Embed Size (px)
Citation preview

TISSUE ENGINEERING IN ORTHOPEDIC SURGERY 0030-5898/00 $15.00 + .OO
BONE CELLS AND MATRICES IN ORTHOPEDIC
TISSUE ENGINEERING
James E. Fleming, Jr, MD, Charles N. Cornell, MD, and George F. Muschler, MD
The use of cells for the purpose of ortho- pedic tissue engineering started more than 300 years ago. The first attempt of bone grafting was reported in 1668 by the Dutch surgeon Job Van Meek'ren.67 In 1867, Ollier performed a se- ries of experiments using transplanted peri- osteum and concluded that transplanted peri- osteum and bone remained alive and formed new bone. The osteogenic potential of trans- planted bone marrow was later documented by G o ~ j o n ~ ~ in 1869, then by MacewerP in 1881. Efforts of Albee1t2 and Phemistergo high- lighted further the utility of bone transplan- tation for the healing of fractures and bone defects. The techniques for autografting pio- neered by these individuals remained largely unchanged until today. Advances in under- standing of the biology of osteogenic cells, the availability of many highly purified peptide growth factors, and the capacity to create highly specialized implantable materials have launched an explosion of new advances in bone grafting and bone regeneration, all under the banner of tissue engineering. This new field is rapidly expanding the armamentarium of orthopedic surgeons in every setting in which
bone healing is required. Composites of cells and matrices are at the core of this revolution.
CORE CONCEPTS IN TISSUE ENGINEERING OF BONE
The ultimate goal of bone tissue engineer- ing is to create a bone-healing response in a precise anatomic area in which bone is desired. Clinical success further requires that the bone formed becomes integrated structurally with the surrounding skeleton and that the bone formed remodels reliably to provide the me- chanical properties of load bearing and fatigue resistance necessary for durable and effective function.
There are several basic tenants of tissue engineering, but among the first principles is that all new tissue regeneration requires the presence of cells that are capable of forming the tissue desired. Using the example of bone formation, one must be confident that the site contains a sufficient number of osteogenic pro- genitors to produce the bone desired. A suffi- cient number of osteogenic progenitors may be
From the Departments of Orthopaedic Surgery UEF, GFM) and Biomedical Engineering (GFM), The Cleveland Clinic Foundation, Cleveland, Ohio; Department of Orthopedic Surgery, Hospital for Special Surgery (CNC); and Department of Orthopaedic Surgery, Weill Medical College of Cornell University (CNC), New York, New York
ORTHOPEDIC CLINICS OF NORTH AMERICA
VOLUME 31 -NUMBER 3 'JULY 2M)O 357

358 FLEMING et a1
present locally in many tissue sites. If the num- ber of osteogenic progenitors is deficient, how- ever, one must either engineer the site to pro- vide the necessary population or use some stimulus to recruit the necessary population of cells to the site.
Assuming that progenitors are present in sufficient numbers, several other objectives must be met. First, the necessary cells must be distributed throughout the grafted volume to ensure that the bone-healing response is con- tiguous and integrates with the adjacent skele- ton. To accomplish this, the site must be filled with a matrix or material that facilitates the attachment, migration, and differentiation of osteoblastic progenitors, to allow the bone- healing response to progress throughout the site. A matrix or material having these prop- erties is considered osteoconductive.
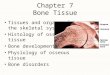
Given a sufficient competent cell popula- tion and the means of distributing the cells necessary for transducing the bone-healing re- sponse throughout the grafted volume, it is also necessary that the cells in the graft site receive stimuli that allow them to progress to- ward a bone phenotype. As discussed subse- quently, the population of osteogenic cells is, in fact, a pleuripotent population, capable of differentiation along pathways leading to many other tissue types. As a result, signals from soluble growth factors secreted as auto- crine or paracrine factors or stimuli from bioactive molecules contained in or on the sur- face of an implanted matrix can influence strongly the end result of tissue formation in a graft site. Many signals are present in the nor- mal cascade of events in osteoblastic differen- tiation, which modulate proliferation, deter- mination, and differentiation, as diagramed schematically in Figure 1. As a group, the stim- uli from these growth factors and adhesion molecules are termed osteoinductive stimuli.
Most of the graft materials that are cur- rently in use possess one or more of these properties: osteogenic cells, osteoconductive matrix, or osteoinductive stimuli (Table 1). These same properties can be found in a va- riety of synthetic materials and purified growth factors. Using these tools, it is the goal of tissue engineers to design combinations of existing materials, or new materials, that can be used clinically to create an optimal bone-
healing environment and grafting methods that equal or exceed the efficacy of existing methods. Such methods may be able to reduce the cost of existing procedures or allow en- tirely new approaches to treatment in some settings.
Before concluding a discussion of core concepts in tissue engineering, two other con- cepts, which are critical to the success of any bone-healing response, need to be mentioned: vascularity and mechanical stability. These two factors are largely in the hands of the surgeon who prepares the patient and the graft site for a procedure requiring bone tissue regenera- tion. Even in the setting of optimal materials combining osteogenic, osteoconductive and osteoinductive stimuli, the fate of cells in a graft site depends on preparation of the tissue bed to ensure a good blood supply and opti- mal preservation of local osteogenic cells through meticulous tissue handling. The vas- cular bed acts as a vehicle to deliver inflam- matory cells, which secrete stimulatory fac- tors. Vascularity also transports oxygen and nutrients to the repair site and acts as a con- ductive pathway for endothelial cells and os- teoblastic progenitors. Patient management and patient selection also remain critical spe- cifically the need to optimize nutritional and health status preoperatively and to avoid pharmacologic agents that may inhibit the bone-healing response (such as nonsteroidal anti-inflammatory drugs, steroids, and nico- tine) during the perioperative period.
The mechanical environment is also impor- tant to the success of the repair. The mechan- ical environment in a graft site is an important biologic stimulus, which, in part, determines the pathway of differentiation selected by cells in the graft site. For example, micromotion may direct local and chemoattracted connective tissue progenitors toward a fibrocartilaginous pathway, resulting in nonunion. Bone is fa- vored in a site in which tissue strain is limited.
Using the overall conceptual framework just described, this article reviews the current concepts related to osteoblastic progenitor cells and osteoconductive matrices, used alone or in combination. A more detailed discussion of the concept of osteoinduction and the pos- sible applications of osteoinductive materials in tissue engineering is presented in another article in this issue.

BONE CELLS AND MATRICES IN ORTHOPEDIC TISSUE ENGINEERING 359
StemCell Progenitor * Preosteoblast * Osteoblast
Resting * Proliferation * Matrixsynthesis * Mineralization
c-fos Cbfal AP Collagen X, BSP c-jun Collagen1 * OP * VDR H4 AP ON Osteocalcin
# " V
IGFsf E2 VitD 6
P BMPS
Figure 1. The osteoblastic pathway. Stages of osteoblastic differ- entiation, the predominant activity of the differentiation cell at each stage, some of the characteristic genes expressed at each stage, and the approximate site of principal action for some of the principal osteotropic growth factors and hormones. H4 = H4 histone; Cbfal =transcription factor core-binding factor (Y, AP = alkaline phosphatase; OP = osteopontin; ON = osteonectin; BSP = bone sialoprotein; VDR = vitamin D receptor; PDGF = platelet-derived growth factor; EGF=epithelial growth factor; bFGF= basic fibro- blast growth factor; TGF-B = transforming growth factor-beta; IGFs = insulin-like growth factors I and II; IL-6 = interleukin-6; E2 = estradiol; Vit D =vitamin D,; PTH = parathyroid hormone; PTHrp = parathyroid hormone related peptide; BMP =bone mor- phogenetic protein family.
OSTEOGENIC CELLS
Sources of Osteogenic Cells
Osteogenic cells are cells capable of pro- ducing bone or differentiating into a bone- forming cell. These cells are found in perios- teum, peritrabecular soft tissues, and bone marrow harvested by aspiration. These cells are presumed to be derived from a small pool of undifferentiated pleuripotential connective tissue stem cells, although the physical loca- tion and precise characteristics of these pro- genitors within bone are not known. Osteo-
blastic progenitors can also be found in soft tissues. Several authors have shown that vas- cular pericytes can be induced to proliferate and differentiate to express a bone phenotype in vitro, suggesting these cells may be a source of osteoblastic progenitors.8,81,w
Most of the work on osteoblastic progen- itors has been done in bone marrow harvested from rats. Classic studies have shown the abil- ity of marrow cells to form bone at a variety of extraskeletal sites, suggesting the presence of an undifferentiated precursor cell in post- natal m a r r o ~ ? ~ , ~ Further studies of bone mar- row-derived progenitors have suggested the
Table 1. PROPERTIES OF CLINICAL AND EXPERIMENTAL GRAFT MATERIALS
Material Osteogenic Osteoinductive Osteoconductive
Autogenous cancellous bone + + + Autogenous cortical bone + + + Vascularized autograft + + + Allograft - + / - + Deproteinated xenograft - -
Collagen - -
+ Bone marrow + + +
+ + DBM - + + Ceramics - -
BMP - - + + DBM = Demineralized bone matrix; BMP = bone morphogenetic protein; + = moderate; - = none; + + = marked; + / - = some.

360 FLEMING et a1
presence of two populations of osteogenic pre- cursor cells: determined osteogenic precursor cells (DOPCs) and inducible osteogenic pre- cursor cells (IOPCS).*~,~ The DOPC is a com- mitted stem cell, which can proliferate but has committed to differentiate toward an osteo- blast phenotype. The DOPCs are capable of proliferation but may have committed irre- versibly to express a bone phenotype at ma- turity, without the need for further induction. DOPCs are found on bone surfaces and in per- itrabecular marrow stroma. In contrast, the IOPC represents a pleuripotent progenitor cell that is capable of differentiation into one or more of a variety of connective tissue pheno- types given appropriate stimulation, including bone,'6,63 cartilage," 91 fibrous tissue,I6 muscle,'6 fat,s5 and glial cells.93 The IOPCs are likely a more immature population of proliferating cells than the DOPCs but derived from the same pool of connective tissue stem cells, be- fore or after a commitment event, as shown in Figure 2. IOPCs are thought to be found pri- marily in bone marrow, periosteum, the spe- cialized pericyte cell of the vasculature, and perhaps the circulating blood.
Pleuripotential progenitor cells derived from bone marrow have been referred to by a variety of names, including mawow stromal cells, connective tissue progenitor cells, and mes- enchymal sfem cells. Usually, these terms have been applied to a small subset of bone marrow cells that exhibit several properties when cul-
Self-renewal
Expansion
Commitment
Differentiation
Terminal differentiation
Figure 2. The expansion of proliferating progenitor cells, resulting from the activation of one resting stem cell. The number of progenitors is expanded exponentially. At some point during this expansion, cells become committed to ter- minal differentiation. Before commitment to osteoblastic differentiation, these cells may be considered to be induc- ible osteoblastic progenitors (IOPCs). After commitment, cells destined to become osteoblasts may be considered determined osteoblastic progenitors (DOPCs).
tured, including the ability to adhere readily to tissue culture plastic and to proliferate ex- tensively while retaining the ability to express several phenotypes. The authors use the term connective tissue progenitor for two main rea- sons: First, the concept of a stem cell is usually reserved for a rare, undifferentiated, and non- dividing cell, which can be induced to divide asymmetrically. This asymmetric division pro- duces one proliferating daughter cell and one resting stem cell, which is identical to the mother cell. In this way, the population of stem cells is preserved for continual generation of new proliferating progenitors. Using this con- cept, proliferating cells, by definition, are not stem cells, although they may remain pleuri- potential. Second, stromal cells in bone mar- row are a histologically defined population of structural connective tissue cells in bone mar- row, which produce cytokines necessary for the support of hematopoiesis. Stromal cells in bone marrow are much more numerous than the pleuripotent proliferative progenitors in bone marrow. It is more likely, in the authors' view, that bone marrow stromal cells are a ma- ture phenotype in bone marrow, possibly de- rived from the same connective tissue stem cells, which give rise to bone and other tissue phenotypes.
Osteoblastic Differentiation
Differentiation of osteoblastic cells, begin- ning from an original stem cell, can be broken down into several theoretic stages. The initial proliferative phase is characterized by expres- sion of nuclear proteins H4 histone, c-fos, and c-jun. After expression of transcription factor core-binding factor a, (Cbfal), one finds up- regulation of gene products for type I collagen, osteopontin, osteonectin, and alkaline phos- phatase. Finally, a matrix mineralization phase culminates in an osteoblastic phenotype dis- tinguished by the expression of osteocalcin, bone sialoprotein, and responsiveness to 125- dihydroxy vitamin D and parathyroid hor- mone.59,m,65,s6 The pathway of osteoblastic dif- ferentiation has been shown to be mediated and potentiated by many osteotrophic factors and cytokines (see Fig. 1).

BONE CELLS AND MATRICES IN ORTHOPEDIC TISSUE ENGINEERING 361
In response to an inducing event, the stem cell may undergo one or more cycles of asym- metric cell division. The term self-renewal is used to describe this process. One cycle pro- duces one proliferating daughter cell and leaves one stem cell. Two cycles of asymmetric cell division produce one proliferating progen- itor but two stem cells. In the latter case, the number of resting stem cells is increased by the event (see Fig. 2).
After the production of a proliferating daughter cell, a period of proliferation or ex- pansion follows. During this phase, the num- ber of progenitors is expanded dramatically. Based on a conservative estimate of the amount of bone made per mature osteoblast and the minimum number of stem cells that might be activated, one can estimate that the average daughter cells may divide 6 to 14 times before committing to a mature bone phe- notype. The number of mitoses between acti- vation of the stem cell and commitment to a mature phenotype is a critical variable in bone physiology because the number of times a daughter cell divides is a principal determi- nant of the number of mature osteoblasts and therefore the amount of bone formed after the activation of a stem cell.
In vitro data, using human and animal cells, indicated that the process of commitment to a mature phenotype is likely a multistep process that begins during the proliferative phase. This process occurs in response to a combination of intracellular and extracellular signals and is mediated by changes in gene ex-
Fibrous Tissue
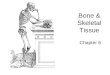
pression, which, in turn, induce further changes leading to a mature phenotype. Often this pro- cess of commitment is signaled by a small number of molecules, known as transcription factors. For example, MyoD and the myogenin are a helix-loop-helix family of molecules, which serve as key genetic regulatory agents in muscle differentiation. When these proteins are expressed in a cell, the cell becomes com- mitted to a muscle phenotype. Peroxisome pro- liferator-activated receptor gamma 2 (PF'Al3-y) is a transcription factor and early response gene involved in the commitment to the adi- pocytic differentiation pathway? At least one of the transcription factors, which regulate commitment to the bone phenotype, has been reported to be Cbfa1.96 Expression of Cbfal ap- pears to be necessary and sufficient to induce a diverse repertoire of genes associated with the osteoblastic phenotype and is hypothe- sized to represent a master switch for osteo- blastic differentiati~n.~,~' Animals engineered to develop without Cbfal show marked de- fects in membranous and endochondral bone formation and essentially an absence of oste- oblastic cells.@ Similarly, lack of expression of one allele of the Cbfal gene forms the basis of the human cleidocranial dysplasia syndrome, an autosomal dominant disorder.70 A brief summary of potential pathways of connective tissue progenitors and key known genetic regulatory elements controlling commitment events is shown in Figure 3.
The commitment step is another critical variable in determining the amount of bone
.
Stromal
\ I h Cell Fat V Cartilage
Bone
Figure 3. Possible lineage pathways for the undifferentiated con- nective tissue after the occurrence of commitment and differentia- tion events. Known genetic regulatory elements that control com- mitment toward a specific cell phenotype include MyoD and Myogenin; PPAR-y (Peroxisome proliferator-activated receptor gamma); and Cbfal (transcription factor core-binding factor a,).

362 FLEMING et a1
formed after activation of an individual stem cell. Because connective tissue progenitors are pleuripotent, they may be induced to commit to several different mature phenotypes. As a result, the decision of one or more progeny of a daughter cell to commit to an alternative pathway has a direct impact on the number of cells available for osteoblastic differentiation (Fig. 4). This decision tree for commitment in- cludes the possibility that some progenitors may be induced to undergo programmed cell death, or apoptosis, rather than complete the process of differentiation. Several authors have suggested that at least one of the causes of os- teoporosis may be an age-related or hormon- ally related increase in adipocytogenesis or apoptosis, at the expense of bone formation?
Tools for Identifying and Using Osteogenic Cells
Osteoblastic cells are the focus of any at- tempt to use the concepts of tissue engineer- ing. Identdymg and characterizing these cells has proved difficult, however. Despite this dif- ficulty, several methods of isolation and char- acterization of osteoblastic progenitors and several potential markers for connective tissue progenitors have become a~a i l ab le .~ ,*~J~ The most easily used marker for the osteoblastic phenotype is alkaline phosphatase, which is expressed relatively early during osteoblastic
em Commits to Commits to
adipocytogenesis apoptosis
\ =* J 0.0-
oo**-*** 0000~**~****0*** - 8 osteoblasts
Figure 4. The effect of commitment to alternative pathways on the number of mature osteoblasts. The adipocytic path- way is shown. During expansion of connective tissue pro- genitor cells, events triggering apoptosis (programmed cell death) or commitment to pathways other than the osteo- blastic pathway ultimately will result in a diminution in the number of bone-forming osteoblasts. This alteration in commitment events may be a contributing mechanism to some clinical disease states such as the relatively adipo- genic marrow seen in osteoporotics.
differentiation. Not all cells, however, that ex- press alkaline phosphatase are osteoblastic. Before expression of alkaline phosphatase, there are only a few markers that can be used to identify human osteoblastic progenitors or connective tissue progenitors. For example, the STRO-1 antibody has been developed and recognizes an antigen expressed by 7% of nu- cleated bone marrow cells, including all oste- oblastic and stromal cell precursors.lW A sub- set of cells expressing the STRO-1 antigen have been shown to have the capacity to differen- tiate along several mesenchymal lineages, in- cluding the osteoblastic lineage.3s This marker is thought to be lost near the time alkaline phosphatase is expressed. Bruder et all1 have reported on several antibodies recognizing hu- man osteoblastic progenitors, including the SB-10 antibody, whose antigen corresponds to leukocyte-cell adhesion molecule (ALCAM) and appears to be expressed during early stages of osteogenic differentiation and lost during the developmental expression into dif- ferentiated phenotypes. The SH2 monoclonal antibody appears to recognize an 80-kd cell surface glycoprotein that is expressed by preosteoblasts in the periosteum in vivo and can be detected on in vitro cultures of human connective tissue progenitors.2s,40 The avail- ability of these markers may help to identdy precursor cells from the heterogeneous mar- row populations from which they reside and may help to define further critical cellular events during osteogenic differentiation.
OSTEOGENIC GRAFT MATERIALS
Autologous Cancellous Bone
Autologous cancellous bone is the current gold standard as the most effective graft ma- terial for the enhancement of bone healing, in- cluding spinal fusion, bone defects, and frac- ture repair.26,43,74,9s An autogenous cancellous graft transplants osteogenic bone and marrow cells; an osteoconductive matrix of collagen, mineral, and matrix proteins; and osteoinduc- tive proteins associated with the matrix. Stud- ies by Burwell16 in the 1960s suggested the for- mation of new bone following autograft was a manifestation of primitive osteogenic cells that

BONE CELLS AND MATRICES IN ORTHOPEDIC TISSUE ENGINEERING 363
survived transplantation and proliferated to form mature osteoblasts.
There are several drawbacks to autoge- nous bone graft that have fueled the interest in orthopedic tissue engineering of cells and matrices that can match or exceed the osseous repair capacity of autogenous cancellous bone. For example, there is significant morbidity as- sociated with the harvest of iliac crest bone graft, the most common site to procure osteo- genic graft. Major complications, such as cu- taneous nerve damage, chronic donor site pain, vascular injury, infection, and iliac frac- ture, have been reported in approximately 10% of patient^.^^,'^ Harvest of autogenous cancel- lous bone results in additional permanent scars in many patients. There are many clinical circumstances when the amount and avail- ability of autogenous bone may be insufficient. Various reports have indicated a failure of fu- sion with autologous bone graft of approxi- mately 34% .Io1 Overall, this situation leaves sigruficant opportunity for improvement.
Bone Marrow as an Osteogenic Cell Source
Bone marrow alone may be used as an effective osteogenic graft and is probably un- derused in current clinical practice. Bone marrow harvested by aspiration contains os- teoblastic progenitors with other bone mar- row-derived cells that are rich in cytokines. It also provides a degradable biologic matrix of fibrin, which can be revascularized rapidly. Connolly et aP1 reported successful treatment of 18 of 20 tibia1 nonunions treated closed or with intramedullary nails plus percutaneous injection of nonheparinized bone marrow. Al- ternatively, autogenous marrow can be used as an adjuvant to augment bone grafting proce- dures by combining it with other materials, such as allograft or engineered
Muschler et a171 have shown that bone marrow aspirated from the iliac crest is diluted 20 to 40 fold by peripheral blood but still con- tains a mean of about 1000 to 1400 connective tissue progenitors (CTPs) per aspirate. They have shown that the concentration of CTPs can be optimized by limiting the aspiration vol- ume to 1 to 2 mL from any individual needle
site. Muschler et aln and Majors et aF3 have shown that women in particular show a sig- nificant age-related decline in the number of CTPs that can be harvested by aspiration, in- dicating that some patients may be better suited as subjects for bone marrow grafts than others.
In an attempt to improve the efficacy of a bone marrow graft, Connolly et a1,2O using a rabbit diffusion chamber model, reported that concentration of the progenitor population us- ing gradient centrifugation could increase the amount of bone formed after transplantation. Muschler et alE have reported data using a ca- nine posterior spinal fusion model that show improved frequency and quality of union when the concentration of bone marrow-de- rived CTPs was increased. Further improve- ments in methods for selection, concentration, and delivery of CTPs using new or existing materials for cell delivery are likely to increase significantly the efficacy of bone marrow-de- rived grafts.
Autologous Cortical Bone
Cortical bone grafts are less successful bi- ologically than autogenous cancellous grafts, owing to several differences in cortical bone graft physiolog~.~~ The vascularization of cor- tical bone takes much longer because of the lack of porosity of cortical bone and conse- quent inhibition of vascular ingrowth. Cortical bone contains fewer osteoblastic progenitors than trabecular bone. The cells of the graft transplant are less likely to survive transplan- tation, principally resulting from the reduced diffusion of oxygen and nutrients through cor- tical matrix compared with trabecular bone. The number of nonosteogenic hematopoietic cells is also reduced, which may decrease the amount of paracrine stimulation in and around a cortical graft. Finally, the remodeling phase of graft incorporation is compromised in a cortical graft because resorption of the graft must precede osteogenic new bone for- mation.82
The principal advantage of cortical bone versus cancellous bone and other graft mate- rials stems from its superior mechanical strength and the availability of cortical seg-

364 FLEMINGetal
ments of sufficient size to fill large skeletal de- fects. The mechanical strength of allograft bone after implantation is a dynamic process. In the early phase, osteoclastic cutting cones re- sult in increased porosity and progressive loss of strength during the first 12 to 24 months after implantation. Subsequent remodeling and new bone formation reconstitute the me- chanical properties of the graft.82 This process results in an associated increased risk of graft failure and collapse during the first 6 to 24 months after implantation. The principal dis- advantage of autogenous cortical bone is that there are relatively few sites where bone can be harvested without accepting a significant morbidity (e.g., fibula, rib, tibia, hemicortex).
Vascularized autogenous bone grafts have all the problems with morbidity at the donor site but avoid the problems created by revas- cularization and creeping substitution over the first 24 months. A vascularized graft can also provide a much-needed source of blood sup- ply in a wound bed and be coupled with an attached free tissue flap to address local soft tissue defects.
OSTEOCONDUCTIVE MATRICES
The term osteoconduction applies to properties of materials that enhance the at- tachment, migration, and distribution of cells responsible for the bone-healing response throughout the volume of the graft site. This is a three-dimensional process that depends on the chemical surface properties of the implant, its three-dimensional structure and porosity, and its rate and mechanism of degradation. When porous osteoconductive structures are implanted into or adjacent to bone, cells from surrounding tissues migrate into available void volume of the matrix. The process is char- acterized by an initial ingrowth of fibrovas- cular tissue and new blood vessels. This tissue invades the void volume of the scaffold and is later followed by formation of new bone.
The osteoconductive substrate is not sim- ply a passive scaffold. Rather, the efficacy of these materials is a function of the chemical surface of the implant. This surface may have a direct effect on the cells that come in contact
with it. The surface may also serve as a site on which a variety of bioactive molecules from the wound site become concentrated, in- cluding growth factors and adhesion mole- cules.35,55,95 This ability to bind or deliver bioactive molecules to a wound-healing site makes many of these materials potential ve- hicles for delivery of exogenous bioactive growth factors. These applications are dis- cussed in other articles in this issue.
Allograft Bone Matrices
The porous structure of allograft bone with a cross-linked collagen matrix supple- mented with many chemical sites for attach- ment of progenitor cells and endothelial cells is perhaps the prototype for an osteoconduc- tive matrix. Allograft bone also contains many growth factors, which are embedded in the bone matrix and can be liberated by osteoclas- tic resorption. These growth factors include in- sulin-like growth factor type 11, transforming growth factor-p, platelet-derived growth fac- tor, fibroblast growth factor, and a small amount of bone morphogenetic proteins, which make allograft bone potentially osteoin- ductive. Demineralization may enhance fur- ther the bioavailability of the growth factors embedded in allograft bone matrix. The fact that allograft bone matrix is fully resorbable through normal metabolic pathways that oc- cur in a physiologic pH environment, which is fully compatible with ongoing osteoblastic dif- ferentiation and the fact that this degradation produces no reactive by-products or debris add greatly to the appeal of allograft bone as a graft material.
Allograft bone has historically been a well-characterized alternative to autogenous bone. The earliest well-documented studies were performed by LexeP in the early 1900s; he transplanted knee joints and found that ap- proximately 50% of the grafts were functional some years later. Modern processing of allo- graft bone involves extensive washing steps to reduce the number of residual cells. This washing significantly reduces the immuno- genic antigens that may remain in the graft and reduces the risk of transmission of virally mediated infections. Although allograft bone

BONE CELLS AND MATRICES IN ORTHOPEDIC TISSUE ENGINEERING 365
lacks any viable cells that might contribute to new bone formation at the graft site, allograft matrix is highly osteoconductive and has some osteoindudive properties."
Allografts have several advantages over standard autografts: (1) The morbidity of har- vesting autologous bone is eliminated. (2) Al- lografts provide an essentially unlimited vol- ume of graft material in settings where the quantity of available autograft bone is insuf- ficient. (3) Because cortical allografts can be se- lected from any bone, they provide the sur- geon with a wider selection of physical sizes and much better structural properties than are available from autograft cortical bone. (4) Al- lograft can be processed into a wide variety of physical forms, which can be customized to specific applications. These forms range from gels, powders, fibers, and pastes to large struc- tural blocks. Products have evolved to provide customized function as a fixation device, such as threaded cylindrical bone dowels or cus- tomized wedges for spinal fixation.9s
The method of sterilization and prepara- tion of allograft tissue has a significant impact on osteoconductive, osteoinductive, and me- chanical properties as well as immunogenic- ity.'" Most grafts are harvested within 24 hours postmortem after the donor's health status and infectious disease status are screened. Immunogenicity is reduced, al- though not eliminated, by freezing to - 20°C, which also allows for preservation of the graft for approximately 1 year or Freeze- drying reduces further the immunogenicity of allogeneic bone and provides essentially in- definite shelf life, but at the price of reducing mechanical strength by 50% compared with fresh frozen bone ( - Z0°C).31,87
Clinical evidence of overt immunologic reaction or graft rejection is rare with allograft transplantation. Histologic evidence of a low- grade inflammatory reaction typical of alter- native tissue allografts is found around essen- tially all allografts, however. Many allograft recipients can be shown to develop antibodies to donor antigens, indicating the presence of some imm~nization.'~,~~ Several canine studies reveal a spectrum of histopathologic sequelae from mild inflammation at the host-donor in- terface to resorption of the graft and have doc-
umented improved biologic behavior in anti- gen-matched allografts.6J02
The principal disadvantages of allograft materials today are cost, the small but mea- surable risk of bacterial or viral infection, and donor-to-donor variation in quality. The time and resources needed for donor screening, sterile harvesting, transport, processing, cut- ting, packaging, quality control, and distribu- tion are large. A small risk of transmission of iatrogenic transmission of viral infection and human immunodeficiency virus (HIV) still ex- ists, although this risk has been minimized greatly by extensive donor screening and test- ing, extensive washing to remove donor cells and cell debris, and sterilization using high- dose radiation. Finally, donors do differ from one another with respect to the biologic effi- cacy of the matrix in standardized biologic as- says. These differences expose patients and physicians to some undesirable variation in performance, which may affect the clinical re- sults of bone grafting.34,35,74
Ceramic Matrices
Ceramic matrices for bone grafting gen- erally means calcium phosphate ceramics, such as hydroxyapatite, and tricalcium phos- phate (TCP). Both have been studied exten- sively. Calcium sulfate salt can also be in- cluded in this group. From a functional perspective, it is most useful to divide these materials into three groups: (1) rapidly resorb- ing ceramics, (2) slowly resorbing ceramics, and (3) injectable ceramic cements. The biol- ogy of these three processes is different, as is the resulting strategy for using these materials in a graft ~ i t e . ~ ~ , ~ ~
Rapidly Resorbing Ceramics and Calcium Salts
The classic rapidly resorbable calcium phosphate ceramic is TCP. Porous TCP im- plants can be created by compacting TCP pow- der with a carrier, such as naphthalene. The carrier is subsequently removed, creating a po- rous structure that is then sintered. The poros- ity in commonly available TCP preparations is approximately 35%, with pores ranging from

366 FLEMING et a1
100 to 300 pm. TCP has much greater solubility than hydroxyapatite, and as a result the im- plants are reabsorbed more rapidly. Because the porosity of bulk TCP implants is too small and the connections between pores are not complete, bone ingrowth within the grafted volume is never achieved before reabsorption of the TCP matrix. This situation makes the bulk form of TCP a poor bone graft substi- h.1te.3~ Granules of TCP may be more effective because the space between the granules in- creases the porosity of the matrix and increases the bioavailable surface.
A calcium and phosphate-rich surface layer and local microenvironment characterize TCP resorption. This region of high calcium phosphate concentration appears to improve the integration of the implants into host bone. The mechanism by which this integration oc- curs is unclear. Some authors have suggested that the high concentration of calcium and phosphate ions may initiate biomineralization or may in some manner influence osteogenic phenotypic commitment in the adjacent or in- grown t i s ~ u e s . ~ , ~ ~ Another proposed mecha- nism for the initiation of bone formation in- volves the osteoclast. The presence of TCP and local deposition of calcium phosphate crystals may stimulate local osteoclasts. Most biopsy specimens of calcium phosphate implants in- dicate an abundance of multinucleated cells appearing to resorb the TCP surface. Because activation of osteoclasts is associated with os- teoblastic activity with new bone f0rmation,3~ it is speculated that stimulation of local oste- oclastic activity may stimulate new bone for- mation. This hypothesis has not been con- firmed experimentally, however. Calcium sulfate implants are also clinically available for use as a bone graft substitute material. If effec- tive, these may function in a similar
Slowly Resorbing Ceramics
The classic slowly resorbing calcium phosphate ceramic is hydroxyapatite. Although hydroxyapatite can be made in a more soluble form by reducing the crystal size and addition of impurities, such as carbonates, highly crys- talline hydroxyapatite is stable in vivo and re- sorbed at a rate of only 5% to 15% per year.
The most representative example of po- rous and highly crystalline hydroxyapatite in current clinical practice is derived in a unique process from coral. Recognizing that a porous structure is needed to allow extensive invasion by host tissue, Chiroff et all9 first realized that corals made by marine invertebrates have a structure similar to cortical and cancellous bone and that they might be suitable grafts for skeletal application. The exoskeleton of the ge- nus Porites has a void volume of 66% with par- allel channels 230 pm in diameter. Intercon- necting fenestrations between channels 190 pm in diameter also occur. This structure is similar to that of cortical bone. The genus Goniporu has a microstructure similar to cancellous bone. Parallel longitudinal pores of 600 pm are in- terconnected with pores of 220 to 260 pm. A simple hydrothermal exchange process con- verts delicate coral calcium carbonate (CaCOJ into mechanically superior hydroxyapatite [Ca,,(PO,),(OH),] without altering the internal structure. Similar porous structures of TCP can also be prepared.
Extensive experimentation in animal models and human trials with hydroxyapatite porous implants has shown that these bulk im- plants are readily invaded by fibrovascular tissue, which later is converted to mature la- mellae bone.l7f6 The bone formed is nearly identical to that seen in autogenous grafts. Histologically, osteoid seams appear with vi- able osteoblasts and multinucleated giant cells and have an appearance suggesting active re- modeling of the newly formed bone.
These multinucleated, osteoclast-like cells also appear to resorb the surface of the im- plant.45 Some surface resorption occurs, but remodeling is extremely slow because of the insoluble, inert structure of crystalline hy- droxyapatite. No immunologic or giant cell re- action is noted surrounding bulk implants. The implants initially are mechanically weaker than host bone, but with invasion of host tis- sue, the strength of the implant increases pro- portionally? By 6 months in vivo, the ultimate strength may exceed that of host cancellous bone.
In the 1990s, bulk implants of coralline hy- droxyapatite have been used successfully to reconstruct contained metaphyseal defects. As yet, however, they have not been recom-

BONE CELLS AND MATRICES IN ORTHOPEDIC TISSUE ENGINEERING 367
mended for comminuted diaphyseal defects. It is expected that brittleness of coralline ceramic implants and the slow remodeling of a coral- line hydroxyapatite implant would leave dia- physeal sites susceptible to fatigue fracture through the residual implant or to fracture at the junction between the implant and the host bone.12
The mechanical environment into which an implant is placed has a critical effect on re- sult. Bucholz et all3 and Nagashima et alm have shown that rigid stability in close opposition to host bone is necessary for bone ingrowth. Micromotion prevents bone invasion into the implant. This fact must be considered when using these implants?
The slow resorption of coralline hydroxy- apatite is considered to be a disadvantage in many clinical settings. As a result, several modifications of hydroxyapatite substrates have been made to increase the rate of resorp- tion. One modification is a composite of hy- droxyapatite and calcium carbonate. This composite is formed by only partial comple- tion of the hydrothermal conversion of cal- cium carbonate to hydroxyapatite. This partial completion produces a material that is almost entirely calcium carbonate having a thin sur- face coating of hydroxyapatite. As a result, the early performance of the implant is the same as a pure hydroxyapatite implant. By a few months after implantation, however, hydroxy- apatite coating becomes eroded, exposing the calcium carbonate, which is then absorbed much more rapidly. Another entirely different modification of a hydroxyapatite ceramic is the preparation of a biphasic calcium phos- phate ceramic. One example of a biphasic ma- terial is composed of both hydroxyapatite (30%) and the more soluble TCP (70%).12,39,109 When this material is implanted, the TCP rap- idly dissolves, which leaves the porous HA structure on which new bone formation can proceed a more stable and long-lasting frame- work.
Injectable Ceramic Cements
Considerable effort has been directed to- ward developing injectable calcium phosphate cements. These cements are usually composed of various mixtures of a-TCP, dibasic dical-
cium phosphate, and tetracalcium phosphate monoxide. Components are mixed together as a liquid paste, which then gradually hardens into a crystalline phase, without generation of significant heat. Although some hydroxyapa- tite is formed, the hardened cement is largely composed of impure crystals of calcium phos- phate ceramic in phases, which are relatively soluble and readily remodeled by osteoclasts. Different formulations can result in cements of different setting times.68 The initial compres- sive strength of the hardened material is simi- lar to cancellous bone.
Histologically, invasion by vascular chan- nels with prominent osteoclastic activity is visible within a few weeks of implantation in vivo with new bone formation directly on the cement implant. Little to no inflammation or foreign body reaction is noted." Clinically, the cements can be injected into fracture sites or bone defects using closed or open methods. These cements have been shown to be useful in treatment of distal radius fractures.",52 They also show promise as adjuncts to the treatment of femoral neck fractures and possibly for ver- tebral body compression fractures and for en- hancing the early fixation of pedicle screws.
Collagen
Type I collagen bonded into its cross- linked fibrillar structure is the most abundant protein in the extracellular matrix of bone. Col- lagen is conducive to bone formation and min- eral deposition. Not only does its surface con- tain sites for deposition of mineral but also it binds the noncollagenous matrix proteins, which provide sites for cell attachment and for control of mineralization. For example, osteo- nectin, when complexed to collagen, becomes a strong promoter of crystal deposition, and acid phospholipid complexes facilitate hy- droxyapatite deposition into the
Clinically available purified bovine type I fibrillar skin collagen is not cross-linked. This collagen, however, provides a flexible sub- strate for preparation of a variety of matrix structures, including gels, powders, and po- rous sponges. Using various cross-linking agents, varying amounts of chemical cross- linking can be achieved, which can reduce

368 FLEMINGetal
significantly the degradation rate of the im- planted collagen matrix.
By itself, soluble fibrillar collagen func- tions poorly as a graft material. It has shown efficacy, however, as a delivery system for ce- ramic granules, bone morphogenetic proteins, and osteoblastic progenitor cells, significantly enhancing the performance of these materials. Werntz et allM showed that although collagen alone was ineffective in healing diaphyseal de- fects in the rat femur, the combination of col- lagen and bone marrow was superior to au- togenous cancellous bone alone. Johnson et ala as well as Grundel and Chapman39 found that a composite of collagen gel with granules of a biphasic ceramic of hydroxyapatite and TCP (Collagraft Zimmer, Warsaw, IN) improved bone regeneration significantly in a defect model compared with the use of the ceramic alone.
Experimental data are not unified with re- spect to the value of Collagraft as a bone graft volume expander. Zerwekh et allm found that Collagraft was effective when mixed with au- togenous bone as a bone graft extender in an- terior spinal fusion. In contrast, Muschler et al,76 in a posterior canine spinal fusion model, found that addition of Collagraft to an equal volume of autogenous bone was inferior to us- ing the smaller volume of autograft without the Collagraft, implying a harmful effect of Collagraft on autograft efficacy.
Bovine collagen presents a small risk of immunogenicity and can elicit a harmful im- mune reaction in a subdermal injection site.= Several studies, however, have shown no ad- verse effect when bovine collagen is implanted in skeletal sites. In a clinical trial of a gel of bovine fibrillar skin collagen combined with granules of a biphasic hydroxyapatite and TCP,17 approximately 5% of patients devel- oped detectable circulating antibody to type I bovine collagen. These antibodies did not show cross-reactivity to human collagen. More importantly, they did not result in dermal hy- persensitivity, and they did not correlate with the clinical outcome of the graft.
Hyaluronan (Hyaluronic Acid)
Hyaluronan is a large biologic molecule found as the central structural element of ag-
grecan in hyaline cartilage and as a large sol- uble component in normal joint fluid. Hyalu- ronan is also abundant in early fracture callus. It is not osteoconductive, in and of itself, but it has many unique features that make it po- tentially useful as a substrate for tissue engi- neering.
Hyaluronan, extracted from the combs of rooster chickens, is now clinically available in several highly purified forms. It is used in the eye, to replace the vitreous humor, and has been approved for intra-articular injection in the knee in early osteoarthritis. The handling and chemical properties of hyaluronan are unique. Hyaluronan can be prepared as a dilute solution and cross-linked to create a highly viscous and mechanically strong matrix with a large void fraction. The degradation rate of hyaluronan can be modulated through covalent cross-linking. At least one graft ma- terial is under development using hyaluronan as a matrix as a delivery system for human recombinant fibroblast growth factor type 2. Early animal data have been pr0mising.9~
Polylactic and Polyglycolic Acid Polymers
Degradable polymers have little osteo- conductive potential, in and of themselves.5o Polylactic acid, polyglycolic acid, and copoly- mers (PLGA) have been used extensively in surgical applications without inducing bone formation. These materials have been of inter- est to tissue engineers primarily because of their biocompatibility, their established safety as suture materials, and the versatility that they offer for producing chemically defined substrates for bone graft matrices. Finally, these polymers offer the potential for use as a time-release delivery system for peptide growth factors. Because degradation occurs by hydrolysis, the degradation rate can be mod- ulated over a wide range.49
The early orthopedic experience with de- gradable polymers was not entirely satisfac- tory. They are well tolerated in the early phase after implantation, but an inflammatory re- sponse is noted in tissues surrounding bulk implants. Hollinger and BattistoneM have studied the degradation of these polymers in

BONE CELLS AND MATRICES IN ORTHOPEDIC TISSUE ENGINEERING 369
muscle pouch models. Bulk implants of PLGA produce an acid environment through local ac- cumulation of the hydrolyzed monomers and incite a fibrinous exudate and edema by 72 hours. By 14 days, this formation evolves into a zone of granulation tissue with a cellular fi- brovascular capsule filled with particulate de- bris of the fragmenting polymer and chronic inflammatory cells. Six weeks after implanta- tion, the polymer is fragmented further and infiltrated by inflammatory cells. As a result, nearly all clinical studies of biodegradable PLGA fracture fixation screws report an ad- verse foreign body rea~tion.~
Despite these early difficulties, these ma- terials remain highly versatile. They can be fabricated in varied three-dimensional struc- tures, as porous foams, fiber mesh, or powders. These can be prepared under conditions that do not denature peptide growth factors, allow- ing these factors to be integrated within and delivered by the polymer in a time-release fashion during hydrolysis. This time-release fashion allows the possibility of multiphase delivery systems. In preliminary studies, post- fabrication mixing of PLGA beads with bone morphogenetic proteins show that inductive agents can be concentrated in a bone defect, resulting in accelerated bone regeneration.”,”
DESIGNING COMPOSITES OF CELLS AND MATRICES
Why Consider Cell-Matrix Composites?
All successful bone healing requires the presence of a sufficient number of osteoblastic progenitor cells. This concept is important be- cause in many clinical settings the number of local osteoblastic progenitors may be limited. As a result, implanting an osteoconductive material alone or even an osteoconductive ma- terial with one or more osteoinductive growth factors may not be adequate to accomplish a reliable and optimal bone-healing response. Settings that are likely to be deficient in oste- oblastic cells include sites of large bone de- fects, sites containing extensive scar tissue from previous surgery or trauma, sites of pre- vious infection or radiation, sites in which
local bone may be diseased, or sites with com- promised vascularity. Systemic conditions, such as diabetes or metabolic bone disease, or pharmaceutical agents, such as nicotine, sys- temic glucocorticoids, or chemotherapy, may also limit the number or function of progenitor cells. These conditions and agents are common in clinical practice.
In contrast, in many clinical settings, there may be no need to deliver osteogenic cells. A satisfactory clinical result may be predictable, for example, when grafting of contained me- taphyseal defects, fresh metaphyseal fractures, or other settings in which small-volume grafts are placed in healthy tissue beds. Even in these settings, however, addition of osteogenic cells may still be additive by increasing the rate of bone formation or the amount of bone formed.
Which Cells Should Be Included?
Given the several sources of osteoblastic cells and many available options for osteocon- ductive matrix materials, one of the next op- portunities in bone tissue engineering is to op- timize the combination of matrices and cells. Because it is the osteoblastic cell that does the work of bone formation, an appropriate first step in this process is defining the questions related to cell delivery. Do cells need to be added to the graft? If so, when? If so, how many cells are needed? Is it necessary only to add osteoblastic progenitors, or might addi- tion of other cells contribute to the success of a graft? If so, what other cells?
Osteoblastic cells or osteoblastic progeni- tors are the obvious candidate for inclusion in a cell matrix composite for bone tissue engi- neering. Osteogenic cells alone may not be op- timal, however. Under normal physiologic conditions, osteoblastic progenitors interact with many cells. Some of these interactions may be critical for optimal progression of bone regeneration. Platelets and growth factors se- creted by platelets play a large role in estab- lishing the biologic environment in an early fracture callus. Similarly, other selected cell types, including monocytes, T cells, and vas- cular endothelial cells, may be desirable part- ners for osteoblastic progenitors in an engi- neered graft site.

370 FLEMING et a1
What Source of Cells Should Be Used?
Any of the potential sources of osteoblas- tic progenitors discussed earlier could likely be used for bone grafting with similar efficacy. Of all of the available sources of osteoblastic cells for bone grafting, however, the only one that does not require an open surgical proce- dure or the added time, cost, and risk of grow- ing cells in vitro is bone marrow harvested by aspiration. Bone marrow aspiration from the pelvis has little risk or morbidity. The principal disadvantage is that the bone marrow-de- rived osteoblastic progenitors harvested by as- piration are diluted markedly by peripheral blood, often 20 to 40 fold lower than the con- centration present in autogenous cancellous bone. This dilution can be minimized by re- ducing the aspiration volume to 2 mL or less71 but cannot be eliminated.
Bone marrow-derived osteoblastic pro- genitors can be partly reconcentrated by selec- tion of low-density cells using diffusion gra- dientsZ0 or simple centrifugation to isolate a buffy coat.63 Experimental data indicate that methods of rapidly concentrating bone mar- row-derived cells may improve the efficacy of cell matrix composite^.^^
Alternatively, cancellous bone can be har- vested by taking percutaneous core biopsy specimens with little morbidity. This approach has the advantage of maintaining the native concentration of osteoblastic progenitors and providing a small volume of matrix and other undiluted bone marrow cells. There are sev- eral disadvantages to this method of harvest, however. The volume of bone tissue available in this way is limited to a few cubic centime- ters. There is greater risk of surgical compli- cations and blood loss. Finally, one must still design a means of extracting the available 0s- teoblastic progenitors from the bone obtained, then distributing them appropriately in the matrix to be implanted. The single cell suspen- sion obtained from bone marrow by aspiration simplifies this last problem.
If large numbers of osteoblastic progeni- tors are needed, the use of in vitro culture and expansion of osteoblastic progenitors har- vested from bone marrow is an available op- ti01-t.~' In vitro expansion of osteoblastic cells also opens up the opportunity to manipulate
the cells obtained, using exogenous growth factors or by infection or transfection using na- ked DNA% or using viral vectors6' to alter gene expression and presumably in vivo behavior after transplantation. These methods add sig- nificant expense to the preparation of a graft material, although such methods may be de- sirable or even critical for success in some set- tings.
Matrix, Matrix Structure, and Surface Chemistry
The concept of designing cell-matrix com- posites opens the opportunity to design or re- fine matrix materials to function specifically as delivery systems for transplanted osteoblastic progenitors. Potential matrix substrates in- clude processed allograft bone, matrices formed from purified collagen or hyaluronic acid, synthetic polymers, calcium phosphate ceramics, and bioglasses. These materials and associated surfaces are likely not yet optimal as osteoconductive or osteoinductive materi- als. Improvements or design of new materials require specific chemical surface modifica- tions, for example, addition of specific surface coatings to optimize biologic performance, such as adhesion m01ecules,2~ or addition of defined growth factors linked to the matrix surface.%
Cell Density, Diffusion, and Cell Survival
Optimal transplantation of cells into a graft bed requires knowledge and control of the relationship between the density of cells transplanted, the capacity of nutrients to dif- fuse through the matrix, and how these vari- ables affect the outcome at the graft site. Be- cause the initial survival of any transplanted cell depends on diffusion of nutrients and ox- ygen through the matrix, the porosity, pore size, and pattern of connectivity within the matrix become more important. This situation is particularly true as the volume of the graft increases, producing a longer diffusion path from the perimeter to cells at the center of a graft site.

BONE CELLS AND MATRICES IN ORTHOPEDIC TISSUE ENGINEERING 371
The density of cells transplanted into a graft site is closely related to the problem of diffusion. Any viable cells transplanted into a graft site create a metabolic demand and com- pete with surrounding cells in the site. This situation inevitably lowers local oxygen ten- sion, decreases pH, and reduces the availabil- ity of glucose and other nutrients. As a result, tissue engineering of larger-volume grafts likely requires not only transplantation of a sufficient number of selected cells but also may require means of limiting the transplantation of cells that are not critical to the end result. How many cells can or should be transplanted per unit volume and still contribute to an im- proved end result? This number depends on the graft setting, the matrix, and the metabolic demand of the cells being transplanted and needs to be examined experimentally in care- fully designed and controlled in vivo experi- ments.
CONCLUSION
The ultimate goal of the orthopedic tissue engineer is to augment the body's repair mechanisms to stimulate the repair or regen- eration of viable remodeling bone tissue. Improving knowledge of the biology of osteo- genic cells and ability to harvest and manip- ulate these cells presents clinicians with the opportunity to harness capacity of these cells for targeted regeneration and repair of skeletal tissues. The attachment, migration, prolifera- tion, and differentiation of these osteogenic cells can be influenced and modulated by se- lected bioactive molecules. The capacity to design specialized matrices that act as con- ductive scaffolds with defined structures, cus- tomized surface chemistries, and controlled degradation properties creates further oppor- tunities to optimize the delivery and trans- plantation of highly selected osteogenic regen- erative cells. Realization of the full potential of engineered matrix materials and cell-matrix composites can be expected to provide new and currently unavailable solutions to many clinical problems in skeletal reconstruction. These solutions should improve the quality of clinical outcomes and reduce the effective cost of care in many settings.
References
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
Albee FH: Transplantation of a portion of the tibia into the spine for Pott's disease. JAMA 5 7 885-886, 1911 Albee FH: Fundamentals in bone transplantation: Ex- periences in three thousand bone graft operations.
Ashton BA, Allen TD, Howlet CR, et al: Formation of bone and cartilage by marrow stromal cells in dif- fusion chambers in vivo. Clin Orthop 151:294,1980 Beresford J N Osteogenic stem cells and the stromal system of bone and marrow. Clin Orthop 240:270- 280,1989 Beresford JN, Bennett JH, Devlin C, et al: Evidence for an inverse relationship between differentiation of adipocytic and osteogenic cells in rat marrow stromal cell cultures. J Cell Sci 102:341-351,1992 Bos G, Goldberg V, Powell A, et al: The effect of his- tocompatibility matching on canine frozen bone al- lografts. J Bone Joint Surg Am 65339-96,1983 Bostman 0, Hirvensalo E, Markmen J, et al: Foreign body reactions to fracture fixation implants of bio- degradable synthetic polymers. J Bone Joint Surg Br
Brighton CT, Lorich DG, Kupcha R, et a1 The pericyte as a possible osteoblast progenitor cell. Clin Orthop
Bruder SP, Caplan AI: A monoclonal antibody against the surface of osteoblasts recognizes alkaline phosphatase isoenzymes in bone, liver, kidney, and intestine. Bone 11:133-139,1990 Bruder SP, Horowitz MP, Haynesworth SE: Monoclo- nal antibodies selective for human osteogenic cell surface antigens. Bone 21:225-235,1997 Bruder SP, Ricalton NS, Boynton RE, et al: Mesen- chymal stem cell surface antigen SB-10 corresponds to activated leucocyte cell adhesion molecule and is involved in osteogenic differentiation. J Bone Min Res 13655-673,1998 Bucholz RW Clinical experience with bone graft sub- stitutes. J Orthop Trauma 3:260-262,1987 Bulcholz RW, Carlton A, Holmes RE: Hydroxyapatite and tricalcium phosphate bone graft substitutes. Or- thop Clin North Am 18:323-334,1987 Burchardt H, Jones H, Glowczewskie F, et al: Freeze- dried allogeneic segmental cortical-bone grafts in dogs. J Bone Joint Surg Am 60:1082,1978 Burwell R Studies in the transplantation of bone: VII. The fresh composite homograft-autograft of cancel- lous bone: An analysis of factors leading to osteogen- esis in marrow transplants and in marrow-containing bone grafts. J Bone Joint Surg Br 46:110,1964 Caplan A1 Mesenchymal stem cells. J Orthop Res
Chapman MW, BuchoIz R, Cornell CN: Treatment of acute fractures with a collagen-calcium phosphate graft material: A randomized clinical trial. J Bone
Chase SW, Herndon CH: The fate of autogenous and homogenous bone grafts, a historical review. J Bone Joint Surg Am 37809-841,1955 Chiroff R, Weber J, White E: Tissue ingrowth of re- plamineform implants. J Biomed Mater Res 6:29,1975 Connolly J, Guse R, Lippiello L, et a1 Development of an osteogenic bone-marrow preparation. J Bone Joint Surg Am 71:684-691,1989 Connolly J, Guse R, Tiedeman J, et al: Autologous marrow injection as a substitute for operative graft-
JAMA 81~1429-1432,1923
2592-596,1990
275~287-299,1992
9641-650,1991
Joint SWg Am 79:495-502,1997

372 FLEMING et a1
ing of tibia1 nonunions. Clin Orthop 266:259-270, 1991
22. Damien CJ, Dasch J, Keefe J, et al: Formation of cal- cium-phosphate rich layer on absorbable calcium carbonate bone graft substitutes. Calif Tissue Int
23. Delustro F, Dasch J, Keefe J, et al: Immune responses to allogenic and xenogenic implants of collagen and collagen derivatives. Clin Orthop 260:264-297,1990
24. Dennis JE, Haynesworth SE, Young RG, et al: Osteo- genesis in marrow-derived mesenchymal cell porous ceramic composites transplanted subcutaneously: Ef- fect of fibronectin and laminin on cell retention and rate of osteogenic expression. Cell Transplant 1 :23- 32,1992
25. Ducy P, Zhang R, Geofioy V, et al: Osf2/Cbfal: A transcriptional activator of osteoblast differentiation. Cell 89:747-754,1997
26. Einhorn T: Current concepts review: Enhancement of fracture healing. J Bone Joint Surg Am 77:940-956, 1995
27. Fleming JE, Caplan Ak Monoclonal antibodies against cells of the mesenchymal lineage reveals key events in embryonic bone formation. Trans Orthop Res SOC 22:592,1997
28. Fleming JE, Haynesworth SE, Casseide P, et a1 A monoclonal antibody against adult marrow-derived mesenchymal stem cells recognizes developing vas- culature in embryonic human skin. Dev Dyn
29. Friedenstein AJ: Determined and inducible osteo- genic precursor cells. In Sognaes R, Vaughan J (eds): Hard Tissue Growth, Repair, and Remineralization. Ciba Foundation Symposium II. New York, Elsevier, 1973, p 169
30. Friedenstein AJ: Precursor cells of mechanocytes. Int Rev Cytol47:327,1976
31. Friedlander G, Mankin H Bone banking: Current methods and suggested guidelines. AAOS Instr Course Lect 3036-55,1981
32. Friedlander G: Bone grafts: The basic science ratio- nale for clinical applications. J Bone Joint Surg Am
33. Frost H: A new direction for osteoporosis research A review and proposal. Bone 12:429-437,1991
34. Garbuz DS, Masri BA, Czitrom AA: Biology of allo- grafting. Orthop Clin North Am 29:199-204,1998
35. Goldberg VM, Stevenson S, Shaffer JW: Biology of autografts and allografts. In Bone and Cartilage Al- lografts. American Academy of Orthopaedic Sur- geons Symposium, Park Ridge, IL, 1991, pp 3-13
36. Goldstein SA, Bonadio J: Potential role for direct gene transfer in the enhancement of fracture healing. Clin
37. Goujon E: Researches experimentales sur Ies proprie- tes physiologiques de la moelle des 0s . Journal de l'Anatomie et de Physiologie Normales et Patholo- giques de I'Homme et des Animaux 6399,1869
38. Gronthos S, Graves SE, Ohta S, et a1 The STl70-1+ fraction of adult human bone marrow contains the osteogenic precursors. Blood M4164-4173, 1994
39. Grundel RE, Chapman Mw: Type I fibrillar collagen and porous biphasic calcium phosphate ceramic for repair of segmental bone defects in the canine ulna. Read at Canadian Orthopaedic Research Society, To- ronto, Canada, May 28,1989
40. Haynesworth SE, Baber MA, Caplan A1 Cell surface antigens on human marrow-derived mesenchymal
55:151-158,1994
212:119-132,1998
69786-790,1987
Orthop 355(~~ppl):154-7 62,1998
cells are detected by monoclonal antibodies. Bone
41. Haynesworth SE, Goshima J, Goldberg VM, et a1 Characterization of cells with osteogenic potential from human marrow. Bone 13:81-88,1992
42. Heckman JD, Boyan BD, Aufdemorte TB, et al: The use of bone morphogenetic protein in the treatment of nonunion in a canine model. J Bone Joint Surg Am
43. Heiple K, Chase S, Herndon C: A comparative study of the healing process following different types of bone transplantation. J Bone Joint Surg Am 45:1592, 1963
44. Hollinger JO, Battistone GC: Biodegradable bone re- pair materials: Synthetic polymers and ceramics. Clin
45. Holmes R, Bucholz R, Mooney V Porous hydroxy- apatite as a bone graft substitute in metaphyseal de- fects. J Bone Joint Surg Am 68904-911,1986
46. Holmes R, Mooney V, Bucholz R, et al: A coralline hydroxyapatite bone graft substitute. Clin Orthop
47. Hu R, Bohlman H Fracture at the iliac bone graft harvest site after fusion of the spine. Clin Orthop
48. Johnson KD, Frierson KE, Keller TS, et al: Porous ce- ramics as bone graft substitutes in long bone defects: A biomechanical, histological, and radiographic analysis. J Orthop Res 14:351-369,1996
49. Jupiter JB, Winters S, Sigman S, et al: Repair of five distal radius fractures with an investigational bone cement: A preliminary report. J Orthop Trauma
50. Kadilaya S, Lo H, Leong KW, et a1 Biodegradable polymers and synthetic bone graft in bone formation and repair. American Academy Orthopaedic Sur- geons Symposium, Park Ridge, IL, 1994, pp 317-324
51. Komori T, Yagi H, Nomura S, et al: Targeted disrup- tion of Cbfal results in a complete lack of bone for- mation owing to maturational arrest of osteoblasts. Cell 89:755-764,1997
52. Kopylov P, Jonsson K, Thorngren KG, et a1 Injectable calcium phosphate in the treatment of distal radius fractures. J Hand Surg Br 21:768-771,1996
53. Kuhl PR, Griffith-Cima LG: Tethered epidermal growth factor as a paradigm for growth factor-in- duced stimulation from the solid phase. Nat Med
54. Kurashina K, Kurita H, Hirano M, et al: In vivo study of calcium phosphate cements: Implantation of an al- pha-tricalaum phosphate/dicalcium phosphate di- basic/tetracalcium phosphate monoxide cement paste. Biomaterials 18:539-543,1997
55. Lane JM, Cornell CN, Sandhu HR, et al: Clinical ap- plication biosynthetics. In: Bone and Cartilage Allo- grafts. American Academy of Orthopaedic Surgeons Symposium, Park Ridge, IL, 1991, pp 279-294
56. Lane JM, Sandhu HS: Current approaches to experi- mental bone grafting. Orthop Clin North Am 18:213- 225,1987
57. Laurencin CT, Lane J M Polylactic acid and polygly- colic acid Orthopaedic surgery applications. In Bone Formation and Repair. American Academy of Ortho- paedic Surgeons Symposium, Park Ridge, IL, 1994,
58. Lexer E: Die Verwendung der freien Knochenplastik nebst versuchen uber Gelenkversteifung und Ge- lenktransplantation. Arch Klin Chir 86939-954,1908
13:69-80,1992
73750-764,1991
Orthop 207:290-305,1986
188:252-262,1984
309:208-213, 1994
11:llO-116,1997
21022-1027,1996
pp 325-339

BONE CELLS AND MATRICES IN ORTHOPEDIC TISSUE ENGINEERING 373
59. Lian JB, Stein GS: Concepts of osteoblast growth and differentiation: Basis for modulation of bone cell de- velopment and tissue formation. Crit Rev Oral Biol Med 3:269-305,1992
60. Lian JB, Stein GS: Development of the osteoblastphe- notype: Molecular mechanisms mediating osteoblast growth and differentiation. Iowa Orthop J 15118- 140,1997
61. Lieberman JR, Le LQ, Wu L, et a1 Regional gene ther- apy with a BMP-2 producing murine stromal cell line induces heterotopic and orthotopic bone formation in rodents. J Orthop Res 16:330-339,1998
62. Macewen W: Observations concerning transplanta- tion of bone illustrated by a case of interhuman os- seous transplantation: Whereby over two-thirds of the shaft of the humerus was restored. Proc R Soc Lond 32:232-247,1991
63. Majors A, Boehm CA, Nitto H, et a1 Characterization of human bone marrow stromal cells with respect to osteoblastic differentiation. J Orthop Res 15:546-557, 1997
64. Mandrup S, Lane MD: Regulating adipogenesis. J Biol Chem 2725367-5370,1997
65. Maniatopoulos C, Sodek J, Melcher AH: Bone for- mation in vitro by stromal cells obtained from bone marrow of young adult rats. Cell Tissue Res 2!54:317- 330,1988
66. Mankin HJ, Gebhardt MC, Tomford WW: The use of frozen cadaveric allografts in the management of pa- tients with bone tumors of the extremities. Orthop Clin North Am 18:275,1987
67. Meek’ren JJV: Observations Medico-Chirurgicae. Amsterdam, H&T Boon, 1632
68. Miyamoto Y, Ishikawa K, Fukao H, et al: In vivo set- ting behavior of fast setting calcium phosphate ce- ment. Biomaterials 162350-860, 1995
69. Moore DC, Chapman M W , Manske D: The evalua- tion of a biphasic calcium phosphate ceramic for use in grafting long bone diaphyseal defects. J Orthop Res 5:356-365,1987
70. Mundlos S, Otto F, Mundlos C, et al: Mutations in- volving the transcription factor Cbfal cause cleido- cranial dysplasia. Cell 89773-779,1997
71. Muschler G, Boehm C, Easley K The harvest of os- teoblastic progenitors from human bone marrow by aspiration: The influence of aspiration volume. J Bone Joint Surg Am 79:1699-1709,1997
72. Muschler G, Lane J, Dawson E: The biology of spinal fusion. In Cotler J, Cotler H (eds): Spinal Fusion, Sci- ence and Technique. New York, Springer Verlag, 1990
73. Muschler GF, Hyodo A, Manning T, et al: Evaluation of human bone morphogenetic protein-2 in a canine spinal fusion model. Clin Orthop 308:229-240,1994
74. Muschler GF, Lane JM: Spinal fusion: Principles of bone fusion. In Rothman, Simeone (eds): The Spine, ed 4. Philadelphia, WB Saunders, 1999
75. Muschler GF, Matsakura Y, Boehm C, et al: Rapid intra-operative concentration of bone marrow de- rived osteoblastic progenitors for use in bone grafts for spinal fusion. 1999 (submitted)
76. Muschler GF, Negami S, Hyodo A, et al: Evaluation of collagen ceramic composite graft materials in a spinal fusion model. Clin Orthop 328:250-260,1996
77. Muschler GF, Nitto H, Boehm CA, et al: Age and gen- der related changes in the cellularity of human bone marrow and the prevalence of osteoblastic progeni- tors. 1999 (submitted)
78. Nade S Osteogenesis after bone and bone marrow transplantation: 11. The initial cellular events follow- ing transplantation of decalcified allografts of can- cellous bone. Acta Orthop Scand 48:572,1977
79. Nade S: Clinical implications of cell function in os- teogenesis: A re-appraisal of bone graft surgery. Ann R Coll Surg Engl61:189,1979
80. Nagashima T, Oshima X, Takeuchi H Osteoconduc- tion in porous hydroxyapatite ceramics grafted into the defect of Lanuna in experimental lanunaplasty. J Jpn Orthop Assoc 69:222-230,1995
81. Nehls V, Drenckhahn D The versatility of microvas- cular pericytes: From mesenchyme to smooth mus- cle. Histochemistry 99:l-12, 1993
82. Ostrum R, Chao Y, Basset CA, et a1 Bone Injury, Re- generation, and Repair. In Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 285-287
83. Otto F, Thornell AP, Crompton T, et a1 Cbfal, a can- didate gene for cleidocranial dysplasia syndrome, is essential for osteoblast differentiation and bone de- velopment. Cell 89765-771,1997
84. Owen M The origin of bone cells in the post natal organism. Arthritis Rheum 23:1074,1980
85. Owen M: Lineage of osteogenic cells and their rela- tionship to the stromal system. Bone Min Res 3:l-25, 1985
86. Owen TA, Aronow M, Shalhoub V, et al: Progressive development of the rat osteoblast phenotype in vitro: Reciprocal relationships in expression of genes as- sociated with osteoblast proliferation and differenti- ation during formation of the bone extracellular ma- trix. J Cell Physiol143:420-430,1990
87. Pelker R, Friedlander G, Markham T: Biomechanical properties of bone allografts. Clin Orthop 17454-57, 1983
88. Perry CR Bone repair techniques, bone graft, and bone graft substitutes. Clin Orthop 360:71-86,1999
89. Pfeiffer, CA Development of bone from transplanted marrow in mice. Anat Rec 102:225,1948
90. Phemister DB: The fate of transplanted bone and re- generative power of its various constituents. Surg Gynecol Obstet 19303-333,1914
91. Piersma AH, Ploemacher RE, Brockbank KG: Br J Haematol54:285, 1983
92. Plenk H Jr, Hollmann K, Wilfert K Experimental bridging of osseous defects in rats by the implanta- tion of Kiel bone containing fresh autologous mar- row. J Bone Joint Surg Br 54:735-743,1972
93. Prockop DJ: Marrow stromal cells as stem cells for nonhematopoietic tissues. Science 276:71-74,1997
94. Radomsky ML, Thompson AY, Spiro RC, et al: Poten- tial role of fibroblast growth factor in enhancement of fracture healing. Clin Orthop 355(suppl):283-293, 1998
95. Ripamonti U: Morphogenesis of bone in replicas of porous hydroxyapatite obtained from concersion of carbonate exoskeletons of coral. J Bone Joint Surg Am
96. Rodan GA, Harada S The missing bone. Cell 89:677- 680,1997
97. Salyer KE, Hall C D Porous hydroxyapatite as an on- lay bone graft substitute for maxillofacial surgery. Plast Reconstr Surg 84:236-244,1989
98. Sandhu H, Boden S: Biologic enhancement of spinal fusion. Orthop Clin North Am 29:621-631,1998
73~692-703,1991

374 FLEMING et a1
99. Schor AM, Allen TD, Canfield AE, et al: Pericytes derived from retinal microvasculature undergo cal- cification in vitro. J Cell Sci 97449-461,1990
100. Simmons PJ, Torok-Storb B Identification of stromal cell precursors in human bone marrow by a novel monoclonal antibody, STRO-I. Blood 78:55-62,1991
101. Steinman J, Herkowitz H Pseudoarthrosis of the spine. Clin Orthop 28480,1992
102. Stevenson S The immune response to osteochondral allografts in dogs. J Bone Joint Surg Am 69:573,1987
103. Tomford W, Starkweather R, Goldman M: A study of the incidence of infection in the use of banked allo- graft bone. J Bone Joint Surg Am 63:244-248,1981
104. Turksen K, Aubin J E Monoclonal antibodies as tools for studying the osteoblast lineage. Microsc Res Tech 33:128-140,1996
105. Turksen K, Bhargava U, Moe HK, et al: Isolation of monoclonal antibodies recognizing rat bone-associ- ated molecules in vitro and in vivo. J Histochem Cy- tochem 40:1339-1352,1992
106. Werntz JR, Lane JM, Piez C: The repair of segmental bone defects with collagen and marrow. Orthop Trans 10262,1986
107. Wilson P: Follow up study of the use of refrigerated homologous bone transplants in orthopaedic opera- tions. J Bone Joint Surg Am 33:307,1951
108. Younger E, Chapman M: Morbidity at bone graft do- nor sites. J Orthop Trauma 3:192-195,1989
109. Zerwekh JE, Kourosh S, Schienbergt R, et al: Fibrillar collagen-biphasic calcium phosphate composite as a bone graft substitute for spinal fusion. J Orthop Res 10562-572,1992
Address reprint requests to George F. Muschler, MD
Department of Orthopaedic Surgery The Cleveland Clinic Foundation
9500 Euclid Avenue Cleveland, OH 44195

本文献由“学霸图书馆-文献云下载”收集自网络,仅供学习交流使用。
学霸图书馆(www.xuebalib.com)是一个“整合众多图书馆数据库资源,
提供一站式文献检索和下载服务”的24 小时在线不限IP
图书馆。
图书馆致力于便利、促进学习与科研,提供最强文献下载服务。
图书馆导航:
图书馆首页 文献云下载 图书馆入口 外文数据库大全 疑难文献辅助工具