Embed Size (px)
Citation preview

bone remodeling rate
bone remodeling rate
The bone remodeling rate (BRR):
the period of time needed for new bone to
replace the existing bone and to allow for
the adaptation of bone to its environment
BRR is expressed as a percentage or
volume of new bone within a specific time
period.
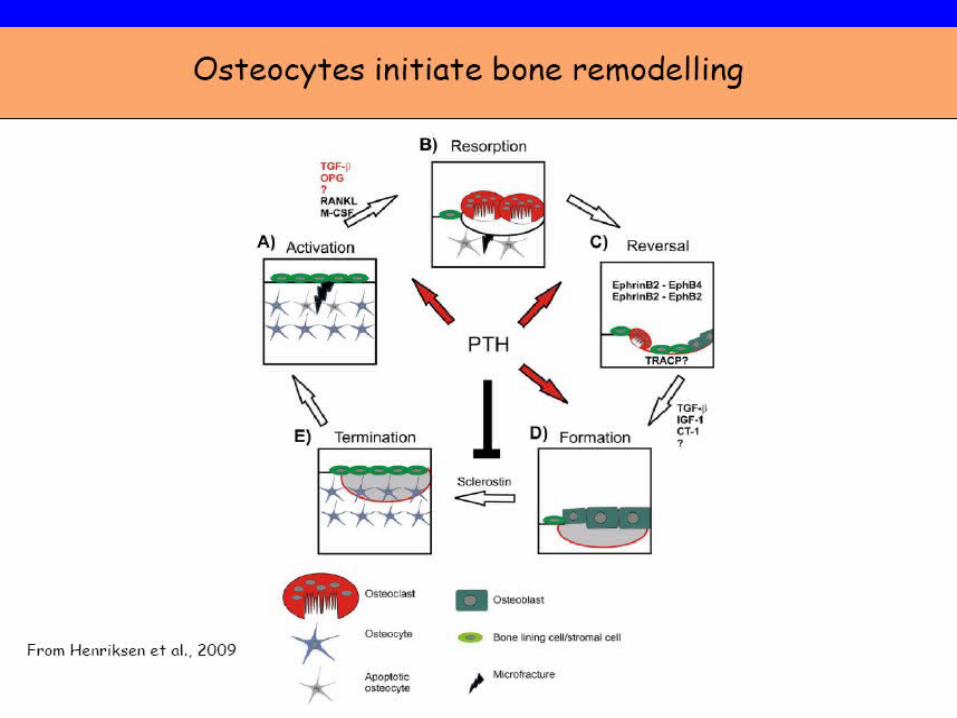
phases of bone remodelling
• :
• activation, resorption, reversal, formation and
• termination.

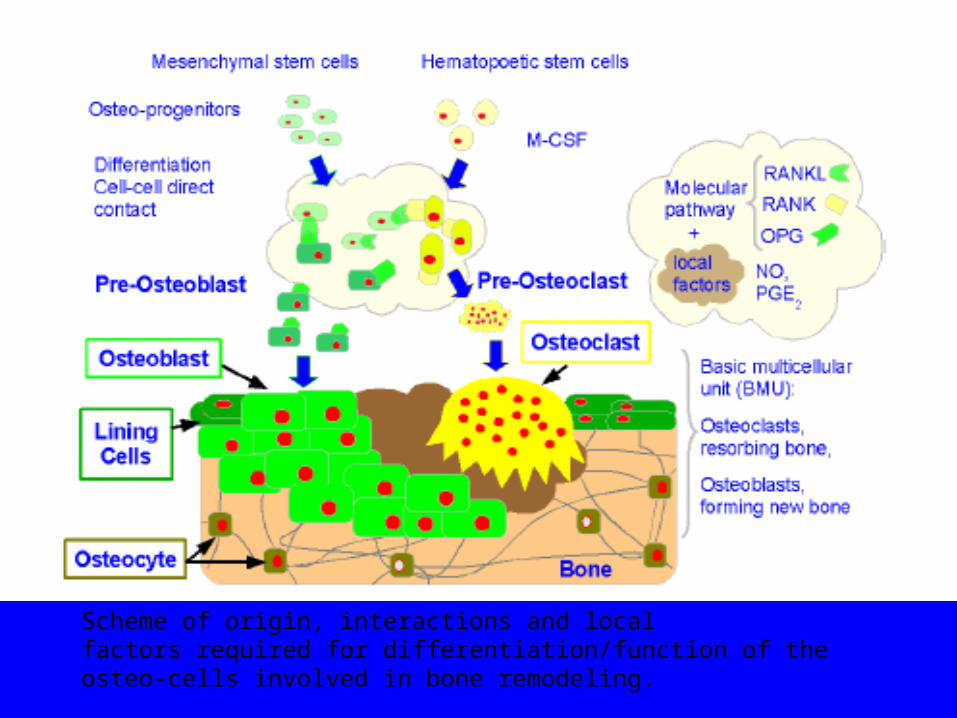
Scheme of origin, interactions and localfactors required for differentiation/function of theosteo-cells involved in bone remodeling.
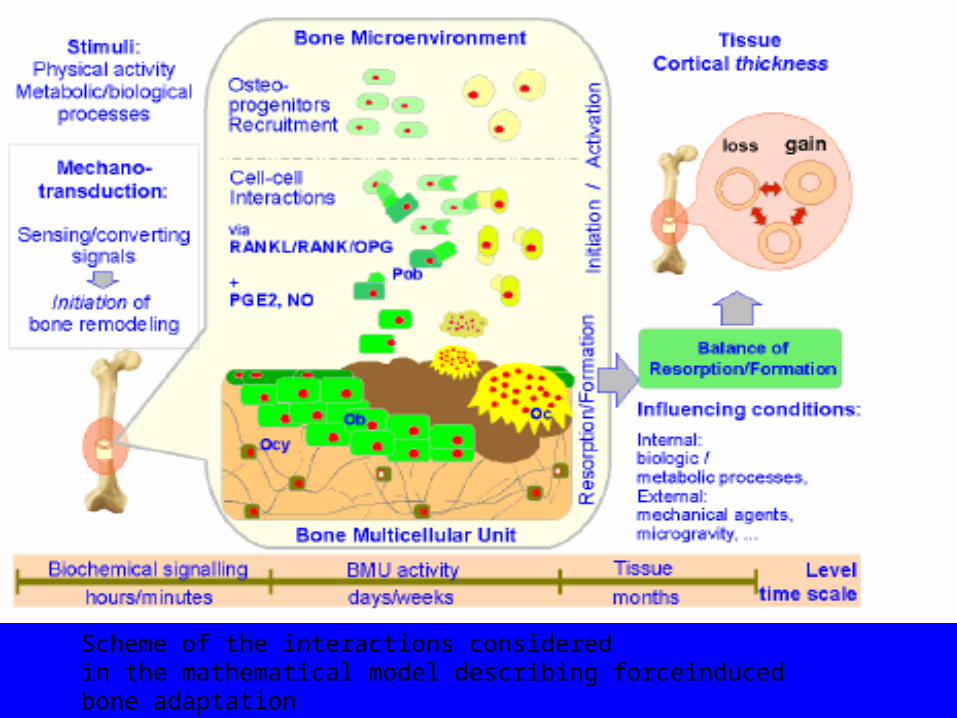
Scheme of the interactions consideredin the mathematical model describing forceinducedbone adaptation
Cells of bone remodling
• 1-Osteoclasts
• 2-Osteocytes
• 3-Osteoblasts
• 4-T-cells and B-cells
• 5-Megakaryocytes
• 6-Osteomacs
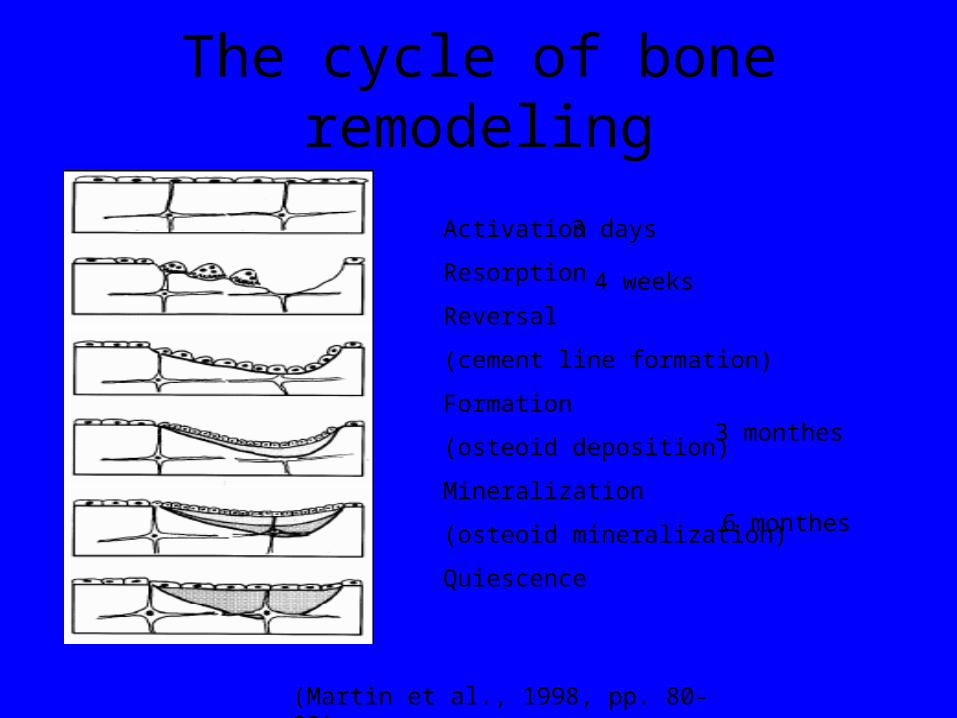
The cycle of bone remodeling
Activation
Resorption
Reversal
(cement line formation)
Formation
(osteoid deposition)
Mineralization
(osteoid mineralization)
Quiescence
3 days
4 weeks
3 monthes
6 monthes
(Martin et al., 1998, pp. 80-83).
• Concurrently with osseointegration process, bone remodelling occurs, where the bone density is
• changed due to the implant induced mechanical loading [5]. Therefore, bone remodelling is in
• essence a process where the bone changes its own property to adapt to its changing mechanical
• loading environment [6]. As bone remodels positively, the quality of the bone will improve, therefore
• leading to the stabilization of the dental implant inside the dental bone. This will have the effect of
• reducing the rate of implant failure. Therefore, in order to optimize the dental implant design, it is
• crucial to understand the magnitude and the development of mechanical stress inside the bony
• tissues. Such predictions can help to minimize the possibility of implantation failure.
mechanotransduction
• The conversion of biophysical force to cellular and biochemical response
• It comprises four phases
• 1-mechanocoupling
• 2-biochemical coupling
• 3-transmision of signal from sensor to effector cells
• 4-effector cell responses

Cellular Response to Loading• Cellular functions to remodel the bone is
controlled by a feedback loop:
Tissue Strains
Proximal Stimuli
Cellular Deformation
Tissue Remodeling
- min = cell
do not add bone add bonecell0

Cellular Mechanoreception• Cells contain specialized structures to detect
mechanical stimuli:
• Most mechanoreceptors require cellular deformation to transduce the signal
+ + + +
voltage activated ion channels
stretch activated ion channels
integrin interactions and cytoskeletal mechanisms
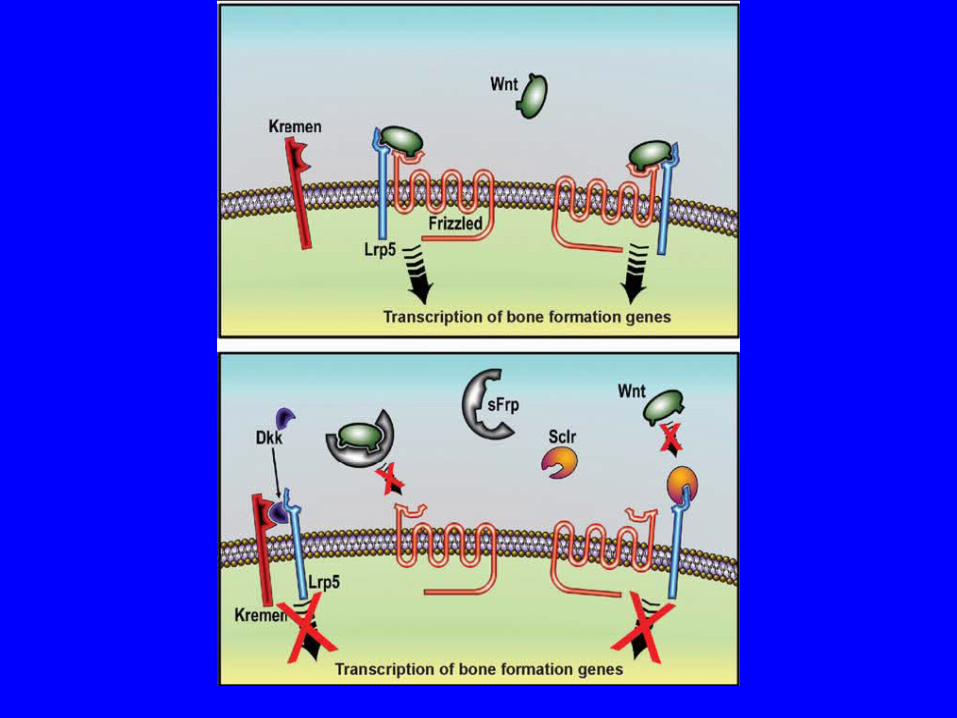
• Mechanical loading requires signaling through the Lrp5 receptor to initiate bone formation.
• This signal is initiated by Wnt, which binds to the receptor complex made up of Lrp5 and
• Frizzled. Wnt signaling can be blocked by Dickkopf related protein (Dkk) when it binds Lrp5
• and Kremen. Sclerostin (Sclr) inhibits Wnt signaling by binding Lrp5 and secreted
• Frizzled-related protein (sFrp) binds to Wnt and prevents signaling. Each of these inhibitors
• blocks mechanotransduction and reduces bone formation.

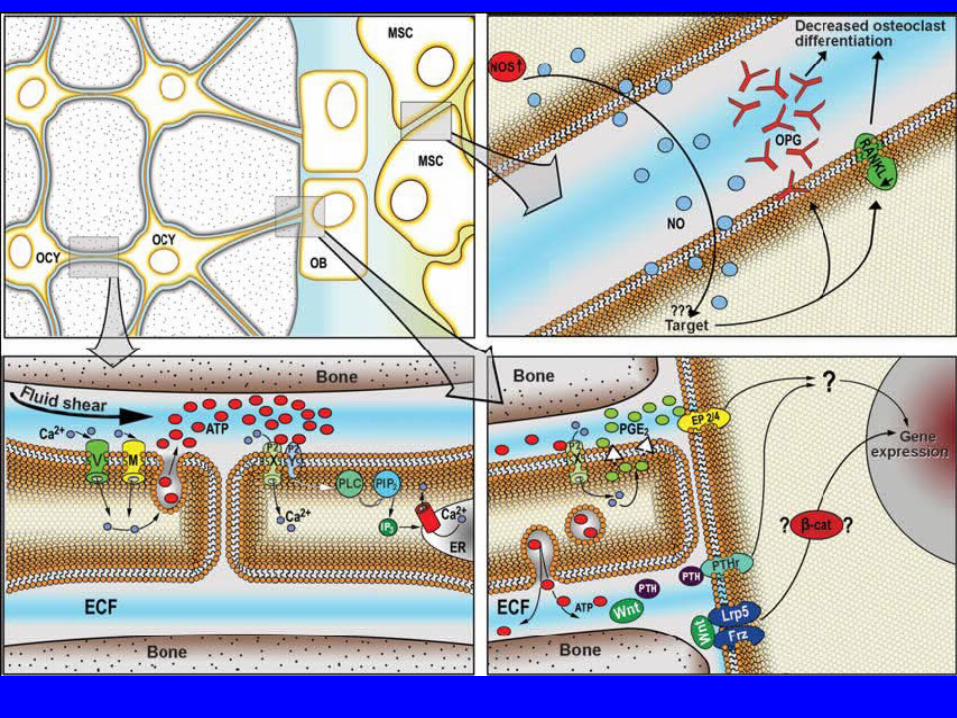
• Fluid shear on osteocytes (OCY) induces an influx of• extracellular Ca2+ via voltage-sensitive (V) and perhaps mechanosensitive (M) channels.
Shear• stress also enhances ATP release, which binds to the purinergic receptors P2X (ionotropic)
and• P2Y (metabotropic). Signaling through P2Y is required for Ca2+ release from intracellular• stores via a Gq – PLC – PIP2 – IP3 pathway. ATP release causes PGE2 release through• signaling downstream of the P2X7 receptor. PGE2 binds and signals through one of the EP• receptors, probably EP4 and/or EP2, and ultimately results in enhanced bone formation. PTH• signaling also appears to be required for mechanotransduction to occur, but the intracellular• pathways involved are not well understood (question mark). Wnt signaling through the Lrp5• receptor, which acts through beta catenin (β-cat) translocation to the nucleus, also appears
to• be important in mechanically induced bone formation. Pressure in the marrow cavity and/or• fluid shear forces on marrow stromal cells (MSC) may stimulate nitric oxide synthase (NOS)• activity and nitric oxide (NO) release. NO is a strong inhibitor of bone resorption and• probably acts by inhibiting RANK-L expression, while increasing osteoprotegerin (OPG)• production (RANK-L enhances osteoclast differentiation, whereas OPG suppresses this• process). OCY = osteocyte; OB = osteoblast; MSC = marrow stromal cell.

• Lrp5 appears to be a potent regulator of bone• mass, size, and strength. One of the main mechanisms of action• for the receptor in bone is through mechanical signaling,• Lrp5 is a late-acting• mediator in the osteogenic response to mechanical loading,• suggesting that skeletal fragility in individuals afflicted with• OPPG might be related to inadequate processing of signals• derived from mechanical stimulation.
• intermittent• PTH might be an effective treatment for improving bone mass• in these patients.
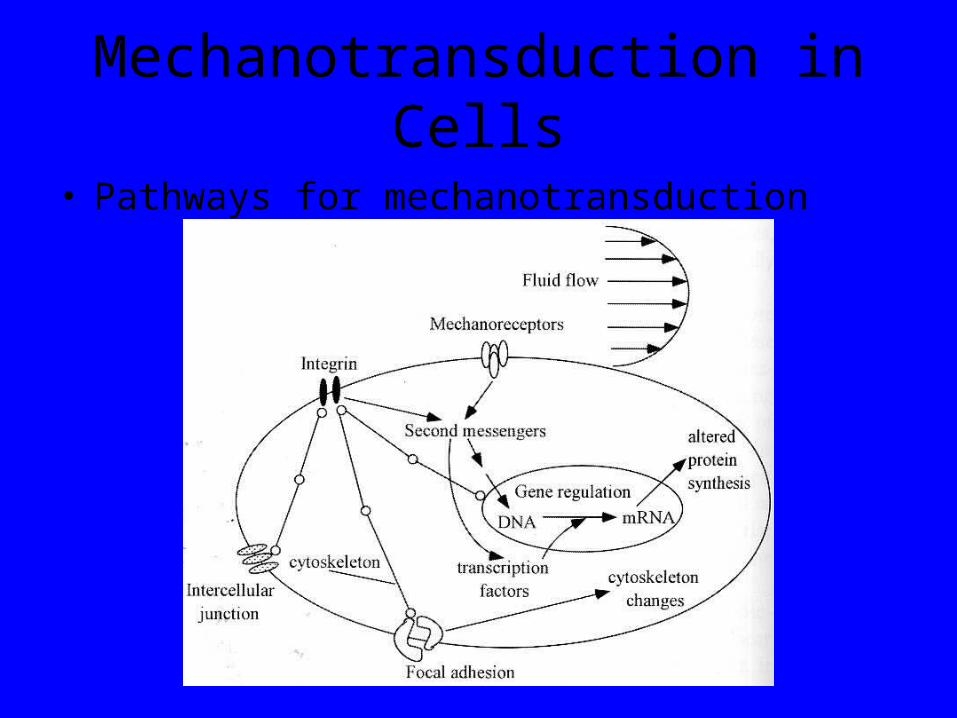
Mechanotransduction in Cells
• Pathways for mechanotransduction
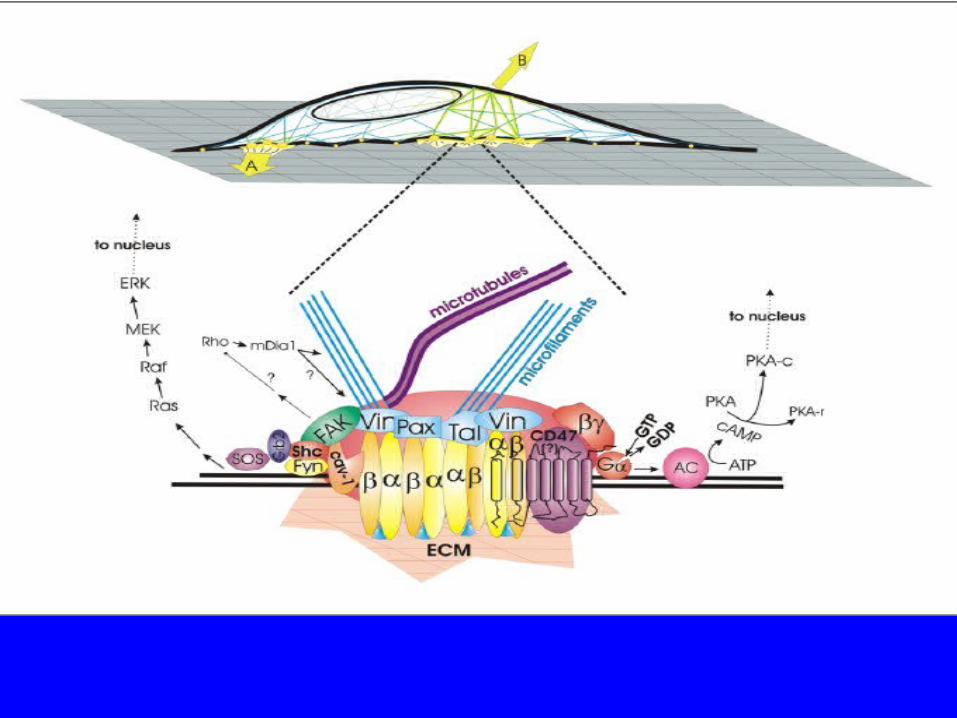
• forces applied through the ECM (A) or directly to the cell• surface (B) travel to integrin-anchored focal adhesions through matrix attachments or
cytoskeletal• filaments, respectively. Internally-generated tension and forces transmitted through• cell-cell contact similarly reach focal adhesions through the cytoskeleton. Forces concentrated• within the focal adhesion (magnified at bottom of figure) can stimulate integrin clustering and• induce recruitment of additional cytoskeletal linker proteins (Vin, vinculin; Pax, paxillin; Tal, talin)• that connect directly to microfilaments and indirectly to microtubules. Forces applied to this• specialized cytoskeletal adhesion complex also activate integrin-associated signal cascades.• Focal adhesion kinase (FAK) may be involved in Shc recruitment as well as modulation of Rho• activity which, in turn, can regulate the force response through mDia1. Caveolin-1 (cav-1) can• also recruit Shc to integrins to activate the ERK cascade. CD47 associates with the integrin• heterodimer to form a protein complex with seven transmembrane segments that mimics the• action of G protein-coupled receptors. In the case shown, when integrins are mechanically• stressed, the complex stimulates Gs-mediated up-regulation of the cAMP cascade through• adenylate cyclase (AC), resulting in nuclear translocation of the catalytic subunit of protein kinase• A, PKA-c
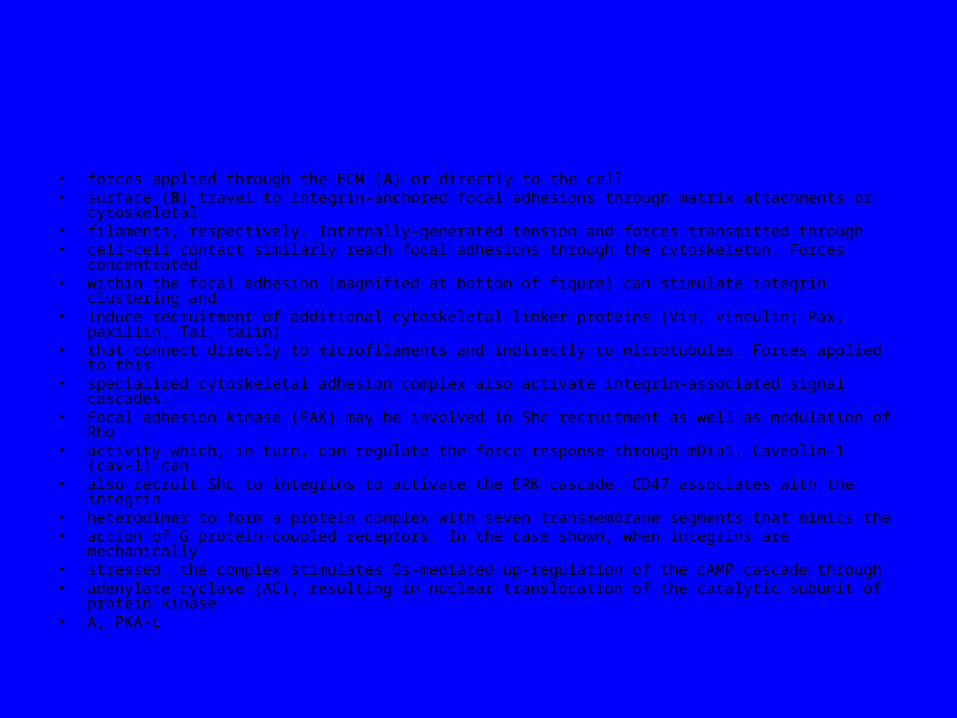
Factors affecting bone modling and remodling around dental implant
In non-human primate studies, itwas observed that five out of eight implantslost osseointegration due to excessiveocclusal overloading after 4.5–15.5months of loading (Isidor 1996, 1997).Among the three remaining implants, oneshowed severe crestal bone loss and theother two showed the highest bone–implant contact and density. The resultssuggested that implant loading might havesignificantly affected the responses of periimplantosseous structures. However, itshould be noted that the loss of osseointegrationobserved might have been attributedto the unrealistically high-occlusaloverload used in the study
• Low-amplitude and low frequency specific strains• (15-30 Hz) were demonstrated to have an osteogenic• effect and act as a growth factor to encourage• bone response to loading (19). Low-magnitude• high frequency (30-50 Hz) mechanical signals• produce, instead, anabolic effects on bone. If• such loading regimens could be applied for dental• implants, a favorable mechanical environment for• osseointegration is promoted. Bone-implant interface• maturation could be faster because bone deposition• increases.
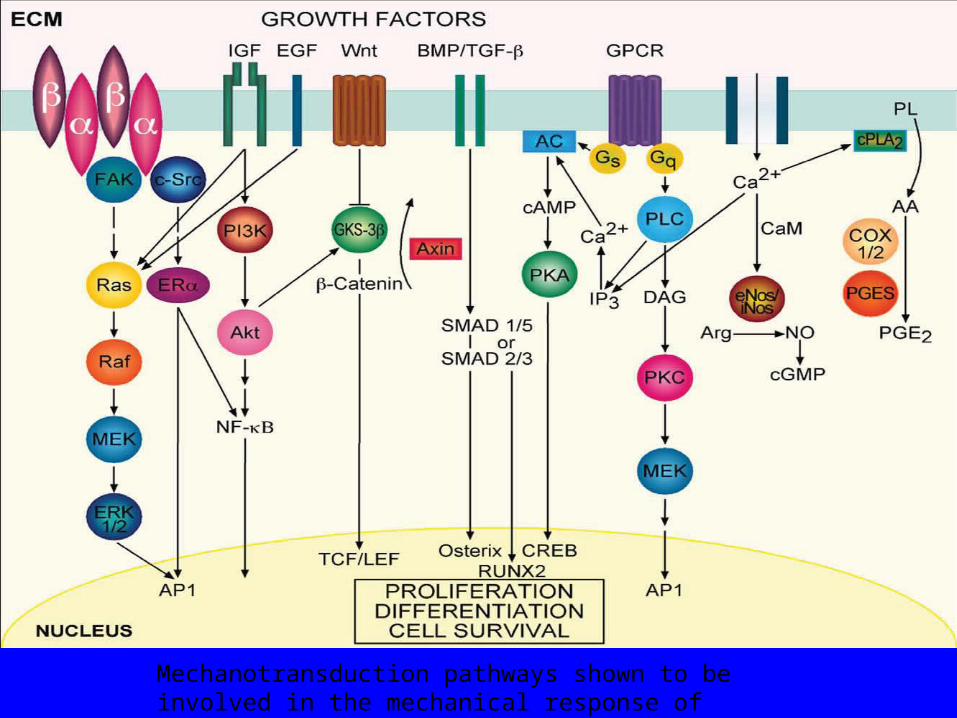
Mechanotransduction pathways shown to be involved in the mechanical response of osteoblastic cells

Local Regulation of Bone HealingGrowth factors
CytokinesProstaglandins/Leukotrienes
HormonesGrowth factor antagonists
• Preserving the Bone Level• Marginal bone remodeling is obviously a multifactorial issue.• The surgery-induced trauma can be highly detrimental for the• release of a flap and induces some cell death, which provokes• an inflammatory process and brings mediators of bone• resorption. The more the bone is exposed and dried by suction,• the more bone resorption occurs. This is the rationale for the• use of conservative surgical approaches in these procedures.
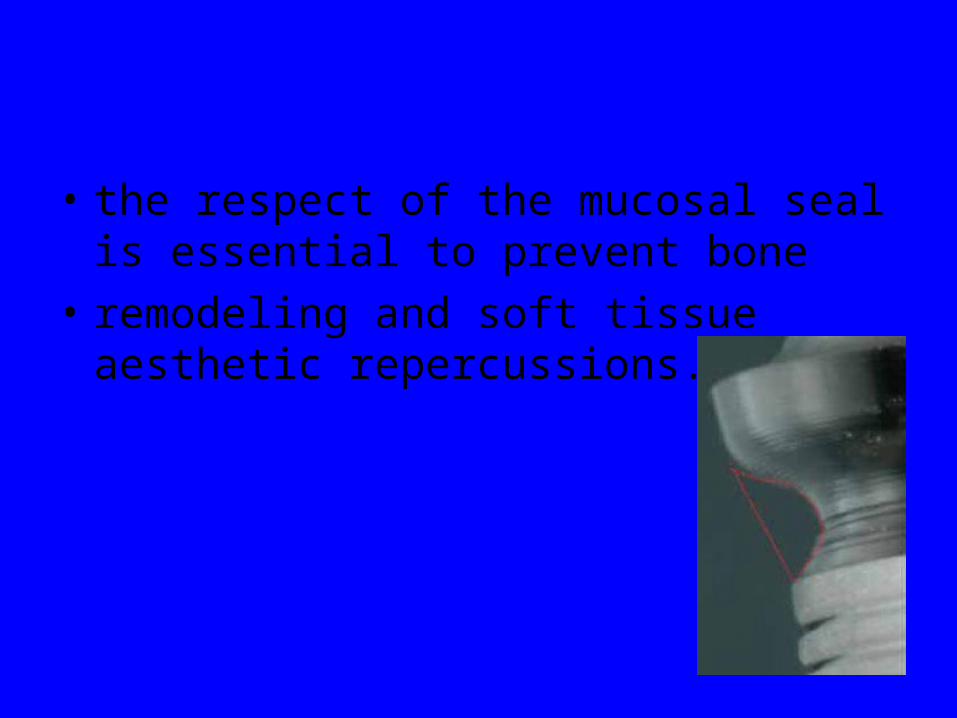
• the respect of the mucosal seal is essential to prevent bone
• remodeling and soft tissue aesthetic repercussions.

• The transmucosal components’
• design should be concave, inwardly narrowed in order to
• positively impact the soft tissues
• The mobility of the peri-implant mucosa is highly deleterious
• because when tearing of connective tissue occurs with
• microbleeding, the protective role of the junctional epithelium
• induces the apicalization of the latter. By consequence, a layer
• of connective tissue of 1mm (in average) has to reform more
• apically – often at the expense of the bone crest
• Growth Factors
• Transforming growth factor
• Bone morphogenetic proteins
• Fibroblast growth factors
• Platelet-derived growth factors
• Insulin-like growth factors
• Transforming Growth Factor• Superfamily of growth factors (~34 members)• Act on serine/threonine kinase cell wall receptors• Promotes proliferation and differentiation of
mesenchymal precursors for osteoblasts, osteoclasts and chondrocytes
• Stimulates both endochondral and intramembranous bone formation– Induces synthesis of cartilage-specific proteoglycans and type II
collagen– Stimulates collagen synthesis by osteoblasts
• Bone Morphogenetic Proteins• Osteoinductive proteins initially isolated from demineralized bone
matrix– Proven by bone formation in heterotopic muscle pouch
• Induce cell differentiation– BMP-3 (osteogenin) is an extremely potent inducer of mesenchymal
tissue differentiation into bone
• Promote endochondral ossification– BMP-2 and BMP-7 induce endochondral bone formation in segmental
defects
• Regulate extracellular matrix production– BMP-1 is an enzyme that cleaves the carboxy termini of procollagens I,
II and III
• Bone Morphogenetic Proteins • These are included in the TGF-β family
– Except BMP-1
• BMP2-7,9 are osteoinductive• BMP2,6, & 9 may be the most potent in
osteoblastic differentiation• Work through the intracellular Smad pathway• Follow a dose/response ratio
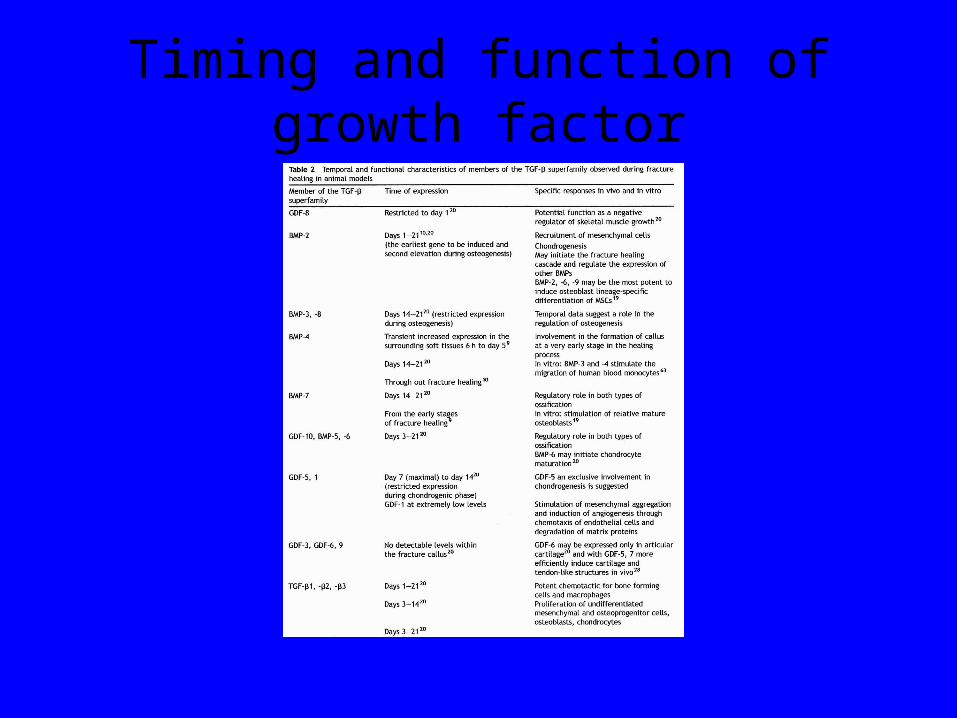
Timing and function of growth factor
• BMP Antagonists
• May have important role in bone formation
• Noggin– Extra-cellular inhibitor– Competes with BMP-2 for receptors

• BMP Future Directions• BMP-2
– Increased fusion rate in spinal fusion
• BMP-7 equally effective as ICBG in nonunions• Must be applied locally because of rapid
systemic clearance • ? Effectiveness in acute fractures• ? Increased wound healing in open injuries• Protein therapy vs. gene therapy

Importance of mechanical aspects
If we know the mechanical aspect well, then one can control bone remodeling through mechanical stress that applied through exercise either voluntarily or with the help of mechanical devices. (orthopedics)
• Fibroblast Growth Factors
• Both acidic (FGF-1) and basic (FGF-2) forms
• Increase proliferation of chondrocytes and osteoblasts
• Enhance callus formation
• FGF-2 stimulates angiogenesis

• Platelet-Derived Growth Factor• A dimer of the products of two genes, PDGF-A
and PDGF-B– PDGF-BB and PDGF-AB are the predominant forms
found in the circulation• Stimulates bone cell growth• Mitogen for cells of mesenchymal origin• Increases type I collagen synthesis by
increasing the number of osteoblasts• PDGF-BB stimulates bone resorption by
increasing the number of osteoclasts
• Insulin-like Growth Factor• Two types: IGF-I and IGF-II
– Synthesized by multiple tissues– IGF-I production in the liver is stimulated by
Growth Hormone
• Stimulates bone collagen and matrix synthesis
• Stimulates replication of osteoblasts• Inhibits bone collagen degradation

• Cytokines • Interleukin-1,-4,-6,-11, macrophage and
granulocyte/macrophage (GM) colony-stimulating factors (CSFs) and Tumor Necrosis Factor
• Stimulate bone resorption– IL-1 is the most potent
• IL-1 and IL-6 synthesis is decreased by estrogen– May be mechanism for post-menopausal bone resorption
• Peak during 1st 24 hours then again during remodeling• Regulate endochondral bone formation

Specific Factor Stimulation of Osteoblasts and Osteoclasts
• OsteoclastsCytokine Bone Formation Bone ResorptionIL-1 + +++TNF-α + +++TNF-β + +++TGF-α -- +++TGF-β ++ ++PDGF ++ ++IGF-1 +++ 0IGF-2 +++ 0FGF +++ 0
• Prostaglandins / Leukotrienes• Effect on bone resorption is species dependent
and their overall effects in humans unknown• Prostaglandins of the E series
– Stimulate osteoblastic bone formation– Inhibit activity of isolated osteoclasts
• Leukotrienes– Stimulate osteoblastic bone formation– Enhance the capacity of isolated osteoclasts to form
resorption pits
• Vascular Factors• Metalloproteinases
– Degrade cartilage and bones to allow invasion of vessels
• Angiogenic factors– Vascular-endothelial growth factors
• Mediate neo-angiogenesis & endothelial-cell specific mitogens
– Angiopoietin (1&2)• Regulate formation of larger vessels and branches

species• Table 1. Summary of four key attributes in terms of similarity between animal and human bone.
Canine Sheep/Goat Pig Rabbit Macrostructure ++ +++ ++ +
Microstructure ++ + ++ +
Bone Composition +++ ++ +++ ++
Bone Remodelling ++ ++ +++ +
+ least similar, ++ moderately similar, +++ most similar.
Signficans of bone remodling
• responsible for removal and repair of damaged
• bone to maintain integrity of the adult skeleton
• and mineral homeostasis.
Bone Remodeling• Bone structural integrity is continually
maintained by remodeling
– Osteoclasts and osteoblasts assemble into Basic Multicellular Units (BMUs)
– Bone is completely remodeled in approximately 3 years
– Amount of old bone removed equals new bone formed
http://www.elixirindustry.com/resource/osteoporosis/jilka.htm

. Currently available bone biochemical markers.
• . • A. Formation • Serum
– Bone specific alkaline phosphatase (BSAP) – Osteocalcin – Carboxy-terminal propeptide of type I collagen (PICP) – Amino-terminal propeptide of type I collagen (PINP
• B. Resorption • Urine
– Hydroxyproline – Free and total pyridinoline (Pyd) – Free and total deoxypyridinoline (Dpd) – N-telopeptide of collagen cross links (NTx) – C-telopeptide of collagen cross links (CTx)
• Serum – Cross-linked C-telopeptide of type I collagen (ICTP) – Tartrate-resistant acid phosphatase (TRAP) – NTx – CTx
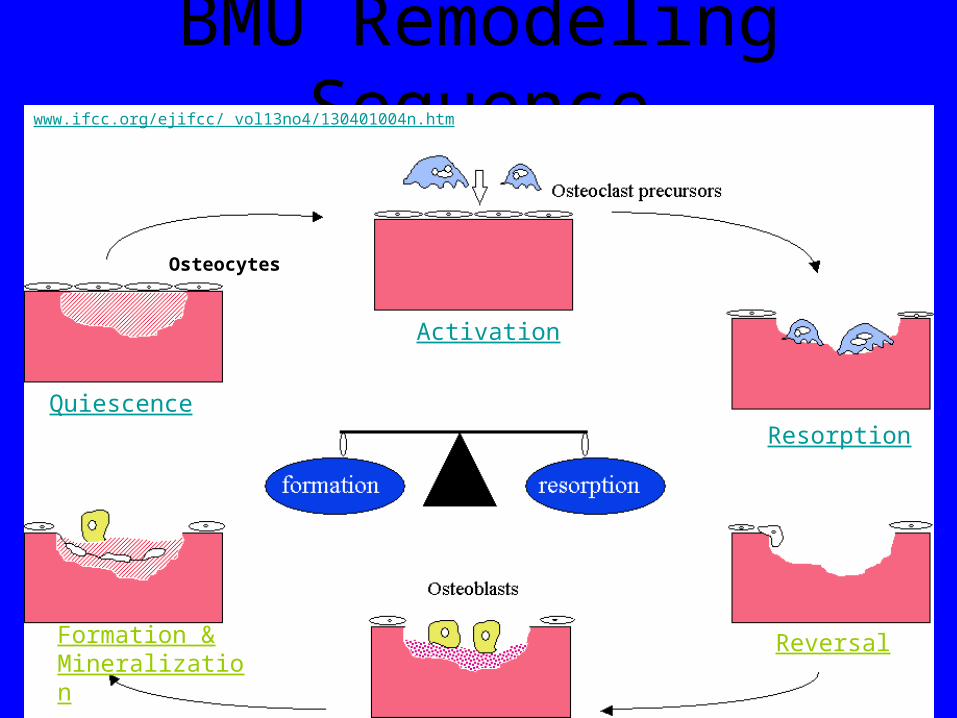
BMU Remodeling Sequence
Activation
Resorption
Reversal
Quiescence
Formation & Mineralization
www.ifcc.org/ejifcc/ vol13no4/130401004n.htm
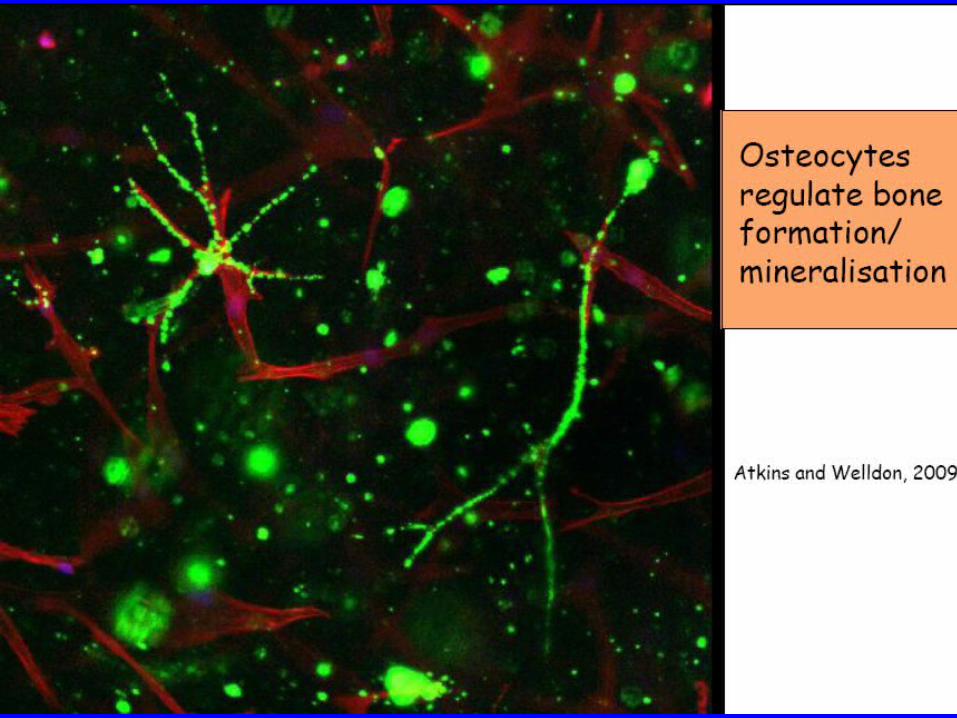
Osteocytes
• Endocrine– STH (somatotropic or growth hormone): increases cell
division & all subsidiary processes (total protein synthesis, net protein synthesis, total turnover, tissue growth)
– ACH (adrenal-cortical hormone) : decreases cell division & subsidiary processes.
– T4 (thyroxine): affects all tissues.– Estrogens: selectively decrease cell division &
subsidiary processes; affect cartilage & lamellar bone.– Vitamins A, C & D & calcitonin
12.6.2 Mechanism for control of remodeling
• Piezoelectricity– Mechanism for bone to sense stress & cause
remodeling– Collagen– Electrical field is capable of activating protein-
synthesizing organelles in osteogenic cells (frog). Electrical field cause tropocollagen alignment.
• Biochemical activity of calcium– Straining bone increases calcium concentration in
interstitial fluid– Change in solubility of HA crystals in response to
stress
Stress-controlled bone development
• Compressive stress stimulates formation of new bone and important factor in fracture healing
• During immobilization, net loss of bone calcium & phosphorous; after resume of normal activity mineral loss phenomena reversed !
• Astronauts subjected to weightlessness has same results: subnormal stresses causes loss of bone strength, radiographic opacity & size.
• Intermittent stress is a morphogenetic stimulus to functional adaptation of bone & effect of compressive stress is same as tensile stress !
• Distribution of material & strength is related to severity of stress in normal activity. Rigid plate fixation in dog yields thinning of femoral diaphysis cortex rather than osteoporosis in cortex !
Bone Remodeling• Bone of the skeleton are continually
remodeled for 2 reasons– Bone remodeling helps maintain constant
concentrations of Ca2+ and PO43- in bodily
fluids– Bones are remodeled in response to the
mechanical stress it experiences• Osteons of compact bone and the trabeculae of
spongy bone are constantly replaced by new osteons and trabeculae that are more precisely aligned with newly experienced compressive and tensile forces

Copyright 2009, John Wiley & Sons, Inc. 61
Factors Affecting Bone Growth and Bone Remodeling
• Normal bone metabolism depends on several factors– Minerals
• Large amounts of calcium and phosphorus and smaller amounts of magnesium, fluoride, and manganese are required for bone growth and remodeling
– Vitamins• Vitamin A stimulates activity of osteoblasts• Vitamin C is needed for synthesis of collagen• Vitamin D helps build bone by increasing the absorption
of calcium from foods in the gastrointestinal tract into the blood
• Vitamins K and B12 are needed for synthesis of bone proteins
medications
• Simvastatin is a lipid lowering agent with osteoanabolic
• effects. Histomorphometric studies have shown increased
• bone ingrowth and mechanical examination, increased interface
• strength, superior stability and osseous adaptation at
• the bone/implant interface in the simvastatin-treated
• group3
Copyright 2009, John Wiley & Sons, Inc. 63
Aging and Bone Tissue • The level of sex hormones diminishes
during middle age, especially in women after menopause.– A decrease in bone mass occurs.– Bone resorption by osteoclasts outpaces
bone deposition by osteoblasts.• Female bones generally are smaller and
less massive than males.– Loss of bone mass in old age has a greater
adverse effect in females.
• Bisphosphonates inhibit osteoclast-mediated bone
• resorption and normalize the high rate of bone turnover that
• characterizes osteoporosis. Consequently, there is a rationale
• for using bisphosphonates to enhance early stability of
• implants in patients with low bone mass30,62,89-
• indomethacin causes a transient
• decrease in attachment strength at early periods, but it
• does not seem to significantly affect long-term osseointegration
• of porous-coated implants98.
• warfarin, Enoxaparin,
• dalteparin and unfractionated heparin led to a significant
• decrease of matrix collagen type II content and calcification
• in concentrations equal or higher than the therapeutic one.
• fondaparinux, a synthetic anticoagulant substance• similar to heparin, showed no inhibitory in vitro• effects on human osteoblasts within the concentration
range• investigated (0.01-100 جg/ml). Therefore, fondaparinux
may• be used to avoid the heparin-related negative influence
on• osteoblast-dependent fracture healing and
endoprosthetic• implant integration99,100.

• radiation therapy seems to delay bone remodeling preand
• post-implantation35,
• Recently, cell-mediated regional• gene therapy was introduced to deliver potent
morphogens• or growth factors in regenerative medicine. Direct
application• of the BMP-2 gene using a liposomal vector enhanced• bone regeneration in a bony defect; gene delivery
combined• with bone grafting could induce rapid osseointegration of• the bone-implant interface at an earlier stage121.
Copyright 2009, John Wiley & Sons, Inc. 70
Aging and Bone Tissue • There are two principal effects of aging on
bone tissue:– Loss of bone mass
• Results from the loss of calcium from bone matrix
• The loss of calcium from bones is one of the symptoms in osteoporosis
– Brittleness• Results from a decreased rate of protein synthesis
• Collagen fibers give bone its tensile strength
• The loss of tensile strength causes the bones to become very brittle and susceptible to fracture
• Meloxicam negatively
• influenced bone healing in the cortical and cancellous
• bone around titanium implants inserted in rats after continuous
• administration
Copyright 2009, John Wiley & Sons, Inc. 72
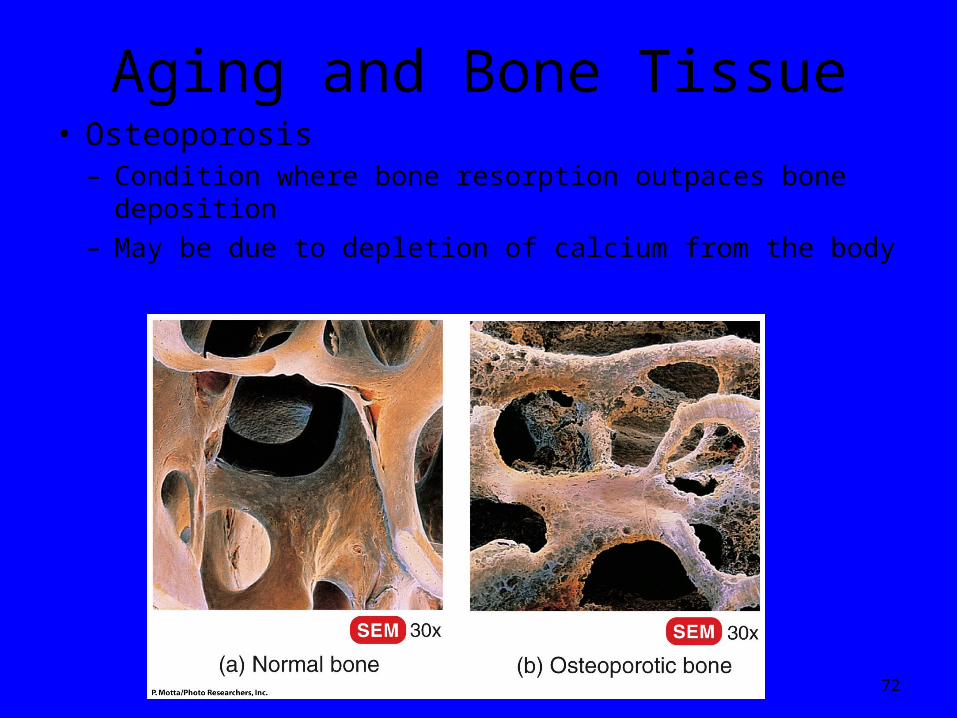
Aging and Bone Tissue• Osteoporosis
– Condition where bone resorption outpaces bone deposition– May be due to depletion of calcium from the body
Copyright 2009, John Wiley & Sons, Inc. 73
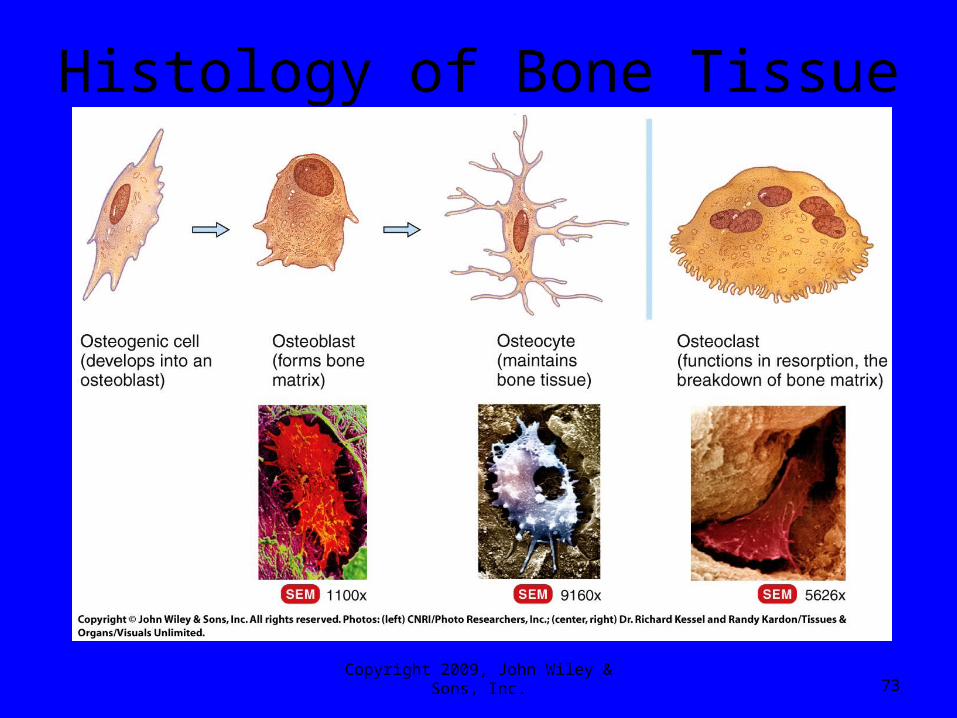
Histology of Bone Tissue

Bone Remodeling• Bone forming osteoblasts form from
mesenchyme-like stem cells located in the periosteum, endosteum, and the connective tissue of nearby bone marrow
• Osteoclasts form in bone marrow from immature blood cells called hematopoietic stem cells
• Many of these stem cells fuse together to form each osteoclast, thus their multinucleate structure
Bone Remodeling• Osteoclasts release calcium ions (Ca2+)
and phosphate ions (PO43-) that enters
the tissue fluid and the bloodstream• Lysosomal enzymes are also released
by the osteoclasts and digest the organic part of the bone matrix
• Finally, osteoclasts take up collagen and dead osteocytes by phagocytosis

Bone Remodeling• The ruffled plasma
membrane forms a tight seal against the bone and HCL dissolves the mineral portion of the matrix
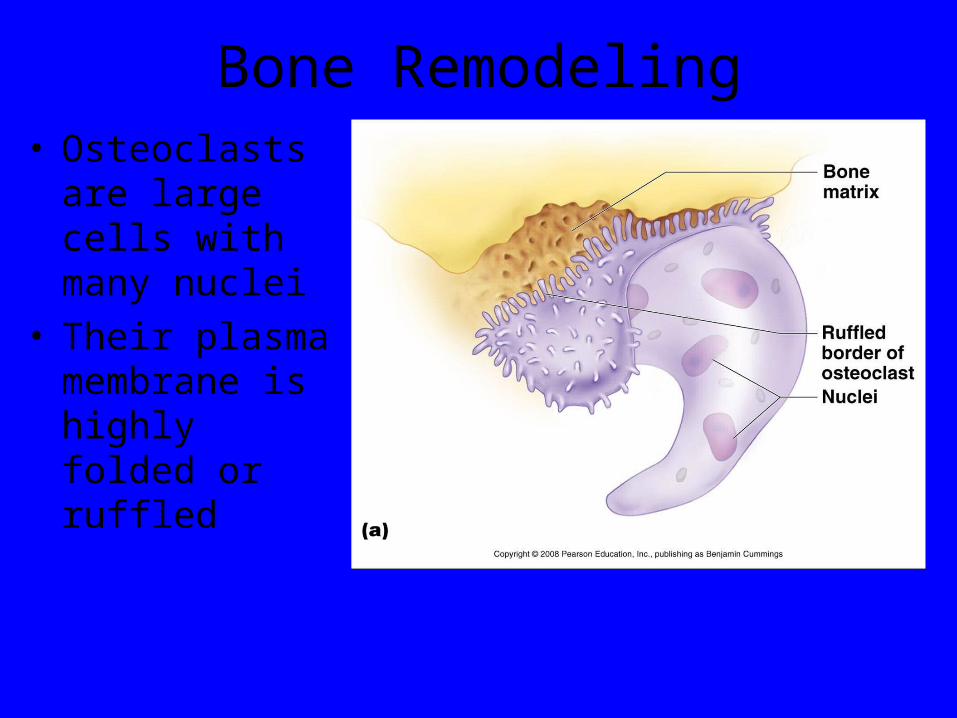
Bone Remodeling• Osteoclasts are
large cells with many nuclei
• Their plasma membrane is highly folded or ruffled
Bone Remodeling
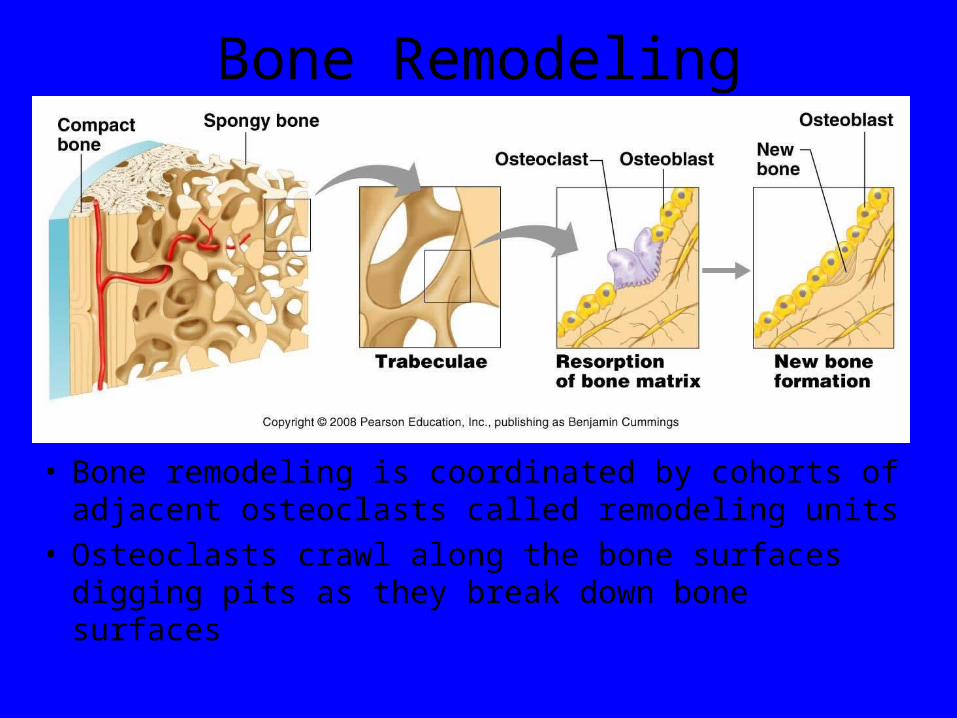
• Bone remodeling is coordinated by cohorts of adjacent osteoclasts called remodeling units
• Osteoclasts crawl along the bone surfaces digging pits as they break down bone surfaces
Bone Remodeling• Bone is dynamic and active tissue
• Long bone growth is accompanied by almost continuous remodeling in order to maintain proper proportions
• Large amounts of bone matrix and thousands of osteocytes are being continually removed and replaced
• The small scale architecture of bones changes constantly
II.Modeling and Remodeling of Bone
• The cellular mechanisms responsible for the adaptation of bone are modeling (construction) and remodeling (reconstruction).
• Bone modeling produces a change in the size and shape of bone when new bone is deposited without previous bone resorption.
• Bone remodeling, resorption by osteoclasts precedes bone formation by osteoblasts.

Bone Remodeling• The spongy bone of the skeleton is
replaced every 3 years
• The compact bone is replaced every 10 years
• The remodeling process is not uniform as some parts experiencing more stress are replaced at a faster rate (every 5-6 months) while other areas change more slowly

Bone as a load sensing tissue
• Bone tissue architecture is influenced by mechanical stresses. This idea was first
• documented by Galilei in 1638 (Galilei 1638) when he suggested that the shape of
• bones is related to loading.
(Wolff 1892),(Frost 1987),
• the• remodeling of bone occurs in response to
physical stresses, and on the other hand,• to the lack of them. Bone develops or adapts its
structure to that most suited to• resist the forces acting upon it (Wolff 1892). In
principle, this means that bone is• deposited in sites subjected to stress and is
resorbed from sites where there is little• stress (Robling et al. 2006).
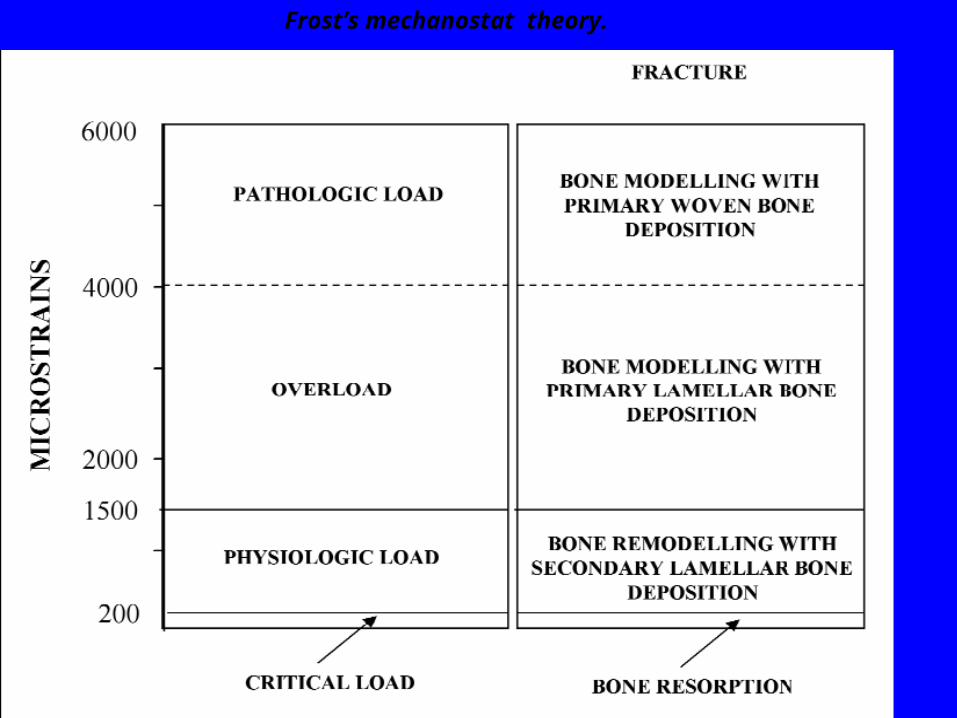
Frost’s mechanostat theory.

Frost’s mechanostat• Disuse:
Strain < circa 800μStrain: Remodeling (bone adaptation and bone repair) Bone mass and bone strength is reduced.
• Adapted State:strain between ca. 800μStrain and ca. 1500μStrain: Remodeling (bone repair) Bone mass and bone strength stays constant
• Overload:Strain > circa 1500μStrain: Modeling (bone growth) bone mass and bone strength his increased
• Fracture:Strain > circa 15000μStrain: maximum elastically deformation excceded - bone fracture.
• a stress diversion design, which promotes bone growth and maturation under normal loading conditions.
• Mechanical stimuli elicit the proliferation of bone
• cells
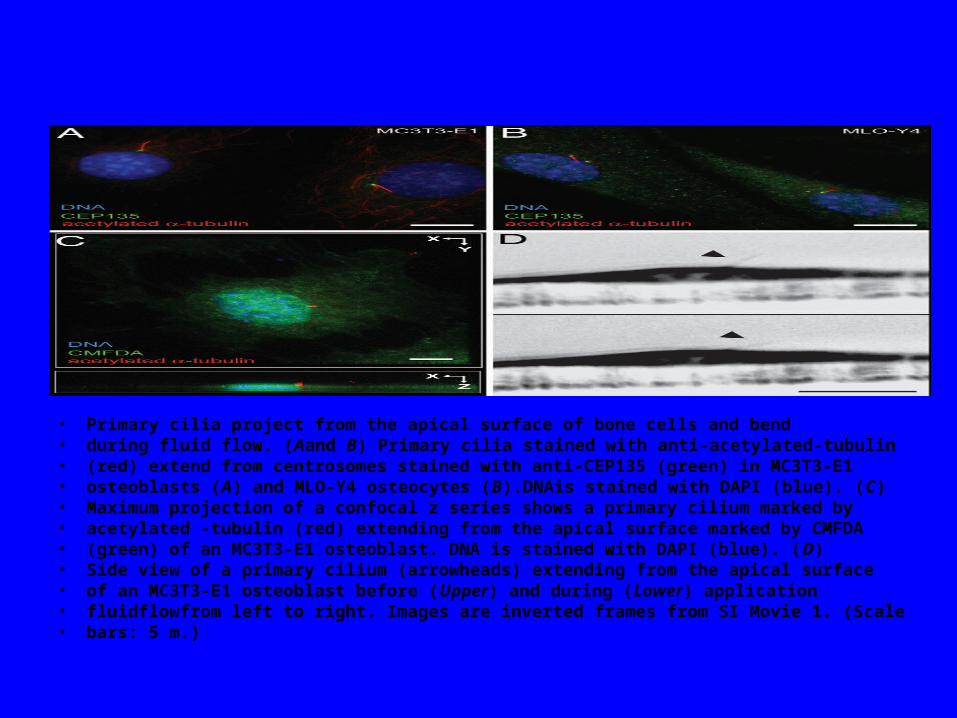
• Primary cilia project from the apical surface of bone cells and bend• during fluid flow. (Aand B) Primary cilia stained with anti-acetylated-tubulin• (red) extend from centrosomes stained with anti-CEP135 (green) in MC3T3-E1• osteoblasts (A) and MLO-Y4 osteocytes (B).DNAis stained with DAPI (blue). (C)• Maximum projection of a confocal z series shows a primary cilium marked by• acetylated -tubulin (red) extending from the apical surface marked by CMFDA• (green) of an MC3T3-E1 osteoblast. DNA is stained with DAPI (blue). (D)• Side view of a primary cilium (arrowheads) extending from the apical surface• of an MC3T3-E1 osteoblast before (Upper) and during (Lower) application• fluidflowfrom left to right. Images are inverted frames from SI Movie 1. (Scale• bars: 5 m.)
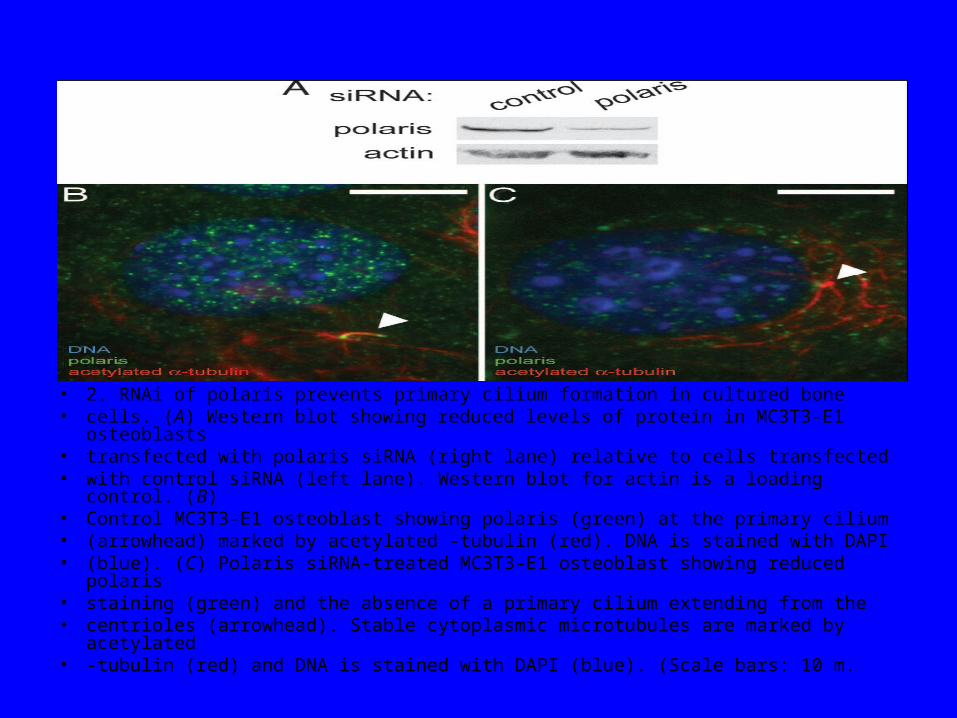
• 2. RNAi of polaris prevents primary cilium formation in cultured bone• cells. (A) Western blot showing reduced levels of protein in MC3T3-E1 osteoblasts• transfected with polaris siRNA (right lane) relative to cells transfected• with control siRNA (left lane). Western blot for actin is a loading control. (B)• Control MC3T3-E1 osteoblast showing polaris (green) at the primary cilium• (arrowhead) marked by acetylated -tubulin (red). DNA is stained with DAPI• (blue). (C) Polaris siRNA-treated MC3T3-E1 osteoblast showing reduced polaris• staining (green) and the absence of a primary cilium extending from the• centrioles (arrowhead). Stable cytoplasmic microtubules are marked by acetylated• -tubulin (red) and DNA is stained with DAPI (blue). (Scale bars: 10 m.
PRNCIPLES OF DENTAL IMPLANT DESIGN
A) Gain initial stability that would reduce the threshold for the ‘tolerated micromotion’ and minimize the waiting-period required for loading the implant.
B) Incorporate design factors,that would diminish the effect of shear forces on the interface (such as surface roughness related and thread features) so that marginal bone is preserved).
C) Design features that maystimulate bone formation, and/ or facilitate bone healing (secondary osseointegration).

Factors concerning implant design which affect the stressdistribution to the periimplant bone of loaded dental implants.
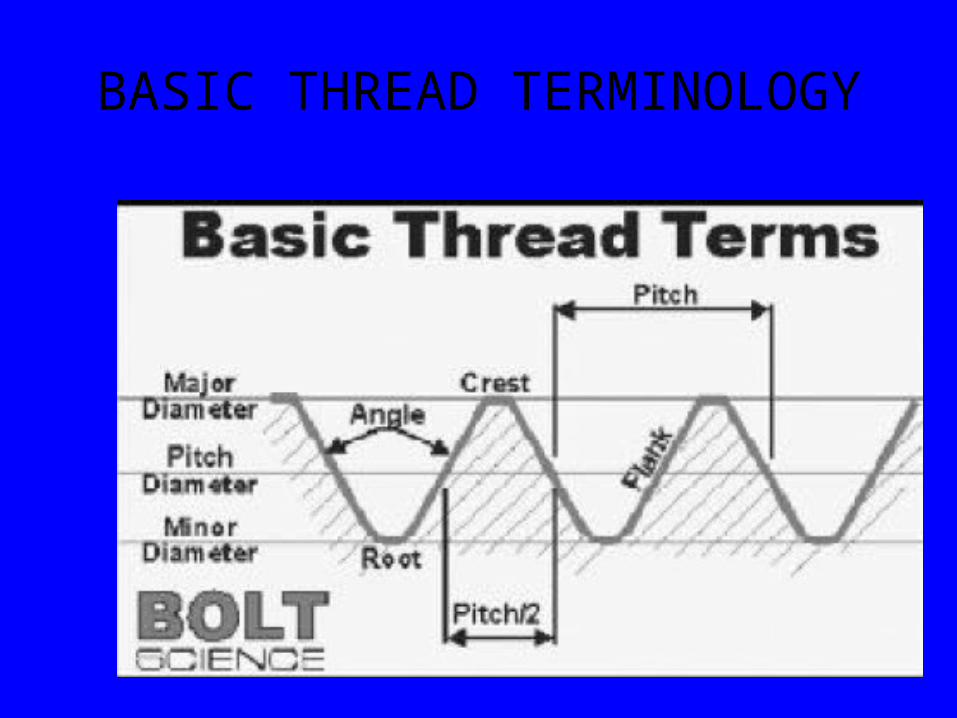
BASIC THREAD TERMINOLOGY



BONE REMODELING SUBSEQUENT TO ABUTMENT
CONNECTION
Figure 1. Illustrates 1.5 to 2 mm of crestal bone loss from implant-abutment interface.
. Illustrates 1.5 to 2 mm of crestal bone loss from implant-abutment interface.

• 1) The rough/smooth border on 1-piece nonsubmerged implants determines the initial bone-to-implant contact.
• (2) In 2-piece implants, the first bone-to-implant contact was located 1.5 to 2 mm apical to the microgap between the 2 pieces (Figure 1).7
• (3) Osseous changes occur after the creation of a microgap at the implant-abutment interface.
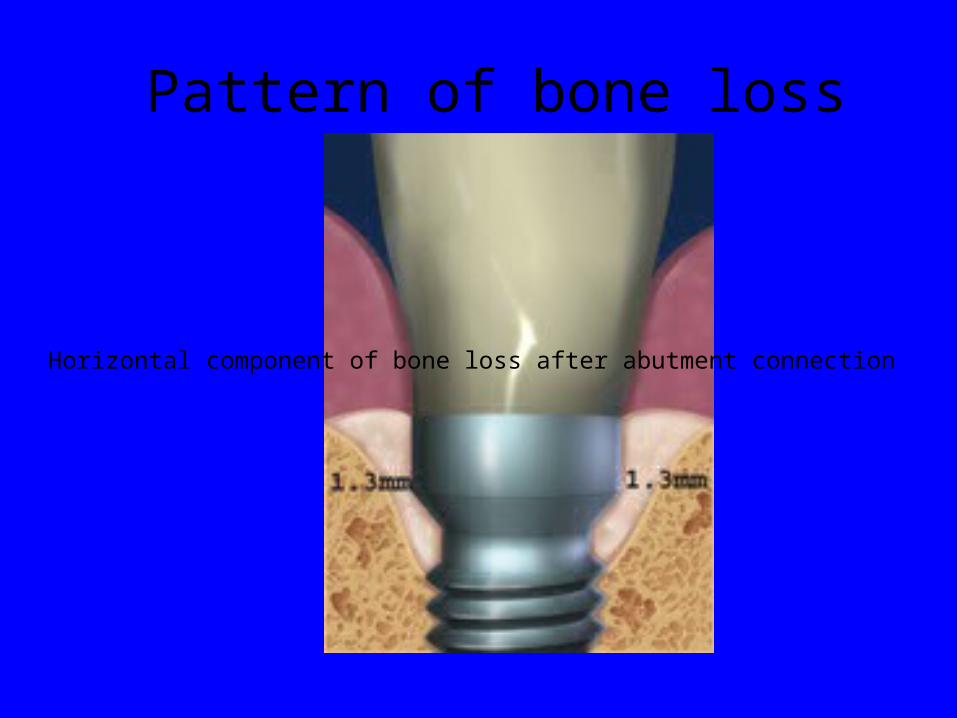
Pattern of bone loss
Figure 2. Horizontal component of bone loss after abutment connection
Horizontal component of bone loss after abutment connection
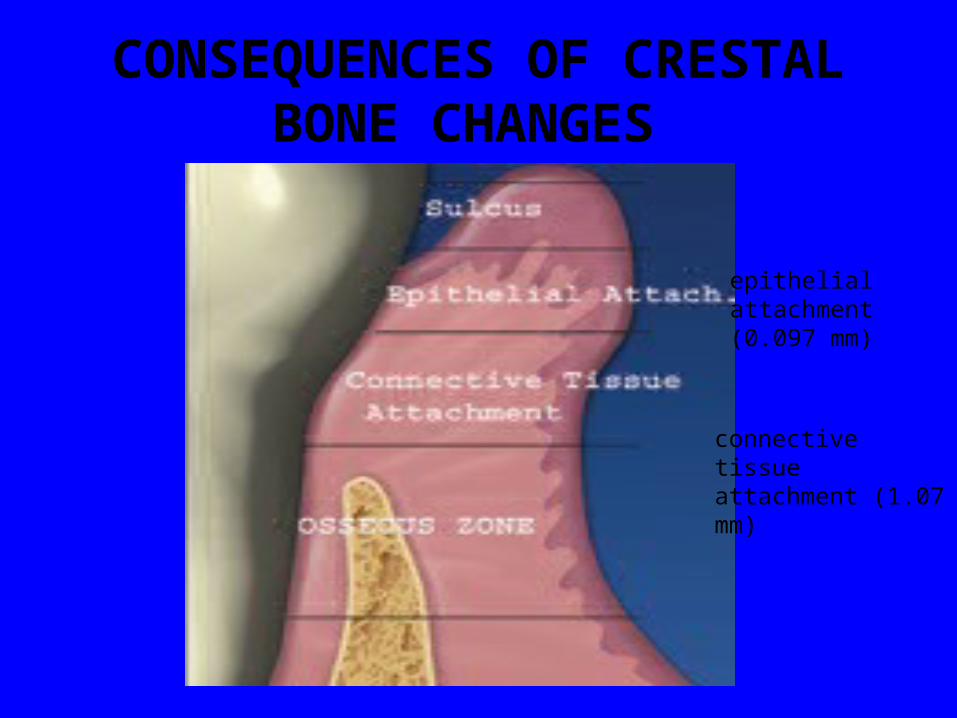
CONSEQUENCES OF CRESTAL BONE CHANGES
Figure 3. The components of biologic
epithelial attachment (0.097 mm)
connective tissue attachment (1.07 mm)
The dentogingival and peri-implant complexes
• similar in their cellular composition, • keratinized oral epithelium and nonkeratinized
junctional epithelium.9 Histologically, • differences • the attachment of the junctional epithelium to
teeth is mediated by glycoproteins, • a pseudo-attachment via hemidesmosomes
exists around endosseous implants • connective tissue fibers mechanically insert into
root cementum • a tight cuff is formed around titanium implants.
• The interproximal height of bone (IHB) has a distinct influence on interdental papillae
• mean papilla length for an implant-tooth relationship was found to be 6.5 mm;
• for an implant-implant relationship the mean papilla length was 4.5 mm.
• Adequate interdental soft tissue depends on the height of the interproximal bone and its relation to the contact point
• When the distance from the contact point to the interproximal height of bone is greater than 5 mm, avoiding the “black triangle” is difficult
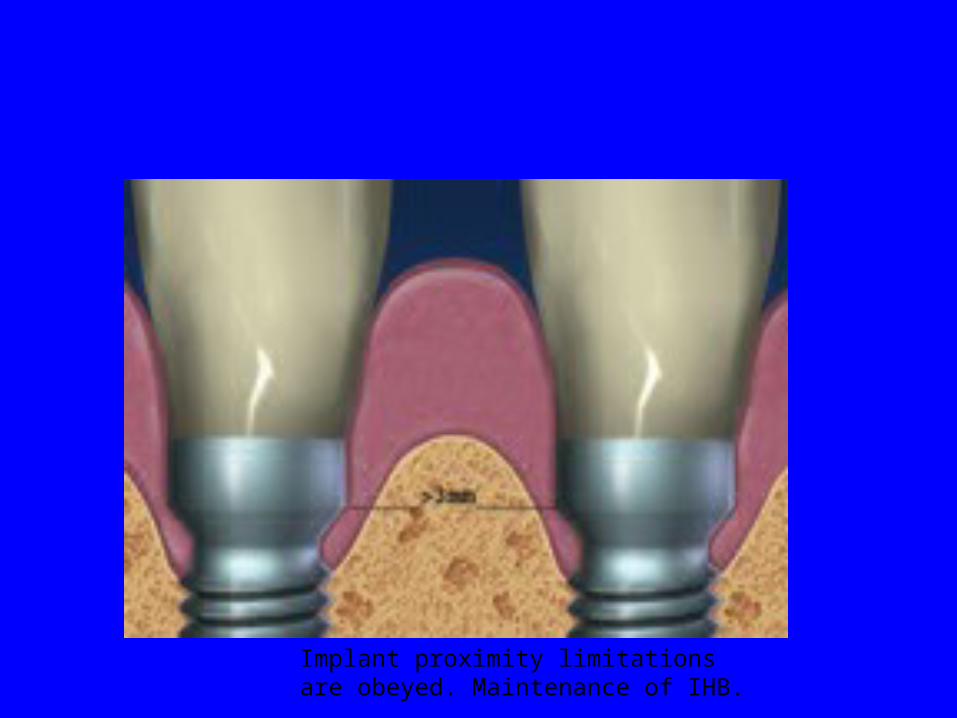
Implant proximity limitations are obeyed. Maintenance of IHB.
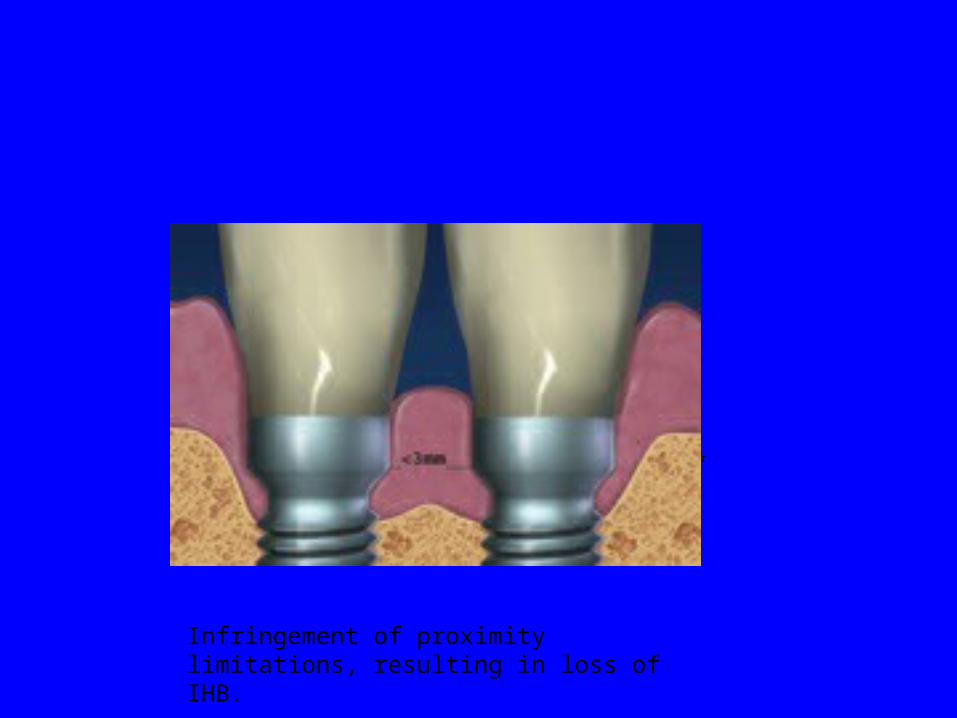
Figure 4. Implant proximity limitations are obeyed. Maintenance of IHB.
Figure 5. Infringement of pr
Infringement of proximity limitations, resulting in loss of IHB.
• If proximity guidelines were not obeyed when placing the implant next to an adjacent implant (3 mm) or tooth (1.5 mm), then interproximal bone will be insufficient to support papilla formation (and a “black triangle” may be evident.
•
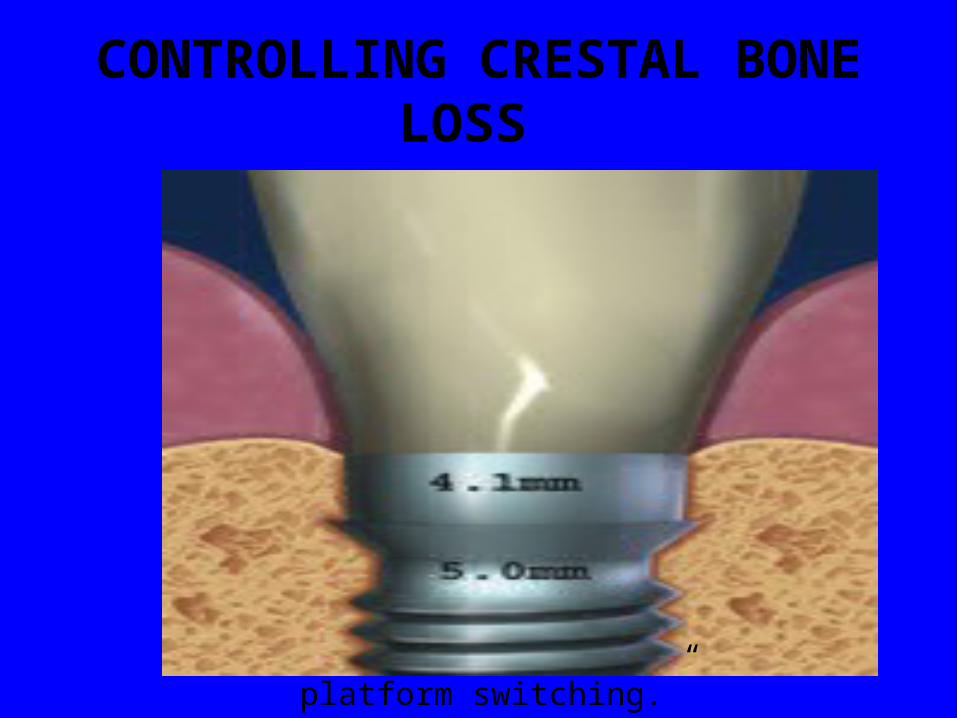
CONTROLLING CRESTAL BONE LOSS
Figure 7.
platform switching.”
• Use of nonsubmerged implants to eliminate bone loss is a proven way to accomplish this
• A scalloped implant platform has been developed to follow the osseous architecture and eliminate crestal bone loss by maintaining the microgap in a supracrestal position
• medializing the position of the microgap, ie, using a smaller abutment. “platform switching.”
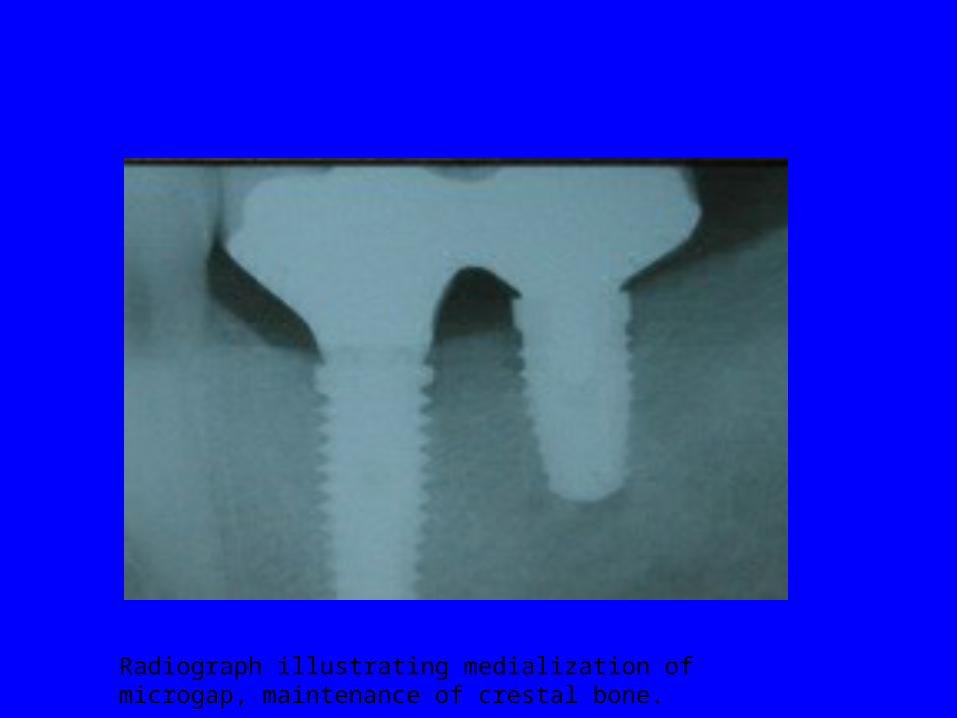
Radiograph illustrating medialization of microgap, maintenance of crestal bone.
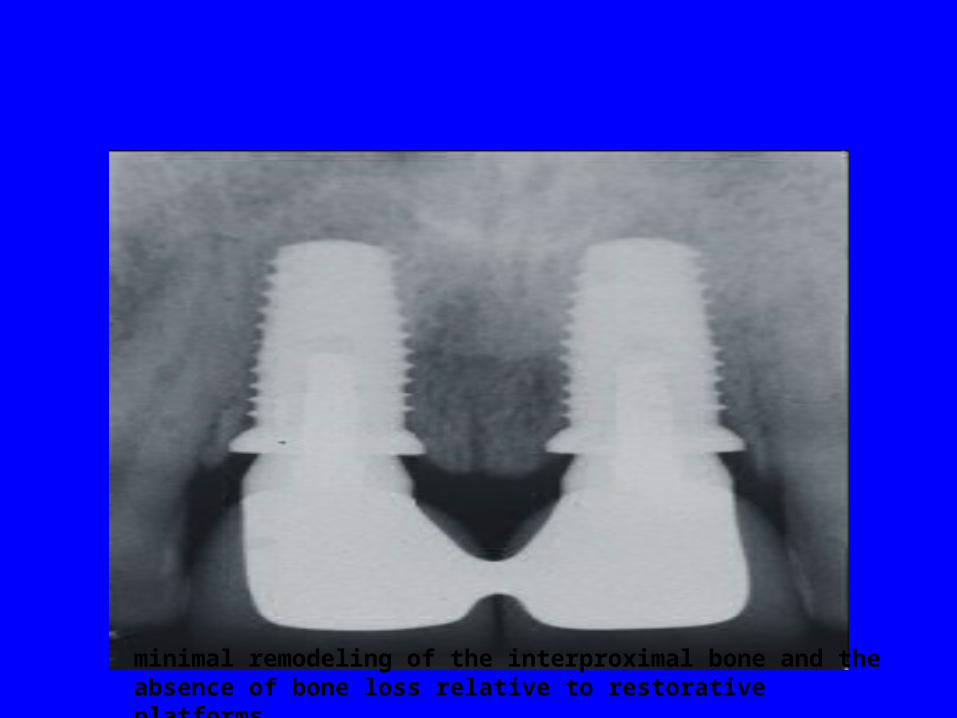
minimal remodeling of the interproximal bone and theabsence of bone loss relative to restorative platforms.

Radiograph at abutment connection, three daysafter implant placement. The implant restorative platformsof the abutments and implants are subcrestal.
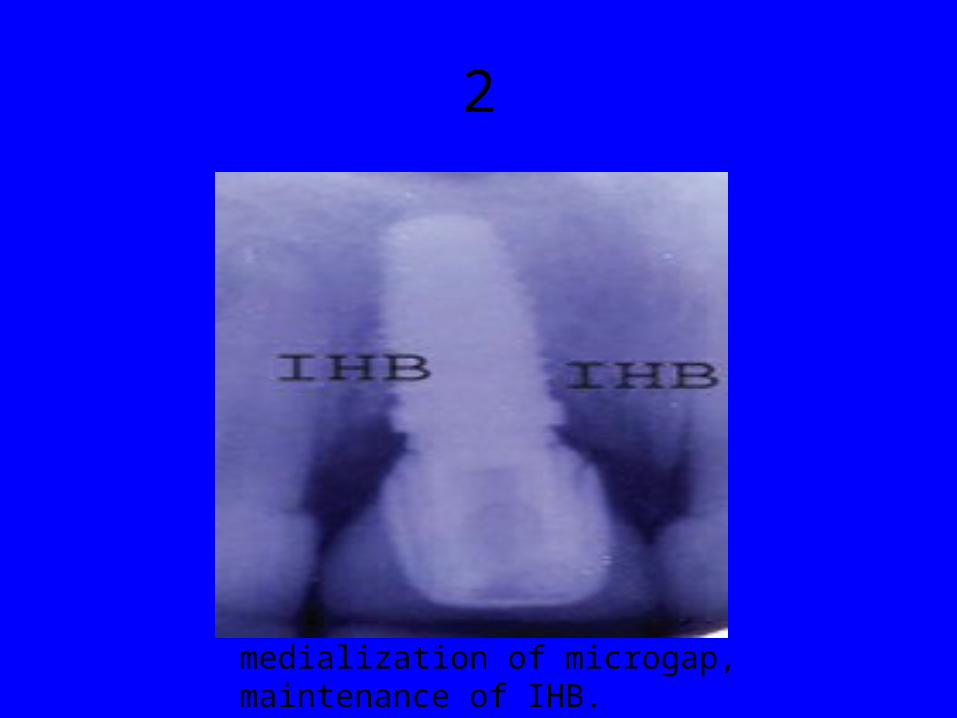
2
medialization of microgap, maintenance of IHB.

platform switching in posterior maxilla. Note maintenance of bone

Implant restoration of central incisor. Note maintenance of soft-tissue contours.