Embed Size (px)
Citation preview

BONE HEALTH IN FEMALE ATHLETES
Dr. L.Hakemi
Internist
Sports Medicine Federation of IRAN
IN THE NAME OF GOD

OSTEOPOROSISone of the most common metabolic disorders
and the most common metabolic bone disease.
.

Osteoporotic Fx
• a principal cause of disability and death.
• Approx. 1.5 million fragility fractures (after trauma no greater than a fall from a standing height) occur annually in the US, and this number increases after 70s.

Exercise has positive effects on bone mass
Factors:
nutritionPhysical activityChronic diseasesMedications GENETIC
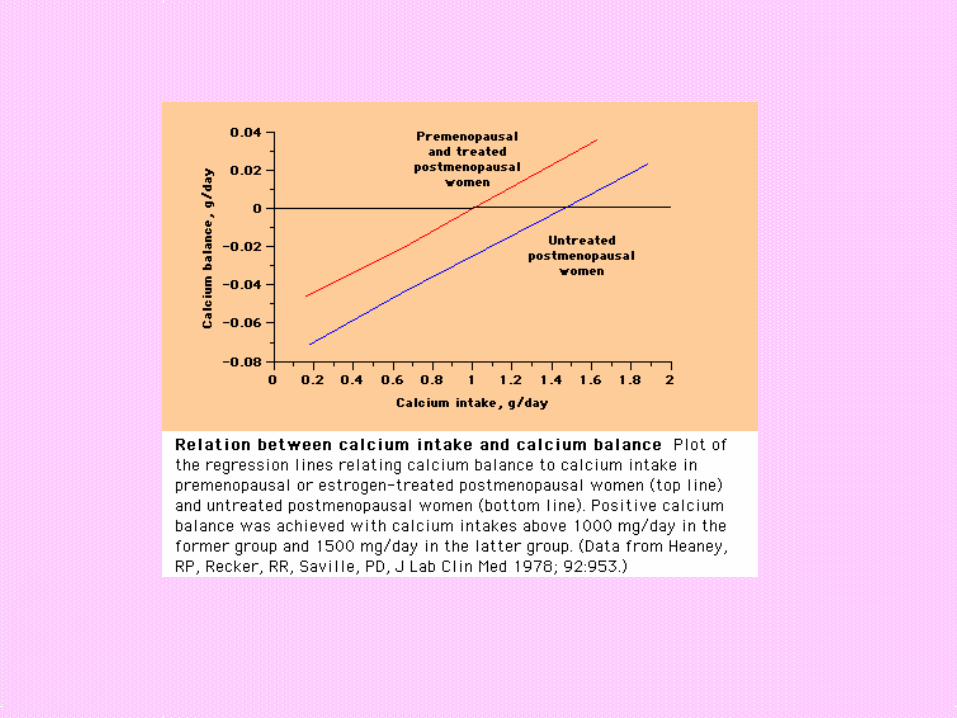

Calcium supplements protect against bone loss in postmenopausal women
Reid, IR, Ames, RW, Evans, MC, et al, N Engl J Med 1993; 328:460.

Calcium supplementation decreases hip bone loss during the winter
Storm, D, Eslin, R, Porter, E, et al, J Clin Endocrinol Metab 1998; 83:3817.

recommendationsDaily calcium
• at least 1000 mg in premenopausal women and men• 1500 mg in postmenopausal women who do not take
estrogen• the total intake of calcium should not routinely exceed 2000
mg/day.
•Vit D• 800 IU/day is for the elderly.

Estimation of calcium intake
•300 mg for each glass of milk or yogurt or 30 ml of cheese.
•Calcium absorption from vegetables such as spinach is less than dairy products.•Calcium from dietary sources probably is less likely to increase the risk of kidney stones.

In an osteoporotic patient contact sports should be avoided
Recommendations
1.Aerobic exercise
2.Balance exercises
3.Strength exercises
4.Flexibility exercises
5.Weight bearing exercises


Osteoporosis prevention must be started from childhood

• Osteoporosis originates early in life and bone mass development in childhood and adolescents influences the risk for bone fractures
• Daily physical activity in adolescence and young adulthood is positively related to bone mineral density in adulthood

• Risk of hip fracture in older females can be reduced by nearly 20% if adolescent and teenage girls engage in regular physical activity

• The amount of exercise a girl gets at 12-18 years age is very important in the density and strength of the proximal femur, and thus a crucial factor in the prevention of hip fractures due to osteoporosis in postmenopausal women
• Among 81 healthy white females exercise was more important than dietary calcium in reaching peak bone mineral density
• As the level of physical activity, fitness and lean body mass increases, BMD also increase


Female Athlete Triad
• Eating disorders/ Disordered eating
• Amenorrhea/ oligomenorrhea
• Osteoporosis/ osteopenia


DURING HEAVY EXERCISE, THE PULSATILE GNRH MAY DISAPPEAR AT THE HYPOTHALAMIC LEVEL

Prevalence
30-60% of elite female athletes
•Highest in: – Aesthetic– Endurance
• Mostly cross country skiersLean habitus
High power/ weight

• Adolescents with anorexia nervosa are often hypogonadal as well, and both causes contribute to reduced bone mass
• Age at onset and duration of anorexia correlate with bone mineral density


• Appropriately programmed exercise has salient effects on the development of healthy bones. However, delayed menarche may have adverse effects on the health of their bones and also on other systems in their body.
• Heavy exercise together with a diet that is low in calories puts the athlete at risk of developing delayed menarche.

Age at Menarche
Gymn/ Poland15.1-/+0.9Swim/ UK13.3-/+ 1.1
Gymn/ Switze14.5-/+1.2Tennis/ UK13.2 -/+ 1.4
Gymn/ Swed14.5-/+1.4Track/Poland12.3 -/+1.1
Gymn/ UK14.3 -/+ 1.4Track/ Hung12.6
Gymn/ Hung15.0 +/- 0.6Row/ Poland12.7 -/+ 0.9
Gymn/ world15.6 +/- 2.1Skate/ US14.2 -/+ 0.5
Eliteballet/ US15.4 -/+ 1.9Diving/ US13.6 +/- 1.1
Soccer/ US12.9 +/- 1.1
In 454 cases that were passed menarche age
mean of age at menarche: 158.2+/- 0.7 m. (13.18 yr)
HAKEMI, TORKAN, KABIR

• Earlier menarche was reported in :
• 1-lower height (p<0.001)
• 2-lower age at beginning exercise (p=0.019)
• 3-lesser number of sisters (p=0.007)
• 4-lesser number of brothers (p=0.003)
• 5-higher percent body fat (p=0.037)
• 6-higher body mass index (p=0.002)
• 7-residing mountain side regions (p=0.001)
HAKEMI, TORKAN, KABIR

Does exercise affect height?
• NATURAL SELECTION• GH SECRETION• ENERGY REQUIREMENTS• MACRO AND MICRONUTRIENT
REQUIREMENTS• AVOIDING APOPHYSIAL INJURIES• AVOIDING TRIAD• AVOIDING BANNED DRUGS

SPORTHT (CENTILE)
WT (CENTILE)
BASKETBALL
>=50>=50
SOCCER+/- 50+/- 50
ICE HOCKEY
+/- 5050
DISTANCE RUNS
+/- 50=<50
SPRINTS>=50>=50
SWIMMING50-9050-75
DIVING<50=<50
GYMNASTICS
<25<25
TENNIS+/-50>=50
FIGURE SKATING
10-2510-25
BALLET<5010-50
MALE FEMALESPORTHT
(CENTILE)WT
(CENTILE)
BASKETBALL
>=7550-75
VOLLEYBALL
7550-75
SOCCER5050
DISTANCE RUNS
>=50<50
SPRINTS>=50=<50
SWIMMING50-9050-75
DIVING=<5050
GYMNASTICS
=<1010-50
TENNIS>50+/-50
FIGURE SKATING
10-5010-50
BALLET=<5010-50

Overuse injuries
• Common overuse injuries include stress fractures, tendonitis, and bursitis.
• Female athletes are more susceptible • Two apparent reasons for this:• a lack of long-term preparation for
vigorous sports and• not beginning sports training until growth
spurt (typically 11-13), a time when musculoskeletal injury incidence is greater

Peak velocity of growth in bone mineral content lags nearly 1 year after peak height spurt, thus during this period the bones are somewhat fragile and more susceptible to injury

• Timing, duration and intensity of physical activity determines whether a positive or negative effect on bone mass density
• Excessive exercise may suppress hypothalamic- gonadal axis, cause primary or secondary amenorrhea and reduced bone mineral density.













![Practical Pharmacology [PRINT VERSION] from a (mostly) practical internist](https://img.pdfslide.us/doc/110x75/56649ee75503460f94bf7972/practical-pharmacology-print-version-from-a-mostly-practical-internist.jpg)