesia using B Mode probe 20Hz.Spinal anaesthesia was performed using 0,5% hyperbar bupivacaine(5mg/kg), needle 26G, nad analgetics including paracetamol (10mg/kg). During postpartal period some subjects reported postpuncture headache. RESULTS: Using Student T-test, our findings don't show the corelation between the change in value of opticus diameter after the spinal anaestesia and the median blood pressure regarding the postpuncture headaches. The probability of change in average blood pressure measurements before and after anaesthesia, is not statistically relevant. CONCLUSION: The obtained clinical measurements confirm preventive measures of postpuncture headache and usage of thin injection needles. Ocular ultrasound is a useful diagnostic tool

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 19
in etiology of headaches.In this study, we currently conclude that papilla stagnans was not observed after spinal anaesthesia. Risk factors involve younger age and positive headache medical history.The results of our study are valid for any spinal anaesthesia.
03 P. Anesthesia and analgesia for French Ambulatory Extraperitoneal Cesarean Section technique of extraabdominal cesarean section IVAN IVANOVSKI 1, KATARINA KLIČAN JAIĆ1, MAJA PEŠIĆ1, ŽELJKO IVANEC1, MARINKO VUČIĆ1, KRUNOSLAV KUNA 2
1Department of Anesthesiology, Intensive Care Medicine and Pain Management, Sestre milosrdnice University Hospital Center, Zagreb, Croatia 2Clinical Department of Obstetrics, "Sestre milosrdnice" University Hospital Center, Zagreb, Croatia E-mail:[email protected] Background and purpose: Cesarean section is correlated with higher number of complications and higher postoperative pain scores which prolongs recovery in comparison with vaginal delivery for three to five days. With relatively new and advanced surgical technique of extraabdominal cesarean section called French Ambulatory Extraperitoneal Cesarean Section (FAUCS) there are fewer postoperative complications and lower pain scores. Materials and methods: In this case report we will be presenting one of our first cases. We started with this surgical technique in the beginning of 2019 for the first time in Croatia. The type of anesthesia for this procedure is a spinal anesthesia as cooperation of the patient is essential for successful extraction of the neonate. Because this procedure is less painful it is possible to reduce the dosage of spinal local anesthetic in comparison with the usual dose for classical cesarean section. Lower local anesthetic dose enables faster recovery of motor function, and with that faster mobilization of the patient. At the end of the procedure we add analgesia with Trans-Abdominal Plain (TAP) block. Results: TAP block led to complete elimination of day one postoperative pain. The necessity for pain medication therapy after the first postoperative day was reduced to the minimal doses, and opiate analgesics were not used. Conclusions: This combination of FAUCS and regional anesthesia enabled faster patient recovery with many benefits for woman and newborn.

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 20
04 P. Trend and development of epidural analgesia and anesthesia in the maternity ward of Sestre Milosrdnice University Hosptal Center over the past ten years (2008-2018) KATARINA KLIČAN JAIĆ1, MAJA PEŠIĆ1, IVAN IVANOVSKI1, IVONA BANOŽIĆ1, KRUNOSLAV KUNA2, MARINKO VUČIĆ1
1Department of Anesthesiology, Intensive Care Medicine and Pain Management, Sestre milosrdnice University Hospital Center, Zagreb, Croatia 2Clinical Department of Obstetrics, "Sestre milosrdnice" University Hospital Center, Zagreb, Croatia E-mail:[email protected] Background and purpose: Epidural analgesia is common pain relieving method for delivery in obstetrics. During last decades epidural analgesia is even more prevalent and is one of the most common regional anesthesia techniques. Application of epidural analgesia relieves pain and enables women to be active during labor. Today it is considered to be the best way to treat labor pain as there are no side effects to the baby and it makes the whole experience pleasant to the mother. Materials and methods: We researched trends in numbers of epidural analgesia and anesthesia for labor delivery in the maternity ward of Sestre Milosrdnice University Hospital Center form 2008 until 2018. It was the retrospective cohort study. We correlated the number of epidural analgesia and number of epidural anesthesia for emergency cesarean section in patients with placed epidural catheter for vaginal delivery to total number of vaginal deliveries. Results: We noticed almost 14% increases in number of epidural analgesia and significant increase in numbers of epidural anesthesia since 2008. Our results could be anticipated as in last few years the number one indication for implementation of epidural anesthesia in vaginal delivery is patient request. Coincidence of increase in epidural analgesia for vaginal delivery and widening of indications for cesarean section expectedly increase the numbers of epidural anesthesia. Same is seen in our data. Conclusion: In our study we showed that epidural analgesia are preferred analgesia method for vaginal delivery and anesthesia method for emergency cesarean section at our ward. Availability of 24 h anesthesia care, good cooperation of obstetric - anesthetic team, and rich experience had definitely contributed to this positive trend in numbers of epidural blocks for vaginal delivery and cesarean section in our hospital.
7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 21
P05 Is regional anaesthesia superior regarding to POCD? MARIJANA ŽURA1, ANDREA PERŠIN BERAKOVIĆ1, IVA BAČAK KOCMAN1, DUBRAVKA BARTOLEK HAMP1, SLOBODAN MIHALJEVIĆ1 1University Hospital Centre Zagreb, Department of Anaesthesiology, Reanimatology and Intensive Care, Zagreb, Croatia E-mail: [email protected] Background and purpose Postoperative cognitive dysfunction (POCD) is a long-lasting cognitive decline after surgery characterized by impared concentration, memory and learning. Untill recently, it has been thought regional anaesthesia prevents POCD in three different ways: by providing superior analgesia, decreasing the use of medication which leads to POCD and by blunting inflammatory and stress response to surgery. There are numerous risk factors which may contribute to POCD. They can be patient-related:advanced age, education, genetics, metabolic syndrome, neurologic disease (vascular dementia and Alzheimer disease) and anaesthesia-related: intraoperative hypotension, hypoxia, embolism, medication, postoperative infection. However, the main reason for POCD is neuroinflammation. Results Studies have shown that derived immune cells stimulate neuroinflammation and subsequent neuronal damage. POCD is associated with elevated levels of plasma inflammatory cytokines, including tumor necrosis factor- α (TNF-α) and interleukin-6 (IL-6). IL-1β and IL-6 levels in the cerebrospinal fluid (CSF) of patients with POCD are higher than those of patients with normal cognitive function after surgery. This explains why studies show that learning and memory function was impared by extensive operations- orthopaedic or cardiovascular- and not by type of anaesthesia. Neuroinflammation, particularly in the hippocampus, has been proved to be one of the main causes of POCD. Microglia are the major resident macrophages in the central nervous system which are activated by protein and other signal from injury sites. Cytokines secreted from microglia can directly damage neurons and recruit more immune cells which penetrate into brain parenchyma further exacerbating brain injury. Materials (Patients) and methods Analysis of medical literature. Conclusion General anaesthetics can produce long-lasting cognitive disfunction under certain circumstances, but the incidence of POCD is similar after regional and general anaesthesia. Therapies which prevent or reduce cytokine secretion may be effective for POCD treatment. In addition, it is of outmost importance to determine which tests and preventive strategies might be useful for preventing POCD.

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 22
06 P. The most common complications of spinal anaesthesia for caesarean section TONKA BUJAS1, TEA MEDVED2, KRISTINA NJERŠ1, IVAN ŠKLEBAR2,3,4,5
1Dr. Josip Benčević General Hospital, Department of Anaesthesiology, Reanimatology and Intensive Care, Slavonski Brod, Croatia 2Sveti Duh University Hospital, Department of Anaesthesiology, Resuscitation and Intensive Care Medicine, Zagreb, Croatia 3Catholic University of Croatia, Zagreb, Croatia 4Faculty of Medicine, Josip JurajStrossmayer University of Osijek, Osijek, Croatia 5Bjelovar University of Applied Sciences, Bjelovar, Croatia E-mail:[email protected] Background and purpose: Spinal anaesthesia (SA) is the preferred method for elective and emergency caesarean section due to its safety, simplicity and quick onset of sensory and motor block. However, it may be accompanied by complications, most commonly hypotension, post-dural puncture headache, nausea and vomiting, pruritus and shivering. The aim of the research was to determine the frequency of the most common complications of spinal anaesthesia for caesarean section in our sample and suggest possible improvements of the internal algorithm for spinal anaesthesia. Materials (Patients) and methods: A prospective study was conducted on a sample of 63 women undergoing caesarean section performed under SA. The parturientsreceived an H2-blocker in premedication and were prehydrated with a crystalloid infusion. A hyperbaric mixture of 8-12.5 mg Levobupivacaine and 12.5-25 mcg Fentanyl was administered intrathecally. The patients were monitored foranycomplications during operation. Haemodynamic monitoring, administration of vasoconstrictors and fluid replacement were applied during the procedure. On the first post-operative day, the patients were monitored for any late onset complications linked to SA. Results: The average age of the patients was 33.19. The block was unsuccessful in 4.76% of the cases. After spinal anaesthesia, 61.9% of the patients experienced hypotension, which was treated with a bolus-dosevasopressor. 46.03% of the patients reported general weakness and 31.75% reported nausea, 30% of which vomited. Post-dural puncture headache was experienced by 7.93% of the patients, 17.46% reported back pain, whereas 19.04% complained of pruritus and 14.28% reported shivering. Postoperatively, 1.59% of the patients presented with hypotension and 15.87% experienced nausea, 20% of which also reported the urge to vomit. Conclusion: The incidence of the most common complications in our study correlates with the results of existing studies. The frequency of hypotension, nausea and vomiting could be reduced with prophylactic and continuous administration of vasopressors instead of bolus doses as well as previous administration of 5-HT3 antagonist.

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 23
07 P. Fascia iliaca compartment block for hip fractures TEA FABIJANIĆ1, DANIELA BANDIĆ PAVLOVIĆ 2,3
1Department of Emergency Medicine Sisak-Moslavina County, The Croatian Institute of Emergency Medicine, Croatia 2 Medical school, University of Zagreb 3 University Hospital Centre Zagreb, Department of anesthesiology, reanimatology and ICM, Zagreb, Croatia E-mail:[email protected] Background and purpose: Considering high incidence of hip fractures and expecting morbidity, as well as need for pain management we searched existing literature for clinical evidence on efficacy of fascia iliaca compartment block (FICB) as adequate or superior mode of analgesia over others in use. Materials and methods: We searched Pubmed, Science Direct and Google Scholar using keywords FICB and hip fracture, with inclusion criteria that the article had to be a clinical trial published in the past 10 years, number of subjects at least 20 or more per trial. Exclusion criteria was if found severe methodological problem. Results: We found in total 22 papers addressing the issue. In 3 papers the patient’s pain was treated with FICB immediately after the injuryin the emergency setting before reaching the hospital performed by paramedics in a single shot or in a hospital setting with the procedure performed by physicians as a continuous drug infusion. The injection method of choice was anatomically or ultrasound guided technique, while electrostimulator was used in just 2 papers. Results were promising in ways that personnel with limited experience could perform the procedure safe and fast, as well as better pain reduction in patients comparing it with systemic analgesics. Other trials used the block as late perioperative and postoperative analgesia care analysing lower rate of complications compared to other treatment modalities. Drugs used in most of the studies were either ropivacaine and bupivacaine, while only 3 studies used levobupivacaine and two epinephrine. Conclusions: Findings were positive in favour of FICB considering postoperative pain management, although some studies showed no significant lower intake of oral analgesics. All 3 studies considering intra-articular analgesia in contrast to FICB had superior analgetic effect. We conclude by reviewing contemporary literature that FICB can be considered as a valuable supplement to the initial hip fracture treatment.

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 24
08 P. QUADRATUS LUMBORUM BLOCK- better immediate patient outcome in abdominal surgery KARMELIĆ DORA1, BUDIĆ NEDILJKA2, PETROVIĆ IGOR2, HABIJANEC BORNA3, MIHALJEVIĆ SLOBODAN1 1Clinic for Anaesthesiology, Reanimatology and Intensive Care Medicine, University Hospital Centre Zagreb, Kišpatićeva 12, Zagreb 1Data Raven, Trpinjska 4, Zagreb 1Clinic for Surgery, Department of Hepatobiliary Surgery and transplantation, University Hospital Centre Zagreb, Kišpatićeva 12, Zagreb E-mail:[email protected] Introduction: Since first time described in 2007, QLB had proved as useful method for post-operative pain control. We intended to evaluate if block implementation can reduce opioidand non-steroidanti-inflammatory drugs (NSAID) intake intraoperatively and postoperatively. Aim: The aim of our study was to evaluate the effect of single shot quadratus lumborum block (QLB) on immediate patient outcomes in open and laparoscopic abdominal surgery. Materials and methods: We examined53 abdominal surgery patients who received the QLB, either pre- or post-operatively during a six months period, and matched them to 23 patients who did not receive a block for the same type of surgery. Theultrasound guided QLB type 2was performed using a linear probe, predominantlyropivacain was used, in dose of up to 3mg/kg and volume of approximately 0.3 ml/kg. Patient refusal was the only exclusion criteria. Patients were examined for sensation changes in trunk area withlight tweakingiceand needle pricking, 5 minutes and 15 minutes afterQLB application. Intraoperatively, patient’s heart rate and blood pressure changes were monitored. Postoperatively, patients were observed for wakefulness, mobility, pain while still, and pain in Valsalva maneuver or during coughing. NRS (numerical rating scale) and VAS (visual analog scale) values were noted as well as opioid and NSAIDadministration 48 hours postoperatively. Results: QLB patient group immediately after surgery was more alert, mobile and had reported lower pain levels. Use of opioids was significantly reduced both during and two days following surgery in the QLB group, while the use of NSAID was not significantly different. No complications of the block were observed. Conclusion: QLB improves early patient outcome in terms of postoperative pain and reduction of need for opioid analgesics in abdominal surgery patients.

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 25
09 P. Intermediate cervical plexus block in cervical spine surgery patients ANITA MISIR1, DANIELA BANDIĆ PAVLOVIĆ1,2, NATAŠA KOVAČ1, MARTINA MIKLIĆ BUBLIĆ1, DINKO TONKOVIĆ1,2, SLOBODAN MIHALJEVIĆ1,2
1University Hospital Centre Zagreb, Department of anesthesiology, reanimatology and ICM, Zagreb, Croatia 2Medical School, University of Zagreb E-mail:[email protected] Background and purpose: Cervical spine surgeries are being performed in an increasing number and with a short stay in hospital.Intermediate cervical plexus block (ICPB) insure analgesia and anesthesia for head and neck surgery and enhance recovery after surgery. Purpose of our research was to establish the correlation between intraoperative hemodynamic stability and the need for intra and postoperative analgesia and the application of the ICPB in patients who underwent elective cervical spine surgery. Materials and methods: We collected retrospectively data from 20 patients, between 33 and 58 years, ASA I-II, operated in our center in period from January 2018 to March 2019. Results: A total of 10 patients (50 %) received ICPB ( 0,375% levobupivacaine)after induction in general anesthesia.The patients who received the ICBP were hemodynamically stable considering intraoperative data od systolic blood pressure, diastolic blood pressure and heart rate (within 20% of baseline value). During the operation the overall need for intraoperative analgesia was lower. There was no major difference in hospital discharge, 2 patients with ICPB (0,1%) and 3 patients without block (0,15%) were discharged first postoperative day; 8 patients with ICPB (0,4%) and 7 patients without block (0,35 %) second postoperativeday. The postoperative analgesic consumption was similar in both groups. Conclusions: We point that ICPB can ensure hemodynamic stability of patient during operation, but we did not find significat coherence with hospital discharge and analgesics consumption.

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 26
10 P. Interscalene block after left upper lobectomy: A case study
AGATA ŠKUNCA 1, ALENKA CAR ŠOŠTARIĆ1, MARIO MANDUŠIĆ2, MIRELA DOBRIĆ1 1 Sestre milosrdnice University Hospital Center, Department of Anesthesiology, Reanimatology and Intensive care, Croatia 2 General hospital Nova Gradiška, Department of Anesthesiology, Reanimatology and Intensive care, Croatia E-mail:[email protected]
The intescalene block is used in procedures on the shoulder and proximal humerus procedures. Using the usual volumes of local anaesthetics an incidence of 100% occurs in the phrenic nerve as well as hemidiaphragmatic paresis and a 25 - 30% reduction of FEV1 and FVC. Due to these consequences that occur while introducing the interscalene block, this procedure might not be suitable for patients with respiratory insufficiency. A 73-year old patient with a right proximal humerus fracture was admitted to the Traumatology Clinic. Her medical history said that she had had an upper left lobectomy three years ago due to lung adenocarcinoma which resulted in left vocal cord paralysis. In addition to that, 30 years ago, she had a mastectomy to treat breast cancer. The patient also had diabetes mellitus type 2, arterial hypertension and had recovered from left facial nerve paralysis, leaving her with a left eyelid ptosis. The patient went through a preoperative anaesthetic assessment and was prepared for surgery. After considering the comorbidity and the possible complications, the method of regional anaesthesia was opted for. An ultrasound guided interscalene block with a 25 mL dose of 0.75% ropivacaine was performed. 20 minutes after administering the local anaesthetic, the oxygen saturation level decreased to 78% and the patient was given an oxygen mask with the flow rate of 4L/min. The patient was put into an upright sitting position and the oxygen saturation level increased to its normal levels. However, after returning the patient into supine position in order to continue the procedure, oxygen saturation started to decrease again. At this point the procedure was terminated and the patient was moved to the Intensive Care Unit for further monitoring. We feel that with careful risk assessment measures, the patients that have been through a lung lobectomy would be able to successfully undergo the method of regional anaesthesia. Nonetheless, it is necessary to take into consideration whether the fracture was ipsilateral or contralateral in regard to the lobectomy as well as reduce the dose of local anaesthetic. In addition to that, the block should be performed by an anaesthesiologist with experience in regional anaesthesia and awareness of possible risks and complications.

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 27
11 P. Femoral block 3 in 1 and auriculopuncture in the treatment of postoperative pain- case report ZRINKA OREŠKOVIĆ, BRANKO TRIPKOVIĆ, IVANA STIPČIĆ, KATICA KODŽOMAN University Hospital Centre in Zagreb, Department of Orthopaedic Surgery, Zagreb, Croatia E-mail:[email protected] Background and purpose: Postoperative pain after operative procedures is extremely strong and sometimes it reaches 8 and 9 on VAS scale, especially after reoperation procedures where bone destruction is extensive. The role of postoperative analgesia is very important. For this purpose, opioid analgesics are used for continuous infusion in combination with intravenous administration of paracetamol, metamizole and ketoprofen. Materials (Patients) and methods: The female patient was admitted to the Orthopedic Clinic for performing the reoperation after the installation of the total hip endoprothesis. Patient has arterial hypertension and hypothyroidism in medical hystory. She is allergic to most analgesic drugs including fentanyl, alfentanil, tramadol, buprenorphine, paracetamol, piroxicam, propifenazone, codeine, caffeine, diclofenac, ibuprofen. The permitted analgesics are only ketoprofen and oxycodonum. The surgical procedure was performed in spinal anesthesia and at the time of the onset of pain the administration of analgesia began. In this case, postoperative analgesia was complicated due to a very narrow analgesic choice. We applied a femoral nerve block 3 in 1 in combination with a auriculopuncture that has a marked analgesic and sedative effect. The femoral block was performed with ultrasound control with combination of lidocaine and levobupivacaine. Acupuncture was performed with single use sterile needles that were placed on five auricule points (omega2, ShenMen, Zero point, Thalamus and girus cinguli) on both ears and left for 30 minutes and then removed. Results: During the 24h postoperative period, the patient received analgesia on demand with ketoprofen 2 x 100 mg iv. and oxycodon 20 mg iv. The most severe pain was observed after attenuation of spinal anesthesia and immediately prior to block and acupuncture application and the VAS scale was 8 and 9. After that, the pain gradually decreases at VAS 5 and 4 and during the night at 3 and 2. The patient was satisfied with the achieved analgesia, and we avoided side effects of analgesics. Conclusions: The use of femoral block 3 in 1 in combination with auriculopuncture is a very effective method of analgesia after major surgical procedures in the hip area. The number of side effects associated with the use of intravenous analgesics is reduced.

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 28
12 P. Ultrasound-guided rectus sheet block; intraoperative and Postoperative analgesic technique for umbilical hernia repair Surgery in a 5 year old child ANA FUĆAK PRIMC1,SLOBODAN MIĆIĆ,1 GORAN PAVELIĆ1,MIROSLAV ŽUPČIĆ1,2,3 1Clinical hospital centre Rijeka, Department of Anestesiology and Intensive Care Medicine,Croatia 2University of Rijeka, Faculty of Medicine,Rijeka,Croatia 3„JJ Strossmayer“University ,Faculty of Medicine,Osijek,Croatia E-mail:[email protected] Backround and purpose: We present a case report to show intraoperative as well as postoperative analgesic effect of ultrasound guided rectus sheet block, for open umbilical hernia repair in children. A 5-year old boy, 17 kg in weight, without previous known medical history or allergies, was scheduled for planned umbilical hernia repair surgery. We decided to combine general anesthesia with regional anesthesia technique; ultrasound guided rectus sheet block (RSB) for postoperative analgesia. Methods: The boy`s parents agreed and signed the informed consent form. He was premedicated with midazolam intravenously. After induction of general anesthesia with minimal induction dose of sufentanyl, propofol and rocuronium we proceeded with the ultrasound guided RSB. The boy was positioned in supine position to obtain the view of transversus abdominis plane and rectus muscle. Aseptic technique was used. A, high frequency probe was used which was placed first in the mid axillary line then the posterior axillary line for the posterior approach. We first visualized the transverses abdominis muscle, then the internal oblique and external oblique forming the aponeurosis and then rectus muscle was visualized. 6 ml of 0,25 % levobupivacaine bilateraly was infiltrated in the posterior fascia of rectus abdominis muscle. Since we performed the RSB, no further drugs were administrated with sevoflurane maintainance. Results: The surgery was performed without adding neuromuscular blockers or further analgesia and the five year old patient emerged without complications. Postoperatively she did not require any further analgesia. After 12 hours he started experiencing pain requiring non steroid analgetics. Conclusion: The RSB could be effective for intraoperative analgesia as for postoperative analgesia. Ultrasound guidance may reduce the risk of peritoneal puncture, bleeding and visceral injury.

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 29
13 P. Plasma levels of interleukin-6 in response to two different techniques of postoperative analgesia GORDANA KRISTEK1,2, IVAN RADOŠ1,2, DALIBOR KRISTEK1,3, SONJA ŠKILJIĆ1,2, NENAD NEŠKOVIĆ1,2, HRVOJE VINKOVIĆ1,2, IVANA HARŠANJI-DRENJANČEVIĆ1,2
1Faculty of Medicine, Josip JurajStrossmayer University of Osijek, J. Huttlera 4, Osijek, Croatia 2UniversityHospital Osijek, Department of Anaesthesiology, Reanimatology and Intensive Care, J. Huttlera 4, Osijek, Croatia 3UniversityHospital Osijek, Department of Orthopaedics and Traumatology, J. Huttlera 4, Osijek, Croatia E-mail:[email protected] Background and purpose: To compare the effect of two different anesthetic techniques, epidural patient-controlled analgesia (PCEA) using 0.125% levobupivacaine and intravenous patient-controlled analgesia (PCIA) with morphine on plasma interleukine-6 (IL-6) levels and to determine whether the IL-6 is related to postoperative cognitive dysfunction (POCD). Materials and methods: Randomized, prospective, controlled study in an academic hospital. Patients were ≥ 65 years old, scheduled for the femoral fracture fixation from July 2016 to September 2017. Plasma IL-6 concentration was assessed in 3 blood samples (before anesthesia, 24h and 72 h postoperatively). Cognitive functions were assessed using Mini-Mental State Examination (MMSE) preoperatively, from the 1st to the 5th postoperative day and on the day of discharge.Analgesia was assessed by Numerical Rating Scale (NRS) every 3 hours after surgery for 72 hours. Results: Study population included 70 patients, 35 in each group. The incidence of POCD was significantly lower in the PCEA group (9%) than in the PCIA group (31%) (p=0,03). IL-6 values were significantly lower in the PCEA group 72h after surgery (p=0,02). The only predictor of POCD in all patients was level of IL-6 72h after surgery (p=0,03).The NRS pain scores were significantly lower in the PCEA group at all postoperative time points. Conclusions: Postoperative PCEA using 0.125% levobupivacaine provides better pain relief and reduces the incidence of POCD compared to PCIA with morphine in studied population. IL-6 might serve as an indicator to guide the prevention and treatment of POCD.
7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 30
14 P. Regional anaesthesia: everyday practice on Department of Traumatology in first quarter of 2019 ANA MILETIĆ, IVANA ROSO, T. BEKER, MIRELA DOBRIĆ Klinika za traumatologiju, KBC Sestre milosrdnice, Draškovićeva 19, Zagreb
Background and purpose: Regional anaesthesia in trauma and orthopaedics is in widespread use, and represents a safe method in experienced hands, acknowledged by patients and surgeons. Peripheral nerve blocks (PNBs), still lack wider acceptance, when compared to neuroaxial techniques and general anaesthesia, but there has been increasing interest in their use with ultrasound guidance, both for anaesthesia and postoperative pain management. Since the arrival of the first ultrasound machine with linear probe to our department in 2012, the number of PNBs has risen, especially in arm surgery. Its most obvious advantage is good postoperative pain control, the sparing of opioids and their side effects, as well as shorter stay in recovery room. Due to the steep learning curve for PNBs, the majority of anaesthesiologists perform blocks, as well as trainees. We were interested to see what the current share of PNBs is, in total numbers of anaesthesia and to outline potential areas for improvement. Patients and methods: We searched our database for patients with upper or lower extremity surgery, and information was gathered on the type of anaesthesia, number and types of nerve blocks performed and technique utilised. The search covered the first quarter of 2019. Results: In the first quarter of 2019, the overall 287 surgical procedures has been performed on the upper extremity with 34.84% in PNB, 38.67% in intravenous regional anaesthesia (IVRA) and 26.48% in general anaesthesia. Among 585 surgical procedures on lower extremity, 3.41% was performed in peripheral nerve block, 0.85% in IVRA, 68.37% in spinal anesthesia, and 27.35% in general anaesthesia. Postoperative analgesia with femoral catheter has been provided to 75 patients after total knee arthroplasty. Conclusions: Although there is an increase in the number of PNBs, especially in the upper arm surgery and postoperative pain management after hip and knee surgery, there is still under use of PNBs in distal arm surgery and lower leg and foot surgery. The number of patients with ankle block or popliteal blocks, either alone or in combination with saphenous block was surprisingly low. However, it was interesting to note that in January 2019 40% of clavicular osteosynthesis has been done under general anaesthesia, while in March 2019 it was 80%. The majority of surgical anaesthesia with PNBs is accompanied by light intravenous sedation, general anaesthesia with laryngeal mask being less employed.

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 31
15.P Enhanced multimodal analgesia controlled by staff - review of the new
paradigm
MARINA MILETIĆ-BARKOVIĆ1, MIRJANA BARIČIĆ2, KATARINA ŠAKIĆ3
1University Hospital for Orthopaedics and Traumatology Lovran, Department of Anesthesiology 2University Hospital for Orthopaedics and Traumatology Lovran, Department of Physiology 3University Faculty of Medicine Osijek at Poliklinika Bagatin Zagreb
E-mail: [email protected]
Promoting an understanding of opioid addiction among young people for the first time became a
public issue when the American President Donald Trump published the state of the opiate crisis
in June 2018. The Department of Health and Secretary Azar proudly supported the President’s
Commission on Combating Drug Addiction.
The opioid epidemic is today widely recognized as a fundamental healthcare problem. During
2016, more than 63 000 Americans died from drug overdoses, 42 000 from overdosing on
prescription opioids or illegal opioids such as heroin, fentanyl or fentanyl derivatives.
Almost 80% of heroin users initially misuse prescribed opioids. Research suggests that the
misuse of prescribed opioids increases the risk of heroin use by a factor of 40 and consequently
the mortality rate has increased by more than 500% in the period from 2013 to 2016. This
mortality rate is partly related to the availability of fentanyl and its derivatives.
The total economic cost of the opioid crisis has grown to more than 500 billion dollars in 2015.
The key initiator of the opioid epidemic is excessive issuing of prescription drugs by clinicians.
In regard to drugs prescribed up to 80% of the tablets remain unused. Unused tablets not safely
disposed create a potential for future abuse.
In our environment, the possibility remains for staff to monitor patients directly over a period of
24-48 hours and along with highly-trained medical personnel, anesthetic techniques in analgesia
can be applied, whereby the patient safety is retained.

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 32
16 P. Fluoroscopic-guided sacroiliac joint injections for relieving chronic axial low back pain in a tertiary Hospital in Croatia: a preliminary study KALAGAC FABRIS LADA, ZANGHIRELLA-MARETIC SAMANTHA, BIBERIĆ MAŠA, ZRNA SINIŠA, KOŠETO ALEKSANDAR, RADOLOVIĆ KREŠIMIR Departement of Anaesthesia and Chronic Pain Service General Hospital Pula, Croatia E-mail:[email protected] Objective: The sacroiliac joint can be a primary source of pain or part of multifactorial syndromes. As there is no physical examination-based, or radiological feature that definitively establishes a diagnosis of sacroiliac joint pain, diagnostic blocks are regarded as the gold standard. The injection of mixture of plain bupivacaine and triamcinalone acetonide into the sacroiliac joint (SIJ) to relieve chronic low back pain is uncommon in Croatia. The objective of this study was to demonstrate that the efficacy of SIJ block will extend existing treatment options for low back pain.This was a prospective observational interventional study. Patients and methods: All twelve (12) patiens were womens, mean age 39,8 years, mean ODI score 62% , mean GAP score, mean VAS score 9. All patients were 100% positive for the Fortin, Thigh Thrust, Gaeslen and Faber test, but in 76% of patients the Compression and the Distraction test were also positive. The judgment was confirmed by the radiologic abnormalities found on plain radiographs or MRI imaging. Among the patients there was no disorders in the hip joint and no signs of lumbar radiculopathy. Fluoroscopic guided SI injection was performed with a 22G,10 cm spinal needle, and after confirming the entry into the joint with 0.3mL of radiopaque contrast, the mixture of triamcinolone acetonide 40mg and bupivacaine 5mg was injected. The VAS score was evaluated the day after injection, as well as at one week, three weeks, three and six months after. Results: The overall success rate of the SIJ injection was 92%. The median VAS score was 5.4 the day after injection, and an decrease to 2.6 in the first weeks following the intervention with high improvement in quality of life. The median VAS score after three weeks, three months and six month were from 2.5, to 3, to 3.7 respectively, showing a gradualy increase in degree of pain. Firedman's test revealed a significant difference between the VAS scores before and after injections, demostrating the beneficial therapeutic effect of the injection (p<0.05) Conclusion: Fluoroscopic guided SIJ injections are safe and effective and can be used as an alternative treatment of choice for reduction in pain intensity and improved physical function in the patient with low axial pain.

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 33
17 P. IVRA and its adjuvants in limb surgery FILIP MEDIĆ1, FILIP MUSTAČ2, MAŠA ALFIREVIĆ1, INGA MLADIĆ BATINICA3 1School of Medicine University of Zagreb, Zagreb, Šalata 3, Zagreb, Croatia 2Department of Emergency medicine of Zagreb, Zagreb, Croatia 3Department of Anesthesiology, Intensive Care Medicine and Pain Management, Sestre milosrdnice University Hospital Center, Zagreb, Croatia E-mail:[email protected]
Background and purpose: Intravenous regional anesthesia (IVRA) or Bier`s block, is used on the body`s distal extremities for surgical procedures lasting up to 60 minutes. The advantages of IVRA are ease of use, realiability and rapid recovery. The technique is limited by the local anesthetic`s (LA) toxicity, slow onset of action, poor myorelaxation and poor postoperative pain control. This leads to the use of adjuvantes along with the LA (lidocaine and prilocaine). The aim of this paper is to assess the effects of following adjuvantes: α2 agonists (dexmedetomidine, clonidine), NSAIDs (ketorolac with/without dexamethasone), opioid analgetics (sufentanil, tramadol) and nondepolarizing muscle relaxants. Methods: Systematic literature review was conducted. Relevant studies and research were reviewed. Results: Dexmedetomidine has shown to effectively lower the time required to achieve sensorimotor blockage, decrease the need for additional preoperative analgesic treatment, improve tolerability of the tourniquet and cause prolonged postoperative sensorimotor blockage. Clonidine is less used because higher doses can cause sedation and hypotension upon releasing the tourniquet.NSAIDs (ketorolac) show preoperative and early postoperative pain relief. This effect is potentiated by addition of dexamethasone. Although studies remain limited, after its addition there seems to be better preoperative tolerance to tourniquet and a faster onset of sensorimotor blockage, but also longer recovery time. Sufentanil slightly accelerates the onset of analgesic activity; as well as tramadol which additionally increases tolerance to distal hemostasis caused by the tourniquet. Nausea, vomiting, and sedation limit the use of opioid analgesics as adjuvantes. Nondepolarizing muscle relaxants have a mildly beneficial effect on the reduction of muscle block so their use is just theoretical. Conclusions: The use of adjuvantes to LA in IVRA is highly necessary in order to minimize the limiting factors of this technique, especially lowering systemic toxicity of the LA. The most studies claim that α2 agonists (especially dexmedetomidine) are the best adjuvant choice.

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 34
18 P. Approaches and Management in Abdominoplasty surgery with von Willebrand Disease in an Ambulatory Setting JUDITH ADRIANNE DEUTSCH 1, DINKO BAGATIN 1,2,JOHANN NEMRAVA 1,2, KATA ŠAKIĆ 1,2, 3, TOMICA BAGATIN 1,2
1 Department of plastic, reconstructive and aesthetic surgery and Anaesthesiology Bagatin Polyclinic, Zagreb, Croatia; 2Faculty of dental medicine and health Osijek, Josip uraj Strossmayer University in Osijek, Osijek, Croatia 3Catholic University of Croatia, Zagreb, Croatia E-mail:[email protected] Anaesthetists can encounter many various difficult and challenging patients throughout their careers. One such challenge can be encountering diseases of coagulation. These may even be asymptomatic, leading to unexpected increased bleeding intra and post-operatively. Careful management of these patients is important to reduce the risks of haemorrhage and even death. Specific recognition and proper planning management are essential with von Willebrand disease. Doing this can also open the possibilities for these patients to undertake elective operations, something as of now, has been discouraged. Preoperative blood tests can be near normal, masking such patients risks. Good patient history may reveal epistaxis, increased bleeding times with cuts and abrasions, and in females very heavy lengthy menstrual periods. All of these mention do not necessarily mean von Willebrand disease, but high suspicion should be considered. This disease affects 1% of the general population, affecting males and females and there is limited epidemiological knowledge as to area prevalence. There remains the need to develop national registries and create basic screening methods and widely available treatments. Encountering such patients should not cause distress within the operative team, with advanced knowledge and preparation this can make the anaesthesia and surgical process safer and smoother. Tranexamic acid (Cyclokapron, Azeptil) 3 x 1g (every 8 hours, 5-10 days) can be given for minor procedures such as dental, local skin excisions. While for larger procedures tranexamic acid (Cyclokapron, Azeptil) combined with DDAVP - Desmopressin (Minirin) is given 30 minutes before starting operations, such as hysterectomy, rhinoplasty, abdominoplasty. Then tranexamic acid is given every 8 hours during and following surgery for 7-10 days. Consultation with a haematologist is always beneficial and eases organisation of a possible tertiary assistance intervention. Regardless of being challenging cases, these patients can be planned for elective procedures safely, leading to a broader horizon of aesthetic options.

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 35
19 P. Local infiltration analgesia for reduction of postoperative pain following general anaesthesia for mammoplasty in day surgery NEMRAVA J1,2, BAGATIN D1,2, ŠAKIĆ KATA 1,2, 3, BAGATIN T1,2, DEUTSCH J.A1
1Department of plastic, reconstructive and aesthetic surgery Bagatin Polyclinic, Zagreb, Croatia; 2Faculty of dental medicine and health Osijek, Josip uraj Strossmayer University in Osijek, Osijek, Croatia 3Catholic University of Croatia, Zagreb, Croatia E-mail:[email protected] Mammoplasty is a breast reduction surgery procedure which is usually done under general anaesthesia. At the end of the mammoplasty procedure, liposuction of the breast is used to get a better contour and aesthetic result. Before starting the liposuction procedure, a tumescent solution is used to eliminate the risksof bleeding associated with liposuction. Thistumescent solution is comprised of epinephrine, lidocaine, saline and sodium bicarbonate, and it is a standard solution used which has revolutionized liposuction procedures. The associated vasoconstriction has permitted the extensive use of microcannulas and superficial liposuction, thus dramatically improving aesthetic results and reduced bleeding into procedural areas. Within a clinical practice setting, patients after mammoplasty surgery with liposuction have reduced postoperative analgesic consumption and have hasten recovery. Nowadays, many techniques are used in multimodal analgesia invarious surgical subdisciplines, in order to achieve a painless recovery period, better patient comfort and to improve patient outcome. Attention needs to be drawn to clinical experience with infiltrating the breast tissue, with the tumescent solution, at the end of breast reduction surgery. This not only contributes to reduce risk of bleeding, following a liposuction procedure, but also to reduce acute postoperative pain within the early postoperative period. The combination of all mentioned leads to faster recovery and earlier release following mammoplasty. This is the ultimate goal of a surgical procedure, when classifying it asa day surgery procedure.

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 36
20 P. Trends in the administration of local anaesthesia for dental procedures
IVANA SPLIVALO1, 2, , TOMISLAV ŠKLEBAR 3, IVAN ŠKLEBAR1,4, 5, 6
1Catholic University of Croatia, Zagreb, Croatia 2University Psychiatric Hospital Vrapče, Croatia 3University of Zagreb, School of Medicine, Zagreb, Croatia 4Sveti Duh University Hospital, Department of Anaesthesiology, Resuscitation and Intensive Care Medicine, Zagreb, Croatia 5Faculty of Medicine, Josip Juraj Strossmayer University of Osijek, Osijek, Croatia 6Bjelovar University of Applied Sciences, Bjelovar, Croatia E-mail:[email protected]
Background and purpose: Anaesthesia has been used in dentistry from its very beginnings, and is an important aspect of modern dental practice. During painful dental procedures, dentists most frequently administer local anaesthesia, and in rare cases even general anaesthesia. The aim of this research is to identify changes in the trends relative to the administration of local anaesthesia for dental procedures in the past ten years using as an example a typical, non-specialised dental practice. Materials and methods: The research compared the number of procedures performed by the same dental team with the use of local anaesthesia in 2017 and ten years before. The share of procedures under local anaesthesia was compared to the total number of procedures in 2007 and in 2017, with an additional disaggregation of data by age and sex of the patients. The data was analysed with the SPSS statistical package. Results: The results have shown that in 2007 local anaesthesia was administered in 14% of the total 3247 visits, whereas in 2017, out of a total of 2584 visits, local anaesthesia was used in 17% of the cases, which is statistically significant (p<0.05). In male patients, local anaesthesia was administered in 12% of the cases in 2007 and in 17% of the cases in 2017. Local anaesthesia was somewhat more frequently used for female patients, i.e. in 15% of the cases in 2007 and in 18% of the cases in 2017. Conclusion: An upward trend in the use of local anaesthesia in dentistry is evident, and a further increase is expected due to the development of new methods for painless administration of local anaesthetics. Consequently, dentists are required to continuously expand their knowledge on contemporary techniques for the administration of local anaesthesia, indications and contraindications, as well as methods for treatment of possible complications.

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 37
21 P. Performance, tolerance and safety of Spinal Anaesthesia for ureterorenoscopy (URS) and in situ lithotripsy (Review) SANDRA NENADIĆ ŠPRAJC1, ELEONORA GOLUŽA1, IGOR VLATKOVIĆ1, MARJAN MARIĆ2, ŽELJKO KAŠTELAN2, SLOBODAN MIHALJEVIĆ1 1. Department of Anaesthesia, University Hospital Centre Zagreb, Zagreb, Croatia 2. Department of Urology, University Hospital Centre Zagreb, Zagreb, Croatia [email protected] Background and purpose: Spinal Anaesthesia has been widely used for urological operations. We aimed to research performance, tolerance and safety of spinal anaesthesia for ureterorenoscopy (URS) and in situ lithotripsy. Materials and methods: The authors searched Medline, Cochrane Database of Systematic Review and Cochrane Central Register of Controlled Trials databases for randomized Controlled Trials database. Results: Since its introduction in 1980 ureterorenoscopy (URS) and in situ lithotripsy have been routine urological procedures. In modern urology, it has become a successful technique in treatment of ureteral stones. Ureteroscopy is a minimally invasive method to treat kidney stones as well as stones located in the ureter. Lithotomy position is the most common in this procedure. Spinal and General Anaesthesia have been used for URS and in situ lithotripsy. If Spinal Anaesthesia is used, a T6 level is required for upper tract instrumentation, whereas a T10 level is adequate for lower track surgery. The change in posture immediately after the injections helps in achieving the adequate level of anaesthesia. The natural curve of spinal cord not only helps us determine the approximate level of block achieved, but also serves as a protection against the respiratory distress that might occur due to higher up spread of the drug. Several studies have been previously done to study the effect of patient positioning on spinal anaesthesia using hyperbaric local anaesthetic. The advantages of spinal anaesthesia include the ability to perform surgery on awake patient with decreased post operative somnolence and less risk of pulmonary aspiration, reduced incidence of coagulation disorders following surgery and less bleeding. Spinal anaesthesia has been associated with minimal postoperative pain, decreased hospital stay and minimal post operativecomplication. Conclusions: Spinal anaesthesia is efficient, well tolerated and safe for ureterorenoscopy (URS) and in situ lithotripsy procedure. It is acceptable for outpatient surgery.

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 38
22 P Scalp block as safe method for emergency operation in paediatric neurosurgery
LUK A VRDOLJAK1 ,MAŠA DELIĆ2, ŽELJKA ZADRO2, BARBARA BORAS2, MARKO BOŠNJAK2, IVANA BULIĆ2, MARIJA BOŠNJAK2, JOSIP PALADINO3, VASILIJE STAMBOLIJA2 1SKB MOSTAR, BIJELI BRIJEG BB, 88000 MOSTAR, BIH 2Department of Anaesthesia, University Hospital Centre Zagreb, Zagreb, Croatia 3Department of neurosurgery, University Hospital Centre Zagreb, Zagreb, Croatia e-mail: [email protected]
Background andpurpose. We present our experience with regional technique such as scalp block for emergency paediatric neurosurgery. Previously we didn’t preform any regional technique for cranial surgery, and relay only on opioids for pain control during surgery. We implemented this regional technique for neurosurgery and in our experience it has showed as superior and safe approach; rather than only usage of opioids and anaesthesia depth. Purpose of our study is presentation of scalp block in children as safe method in emergency neurosurgery operations. Materials(Patients) and methods We present on four year old female child with urgent posterior fossa tumour and one 33 days old male – newborn with severe intracranial haemorrhage due to late vitamin K deficiency bleeding. Both of patients were presented with low GCS ˂6, hemodynamic instability and with epileptic seizures. After initial treatment and arriving in operating room we administrated scalp block with levobupivacaine. We used dose of 2 mg per kg of body weight. The local anaesthetic was administrated thru plastic 20 mL syringe and we used 23 G baby set for percutaneous application of local anaesthetic. Results. In our case we didn’t experience any local or systemic complication due the local aesthetic application. Scalp block in our paediatric emergency neurosurgery provided safe method for pain control during the first phase of neurosurgery. Conclusions Scalp block demonstrated as safe and superior method combined with TIVA in paediatric emergency neurosurgery. Previous experience showed grater hemodynamic oscillations and unpredicted usage of opioids in the early phase of craniotomy especially when the head was pinned on a frame. Also previous technique which combined usage of bolus opioids and deepening of anaesthesia showed prolonged duration of hemodynamic instability. With the usage of scalp block we demonstrated hemodynamic stability in early phase of neurosurgery. During the performance of scalp block we advise caution when inserting needle and applying pressure because of soft bones, so that we don’t puncture bone and cause damage to bone itself or worse to the brain. We will continue to use scalp block in children’s neurosurgery as superior method for pain control during critical stages of neurosurgery.

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 39
23. P Bilateral intermediate cervical block with general anesthesia for right sided thyroid lobectomy, a case report DANIJEL KNEŽEVIĆ1, EMANUEL BOROVIĆ1, BERISLAV BARBALIĆ1 1 Clinical Hospital Centre Rijeka, Department for Anesthesiology and Intensive care, Rijeka, Croatia Email: [email protected] Background and purpose: As in any type of surgery postoperative pain management is very important for early mobilization and recovery. The incision site for classic thyroid surgery is located in a very mobile area which can effect postoperative pain. In addition, swelling is one of the major complications of thyroid surgery due to potential airway compromise, there are studies associated with the effect of local anesthetics on reduction of swelling and edema. Opioids are the main analgesic treatment during surgery but they are associated with postoperative nausea and vomiting, so if possible we try to apply opioid sparing techniques during- and post surgery. Patients and methods: A 39 year old female patient with no significant comorbidities was scheduled for an elective right sided thyroid lobectomy due to a potential malignant node. She was classified as ASA (American Society of Anesthesiologists) class 1 with a MET >4. Prior to induction of general anesthesia bilateral intermediate cervical block was applied under ultrasound guidance with a 25G needle, with 20ml 0.25% Levobupivacainebeing injected to each side. There were no neurological deficits post injection, no hoarseness, dyspnea or problems swallowing. Approximately half and hour post injection general anesthesia was induced with a combination of Sufentanyl, Propofol and Rocuronium. Maintance of anesthesia was done with Sevoflurane and Sufentanyl. Results: There were no perioperative complications, the total dose of Sufentanyl given was 40 mcg for the duration of approximately 2,5 hours. After the procedure she was transferred to the postoperative recovery room (PRR) where she spent 1 hour. During the time in the PRR she had no complaints of pain, hoarseness, dyspnea, just some mild discomfort/pain while swallowing. Six hours post surgery, her only complaint was moderate pain while swallowing, the incision site was numb and no local pain was present, she declined additional pain medication at the time. 20 hours postoperatively she was given 1g Paracetamol due to increasing pain. Conclusions: BICB is a feasible option for postoperative pain management. It should be used with caution in patients with potential respiratory complications.

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 40
24. P. Effect of superficial cervical block on early postoperative recovery and reduction of analgesia in patients following anterior approach cervical spine surgery
JOSIP KOVAČEVIĆ1, VASILIJE STAMBOLIJA
1, MIROSLAV VUKIĆ
2, MARIN LOZIĆ
1, IVAN DOMAZET
1,
MARTINA MIKLIĆ BUBLIĆ1, LUKA VRDOLJAK
1, DUJE ŠTAMBUK
1
1Department of Anaesthesiology and Intensive medicine , University Hospital Centre Zagreb, Zagreb, Croatia 2Department of neurosurgery, University Hospital Centre Zagreb, Zagreb, Croatia
BACKGROUND: The cervical plexus block provides adequate anesthesia and analgesia for surgery in the region of
the head and neck. The aim of our study was to demonstrate the effect of the superficial cervical block (engl.SCPB)
in cervical spine surgery with anterior approach for reduced use of NSAIDs and synthetic opioids in Group of
patient that received SCPB compared with No block group in the first 24 hours after surgery and during the stay.
METHODS: The study was conducted at the Neurosurgery Department at KBC Zagreb. The study included elective
cervical spine surgerys where SCPB was used in addition to general anesthesia and those who did not receive SCPB.
Data was obtained retrospectively from disease history, therapeutic lists and patient satisfaction index score
(abr.PSI) and VAS score that were estimated at the
first 24 hours after surgery and during the stay until release.
RESULTS: The study included patients scheduled for elective cervical spine surgery with anterior approach. There
were one hundred and thirty-six patients randomly assigned in two groups. In the Group A eighty-five patients with
SCPB showed a significantly better score on the PSI and VAS scale in the first 24 hours postoperatively compared
with No block group. There was also a considerable decrease in use of NSAID's and synthetic opioids in the first 24
hours in Block group compared to No block. CONCLUSION: Pain and discomfort after the cervical spine surgery is described as a moderate to severe pain. In regard to operating arrea patients are more prone to postoperative complications and postoperative nausea and vomiting (abbr.PONV). Since opioid analgesics are not always effective in pain control and may further exacerbate postoperative nausea and vomiting with subsequent slower postoperative recovery, the use of multimodal analgesia with peripheral blocks should be part of a standard procedure for threating patients scheduled for cervical spine surgery. We have shown that SCPB is an excellent method in pain control for early recovery after surgery. Our study showed considerable increase in quality of postoperative recovery with significantly reduced use of analgesics in the first 24 hours.

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 41
Oral presentation 01. OP. DEXAMETHASONE - INTRATHECAL MINIMISER OF SIMPLE HAEMATHOLOGIC STRESS BIOMARKERS IN HIP FRACTURE LIVIJA ŠAKIĆ1, DINKO TONKOVIĆ2, and KATA ŠAKIĆ3 1Department of Anaesthesiology, Reanimatology and Intensive Medicine, University Hospital “Sveti Duh”, Zagreb, Croatia; 2Department of Anaesthesiology, Reanimatology and Intensive Th erapy, University Hospital Centre Zagreb “Rebro”, School of Medicine, University of Zagreb, Zagreb, Croatia; 3Department of Anaesthesiology and Pain Th erapy at Maxillofacial, General and Plastic surgery Polyclinic “Bagatin”, Zagreb, Croatia Proximal femoral fractures are the most common cause of emergency admission to hospital with high postoperative morbidity. The hypothesis was that a single shot of intrathecal dexamethasone and levobupivacaine in anaesthesia for surgical correction of proximal femoral fracture in elderly patients reduces surgical stress with better quality hospitalisation. The study included sixty elderly patients with proximal femoral fracture, ASA status 2 and 3, randomised into two groups. Th e study group of thirty patients received 8 mg of dexamethasone and 12,5 mg of levobupivacaine 0,5 % intrathecally, DLSA group, and the parallel group of thirty patients received 12, 5 mg of levobupivacaine 0,5% intrathecally, LSA group. Plasma cortisol and glucose concentrations were assessed before and after anaesthesia, pain intensity was evaluated using Visual Analogue Scale score and hospitalisation was analysed. Results showed decreased cortisol concentrations, longer analgesia duration and shorter hospitalisation in the DLSA group. Glucose concentrations did not diff er signifi cantly between the patients in either group. Enlightening the study results collected, single shot of intrathecal administration of dexamethasone in spinal anaesthesia for surgical treatment of proximal femoral fractures reduces the stress response by decreasing plasma cortisol concentrations prolonging analgesia with better rehabilitation possibilities, hence shortening hospitalisation which explains this pattern of anaesthesia.

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 42
02. OP. COMPARISON OF PLEXUS BRACHIAL BLOCKADE EFFECT BY SUPRACLAVICULAR AND AXILLARY APPROACH - OUR EXPERIENCE ISMET SULJEVIĆ1, OMERSULJEVIĆ 2, MAIDA TURAN3, AMELAGRBO 1 and ISMANA ŠURKOVIĆ4 1University Clinical center Sarajevo, Clinic for anesthesiology and resuscitation, Bosnia and Herzegovina; 2Medical Faculty of Univesity in Sarajevo, Bosnia i Herzegovina, Bosnia and Herzegovina; 3Achibadem Office in Sarajevo, Bosnia and Herzegovina; 4University Clinical center Sarajevo, Department for Endocrinology, diabetes and metabolic diseases Introduction: Brachialis plexus block is a frequently used method of regional anesthesia that can be performed in several ways and locations. It has been successfully performed to provide good anesthesia and analgesia lasting several hours for operative procedures onhands. It can be performed by paresthesia technique or by ultrasound that has almost pushed out the old conventional technique since it allowsthe visualization of the blockade performance. Target. In the paper we use our sample to try to determinewhichof the two locations of the blockageis more favorable for the patient, and whichone gives a higher percentage of success or a better sensory blockade. Method: This is a retrospective study and includes 40 patients of both sexes that were operated on at the Clinic for Traumatology and the Clinic for Plastic Surgery of the University Clinical Center in Sarajevo in the period 30 August 1993 to 30 August 1994. Patients are divided into two groups. Group I are patients who had an axillary approach to plexus brachialis (n-21) ASA I-II. Group II were patients who had supraclavicular access to plexus brachialis (n-19) ASA I-II. All patients received 0.5 ml / kg Bupivacaine 0.5%. In the study, we analyzed sex, age, duration of blockade and complications. Analgesia and motor block were evaluated 20 minutes after the local anesthetic injection. The complete block is defined as analgesia in all dermatomes (C5-Th 1) 20 minutes after injection. Results: Group I had 20 male and 1 female patients while group II had 17 male and 2 female patients. The supraclavicular block enabled complete blockade in 18 patients (95.23%), and the axillary approach had a successful blockade in 17 patients (80.95%). In both groups the corresponding motor block was similar. The start of the engine block was similar in both groups. There were no signifi cant complications in either group. Conclusion: Regarding clinical efficacy, both brachial plexus blocking approaches provided a good motor block, anesthesia and analgesia for the forearm or hand surgery. Supraclavicular approach proved to be more favorable.

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 43
03. OP.INFLUENCE OF LOCAL INFILTRATION ANALGESIA ON POSTOPERATIVE PAIN IN ABDOMINOPLASTY PATIENTS DINKO BAGATIN1,4, TOMICA BAGATIN2,4, JOHANN NEMRAVA1,4, KATA ŠAKIĆ3,4
1Department of General and Plastic Surgery at Maxillofacial, General and Plastic Surgery Polyclinic “Bagatin”, Zagreb, Croatia; 2Department of Maxillofacial Surgery at Maxillofacial, General and Plastic Surgery Polyclinic “Bagatin”, Zagreb, Croatia; 3Department of Anaesthesiology and Pain Therapy at Maxillofacial, General and Plastic Surgery Polyclinic “Bagatin”, Zagreb, Croatia; 4Faculty of Dental Medicine and Health Osijek, Josip Juraj Strossmayer University of Osijek, Osijek, Croatia The aim of this study was the infl uence of local infi ltrating analgesia with levobupivacaine on acute postoperative pain in patients that underwent abdominoplasty in day surgery. Local infiltration anesthesia is an injection of local anesthetic solution in painful areas. General anesthesia and tumescent fl uid solution were performed in all patients. The study included 55 patients within age range from 20 to 72 years old. Study was conducted from January 2016 to February 2019.Postoperative pain after abdominoplasty was evaluated. LIA were performed before closure of abdominal wall after resection of skin and subcutaneous fat in lower part of abdominal wall. Infiltration was performed after plication of rectus abdominis muscles with single shot of 40 ml 0.25 % Bupivacaine. Postoperative pain was reduced in the abdominal wall and in the wound area around umbilicus and in lower abdomen scar after waking from general anesthesia. Occurrence of acute postoperative was noticed in all participants. 85% of patients required an additional dose of analgesics and only in 3% of patients was required during the fi rst postoperative day discharged during 48 hours. The research has shown that the appearance of acute postoperative pain did not lead to prolonged stay in the facility for day surgery.

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 44
04. OP. HOLISTIC APPROACH TO THE IMMUNOBIOLOGY OF AGING (VIEW ON THE TURN OF MILLENIUM) BRANKO VITALE Academy of Medical Sciences of Croatia, Zagreb, Croatia Among many functions of the body affected by the complex process of aging,the immune system, primarily due to declining of thymic function, the ancient and conserved evolutionary process, undergoes complex remodelling in the second part of life, with recapitulation of inversely evolutionary pattern of the immune system. In approaching the complex analysis of age-associated derangement of the immune system homeostasis and its clinical consequences, classical monoclonal lymphoproliferative syndrome (CLL) accompanied by a myriad of cellular and humoral defects, has been selected as appropriate and useful model for studies of impact T-cell and B-cell defects on appearance, evolution of clinical manifestations and outcome of CLL syndrome. Therefore imbalance in cascade secretion of a number of Th-1 (pro-inflammatory cytokines)and/or Th-2(anti-inflammatory cytokines) in CLL patients with their pleiotropy,redundancy,synergistic and antagonistic activity and parallelism can cause variety of clinical manifestations as reccurent infections, systemic inflammation/sepsis, immunodeficiency, autoimmune disorders, indolent anti-self malignancy, and other secondary tumours.

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 45
05. OP. THE ANATOMY OF OROFACIAL INNERVATION IVANA BICANIC, ANA HLADNIK, DOMAGOJ DZAJA, ZDRAVKO PETANJEK University of Zagreb, School of Medicine, Department of Anatomy and Clinical Anatomy, Zagreb, Croatia The whole human body receives rich sensory innervation with only one exception and that is the brain tissue. The orofacial region is hence no exception. Th e head region consequently receives a rich network of sensory nerves making it special because the two types of sensory fi bres, visceral and somatic overlap, especially in the pharynx. Also, diff erent pain syndromes that affect this region are rather specifi c in comparison to their presentation in other body regions. With this review article we wanted to show the detailed anatomy of the peripheral sensory pathways, because of its importance in everyday body functions (eating, drinking, speech) as well as the importance it has in pathological conditions (pain syndromes), in diagnostics and regional analgesia and anaesthesia.

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 46
06. OP. THE ROLE OF PARAVERTEBRAL BLOCKS IN AMBULATORY SURGERY: REVIEW OF THE LITERATURE
MIROSLAV ZUPCIC1,2,3, DAVID DEDIC4, SANDRA GRAF ZUPCIC2,5, VIKTOR DUZEL6, TATJANA SIMURINA3,7,8, LIVIJA SAKIC9, IGOR GRUBJESIC1, INGRID SUTIC2 ,IVANA SUTIC10 AND ANDJELKO KORUSIC3,4
1Clinical Hospital Centre Rijeka, Clinic of Anesthesiology and Intensive Care Medicine, Rijeka, Croatia; 2 University of Rijeka, Faculty of Medicine, Department of Physiology and Immunology,Rijeka, Croatia; 3J. J. Strossmayer University, Faculty of Medicine, Osijek, Croatia; 4Clinical Hospital Dubrava, Clinic of Anesthesiology, Reanimatology and Intensive Care Medicine, Zagreb, Croatia; 5Clinical Hospital Centre Rijeka, Clinic of Neurology, Rijeka, Croatia; 6Barking, Havering and Redbridge University Hospitals NHS Trust, Department of Anaesthesia, London, United Kingdom; 7General Hospital Zadar, Department of Anesthesiology and Intensive Care Medicine, Zadar, Croatia; 8Department of Health Studies University of Zadar, Zadar,Croatia; 9University Hospital “Sveti Duh“,Clinic of Anesthesiology, Reanimatology and Intensive Care Medicine, Zagreb, Croatia; 10 University of Rijeka, Faculty of Medicine, Department of Family medicine,Rijeka,Croatia E-mail: [email protected]
Ambulatory surgery often involves surgical procedures on the thorax, abdomen and limbs, which can be associated with substantial postoperative pain. The aim of this narrative review is to provide an analysis of the effectiveness of paravertebral block (PVB) alone or in combination with general anaesthesia, in this setting, with an emphasis on satisfactory postoperative analgesia in comparison to other modalities. We have conducted a search of current medical literature written in English through PubMed, Google Scholar and Ovid Medline®. Peer-reviewed professional articles, review articles, retrospective and prospective studies, case reports and case series were systematically searched for during the time period between November 2003 until February 2019. The literature used for the purpose of creating this review showed that utilisation of paravertebral block either alone or in combination with general anaesthesia, has a positive effect on satisfactory analgesia in ambulatory surgery. With a multimodal analgesic approach of PVB and other techniques of anaesthesia and analgesia there is a reduction in postoperative opioid consumption, fewer side effects, lower pain scores, decreased mortality, earlier mobilisation of patients and reduced hospital stay.

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 47
07. OP. REGIONAL ANESTHESIA FOR NEUROSURGERY DINKO TONKOVIĆ1,2, DANIELA BANDIĆ PAVLOVIĆ1,2, ROBERT BARONICA2, IGOR VIRAG2, MARTINA MIKLIĆ BUBLIĆ2, NATAŠA KOVAČ2, DRVAR ŽELJKO2
1School of Medicine, University of Zagreb; 2University Hospital Zagreb, Department of Anesthesiology, Reanimatology and Intensive care During neurosurgery procedures it is vital to assure optimal cerebral perfusion and oxygenation. Despite physiological autoregulation of brain perfusion, maintaining hemodynamic stability and good oxygenation during anesthesia is vital for success. General anesthesia with mechanical ventilation and current drugs provide excellent hemodynamic condition and it is the fi rst choice for most neurosurgery procedures. However, sometimes it is very hard to avoid brief increase or decrease in blood pressure especially during period of intense pain, or without pain stimulation. This could be detrimental for patients presented with high intracranial pressure and brain edema. Modifying anesthesia depth or treatment with vasoactive drugs usually is needed to overcome such circumstances. On the other hand it is important to wake the patients quickly after anesthesia for neurological exam. Th at is why regional anesthesia of scalp and spine could show benefi cial eff ects by decreasing pain stimuli and hemodynamic variability with sparing eff ect of anesthetics drugs. Also regional techniques provide excellent postoperative pain relief, especially after spinal surgery.

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 48
08. OP. LOCAL ANESTHETICS AND STEROIDS: CONTRAINDICATIONS AND COMPLICATIONS. AN OVERVIEW OF CURRENT CLINICAL ISSUES TATJANA ŠIMURINA1,2,3, BORIS MRAOVIĆ4, ŽUPČIĆ5,6, SANDRA GRAF ŽUPČIĆ5,7, MARINA VULIN3
1Department of Anesthesiology, Resustitation, Intensive Medicine and Pain Management, Faculty of Medicine, “Josip JurajStrossmayer” University, Osijek, Croatia; 2Department of Health Studies, University of Zadar, Zadar, Croatia; 3Department of Anesthesiology, Reanimatology and Intensive Care Medicine, Zadar General Hospital, Zadar, Croatia; 4Department of Anesthesiology and Perioperative Medicine, School of Medicine, University of Missouri, Columbia, USA; 5School of Medicine, University of Rijeka, Rijeka, Croatia; 6Clinic of Anesthesiology and Intensive Care Medicine, Clinical Hospital Centre Rijeka, Rijeka, Croatia; 7Clinic of Neurology, Clinical Hospital Centre Rijeka, Rijeka, Croatia The objective of this clinical update, based on recentlypublished literature, was to discuss incidence and characteristics of the most relevant clinical adverse eff ects associated with local anesthetic and steroid use in regional anesthesia and treatment of acute or chronic pain. A comprehensive review of the English-language medical literature search utilizing PubMed, Ovid MedlineR and Google Scholar from 2015 to 2018 wasperformed. This narrative review provides anesthesia practitioners with updated evidences on complicationsand contraindications of local anesthetic and steroid use with emphasis oncurrent points of view regardingprevention, early diagnosis and treatment ofadverse events.

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 49
09. OP. IMPACT OF LOCAL INFILTRATION ANESTHESIA ON POSTOPERATIVE PAIN MANAGEMENT AFTER RHINOPLASTYIN DAY CARE SURGERY TOMICA BAGATIN1,5, DINKO BAGATIN2,5, LIVIJA ŠAKIĆ3 AND KATA ŠAKIĆ4,5
1Department of Maxillofacial Surgery at Maxillofacial, General and Plastic Surgery Polyclinic “Bagatin”, Zagreb, Croatia; 2Department of General and Plastic Surgery at Maxillofacial, General and Plastic Surgery Polyclinic “Bagatin”, Zagreb, Croatia; 3Department of Anaesthesiology, Reanimatology and Intensive Medicine, University Hospital “Sveti Duh”, Zagreb, Croatia; 4Department of Anaesthesiology and Pain Th erapy at Maxillofacial, General and Plastic Surgery Polyclinic “Bagatin”, Zagreb, Croatia; 5Faculty of dental medicine and Health Osijek, Josip Juraj Strossmayer University in Osijek, Croatia Use of local infi ltration anaesthesia with 2% lidocaine in combination with epinephrine 1/100000 in rhinoplasty and 0.25% levobupivacaine in this research as an adjunct to general anaesthesia is compared analysing the need for postoperative analgesia in rhinoplasty patients. 30 patients received lidocaine combined with epinephrine (LA) and other 30 patients received levobupivacaine (LB). Comparison is done with Visual Analogue Scale in 30 min and 1, 3, 6 h postoperatively. Also 24 h need for analgesic treatment was recorded. In conclusion postoperative analgesia in LB group with general anaesthesia was signifi cantly prolonged (P = 0.038).

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 50
10. OP. COMPARISONS OF LOCAL INFILTRATION ANALGESIA EFFECTS IN DIFFERENT SURGICAL PROCEDURES IN DAY SURGERY KATA ŠAKIĆ1,4, DINKO BAGATIN2,4, TOMICA BAGATIN3,4, LIVIJA ŠAKIĆ5 MARTINA ŠAREC IVELJ2, SLOBODAN MIHALJEVIĆ7 AND ALEKSANDAR VČEV4,6
1Department of Anaesthesiology and Pain Th erapy at Maxillofacial, General and Plastic Surgery Polyclinic “Bagatin”, Zagreb, Croatia; 2Department of General and Plastic Surgery at Maxillofacial, General and Plastic Surgery Polyclinic “Bagatin”, Zagreb, Croatia; 3Department of Maxillofacial Surgery at Maxillofacial, General and Plastic Surgery Polyclinic “Bagatin”, Zagreb, Croatia; 4Faculty of Dental Medicine and Health Osijek, Josip Juraj Strossmayer University of Osijek, Osijek, Croatia; 5Department of Anaesthesiology, Reanimatology and Intensive Medicine, University Hospital “Sveti Duh”, Zagreb, Croatia; 6Department of Internal medicine, University Hospital Centre Osijek, Osijek, Croatia 7Department of Anaesthesiology, Reanimatology and Intensive Medicine, Clinical Hospital Center Zagreb, Zagreb, Croatia Purpose of this study was assessing of local infi ltration analgesia (LIA) with levobupivacaine on the trend of acute postoperative pain and outcome in individuals who underwent rhinoplasty procedure and abdominoplasty performed in general anaesthesia. Th e research was conducted on 60 patients, of which 30 patients underwent rhinoplasty procedure and the other 30 patients underwent abdominoplasty procedure in general anaesthesia with LIA in “Bagatin” Polyclinic in the time period between 01.01.2014. and 01.01.2017. Postoperative analgesics doses on the same day of surgery were noted in 85% of participants who underwent an abdominoplasty procedure and in 45% of participants underwent rhinoplasty procedure. Patients who underwent abdominoplasty were discharged from the facility within 48 hours, while all patients who underwent rhinoplasty procedure were discharged on the same day of the surgery. During the fi rst postoperative day patients who underwent a rhinoplasty procedure did not require analgesics, while only 3% of patients who underwent an abdominal liposuction procedure required an additional dose of analgesics. Th e research results had shown, when LIA was performed, the manifestation of acute postoperative pain and vomiting did not lead to prolonged stay in day surgery.

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 51
11. OP. ULTRASOUND SKILLS IN LOWER EXTREMITY TRAUMATOLOGY AND ORTHOPEDICS – REGIONAL ANESTHESIA AND BEYOND KREŠIMIR OREMUŠ AKROMION Special Hospital for Orthopedic Surgery, Krapinske Toplice During the last two decades ultrasound guidance has been established as an invaluable tool for performing peripheral nerve blocks. Ultrasound guidance reduces block performance time, volume of local anesthetic, risk of intravascular injection and need for opioid rescue analgesia compared to landmark based and neurostimulator guided techniques. Th e use of ultrasound guidance must not be understood as a surrogate to, but should complement a thorough understanding of anatomy. Th e purpose of this overview is to present ultrasound guided techniques for performing basic lower extremity blocks, as well as to discuss more recent trends in providing regional analgesia for patients undergoing lower extremity surgery.

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 52
12. OP. OROFACIAL PAIN – DIAGNOSTIC AND THERAPEUTIC CHALLENGES TOMISLAV BADEL1, DIJANA ZADRAVEC2, VANJA BAŠIĆ KES3, MIA SMOLJAN2, SANDRA KOCIJAN LOVKO4, IRIS ZAVOREO3, LADISLAV KRAPAC5, SANDRA ANIĆ MILOŠEVIĆ6 1Department of Removable Prosthodontics, School of Dental Medicine, University of Zagreb, Zagreb, Croatia; 2Department of Diagnostic and Interventional Radiology, Sestre milosrdnice University Hospital Center, University of Zagreb, Zagreb, Croatia; 3Department of Neurology, Sestre milosrdnice University Hospital Center, University of Zagreb, Zagreb, Croatia; 4Psychiatry Hospital “Sv Ivan”, Zagreb, Croatia; 5Academy of Medical Sciences of Croatia, Department of Public Health, Zagreb, Croatia; 6Department of Orthodontics, School of Dental Medicine, University of Zagreb, Zagreb, Croatia The concept of diagnostics and therapy of musculoskeletal and neuropathic diseases of the stomatognathic system, which are the subject of this paper, has been developing for decades. It can be said that in order to avoid misunderstanding, the orofacial pain as a clinical problem, in the narrower sense, involves non-odontogenic and non-malignant causes of orofacial region. In this study, the results of clinical diagnosis of the population of 557 consecutive patients with orofacial pain based on multidisciplinary diagnostics were evaluated. 15.6% of patients have given up on the participation in the study. It has been shown that the patients who dropped out of the study were significantly older (p=0.0411) than those who agreed to participate, but there was no difference in gender ratio (p=0.185) since the proportion of female patients prevailed. In an analysis of 84.4% of patients participating in the study, the elevated anxiety values were established (mean value on STAI 1 was 39.2 and STAI 2 was 41.1) and statistical signifi cance was found in correlation between elevated anxiety and intensity of pain as shown on visual analogue scale on open mouth (p<0.0001). Compared to the age, the statistical signifi cance was for STAI 1 (p=0.0097) but not for STAI 2 (p=0.5599). Th e most common form of therapy is Michigan stabilization splint: for disc displacement of temporomandibular joint (TMJ) in 38.9% of patients and in combination with physiotherapy in 18.7% of patients; for osteoarthritis of TMJ in 28.4% and in combination with physiotherapy in 26.4% of patients. Th e treatment with anticonvulsant drugs for trigeminal neuralgia predominates in 54.3% of patients, which is combined with acupuncture in 25.7% of patients and only acupuncture in 17.1% of patients. In this study, a multidisciplinary co-operation in initial diagnostics and diff erential was designed to develop subspecialist knowledge on orofacial pain.

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 53
13. OP. SPINAL ANAESTHESIA-INDUCED HYPOTENSION IN OBSTETRICS: PREVENTION AND THERAPY IVAN ŠKLEBAR1,2,3,4, TONKA BUJAS5 AND DUBRAVKO HABEK2,6
1Clinic for Anaesthesiology, Reanimatology and Intensive Care, “Sveti Duh” University Hospital Zagreb, Zagreb, Croatia; 2Catholic University of Croatia; 3Osijek Faculty of Medicine, Osijek, Croatia; 4Bjelovar University of Applied Sciences, Bjelovar, Croatia; 5Dr. Josip Benčević General Hospital, Department of Anaesthesiology, Reanimatology and Intensive Care, Slavonski Brod, Croatia; 6Sveti Duh University Hospital, Clinic for Gynaecology and Obstetrics, Zagreb, Croatia Regional centro-axial anaesthesia, primarily spinal block, is the preferred method of anaesthesia for elective caesarean section because it entails fewer risks for the mother and the foetus compared to general anaesthesia. Th e most common side effect associated with spinal block is hypotension due to sympatholysis, occurring in up to 75% of cases. Spinal block-induced sympatholysis leads to vasodilatation and consequently causes maternal hypotension, which may compromise uterine blood fl ow and foetal circulation, and thus cause foetal hypoxia, bradycardia and acidosis. Th e selection of the most effi cient treatment strategy to achieve haemodynamic stability during spinal anaesthesia for caesarean section continues to be one of the main challenges in obstetric anaesthesiology. A number of measures for the prevention and treatment of spinal block-induced hypotension are used in clinical practice, such as preloading and coloading with crystalloid and/or colloid infusion, wrapping of lower limbs with compression stockings or bandages, administering an optimal dose of local anaesthetic and achieving an optimal spinal block level, left tilt positioning, and administering inotropes and vasopressors. Instead of administering vasopressors after a drop in blood pressure has already occurred, the latest algorithms recommend a prophylactic administration of vasopressor infusion. The preferred vasoconstrictor in this case is phenylephrine, which is associated with a lower incidence of foetal acidosis, and maternal nausea and vomiting compared to other vasoconstrictors.

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 54
14. OP. REGIONAL ANAESTHESIA IN THORACIC AND ABDOMINAL SURGERY VESNA NOVAK-JANKOVIC, JASMINA MARKOVIC-BOZIC Clinical department of Anaesthesiology and Intensive Th erapy, University Medical Centre Ljubljana, Ljubljana, Slovenia Surgical procedure causes tissue damage which activates systemic infl ammation response andleads to changes in endocrine and metabolic system. Anaesthesia and pain can further disrupt immune performance. Regional anaesthesia causes aff erent nerve blockade and in this way mediates immune protection. Th oracic epidural analgesia (TEA) is the cornerstone of pain relief in thoracic and abdominal surgery. Alternatively thoracic paravertebral block (TPB) can be used with less side eff ects and good analgesic properties. Drugs that interfere with blood coagulation obstruct the use of central regional blocks. Surgery has also changed recently from open to minimally invasive. Also pain treatment for this procedures has changed to less aggressive, systemic or locoregional techniques. It was shown that transversus abdominis plane block (TAP) and epidural analgesia have the same effect on postoperative pain, but TAP block was better regarding hemodynamic stability and hospital stay. Multimodal approach combining regional and systemic analgesia is currently the most appropriate perioperative pain management strategy. More studies should be done to give recommendations.
7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 55
15. OP. REGIONAL ANALGESIA MODALITIES IN ABDOMINAL AND LOWER LIMB SURGERY – COMPARISON OF EFFICACY JASMINKA PERŠEC1,2, MONIKA ŠERIĆ1
1Clinic for Anesthesiology, Reanimatology and Intensive Care Medicine, Clinical Hospital Dubrava; 2School of Dental Medicine, University of Zagreb, Croatia A significant component of all surgical procedures and postoperative treatment is pain management.Due to the physiological and psychological advantages of pain relief, it is one of the foremost indicators of quality of care. Today, there are various modalities of pain reduction, aimed to reduce patient discomfort andminimize side eff ects, which can be divided by therapeutic agents used (opioid or non-opioid), route of administration (intravenous, regional, oral, etc.) and modality (controlled by patients or “as needed”). Although opioids have proven to be very effective pain relief agents and are commonly used in postoperative analgesia, concerns about their side eff ects have spurred the development of modified, multimodal treatments that seek to minimize opioid use and associated drawbacks. Enhanced recovery protocols that emphasize sparing administration of opioids are growing in importance, andresulting in reduced length of hospital stay after abdominal and lower limb surgery. To further improve such protocols and optimize postoperative care for individual patient needs, it is imperative to fully assess the effi cacy of available drugs andanalgesia modalities.

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 56
16. OP. INERVATION OF THE HIP JOINT AND APPLICATIONS OF FASCIA ILIACA BLOCK, CRITICAL EVALUATION OF QUADRATES LUMBORUM BLOCK IVAN BOHAČEK Department of Orthopaedic Surgery, University Hospital Centre Zagreb, School of Medicine, University of Zagreb, Zagreb, Croatia [email protected] Anterior section of the hip joint capsule is innervated by femoral nerve and obturatornerve, and posterior section is innervated by the nerve to quadratus femoris muscle and occasionallyby the superior gluteal (posterolateral region) and sciatic nerve (posterosuperior region). Oneof the regional anesthesia options for hip surgery is the fascia iliaca compartment block (FICB) thataff ects nerves important for hip innervation and sensory innervation of the thigh - femoral, obturatorand lateral femoral cutaneous nerve. FICB can be easily performed and is often a good solution formanagement of hip fractures in emergency departments. Its' use reduces morphine pre-operative requirementfor patients with femoral neck fractures and can also be indicated for hip arthroplasty, hiparthroscopy and burn management of the region. Quadratus lumborum block (QLB) is a block of theposterior abdominal wall performed exclusively under ultrasound guidance, with still unclarifiedmechanism of action. When considering hip surgery and postoperative management, the anteriorQLB has shown to reduce lengthy hospital stay and opioid use, it improves perioperative analgesia inpatients undergoing hip and proximal femoral surgery compared to standard intravenous analgesiaregimen, provides early and rapid pain relief and allows early ambulation, thus preventing deep veinthrombosis and thromboembolic complications etc. However, some nerve branches responsible forinnervation of the hip joint are not affected by QLB, which has to be taken into consideration. QLB has shown potential for use in hip surgery and perioperative pain management, but still needs to bevalidated as a reliable treatment approach.

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 57
17. OP. Medico-legal responsibility in management of acute and chronic pain in obstetrics DUBRAVKO HABEK1,3, IVAN ŠKLEBAR2,3
1Clinical Departement of Obstetrics and Gynecology Clinical Hospital „Sveti Duh“ Zagreb, Croatia; 2Anestesiology, Reanimaology and Intensive Medicine** Clinical Hospital „Sveti Duh“ Zagreb, Croatia; 3Croatian Catholic University Zagreb, Croatia Medico-legal responsibility in the management of acute or chronic pain in broad sense implies acting by the rules of good clinical practice and reducing the potential treatment side effects and complications that may entail health impairment and possible legal proceedings. Patients with acute or chronic obstetric or nonobstetric pain should be informed on the mode and method of treatment, possible side eff ects, and eff ects of drugs or procedures on fetal growth and development (informed consent). The principles of perinatal pharmacology and toxicology should be respected, choosing the mode of treatment associated with the lowest rate of side eff ects and a minimally invasive procedure (Accordingly, medico-legal responsibility is a professional and deontological category that should be fostered and implemented in line with professional guidelines and safety for both patients and medical staff .)

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 58
18. OP. EPIDURAL ANALGESIA IN MULTIPY INJURED PATIENTS WITH SEVERE CHEST TRAUMA: TWO CASE REPORTS AND LITERATURE REVIEW NINA SULEN1, TATJANA ŠIMURINA1,2,3, EDI KARUC1, ANELA TOLIĆ4
1Department of Anesthesiology, Resuscitation and Intensive Care Medicine, General Hospital Zadar, Zadar, Croatia; 2Department of Anesthesiology, Resuscitation, Intensive Medicine and Pain Management, Faculty of Medicine „Josip Juraj Strossmayer“ University, Osijek, Croatia; 3Department of Health Studies, University of Zadar, Zadar, Croatia; 4Department of Radiology, General Hospital Zadar, Zadar, Croatia Multiply injured patients with severe chest trauma have different combinations of associated extra thoracic injuries making their treatment complex. Severe pain is a prominent symptom in a vast majority of severe chest injuries and causes deterioration of respiratory function. Epidural analgesia provides efficient pain relief but its use in this group of patients is burdened with complications, contraindications and technical diffi culties. We present two cases in which epidural analgesia was successfully used in polytrauma patients with severe chest injuries and hypoxemic respiratory failure, and discuss advantages, possible pitfalls and complications.

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 59
19. OP Major obstetric haemorrhage MANO DORAISWAMI
Barking, Havering and Redbridge University Hospitals NHS Trust, London, United Kingdom E-mail: [email protected] Summary:
Major Obstetric haemorrhage is a leading cause of maternal mortality in developed and developing countries. It accounts for 25% of all maternal deaths. Globally one woman dies every 6 minutes following postpartum haemorrhage. Physiological changes of normal pregnancy can mask the clinical picture of haemorrhage, leading to delayed recognition of massive obstetric haemorrhage. Estimation of obstetric blood loss can be challenging and inaccurate because of contamination with amniotic fluid and concealed losses. There are several definitions of postpartum obstetric haemorrhage but there is no universally accepted definition of Major Obstetric Haemorrhage. Failure to recognise and treat primary postpartum haemorrhage can quickly lead to major obstetric haemorrhage. Woman’s stature and original haemoglobin should be taken into account when estimating blood loss. A blood loss of more than 40% of total blood volume can be life threatening. Uterine atony is a frequent cause of major obstetric haemorrhage. Growing number of caesarean sections has led to increase in placenta accrete and abnormal placentation leading to increased incidence of major obstetric haemorrhage. Management of massive obstetric haemorrhage requires a multidisciplinary team approach. Prompt resuscitation, early transfusion of blood and clotting factorsand surgical assistance with source control is key. Because of the dynamic nature of major obstetric haemorrhage laboratory tests can delay management, point of care testing should be used. Early use of tranexamic acid is recommended with clinically diagnosed postpartum haemorrhage. Intraoperative cell salvage is useful in high risk patients. Fibrinogen is an early biomarker for progression of Postpartum haemorrhage. Risk of progression to severe PPH is increased 2.6-fold with each gram/dl decrease in plasma fibrinogen. Judicious use of uterotonics is necessary to prevent atony. Intraoperative balloon tamponade is an appropriate first line surgical intervention in uterine atony. Hysterectomy should not be delayed until the woman is in extremis.

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 60
20.OP Enhanced recovery in caesarean section VIKTOR DUZEL Barking, Havering and Redbridge University Hospitals NHS Trust, London, United Kingdom E-mail: [email protected] Summary:
Caesarean Section (CS) is one of the most commonly performed surgical procedures worldwide. In many countries there is evidence that planned or “elective” operations account for a growing proportion of all CS. Birth by CS is associated with prolonged hospital stay in comparison to spontaneous birth and the majority of women remain in hospital for at least two days after a planned CS procedure. Enhanced Recovery (ER), also known as accelerated or fast track recovery involves a number of interventions designed to improve quality of care by helping patients getting well sooner, as well as reducing their hospital stay and providing a much better experience. More and more studies are providing strong evidence that this is not just a safe practice but that patient satisfaction is much higher. Enhanced Recovery in Obstetrics is a relatively new concept but has been implemented in our unit with positive outcomes. The key to ensure successful implementation of enhanced recovery is engagement, commitment and involvement of the multidisciplinary team across the local health community. The plan for ER begins in the antenatal period, engages the patient in planning for the process and the successful implementation of the pathway requires components from the antenatal period through to discharge and follow-up.

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 61
21.OP Minimally invasive treatments for chronic pain
IVAN RADOŠ1 1The Clinic of Anaesthesiology, Reanimatology and Intensive Care, Department of Pain
Management, University Hospital Osijek, Osijek, Croatia
e-mail: [email protected]
Interventional and minimally invasive procedures in the treatment of chronic pain are often used
as one of the last options in treating pain when analgesics and physical therapy have proved
insufficient. Such an attitude is overcome by the "elevator model in pain management" in
treating cancer pain, but also for intense and very intense chronic pain. Long titration of
analgesics by “the three step analgesic ladder model” of non-opioid analgesics, through weak to
strong opioids, and the use of adjuvant analgesics often require a longer period of time until an
effective analgesic therapy is achieved or until adequate analgesic therapy at maximum dose
shows ineffective. During this time the patient suffers from severe pain which can often be
successfully treated with intervention procedures in the treatment of pain. The lift model has
placed severe and very severe pain interventions in the treatment algorithm of as a possible first
step in the treatment of pain. Intervention procedures may be diagnostic, prognostic or
therapeutic.
Prior to conducting the procedure, an informative interview with the patient should be made and
the mechanism of recommended invasive procedure explained in an understandable way, to
evaluate the patient's neurological status, to exclude possible contraindications. It is also
necessary to renew knowledge about the anatomy and technical aspects of blockage before
performing the block itself, to be aware of the potential complications and the possibilities of
their prevention and treatment, to choose the most appropriate intervention procedure, and no
less important to have manual skill and theoretical knowledge. Of the least invasive interventions
in the pain treatment clinics, epidural steroid use, epidurolysis, block joints, radiofrequency
denervation of the facetl joints, percutaneous laser disc decompression, cryo analgesia, etc. are
most commonly used.

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 62
AUTHORS’ INDEX (Lectures L, Posters P, Abstracts A, Workshops W,
Organization O) Alfirević Maša P17 Anić Milošević Sandra A12 Bačak Kocman Iva P5 Badel Tomislav L24, A12 Bagatin Dinko P18, P19, P21, P23, A3, A9, A10 Bagatin Tomica P 18, P19, P21, L3, A3, A9, A10 Bandić-Pavlović Daniela L16, P7, P9, A7 Banožić Ivona P4 Barković Marina P15
Baronica Robert A7 Baričić Mirjana P15 Bartolek Hamp Dubravka P5 Bašić Kes Vanja A12 Beker T. P14 Biberić Maša P16 Bičanić Ivana P22, A5 Bohaček Ivan L9, A16 Boras Barbara P22 Bošnjak Marija P22 Bošnjak Marko P22 Budić Nediljka P8 Bujas Tonka P6, A13 Bulić Ivana P22 Bureš Ivana P1 Car Šoštarić Alenka P10 Čimić Mislav A16 Dedić David A6 Delbos Alain L17
Delić Maša P22 Delimar Domagoj A16 Deutsch Judith Adrianne P18,P19 Djulabić Luka O Dobrić Mirela P10, P14 Doraiswami Mano L19 Drvar Željko A7 Dzaja Domagoj P22, A5 ðuzel Viktor L20, A6 Elezović Neven W4, O Fabijanić Tea P7 Fućak Primc Ana P12 Gligorijevic Slobodan L13 Goluža Eleonora O Graf Župčić Sandra A6, A8 Grbo Amela A1
Grubješić Igor A6 Habek Dubravko L27, A13, A17 Habijanec Borna P8 Haršanji-Drenjančević Ivana P13 Hladnik Ana P22, A5 Ivanec Željko P3 Ivanovski Ivan P3, P4 Jeleč Vjekoslav O Jelić Mislav A16 Kalagac Fabris Lada P16
Karmelić Dora P8 Karuc Edi P24, A18 Kaštelan Željko P21 Kličan Jaić Katarina P3, P4 Kocijan Lovko Sandra A12 Kodžoman Katica P11 Kontic Maša P2 Korušić Andjelko A6 Košeto Aleksandar P16 Kovač Nataša P9,A7
Kozmar Ana P1 Krapac Ladislav A12 Kristek Gordana P13 Kuna Krunoslav P3, P4 Lacković Martin Likić Robert P1 Mandušić Mario P10
Marić Marjan P21 Markovic-Bozic Jasmina A14 Matas Marijana P1 Medić Filip P17 Medved Tea P6 Mićić Slobodan P12 Mihaljević Dragan W1,W2 Mihaljević Slobodan L6, P5,P8, P9, A10, W1, W2 Miklić Bublić Martina P9, A7 Miletić Ana P14 Misir Anita P9 Mladić Batinica Inga P17 Mraović Boris A8 Mustač Filip P17 Nemrava Johann P18, P19, P21, A3 Nenadić Šprajc Sandra P21 Nešković Nenad P13

7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 63
Novak Jankovič Vesna L22, A14 Njerš Kristina P6 Oremuš Krešimir L21, A11 Orešković Zrinka P11
Paladino Josip P22 Pavelić Goran P12 Peršec Jasminka L18, A15 Peršin Beraković Andrea P5 Petanjek Zdravko L8, P22, A5 Petrović Igor P8 Pešić Maja P3, P4
Plečko Mihovil A16 Ptičar Tihana O Radolović Krešimir P16 Radoš Ivan L21, P13, W3
Rawal Narinder L2, L12 Roso Ivana P14
Rotim Krešimir O Rožanković Sanda P2 Sekulić Ante P1 Smoljan Mia A12 Sotošek Tokmadžić Vlatka P1 Splivalo Ivana P14
Stambolija Vasilije P22 Stipčić Ivana P11 Sulen Nina P24, A18 Suljević Ismet L7, A1 Suljević Omer A1 Šakić Kata L1, P15, P18, P19, P21, P23, A3, A9, A10 Šakić Livija L26, P23, A1, A6, A9, A10, W1, W2, O
Šakić Šimun O Šerić Monika A15 Šimurina Tatjana L15, P24, A6, A8, A18 Škiljić Sonja P13 Šklebar Ivan L5, P6, P20, A13, A17, W4 Šklebar Tomislav P20
Šurković Ismana A1 Škunca Agata P10 Šutić Ingrid A6 Šutić Ivana A6 Tolić Anela P24, A18 Tonković Dinko L23, P2, P9, A1, A7
Tripković Branko L10, P11, A16 Turan Maida A1 Van De Velde Marc L3, L4 Včev Aleksandar A10 Vinković Hrvoje P13 Virag Igor A7 Vitale Branko L11, A4
Vlatković Igor P21 Vrdoljak Luk A P22 Vučić Marinko P3 Vulin Marina A8 Zadravec Dijana A12 Zadro Željka P22 Zanghirella-Maretic Samantha P16 Zavoreo Iris A12 Zrna Siniša P16 Župčić Miroslav L14, P12, P15, A6, A8, W3 Žura Marijana P5


7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 65
7th CROATIAN CONGRESS OF REGIONAL ANAESTHESIA AND ANALGESIA WITH INTERNATIONAL PARTICIPATION
School of medicine University of Zagreb,Croatia, June 14 – June 15, 2019
Book of abstracts Final Programme 66