Embed Size (px)
Citation preview
Int. J. Oral Maxillofac. Surg. 1997; 26:428~134 Printed in Denmark. All rights reserved
Copyright �9 Munksgaard 1997
[ntemationaIJoumd of
Oral 8c Max~ofacial Surgery
ISSN 0901-5027
Bone grafting to the maxilla s nuses, nasal floor and anterior maxilla in the atrophic edentulous maxilla A tw0-stage technique
Stefan Lundgren 1, Elisabeth Nystr6m 1, Hans Nilson 2, Johan Gunne 2, Ove Lindhagen 3 Departments of 1Oral and Maxillofacial Surgery, and 2prosthetic Dentistry, Ume& University; 3Department of Plastic Surgery, Ume& University Hospital, Umef, Sweden
S. Lundgren, E. Nystrdm, H. Nilson, J. Gunne, O. Lindhagen." Bone graJiing to the maxillary sinuses, nasal floor and anterior maxilla in the atrophic edentulous maxilla. A two-stage technique. Int. J. Oral Maxillofac. Surg. 1997; 26: 428-434. �9 Munksgaard, 1997
Abstract. This study presents the results from 20 consecutive patients treated with an autogenous bone graft from the iliac crest. In ten patients the graft was placed in the maxillary sinuses and the floor of the nose (inlay group). Ten patients, in addition to the inlay graft, had a corticocancellous bone block secured with mini-screws to the anterior maxillary ridge (inlay/onlay group). Endosteal implants (BNnemark | were placed six months after surgery. A total of 136 implants were placed, of which eight failed to integrate during the six-month healing period. A further 15 implants were lost during the follow-up period. For the inlay group the average follow-up period was 22 months and for the inlay/ onlay group 19 months. Donor site morbidity was significantly less when iliac bone was harvested with a trephine (inlay group) than in patients treated with our routine procedure for bone harvesting (inlay/onlay group). Surgical technique, donor site morbidity, implant survival and patient acceptance are presented.
Key words: bone grafting; autogenous bone; iliac crest; maxilla; implants.
Accepted for publication 29 June 1997
The reconstruction of the severely re- sorbed edentulous maxilla with iliac crest bone grafts to accommodate end- osteal implants has been the subject of many studies. The full-arch onlay tech- niquO ,x4, bone grafting to the maxillary sinus floor 5,8,9 and grafting to the nasal cavity 7,9 are examples of techniques de- scribed in some of the recent publi- cations.
In some patients with severe maxil- lary atrophy (Class V and VI 2) a re- versed intermaxillary relation or an in- creased vertical d is tancebetween the jaws 3 may be the result. In other pa-
tients the final state of resorption re- sults in a thin remaining alveolar ridge, while some patients lose all vertical height of the alveolar process. Since re- construction with bone grafts and im- plants should aim to restore the facial morphology, the final state of resorp- tion should influence the surgical tech- nique selected, so that optimal results can be achieved, both functionally and aesthetically.
This study presents the results from 20 consecutively treated patients: the first ten patients were treated with an inlay bone graft in the maxillary sinus and the
nasal floor (inlay group), and the second ten with an inlay graft in combination with an onlay bone graft to the anterior maxilla (inlay/onlay group).
Material and methods
The inlay group included four women and six men with an average age of 57 years (range 46-70). The patients had been totally edentulous in the maxilla for an average of 29 years (range 240). A preoperative clinical examination and radiograms, including a panoramic radiograph, lateral tomograms and a cephalometric film revealed severe al- veolar atrophy (class VVI according to CA-
50
451 111 Inlay/onlay
40 [ ] nay
0 - - 4
~" 30 0
25 0
2o
e~ E 15
10
e~ E 5
Z 0
5 - - 9
35
10- -14 15--19
Bone height (mm) > 4 mm in width
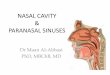
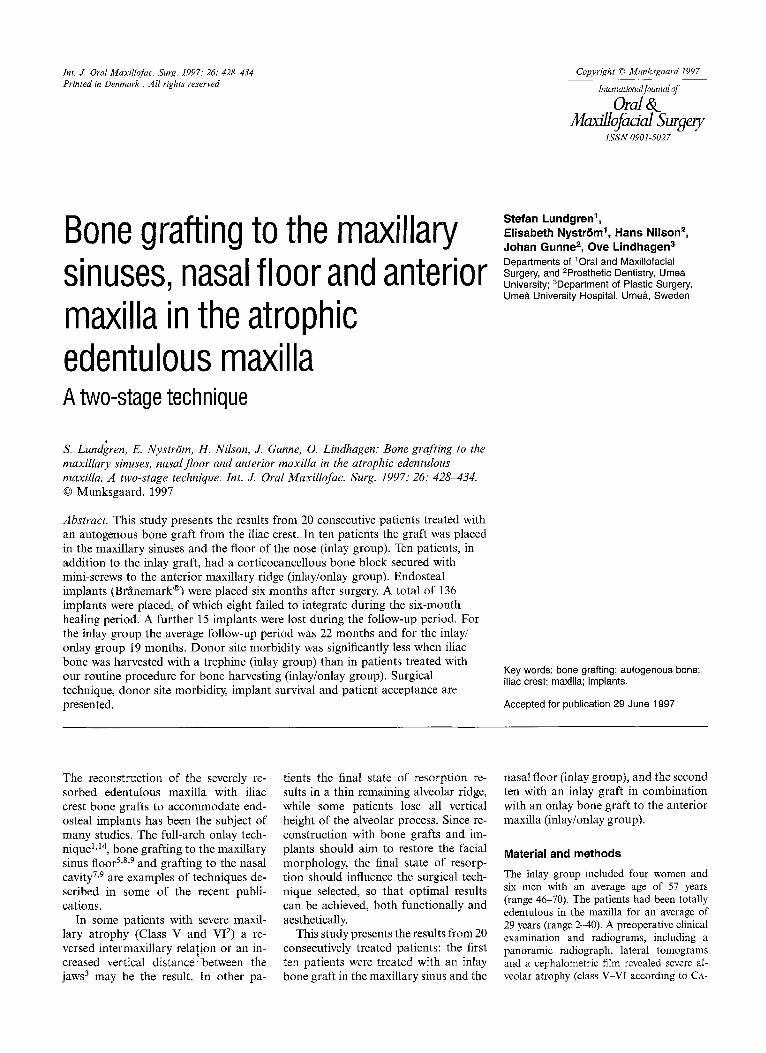
Fig. 1. Residual bone height with min. width of 4 mm in preoperative situation evaluated from lateral tomograms. Planned implant positions were indicated with lead spheres before the radiological investigation. Black bars: inlay/onlay group of patients. White bars: inlay group of patients.
WOOD & HOWELL 2, Fig. 1). One patient had previously lost six endosteal implants. One patient said that he smoked.
The inlay/onlay group included nine women and one man with an average age of 55 years (range 43-71). The patients had been totally edentulous in the maxilla for an average of 27 years (range 9 39). A preopera- tive clinical examination and radiograms re- vealed severe alveolar atrophy (class VI ac-
cording to CAWOOD & HOWELL 2, Fig. 1) with a normal sagittal intermaxillary relation but a reduced alveolar height in the anterior maxilla. Two patients had each lost six maxil- lary implants prior to the grafting procedure. Two patients were smokers, but one had stopped smoking before the treatment.
Surgery was performed under general an- aesthesia with oral endotracheal intubation. A local anaesthetic with a vasoconstrictor
Inlay/onlay grafting 499
was used for hemostasis. Three grams of ben- zylpenicillin were administered at the start of the operation. The left iliac crest was chosen as the donor site.
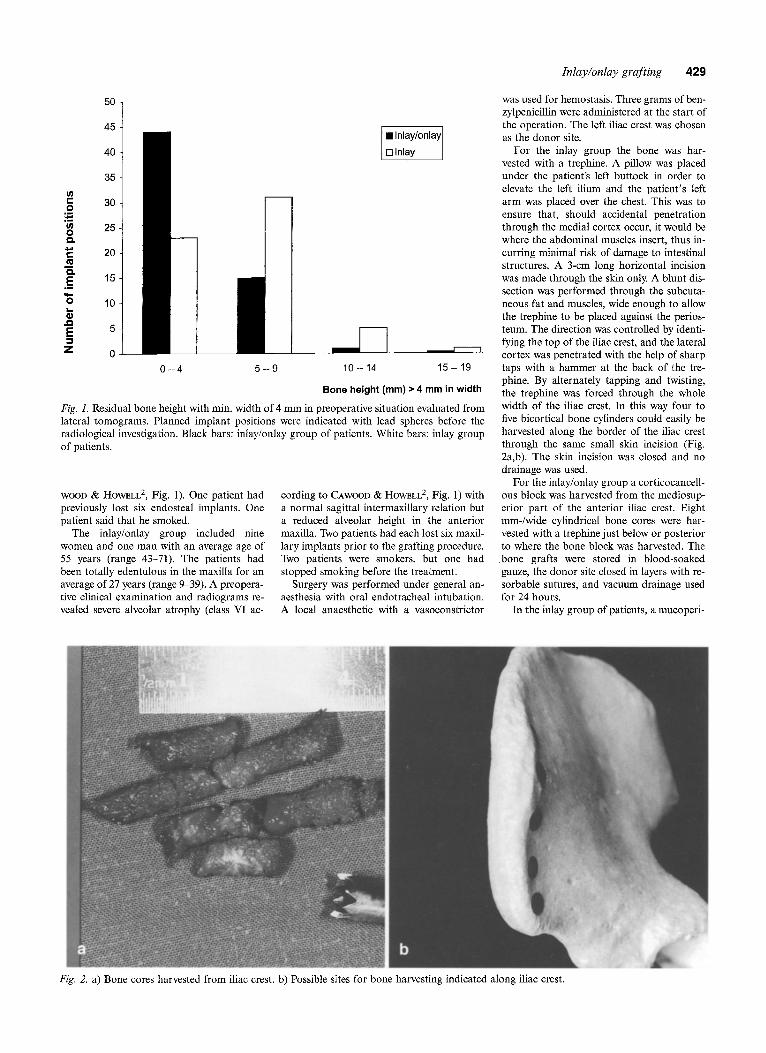
For the inlay group the bone was har- vested with a trephine. A pillow was placed under the patient's left buttock in order to elevate the left ilium and the patient 's left arm was placed over the chest. This was to ensure that, should accidental penetration through the medial cortex occur, it would be where the abdominal muscles insert, thus in- curring minimal risk of damage to intestinal structures. A 3-cm long horizontal incision was made through the skin only. A blunt dis- section was performed through the subcuta- neous fat and muscles, wide enough to allow the trephine to be placed against the perios- teum. The direction was controlled by identi- fying the top of the iliac crest, and the lateral cortex was penetrated with the help of sharp taps with a hammer at the back of the tre- phine. By alternately tapping and twisting, the trephine was forced through the whole width of the iliac crest. In this way four to five bicortical bone cylinders could easily be harvested along the border of the iliac crest through the same small skin incision (Fig. 2a,b). The skin incision was closed and no drainage was used.
For the inlay/onlay group a corticocancell- ous block was harvested from the mediosup- erior part of the anterior iliac crest. Eight mm-/wide cylindrical bone cores were har- vested with a trephine just below or posterior to where the bone block was harvested. The .bone grafts were stored in blood-soaked gauze, the donor site closed in layers with re- sorbable sutures, and vacuum drainage used for 24 hours.
In the inlay group of patients, a mucoperi-
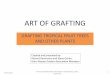
Fig. 2. a) Bone cores harvested from iliac crest, b) Possible sites for bone harvesting indicated along iliac crest.

4 3 0 Lundgren et al.
osteal flap was raised labially at the recipient site through a midcrestal incision and divided along the midline. The nasal mucosa was then carefully elevated in the anterior part of the nasal floor and the nasal aperture was widened with a large round bur to allow the bone cylinders to be more easily placed. The lateral wall of the maxillary sinus was ex- posed and a bone window was created. The preparation o f the sinus area was completed in a manner similar to that described earlier
Fig. 3. Bone cores placed vertically in maxillary sinus against anterior wall with lateral cortical part of core facing up- wards.
by KENT ~,r BLOCK 11. The bone window, ap- prox. 15 m m wide and 20 m m high, was out- lined with a round bur. The uppermost part was scored and left intact so that a greenstick fracture would allow for infraction of the lat- eral wall, thus creating a trapdoor. Care was taken not to lacerate the sinus membrane through the inferior cuts. The sinus mem- brane was carefully elevated through the oss- eous cut using a blunt elevator and the lateral bone window was pushed in to create a ceil-
ing. In this way, the recipient site was separ- ated from the upper port ion of the maxillary sinus. The procedure was performed bilater- ally. If the sinus membrane was perforated, it was dissected more excessively in the pos- terior part of the sinus, allowing the mem- brane to fold over the perforation. The bone cylinders were placed vertically against the anterior wall of the maxillary sinus (Fig. 3). The flap was then closed with a resorbable suture. Penicillin was administered for one week and a soft diet was recommended for the first two postoperative weeks. The pa- tients were not allowed to wear a denture during the first six postoperative weeks.
In the inlay/onlay patients, a labially di- rected circumvestibular incision was used to expose the lateral wall of the maxillary sinus and nasal aperture, as well as the anterior maxillary alveolar process. The bone cylin- ders were placed vertically against the an- terior wall of the maxillary sinus and in the anterior part of the nasal floor. The cortico- cancellous bone block was adjusted and placed on the alveolar process and ridgidly fixed with 2 mm-/wide t i tanium mini-screws. The mini-screws were placed on the palatal aspect so as not to interfere with the planned implant positions (Fig. 4a, b). In order to stretch the flap over the graft and to avoid tension on the incision, a horizontal incision was made in the labial flap and the flap was stretched and closed with periosteal sutures. The mucosal layer was then closed with a running suture. The patients were not allowed to wear a denture during the first eight postoperative weeks.
Six months after the bone grafting, im- plants were inserted under local anesthesia
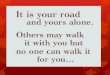
Fig. 4. a) Onlay corticocancel~!0us bone graft placed on alveolar process in anterior maxilla. Corticocancellous bone graft (black arrows). Palatal positioned t i tanium mini-screws for rigid fixation of graft (white arrows), b) Postoperative lateral view of graft placed vertically on maxillary alveolar process.
Inlay/onlay grafting 431
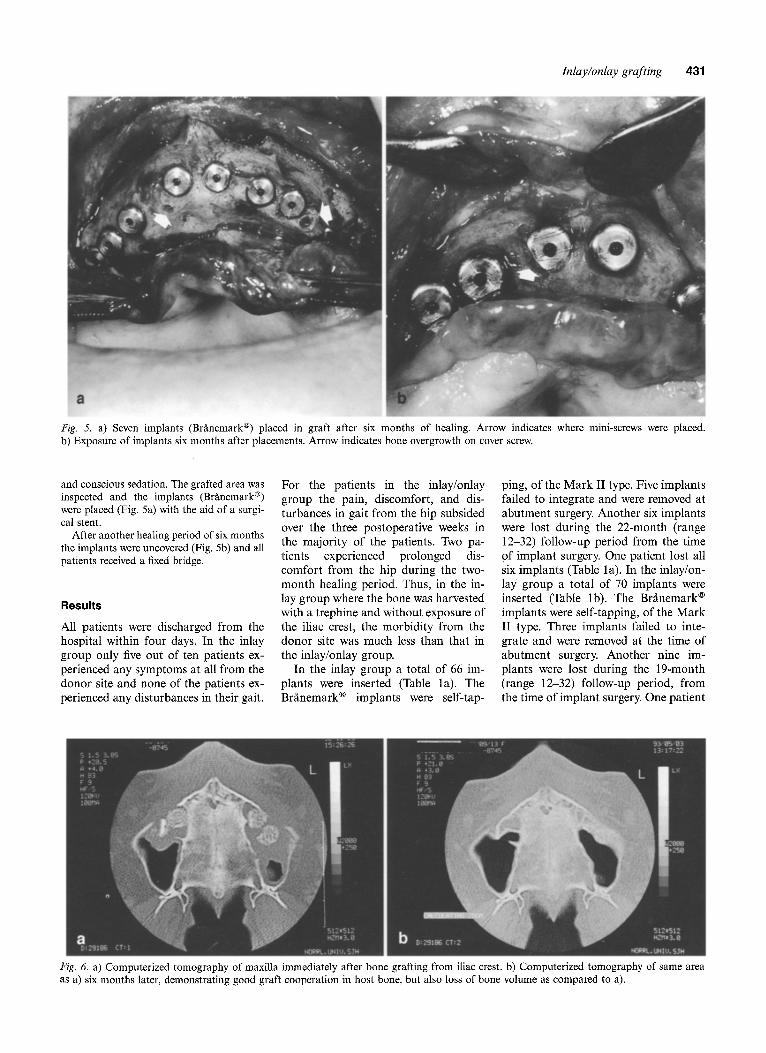
Fig. 5. a) Seven implants (Bffmemark | placed in graft after six months of healing. Arrow indicates where mini-screws were placed. b) Exposure of implants six months after placements. Arrow indicates bone overgrowth on cover screw.
and conscious sedation. The grafted area was inspected and the implants (Brgmemark | were placed (Fig. 5a) with the aid of a surgi- cal stent.
After another healing period of six months the implants were uncovered (Fig. 5b) and all patients received a fixed bridge.
Results
All patients were discharged from the hospital within four days. In the inlay group only five out of ten patients ex- perienced any symptoms at all from the donor site and none of the patients ex- perienced any disturbances in their gait.
For the patients in the inlay/onlay group the pain, discomfort, and dis- turbances in gait from the hip subsided over the three postoperative weeks in the majority of the patients. Two pa- tients experienced prolonged dis- comfort from the hip during the two- month healing period. Thus, in the in- lay group where the bone was harvested with a trephine and without exposure of the iliac crest, the morbidity from the donor site was much less than that in the inlay/onlay group.
In the inlay group a total of 66 im- plants were inserted (Table l a). The Bffmemark | implants were self-tap-
ping, of the Mark II type. Five implants failed to integrate and were removed at abutment surgery. Another six implants were lost during the 22-month (range 12-32) follow-up period from the time of implant surgery. One patient lost all six implants (Table 1 a). In the inlay/on- lay group a total of 70 implants were inserted (Table lb). The Brgmemark | implants were self-tapping, of the Mark II type. Three implants failed to inte- grate and were removed at the time of abutment surgery. Another nine im- plants were lost during the 19-month (range 12-32) follow-up period, from the time of implant surgery. One patient
Fig. 6. a) Computerized tomography of maxilla immediately after bone grafting from iliac crest, b) Computerized tomography of same area as a) six mouths later, demonstrating good graft cooperation in host bone, but also loss of bone volume as compared to a).
432 Lundgren et al.
Table la. Implant length and positions (inlay group)
Position
Length R4 R3 R2 R1 L1 L2 L3 L4
10 mm 0 2 1 5* 6* 0 1 0 13 mm 2 4* 4 5 4 7 5** 2* 15 mm 1" 3 4* 0 0 3** 4* 1 18 mm 0 1 1 0 0 0 0 0
* One implant failed to integrate. ** Two implants failed to integrate. Left (L), right (R), incisor (1), canine (2), premolar (3), and molar (4) positions.
Table lb. Implant length and positions (inlay/onlay group)
Position
Length R4 R3 R2 R1 L1 L2 L3 L4
10 mm 1 5 2* 3* 4* 3 4* 1 13 mm 5* 2* 5 6* 5** 6* 3* 2 15 mm 1 2 3* 2 1 2 3 0 18 mm 0 0 0 0 0 0 0 0
* One implant failed to integrate. ** Two implants failed to integrate. Left (L), right (R), incisor (1), canine (2), premolar (3), and molar (4) positions.
lost all seven implants (Table lb). Asked if they ,would consider recommending the treatment to a family member, 19 patients said yes; asked if they would consider repeating the treatment if necessary, all but four replied affirm- atively.
Discussion
The most common postoperative com- plications when bone is harvested from the ilium arg postsurgical pain and gait disturbance 6,13,16. Previous reports con- cerning donor site morbidity have dem- onstrated pain and gait disturbance for
a significant number of patients throughout the first postoperative month, and persistent gait disturbance for a few patients lasting as long as sev- eral months 4,m,13'~4,17. In the inlay group of patients, where through-by- through bone cylinders were harvested with a trephine with no previous reflec- tion of muscles and periosteum from the iliac crest, the morbidity was sig- nificantly lower than in the inlay/onlay group. All the inlay patients were able to walk within a few hours after the op- eration and none of them reported any disturbances in their gait. Only five of the patients reported any donor site
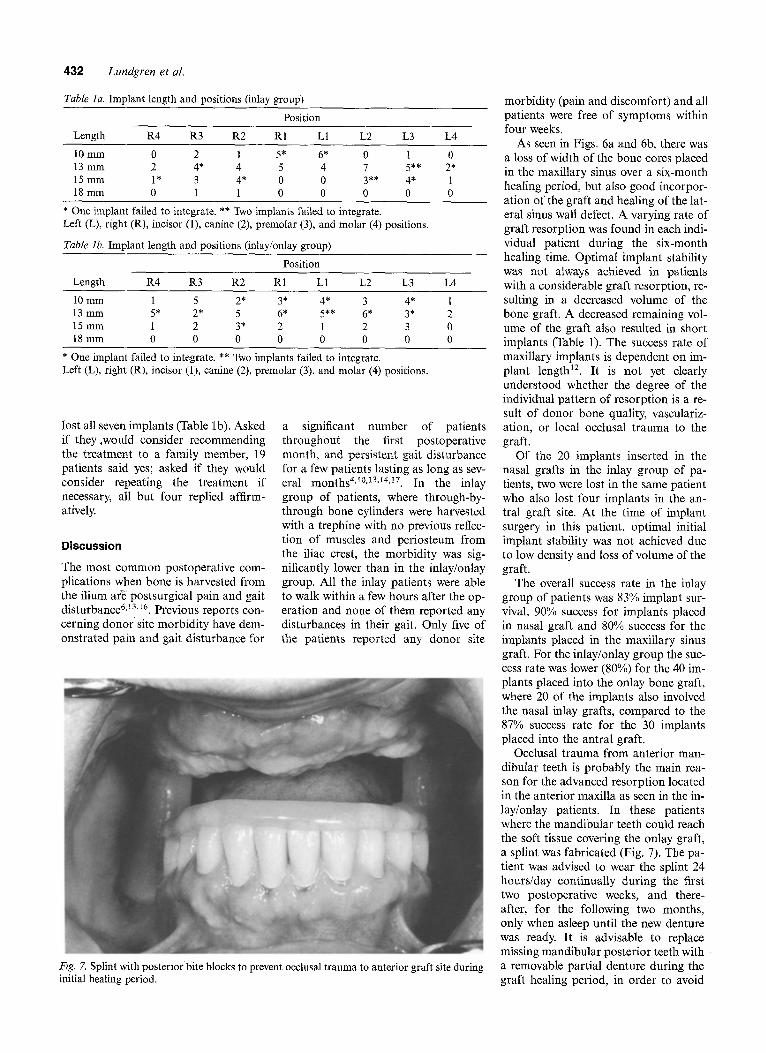
Fig, 7. Splint with posterior bite blocks to prevent occlusal trauma to anterior graft site during initial healing period.
morbidity (pain and discomfort) and all patients were free of symptoms within four weeks.
As seen in Figs. 6a and 6b, there was a loss of width of the bone cores placed in the maxillary sinus over a six-month healing period, but also good incorpor- ation of the graft and healing of the lat- eral sinus wall defect. A varying rate of graft resorption was found in each indi- vidual patient during the six-month healing time. Optimal implant stability was not always achieved in patients with a considerable graft resorption, re- sulting in a decreased volume of the bone graft. A decreased remaining vol- ume of the graft also resulted in short implants (Table 1). The success rate of maxillary implants is dependent on im- plant length 12. It is not yet clearly understood whether the degree of the individual pattern of resorption is a re- sult of donor bone quality, vasculariz- ation, or local occlusal trauma to the graft.
Of the 20 implants inserted in the nasal grafts in the inlay group of pa- tients, two were lost in the same patient who also lost four implants in the an- tral graft site. At the time of implant surgery in this patient, optimal initial implant stability was not achieved due to low density and loss of volume of the graft.
The overall success rate in the inlay group of patients was 83% implant sur- vival, 90% success for implants placed in nasal graft and 80% success for the implants placed in the maxillary sinus graft. For the inlay/onlay group the suc- cess rate was lower (80%) for the 40 im- plants placed into the onlay bone graft, where 20 of the implants also involved the nasal inlay grafts, compared to the 87% success rate for the 30 implants placed into the antral graft.
Occlusal trauma from anterior man- dibular teeth is probably the main rea- son for the advanced resorption located in the anterior maxilla as seen in the in- lay/onlay patients. In these patients where the mandibular teeth could reach the soft tissue covering the onlay graft, a splint was fabricated (Fig. 7). The pa- tient was advised to wear the splint 24 hours/day continually during the first two postoperative weeks, and there- alter, for the following two months, only when asleep until the new denture was ready. It is advisable to replace missing mandibular posterior teeth with a removable partial denture during the graft healing period, in order to avoid
Inlay/onlay grafting 433
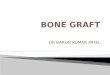
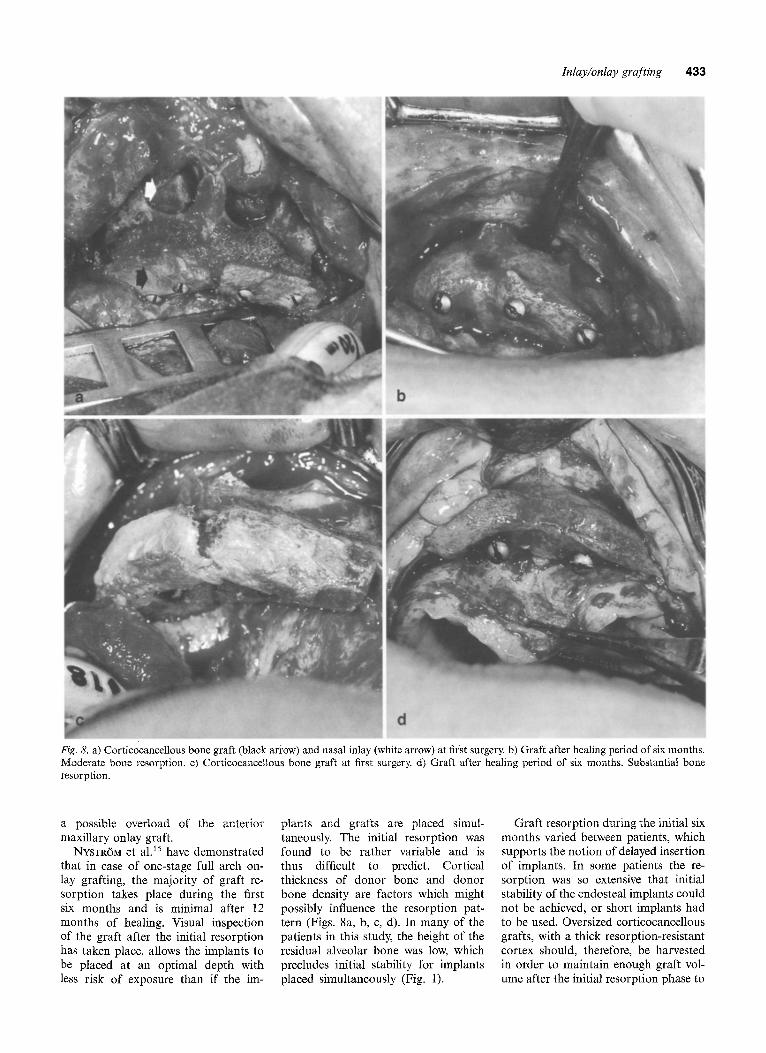
Fig. 8. a) Cortic0cancellous bone graft (black ari'ow) and nasal inlay (white arrow) at first surgery, b) Graft after healing period of six months. Moderate bone resorption, c) Corticocancellous bone graft at first surgery, d) Graft after healing period of six months. Substantial bone resorption.
a possible overload of the anterior maxillary onlay graft.
NYSTR6M et al. 15 have demonstrated that in case of one-stage full arch on- lay grafting, the majority of graft re- sorption takes place during the first six months and is minimal after 12 months of healing. Visual inspection of the graft after the initial resorption has taken place, allows the implants to be placed at an optimal depth with less risk of exposure than if the ira-
plants and grafts are placed simul- taneously. The initial resorption was found to be rather variable and is thus difficult to predict. Cortical thickness of donor bone and donor bone density are factors which might possibly influence the resorption pat- tern (Figs. 8a, b, c, d). In many of the patients in this study, the height of the residual alveolar bone was low, which precludes initial stability for implants placed simultaneously (Fig. 1).
Graft resorption during the initial six months varied between patients, which supports the notion of delayed insertion of implants. In some patients the re- sorption was so extensive that initial stability of the endosteal implants could not be achieved, or short implants had to be used. Oversized corticocancellous grafts, with a thick resorption-resistant cortex should, therefore, be harvested in order to maintain enough graft vol- ume after the initial resorption phase to

434 Lundgren et al.
allow for long implan ts wi th good in- itial stability.
References
1. ADELL R, LEKHOLM U, GRONDAHL K, BRXNEMARK P-I, LINDSTR6M J, JACOBS- SON M. Reconstruction of severely re- sorbed edentulous maxillae using osseo- integrated fixtures in immediate autog- enus bone grafts. Int J Oral Maxillofac Implants 1990: 5: 233-46.
2. CAWOOD JL, HOWELL RA. A classifi- cation of the edentulous jaw. Int J Oral Maxillofac Surg 1988: 17: 232-6.
3. CAWOOD JL, STOEEINGA PJW, BROUNS JJA. Reconstruction of the severely re- sorbed (Class VI) maxilla. A two-step procedure. Int J Oral Maxillofac Surg 1994: 23: 219-25.
4. GRILEON GL, GUNTHER SL, CONNOLE PW. A new technique for obtaining iliac bone grafts. J Oral Maxillofac Surg 1984: 42: 172-6.
5. HALL HI), McKENNA SJ. Bone graft of the maxillary sinus floor for Brfinemark implants: a preliminary report. In: WORTHINGTON P, BREINE OR, eds.: Oral and Maxillofacial Surgery Clinics. Phila- delphia: Saunders, 1991: 3: 869-73.
6. HALL MB, SMITH RG. The medial ap- proach for obtaining iliac bone. J Oral Surg 1981: 39: 462-5.
7. HIGUCHI KW. Nasal inlay bone graft technique. In: LONEY W~ TOLMAN DE, eds.: Tissue integration in oral, ortho- paedic, maxillofacial reconstruction. Pro- ceedings of the Second International Congress on Tissue Integration in Oral, Orthopaedic, and Maxillofacial Recon- struction, Rochester 23-27 Sept. 1990. Chicago: Quintessence, 1992: 318-20.
8. JENSEN J, SINDET-PEDERSEN S, OLIVER AJ. Varying treatment strategies for recon- struction of maxillary atrophy with im- plants: results in 98 patients. J Oral and Maxillofac Surg 1994: 52: 210-6.
9. KELLER EL, ECKERT SE, TOLMAN DE. Maxillary antral and nasal one-stage in- lay composite bone graft. Preliminary re- port on 30 recipient sites. J Oral and Maxillofac Surg 1994: 52: 438-48. KELLER EL, TRIPLETT W~. Iliac bone grafting: review of 160 consecutive cases. J Oral Maxillofac Surg 1987: 45:11-4. KENT JN, BLOCK MS. Simultaneous maxillary sinus floor bone grafting and placement of hydroxyapatite-coated im- plants. J Oral Maxillofac Surg 1989: 47: 238-42. LOZADA JL, EMANUELLI S, JAMES RA, BOSKOVlC M, INDSTED K. Root-form im- plants placed in subanthral grafted sites. California Dent J 1993: 21: 31-5. MARX RE, MORALES MJ. Morbidity from bone harvest in major jaw recon- struction: a randomized trial comparing
10.
11.
12.
13.
the lateral anterior and posterior ap- proaches to the ilium. J Oral Maxillofac Surg 1988: 8: 19t%203.
14. NYSTROM E, KAHNBERG K-E, GUNNE J. Bone grafts and Br~nemark implants in the treatment of the severely resorbed maxilla: a 2-year longitudinal study. Int J Oral Maxillofac Implants 1993: 8: 45-53.
15. NYSTR6M, LEGRELL P-E, FORSSELL ilk, KAHNBERG K-E. Combined use of bone grafts and implants in the severely re- sorbed maxillae. Postoperative evaluation utilizing computerized tomography. Int J Oral Maxillofac Surg 1995: 24: 20-5.
16. STOLE P~ SCHIEEI W. Long-term follow-up of donor and recipient sites after auto- logous bone grafts for reconstruction of the facial skeleton. J Oral Surg 1981: 39: 676-7.
17. TAYAPONGSAK R WIMSATT JA, LA BANC JP, DOEWICK ME Morbidity from an- terior ilium bone harvest. A comparative study of lateral versus medial surgical ap- proach. Oral Surg 1994: 78: 296-300.
Address: Dr S. Lundgren Department of Oral and Maxillofacial
Surgery Umed University S-901 87 Umed Sweden