Embed Size (px)
Citation preview

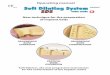
Dental Implants in the Aesthetic ZoneNavigating Unvharted Waters ..!
Ideal Aesthetic Function
Soft Tissues
!
Implant !Phil
osophy !
Bone !
ideal
prosthetic
positionNikos Mattheos, DDS, MASc, PhD Clinical Associate Professor in Implant Dentistry
Jakarta, October 2019
2 yrs part time MSc in Implant Dentistry3 yrs full time MDS in Implant Dentistrypatient care, research.
⾺ 毅 剛
Immediate Implants ?
Ridge Preservation ?
Early + Simultaneous Augmentation ?
2 stage augmentation?
Block Graft ? Non- Resorbable membrane
Surgical Protocols - bone
Reduced diametre implants ? 2.9 mm? Tapered self-cutting implants ? BLX Implant?
Free gingival graft ?
Connective tissue graft ?
Repositioned flaps ?
Pedicle grafts?
Xenograft / Allograft?
Surgical Protocols - soft tissue
Timing?
Before, during , after implant ?
Immediate provisional/ loading
Removable denture
Transmucosal healing
Submerged healing - second stage
Early loading (<2 months)
Conventional Loading (2-4 months)
Delayed Loading ( <4 months)
Temporary and Restorative protocols

Surgical and Restorative protocols
Immediate Implants ?
Ridge Preservation ?
Simultaneous Augmentation ?
2 stage augmentation?
Block Graft ? Non- Resorbable membrane
Reduced diametre implants ? 2.9 mm?
Tapered self-cutting implants ?
BLX implant ?
Free gingival graft ?
Connective tissue graft ?
Repositioned flaps ?
Pedicle grafts?
Xenograft / Allograft?
Immediate provisional/ loading
Removable denture
Transmucosal healing
Submerged healing - second stage
Early loading (<2 months)
Conventional Loading (2-4 months)
Delayed Loading ( <4 months)
ideal implant position
Soft Tissues!
Bone !
Assess local Anatomy
Prosthesis !Implant !
Optimal clinical outcomeProtocol !
1
23
What happens after the extraction a tooth ? Assess local
Anatomy
1
Cardaropoli et al. J Clin Periodontol 2003 Araujo & Lindhe. J Clin Periodontol 2005
• Maximum loss of tissue contour occurs within the first 3 months Johnson 1969 et al
• A width reduction of approximately 50% over 12 months. 2/3rds of this occurs within the first 3 months Schropp et al 2003
• Mean horizontal: 3.8mm Mean vertical: 1.24mm 6 months post extraction Hammerle 2012
Average Hong Kong Patient Your Patient

Chappuis et al. Ridge alterations post-extraction in the esthetic zone: a 3D analysis with CBCT. J Dent Res 2013: 92: 195S–201S.
Extraction 8 weeks
Bone: width: - 62%
Buccal wall
< 1mm
> 1mm
Soft tissuethickness: x 7
Bone: width: - 9%
Soft tissuethickness: 0 Anatomy : buccal wall thickness
Neighbouring teeth Angle of the ridge Soft tissue biotype, thickness, height Apical bone volume
Implant Placement in the Aesthetic Zone
Checkpoint !Don’t generalise…Individualise
Patient
Systemic
Oral
Local site
to establish and satisfy the patient‘s needs for esthetics and function ...
... under healthy and sustainable conditions
Principle Driven Implant Dentistry: Our mission statement:
h
wImplant shoulder
2;!How much height?3;!How much width ? (thickness)4;!How much keratinised mucosa?5: How to design the prosthesis?
Soft tissue outcomes:
Necessary ?
Desired ?
Irrelevant ?
Clin Oral Implan.ts Res. 1991 Apr-Jun;2(2):81-90. The soft tissue barrier at implants and teeth. Berglundh T1, Lindhe J, Ericsson I, Marinello CP, Liljenberg B, Thomsen P
3.8

Biologic width is not related to the soft tissue height !
ConnectiveTissue
JunctionalEpithelium
Sulcus
Biofilm
Prosthesis
Bone
Implant
Internal Connection
Supracrestal Complex
Screw
Abutment
Connective Tissue
Epithelium
Peripendicula Collagen Fibres
Bone
Sharpey’s fibres
Junctional EpitheliumJunctional Epithelium
Tooth Implant
Cementum
Periodontal ligament
⎬⎭ ⎫
Attachment Adhesion
Attachment Adhesion
Sulcus Sulcus Sulcus
Genetics
Anatomy
Critical zone
Critical zone
Sulcus
Sulcus
Attachment
Attachment
w
h3 mm Implant shoulder
Papilla
Mid buccal
p2-4 mm
height? 3mm / 2-4 mm
width ? 2mm
keratinised? 2mm
Optimal clinical outcome
2
2 mm
Soft tissues:
Checkpoint !
Bone: 1-1.5 mm

Prosthetic Manipulation?
Immediate implant?
Ridge Preservation?
How can we overcome the compromised Bone ? Loading Protocol
Surgical Protocol
Immediate Type A
Early Type B(<2 m)
Conventional Type C(>2 m)
Immediate Type 1 1A 1B 1C
Early Type 2(4-12 w)
2A 2B 2C
Conventional Type 3(>6 m)
3A 3B 3C
Clinically Documented
Clinically Insufficient Documentation
Scientific and Clinically Validated
Gallucci et al 2018 COIR
Immediate implant with Immediate Provisional 1A
Immediate implant with early / conventional loading 1B/C
Protocols 1A - 1B - 1C
Immediate Flapless:
ImmediateCrown
Customised Healing abutment
Immediate with Flap:
Immediate Implant?
2
31
Flapless - atraumatic (?)
Palatal placement
Augmentation
Immediate temporary
Permanent restoration
Immediate Implant? With Immediate Temporary Crown: 1 Success factors:
High Survival
Lower success
Higher complexity
Higher risk
Immediate Implants Protocols 1A - 1B - 1C

Success factors:
High Survival
Lower success
Higher complexity
Higher risk
Digital Workflow?
Immediate Implants Protocols 1A - 1B - 1C
Checkpoint 3 !
Free-hand SurgeryGuided Surgery
Computer-aided
Predetermined placement posistion
pre-Identified placement posistion
Comparison of the accuracy of of single tooth implant placed using static, dynamic and free-hand Computer Assisted Implant Surgery.
P. Smitkarn, , K. Subhalenka, N. Mattheos, A. Pimkhaokam
Immediate Implant?
With Custom healing abutment: 2
Not adequate primary stability
Unfavorable occlusion?
Maintain soft tissue architecture
Scientific evidence
soft tissues changes. In case of parametric data, a pairedt-test was used, whereas in nonparametric data aWilcoxon signed-rank test was used. A frequencyanalysis was used to describe the distribution of hardand soft tissue changes among the patients. Allcalculations were performed with the SPSS statisticalsoftware program (version 16.0, SPSS, Inc., Chicago, IL,USA).
RESULTS
The reasons for tooth loss of the 15 implants (13incisors, 1 canine, and 1 premolar) included in thisstudy are outlined in Table 1. The patient
demographics, implant characteristics and follow-upintervals are shown in Table 2. No implant loss orimplant associated pathology was observed atthe final follow-up visit. Representativeoutcomes of the treatment are illustrated inFigures 4 to 6.
Hard Tissue Measurements
Radiographic evaluation revealed a mean mesial bonegain of 1.20 ± 1.01 mm (p < 0.0001), which reachedstatistical significance. The mean distal bone gain was0.80 ± 1.14 mm (p = 0.01), which also reached statisticalsignificance. Table 3 shows that there was a significantchange in both the mesial and distal bone level betweenthe time of implant placement and the follow-upassessment. Table 4 shows the distribution of bone gainand loss in millimeters for individual patients. Themajority of the readings demonstrated bone gain!0.5 mm (13/15 cases).
Soft Tissue Measurements
The mean mid-buccal gingiva recession was 0.20 ± 0.78mm (p = 0.44). The mesial papillary height loss was0.50 ± 1.12 mm (p = 0.24), whereas the distal papillaryheight loss was 0.30 ± 0.82 mm (p = 0.27) Table 5. The
A B
FIGURE 2. Illustration of hard tissue measurements onperiapical X-ray. Cl = coronal line; Dbc = distal bone contact;Mbc = mesial bone contact.A set of paired radiographs usedfor measurements. A = baseline radiograph; B = follow-upradiograph.
FIGURE 3. Illustration of the measurements of soft tissue onphotographs. Bm = distance to middle of buccal gingival margin;Dp = distance to distal papilla; Mp = distance to mesial papilla;Ocl = occlusal line.
IMMEDIATE PLACEMENT AND RESTORATION OF DENTAL IMPLANTS Khzam et al.
© 2013 Wiley Periodicals, Inc. DOI 10.1111/jerd.12083 Journal of Esthetic and Restorative Dentistry Vol •• • No •• • ••–•• • 2013 5
soft tissues changes. In case of parametric data, a pairedt-test was used, whereas in nonparametric data aWilcoxon signed-rank test was used. A frequencyanalysis was used to describe the distribution of hardand soft tissue changes among the patients. Allcalculations were performed with the SPSS statisticalsoftware program (version 16.0, SPSS, Inc., Chicago, IL,USA).
RESULTS
The reasons for tooth loss of the 15 implants (13incisors, 1 canine, and 1 premolar) included in thisstudy are outlined in Table 1. The patient
demographics, implant characteristics and follow-upintervals are shown in Table 2. No implant loss orimplant associated pathology was observed atthe final follow-up visit. Representativeoutcomes of the treatment are illustrated inFigures 4 to 6.
Hard Tissue Measurements
Radiographic evaluation revealed a mean mesial bonegain of 1.20 ± 1.01 mm (p < 0.0001), which reachedstatistical significance. The mean distal bone gain was0.80 ± 1.14 mm (p = 0.01), which also reached statisticalsignificance. Table 3 shows that there was a significantchange in both the mesial and distal bone level betweenthe time of implant placement and the follow-upassessment. Table 4 shows the distribution of bone gainand loss in millimeters for individual patients. Themajority of the readings demonstrated bone gain!0.5 mm (13/15 cases).
Soft Tissue Measurements
The mean mid-buccal gingiva recession was 0.20 ± 0.78mm (p = 0.44). The mesial papillary height loss was0.50 ± 1.12 mm (p = 0.24), whereas the distal papillaryheight loss was 0.30 ± 0.82 mm (p = 0.27) Table 5. The
A B
FIGURE 2. Illustration of hard tissue measurements onperiapical X-ray. Cl = coronal line; Dbc = distal bone contact;Mbc = mesial bone contact.A set of paired radiographs usedfor measurements. A = baseline radiograph; B = follow-upradiograph.
FIGURE 3. Illustration of the measurements of soft tissue onphotographs. Bm = distance to middle of buccal gingival margin;Dp = distance to distal papilla; Mp = distance to mesial papilla;Ocl = occlusal line.
IMMEDIATE PLACEMENT AND RESTORATION OF DENTAL IMPLANTS Khzam et al.
© 2013 Wiley Periodicals, Inc. DOI 10.1111/jerd.12083 Journal of Esthetic and Restorative Dentistry Vol •• • No •• • ••–•• • 2013 5
Bone Soft tissue measurements2013Immediate placement and restoration of dental implants
In the aesthetic region: Clinical Case Series
Immediate Placement and Restoration of Dental Implantsin the Esthetic Region: Clinical Case SeriesNABIL KHZAM, BDS, MPhil, DClinDent*, NIKOS MATTHEOS, DDS, MASc, PhD†, DAVID ROBERTS, BDSc, MDSc‡,
WILLIAM L BRUCE, BDSc, MDSc§, SASO IVANOVSKI, BDSc, BDentSt, MDSc, PhD¶
ABSTRACT
Aim: The objective of this study was to assess the hard and soft tissue changes following immediate placement andprovisional restoration of single-tooth implants in the aesthetic zone.Methods: Thirteen patients with immediately placed and restored implants were included in this study. All participatingpatients underwent the same treatment strategy that involved removal of the failed tooth, flapless surgery, immediateimplant placement, and connection of a screw-retained provisional restoration.Three months following implantplacement, the temporary crowns were replaced by the definitive restorations. Implant survival rates, and hard and softtissue changes were measured using periapical X-rays and photographs.The range of the observation period wasbetween 12 and 37 months with a mean period of 23.2 ± 7.6 months.Results: At the time of follow-up, all implants were present with no complications. Radiographic evaluation revealed amean mesial bone gain of 1.20 ± 1.01 mm and a mean distal bone gain of 0.80 ± 1.14 mm, which reached statisticalsignificance.The mean mid-buccal recession was 0.20 ± 0.78 mm, whereas the mesial and distal papillae height loss was0.50 ± 1.26 mm and 0.30 ± 0.82 mm, respectively.The changes in the soft tissues did not reach statistical significance.Conclusion: Notwithstanding the limitation of a small sample size, this study shows that immediate implant placementand provisional restoration in the maxillary aesthetic zone can result in favorable treatment outcomes with regards tosoft and hard tissues changes over a follow-up period of 23.2 ± 7.6 months.
CLINICAL SIGNIFICANCE
Most clinical trials investigating immediate implant placement and immediate restoration in the maxillary anterior zonehave focused on implant survival and implant success, with particular emphasis on radiographically assessed hard tissueschanges. However, this study assesses the soft tissue changes associated with this procedure, which is an importantarea of study given the esthetic demands of implant therapy in the maxillary anterior region.(J Esthet Restor Dent ••:••–••, 2013)
INTRODUCTION
Single tooth replacement with an implant supportedcrown is often the treatment of choice for missing teethin the anterior maxilla. The original implant treatmentprotocol described by Branemark involved 3 months of
healing following extraction of a failed tooth, and anadditional 3 to 6 months of a load-free period followingimplant placement.1,2 In the last 20 years, implantdentistry has evolved dramatically, with the originaltwo-stage protocol modified to include one-stagesurgery,3 immediate implant placement into a fresh
*Specialist Periodontist, Private Practice, University of Tripoli, Libya†Associate Professor, The University of Hong Kong, Hong Kong‡Specialist Prosthodontist, Private Practice, Brisbane, Qld, Australia§Specialist Prosthodontist, Private Practice, Brisbane, Qld, Australia¶Professor of Periodontology, School of Dentistry and Oral Health, Griffith University, Gold Coast, Qld, Australia
RESEARCH ARTICLE
© 2013 Wiley Periodicals, Inc. DOI 10.1111/jerd.12083 Journal of Esthetic and Restorative Dentistry Vol •• • No •• • ••–•• • 2013 1
has some limitations, namely that the restorativecontact point is not going to be constant as theprovisional crowns will undergo replacement withpermanent restorations, whereas the radiographiclocation of the apical/coronal shoulder is easily a!ectedby image distortion.24
The results of the present study, which showed arelatively high amount of bone gain, compares favorablywith other studies involving implant therapy in the
maxillary anterior zone.18,19,22,25–28 Using the immediateplacement and restoration protocol, Kan and colleaguesshowed a mean marginal bone loss ranging from 0.26 to0.40 mm on the mesial and 0.22 to 0.28 mm on thedistal aspect of the implant at 1-year follow-up.23
Several other investigators have shown even greateramounts of bone loss. The study by De Rouck andcolleagues revealed a mean bone loss of 0.98 mm on themesial aspect of the implant and 0.78 mm distally at1-year follow-up.6 Other studies using the immediateimplant placement and immediate restoration approachhave shown similar outcomes.23,24,29–31 On the otherhand, Kan and colleagues reported that “scalloped”shaped implants placed into extraction sites showed amean bone gain of 1.0 mm after 1 year of follow-up.7The amount of bone gain in this study was attributed tothe placement of a bone graft into the gap between theimplant and walls of the extraction socket thatsubsequently resulted in radiographically assessed bonefill. Our study used a “platform switching” implant
FIGURE 6. Illustration of soft tissue on photographs,(21)-baseline and follow-up.
TABLE 3. Bone level changes (presented as millimeterschange)
Parameters Change in mm p-value
Mesial bone level 1.20 ± 1.01 0.001*
Distal bone level 0.80 ± 1.14 0.01*
Mean ± standard deviation.*Significant.
TABLE 4. Frequency analysis of hard tissue changes inmillimeters
Bone changes inmm/patients
2.5 and 2 mm 2.23 2.19 2.18
2 and 1.5 mm 1.79 1.75 1.58
1.5 and 1 mm 1.29 1.04 –
1 and 0.5 mm 0.82 0.71 –
0.5 and 0 mm 0.22 0.2 0.01
0 and !0.5 mm 0.09 – –
!0.5 and !1 mm 0.63 – –
TABLE 5. Soft tissue level changes (presented as millimeterschange)
Parameters Change in mm p-value
Mesial papilla level !0.50 ± 1.12 0.24
Distal papilla level !0.30 ± 0.82 0.27
Mid-buccal ginigval level !0.20 ± 0.78 0.44
Mean ± standard deviation.
IMMEDIATE PLACEMENT AND RESTORATION OF DENTAL IMPLANTS Khzam et al.
DOI 10.1111/jerd.12083 © 2013 Wiley Periodicals, Inc.Vol •• • No •• • ••–•• • 2013 Journal of Esthetic and Restorative Dentistry8
13 patients 2 years
Immediate Implant?

OR I G I N A L A R T I C L E
Immediate implant placement and restoration in the anteriormaxilla: Tissue dimensional changes after 2-5 year follow up
Himanshu Arora, MDS1 | Nabil Khzam, DClinDent2 | David Roberts, MDSc3 |
William L Bruce, MDSc3 | Saso Ivanovski, MDSc, PhD1
1School of Dentistry and Oral Health,
Griffith University, Gold Coast, Queensland,
Australia2Private practice, Perth, Western Australia,
Australia3Private practice, Brisbane, Queensland,
Australia
CorrespondenceSaso Ivanovski, School of Dentistry and
Oral Health, Griffith Health Centre, Griffith
University - Gold Coast Campus, Parklands
Drive, Queensland 4222, Australia.
Email: [email protected]
Abstract
Background: Immediate implant placement followed by an immediate restoration has proven to
be a viable technique in the anterior maxillary region.
Purpose: This prospective study evaluated the mid-long term (2-5 years) tissue changes around
immediately placed and restored implants in the anterior maxilla using flapless surgery and simulta-
neous hard tissue augmentation.
Materials and methods: Thirty AstraTech implants were immediately placed in 30 patients, fol-
lowed by the delivery of an immediate provisional restoration on the same day. All participating
30 patients underwent the same treatment strategy that involved flapless removal of a failing max-
illary anterior tooth, immediate implant placement, simultaneous augmentation with a
deproteinized particulate xenograft, followed by the connection of a screw-retained provisional
restoration. Radiographs and photographs were used to measure hard and soft tissue changes.
Aesthetic evaluation was performed using the Pink Esthetic Score (PES).
Results: All implants remained osseointegrated during the follow up period of 2-5 years (mean
47615 months). Twelve of the thirty patients completed the 5 year follow up. Radiographic eval-
uation revealed average gains in bone levels of 0.18 and 0.34 mm mesially and distally,
respectively. Soft tissue evaluation showed a mean tissue loss of 0.0560.64 mm and 0.166
0.63 mm at the mesial and distal papillae, respectively, while mid-facial mucosal recession was
0.2960.74 mm. A significant improvement in the Pink Esthetic Scores was seen at the final
follow-up (mean PES 11.50), as compared to the baseline (mean PES 10.27) (P5 .001).
Conclusions: In addition to a favorable implant success rate and peri-implant bony response, the
soft tissue levels and overall aesthetics around single immediately placed and restored implants
can also be maintained in the mid-long term.
K E YWORD S
aesthetics, dental implants, immediate placement and restoration, osseointegration, soft tissue
1 | INTRODUCTION
Implant dentistry has progressed considerably since its introduction,
with modifications and enhancements being made to the surgical tech-
niques, restorative protocols, and the implants themselves. The initial
delayed loading and placement protocols1,2 have been modified to
expedite the treatment process. These modified protocols (immediate
placement and immediate loading) have been successfully applied in
both fully and partially edentulous patients.3,4 Additionally, immediate
implant placement has been combined with immediate restoration to
eliminate the load free healing period. Since first reported,5 the imme-
diate placement and restoration (IPR) technique has been recognized
as a viable treatment modality for partially edentulous situations.6
The nature of IPR treatment makes it particularly suited to implant
treatment in the anterior maxilla. Therefore, the focus has now shifted
from hard tissue and osseointegration outcomes to the aesthetic and
694 | VC 2017Wiley Periodicals, Inc. wileyonlinelibrary.com/journal/cid Clin Implant Dent Relat Res. 2017;19:694–702.
Received: 29 December 2016 | Revised: 19 March 2017 | Accepted: 3 April 2017
DOI: 10.1111/cid.12487OR I G I N A L A R T I C L E
Immediate implant placement and restoration in the anteriormaxilla: Tissue dimensional changes after 2-5 year follow up
Himanshu Arora, MDS1 | Nabil Khzam, DClinDent2 | David Roberts, MDSc3 |
William L Bruce, MDSc3 | Saso Ivanovski, MDSc, PhD1
1School of Dentistry and Oral Health,
Griffith University, Gold Coast, Queensland,
Australia2Private practice, Perth, Western Australia,
Australia3Private practice, Brisbane, Queensland,
Australia
CorrespondenceSaso Ivanovski, School of Dentistry and
Oral Health, Griffith Health Centre, Griffith
University - Gold Coast Campus, Parklands
Drive, Queensland 4222, Australia.
Email: [email protected]
Abstract
Background: Immediate implant placement followed by an immediate restoration has proven to
be a viable technique in the anterior maxillary region.
Purpose: This prospective study evaluated the mid-long term (2-5 years) tissue changes around
immediately placed and restored implants in the anterior maxilla using flapless surgery and simulta-
neous hard tissue augmentation.
Materials and methods: Thirty AstraTech implants were immediately placed in 30 patients, fol-
lowed by the delivery of an immediate provisional restoration on the same day. All participating
30 patients underwent the same treatment strategy that involved flapless removal of a failing max-
illary anterior tooth, immediate implant placement, simultaneous augmentation with a
deproteinized particulate xenograft, followed by the connection of a screw-retained provisional
restoration. Radiographs and photographs were used to measure hard and soft tissue changes.
Aesthetic evaluation was performed using the Pink Esthetic Score (PES).
Results: All implants remained osseointegrated during the follow up period of 2-5 years (mean
47615 months). Twelve of the thirty patients completed the 5 year follow up. Radiographic eval-
uation revealed average gains in bone levels of 0.18 and 0.34 mm mesially and distally,
respectively. Soft tissue evaluation showed a mean tissue loss of 0.0560.64 mm and 0.166
0.63 mm at the mesial and distal papillae, respectively, while mid-facial mucosal recession was
0.2960.74 mm. A significant improvement in the Pink Esthetic Scores was seen at the final
follow-up (mean PES 11.50), as compared to the baseline (mean PES 10.27) (P5 .001).
Conclusions: In addition to a favorable implant success rate and peri-implant bony response, the
soft tissue levels and overall aesthetics around single immediately placed and restored implants
can also be maintained in the mid-long term.
K E YWORD S
aesthetics, dental implants, immediate placement and restoration, osseointegration, soft tissue
1 | INTRODUCTION
Implant dentistry has progressed considerably since its introduction,
with modifications and enhancements being made to the surgical tech-
niques, restorative protocols, and the implants themselves. The initial
delayed loading and placement protocols1,2 have been modified to
expedite the treatment process. These modified protocols (immediate
placement and immediate loading) have been successfully applied in
both fully and partially edentulous patients.3,4 Additionally, immediate
implant placement has been combined with immediate restoration to
eliminate the load free healing period. Since first reported,5 the imme-
diate placement and restoration (IPR) technique has been recognized
as a viable treatment modality for partially edentulous situations.6
The nature of IPR treatment makes it particularly suited to implant
treatment in the anterior maxilla. Therefore, the focus has now shifted
from hard tissue and osseointegration outcomes to the aesthetic and
694 | VC 2017Wiley Periodicals, Inc. wileyonlinelibrary.com/journal/cid Clin Implant Dent Relat Res. 2017;19:694–702.
Received: 29 December 2016 | Revised: 19 March 2017 | Accepted: 3 April 2017
DOI: 10.1111/cid.12487
2017
30 patients 4 years (2-5)
1year 5 years
Distal - 0.1 (0.4) - 0.06 (0.6)
Mid Facial - 0.2 (0.4) - 0.2 (0.4)
Mesial - 0.3 (0.5) - 0.06 (0.6) OR I G I N A L A R T I C L E
Immediate implant placement and restoration in the anteriormaxilla: Tissue dimensional changes after 2-5 year follow up
Himanshu Arora, MDS1 | Nabil Khzam, DClinDent2 | David Roberts, MDSc3 |
William L Bruce, MDSc3 | Saso Ivanovski, MDSc, PhD1
1School of Dentistry and Oral Health,
Griffith University, Gold Coast, Queensland,
Australia2Private practice, Perth, Western Australia,
Australia3Private practice, Brisbane, Queensland,
Australia
CorrespondenceSaso Ivanovski, School of Dentistry and
Oral Health, Griffith Health Centre, Griffith
University - Gold Coast Campus, Parklands
Drive, Queensland 4222, Australia.
Email: [email protected]
Abstract
Background: Immediate implant placement followed by an immediate restoration has proven to
be a viable technique in the anterior maxillary region.
Purpose: This prospective study evaluated the mid-long term (2-5 years) tissue changes around
immediately placed and restored implants in the anterior maxilla using flapless surgery and simulta-
neous hard tissue augmentation.
Materials and methods: Thirty AstraTech implants were immediately placed in 30 patients, fol-
lowed by the delivery of an immediate provisional restoration on the same day. All participating
30 patients underwent the same treatment strategy that involved flapless removal of a failing max-
illary anterior tooth, immediate implant placement, simultaneous augmentation with a
deproteinized particulate xenograft, followed by the connection of a screw-retained provisional
restoration. Radiographs and photographs were used to measure hard and soft tissue changes.
Aesthetic evaluation was performed using the Pink Esthetic Score (PES).
Results: All implants remained osseointegrated during the follow up period of 2-5 years (mean
47615 months). Twelve of the thirty patients completed the 5 year follow up. Radiographic eval-
uation revealed average gains in bone levels of 0.18 and 0.34 mm mesially and distally,
respectively. Soft tissue evaluation showed a mean tissue loss of 0.0560.64 mm and 0.166
0.63 mm at the mesial and distal papillae, respectively, while mid-facial mucosal recession was
0.2960.74 mm. A significant improvement in the Pink Esthetic Scores was seen at the final
follow-up (mean PES 11.50), as compared to the baseline (mean PES 10.27) (P5 .001).
Conclusions: In addition to a favorable implant success rate and peri-implant bony response, the
soft tissue levels and overall aesthetics around single immediately placed and restored implants
can also be maintained in the mid-long term.
K E YWORD S
aesthetics, dental implants, immediate placement and restoration, osseointegration, soft tissue
1 | INTRODUCTION
Implant dentistry has progressed considerably since its introduction,
with modifications and enhancements being made to the surgical tech-
niques, restorative protocols, and the implants themselves. The initial
delayed loading and placement protocols1,2 have been modified to
expedite the treatment process. These modified protocols (immediate
placement and immediate loading) have been successfully applied in
both fully and partially edentulous patients.3,4 Additionally, immediate
implant placement has been combined with immediate restoration to
eliminate the load free healing period. Since first reported,5 the imme-
diate placement and restoration (IPR) technique has been recognized
as a viable treatment modality for partially edentulous situations.6
The nature of IPR treatment makes it particularly suited to implant
treatment in the anterior maxilla. Therefore, the focus has now shifted
from hard tissue and osseointegration outcomes to the aesthetic and
694 | VC 2017Wiley Periodicals, Inc. wileyonlinelibrary.com/journal/cid Clin Implant Dent Relat Res. 2017;19:694–702.
Received: 29 December 2016 | Revised: 19 March 2017 | Accepted: 3 April 2017
DOI: 10.1111/cid.12487OR I G I N A L A R T I C L E
Immediate implant placement and restoration in the anteriormaxilla: Tissue dimensional changes after 2-5 year follow up
Himanshu Arora, MDS1 | Nabil Khzam, DClinDent2 | David Roberts, MDSc3 |
William L Bruce, MDSc3 | Saso Ivanovski, MDSc, PhD1
1School of Dentistry and Oral Health,
Griffith University, Gold Coast, Queensland,
Australia2Private practice, Perth, Western Australia,
Australia3Private practice, Brisbane, Queensland,
Australia
CorrespondenceSaso Ivanovski, School of Dentistry and
Oral Health, Griffith Health Centre, Griffith
University - Gold Coast Campus, Parklands
Drive, Queensland 4222, Australia.
Email: [email protected]
Abstract
Background: Immediate implant placement followed by an immediate restoration has proven to
be a viable technique in the anterior maxillary region.
Purpose: This prospective study evaluated the mid-long term (2-5 years) tissue changes around
immediately placed and restored implants in the anterior maxilla using flapless surgery and simulta-
neous hard tissue augmentation.
Materials and methods: Thirty AstraTech implants were immediately placed in 30 patients, fol-
lowed by the delivery of an immediate provisional restoration on the same day. All participating
30 patients underwent the same treatment strategy that involved flapless removal of a failing max-
illary anterior tooth, immediate implant placement, simultaneous augmentation with a
deproteinized particulate xenograft, followed by the connection of a screw-retained provisional
restoration. Radiographs and photographs were used to measure hard and soft tissue changes.
Aesthetic evaluation was performed using the Pink Esthetic Score (PES).
Results: All implants remained osseointegrated during the follow up period of 2-5 years (mean
47615 months). Twelve of the thirty patients completed the 5 year follow up. Radiographic eval-
uation revealed average gains in bone levels of 0.18 and 0.34 mm mesially and distally,
respectively. Soft tissue evaluation showed a mean tissue loss of 0.0560.64 mm and 0.166
0.63 mm at the mesial and distal papillae, respectively, while mid-facial mucosal recession was
0.2960.74 mm. A significant improvement in the Pink Esthetic Scores was seen at the final
follow-up (mean PES 11.50), as compared to the baseline (mean PES 10.27) (P5 .001).
Conclusions: In addition to a favorable implant success rate and peri-implant bony response, the
soft tissue levels and overall aesthetics around single immediately placed and restored implants
can also be maintained in the mid-long term.
K E YWORD S
aesthetics, dental implants, immediate placement and restoration, osseointegration, soft tissue
1 | INTRODUCTION
Implant dentistry has progressed considerably since its introduction,
with modifications and enhancements being made to the surgical tech-
niques, restorative protocols, and the implants themselves. The initial
delayed loading and placement protocols1,2 have been modified to
expedite the treatment process. These modified protocols (immediate
placement and immediate loading) have been successfully applied in
both fully and partially edentulous patients.3,4 Additionally, immediate
implant placement has been combined with immediate restoration to
eliminate the load free healing period. Since first reported,5 the imme-
diate placement and restoration (IPR) technique has been recognized
as a viable treatment modality for partially edentulous situations.6
The nature of IPR treatment makes it particularly suited to implant
treatment in the anterior maxilla. Therefore, the focus has now shifted
from hard tissue and osseointegration outcomes to the aesthetic and
694 | VC 2017Wiley Periodicals, Inc. wileyonlinelibrary.com/journal/cid Clin Implant Dent Relat Res. 2017;19:694–702.
Received: 29 December 2016 | Revised: 19 March 2017 | Accepted: 3 April 2017
DOI: 10.1111/cid.12487
2017
protocol in 30 patients (9 males and 21 females) with an age range of
20-78 years. Sixteen implants replaced central incisors, 12 replaced lat-
eral incisors, and 2 implants were placed in the canine region. The rea-
sons for tooth failure were recorded as fracture (21 cases), endodontic
failure (7 cases), and root resorption (2 cases). Implants placed had
diameters ranging from 3.5 to 5.0 mm and length ranging from 11 to
15 mm. After a mean postoperative period of 48 months (range: 2-5
years), all implants were stable with no loss of osseointegration result-
ing in a cumulative implant survival rate of 100%.
3.1 | Hard tissue measurements
Bone levels around the implants showed an overall gain in bone height
at the final follow up when compared to baseline. Mesial bone levels
showed a mean gain of 0.1861.38 mm (P5 .85), while distal bone lev-
els showed a mean gain of 0.3461.40 mm (P5 .22). Figure 2 shows
the frequency analysis of bone level changes mesially and distally.
Bone changes ranged from >2 mm mean loss (3%) to mean gains of
>2 mm (10%) with most of the values lying (30%) between 0.5 mm
loss to 0.5 mm gain (Figure 2).
3.2 | Soft tissue measurements
After a follow-up period of 2-5 years, the mesial and distal papillae
showed a mean recession of 0.0560.64 mm and 0.1660.63 mm,
respectively, while mid-facial mucosal margin showed a mean recession
of 0.2960.74 mm, with no value reaching statistical significance. A
frequency analysis of the soft tissue dimensional changes from baseline
to the final follow-up is shown in Figure 3. Most of the changes were
between 0.5 mm of tissue loss to 0.5 mm tissue gain (Figure 1).
Advanced soft tissue recession (defined as >1 mm by)22 was identified
in the mid-facial mucosa of four patients (13%). Further evaluation
revealed that two of these four patients had no soft tissue level dis-
crepancy when compared to the contralateral natural teeth (Figure 4).
To evaluate the effect of the IPR protocol on the soft tissue
changes in the long-term, a comparison between the 1- and 5-year
FIGURE 3 Frequency analysis of soft tissue changes frombaseline to final follow-up
FIGURE 4 Case with “advanced” mid-facial recession (>1 mm). (A) Pre-extraction view of maxillary right lateral incisor, (B) advanced mid-facial recession evident after definitive restoration, (C) comparison with the contralateral natural tooth reveals no discrepancy between thesoft tissue levels after 1 year, (D) soft tissue levels maintained after 5 years
FIGURE 2 Bone level changes from baseline to final follow-up
ARORA ET AL. | 697
30 patients 4 years (2-5)
OR I G I N A L A R T I C L E
Immediate implant placement and restoration in the anteriormaxilla: Tissue dimensional changes after 2-5 year follow up
Himanshu Arora, MDS1 | Nabil Khzam, DClinDent2 | David Roberts, MDSc3 |
William L Bruce, MDSc3 | Saso Ivanovski, MDSc, PhD1
1School of Dentistry and Oral Health,
Griffith University, Gold Coast, Queensland,
Australia2Private practice, Perth, Western Australia,
Australia3Private practice, Brisbane, Queensland,
Australia
CorrespondenceSaso Ivanovski, School of Dentistry and
Oral Health, Griffith Health Centre, Griffith
University - Gold Coast Campus, Parklands
Drive, Queensland 4222, Australia.
Email: [email protected]
Abstract
Background: Immediate implant placement followed by an immediate restoration has proven to
be a viable technique in the anterior maxillary region.
Purpose: This prospective study evaluated the mid-long term (2-5 years) tissue changes around
immediately placed and restored implants in the anterior maxilla using flapless surgery and simulta-
neous hard tissue augmentation.
Materials and methods: Thirty AstraTech implants were immediately placed in 30 patients, fol-
lowed by the delivery of an immediate provisional restoration on the same day. All participating
30 patients underwent the same treatment strategy that involved flapless removal of a failing max-
illary anterior tooth, immediate implant placement, simultaneous augmentation with a
deproteinized particulate xenograft, followed by the connection of a screw-retained provisional
restoration. Radiographs and photographs were used to measure hard and soft tissue changes.
Aesthetic evaluation was performed using the Pink Esthetic Score (PES).
Results: All implants remained osseointegrated during the follow up period of 2-5 years (mean
47615 months). Twelve of the thirty patients completed the 5 year follow up. Radiographic eval-
uation revealed average gains in bone levels of 0.18 and 0.34 mm mesially and distally,
respectively. Soft tissue evaluation showed a mean tissue loss of 0.0560.64 mm and 0.166
0.63 mm at the mesial and distal papillae, respectively, while mid-facial mucosal recession was
0.2960.74 mm. A significant improvement in the Pink Esthetic Scores was seen at the final
follow-up (mean PES 11.50), as compared to the baseline (mean PES 10.27) (P5 .001).
Conclusions: In addition to a favorable implant success rate and peri-implant bony response, the
soft tissue levels and overall aesthetics around single immediately placed and restored implants
can also be maintained in the mid-long term.
K E YWORD S
aesthetics, dental implants, immediate placement and restoration, osseointegration, soft tissue
1 | INTRODUCTION
Implant dentistry has progressed considerably since its introduction,
with modifications and enhancements being made to the surgical tech-
niques, restorative protocols, and the implants themselves. The initial
delayed loading and placement protocols1,2 have been modified to
expedite the treatment process. These modified protocols (immediate
placement and immediate loading) have been successfully applied in
both fully and partially edentulous patients.3,4 Additionally, immediate
implant placement has been combined with immediate restoration to
eliminate the load free healing period. Since first reported,5 the imme-
diate placement and restoration (IPR) technique has been recognized
as a viable treatment modality for partially edentulous situations.6
The nature of IPR treatment makes it particularly suited to implant
treatment in the anterior maxilla. Therefore, the focus has now shifted
from hard tissue and osseointegration outcomes to the aesthetic and
694 | VC 2017Wiley Periodicals, Inc. wileyonlinelibrary.com/journal/cid Clin Implant Dent Relat Res. 2017;19:694–702.
Received: 29 December 2016 | Revised: 19 March 2017 | Accepted: 3 April 2017
DOI: 10.1111/cid.12487OR I G I N A L A R T I C L E
Immediate implant placement and restoration in the anteriormaxilla: Tissue dimensional changes after 2-5 year follow up
Himanshu Arora, MDS1 | Nabil Khzam, DClinDent2 | David Roberts, MDSc3 |
William L Bruce, MDSc3 | Saso Ivanovski, MDSc, PhD1
1School of Dentistry and Oral Health,
Griffith University, Gold Coast, Queensland,
Australia2Private practice, Perth, Western Australia,
Australia3Private practice, Brisbane, Queensland,
Australia
CorrespondenceSaso Ivanovski, School of Dentistry and
Oral Health, Griffith Health Centre, Griffith
University - Gold Coast Campus, Parklands
Drive, Queensland 4222, Australia.
Email: [email protected]
Abstract
Background: Immediate implant placement followed by an immediate restoration has proven to
be a viable technique in the anterior maxillary region.
Purpose: This prospective study evaluated the mid-long term (2-5 years) tissue changes around
immediately placed and restored implants in the anterior maxilla using flapless surgery and simulta-
neous hard tissue augmentation.
Materials and methods: Thirty AstraTech implants were immediately placed in 30 patients, fol-
lowed by the delivery of an immediate provisional restoration on the same day. All participating
30 patients underwent the same treatment strategy that involved flapless removal of a failing max-
illary anterior tooth, immediate implant placement, simultaneous augmentation with a
deproteinized particulate xenograft, followed by the connection of a screw-retained provisional
restoration. Radiographs and photographs were used to measure hard and soft tissue changes.
Aesthetic evaluation was performed using the Pink Esthetic Score (PES).
Results: All implants remained osseointegrated during the follow up period of 2-5 years (mean
47615 months). Twelve of the thirty patients completed the 5 year follow up. Radiographic eval-
uation revealed average gains in bone levels of 0.18 and 0.34 mm mesially and distally,
respectively. Soft tissue evaluation showed a mean tissue loss of 0.0560.64 mm and 0.166
0.63 mm at the mesial and distal papillae, respectively, while mid-facial mucosal recession was
0.2960.74 mm. A significant improvement in the Pink Esthetic Scores was seen at the final
follow-up (mean PES 11.50), as compared to the baseline (mean PES 10.27) (P5 .001).
Conclusions: In addition to a favorable implant success rate and peri-implant bony response, the
soft tissue levels and overall aesthetics around single immediately placed and restored implants
can also be maintained in the mid-long term.
K E YWORD S
aesthetics, dental implants, immediate placement and restoration, osseointegration, soft tissue
1 | INTRODUCTION
Implant dentistry has progressed considerably since its introduction,
with modifications and enhancements being made to the surgical tech-
niques, restorative protocols, and the implants themselves. The initial
delayed loading and placement protocols1,2 have been modified to
expedite the treatment process. These modified protocols (immediate
placement and immediate loading) have been successfully applied in
both fully and partially edentulous patients.3,4 Additionally, immediate
implant placement has been combined with immediate restoration to
eliminate the load free healing period. Since first reported,5 the imme-
diate placement and restoration (IPR) technique has been recognized
as a viable treatment modality for partially edentulous situations.6
The nature of IPR treatment makes it particularly suited to implant
treatment in the anterior maxilla. Therefore, the focus has now shifted
from hard tissue and osseointegration outcomes to the aesthetic and
694 | VC 2017Wiley Periodicals, Inc. wileyonlinelibrary.com/journal/cid Clin Implant Dent Relat Res. 2017;19:694–702.
Received: 29 December 2016 | Revised: 19 March 2017 | Accepted: 3 April 2017
DOI: 10.1111/cid.12487
2017
reported the incidence of advanced mid-facial recession in 8% of
cases (2/25 patients).22 Another study by the same group evaluating
the effect of the IPR technique found early aesthetic complications
(advanced mid-facial recession) in 5/22 cases after 3 months, which
were treated with a connective tissue graft.37 After a follow-up of 5
years, the cases treated with the soft tissue graft maintained
acceptable soft tissue levels, but the authors observed a late
advanced recession in three other cases leading to a high aesthetic
complication rate.9 In our study, advanced recession was seen in
13% of cases (four patients), which is in accordance with the results
from previous studies.12 No soft tissue grafting was performed in
any of the patients included in the current study. It is noteworthy
that out of these four cases with advanced recession, two had no
discrepancy when compared to the contralateral tooth at the final
follow-up and were given a score of 2 for the respective PES param-
eter (Figure 3). This is an interesting finding as sometimes gingival
recession can be deliberately induced by the prosthodontist to cre-
ate harmony with the soft tissue level on the contralateral tooth,
TABLE 2 PES change from baseline to final follow-up
Parameter Score Preoperative Final follow-up P value
Mesial papilla 0 0 0 .10
1 8 62 22 24
Distal papilla 0 1 1 .25
1 4 12 25 28
Midfacial level 0 3 2 .03
1 12 112 15 17
Midfacial contour 0 3 0 .01
1 16 132 11 17
Alveolar processde!ciency
0 0 1 .09
1 9 92 21 20
Soft tissue color 0 8 1 .007
1 9 132 13 16
Soft tissue texture 0 5 0 .001
1 14 102 11 20
Overall PES Mean (SD) {Median (IQR)} [Range] 10.27 (2.13) 11.50 (1.36) .001
{11.0 (9.0-12.0)} {12.0 (11.0-12.25)}[5-13] [8-13]
FIGURE 5 Pink esthetic score results over the time course of the study. (A) Cumulative percent scores for baseline and final follow-up, (B)average scores for individual variables
ARORA ET AL. | 699
11.5 Post treatment
10.2 pre treatment
30 patients 4 years (2-5)
Immediate Implant?
With Flap:3
Compromise soft tissue architecture
Socket and buccal augmentation (?)
Immediate Implant?
With Flap:
Immediate versus delayedimplant placement after anteriorsingle tooth extraction: the timingrandomized controlled clinical trialTonetti MS, Cortellini P, Graziani F, Cairo F, Lang NP, Abundo R, Conforti GP,Marquardt S, Rasperini G, Silvestri M, Wallkamm B, Wetzel A. Immediate versusdelayed implant placement after anterior single tooth extraction: the timingrandomised controlled clinical trial. J Clin Periodontol 2017; 44: 215–224. doi: 10.1111/jcpe.12666.
AbstractAim: To compare need for bone augmentation, surgical complications, periodontal,radiographic, aesthetic and patient reported outcomes in subjects receiving implantplacement at the time of extraction (Immediate Implant) or 12 weeks thereafter.Methods: Subjects requiring single tooth extraction in the anterior and premolarareas were recruited in seven private practices. Implant position and choice ofplatform were restoratively driven. Measurements were performed by calibratedand masked examiners.Results: IMI was unfeasible in 7.5% of cases. One hundred and 24 subjects wererandomized. One implant was lost in the IMI group. IMI required bone augmen-tation in 72% of cases compared with 43.9% for delayed (p = 0.01), while woundfailure occurred in 26.1% and 5.3% of cases, respectively (p = 0.02). At 1 year,IMI had deeper probing depths (4.1 ! 1.2 mm versus 3.3 ! 1.1 mm, p < 0.01). Atrend for greater radiographic bone loss was observed at IMI over the initial 3-year period (p-trend < 0.01). Inadequate pink aesthetic scores were obtained in19% of delayed and in 42% of IMI implant cases (p = 0.03). No differences inpatient reported outcomes were observed.Conclusions: Immediate implant placement should not be recommended whenaesthetics are important, IMI should be limited to selected cases. Longer follow-up is needed to assess differences in complication rates.
Maurizio S. Tonetti1,2,Pierpaolo Cortellini1,Filippo Graziani1, Francesco Cairo1,Niklaus P. Lang1, Roberto Abundo1,Gian Paolo Conforti1,Siegfried Marquardt1,Giulio Rasperini1,Maurizio Silvestri1, Beat Wallkamm1
and Anton Wetzel1
1European Research Group onPeriodontology, Genova, Italy; 2Departmentof Periodontology, Hong Kong University,Hong Kong SAR, China
Key words: bone augmentation; dentalimplants; human; randomized controlledclinical trial; tooth extraction
Accepted for publication 1 December 2016
Tooth extractions requiring pros-thetic replacement represent a majorindication for dental implant
placement. Immediate installation atthe time of extraction offers poten-tial advantages for both practitioners
and patients. It allows a decrease intreatment time and may result in anincrease in patient satisfaction. Some
Conflict of interest and source of funding statementThe authors have stated explicitly that there are no conflicts of interest in connection with this article.This study was sponsored by the European Research Group on Periodontology (ERGOPerio). The study was financially sup-ported in part by an unrestricted grant from Thommen Medical AG, Switzerland. The employed regenerative materials wereprovided at no cost by Geistlich AG, Switzerland. This research was initiated by the investigators who independently per-formed all phases of the study including protocol development, experimental procedures, data analysis and reporting. Anearly report of this trial received the 2010 clinical research award of the European Association of Osseointegration.
© 2016 The Authors. Journal of Clinical Periodontology Published by John Wiley & Sons Ltd. 215This is an open access article under the terms of the Creative Commons Attribution-NonCommercial License,which permits use, distribution and reproduction in any medium, provided the original work is properly cited andis not used for commercial purposes.
J Clin Periodontol 2017; 44: 215–224 doi: 10.1111/jcpe.12666
2017
the majority of cases had WESscores greater than the arbitrarily setclinical acceptability level in an aes-thetic site. PES scores differed com-paring immediate and delayedimplants: arbitrarily set inadequatePES was obtained in 19% of delayedimplant cases and in 42% of imme-diate implant cases. The differencewas statistically significant (Chi-squared test, p = 0.03).
Discussion
This study shows the possibility tocomplete an ethically challengingtrial on a controversial topic inimplant dentistry with an appropri-ate control of potential sources ofbias. These results contribute to clar-ification of the relative merits ofimmediate and delayed implantplacement after single tooth extrac-tion in the anterior portion of thedentition.
The results challenge a series ofwidely held paradigms. Undisturbedhealing of extraction sockets withoutthe application of any ridge preser-vation/augmentation approachallowed restoratively guided implantpositioning in the control group. Insome cases a total buccal bone thick-ness >1.5 mm was obtained with theaddition of bone augmentation
materials at the time of implantplacement, in others without it. Aninteresting result was that, compar-ing immediate implant placement atthe time of extraction with delayedimplant placement, bone augmenta-tion was more frequently needed atimmediate implant placement. Thisresult may be partly due to the deci-sion to choose the implant diameterbased upon the cervical dimension ofthe tooth that needed to be replacedrather than selection based upon thesize of the alveolus. The lower fre-quency of bone augmentation in thedelayed implant seems to provide animportant argument for selection ofthis approach as bone augmentationincreases both the cost and the com-plexity of the procedure. Anotherimportant element related to theconditions of the alveoli after extrac-tion. In this trial significant loss ofboth the buccal and palatal wall waspresent and this increased the needfor bone augmentation at immediateimplant sites. The observation thatbone augmentation was less fre-quently needed in delayed placementchallenges the current paradigms ofthe significance of spontaneous alve-olar bone resorption during extrac-tion socket healing (Van der Weijdenet al. 2009). Recent research synthe-sis on interventions to preserve
extraction alveoli recognizes both theeffectiveness of the preservation/re-construction procedures (Avila-Ortizet al. 2014) and questions their clini-cal relevance (Atieh et al. 2015).More high quality research is neededto convincingly answer these ques-tions.
The issues related to timing ofimplant placement are complicatedby the lack of consensus on effectiveand established procedures and bythe wide array of confounders thathave played a role in previous trials.In this study we decided to use a flapat the time of extraction and implantplacement to be able to standardizesurgery in the two groups. Raising aflap will undoubtedly affect the heal-ing of the site. This has been shownin both preclinical (Blanco et al.2008) and clinical studies (Cosynet al. 2016, Stoupel et al. 2016). Thechoice not to immediately place atemporary reconstruction may havefurther influenced the results (Slagteret al. 2015, Stoupel et al. 2016).
Wound failure was observed at26% of immediate implant place-ment sites and almost five timesmore frequently than in the delayedgroup. It mostly related to relativelyminor complications that can beattributed to the challenge of achiev-ing primary wound closure. This has
Fig. 5. Twelve-month post-crown insertion comparison of pink and white aesthetic scores at immediate and delayed implants.Twelve month soft tissue (pink) aesthetic score (PES, blue box plot) and crown (white) aesthetic score (WES, red box plot) wereevaluated by two independent and calibrated examiners using photographs and study models as indicated by Belser et al. (2009).The red vertical dashed line highlights the level of clinical acceptability arbitrarily defined according to Belser et al. (2009). Out-comes above 6 have been considered clinically acceptable by a professional assessment.
© 2016 The Authors. Journal of Clinical Periodontology Published by John Wiley & Sons Ltd.
222 Tonetti et al.
(p < 0.01). Over the following36 months, immediate implantsshowed a statistically significanttrend for more RBL loss comparedto delayed implants (p fortrend = 0.03). No significant changesin RBL were observed comparingcrown insertion with 12, 24 and36 months in the delayed implantgroup.
Aesthetic outcomes
Figure S3 reports the dimensions ofthe keratinized tissue before theextraction, at the time of prostheticreconstruction and 12 months laterat the implant site (panel a) and atthe neighbouring teeth (panel b).The band of keratinized tissue
Table 1. Study population
Immediate Delayed Significance
Age (years) 50 ! 14 55 ! 13 p = 0.076Females 63% 73% p = 0.376Smokers 15% 15% p = 0.983FMPS 20 ! 16 17 ! 14 p = 0.333FMBS 11 ! 11 12 ! 16 p = 0.875
FMBS, full mouth bleeding score; FMPS, full mouth plaque score.Means ! SD.
Table 2. Comparison of surgical outcomes in the test and control groups
Immediate (%) Delayed (%) Significance
Need for bone augmentation 72 43.9 p = 0.01Primary wound closure 61.7 82.1 p = 0.05Wound failure 26.1 5.3 p = 0.02Patient post-op complaints 18.9 4.9 p = 0.06
Fig. 2. Bone measurements after implant placement. All measurements were taken using the implant shoulder as the reference pointto the nearest mm using a UNC-15 periodontal probe. Implant shoulder to bottom of the defect = depth of bone defect; Implantshoulder to bone crest – 1.5 mm = vertical implant position; implant shoulder to bone crest in a horizontal direction = width ofbone gap. (Panel a) Measurement scheme. (Panel b) Vertical implant position with reference to the mesio-distal bone level of thetwo adjacent teeth. (Panel c) Horizontal width of the implant to alveolar bone crest defect. At immediate implants, this alsoincludes the horizontal gap between the implant surface and the alveolar crest. At delayed implants it includes the buccal or lingualdefect with respect to the ideal bone contour. (Panel d) Depth of the vertical component of the defect around the restorativelyplaced implant. In all panels the measurements are taken at four points around the implant: mesial, distal, mid-buccal and mid-lin-gual. All data displayed are box-plots. p-values are reported for test versus control treatments and t-test after Bonferroni correctionfor multiple testing.
© 2016 The Authors. Journal of Clinical Periodontology Published by John Wiley & Sons Ltd.
220 Tonetti et al.

Immediate Implant?
With Flap:
Extraction
Yes No
Anterior Maxilla: The art and the Science Nikos Mattheos. 2019
Buser et al 2017
Immediate Implant
Indications for Flapless Immediate Implant ?
?
Prosthetic Manipulation?
Immediate implant?
Ridge Preservation?
How can we overcome the compromised Bone ?
Tissue Left CenterRigh
tMea
Bone 34 34 40 36Fibrous 30 22 18 23.33
Materials 36 44 42 40.67Total 100 100 100 100
Alveolar ridge preservation with guided bone regeneration and a synthetic bone substitute or a bovine-derived xenograft: a randomized, controlled clinical trial Mardas et al 2010 Clin Oral Implants Res. 2010: 21:688-98.
26 patients » 13 SBC » 13 BioOss
Alveolar ridge preservation with guided bone regeneration and a synthetic bone substitute or a bovine-derived xenograft: a randomized, controlled clinical trial Mardas et al 2010 Clin Oral Implants Res. 2010: 21:688-98.
New bone apically and middle part of socket but centrally and coronally graft particles surrounded by dense connective tissue
Both biomaterials partially preserved the width and the interproximal bone height of alveolar ridge
9/13 in SBC group and 8/12 in DBBM group required additional simultaneous augmentatio

Will reduce horizontal and vertical bone resorbtion
Clinical image is not always corresponding to bone profile
delays healing
delays implant placement
compromises bone quality
might not eliminate need for second augmentation
cost
Implant Placement in the Aesthetic Zone
Checkpoint !Ridge Augmentation
Extraction
Yes No
Immediate Implant
Indications for Flapless Immediate
Implant ?
Place the implant ASAP?
Ridge Preservationa) young ageb) postponed implant treatment
No Yes
?
Anterior Maxilla: The art and the Science Nikos Mattheos, Hong Kong, 2018
Cone Beam CT
Use radio-opaque crown in a splint !
Use lip / cheek retractors !
Step 2: Diagnose !
Check the Height
Check the Width
Check the bone quality (?) and neighbouring anatomy
Step 3: Plan !
height
ideal Block GraftGBR

ideal
Width
favorable unfavorable
Width
unfavorable
Width
unfavorable
ideal
favorable
Width If A or B or C is (1 out of 3):
then GBR
If A , B and C is :
then GBR
If A , B and C is : then Block Graft
A
B
C
BLX
C
B
A
Width If A or B or C is (1 out of 3):
then GBR
If A , B and C is :
then GBR
If A , B and C is : then Block Graft
A
B
C
BLX

Cone Beam CT
Use radio-opaque crown in a splint !
Use lip / cheek retractors !
Step 2: Diagnose !
Cone Beam CT
Januario et al 2008 Use radio-opaque crown in a splint !
Use lip / cheek retractors !
Check the Height
Check the Width
Check the bone quality (?) and neighbouring anatomy
Step 3: Plan !
height
ideal Block GraftGBR
ideal
Width
favorable

unfavorable
Width
unfavorable
Width
unfavorable
ideal favorable
Width If A or B or C is (1 out of 3):
then GBR
If A , B and C is :
then GBR
If A , B and C is : then Block Graft
A
B
C
BLX
C
B
A
Width If A or B or C is (1 out of 3):
then GBR
If A , B and C is :
then GBR
If A , B and C is : then Block Graft
A
B
C
BLX
Immediate implants
GBR or CT
No GBR

A randomized controlled study comparing guided bone regeneration with connective tissue graft to re-establish convexity at the buccal aspect of single implants: a one-year CBCT analysis
Thomas De Bruyckere et al, J Clin Perio 2018
RCT21 patients1 year
GBR and CTG were equally effective
in re-establishing the convexity
Xenograft Ridge augmentation by applying bioresorbable membranes and deproteinized bovine bone mineral: a report of twelve consecutive cases. Clin Oral Implants Res 2008;19(January (1)):19–25.Hämmerle CH, Jung RE, Yaman D, Lang NP.
Bone width increased from 3.2 to 6.9 mm
10 months
Guided Bone Regeneration
Increase in clinical ridge width
Long term stability of ridge
High Survival
technique sensitive
Implant Placement in the Aesthetic Zone
Checkpoint ! Primary Stability?
2 stage augmentation
GBRa) sufficient height (palatal wall)b) primary b) ⅓ length fully in bone ORc) full length: bone contact > implant O!
Local Anatomy:
GBRBlock Graft
a) deficient height/widthb) gap <2-3 teeth
a) deficient widthb) self contained defect
a) deficient height/widthb) gap > 2-3 teeth
Non Resorbable
?
NoYes
Anterior Maxilla: The art and the Science Nikos Mattheos, Hong Kong, 2018
Extraction
Yes
Early Placement
No
2 stage augmentation
Immediate Implant
Yes
a) fully intact buccal bone b) thick wall (>1mm) c) thick gingival biotyped) no inflammatione) sufficient bone for primary stability (35Ncm)
Yes
GBR
a) sufficient height (palatal wall)b) primary b) ⅓ length fully in bone ORc) full length: bone contact > implant O!
Reduced diametre implants (2.9 - 3.3)
Ridge Preservation
No
a) young ageb) postponed implant treatment
Technology
Self-cutting / tapered implants
Increased Osseoconductivity surfaces
piezoelectric surgery
resorbable barrier membrane
xenograft / allograft
5-10 %
5%
60-70 %
10 - 15 % Block Graft
Local Anatomy:
GBR
a) deficient height/widthb) gap <2-3 teeth
a) deficient height/widthb) gap > 2-3 teeth
a) deficient widthb) self contained defect
Non Resorbable
Place the implant ASAP?
No
Primary Stability?
Indications for Immediate Flapless Implant ?
Anterior Maxilla: The art and the Science Nikos Mattheos, Hong Kong, 2019