Embed Size (px)
Citation preview

BONE IN RENAL TRANSPLANTATION
M. COURBEBAISSE,Service de Néphrologie et Dialyses, Hôpital Tenon
NECKER SEMINARS IN NEPHROLOGY, 2011

• Introduction : Epidemiology and Physiopathology of bone loss and fracture after renal transplantation
• Corticosteroid-induced osteoporosis and steroid avoidance or withdrawal
• Bisphosphonates after renal transplantation
• Active and native vitamin D after renal transplantation
• Conclusions and Perspectives

BONE STORY OF A RENAL TRANSPLANT RECIPIENT…
Avascular necrosis

BONE STORY OF A RENAL TRANSPLANT RECIPIENT…
Avascular necrosis
Bilateral arthroplasty

BONE STORY OF A RENAL TRANSPLANT RECIPIENT…
Avascular necrosis
Bilateral arthroplasty

BONE STORY OF THE RENAL TRANSPLANT RECIPIENTS…Incidence of low BMD : 50%
• Immedialtely after transplantation- High dosage of steroid- Persistent abnormalities of
phosphocalcic metabolism
Leidig-Bruckner G. et al. Lancet 2001;357:342
• Stabilization-↓Immunosuppressive treatment- Improvement of phosphocalcic metabolism
• Worsening with chronic renal graft dysfunction….
• Before transplantation : renal osteodystrophy : 50 % Osteitis fibrosa, 30 % : Adynamic renal bone disease, 20 % : Mixed uremic osteodystrophy +/- OsteomalaciaCoco M et al. JASN 2003;14:2669.

BONE STORY OF THE RENAL TRANSPLANT RECIPIENTS…Incidence of low BMD : 50%
• Immedialtely after transplantation- High dosage of steroid- Persistent abnormalities of
phosphocalcic metabolism
Leidig-Bruckner G. et al. Lancet 2001;357:342
• Stabilization-↓Immunosuppressive treatment- Improvement of phosphocalcic metabolism
• Worsening with chronic renal graft dysfunction….
• Before transplantation : renal osteodystrophy : 50 % Osteitis fibrosa, 30 % : Adynamic renal bone disease, 20 % : Mixed uremic osteodystrophy +/- OsteomalaciaCoco M et al. JASN 2003;14:2669.

CsACsA
M. Bia, Transplantations reviews, 2008; 22 : 52-61
Poor muscle mass
Specific and non specific risk factors
Diuretic treatment :Increased urinaryCa excretion

CsACsA
M. Bia, Transplantations reviews, 2008; 22 : 52-61
Poor muscle mass
Specific and non specific risk factors
Diuretic treatment :Increased urinaryCa excretion
Classical risk factors of low BMD- Age- Low BMI- Menopause- Smoking- Familial history (hip fracture++)

FRACTURE : HIGH RISK AFTER RENAL TRANSPLANTATION

FRACTURE : HIGH RISK AFTER RENAL TRANSPLANTATION
- Most fractures occur during the first 3 years after transplantation (Nisbeth, U., Transplantation, 1999) but the risk remains increased on the long-term (Vautour, L.M., Osteoporos Int, 2004)
→ After renal transplantation: Bad correlation between BMD and fracture risk(Grotz, W.H., Transplantation, 1994; Vautour, L.M., Osteoporos Int, 2004; Durieux, S., Transplantation, 2002)

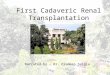
Bone biopsy after renaltransplantation5.4 ± 0.8 [6 mo-27 year](n= 57)
37% 45%
OsteomalaciaAdynamic renal bone disease
BONE DISEASE AFTER KIDNEY TRANSPLANTATION
-Severe 25OHD deficiency-hypophosphataemia

– Pain
– Invalidity
– Skeletal deformation
– Poor quality of life
– Hospitalizations
– High cost
SEVERE CONSEQUENCES…..

• Introduction : Epidemiology and Physiopathology of bone loss and fracture after renal transplantation
• Corticosteroid-induced osteoporosis and steroid avoidance or withdrawal
• Bisphosphonates after renal transplantation
• Active and native vitamin D after renal transplantation
• Conclusions and Perspectives

CORTICOSTEROID-INDUCED OSTEOPOROSIS
Maalouf NM, JCEM, 2005

Monier-Faugere et al, JASN 2000
53 renal transplant recipientsBone biopsy after renal transplantation
5.4 ± 0.8 [6 mo‐27 year]
Relationship between cumulative dose of prednisone and bone volume

SteroidNo Steroid
Fracture risk Fracture risk

SteroidNo Steroid
Fracture risk Fracture risk
STEROIDTscore < -1,5 : Increased fracture risk

A dose dependence of fracture risk is observed even forlow doses of oral cortocosteroids
< 2.5 mg/day 2.5‐7,5 mg/day > 7.5 mg/day
RR of Hip fracture
0.99 1.77 2.27
RR of Vertebral fracture
1.55 2.59 5.18
Van Staa TP, JBMR, 2000

A dose dependence of fracture risk is observed even forlow doses of oral cortocosteroids
< 2.5 mg/day 2.5‐7,5 mg/day > 7.5 mg/day
RR of Hip fracture
0.99 1.77 2.27
RR of Vertebral fracture
1.55 2.59 5.18
Van Staa TP, JBMR, 2000

Early corticosteroid withdrawal
Withdrawal at 7days
posttransplant(n=191)
5 mg/d after 6months
posttransplant(n=195)
p
OSTEONECROSIS 0 % 2,6 % 0.06
FRACTURE 5.2 % 9.7 % 0.12
OSTEONECROSIS + FRACTURE
5.2 % 11.3 % 0.041
Woodle ES, Ann Surg 2008;248:564.
5 years of follow up

Late low-dose steroid withdrawal increases BMD
Control group Withdrawal group
Time post transplantation (yr) 7.3 (1.0–13.1) 6.5 (1.0–14.7)
Start of the study : Prednisolone dose (mg)
5.9 (0.2) 6.0 (0.3)
Farmer CTK, Am J Transplant 2006(6):2929.
92 RTR, > 1 year post transplant, randomized
One year follow-up

Steroid avoidance or withdrawal and graft survival
Knight SR, Transplantation. 2010 Jan 15;89(1):1-14. Review
• cardiovascular riskHypertension (RR 0.90, p<0.0001) New onset diabetes (RR 0.64, P=0.0006),Hypercholesterolemia (RR 0.76, p<0.0001)
• risk of Acute Rejection (RR 1.56, p<0.0001)•No significant differences in -patient survival-graft survival
META-ANALYSIS: 34 RTCs, including 5,637 patients

• Introduction : Epidemiology and Physiopathology of bone loss and fracture after renal transplantation
• Corticosteroid-induced osteoporosis and steroid avoidance or withdrawal
• Bisphosphonates after renal transplantation
• Active and native vitamin D after renal transplantation
• Conclusions and Perspectives

Effects of Bisphosphonates
Gennari L et al, Lancet, 2009

37% 45%
OsteomalaciaAdynamic renal bone disease
Bisphosphonates treatment should be used with caution…

37% 45%
OsteomalaciaAdynamic renal bone disease
Bisphosphonates treatment should be used with caution…
!! Bisphosphonate treatment

Fan et al, Kidney International, 2000
Femoral neck
Controln = 13
Pamidronaten = 13
Lumbar spine
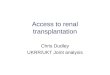
Bisphosphonates : IV Pamidronate prevents bone loss during the first year after renal transplantation
26 male RTR : randomized to receive either placebo or IV pamidronate (0.5 mg/kg) at thetime of transplantation and again one month later, BMD T0, M3 and M12
- 6.4%- 9%
stable stable

Femoral Neck
Lumbar spine
Fan et al, Kidney International, 2003
-12.3%
-4.64%
stable
stable
4-year data from 17 of the 26 original cohort
Bisphosphonates : pamidronate (T0 and M1) protects femoral neck from significant bone loss over the 4 years after transplantation.

80 RTR, Randomization– Ibandronate : 1 mg IV immediately
before, and 2 mg 3, 6, and 9 mo after transplantation
– Placebo
Grotz W et al. J Am Soc Nephrol 2001;12:1530-7.
Bisphosphonates : Ibandronate (T0 ,M3, M6, M9) protects from significant bone loss, spinal deformation and loss of body height
During the first year after kidneytransplantation Ibandronate also prevents- Spinal deformation - Loss of body height
Lumbar spine
Femoral Neck
Ibandronate
Placebo

Reid DM, Lancet, 2009;373:1253
A single 5 mg IV infusion of zoledronic acid is non-inferior, possibly more effective,and more acceptable than is 5 mg of oral risedronate daily for prevention and
treatment of corticosteroid-associated bone loss
TreatmentSteroid>3 months
PreventionSteroid<3 months
Femoral neck
Lumbar spine


Bisphosphonates and the kidney….
Palmer SC, Cochrane Databse Syt Rev 2007;CD005015.
Pamidronate and Alendronate : collapsing HSFZolendronate : acute tubular necrosisPerazella MA, Kidney Int, 2008
European Best Practice Guidelines :Bisphosphonates Ok if GFR stable and > 50-60 ml/min

• Introduction : Epidemiology and Physiopathology of bone loss and fracture after renal transplantation
• Corticosteroid-induced osteoporosis and steroid avoidance or withdrawal
• Bisphosphonates after renal transplantation
• Active and native vitamin D after renal transplantation
• Conclusions and Perspectives

Maalouf NM, JCEM, 2005
Calcitriol
?
Influence of calcitriol on corticosteroid-induced osteporosis
Impaired calcitriol production after successful renal transplantationFleseriu M, Osteoporos Int, 2007
+
_

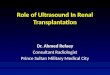
• 40 RTR• Randomization
– Alfacalcidol 0,5 µg/D + 500mg Ca– Placebo + 500 mg Ca
• % change in BMD at 1 year :
El-Agroudy AE. JASN 2003
Preventive treatment : Active vitamin D
Placebo (n = 20)
Alfacalcidol(n = 20)
p
Lumbar spine ‐ 3,2 % + 2,1% p<0,05
Femoral neck ‐ 3,8% + 1,8% p<0,05
Forearm ‐ 1,8 % + 3,2% p<0,05
- Decreased PTH in the treated group
- Similar urinary calcium excretion in both groups
- Similar rate of acute rejection in both groups

2
Courbebaisse M, Transplantation. 2010, 89(2):131-137.
1α-hydroxylase
25-hydroxylase
24-hydroxylase
NATIVE VITAMINE D

25(OH)vit D (ng/ml)
Post-transplant 25OHD insufficiency (< 30 ng/ml)
PREVALENCE• Day 0 : 88% • One year : 89 % • 7 years : 75.5 %
Sadlier, D.M. Clin Transplant, 2007Boudville, N.C. Nephrol Dial Transplant, 2006
CAUSES
• Insufficient intake
• Reduced sun exposure
• Increased 25OHD catabolism
due to 24-hydroxylase activation
(steroid and FGF23)
Prié D, non published data
Bhan, I., Kidney Int, 2006

Wissing, K.M., Transplantation, 2005
Inverse correlation between[25OHD] and [PTH]
Consequences of 25OHD deficiency and insufficiency
(n = 90 RTR, Month 9 post-transplant)
• 250HD insufficiency (<30 ng/ml) causes secondary hyperparathyroidism.
•Severe 25OHD (<10 ng/ml) deficiency causes osteomalacia.

M3 M12transplantation
Exploration 1 GFR (iohexol)25(OH)D, PTH,CaT, P, urinary Ca/creat
M6
25(OH)D, PTHCaT, P, urinaryCa/creat
Exploration 2 GFR (iohexol)25(OH)D, PTH,CaT, P, ,urinaryCa/creat
M4
INTENSIVE TREATMENTCholecalciferol100 000 IU/15 days
MAINTENANCE TREATMENTCholecalciferol100 000 IU/2 months
TREATED GROUP2006
CONTROL GROUP2005
No vitamin D treatment
TREATED AND CONTROL GROUPS TREATED AND CONTROL GROUPSTREATED GROUP
47 adult RTR-[25OHD] < 30 ng/ml-[Ca] < 2.70 mmol/l
49 adult RTR-[25OHD] < 30 ng/ml-[Ca] < 2.70 mmol/l
Courbebaisse M, Kidney Int 2009; 75:646-51.

-25OHD deficiency does not spontaneously normalize in RTR.
- 100 000 UI of CLF every two weeks during 2 months correct 25OHDinsufficiency.
- Maintenance treatment (100 000 UI of CLF every two months) cannot maintain 25OHD ≥ 30 ng/ml in half of patients and should be 100 000 UIevery month.
- In RTR, increasing 25OHD ≥ 30 ng/ml decreases serum PTH level.
- Doses used to correct 25OHD deficiency are safe : no hypercalcaemia, nohyperphosphataemia, no induced hypercalciuria, stable mesured GFR
Treatment of 25OHD insufficiency after renal transplantation
Courbebaisse M, Kidney Int 2009; 75:646-51.

• Introduction : Epidemiology and Physiopathology of bone loss and fracture after renal transplantation
• Corticosteroid-induced osteoporosis and steroid avoidance or withdrawal
• Bisphosphonates after renal transplantation
• Active and native vitamin D after renal transplantation
• Conclusions and Perspectives

After transplantation : General preventive rules- Steroid avoidance or withdrawal ++++
- Control of hypercalciuria : NaCl and protein intake/avoidance of furosemide- Adequate calcium intake (≥ 1200 mg/jour)
- Replete vitamin D status (25OHD≥30 ng/mL)- Encourage weight-bearing physical activity
First year post transplantation (KDIGO)- BMD
-Serum calcium, Serum phosphate, Serum PTH, Total Alkaline Phosphatases
Before transplantation : Prevention of renal osteodystrophy
BMD> -1.5No fracture history
No osteoporosis risk factorNo hypogonadism
No specific treatment
Other Cases Oral or IV Bisphosphonates-CI : osteomalacia, low bone turn over-GFR<30/ml/min??-Dental care BEFORE initiation
Active form of vitamin D
Treatment of symptomatic hypogonadism
Other Cases
P. Ebeling, J Clin Endocrinol Metab 94: 1483–1490, 2009; KDIGO: Am J Transplant 2009;9(S3):S93-S96; AFSSAPS

Perspective : Anti RANK ligand antibody = DENOSUMAB
Pre osteoclastPre osteoclast
RANKRANK
OsteoblastOsteoblaststromal cellstromal cell
RANKLRANKL
osteoclastosteoclast
OPGOPG

Perspective : Anti RANK ligand antibody = DENOSUMAB
Pre osteoclastPre osteoclast
RANKRANK
OsteoblastOsteoblaststromal cellstromal cell
RANKLRANKL
osteoclastosteoclast
OPGOPG AntiAnti RANKL AbRANKL Abdenosumabdenosumab

Perspective : Anti RANK ligand antibody = DENOSUMAB
Pre osteoclastPre osteoclast
RANKRANK
OsteoblastOsteoblaststromal cellstromal cell
RANKLRANKL
osteoclastosteoclast
OPGOPG AntiAnti RANKL AbRANKL Abdenosumabdenosumab

Perspective : Anti RANK ligand antibody = DENOSUMAB
Pre osteoclastPre osteoclast
RANKRANK
OsteoblastOsteoblaststromal cellstromal cell
RANKLRANKL
osteoclastosteoclast
OPGOPG AntiAnti RANKL AbRANKL Abdenosumabdenosumab
- Phase 3 clinical trial (FREEDOM) : fractures

Perspective : Anti RANK ligand antibody = DENOSUMAB
Pre osteoclastPre osteoclast
RANKRANK
OsteoblastOsteoblaststromal cellstromal cell
RANKLRANKL
osteoclastosteoclast
OPGOPG AntiAnti RANKL AbRANKL Abdenosumabdenosumab
- Phase 3 clinical trial (FREEDOM) : fractures
- Sub cutaneous injection every 6 months

Perspective : Anti RANK ligand antibody = DENOSUMAB
Pre osteoclastPre osteoclast
RANKRANK
OsteoblastOsteoblaststromal cellstromal cell
RANKLRANKL
osteoclastosteoclast
OPGOPG AntiAnti RANKL AbRANKL Abdenosumabdenosumab
- Phase 3 clinical trial (FREEDOM) : fractures
- Sub cutaneous injection every 6 months- Pharmocokinetic and pharmocodynamic
not influenced by GFR++

Perspective : Anti RANK ligand antibody = DENOSUMAB
Pre osteoclastPre osteoclast
RANKRANK
OsteoblastOsteoblaststromal cellstromal cell
RANKLRANKL
osteoclastosteoclast
OPGOPG AntiAnti RANKL AbRANKL Abdenosumabdenosumab
- Phase 3 clinical trial (FREEDOM) : fractures
- Sub cutaneous injection every 6 months- Pharmocokinetic and pharmocodynamic
not influenced by GFR++- Safety OK

‐RTR, 12‐48 months post‐transplant ‐25OHD< 30 ng/ml
RANDOMIZATION
CLC : 100 000 IU every other week
= intensive treatment(Eq 6600 IU/D)
CLC : 100 000 IU/month= maintenance treatment
(Eq 3300 IU/D)
M2 M24M0
CLC : 12000 IU every other week(Eq 800 IU/D)
CLC 12000 IU/month(Eq 400 IU/D)
Follow‐up= 2 years
Statistical analysis
Inclusion = 1 year
Treated groupn = 320
Control groupn = 320
VITALE : « Etude prospective, multicentrique, randomisée, en double aveugle, évaluant le bénéfice d’un traitement par vitamine D3 chez des patients transplantés
rénaux », Pr. Thervet, Dr. Courbebaisse, PHRC 2010
composite criteria : NODAT Cardiovascular events de novo cancerDeath

‐RTR, 12‐48 months post‐transplant ‐25OHD< 30 ng/ml
RANDOMIZATION
CLC : 100 000 IU every other week
= intensive treatment(Eq 6600 IU/D)
CLC : 100 000 IU/month= maintenance treatment
(Eq 3300 IU/D)
M2 M24M0
CLC : 12000 IU every other week(Eq 800 IU/D)
CLC 12000 IU/month(Eq 400 IU/D)
Follow‐up= 2 years
Statistical analysis
Inclusion = 1 year
Treated groupn = 320
Control groupn = 320
VITALE : « Etude prospective, multicentrique, randomisée, en double aveugle, évaluant le bénéfice d’un traitement par vitamine D3 chez des patients transplantés
rénaux », Pr. Thervet, Dr. Courbebaisse, PHRC 2010
composite criteria : NODAT Cardiovascular events de novo cancerDeath
Among secondary criteria : BMDFractureSerum PTH

THANK YOU FOR YOUR ATTENTION