Embed Size (px)
Citation preview

Archives of Gerontology and Geriatrics 52 (2011) 23–27
Body position and cardio-respiratory variables in older people
Susan Gordon *, Anne Jones, Rebecca Sealey, Petra Buettner
School of Public Health, Tropical Medicine and Rehabilitation Sciences, James Cook University, Townsville 4810, Australia
A R T I C L E I N F O
Article history:
Received 7 April 2009
Received in revised form 1 November 2009
Accepted 4 November 2009
Available online 30 November 2009
Keywords:
Position of older people
Age and cardio-respiratory system
Cardio-vascular aging
A B S T R A C T
What effect does body position have on cardio-respiratory variables in active older people? An
experimental laboratory study was undertaken measuring heart rate, systolic and diastolic blood
pressure and oxygen saturation when 26 active people aged 60 years and over adopted five standardized
body positions. Measurements were taken every 2 min over a 10-min period in sitting, right side lying,
left side lying, supine and supine with the head 208 below the level of the body. Rate pressure product
and mean arterial pressure were calculated. Smoking history, medication use, health conditions and
activity level were recorded. Height, weight and body fat were measured. Left and right side lying
produced significantly lower diastolic and systolic blood pressure, rate pressure product and mean
arterial pressure than supine with the head down. Excluding oxygen saturation mean values for all
variables remained within recommended normal limits in all positions. Significant differences in cardio-
respiratory variables occur when active older people change body position. Positioning as a treatment
intervention appears safe in supine, side lying and sitting for this population. Head down supine position
should be adopted with caution.
� 2009 Elsevier Ireland Ltd. All rights reserved.
Contents lists available at ScienceDirect
Archives of Gerontology and Geriatrics
journa l homepage: www.e lsev ier .com/ locate /archger
1. Introduction
Body position alters the effect of gravity on body function hencepositional advice is often implemented in the management of cardio-vascular, respiratory, digestive and musculoskeletal conditions(Martin-Du Pan et al., 2004). Positions commonly adopted formedical, nursing and physiotherapy management, rest and sleepinclude sitting, lying supine or lying in the lateral position. Further,lying supine with the head positioned inferior to the body is used byphysiotherapists to treat respiratory conditions. There is littleevidence to determine the potentially detrimental effects ofpositioning alone as a treatment (Stiller, 2000). This is importantin older people who may have age-related compromise of cardio-respiratory function.
Reported findings related to body position and cardio-respiratory factors have varied for healthy, young adults (Ryanet al., 2003; Jones and Dean, 2004; Watanabe et al., 2007) and onestudy has investigated these factors in a middle aged group (Tabaraet al., 2005). Numerous studies have reported the effect of bodyposition on cardio-respiratory function in specific patient groups(Zack et al., 1974; Cartwright, 1984; Oksenberg et al., 1997;Rosenberg-Adamsen et al., 1997; Kuo and Chen, 1998; Khouryet al., 1999; Fujita et al., 2000; Leung et al., 2003). However there isscant information regarding the effect of body position on cardio-respiratory variables in older people. Due to age-related cardio-respiratory changes it is unlikely that findings in young and middle
* Corresponding author. Tel.: +61 7 4781 6734; fax: +61 7 4781 6868.
E-mail address: [email protected] (S. Gordon).
0167-4943/$ – see front matter � 2009 Elsevier Ireland Ltd. All rights reserved.
doi:10.1016/j.archger.2009.11.005
aged adults are generalizable to an older population. Factors whichmay alter cardio-respiratory response to different body positionsinclude obesity, history of smoking, medication use, presence ofmedical conditions and general fitness level.
Older, healthy people have decreased forced vital capacity andforced expiratory volume after 1 s in side lying when compared tositting (Manning et al., 1999). Further healthy, seated oldersubjects (>65 years) have significant impairment of ventilationdistribution to dependent lung zones (Leblanc et al., 1970).
Older people exhibit significant increased preference for the rightside sleep position (De Koninck et al., 1992). This has beenpostulated to be due to age-related alterations in cardio-vascularfunction (Leblanc et al., 1970) or compression from other structurescausing reduction in ventricular distensibility (Lange et al., 1988).
This study investigates the effect of five standardized bodypositions on cardio-respiratory variables in a group of healthy,older people. Comparisons are made to previously reportedfindings for young and middle aged healthy people.
2. Materials and methods
The method of this observational study largely replicates Jonesand Dean (2004). It is described here for the convenience of thereader and to identify alterations for this study.
2.1. Study participants
Participants were recruited from four Probus clubs (a commu-nity organisation for people aged over 60 years) in Townsville,

S. Gordon et al. / Archives of Gerontology and Geriatrics 52 (2011) 23–2724
Australia. Human research ethics approval was provided by JamesCook University and signed informed consent was gained prior toparticipation.
Participants were eligible to participate if they were over 60years of age. A screening questionnaire (see Appendix 1 insupplementary data in the journal website) was completed byparticipants to identify the presence of any physical or medicalcondition which would prevent participants from comfortablyadopting each position included in the study for 20 min.Information regarding smoking history, usual exercise level,medication use, medical history and recent illness was alsocollected.
2.2. Anthropometric measures
Height was measured using a portable stadiometer and masswas measured using digital scales (BF-681, Tanita UK, Middlesex)as per the protocols described by Norton and Olds (1996). Ameasure of body fat using bioelectrical impedance analysis wasprovided by the digital scales. For these measures participantswere required to remove their shoes and socks but not theirclothes.
2.3. Standardized body positions
Physiological measures were taken in five standardized bodypositions; sitting (S), the participant sat in a standard office chairwith the ankles and hips at right angles and feet on the floor. Thearms were relaxed, and the hands were rested in the lap.Horizontal supine flat position (HS), the participant lay horizon-tally on an examination table with their head supported by apillow. Head down (208) supine flat position (HDS), the participantwas positioned in the horizontal supine position with a pillowsupporting their head. The examination table was angled down-wards at 208 so that from the waist to the head participants wereangled downwards. Right- and left side lying (908) positions (RSLand LSL, respectively) the participant lay with the trunk at 908 tothe examination table. To avoid the participant shifting position,pillows were positioned to support the head to maintain vertebralalignment, and under the upper leg, which was positioned with hipflexion standardized at 458.
In all recumbent positions, the arms rested comfortably in frontof the participant. The order of position was randomized by ballotfor each participant.
2.4. Physiological measures
Heart rate (HR) and arterial saturation of hemoglobin (SpO2)were measured using a pulse oximeter (Nonin Onyx) attached tothe index finger. Blood pressure (BP) was measured with a manualsystem aneroid sphygmomanometer and spirit majestic stetho-scope. The BP cuff was applied to the mid-humerus of the right armat the level of the heart and when in the right side lying position tothe mid-humerus of the left arm.
2.5. Procedure
Before testing, participants did not to undertake any unusualactivity for 24 h and on the day of testing refrained fromcaffeinated beverages, unusual exercise, heavy meals, and unduestress prior to the data collection session (Jones and Dean, 2004).All measurements were undertaken in the Physiotherapy Clinic atJames Cook University. The temperature (23 8C) and humidity ofthe clinic was constant across testing sessions.
On arrival at the clinic participants’ anthropometric measureswere taken. Participants then sat quietly for 30 min before being
placed in their first test position. After the participants had beenresting in this position for 10 min, all physiological measures weretaken every 2 min over a further 10-min period. Participantstherefore rested in each position for 20 min. Additionally whenparticipants were in HDS data was recorded every 2 min for thefirst 10 min as well as the second 10 min. After data collection inthe first position, based on the random order, the participant wasslowly positioned in the subsequent randomized position.Participants were asked to avoid excessive movement whenchanging from one position to another and to avoid talking whileresting in each position. The total time for data collection wasapproximately 2 h and 15 min, including 30 min of baseline restand 10 min rest and 10 min measurement time in each of the fivebody positions.
2.6. Data management
For purposes of analysis, rate pressure product (RPP) wasdefined as the product of HR and systolic blood pressure (SBP)(Gobel et al., 1978). Mean arterial pressure (MAP) was calculatedusing the equation MAP = DBP + 1/3(SBP � DBP) (Gobel et al.,1978).
Participant’s level of physical activity was classified as (Black,2000). Sedentary: seated work with discretion and requirements tomove around but little or no strenuous leisure activity slightlyactive: standing work e.g., housewife moderately active: signifi-cant amounts of sport or strenuous activity 30–60 min, 4–5 times aweek, and very active: strenuous work or highly active therefore>30–60 min, five times/week.
Smoking history was classified into: never smoked, ceasedmore than 20 years ago or ceased less than or equal to 20 years ago.The cut off point of 20 years was chosen due to studies reportingthe reduced risk of coronary heart disease and lung cancergradually returns towards normal over a 20-year period (Ockeneet al., 1990).
Participants were asked to disclose their current medications.For statistical analysis the medications were grouped according tomedication types: anti-hypertensive, anti-cholesterol, anticoagu-lant, diabetic medication, medication to treat/prevent osteoporo-sis, gastrointestinal/anti-reflux, medication to treat/prevent gout,hormone replacement medication, non-steroidal anti-inflamma-tory medications, respiratory medications.
2.7. Data analysis
Numerical data was approximately normally distributed andwas therefore described using mean � SD. To test the influence offive positions (RSL, LSL, S, HS, HDS) on resting HR, SBP, diastolic bloodpressure (DBP), SpO2, RPP and MAP repeated measures analyses ofvariance (ANOVA) were conducted. If the overall ANOVA result wassignificant, paired t-tests adjusted for multiple testing usingBonferroni were used to identify positions with statistically differentresults. Repeated measurement ANOVA with covariates (such as age,body mass index) or between-subject factors (such as gender) wereutilised to identify significant main effects and interactions. Theanalysis was conducted using SPSS for Windows, version 14 (SPSS,Chicago, IL, USA).
3. Results
Of the 26 participants age ranged between 62 and 86 years(mean: 73.3 � 5.4), 46.2% were female. Mean body mass indexwas 29.3 � 6.3 kg m2 (range 19.1–49.6), with 34.6% of participantsdescribing themselves as moderately active and 65.4% reportedthey had never smoked and no participant was currently smoking.Overall 42.3% were using anti-hypertensive, 34.6% anti-cholesterol,
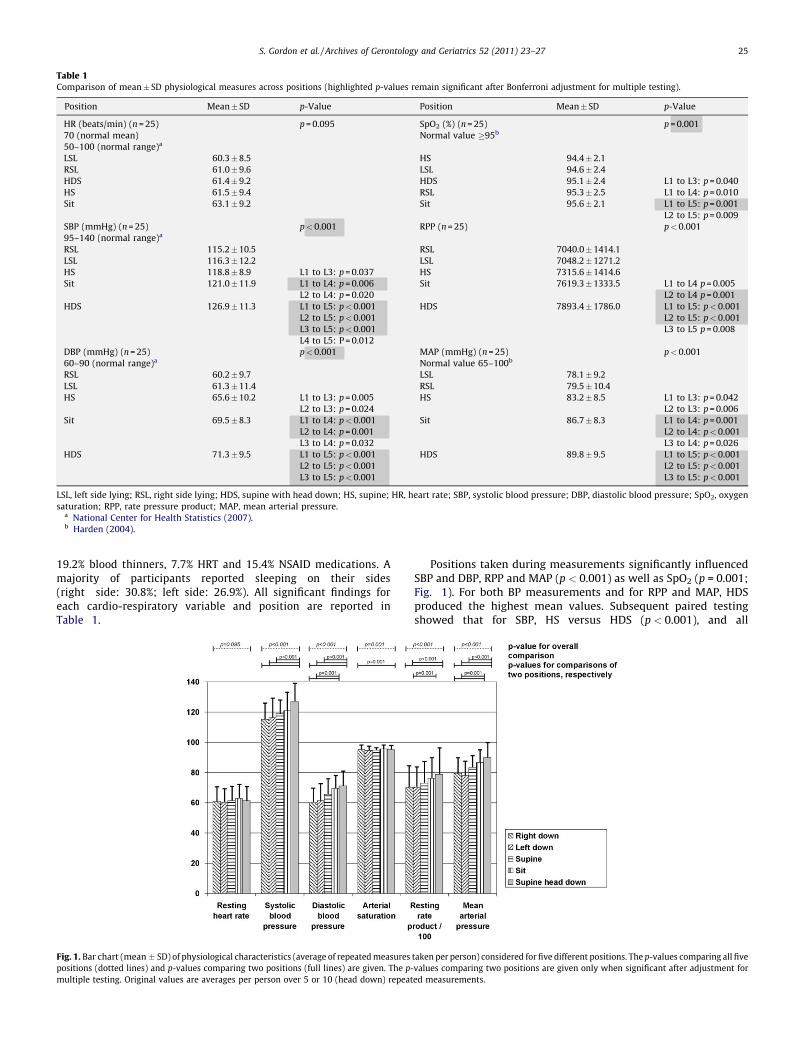
Table 1Comparison of mean� SD physiological measures across positions (highlighted p-values remain significant after Bonferroni adjustment for multiple testing).
Position Mean� SD p-Value Position Mean� SD p-Value
HR (beats/min) (n = 25) p = 0.095 SpO2 (%) (n = 25) p = 0.001
70 (normal mean) Normal value �95b
50–100 (normal range)a
LSL 60.3�8.5 HS 94.4�2.1
RSL 61.0�9.6 LSL 94.6�2.4
HDS 61.4�9.2 HDS 95.1�2.4 L1 to L3: p = 0.040
HS 61.5�9.4 RSL 95.3�2.5 L1 to L4: p = 0.010
Sit 63.1�9.2 Sit 95.6�2.1 L1 to L5: p = 0.001
L2 to L5: p = 0.009
SBP (mmHg) (n = 25) p<0.001 RPP (n = 25) p<0.001
95–140 (normal range)a
RSL 115.2�10.5 RSL 7040.0�1414.1
LSL 116.3�12.2 LSL 7048.2�1271.2
HS 118.8�8.9 L1 to L3: p = 0.037 HS 7315.6�1414.6
Sit 121.0�11.9 L1 to L4: p = 0.006 Sit 7619.3�1333.5 L1 to L4 p = 0.005
L2 to L4: p = 0.020 L2 to L4 p = 0.001
HDS 126.9�11.3 L1 to L5: p<0.001 HDS 7893.4�1786.0 L1 to L5: p<0.001
L2 to L5: p<0.001 L2 to L5: p<0.001
L3 to L5: p<0.001 L3 to L5 p = 0.008
L4 to L5: P = 0.012
DBP (mmHg) (n = 25) p<0.001 MAP (mmHg) (n = 25) p<0.001
60–90 (normal range)a Normal value 65–100b
RSL 60.2�9.7 LSL 78.1�9.2
LSL 61.3�11.4 RSL 79.5�10.4
HS 65.6�10.2 L1 to L3: p = 0.005 HS 83.2�8.5 L1 to L3: p = 0.042
L2 to L3: p = 0.024 L2 to L3: p = 0.006
Sit 69.5�8.3 L1 to L4: p<0.001 Sit 86.7�8.3 L1 to L4: p = 0.001
L2 to L4: p = 0.001 L2 to L4: p<0.001
L3 to L4: p = 0.032 L3 to L4: p = 0.026
HDS 71.3�9.5 L1 to L5: p<0.001 HDS 89.8�9.5 L1 to L5: p<0.001
L2 to L5: p<0.001 L2 to L5: p<0.001
L3 to L5: p<0.001 L3 to L5: p<0.001
LSL, left side lying; RSL, right side lying; HDS, supine with head down; HS, supine; HR, heart rate; SBP, systolic blood pressure; DBP, diastolic blood pressure; SpO2, oxygen
saturation; RPP, rate pressure product; MAP, mean arterial pressure.a National Center for Health Statistics (2007).b Harden (2004).
S. Gordon et al. / Archives of Gerontology and Geriatrics 52 (2011) 23–27 25
19.2% blood thinners, 7.7% HRT and 15.4% NSAID medications. Amajority of participants reported sleeping on their sides(right side: 30.8%; left side: 26.9%). All significant findings foreach cardio-respiratory variable and position are reported inTable 1.
Fig. 1. Bar chart (mean � SD) of physiological characteristics (average of repeated measures
positions (dotted lines) and p-values comparing two positions (full lines) are given. The p-
multiple testing. Original values are averages per person over 5 or 10 (head down) repeat
Positions taken during measurements significantly influencedSBP and DBP, RPP and MAP (p < 0.001) as well as SpO2 (p = 0.001;Fig. 1). For both BP measurements and for RPP and MAP, HDSproduced the highest mean values. Subsequent paired testingshowed that for SBP, HS versus HDS (p < 0.001), and all
taken per person) considered for five different positions. The p-values comparing all five
values comparing two positions are given only when significant after adjustment for
ed measurements.
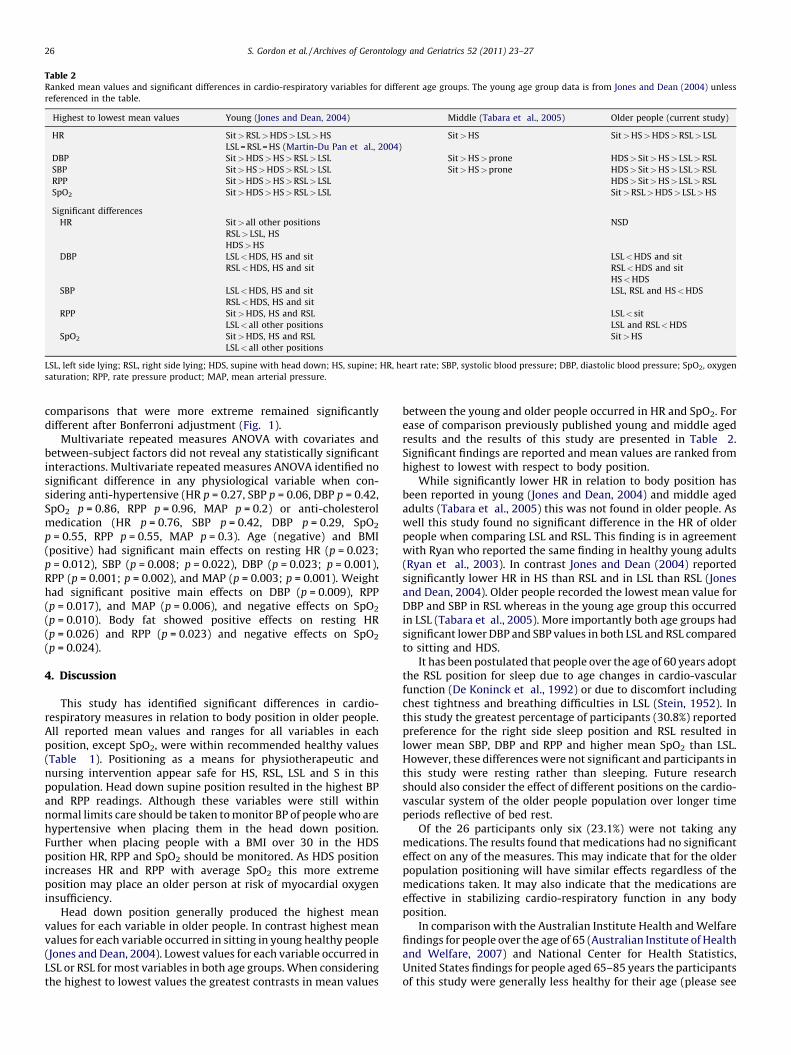
Table 2Ranked mean values and significant differences in cardio-respiratory variables for different age groups. The young age group data is from Jones and Dean (2004) unless
referenced in the table.
Highest to lowest mean values Young (Jones and Dean, 2004) Middle (Tabara et al., 2005) Older people (current study)
HR Sit>RSL>HDS> LSL>HS Sit>HS Sit>HS>HDS>RSL> LSL
LSL = RSL = HS (Martin-Du Pan et al., 2004)
DBP Sit>HDS>HS>RSL> LSL Sit>HS>prone HDS> Sit>HS> LSL>RSL
SBP Sit>HS>HDS>RSL> LSL Sit>HS>prone HDS> Sit>HS> LSL>RSL
RPP Sit>HDS>HS>RSL> LSL HDS> Sit>HS> LSL>RSL
SpO2 Sit>HDS>HS>RSL> LSL Sit>RSL>HDS> LSL>HS
Significant differences
HR Sit>all other positions NSD
RSL> LSL, HS
HDS>HS
DBP LSL<HDS, HS and sit LSL<HDS and sit
RSL<HDS, HS and sit RSL<HDS and sit
HS<HDS
SBP LSL<HDS, HS and sit LSL, RSL and HS<HDS
RSL<HDS, HS and sit
RPP Sit>HDS, HS and RSL LSL< sit
LSL<all other positions LSL and RSL<HDS
SpO2 Sit>HDS, HS and RSL Sit>HS
LSL<all other positions
LSL, left side lying; RSL, right side lying; HDS, supine with head down; HS, supine; HR, heart rate; SBP, systolic blood pressure; DBP, diastolic blood pressure; SpO2, oxygen
saturation; RPP, rate pressure product; MAP, mean arterial pressure.
S. Gordon et al. / Archives of Gerontology and Geriatrics 52 (2011) 23–2726
comparisons that were more extreme remained significantlydifferent after Bonferroni adjustment (Fig. 1).
Multivariate repeated measures ANOVA with covariates andbetween-subject factors did not reveal any statistically significantinteractions. Multivariate repeated measures ANOVA identified nosignificant difference in any physiological variable when con-sidering anti-hypertensive (HR p = 0.27, SBP p = 0.06, DBP p = 0.42,SpO2 p = 0.86, RPP p = 0.96, MAP p = 0.2) or anti-cholesterolmedication (HR p = 0.76, SBP p = 0.42, DBP p = 0.29, SpO2
p = 0.55, RPP p = 0.55, MAP p = 0.3). Age (negative) and BMI(positive) had significant main effects on resting HR (p = 0.023;p = 0.012), SBP (p = 0.008; p = 0.022), DBP (p = 0.023; p = 0.001),RPP (p = 0.001; p = 0.002), and MAP (p = 0.003; p = 0.001). Weighthad significant positive main effects on DBP (p = 0.009), RPP(p = 0.017), and MAP (p = 0.006), and negative effects on SpO2
(p = 0.010). Body fat showed positive effects on resting HR(p = 0.026) and RPP (p = 0.023) and negative effects on SpO2
(p = 0.024).
4. Discussion
This study has identified significant differences in cardio-respiratory measures in relation to body position in older people.All reported mean values and ranges for all variables in eachposition, except SpO2, were within recommended healthy values(Table 1). Positioning as a means for physiotherapeutic andnursing intervention appear safe for HS, RSL, LSL and S in thispopulation. Head down supine position resulted in the highest BPand RPP readings. Although these variables were still withinnormal limits care should be taken to monitor BP of people who arehypertensive when placing them in the head down position.Further when placing people with a BMI over 30 in the HDSposition HR, RPP and SpO2 should be monitored. As HDS positionincreases HR and RPP with average SpO2 this more extremeposition may place an older person at risk of myocardial oxygeninsufficiency.
Head down position generally produced the highest meanvalues for each variable in older people. In contrast highest meanvalues for each variable occurred in sitting in young healthy people(Jones and Dean, 2004). Lowest values for each variable occurred inLSL or RSL for most variables in both age groups. When consideringthe highest to lowest values the greatest contrasts in mean values
between the young and older people occurred in HR and SpO2. Forease of comparison previously published young and middle agedresults and the results of this study are presented in Table 2.Significant findings are reported and mean values are ranked fromhighest to lowest with respect to body position.
While significantly lower HR in relation to body position hasbeen reported in young (Jones and Dean, 2004) and middle agedadults (Tabara et al., 2005) this was not found in older people. Aswell this study found no significant difference in the HR of olderpeople when comparing LSL and RSL. This finding is in agreementwith Ryan who reported the same finding in healthy young adults(Ryan et al., 2003). In contrast Jones and Dean (2004) reportedsignificantly lower HR in HS than RSL and in LSL than RSL (Jonesand Dean, 2004). Older people recorded the lowest mean value forDBP and SBP in RSL whereas in the young age group this occurredin LSL (Tabara et al., 2005). More importantly both age groups hadsignificant lower DBP and SBP values in both LSL and RSL comparedto sitting and HDS.
It has been postulated that people over the age of 60 years adoptthe RSL position for sleep due to age changes in cardio-vascularfunction (De Koninck et al., 1992) or due to discomfort includingchest tightness and breathing difficulties in LSL (Stein, 1952). Inthis study the greatest percentage of participants (30.8%) reportedpreference for the right side sleep position and RSL resulted inlower mean SBP, DBP and RPP and higher mean SpO2 than LSL.However, these differences were not significant and participants inthis study were resting rather than sleeping. Future researchshould also consider the effect of different positions on the cardio-vascular system of the older people population over longer timeperiods reflective of bed rest.
Of the 26 participants only six (23.1%) were not taking anymedications. The results found that medications had no significanteffect on any of the measures. This may indicate that for the olderpopulation positioning will have similar effects regardless of themedications taken. It may also indicate that the medications areeffective in stabilizing cardio-respiratory function in any bodyposition.
In comparison with the Australian Institute Health and Welfarefindings for people over the age of 65 (Australian Institute of Healthand Welfare, 2007) and National Center for Health Statistics,United States findings for people aged 65–85 years the participantsof this study were generally less healthy for their age (please see

S. Gordon et al. / Archives of Gerontology and Geriatrics 52 (2011) 23–27 27
Appendix 2 in supplementary data on the journal website)(National Center for Health Statistics, 2007). In spite of this nonegative effects occurred as a result of this study and during testingparticipants cardio-respiratory variables remained within thenormal range. Although these comparisons indicate the possibilitythat the findings of this study are generalizable across the olderpopulation further research in this area is required.
Conflict of interest statement
None.
Acknowledgement
The authors acknowledge the kind support of James CookUniversity.
Appendix A. Supplementary data
Supplementary data associated with this article can be found, in
the online version, at doi:10.1016/j.archger.2009.11.005.
References
Australian Institute of Health and Welfare, 2007. Older Australia at a Glance, 4th ed.,Australian Government ISBN-139781740247320.
Black, A., 2000. Critical evaluation of energy intake using the Goldberg cut-off forenergy intake, basal metabolic rate. A practical guide to its calculation. Int. J.Obesity 24, 1119–1130.
Cartwright, R.D., 1984. Effect of sleep position on sleep apnea severity. Sleep 7, 110–114.
De Koninck, J., Lorrain, D., Gagnon, P., 1992. Sleep positions and position shifts infive age groups. An ontogenetic picture. Sleep 15, 143–149.
Fujita, M., Miyamoto, S., Sekiguchi, H., Eiho, S., Sasayama, S., 2000. Effects of postureon sympathetic nervous modulation in patients with chronic heart failure.Lancet 356, 1822–1823.
Gobel, F., Nordstrom, P., Nelson, R., Jorgensen, C., Wang, Y., 1978. The rate-pressureproduct as an index of myocardial oxygen consumption during exercise inpatients with angina pectoris. Circulation 57, 549–556.
Harden, B. (Ed.), 2004. Emergency Physiotherapy, an On-call Survival Guide.Churchill Livingstone, Edinburgh.
Jones, A.Y.M., Dean, E., 2004. Body position change and its effect on hemodynamicand metabolic status. Heart Lung 33, 281–290.
Khoury, R.M., Camach-Lobato, L., Katz, P.O., Mohiuddin, M.A., Castell, D.O., 1999.Influence of spontaneous sleep positions on nighttime recumbent reflux inpatients with gastroesophageal reflux disease. Am. J. Gastroenterol. 94, 2069–2073.
Kuo, C.D., Chen, G.Y., 1998. Comparison of three recumbent positions on vagal andsympathetic modulation using spectral heart rate variability in patients withcoronary artery disease. Am. J. Cardiol. 81, 392–396.
Lange, R.A., Katz, J., McBride, W., Moore, D.M., Hillis, L.D., 1988. Effects of supine andlateral positions on cardiac output and intracardiac pressures. J. Am. Coll.Cardiol. 62, 330–333.
Leblanc, P., Ruff, F., Milic-Emili, J., 1970. Effects of age and body position on ‘‘airwayclosure’’ in man. J. Appl. Physiol. 28, 448–451.
Leung, R.S.T., Bowman, M.E., Parker, J.D., Newton, G.E., Bradley, T.D., 2003. Avoid-ance of left lateral decubitus position during sleep in patients with heart failure,relationship to cardiac size and function. J. Am. Coll. Cardiol. 41, 227–230.
Manning, F., Dean, E., Ross, J., Abboud, R.T., 1999. Effects of side lying on lungfunction in older individuals. Phys. Ther. 76, 456–466.
Martin-Du Pan, R.C., Benoit, R., Girardier, L., 2004. The role of body position andgravity in the symptoms and treatment of various medical diseases. Swiss Med.Wkly 134, 543–551.
National Center for Health Statistics, 2007. United States. U.S. Government PrintingOffice, Washington.
Norton, K., Olds, T., 1996. Anthropometrica. University of New South Wales Press,Sydney.
Nonin Onyx 9500 Medical Nonin Medical, Inc.13700 1st Avenue North, Plymouth,Minnesota 55441-5443, USA.
Ockene, J., Kuller, L., Svendsen, K., Meilahn, E., 1990. The relationship of smokingcessation to coronary heart disease and lung cancer in the multiple risk factorintervention trial (MRFIT). Am. J. Public Health 80, 954–958.
Oksenberg, A., Silverberg, D.S., Arons, A., Radwan, H., 1997. Positional vs. nonposi-tional obstructive sleep apnoea patients. Chest 112, 629–785.
Rosenberg-Adamsen, S., Stausholm, K., Edvardsen, L., Zwarts, M., Kehlet, H., Rosen-berg, J., 1997. Body position and late post-operative nocturnal hypoxaemia.Anaesthesia 52, 586–602.
Ryan, A.D., Larsen, P.D., Galletly, D.C., 2003. Comparison of heart rate variability insupine, and left and right lateral positions. Anaesthesia 58, 432–436.
Stein, P., 1952. Tendency toward hypotension in the left lateral recumbency. Arch.Intern. Med. 9, 234–242.
Stiller, K., 2000. Physiotherapy in intensive care. Chest 118, 1801–1813.Tabara, Y., Tachibana-Iimori, R., Yamamoto, M., Abe, M., Kondo, F., Miki, T., 2005.
Hypotension associated with prone body position, a possible overlooked pos-tural hypotension. Hypertens. Res. 28, 741–746.
Watanabe, N., Reece, J., Polus, B., 2007. Effects of body position on autonomicregulation of cardiovascular function in young, healthy adults. Chiropr. Osteo-path. 5, 19.
Zack, M.B., Pontoppidan, H.K., Lazemi, H., 1974. The effect of lateral positions on gasexchange in pulmonary disease. Am. Rev. Respir. Dis. 110, 49–55.