Embed Size (px)
Citation preview

Bone Density, Turnover, and Estimated Strength inPostmenopausal Women Treated With Odanacatib:A Randomized Trial
Kim Brixen, Roland Chapurlat, Angela M. Cheung, Tony M. Keaveny,Thomas Fuerst, Klaus Engelke, Robert Recker, Bernard Dardzinski,Nadia Verbruggen, Shabana Ather, Elizabeth Rosenberg, and Anne E. de Papp
Context: Odanacatib, a cathepsin K inhibitor, increases spine and hip areal bone mineral density(BMD) in postmenopausal women with low BMD and cortical thickness in ovariectomized monkeys.
Objective: The objective of the study was to examine the impact of odanacatib on the trabecularand cortical bone compartments and estimated strength at the hip and spine.
Design: This was a randomized, double-blind, 2-year trial.
Setting: The study was conducted at a private or institutional practice.
Participants: Participants included 214 postmenopausal women with low areal BMD.
Intervention: The intervention included odanacatib 50 mg or placebo weekly.
Main Outcome Measures: Changes in areal BMD by dual-energy x-ray absorptiometry (primary endpoint, 1 year areal BMD change at lumbar spine), bone turnover markers, volumetric BMD byquantitative computed tomography (QCT), and bone strength estimated by finite element analysiswere measured.
Results: Year 1 lumbar spine areal BMD percent change from baseline was 3.5% greater withodanacatib than placebo (P � .001). Bone-resorption marker C-telopeptide of type 1 collagen wassignificantly lower with odanacatib vs placebo at 6 months and 2 years (P � .001). Bone-formationmarker procollagen I N-terminal peptide initially decreased with odanacatib but by 2 years did notdiffer from placebo. After 6 months, odanacatib-treated women had greater increases in trabec-ular volumetric BMD and estimated compressive strength at the spine and integral and trabecularvolumetric BMD and estimated strength at the hip (P � .001). At the cortical envelope of thefemoral neck, bone mineral content, thickness, volume, and cross-sectional area also increasedfrom baseline with odanacatib vs placebo (P � .001 at 24 months). Adverse experiences were similarbetween groups.
Conclusions: Over 2 years, odanacatib decreased bone resorption, maintained bone formation,increased areal and volumetric BMD, and increased estimated bone strength at both the hip andspine. (J Clin Endocrinol Metab 98: 571–580, 2013)
Osteoporosis is a disease characterized by low bonemass and microarchitectural deterioration, leading
to bone fragility and increased risk of fracture (1). Currenttreatments for osteoporosis include antiresorptive agentssuch as bisphosphonates and denosumab that preserve
bone mass by decreasing the rate of bone turnover. Thesetreatments reduce the number and/or activity of bone-re-sorbing osteoclasts. Because osteoclasts have a role in thestimulation of bone formation by osteoblasts, these treat-ments indirectly lower bone formation (2–5).
ISSN Print 0021-972X ISSN Online 1945-7197Printed in U.S.A.Copyright © 2013 by The Endocrine Societydoi: 10.1210/jc.2012-2972 Received August 2, 2012. Accepted December 7, 2012.First Published Online January 21, 2013
* Author affiliations are shown at the bottom of the next page.Abbreviations: aBMD, Areal bone mineral density; AE, adverse experience; ANCOVA, anal-ysis of covariance; BMD, bone mineral density; CT, computed tomography; CTX, C-telo-peptide of type 1 collagen; 3D, 3 dimensional; DXA, dual-energy x-ray absorptiometry; FEA,finite-element analysis; FOV, field of view; P1NP, procollagen I N-terminal peptide; QCT,quantitative computerized tomography; vBMD, volumetric BMD.
O R I G I N A L A R T I C L E
E n d o c r i n e C a r e
J Clin Endocrinol Metab, February 2013, 98(2):571–580 jcem.endojournals.org 571

Odanacatib, currently in phase 3 development for thetreatment of postmenopausal osteoporosis, is a highly se-lective and reversible oral inhibitor of the collagenase ca-thepsin K that is secreted by osteoclasts. Odanacatib re-duces bone resorption without reducing osteoclastnumber and hence appears to preserve bone formation(6–9). In a phase 2 trial of women with low areal bonemineral density (aBMD), bone resorption markers re-mained reduced in women treated for 5 years with odana-catib 50 mg once weekly (9). In contrast, although boneformation markers were initially reduced in odanacatib-treated women, they returned to near baseline levels with2 years of continued therapy (7, 8). In the phase 2 trialextension, continuous treatment with odanacatib 50 mgweekly for 5 years resulted in mean increases in aBMDfrom baseline of 11.9% at the lumbar spine, 8.5% at thetotal hip, and 9.8% at the femoral neck (9).
In studies of ovariectomized, skeletally mature rhesusmonkeys, odanacatib prevented bone mineral density(BMD) loss induced by estrogen deficiency at the spine andhip (6, 10–12). Compared with vehicle, odanacatib wasassociated with increases in cortical thickness of 21% atthe femoral neck and 19% in the overall proximal femur(10). Odanacatib also increased periosteal bone formationrates at the femoral neck and proximal femur 3- to 6-fold,respectively, consistent with changes observed with an-other cathepsin K inhibitor, balicatib (13). Three-pointbending of the central femurs revealed greater bonestrength with odanacatib compared with vehicle-treatedanimals and normal biomechanical properties (10).
In this study, we sought to extend our clinical charac-terization of odanacatib in postmenopausal women, fo-cusing on changes in the cortical and trabecular compart-ments. Given the limitations of using dual-energy x-rayabsorptiometry (DXA) for such purposes (14), we usedquantitative computerized tomography (QCT) and finite-element analysis (FEA) of the QCT images to assess bonedensity, geometry, and strength (15–17). In particular, weused QCT and FEA as well as assessments of aBMD byDXA and bone turnover to compare the effects of odana-catib vs placebo at the spine and hip in postmenopausalwomen with low aBMD.
Materials and Methods
Study designThis was a randomized, double-blind, international, 2-year,
phase 3 trial comparing odanacatib 50 mg once weekly with
placebo in postmenopausal women treated with calcium andvitamin D. The primary end point was percent change from base-line in aBMD at the lumbar spine at 1 year, assessed by DXA.Secondary end points included percentage changes from baselineat 1 year in aBMD at the hip (total hip, femoral neck, and tro-chanter), 2-year aBMD at the spine and hip, 1- and 2-yearchanges in bone turnover markers [C-telopeptide of type 1 col-lagen (CTX) and procollagen I N-terminal peptide (P1NP)], and1- and 2-year trabecular volumetric BMD (vBMD) at the lumbarspine, assessed by QCT. Exploratory end points includedchanges from baseline in integral, trabecular, and cortical vBMDand cortical thickness at the hip by QCT and estimates of bonestrength assessed by FEA. High-resolution peripheral QCT withFEA of the distal radius and tibia was also performed in this studyand will be the subject of a separate publication.
Six study visits were conducted at screening, randomization,and months 6, 12, 18, and 24, with a follow-up phone call 2weeks after the final visit to record possible adverse experiences(AEs).
All participants gave written informed consent. The studywas conducted in accordance with principles of good clinicalpractice and was approved by the appropriate institutional re-view boards and regulatory agencies.
ParticipantsWomen enrolled from 7 countries and 13 investigative sites
were 45–85 years old and postmenopausal for 3 years or longer.T-scores at the lumbar spine, total hip, femoral neck, or tro-chanter were �1.5 or less but greater than �3.5. Women wereexcluded if they had had a prior hip fracture at any time, a nonhipfragility fracture (excluding finger, toe, or skull) within 24months, or more than 1 prior clinical vertebral fracture. Womenwere also excluded if they had disorders causing persistent trem-ors; metabolic bone disorders other than osteoporosis; renalstones with serum calcium, 25-hydroxyvitamin D, or PTH out-side the normal range; active parathyroid disease; poorly con-trolled thyroid disease; or serum-creatinine greater than 1.6mg/dL with severe renal insufficiency. Excluded medicationswere estrogen, selective estrogen receptor modulators, systemicglucocorticoids (equivalent to �5 mg/d prednisone), or cyclo-sporine for longer than 2 weeks within 6 months of study entry;teraparatide or PTH(1–84) within 12 months; activated vitaminD within 3 months; strontium ranelate; or any anabolic steroid,GH, cathepsin K inhibitor, or receptor activator of nuclear fac-tor-�B ligand inhibitor at any time in the past. Also prohibitedwere use of any oral bisphosphonate within 6 months of studyentry, for longer than 3 months within the prior 2 years, or longerthan 6 months at any time, any use of IV zoledronate, and ivibandronate within a year of screening. Concurrent use of bone-active agents other than study medications as well as heparin,protease inhibitors for HIV, or strong CYP3A4 inducers wasprohibited.
Department of Endocrinology, Institute of Clinical Research (K.B.), University of Southern Denmark, DK-5000 Odense C., Denmark; INSERM UMR 1033 and Université de Lyon (R.C.), 69372Lyon, France; Departments of Medicine and Medical Imaging (A.M.C.), University Health Network, Toronto, Ontario, Canada M5G 2C4; Departments of Mechanical Engineering andBioengineering (T.M.K.), University of California and ON Diagnostics, Berkeley, California 94720; Synarc Inc (T.F.), Newark, California 94569; Institute of Medical Physics (K.E.), Universityof Erlangen, 91052 Erlangen, Germany; Syncarc Inc (K.E.), 20354 Hamburg, Germany; Osteoporosis Research Center (R.R.), Creighton University, Omaha, Nebraska 68131; Merck Sharp& Dohme (B.D., S.A., E.R., A.E.d.P.), Whitehouse Station, New Jersey 08889; and Merck Sharp & Dohme (N.V.), 1200 Brussels, Belgium
572 Brixen et al Bone Density and Strength With Odanacatib J Clin Endocrinol Metab, February 2013, 98(2):571–580

TreatmentPatients were randomized using a computer-generated ran-
domized allocation schedule to blinded therapy with eitherweekly oral odanacatib 50 mg or matching placebo. Open-labelvitamin D3 5600 IU weekly was provided to all subjects. Partic-ipants were instructed to take their study medication on approx-imately the same day each week, without regard to food intake.Open-label calcium supplements were provided so that totaldaily calcium intake was approximately 1200 mg.
Assessments
Bone turnover markersSamples for analyses of serum CTX and P1NP were obtained
in the morning, after the participants had refrained from food ordrink except water for at least 8 hours. Analyses were performedcentrally for CTX (Serum Crosslaps ELISA assay; Quest Diag-nostics, Valencia, California) and for P1NP (electrochemilumi-nescence assay; Pacific Biometrics, Seattle, Washington). Thesamples were then stored frozen, and all the assays were runtogether at 24 months.
Densitometry and imagingDXA. Areal BMD by DXA at lumbar spine (L1-L4), total hip,femoral neck, and trochanter were measured using a Hologic(Waltham, Massachusetts) or GE Lunar (Indianapolis, Indiana)scanner less than 9 years old. Mean BMD measurements were of3 or more evaluable vertebrae. Vertebrae fractured at baseline orduring the study were excluded from the analysis. Hip scans wereperformed on the left side unless the left hip was unavailable.Longitudinal calibration phantoms were used.
QCT. QCT imaging of the lumbar spine (L1 and L2) used helicalcomputed tomography (CT) scanners with 4 or more detectorrows. All CT scans were obtained at 120 kV. Default exposurewas 100 mA (spine) and 170 mA (hip), adapted to the individualpatient using CT scanner specific radiation exposure reductionprotocols. For reconstruction, a slice thickness of 1 or 1.25 mm(depending on scanner), a reconstruction increment of 1 (ie, nooverlap or gap between slices), and a medium kernel were used.Two reconstructions with different diameter fields of view(FOVs) were obtained from each scan: a large FOV to analyze thecalibration phantom measured simultaneously with each patientplus an FOV of 20 cm in the hip (corresponding to an in planepixel size of 0.39 mm) and 12 cm in the spine (in plane pixel sizeof 0.23 mm). The small FOV reconstructions were analyzed tomeasure the QCT parameters by segmenting bone compart-ments and placing regions of interest.
Longitudinal (QCTPro QA phantom; Mindways Software,Inc, Austin, Texas) and cross-calibration (European spine phan-tom; QRM GmbH, Moehrendorf, Germany) phantoms wereused to correct for any equipment-related differences within andbetween sites. QCTPro (Mindways Software) was used for theBMD analysis of the QCT scans. At the hip, integral, trabecular,and cortical vBMD were assessed. At the lumbar spine, QCTProcan measure vBMD only in the trabecular region of the vertebralbody centrum. Cross-sectional area, cortical area, and corticalthickness were determined at the smallest cross section of thefemoral neck using the Bone Investigational Toolkit of QCTPro.
For the hip analysis, QCTPro uses a default threshold valueof 100 mg/cm3 to separate bone from soft tissue and a default
threshold value of 350 mg/cm3 to separate cortical and trabec-ular bone. In some patients the value of the bone soft tissuethreshold had to be adapted to improve the segmentation, but forall visits of a given patient, the same segmentation settings wereused. Quality control and analysis of all DXA and QCT scanswere performed centrally by Synarc, Inc (Hamburg, Germany).
Finite element analysisPatient-specific femoral strength for a simulated sideways fall
and L1 vertebral strength for simulated axial compression over-load were estimated using nonlinear 3-dimensional (3D) FEA ofthe QCT scans. All FEA analyses were performed centrally byO.N. Diagnostics (Berkeley, California), as described previously(16, 18).
Bone biopsyParticipants willing to undergo a transilial bone biopsy re-
ceived a bone-labeling agent (eg, meclocycline) at month 23.Biopsies were performed at month 24 and analyzed centrally byCreighton University (Omaha, Nebraska). Fluorochrome dou-ble-labeling, biopsy sample handling, qualitative histologicalanalysis, and quantitative histomorphometric analysis were per-formed as described (19). Biopsies were evaluated for the endpoints of dynamic histomorphometry and for evidence of pos-sible drug-induced abnormalities, including woven bone andmineralization abnormalities. Micro-CT (Scanco, Bassersdorf,Switzerland) was performed on all biopsies prior to embeddingto evaluate 3D trabecular microstructure.
SafetySafety was assessed via evaluation of AEs, physical examina-
tion, and laboratory tests. Central adjudication committees wereestablished for dental AEs consistent with osteonecrosis of thejaw, skin AEs suggestive of morphea, cases of delayed fractureunion, and all respiratory AEs meeting serious AE criteria.
Statistical methodsAnalyses of BMD were performed using the full analysis set
population (treated participants with baseline and at least 1 on-treatment measurement). Areal BMD results were analyzed us-ing a longitudinal analysis of covariance (ANCOVA) model withterms for treatment, time, geographic region, and the interactionof time by treatment and the corresponding baseline aBMD valueas a covariate. Analysis of vBMD results used a similar longitu-dinal ANCOVA model with baseline vBMD as a covariate andtreatment, time, region, and treatment-by-time interaction asfixed effects. The same statistical methods were used for FEAchanges from baseline. Bone turnover markers were analyzed onthe per-protocol population using the log-transformed fractionfrom baseline (backtransformed for presentation) and using theANCOVA model described above for aBMD.
Sample size was chosen to achieve significant results for thevBMD end points, based on the results of Black et al (20) with anassumption that the treatment effect of odanacatib on vBMD atthe spine would be equivalent to that of alendronate. The studyhad greater than 99% power to show a significant difference(type I error �0.05) between treatment groups in lumbar spine,femoral neck, and total hip aBMD at 1 year.
For safety monitoring, AEs of special interest (skin AEs re-ported as events of clinical interest or events suggestive of mor-phea or scleroderma; serious respiratory infections; osteonecro-
J Clin Endocrinol Metab, February 2013, 98(2):571–580 jcem.endojournals.org 573

sis of the jaw; and delayed fracture unions, when at an incidenceof 4 or more patients in either treatment group) were subject toinferential testing for statistical significance. Clinical, seriousclinical, drug-related clinical AEs, or AEs leading to discontin-uation of study medication, when at an incidence of 4 or morepatients in either treatment group, were assessed via point esti-mates and 95% confidence intervals for treatment comparison.Other AEs were assessed by point estimates only. Bone biopsyend points are presented in summary statistics.
Results
A total of 214 postmenopausal women, with an averageage of 64 years and baseline T-scores of �1.8 at the lumbarspine, �1.8 at the femoral neck, and �1.3 at the total hipwere enrolled. Women randomized to odanacatib 50 mgor placebo, once weekly, had similar characteristics atbaseline except that the lumbar spine aBMD was slightlylower in the placebo group (Table 1). Eighty-one percentof the participants completed the trial.
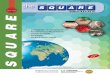
Areal BMDThe percent change from baseline in aBMD at the lum-
bar spine at 1 year, the primary end point of the trial, wassignificantly (P � .001) higher in women receiving odana-catib compared with placebo (treatment difference 3.5%).The treatment difference increased in the second year to5.4% (Figure 1A). Mean percent change in aBMD at thefemoral neck (Figure 1B), total hip, and trochanter werealso significantly greater (P � .001) in women receivingodanacatib, with treatment differences at 2 years of 3.8%,3.3%, and 5.5%, respectively.
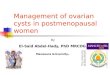
Bone turnover markersDuring the first 6 months of the trial, serum concen-
trations of both CTX and P1NP decreased significantly(P � .001) in odanacatib-treated women compared withplacebo-treated women (Figure 2). In the odanacatibgroup, CTX remained low over the course of the trial, witha treatment difference vs placebo at 2 years of �45.6%(P � .001). In contrast, P1NP concentrations rose overtime toward baseline, from a mean treatment difference of�31.3% at 6 months (P � .001) to treatment difference of�9.1% at 2 years (P � .225).
QCT measurement and FEA analysis
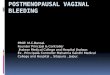
Volumetric BMD and estimated strength at the spineSignificant differences between odanacatib and pla-
cebo in percentage changes from baseline in trabecularvolumetric BMD at L1 were seen as early as 6 months(Figure 3A). At 2 years, the treatment difference was11.5% (P � .001). Similar treatment differences were seenfor L2 (data not shown).
FEA estimates of compressive strength in the L1 verte-bra also showed a significant difference between odana-catib and placebo, with a treatment difference of 14.3% at2 years (P � .001) (Figure 3B).
Table 1. Patient Disposition and BaselineCharacteristics
Patient DispositionODN 50 mg OW
(n � 109)Placebo OW
(n � 105)Completed study, n, % 84 (77) 90 (86)Discontinued, n, % 25 (23) 15 (14)
Adverse event 11 (10) 5 (5)Lack of efficacy 0 1 (1)Lost to follow-up 3 (3) 1 (1)Physician decision 1 (1) 1 (1)Protocol violation 1 (1) 0Withdrawal by subject 9 (8) 7 (7)
Baseline characteristicAge, mean (SD) 63.9 (7.3) 64.0 (6.2)Ethnicity, n, %
Caucasian 101 (93) 98 (93)Asian 8 (7) 3 (3)Black 0 2 (2)American Indian or
Alaskan Native0 1 (1)
Multiethnic 0 1 (1)Geographic region, n, %
Europe 66 (61) 63 (60)Non-Europe 43 (39) 42 (40)
Fracture history sincemenopause, n, %
Hip or vertebra 0 0Nonvertebra 26 (24) 27 (26)
Bone turnover markersCTX, pg/mL (SD) 0.58 (0.23) 0.57 (0.24)P1NP unit, ng/mL 49.3 (19.2) 49.7 (17.7)
Areal BMD T-score,mean (SD)
Lumbar spine �1.71 (0.74) �1.90 (0.91)Femoral neck �1.78 (0.53) �1.76 (0.55)Trochanter �1.22 (0.79) �1.20 (0.83)Total hip �1.30 (0.64) �1.28 (0.71)
QCT, mg/cm3 (SD)Trabecular vBMD
Spine 98.7 (21.7) 97.9 (23.4)Total hip 104.1 (14.4) 104.6 (15.4)Femoral neck 102.3 (16.0) 102.5 (17.2)Trochanter 105.5 (15.9) 104.9 (16.2)
Cortical vBMDTotal hip 603.2 (29.8) 604.0 (29.2)Femoral neck 596.8 (39.9) 598.6 (44.4)Trochanter 466.8 (26.8) 465.2 (27.9)
Integral vBMDTotal hip 230.5 (29.8) 232.0 (30.5)Femoral neck 237.0 (30.2) 240.8 (31.4)Trochanter 168.3 (23.8) 167.8 (26.0)
FEA, n (SD)Compressive strength of
vertebral body (L1)3667 (795) 3685 (852)
Hip strength, sidewaysfall
3176 (454) 3191 (414)
Abbreviations: ODN, odanacatib; OW, once weekly.
574 Brixen et al Bone Density and Strength With Odanacatib J Clin Endocrinol Metab, February 2013, 98(2):571–580

vBMD and estimated strength at the hipIntegral volumetric BMD percent change from baseline
at 2 years differed significantly between odanacatib andplacebo at the total hip, femoral neck, and trochanter,with treatment differences of 3.7%, 3.3%, and 6.0%, re-spectively (P � .001) (Figures 3C and 4A). TrabecularvBMD followed a similar pattern: treatment differencesbetween odanacatib and placebo at the total hip, femoralneck, and trochanter were 4.2%, 3.4%, and 4.0%, re-spectively (P � .001).
FEA indicated that odanacatib increased the estimatedstrength at the hip, whereas that of the placebo groupdecreased. The 2-year treatment difference was 5.6% (P �.001) (Figure 3D).
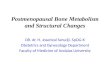
Additional QCT analyses at the femoral neckAfter 2 years, at the smallest cross-section of the fem-
oral neck, cortical thickness increased with odanacatibbut decreased with placebo (treatment difference 6.0%,P � .001) (Figure 4B). Cortical area also increased overtime with odanacatib (treatment difference 4.9%, P �
.001), whereas the total (cortical and trabecular) area didnot change (treatment difference �1.3%, P � .102) (Fig-ure 4B).
Cortical vBMD at the femoral neck did not significantlydiffer between odanacatib and placebo (Figure 4A). How-ever, cortical bone mineral content of the femoral neckincreased with odanacatib (treatment difference 3.2%,P � .021), as did the cortical volume of the femoral neck(treatment difference 3.1%, P � .009) (Figure 4A).
Bone biopsiesIliac crest biopsies were performed on 13 participants
with 10 evaluable biopsies obtained (Table 2). There waslittle difference between odanacatib and placebo in severalindices of bone formation; most notably the activationfrequency with odanacatib treatment was not significantlyreduced as compared with placebo. There was no evidenceof mineralization abnormalities or woven bone. Both 2-and 3D measures of trabecular thickness were greater inthe odanacatib-treated women, as was the 3D measure oftrabecular number, although the number of biopsies avail-able for analysis was limited.
Baseline Month 6 Month 12 Month 24
Time
Baseline Month 6 Month 12 Month 24Time
LS M
ean
% C
hang
e Fr
om B
asel
ine
(SE)
LS M
ean
% C
hang
e Fr
om B
asel
ine
(SE)
-4
-2
0
2
4
6
-4
-2
0
2
4
6
A Lumbar spine
B Femoral neck
ODN 50 mg OWPlacebo OW
ODN 50 mg OWPlacebo OW
**
**
*
*P≤0.001
Figure 1. Areal BMD by DXA. *P between treatments �.001. LS,least means; ODN, odanacatib.
Baseline Month 6 Month 12 Month 18 Month 24
-60
-40
-20
0
20
Time
LS
Mea
n %
Cha
nge
From
Bas
elin
e (S
E)
Baseline Month 6 Month 12 Month 18 Month 24
-60
-40
-20
0
20
Time
LS
Mea
n%
Cha
nge
From
Bas
elin
e (S
E)
ODN 50 mg OWPlacebo OW
A CTX
B P1NP
* *
**
* *
*P<0.001 between treatments
Figure 2. Bone turnover markers. *P between treatments �.001. LS,least means; ODN, odanacatib; OW, once weekly.
J Clin Endocrinol Metab, February 2013, 98(2):571–580 jcem.endojournals.org 575

SafetyOdanacatib was generally well tolerated. There were
no events that met the adjudication criteria for AEs of skin,respiratory, dental, or delayed fracture union. In fact,there were fewer skin AEs overall with odanacatib (11%)than with placebo (18%). Five participants (4.6%) in theodanacatib group and 1 (1.0%) in the placebo group dis-continued due to a serious AE, but none of these was con-sidered to be treatment related (2 breast cancer, 2 ovariancancer, and 1 sarcoidosis). Clinical fractures were cap-tured as AEs; there were 10 patients with fractures (9.5%)in the placebo group and 3 (2.8%) in the odanacatib-treated group.
Discussion
In this 2-year, placebo-controlled, randomized imagingstudy of odanacatib in postmenopausal women with lowaBMD, women who received odanacatib had significantly
greater gains in areal BMD, integral vBMD, and FEA-estimated strength at both the hip and spine than womentreated with calcium and vitamin D alone. Odanacatibwas generally well tolerated.
Bone strength and fracture risk are associated withbone macro- and microarchitecture as well as bone density(14, 15, 21–24). Because QCT is based on 3D volumetricmeasures, rather than the projectional 2-dimensional im-ages generated with DXA, QCT provides additional in-formation, including input forassessmentofbone strengthby FEA. Finite-element models of spine and hip strengthhave been shown to correlate well with biomechanicaltests in cadaveric specimens (16, 25, 26). Finite-elementmodeling has also been shown to be a powerful predictorof spine (22, 26–28), hip (29–31), and overall osteopo-rotic fractures (17). Thus, the increase in bone strengthwith odanacatib as estimated by FEA in the current studysuggests a decreased risk of fracture. Estimated bonestrength with odanacatib treatment was significantly dif-
ODN 50 mg OWPlacebo OW
* **
*
* * ***
*
LS M
ean
% C
hang
e Fr
om B
asel
ine
(SE)
-10
-5
0
5
10
15
Baseline Month 6 Month 12 Month 24
Time
-10
-5
0
5
10
Baseline Month 6 Month 12 Month 24
Time
LS M
ean
% C
hang
e Fr
om B
asel
ine
(SE)
A QCT L1 spine trabecular vBMD
C QCT TH integral vBMD
B FEA compressive strength (L1)
D FEA hip strength, sideways fall
Baseline Month 6 Month 12 Month 24
-4
-2
0
2
4
6
Time
LS M
ean
% C
hang
e Fr
om B
asel
ine
(SE)
Baseline Month 6 Month 12 Month 24
-4
-2
0
2
4
6
Time
LS M
ean
% C
hang
e Fr
om B
asel
ine
(SE)
*P<0.001
Figure 3. Volumetric BMD and estimated strength from QCT analysis. *P between treatments �.001. LS, least means; ODN, odanacatib;OW, once weekly; TH, total hip.
576 Brixen et al Bone Density and Strength With Odanacatib J Clin Endocrinol Metab, February 2013, 98(2):571–580

ferent from placebo as early as 6 months. The changes inpredicted strength at the hip after 2 years of odanacatibtreatment are of similar magnitude to those reported fordenosumab (32), an agent with proven hip fracture riskreduction (33).
The spine consists mostly of trabecular bone, and theincrease in estimated strength at the spine correlates withan increase in trabecular vBMD [although the exact re-gions analyzedbyFEAandQCTPro(MindwaysSoftware)aredifferent]. At the hip, the situation is more complex. In ouranalysis using the QCTPro software, gains in integralvBMD (a combined QCT based measure of trabecular and
cortical vBMD) were significantly higher with odanacatibthan placebo, consistent with the DXA measures of aBMDand the FEA estimates of strength. In comparison, changesin cortical vBMD at the hip and hip subregions, assessedby QCTPro software, were the same or lower for odana-catib than placebo. Interestingly, in the femoral neck, mea-sures of cortical bone mineral content and cortical volumeincreased significantly more with odanacatib comparedwith placebo; furthermore, cortical thickness and corticalarea also increased with odanacatib compared with pla-cebo, whereas total cross-sectional area did not. Takentogether, these findings suggest the deposition of new boneon the endosteum of the femoral neck, which is biome-chanically advantageous.
In interpreting the changes assessed by these differentmodalities (DXA and QCT), it is important to appreciate
% C
hang
e Fr
om B
asel
ine
(SE)
-4
6
5
4
3
2
1
0 2 4 6 8 10Time (months)
12 14 16 18 20 22 24
0
-1
-2
-3
-4
-2
0
2
4
6
8ODN 50 mg OWPlacebo OW*
**
**
**
*
**
**
*
** †
*P<0.001, **P<0.05, †P<0.01
Volumetr ic BMD
TH in
tegr
al
TH tr
abec
ular
TH co
rtica
lTr
inte
gral
Tr tr
abec
ular
Tr co
rtica
lFN
inte
gral
FN tr
abec
ular
FN co
rtica
lFN
corti
cal B
MC
FN co
rtica
l volu
me
A
B
Mea
n %
Cha
nge
From
Bas
elin
e
PBO Cortical ThicknessODN Cortical ThicknessPBO Total AreaODN Total AreaPBO Cortical AreaODN Cortical Area
Figure 4. Additional QCT imaging at the hip. A, Twenty-four-monthvBMD, femoral neck cortical bone mineral content (BMC), and corticalvolume. FN, femoral neck; ODN, odanacatib; PBO, placebo; TH, totalhip; Tr, trochanter. B, QCT measurements over time at the femoralneck using Bone Investigational Toolkit software (measurementsperformed at the smallest cross-section of the femoral neck).*P � .001; **P � .05; †P � .01.
Table 2. Iliac Crest Bone Biopsies
Bone BiopsyEnd PointMean (SD)
Odanacatib50 mg OW
(n � 5)
PlaceboOW
(n � 5)2D
Bone volume/total volume 0.22 (0.07)a 0.13 (0.04)a
Osteoid thickness, �m 5.06 (1.07) 5.60 (0.85)Osteoid volume, % 0.61 (0.60) 1.87 (1.02)Mineral apposition rate,
�m/d0.58 (0.05)b 0.56 (0.10)
Mineralizing surface, % 5.52 (5.88) 6.32 (4.22)Mineralization lag time, d 21.03 (23.88)b 31.96 (36.63)Bone formation rate, total
volume referent, %/y18.72 (16.29)b 23.14 (13.94)
Bone formation rate, totalsurface referent,�3/�2�d
0.04 (0.03)b 0.03 (0.02)
Eroded bone surface, % 1.90 (1.32) 1.66 (1.13)Activation frequency per
year0.47 (0.38)b 0.50 (0.30)
Mean wall thickness,�m
28.20 (2.44) 25.1 (0.77)
Cortical thickness �m 760 (184) 760 (165)Trabecular thickness �m 150 (41) 108 (8)Osteoclast bone surface,
% trabecular surfacecovered by osteoclasts
0.93 (0.92) 0.35 (0.23)
3DBone volume/total
volume, %0.21 (0.07)a 0.13 (0.04)
Connectivity density,number/mm
3.08 (1.07)a 3.79 (1.41)
Structure model index,0–3
1.14 (0.60) 1.29 (0.41)
Trabecular number,number/mm
1.22 (0.21)a 1.17 (0.15)
Trabecular thickness, mm 0.21 (0.04)a 0.14 (0.01)Trabecular separation, mm 0.80 (0.15)a 0.82 (0.11)
Abbreviations: 2D, 2-dimensional; ODN, odanacatib; OW, onceweekly.a n � 6.b n � 4.
J Clin Endocrinol Metab, February 2013, 98(2):571–580 jcem.endojournals.org 577

some of the underlying technical issues. First, the dataindicate a different pattern of change with odanacatibtreatment for vBMD compared with aBMD and estimatedstrength by FEA. However, changes in vBMD and aBMDwill be the same only if the regions are well matched andthere are no changes in volume of the bone and no changesin the size of the region of interest used for the measure-ment. At the spine, the regions are not matched, with QCTmeasuring only trabecular bone of 2 vertebrae, whereasDXA included the whole vertebral body as well as theposterior elements of the 4 vertebrae. At the hip, the re-gions are more closely matched, but differences in thephysics of the measurement and analysis software couldcontribute to the observed differences. Second, measuresof cortical properties from QCT scans depend on the im-age resolution and the assumptions made by the analysissoftware in terms of what is true endosteal cortical bone vsadjacent trabecular bone and what is the true periostealsurface. The increase in cortical thickness in conjunctionwith the lack of increase in cortical BMD, as analyzed byQCTPro (Mindways Software), could be an artifact of thesoftware’s edge detection routine (the FEA software doesnot have this particular limitation). Finally, it should benoted that FEA reflects the biomechanical effects of thetotal bone mass and its distribution in these regions. FEAstrength estimates are insensitive to whether a region isclassified by the software as trabecular or cortical bone.Thus, although DXA and FEA are consistent in showingimprovements with odanacatib from 12 to 24 months,further analyses are required to better elucidate thechanges in the individual cortical and trabecular compart-ments and at the endosteal and periosteal surfaces.
In preclinical primate studies of odanacatib, periostealbone deposition was stimulated at the proximal femur andfemoral neck (10, 12). Similar observations were reportedwith another cathepsin K inhibitor, balicatib (13). TheQCT methodology in the current study did not have theresolution to detect periosteal bone formation, so it is notknown from this analysis whether bone formation on theperiosteal surface might also be contributing to the in-crease in measures of cortical thickness in this study.
Bone turnover markers are a means of detecting sys-temic changes in bone formation and resorption. Thechanges in bone turnover markers in the current study areconsistent with results of the phase 2 trial, showing per-sistent reduction in bone resorption markers but only tran-sient reduction in bone formation markers that resolvedwithin approximately 2 years (7). The reduction in boneresorption markers in the current study was accompaniedby a trend toward increases in osteoclast surface and num-bers, although resorption lacunae tended to be either non-existent or very shallow. Iliac crest bone biopsy results are
also consistent with the bone formation marker results.Although the biopsies in the current study were limited innumber, the results were similar to the phase 2 trial (7) inwhich indices of bone formation in odanacatib-treatedwomen showed little difference from the placebo-treatedwomen after 2 years. In this trial, both 2- and 3D measuresof trabecular thickness were greater in the odanacatib-treated women, as was the 3D measure of trabecular num-ber, suggesting that odanacatib treatment may increaseboth trabecular number and thickness, as well as trabec-ular connectivity. However, 3D measures of connectivitydensity were not increased, and the sample size is insuffi-cient to reach firm conclusions regarding connectivity.
Taken together, the biopsy results from both studies, aswell as the bone formation marker results, support a rel-ative sparing of bone formation, which is unique to themechanism of action of this drug. Although the exact cel-lular mechanism is not completely understood, odana-catib treatment in primates has been shown to clearly in-crease osteoclast number (6), and in the odanacatib phase2 clinical study, the osteoclast marker tartrate-resistantacid phosphatase 5b was seen to increase after 3 years oftreatment (8, 9). It is likely that this osteoclast-rich envi-ronment provides the stimulus for osteoblastic bone for-mation. This is distinctly different from what is seen his-torically with the use of bisphosphonates and denosumab,which reduce both bone formation and bone resorption(2–5).
Odanacatib was generally well tolerated. There wereno signals of skin, respiratory, dental, delayed fractureunion, or other AEs and no AEs suggestive of a scleroderma-like skin thickening, as reported with balicatib in phase 2clinical trials (34, 35). The limited number of iliac crestbone biopsies revealed no evidence of mineralization ab-normalities or woven bone.
In conclusion, treatment of postmenopausal womenwith low aBMD with odanacatib, compared with placebo,resulted in increased aBMD at the spine and hip; increasedtrabecular vBMD at the spine, hip, and hip subregions;increased integral vBMD at the hip and hip subregions;and decreased bone resorption with preservation of boneformation. Finite element-estimated strength also in-creased with odanacatib at the hip and spine. The resultssuggest that odanacatib treatment improved overall prox-imal femoral strength, in part by increasing trabecularBMD and endosteal bone apposition at the femoral neck.
Acknowledgments
We thank Dr. Vincent Lemoine for assistance in statistical analysis.
578 Brixen et al Bone Density and Strength With Odanacatib J Clin Endocrinol Metab, February 2013, 98(2):571–580

Address all correspondence and requests for reprints to: KimBrixen, Professor, MD, PhD, Head of the Institute of ClinicalResearch, University of Southern Denmark, Winsloewsvej 19,DK-5000 Odense C, Denmark. E-mail: [email protected].
This study was registered at clinicaltrials.gov, numberNCT00729183.
This work was funded by Merck Sharp & Dohme Corp, asubsidiary of Merck & Co, Inc.
Disclosure Summary: K.B. has received grant support, con-sulting fees, and payment for speakers bureau from MSD; R.C.has received grant support and consulting fees from MSD;A.M.C. has received honorarium from MSD for speaking at aninternational scientific symposium, and her institution has re-ceived grant support for this study; T.M.K. has received grantsupport, consulting fees, support for travel, and payment fordata review; T.F. has received grant support, consulting fees,support for travel, and fees for participation of data review ac-tivities as an employee of Synarc Inc; K.E. has received grantsupport, consulting fees, support for travel, and fees for partic-ipation of data review activities as an employee of Synarc Inc;R.R. is a paid consultant for Merck, Lilly, Amgen, and Novartis;B.D., N.V., S.A., E.R., and A.E.d.P. are employees of MerckSharp & Dohme Corp.
References
1. US Department of Health and Human Services. Bone health andosteoporosis: a report of the surgeon general. Rockville, MD: USDepartment of Health and Human Services, Office of the SurgeonGeneral; 2004.
2. Black DM, Schwartz AV, Ensrud KE, et al. FLEX Research Group.Effects of continuing or stopping alendronate after 5 years of treat-ment: the Fracture Intervention Trial Long-term Extension (FLEX):a randomized trial. JAMA. 2006;296(24):2927–2938.
3. Harris ST, Watts NB, Genant HK, et al. Effects of risedronate treat-ment on vertebral and nonvertebral fractures in women with post-menopausal osteoporosis: a randomized controlled trial. VertebralEfficacy With Risedronate Therapy (VERT) Study Group. JAMA.1999;282(14):1344–1352.
4. McClung MR, Bolognese MA, Sedarati F, Recker RR, Miller PD.Efficacy and safety of monthly oral ibandronate in the prevention ofpostmenopausal bone loss. Bone. 2009;44(3):418–422.
5. Cummings SR, San Martin J, McClung MR, et al. FREEDOMTrial. Denosumab for prevention of fractures in postmenopausalwomen with osteoporosis. N Engl J Med. 2009;361(8):756–765.
6. Masarachia PJ, Pennypacker BL, Pickarski M, et al. Odanacatibreduces bone turnover and increases bone mass in the lumbar spineof skeletally mature ovariectomized rhesus monkeys. J Bone MinerRes. 2012;27:509–523.
7. Bone HG, McClung MR, Roux C, et al. Odanacatib, a cathepsin-Kinhibitor for osteoporosis: a two-year study in postmenopausal womenwith low bone density. J Bone Miner Res. 2010;25(5):937–947.
8. Eisman JA, Bone HG, Hosking DJ, et al. Odanacatib in the treatmentof postmenopausal women with low bone mineral density: three-year continued therapy and resolution of effect. J Bone Miner Res.2011;26(2):242–251.
9. Langdahl B, Binkley N, Bone H, et al. Odanacatib in the treatmentof postmenopausal women with low bone mineral density: Fiveyears of continued therapy in a phase 2 study. J Bone Miner Res.2012;27(11):2251–2258.
10. Cusick T, Chen CM, Pennypacker BL, et al. Odanacatib treatmentincreases hip bone mass and cortical thickness by preserving endo-cortical bone formation and stimulating periosteal bon formation in
the ovariectomized adult rhesus monkey. J Bone Miner Res. 2011;27(3):524–537.
11. Cusick T, Pennypacker B, Pickarski M, Duong LT. Differential ef-fects of odanacatib and alendronate on bone turnover in the femoralneck of adult ovariectomized rhesus monkeys. J Bone Miner Res.2011;26(suppl 1).
12. Somayajula S, Kummari S, Bredbenner T, et al. Differentiation oftreatment effects of odanacatib from alendronate in ovariecto-mized rhesus monkeys using voxel based morphometry of quan-titative computed tomography images. J Bone Miner Res. 2011;26(Suppl 1).
13. Jerome C, Missbach M, Gamse R. Balicatib, a cathepsin K inhibitor,stimulates periosteal bone formation in monkeys. Osteoporos Int.2011;22(12):3001–3011.
14. Felsenberg D, Boonen S. The bone quality framework: determinantsof bone strength and their interrelationships, and implications forosteoporosis management. Clin Ther. 2005;27(1):1–11.
15. Bouxsein ML, Seeman E. Quantifying the material and structuraldeterminants of bone strength. Best Pract Res Clin Rheumatol.2009;23(6):741–753.
16. Crawford RP, Cann CE, Keaveny TM. Finite element models predictin vitro vertebral body compressive strength better than quantitativecomputed tomography. Bone. 2003;33(4):744–750.
17. Amin S, Kopperdhal DL, Melton LJ 3rd, et al. Association of hipstrength estimates by finite-element analysis with fractures inwomen and men. J Bone Miner Res. 2011;26(7):1593–1600.
18. Keaveny TM, Hoffmann PF, Singh M, et al. Femoral bone strengthand its relation to cortical and trabecular changes after treatmentwith PTH, alendronate, and their combination as assessed by finiteelement analysis of quantitative CT scans. J Bone Miner Res. 2008;23(12):1974–1982.
19. Recker RR, Delmas PD, Halse J, et al. Effects of intravenous zole-dronic acid once yearly on bone remodeling and bone structure.J Bone Miner Res. 2008;23(1):6–16.
20. Black DM, Greenspan SL, Ensrud KE, et al. The effects of parathy-roid hormone and alendronate alone or in combination in post-menopausal osteoporosis. N Engl J Med. 2003;349(13):1207–1215.
21. Sornay-Rendu E, Boutroy S, Munoz F, Delmas PD. Alterations ofcortical and trabecular architecture are associated with fractures inpostmenopausal women, partially independent of decreased BMDmeasured by DXA: the OFELY study. J Bone Miner Res. 2007;22(3):425–433.
22. Melton LJ 3rd, Riggs BL, Keaveny TM, et al. Structural determi-nants of vertebral fracture risk. J Bone Miner Res. 2007;22(12):1885–1892.
23. Black DM, Bouxsein ML, Marshall LM, et al. Proximal femoralstructure and the prediction of hip fracture in men: a large prospec-tive study using QCT. J Bone Miner Res. 2008;23(8):1326–1333.
24. Hernandez CJ, Keaveny TM. A biomechanical perspective on bonequality. Bone. 2006;39(6):1173–1181.
25. Roberts BJ, Kopperdahl D, Thrall E, Muller JA, Keaveny TM,Bouxsein ML. Prediction of femoral strength in a sideways fall con-figuration using QCT-based finite element analysis. Proceedings ofthe International Bone and Mineral Society. Bone. 2009;44(suppl1):S72.
26. Wang X, Sanyal A, Cawthon PM, et al. Prediction of new clinicalvertebral fractures in elderly men using finite element analysis of CTscans. J Bone Miner Res 2012;27(4):808–816.
27. Imai K, Ohnishi I, Matsumoto T, Yamamoto S, Nakamura K. As-sessment of vertebral fracture risk and therapeutic effects of alen-dronate in postmenopausal women using a quantitative computedtomography-based nonlinear finite element method. OsteoporosInt. 2009;20(5):801–810.
28. Melton LJ 3rd, Riggs BL, Keaveny TM, et al. Relation of vertebraldeformities to bone density, structure, and strength. J Bone MinerRes. 2010;25(9):1922–1930.
29. Orwoll ES, Marshall LM, Nielson CM, et al. Finite element analysis
J Clin Endocrinol Metab, February 2013, 98(2):571–580 jcem.endojournals.org 579

of the proximal femur and hip fracture risk in older men. J BoneMiner Res. 2009;24(3):475–483.
30. Keyak JH, Sigurdsson S, Karlsdottir G, et al. Male-female differ-ences in the association between incident hip fracture and proximalfemoral strength: a finite element analysis study. Bone. 2011;48(6):1239–1245.
31. Kopperdahl DL, Hoffmann P, Sigurdsson S, et al. Enhancementof hip fracture prediction using finite element analysis of CTscans. Proc Annual Meeting of the American Society for Bone andMineral Research, October 15–19, 2010; Toronto, Ontario, Can-ada. Abstract FR0300.
32. Keaveny T, McClung M, Genant H, et al. Denosumab improvesboth femoral and vertebral strength in women with osteoporosis:
results from the FREEDOM Trial. Annual Meeting of the AmericanSociety for Bone and Mineral Research, October 15–19, 2010, To-ronto, Ontario, Canada. Abstract 1099.
33. Boonen S, Adachi JD, Man Z, et al. Treatment with denosumabreduces the incidence of new vertebral and hip fractures in post-menopausal women at high risk. J Clin Endocrinol Metab. 2011;96(6):1727–1736.
34. Peroni A, Zini A, Braga V, Colato C, Adami S, Girolomoni G. Drug-induced morphea: report of a case induced by balicatib and reviewof the literature. J Am Acad Dermatol. 2008;59(1):125–129.
35. Runger TM, Adami S, Benhamou CL, et al. Morphea-like skin re-actions in patients treated with the cathepsin K inhibitor balicatib.J Am Acad Dermatol. 2012;66(3):e89–e96.
Members have FREE online access to current endocrine Clinical Practice Guidelines.
www.endo-society.org/guidelines
580 Brixen et al Bone Density and Strength With Odanacatib J Clin Endocrinol Metab, February 2013, 98(2):571–580