Embed Size (px)
Citation preview

New Currents in Treatment of Bone Metastases: A Case-Based Approach
For additional
updates, go to
www.projectsinknowledge.com
There is no fee for this activity.
Part 2 of a 5-Part Series
Release Date: September 8, 2003. Termination Date: December 31, 2004. Estimated time for completion of thisnewsletter/audio CD: 1 hour
Part 2 of 5: Bone Metastases in Breast Cancer
Download this 5-part series—New Currents in Treatment
of Bone Metastases: A Case-Based Approach—
available atwww.projectsinknowledge.com/oncol/
Dear Colleague:
Bone is the most common site of metastasis in patients with breast cancer.An estimated 211,300 women will develop breast cancer in the United States this year, according to the American Cancer Society. About half of all women diagnosed with breast cancer develop bone metastases. Skeletalcomplications of bone metastases are common and can substantially erodethe patient’s quality of life. Part 2 of New Currents in Treatment of BoneMetastases: A Case-Based Approach uses the case of a typical patient withbreast cancer and bone metastases to evaluate the best approach to preventingskeletal complications.
This 5-part series opened with an overview of bone metastases andbisphosphonates (Part 1), and continues here with the first of four case-based discussions (Parts 2–5) of the use of bisphosphonates in treatingskeletal complications of breast, lung, prostate, and renal cancers. This allows an in-depth look at specific patient populations and providesinformation on applying the data on bisphosphonates to actual clinicalpractice.
Each issue in this 5-part series consists of a Tx Reporter newsletter, an audioCD featuring an interview with expert faculty on related issues, and a recentreprint with information that has largely determined the current standard ofcare. These issues focus on the next generation of bisphosphonate therapy.However, fair balance is critical to this discussion, and the faculty and I alsopresent data on other bisphosphonates.
I hope that you enjoy the series and find it helpful and informative.
Yours truly,
ChairJames R. Berenson, MD
Chief Executive OfficerInstitute for Myeloma and
Bone Cancer ResearchLos Angeles, California
& Ask the Experts" Audio Edition"
James R. Berenson, MD
Allan Lipton, MD
This Tx Reporter series discusses theuse of bisphosphonates to help preventskeletal-related events in patients withbone metastases from solid tumors.This second issue includes the case ofa 78-year-old woman who developsbreast cancer that metastasizes tobone. This continuing professionaleducation activity also includes the enclosed audio CD, in which Dr. Lipton discusses:
• Factors that contribute to bone lossin breast cancer patients
• Use of bone mineral density testingto evaluate bone loss, and imaging to detect bone metastases
• Prognosis of patients with breastcancer metastases to bone, including survival and risk of skeletal complications
• Mechanisms of bisphosphonates in preventing skeletal complicationsin breast cancer patients
• Efficacy and safety of various bisphosphonates in breast cancerpatients with bone metastases
• Studies on adjuvant use of bisphos-phonates to prevent bone metastasesin breast cancer patients
FacultyAllan Lipton, MD
Professor of Medicine/OncologyPenn State UniversityMilton S. Hershey Medical CenterHershey, Pennsylvania
1657-TxReporter2of5-BB11-11 11/11/03 5:34 PM Page 1

R E P O R T E RSM : O N C O L O G Y
2
Copyright © 2003, Projects In Knowledge, Inc.Little Falls, NJ 07424. All rights reserved.
Target AudienceThis activity is designed for oncologists and oncologic healthcareprofessionals who treat patients with bone metastases.
Activity GoalThe goal of this activity is to provide an overview of bone metas-tases and the latest developments in preventing related skeletalcomplications using bisphosphonate therapies.
Learning ObjectivesAfter completing this activity, the participant should be able to:• Review the incidence of bone metastases among patients with
metastatic cancer, including multiple myeloma, breast, prostate,lung, kidney, thyroid, and other solid tumors.
• Describe the complications caused by bone metastases in the clinical management of various solid tumors.
• Examine the mechanisms of action of bisphosphonates and theirrole in improving bone strength and inhibiting malignant cellfunction.
• Discuss the safety and efficacy of currently available agents andnext generation bisphosphonates.
• Consider the use of intravenous therapy in the treatment armamentarium to delay and reduce skeletal complications ofbone metastases in patients with multiple myeloma, breast,prostate, lung, kidney, thyroid, and other solid tumors.
• Describe appropriate techniques for administration of intravenousbisphosphonates.
• Improve quality of life for patients with bone metastases.
Statement of AccreditationProjects In Knowledge is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians.
Credit DesignationProjects In Knowledge designates this educational activity for amaximum of 1 category 1 credit toward the AMA Physician’sRecognition Award. Each physician should claim only those creditsthat he/she actually spent in the activity.To receive documentation of your participation in this newsletter/CDactivity, you must achieve a passing score of 70% or higher on theposttest. Full instructions for submission are included on the posttest.
CPE InformationProjects In Knowledge is accredited by the American Councilon Pharmaceutical Education (ACPE) as a provider of continuing pharmaceutical education. This activity has been
planned and implemented in accordance with the ACPE Criteria forQuality and Interpretive Guidelines. The ACPE Universal ProgramNumber assigned to this program, for 1 contact hour (0.1 CEU), is 052-000-03-054-H01.
CE InformationThe National Center for Advanced Medical Education (a division ofCMEinfo.com) is accredited as a provider of continuing nursing edu-cation by the American Nurses Credentialing Center’s Commission onAccreditation. The National Center for Advanced Medical Education(a division of CMEinfo.com) designates this educational activity for1.2 contact hours. Provider approved by the California Board ofRegistered Nursing, Provider Number 13776 for 1.2 contact hours.
Disclosure InformationThe Disclosure Policy of Projects In Knowledge and The NationalCenter for Advanced Medical Education (a division of CMEinfo.com)requires that faculty participating in a CME/CPE/CE activity disclose to the audience: any significant relationship they may havewith a pharmaceutical or medical equipment company, product, orservice that may be mentioned as part of their presentation; anyrelationship with the commercial supporter of this activity; whetherany drugs or products under discussion are unapproved for use orinvestigational, ongoing research, or preliminary data.James R. Berenson, MD, has received grant/research support fromAmgen Inc, Chugai Pharmaceuticals Company, MillenniumPharmaceuticals, Inc, and Novartis Pharmaceuticals Corporation.Susan Bove, MSN, APRN, BC, has no significant relationships withindustry. Allan Lipton, MD, is on the speakers bureau of and is astock shareholder in Novartis Pharmaceuticals Corporation. ChristineWilson, PhD, APRN, BC, NP-C, is on the speakers bureau of Bristol-Myers Squibb Company; and is a stock shareholder in Pfizer Inc.The opinions expressed during this activity are those of the facultyand do not necessarily reflect those of Projects In Knowledge, TheNational Center for Advanced Medical Education (a division ofCMEinfo.com), or the commercial supporter.This independent CME activity is planned and implemented in accordance with the ACCME Essential Areas and Policies.This CME/CPE activity is provided by Projects In Knowledge, and the CE activity is provided by The National Center for AdvancedMedical Education (a division of CMEinfo.com) solely as an educa-tional service. Please note that although faculty will discuss specifictreatment modalities, neither Projects In Knowledge, the accreditedand approved CME provider, nor The National Center for AdvancedMedical Education (a division of CMEinfo.com), the accredited andapproved CE provider, nor their CME/CE regulatory bodies, includingthe ANCC, endorse any of the modalities mentioned in the course ofdiscussion. Specific patient care decisions are the responsibility of thehealthcare professional caring for the patient.This independent CME/CPE/CE activity is supported by an unrestricted educational grant from Novartis PharmaceuticalsCorporation.Nurse Planner: Christine Wilson, PhD, APRN, BC, NP-C, Visiting AssistantProfessor, University of South Florida, Tampa, Florida. NurseReviewer: Susan Bove, MSN, APRN, BC, Private Practice, Reading,Massachusetts.
Case DescriptionMs. R, a 78-year-old Caucasian womanwho is a retired nurses’ aide, presentedin January 2002 with low back pain.Her past medical history included mildhypertension and surgery for a brainaneurysm. Family history included a mother with breast cancer at age 56 years and a brother with lung cancer. Ms. R has smoked cigarettes for50 years. She does not drink alcohol.
On examination, a mass in the upperouter quadrant of her right breast was found. Physical examination wasotherwise negative. Mammography was positive for malignancy. Ms. Runderwent a right partial mastectomyand was determined to have a 4-cminfiltrating duct cancer with 2/12positive lymph nodes. Her tumor wasfound to be positive for estrogen andprogesterone receptors and negative forHER-2/neu. Computed tomography scanof the chest and abdomen was negative,but bone scan revealed multiplemetastases in her spine, pelvis, and ribs.
Shortly thereafter, she reported low back pain rated as 7 out of 10 on visual analog scale. She was started onnarcotics (morphine sulfate 30 mg BID).
Initiating TreatmentQuestion 1: What treatment would yourecommend at this point?
a. Hormone therapy alone
b. Hormone therapy plus strontium-89
c. Hormone therapy plus pamidronate
d. Hormone therapy plus zoledronic acid
Discussion(d) Hormone therapy plus zoledronicacid is the most appropriate treatmentoption for this patient.
Hormone therapy is indicated asprimary treatment because Ms. R hasestrogen- and progesterone-receptor–positive breast cancer. Because she
also has multiple bone metastases,additional treatment is necessary toprevent skeletal complications, such as pathologic fractures, spinal cordcompression, or hypercalcemia. Aretrospective study of 718 unselectedwomen diagnosed with metastaticbreast cancer at Massachusetts GeneralHospital in Boston, between 1981 and1991, found that more than halfdeveloped skeletal complications. Ofthose with complications, about halfhad more than one.1 Surgery andradiation are often needed to treat orprevent pathologic fractures. Thus,hormone therapy alone would leave this patient at considerable risk formorbidity and mortality.
Strontium-89 has been found to beeffective in palliating bone pain inpatients with breast cancer.2,3 Pain relief has been reported as “good” in60% of patients and “partial” in 32%.Duration of pain relief ranges from 2 to 14 months.3 Retreatment produces agood response in up to 83% of cases,but with shorter duration.2 Unlikebisphosphonates, strontium-89 does notinhibit bone resorption and thereforedoes not affect disease progression.Thus, while strontium-89 may palliatebone pain, bisphosphonates are apreferred therapy because they inhibitbone resorption, thereby reducing the associated clinical complications.Moreover, strontium-89 has myelo-suppressive effects that can impairquality of life and compromise thepatient’s ability to tolerate chemo-therapy. Platelet and white blood cellcounts generally return to baselinelevels within 12 weeks afteradministration.3
Pamidronate was the firstbisphosphonate approved for thetreatment of bone metastases in the United States. The 1996 Food and Drug Administration approval was based on data from two large,multicenter, phase III studies in which
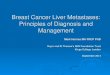
Table 1. Pamidronate Versus Placebo in Women with Breast Cancer Metastatic toBone: Two Randomized, Phase III Studies
Chemotherapy (Protocol 19)4 Hormone Therapy (Protocol 18)5
Pamidronate Placebo Pamidronate Placebo
n 185 195 182 189
Proportion withSRE at
12 months 43% 56% 47% 57%
Time to first SRE (months) 13.1 7.0 10.4 6.9
SRE = skeletal-related event
1657-TxReporter2of5-BB11-11 11/11/03 5:34 PM Page 2

3
TREATMENT REPORTER New Currents in Treatment of Bone Metastases: A Case-based Approach
breast cancer and myeloma patientswere given 90 mg of pamidronateintravenously or placebo Q3–4wk inconjunction with hormonal therapy in one study and chemotherapy in the other. Long-term (24-month) data from both studies indicated that pamidronate resulted in asignificantly lower incidence of skeletalcomplications (51% versus 64% withplacebo; P < .001). Pamidronate alsoprolonged the time to first skeletalcomplication (12.7 versus 7 months; P < .001). Results were similarregardless of whether patients werereceiving chemotherapy or hormonetherapy (Table 1).4,5 Patients in thepamidronate group had less pain andrequired less analgesia than did patientsgiven placebo.6
Zoledronic acid is the most potentbisphosphonate currently available andis 87- to 940-fold more potent thanpamidronate in preclinical models ofosteoclast-mediated bone resorption.7A double-blind, phase III comparativetrial of zoledronic acid and pamidronatein advanced breast cancer and myelomapatients established zoledronic acid asthe standard of care in this population.In this study, 1646 patients with stageIII multiple myeloma or breast cancerand at least one bone metastasis were randomized to either 4 or 8 mg of zoledronic acid or 90 mg ofpamidronate Q3–4wk for 12 months.Zoledronic acid was initially given as a5-minute infusion, but the protocol wassubsequently changed to a 15-minuteintravenous infusion due to renal safetyconcerns; pamidronate was given as a2-hour intravenous infusion. Concernsover renal safety at the higher dose of zoledronic acid resulted in an addi-tional protocol amendment switchingpatients in this arm to 4 mg. Mostparticipants (81%) were also receivingchemotherapy.
During 13 months of follow-up, nearlyhalf of all patients experienced skeletal-related events (SREs), with similar rates in both treatment arms (Table 2).Median time to first SRE was alsosimilar in both treatment groups. Bothdrugs were similarly effective inrelieving pain and reducing the needfor analgesics. However, significantlyfewer zoledronic acid patients receivedpalliative radiation to bone both overall(15% versus 20%; P = .031) and amongbreast cancer patients receivinghormone therapy (16% versus 25%; P = .022). Moreover, the mean skeletal
morbidity rate for all SREs, includinghypercalcemia of malignancy, waslower with zoledronic acid than with pamidronate (1.113 versus 1.47 events/y; P = .018). The level of N-telopeptide, a marker of boneresorption, was reduced to a greaterextent by zoledronic acid than bypamidronate at every time pointstudied.8
Twenty-five month final analysis ofsafety and efficacy from this study wasrecently published in Cancer. Theextension phase included 606 patients(<40% of the original population) whoextended their double-blind treatmentfor an additional year after the first 13-month core phase described above.A similar proportion of patients in eachtreatment group experienced an SREother than hypercalcemia: 47% for 4 mg zoledronic acid versus 51% forpamidronate. When individual types of SREs were looked at separately, the proportion of affectedpatients wasconsistently lowerwith zoledronic acid, and thedifference wassignificant forpatients requiringradiotherapy tobone (19% withzoledronic acidversus 24% withpamidronate; P = .037). Time to first SRE wascomparable withboth treatmentsin the study pop-ulation overall,multiple myelomapatients, and inchemotherapy-treated breast
cancer patients, but was significantlyextended with zoledronic acid inhormone therapy–treated breast cancerpatients (415 versus 370 days forpamidronate; P = .047). Zoledronic acid reduced the skeletal morbidity rateby 25% compared with pamidronate(1.04 versus 1.39 events/y, respectively).Anderson-Gill multiple event analysisshowed that, compared with
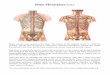
pamidronate, zoledronic acid reduced the risk of developing a skeletal complication by an additional16% overall (P = .030), 20% in allbreast cancer patients (P = .025), and 30% among breast cancer patients treated with hormone therapy(P = .009) (Fig. 1). No differences were found between treatments with regard to median survival andperformance status scores. Most adverse events were mild to moderateand managed easily with supportivetherapy. There were no differences
Table 2. Proportion of Patients with any SRE (without HCM) by Stratum and TreatmentGroup at Month 13 (Intent-to-Treat Analysis)
Stratum Zoledronic Acid Zoledronic Acid Pamidronate (4 mg) (8/4 mg) (90 mg)
Multiple myeloma 47% (86/183) 49% (79/160) 49% (82/167)
Breast cancer chemotherapy 44% (79/178) 47% (80/172) 43% (78/181)
Breast cancer hormonal therapy 42% (83/200) 43% (83/192) 47% (97/207)
Total 44% (248/561) 46% (242/524) 46% (257/555)HCM = hypercalcemia of malignancy; SRE = skeletal-related eventReprinted from Rosen et al.8 “Zoledronic acid versus pamidronate in the treatment of skeletal metastases in patients withbreast cancer or osteolytic lesions of multiple myeloma: a phase III, double-blind, comparative trial,” 2001, Jones and BartlettPublishers, Sudbury, MA, www.jbpub.com. Reprinted with permission.
Figure 1. Relative Risk Ratios for Skeletal-Related Events(Including Hypercalcemia of Malignancy) in PatientsTreated With 4 mg Zoledronic Acid Versus 90 mgPamidronate: 25-Month Follow-up Data.
Reprinted from Rosen et al.9 Copyright © 2003 American Cancer Society. Reprinted by permission of Wiley-Liss, Inc, a subsidiary of John Wiley & Sons, Inc.
.593Multiplemyeloma
Breastcancer
Total
Hazard ratio (4 mg zoledronic acid vs pamidronate)
0 0.2 0.4 0.6 0.8 1 1.2 1.4 1.81.6 2
In favor of zoledronic acid In favor of pamidronate
P value
.025
.030
1657-TxReporter2of5-BB11-11 11/11/03 5:34 PM Page 3

in incidence of serious adverse eventsor renal safety between treatmentgroups.9
Case ContinuesMs. R was treated with zoledronic acid 4 mg IV infused for 15 minutes.One month later, in March 2002, shereported that her back pain haddecreased to a level of 3/10 on thevisual analog scale. Zoledronic acid was continued Q3–4wk, and hormonetherapy was started with letrozole 2.5 mg/d. By June 2002, she reportedthat she no longer had back pain anddiscontinued narcotics. She experiencedslight nausea with treatment, but wasotherwise tolerating it well. Bone scanwas repeated and showed no change. InJanuary 2003, Ms. R fractured her leftfemur while walking in her backyard.Ms. R had sudden onset of pain in her left upper hip. Further radiologicevaluation showed her to have a newfracture of the left femur.
After an SREQuestion 2: Would you continuebisphosphonate therapy?
a. Yes
b. No
Discussion(a) Bisphosphonate therapy should becontinued after an SRE.
In the phase III clinical trial ofzoledronic acid and pamidronate,bisphosphonate therapies werecontinued for 2 years regardless of theoccurrence of SREs. Bisphosphonatesmay also delay or prevent subsequentevents, as suggested by Anderson-Gillmultiple events analysis, whichprovides a robust hazard ratio thattakes into account cumulative totalnumber of events experienced as wellas time between events. As notedabove, 25-month Anderson-Gillmultiple events analysis of zoledronicacid versus pamidronate found thatbreast cancer patients receivingzoledronic acid had a significant 20% lower risk for development of an SRE compared with patients in the pamidronate group (P = .025).9
A preliminary report by Gleason et al10
also suggests a benefit to continuingtreatment after a first SRE. Theyconducted a retrospective analysis ofskeletal complications occurring after a first SRE in a randomized, placebo-controlled study of patients withprostate cancer metastases to bone.Second SREs occurred in 21% of thosetreated with zoledronic acid versus 31% of placebo-treated patients (P = .017)—a 32% relative reduction.The annual SRE incidence decreasedfrom 0.80 event/y with placebo to 0.47 event/y with zoledronic acid.Multiple event analysis indicated a 40% reduction in the risk of subsequent
SREs with continued zoledronic acidversus placebo (P = .011).
Case ContinuesMs. R underwent surgical treatment for the left femur followed by a courseof local radiologic therapy. Ms. Rcontinued on zoledronic acid. Letrozole was discontinued.
ConclusionThe standard of care for patients with breast cancer metastatic to theskeleton is either hormone therapy or chemotherapy coupled with abisphosphonate. Zoledronic acid hasbeen shown to be at least as effectiveas pamidronate, the previous standardof care, in reducing the overall risk of skeletal complications. Similar ratesof SREs occurred with both therapies in a randomized, phase III trial, butmultiple-event analysis suggests a 20%lower risk of an SRE among breastcancer patients treated with zoledronicacid. Administration of zoledronic acidis also more convenient for patients,because it requires a 15-minute ratherthan 2-hour infusion.
In this patient, zoledronic acid was welltolerated and contributed to a decreasein pain during the course of her care.Zoledronic acid was continued after the femoral fracture, and likely willresult in fewer total SREs during Ms. R’s life span.
4
References
1. Domchek SM, Younger J, Finkelstein DM, Seiden MV. Predictors of skeletal complications in patients with metastatic breastcarcinoma. Cancer. 2000;89:363-368.
2. Fuster D, Herranz D, Vidal-Sicart S, et al. Usefulness of strontium-89 for bone pain palliation in metastatic breast cancer patients.Nucl Med Commun. 2000;21:623-626.
3. Sciuto R, Festa A, Pasqualoni R, et al. Metastatic bone pain palliation with 89-Sr and 186-Re-HEDP in breast cancer patients.Breast Cancer Res Treat. 2001;66:101-109.
4. Hortobagyi GN, Theriault RL, Porter L, et al. Efficacy of pamidronate in reducing skeletal complications in patients with breastcancer and lytic bone metastases. Protocol 19 Aredia Breast Cancer Study Group. N Engl J Med. 1996;335:1785-1791.
5. Theriault RL, Lipton A, Hortobagyi GN, et al. Pamidronate reduces skeletal morbidity in women with advanced breast cancer andlytic bone lesions: a randomized, placebo-controlled trial. Protocol 18 Aredia Breast Cancer Study Group. J Clin Oncol.1999;17:846-854.
6. Lipton A, Theriault RL, Hortobagyi GN, et al. Pamidronate prevents skeletal complications and is effective palliative treatment inwomen with breast carcinoma and osteolytic bone metastases: long term follow-up of two randomized, placebo-controlled trials.Cancer. 2000;88:1082-1090.
7. Green JR, Müller K, Jaeggi KA. Preclinical pharmacology of CGP 42’446, a new, potent, heterocyclic bisphosphonate compound. J Bone Miner Res. 1994;9:745-751.
8. Rosen LS, Gordon D, Kaminski M, et al. Zoledronic acid versus pamidronate in the treatment of skeletal metastases in patientswith breast cancer or osteolytic lesions of multiple myeloma: a phase III, double-blind, comparative trial. Cancer J. 2001;7:377-387.
9. Rosen LS, Gordon D, Kaminski M, et al. Long-term efficacy and safety of zoledronic acid compared with pamidronate disodium in the treatment of skeletal complications in patients with advanced multiple myeloma or breast carcinoma: a randomized,double-blind, multi-center, comparative trial. Cancer. 2003;98:1735-1744.
10. Gleason D, Saad F, Goas A, Zheng M. Continuing benefit of zoledronic acid in preventing skeletal complications after the firstoccurrence in patients with prostate cancer and bone metastases [abstract 1522]. Presented at: American Society of ClinicalOncology annual meeting; May 31-June 3, 2003; Chicago, Ill.
1657.02
TX
1657-TxReporter2of5-BB11-11 11/11/03 5:34 PM Page 4

New Currents in Treatment of Bone Metastases: A Case-Based Approach, Part 2Bone Metastases in Breast Cancer
Instructions for Documentation of Participation in This Activity:To receive an acknowledgment of your participation for CME/CPE/CE credit, please complete the following steps:
1. Carefully read this newsletter and listen to the audio CD.
2. Complete the Posttest below, selecting the most appropriate response to each question.
3. Complete the Evaluation.
4. Send photocopies of the Posttest and Evaluation to Projects In Knowledge, Overlook at Great Notch, 150 Clove Rd,Little Falls, NJ 07424, or fax to: 973-890-8866 by December 31, 2004.
If you complete these steps and score 70% or higher, Projects In Knowledge will mail you an acknowledgment of participation for up to 1 hour of CME creditfor physicians, 1 contact hour of credit for pharmacists, or 1.2 contact hours for nurses within 6 weeks of receipt of your materials. If you score lower than70%, Projects In Knowledge will notify you by mail and you will be given another chance to take the Posttest.
Name __________________________________________________________________ Degrees/Credentials _________________
Mailing Address _____________________________________________________________________________________________
City _____________________________________________________________________ State ________ ZIP ________________
Phone ________________________________________________ Fax _________________________________________________
E-mail _____________________________________________________________________________________________________
Please indicate your answers below:
1. About half of all breast cancer patients with bone metastases will develop skeletal complications.
a. Trueb. False
2. In patients with bone metastases, strontium-89 has been found to be effective in:
a. Relieving painb. Preventing fracturesc. Preventing hypercalcemiad. Reducing markers of bone resorptione. All of the above
3. Pamidronate was found to be significantly more effective than placebo in reducing skeletal complications in patients withbreast cancer and bone metastases who were receiving concomitant:
a. Hormone therapyb. Chemotherapyc. Either one
CME Posttest
Part 2 of 5
& Ask the Experts" Audio Edition"
1657.BPT—Page 1 of 2

1657.BPT—Page 2 of 2
Name ______________________________________________________________________________________________________
Thank you for your participation.
CME Posttest (cont’d)
4. Multiple event analysis of data from phase III trials of breast cancer and myeloma patients found which of the followingdrugs to be significantly more effective at reducing the overall risk of a skeletal complication?
a. Pamidronateb. Zoledronic acidc. Neither—they were found to be equivalent.
5. The development of a skeletal-related event during bisphosphonate therapy means that the agent has failed and should bediscontinued.
a. Trueb. False
6. Skeletal complications that may occur in patients with bone metastases include:
a. Need for radiation therapy or surgeryb. Pathologic fracturec. Spinal cord compressiond. Hypercalcemiae. All of the above
7. Which of the following tests is recommended to assess for bone loss in patients with breast cancer?
a. MRIb. CTc. Bone scand. X-raye. Bone mineral density
8. Which of the following is the most potent bisphosphonate?
a. Etidronateb. Zoledronic acidc. Pamidronated. Clodronate
9. Which of the following is associated with greater renal toxicity?
a. A 2-hour infusion of pamidronate 90 mgb. A 15-minute infusion of zoledronic acid 4 mgc. Neither; the risk of renal toxicity is equivalent.
10. Compared with the era prior to bisphosphonate use, bisphosphonates have:
a. Reduced the rate of skeletal-related eventsb. Delayed time to skeletal complicationsc. Reduced the incidence of hypercalcemiad. All of the above
& Ask the Experts" Audio Edition"

1657.BES—Page 1 of 2
Name _____________________________________________________ Degrees/Credentials _______________________________
Address ___________________________________________________________________________________________________
City ______________________________________________________ State ________________ ZIP _______________________
CME Evaluation Survey
Instructions: Please complete this survey, along with the Posttest, and mail or fax (both sides) to Projects In Knowledge, Overlook at Great Notch,150 Clove Road, Little Falls, NJ 07424; fax: 973-890-8822.
1. Please rate the extent to which you achieved the learning objectives: Excellent Very Good Good Satisfactory Poor
� Review the incidence of bone metastases in patients with metastaticcancer, including multiple myeloma, breast, prostate, lung, kidney,thyroid, and other solid tumors. ❑ ❑ ❑ ❑ ❑
� Describe the complications imposed by bone metastases in the clinical management of various solid tumors. ❑ ❑ ❑ ❑ ❑
� Examine the mechanisms of action of bisphosphonates and their rolein improving bone strength and inhibiting malignant cell function. ❑ ❑ ❑ ❑ ❑
� Discuss the safety and efficacy of currently available agents and next generation bisphosphonates. ❑ ❑ ❑ ❑ ❑
� Consider the use of intravenous therapy in the treatment armamentarium to delay and reduce skeletal complications of bone metastases in patients with multiple myeloma, breast, prostate, lung,kidney, thyroid, and other solid tumors. ❑ ❑ ❑ ❑ ❑
� Describe appropriate techniques for administration of intravenous bisphosphonates. ❑ ❑ ❑ ❑ ❑
� Improve quality of life for patients with bone metastases. ❑ ❑ ❑ ❑ ❑
2. Please rate the relevance of the objectives to the overall purpose/goals of the educational activity:
Excellent Very Good Good Satisfactory Poor
� Review the incidence of bone metastases in patients with metastaticcancer, including multiple myeloma, breast, prostate, lung, kidney,thyroid, and other solid tumors. ❑ ❑ ❑ ❑ ❑
� Describe the complications imposed by bone metastases in the clinical management of various solid tumors. ❑ ❑ ❑ ❑ ❑
� Examine the mechanisms of action of bisphosphonates and their rolein improving bone strength and inhibiting malignant cell function. ❑ ❑ ❑ ❑ ❑
� Discuss the safety and efficacy of currently available agents and next generation bisphosphonates. ❑ ❑ ❑ ❑ ❑
� Consider the use of intravenous therapy in the treatment armamentarium to delay and reduce skeletal complications of bone metastases in patients with multiple myeloma, breast, prostate, lung,kidney, thyroid, and other solid tumors. ❑ ❑ ❑ ❑ ❑
� Describe appropriate techniques for administration of intravenous bisphosphonates. ❑ ❑ ❑ ❑ ❑
� Improve quality of life for patients with bone metastases. ❑ ❑ ❑ ❑ ❑
New Currents in the Treatment of Bone Metastases: A Case-Based Approach, Part 2Bone Metastases in Breast Cancer
CME/CE PARTICIPANT EVALUATION
The goal of this activity is to provide an overview of bone metastases and the latest developments in preventing related skeletal complications using bisphosphonate therapies. Please rate the extent to which each objective was related to the goal of the activity.
& Ask the Experts" Audio Edition"

1657.BES—Page 2 of 2
Excellent Very Good Good Satisfactory Poor
3. Please rate the overall value of this enduring material: ❑ ❑ ❑ ❑ ❑
Strongly StronglyAgree Agree Disagree Disagree
4. Course was free from commercial bias: ❑ ❑ ❑ ❑
If you “Disagree” or “Strongly Disagree,” why?.....................................................................................................................................................
..................................................................................................................................................................................................................................
Just Right Too Advanced Too Basic
5. Please rate the level of the material presented: ❑ ❑ ❑
6. Please list any changes in your practice that you would consider making as a result of participating in this activity:
..................................................................................................................................................................................................................................
..................................................................................................................................................................................................................................
..................................................................................................................................................................................................................................
7. Please rate your interest in self-directed or distance learning in the following formats: Very Interested Moderately Interested Not Interested
a. Audioconference ❑ ❑ ❑
b. Videoconference ❑ ❑ ❑
c. Enduring materials (audiocassettes, videotapes, monographs) ❑ ❑ ❑
d. Internet (online discussions with experts, educational activities) ❑ ❑ ❑
e. Multimedia (online, CD-ROM) ❑ ❑ ❑
8. Please tell us how long it took you to complete this course (in minutes): ............................................................................................................
9. Please list topics and/or experts you would find interesting and professionally relevant for future CME activities:
..................................................................................................................................................................................................................................
..................................................................................................................................................................................................................................
..................................................................................................................................................................................................................................
..................................................................................................................................................................................................................................
10. Follow-up:As part of our ongoing continuous quality-improvement effort, we conduct postactivity follow-up surveys to assess the impact of ourCME courses on professional practice. Please indicate your willingness to participate in such a survey:❑ Yes, I would be interested in participating in a follow-up survey.❑ No, I’m not interested in participating in a follow-up survey.
Additional comments about this activity: ......................................................................................................................................................................
..................................................................................................................................................................................................................................
..................................................................................................................................................................................................................................
..................................................................................................................................................................................................................................
Name ______________________________________________________________________________________________________
CME Evaluation Survey(cont’d)
New Currents in the Treatment of Bone Metastases: A Case-Based Approach, Part 2Bone Metastases in Breast Cancer
CME/CE PARTICIPANT EVALUATION
Thank you for your participation.
& Ask the Experts" Audio Edition"