Embed Size (px)
Citation preview

Bone trabecular pattern analysis in Down syndrome with the use of computed panoramic radiography Part II: Visual pattern analysis with the frequency and gradational enhancement
Isamu Kashima, DDS, PhD,” Shiro Bando, DDS,” Daisuke Kanishi, DDS,a Kumeo Miyake, DDS, PhD,b Ryo Yamane, DDS,’ and Masao Takano, MS,d Kanagawa, Japan
KANAGAWA DENTAL COLLEGE
Visual pattern analysis of mandibular bone trabeculation of 51 patients with Down syndrome and 78 normal
persons was performed by using rotational panoramic radiography with a laser scan system. The findings for patients with Down syndrome were consistent with geromorphism, one of the somatic characteristics of Down syndrome. (ORAL SURC ORAL MED ORAL PATHOL 1990;70:360-4)
R ecent reports have shown a high incidence of pe- riodontal diseases among patients with Down syndrome.1-5 Incomplete oral cleaning has been held responsible for the susceptibility of patients with Down syndrome to periodontal diseases. Other fac- tors considered important include gingival abnormal- ity, alteration of the salivery components, and immu- nologic disorders due to trisomy 2 1 .6-9
Reports with respect to the mandibular bone tra- beculae in patients with Down syndrome have been rare. ‘, lo Analysis of mandibular bone trabeculae may not only help elucidate the etiology of periodontal diseases that occur at a high frequency in patients with Down syndrome but also provide important data on systemic bone metabolism due to aging. The man- dibular bone trabeculae of patients with Down syn- drome were compared with those of normal subjects by panoramic radiography with a laser scan system. This system has previously been reported by Kashima and coworkers.’ 1
MATERIAL AND METHODS Subjects
Fifty-one patients with Down syndrome and 78 normal persons with no deformity, congenital abnor-
aDepartment of Oral Radiology. bDepartment of Anesthesiology. cDepartment of Oral Diagnosis. dTechnology Development Center, Miyanodai Fuji Photo Film Company. 7/16/19353
360
9 7
5
Y3
ii 0 a1 v) Y u
0.0 1 0.1 0.25 0.5 1.0 2.0 10.0
SPATIAL FREQUENCY ( c/mm 1
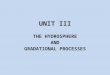
Fig. 1. The four spatial frequency processing conditions (A, B, C, D) used. Enhancement rank increased with increasing frequency.
mality, or contributory history were studied. Chro- mosomal karyotype examination revealed that 50 of the patients with Down syndrome had the trisomy, and one the translocation type. Table I shows the ages and gender ratios of the patients with Down syndrome and the normal control subjects.
Image processing
The spatial frequency range that provides accept- able visible images is believed to be 0.5 to 2.0 cycles/ mm. The four types of spatial frequency processing conditions used are shown in Fig. 1.

Volume 70 Number 3
Bone trabecular pattern analysis in Down syndrome: Part II 361
Fig. 2. Trabecular patterns of normal persons and patients with Down syndrome were classified into four patterns: AC, AD, BC, and BD. A, Clear bone trabeculae with high contrast. B, Unclear bone trabeculae with low contrast. C, Coarse bone trabeculae with large intramedullary cavities. D, Dense bone trabeculae with small intramedullary cavities.
Image classification
The image of trabecular patterns produced by computed panoramic radiography with a laser scan system can be visually recognized by both contrast and morphologic changes. Therefore the following four criteria were adopted for classification on the basis of contrast and morphology:
l A: Clear bone trabeculae with high contrast l B: Unclear bone trabeculae with low contrast l C: Coarse bone trabeculae with large intrame-
dullary cavities l D: Dense bone trabeculae with small intrame-
dullary cavities The trabecular patterns of the normal subjects and
patients with Down syndrome were classified into four patterns, AC, AD, BC, and BD (Fig. 2), by three dentists who made alternative judgments, that is, A or B and C or D. Only the premolar to the molar region of the mandible was analyzed.
RESULTS
Computed radiographs of patients with spatial fre- quency enhancement at 0.25 cycle/mm (Fig. 3, A), 0.5 cycle/mm (Fig. 3, B), 1 .O cycle/mm (Fig. 3, C), and 2.0 cycles/mm (Fig. 3, D) are illustrated. En- hancement rank increased with increasing frequency. In Fig. 3, A, and Fig. 3, B, coarse bone trabeculae were enhanced, but fine trabecular components remained obscure. On the contrary, fine components were excessively enhanced in Fig. 3, D. In Fig. 3, C, both the coarse and fine trabeculae are clearly visualized, giving a clear-cut image. For the visual analysis of trabecular patterns, enhanced imaging at a spatial
Table I. Ages and gender ratios for patients with Down syndrome and normal persons surveyed
Down syndrome Normal persons IWFJ MW
18-29 30-39 40-49 so-59 Total
35 (18:17) 25 (14:ll) 14 (7:7) 22 (12:lO) 2 (1:l) 15 (7:8)
16 (6:lO) ?l (26:25) 78 (39:39)
frequency of 1 .O cycle/mm and an enhancement rank of 7 were employed, as shown in Fig. 3, C. The gra- dational enhancement was linear. A distribution of the trabecular patterns of the normal subjects and patients is shown in Fig. 4. In the normal group, the AC pattern accounted for 53% and the percentage of the AD, BD, and BC patterns was 3 1%, 16%, and 0%, respectively. In the Down syndrome patient group, the BD pattern ranked the highest frequency (80%). The percentage having the AC pattern was 2.2%, and for the AD pattern it was 4.5%.
The four types of pattern according to age subgroup are illustrated in Fig. 5. In the young normal subgroup (18 to 29 years), the AC pattern showed the highest rate (90%), followed by the BD pattern (10%). None showed the BC pattern. In the older age subgroup (50 to 59 years), the AD pattern accounted for 68.5%, and the AC pattern for 12.5%. Thus, with increasing age, the AC pattern showed a decrease, and the BD and AD patterns, an increase.
In the patients with Down syndrome, the BD pat-

362 Kashima et al. ORAL SURC ORAL MED ORAL PATH~L September 1990
% 1OOr
Fig. 3. Computed panoramic radiographs with spatial frequency enhancement at 0.25 cycle/mm, rank 3 (A), 0.5 cycle/mm, rank 5 (B), 1.0 cycle/mm, rank 7 (C), and 2.0 cycles/mm, rank 9 (D). Gradational enhancement was linear.
20
0 A .C A .D B .C B .D
Fig. 4. Distribution of mandibular bone trabecular pat- terns (AC, AD, BC, BD) of normal control subjects and pa- tients with Down syndrome.
tern was most frequent, irrespective of age, account- ing for 73.3% in the 18- to 29-year-old subgroup and 91.6% in the 30- to 39-year-old subgroup. The BC pattern, which was absent in the normal group, was observed in 16.6% of the 18- to 29-year-old patients and 8.3% of the 30- to 39-year-old patients with Down syndrome.
Figs. 6 and 7 show the correlations between age and the trabecular pattern criteria A, B, C, and D for the normal and Down syndrome patient groups. In the normal control subjects, types A and C showed high rates, but were gradually replaced by types B and D with increasing age. The rate of change (morphologic changes on the image of bone trabeculae) for the C, D pattern tended to be higher than that for the A, B pattern (contrast changes).
In the patients with Down syndrome, all age sub-
% DOW” Normal Down Norma i Down Normal
Fig. 5. Ratio of four patterns (AC, AD, BC, BD) accord- ing to age subgroup in normal and Down syndrome subjects.
groups showed a high rate for pattern B, and none of the patients aged between 30 and 40 years showed pattern A. This tendency was contrary to that in the normal group. Patterns C and D exhibited similar tendencies to those of the 40- to 59-year-old normal subjects, irrespective of age.
DISCUSSION
The presence or absence of an abnormality in the structure of the mandible was the focus of this study as one of the possible causes for the susceptibility of patients with Down syndrome to periodontal disease. The bone structure consists basically of the perios- teum, bone cortex, and intramedullary cavity. The cancellous bone forming the intramedullary cavity is visualized as a linear or reticular pattern of bone tra- beculae on the radiographic image. Bone tissue is dy-

Volume 70 Number 3
Bone trabecular pattern analysis in Down syndrome: Part ZZ 363
E
A
-
% % 100 100
80 60
60 60
40 40
20 20
0 - 18-B 30-40
0 18-29 30-40 AGE
-59 AGE Fig. 7. Correlation between age and criteria in Down syndrome group. Constant contrast (A,B) and morphology (C,DJ with no age-related changes.
0 18-29 30-39 40-49 So-59 AGE
Fig. 6. Correlation between age and criteria A, B, C, and D in normal group. Rate of change (morphologic changes on the image of bone trabeculae) for the C, D pattern tended to be higher than that for the A,B pattern (contrast changes).
namic in that it undergoes repeated resorption and formation. In particular, the mineral content of the cancellous bone fluctuates in close response to changes in bone metabolism. Generally, it has been said that bone loss and calcification of abnormalities can only be detected by conventional radiography when the bone demineralization or hypermineralization is more than 30% to 40%.‘*, l3
Rotational panoramic radiography, a procedure that is relatively standardized, was employed because it is simple to manipulate and allows evaluation of the entire mandible. Because of the blurred images spe- cific to tomographs, conventional panoramic radio- graphs are not suitable for the visual analysis of the mandibular bone trabeculae. This problem was over- come by using a laser scan system, which visualized the trabeculae clearly and allowed relatively accu- rate classification of the patterns on the image produced.
The mandibular trabeculae of the normal subjects showed morphologic changes with increasing age, but with a fairly constant contrast. It was found that the mineral content of the bone rarely demonstrated image changes in normal persons aged between 18
and 50 years. In contrast, the patients with Down syndrome continued to exhibit nearly a constant con- trast and morphology of the mandibular trabeculae, with no age-related changes. The trabecular form found in patients with Down syndrome was invariably similar to that of the 50- to 59-year-old normal sub- jects. This indicates that from childhood, the man- dibular trabeculae of patients with Down syndrome are similar to those of aged healthy persons. Thus, the trabecular patterns in the patient group were consis- tent with geromorphism, a somatic characteristic of Down syndrome.
CONCLUSIONS
The visual pattern of the mandibular trabeculae in patients with Down syndrome was analyzed by com- puted panoramic radiography. The results were com- pared with those from normal subjects, and the following conclusions were reached:
1. The mandibular trabeculae of the normal sub- jects changed with increasing age.
2. The mandibular trabeculae of the patients with Down syndrome showed a dense pattern with weak radiopacity that showed no correlation to patient age.
REFERENCES
1. Johnson NP, Young MA. Periodontal disease in mongols. J Periodontol 1963;34:41-7.
2. &tress TW. Periodontal disease and oral hygiene in trisomy 21. Arch Oral Biol 1971;16:1345-55.
3. Saxen L, Aula S. Periodontal bone loss in patients with Down syndrome: a follow-up study. J Periodontol 1982;53:158-62.
4. Omori S, Omori H, Kato T. A case of the periodontal disease associated with Down syndrome. J Jpn Assoc Periodont 1951; 23:526-30.
5. Miyake K, Iwasaki K. Periodontal disease in the physically handicapped persons. II. Down syndrome. J Jpn Assoc Perio- dont 1983;25:636.
6. Sznajder N, Carraro J. Clinical periodontal findings in trisomy 21 (mongolism). J Periodont Res 1968;3:1-5.

364 Kashima et al.
7. Lovey TH. Periodontal disease in patients with Down syn- drome. Chicago Dental Society Rev 1979;72:23-6.
8. O’Donnel J, Cohen M. Dental care for the institutionalized retarded individual. J Pedod 1984;9:3-38.
9. Remand-Bosmd W, van Dijke LJ. Periodontal disease in Down syndrome: a review. J Clin Periodontol 1986;13:64-73.
IO. Kashima I, Kanno M, Oguro T, Higashi T. Sakai N, et al. Bone trabecular pattern analysis in Down syndrome with the use of computed panoramic tomography with a laser scan system: quantitiative analysis with the power spectrum method. ORAL SURG ORAL MED ORAL PATHOL 1988;65:366-70.
Il. Kashima 1, Kanno M, Higashi T, Takano M. Computed pan- oramic tomography with scanning laser-stimulated lumines- cence. ORAL SURG ORAL MED ORAL PATHOL 1985;60:448-53.
12.
13.
Reprint requests to. Dr. Isamu Kashima Department of Oral Radiology Kanagawa Dental College 82, Inaoka-cho. Yokosuka Kanagawa Japan
ORAL SURG ORAL h(tD ORhL PATHo September 1990
Agus ZS, Goldberg M. Pathogenesis of uremic osteodystro- phy. Radio1 Clin North Am 1972;10:545-56. Shapiro R. Radiologic aspects of renal osteodystrophy. Radio1 Clin North Am 1972: IO:557-68.