Embed Size (px)
Citation preview

Obesity Research & Clinical Practice (2009) 3, 141—148
ORIGINAL ARTICLE
Body mass index and body fat among adultBengalee male slum dwellers in West Bengal, India
Raja Chakrabortya,b, Kaushik Bosea,∗, Romendro Khongsdierc,Samiran Bisai a,c
a Department of Anthropology, Vidyasagar University, Midnapore 721102, West Bengal, Indiab Department of Anthropology, Dinabandhu Mahavidyalaya, Bongaon, North 24 Paraganas, West Bengal,Indiac Department of Anthropology, North-Eastern Hill University, Shillong 793022, India
Received 20 November 2008; received in revised form 5 March 2009; accepted 18 March 2009
KEYWORDSBengalee;Slum;Body mass index;Percent body fat;Receiver operatingcharacteristic;Obesity
SummaryObjective: The objective of the study is to explore the relationship between bodymass index (BMI) and percent body fat (PBF) in relation to hypertension among adultBengalee males of low socio-economic status living in a slum area of West Bengal,India.Methods: A cross-sectional survey was carried on 436 males aged 18—60 years ina slum area called Bidhan Colony, which is approximately 15 km from Kolkata city.Data on anthropometric measurements and blood pressure were collected, followingstandard techniques. Logistic regression and receiver operating characteristic (ROC)curve analysis were used for testing the relationship between BMI and PBF relativeto hypertension.Results: About 4.25% and 50% of the normal (BMI 18.5—22.9 kg/m2) and overweight(BMI 23.0—24.9 kg/m2) subjects, respectively, were obese according to the PBF cut-off point of >25%. The ROC curve analysis indicated that the BMI cut-off ≥23 kg/m2
was appropriate for detecting obesity relative to hypertension. It was observed thatthe prevalence of hypertension increased significantly with age (r = 0.226, p < 0.001).
2
Adjusting for age, the subjects with BMI 23—24.99 kg/m had about 3.2 times (95%CI: 1.61—6.27) greater risk of hypertension than those with BMI < 23 kg/m2, and therisk for those with BMI ≥ 25 kg/m2 was about 4.5 times (95% CI: 2.06—9.57). As forPBF, the risk of hypertension was about 2.6 times (95% CI: 1.38—4.80) for the subjectswith PBF > 25% compared to those with PBF ≤ 25%.∗ Corresponding author. Tel.: +91 09433403815.E-mail address: [email protected] (K. Bose).
1871-403X/$ — see front matter © 2009 Asian Oceanian Association for the Study of Obesity. Published by Elsevier Ltd. All rights reserved.
doi:10.1016/j.orcp.2009.03.003

142
However, such data should be substantiated by independent risks of adverse healthoutcomes that need for public health intervention.
ssociation for the Study of Obesity. Published by Elsevier Ltd.
ubc
daagoht[abmmthsWmg
M
S
TraDocIr1o1sHindu castes. The slum is situated at the right sideof the railway tracks between Dum Dum Junctionand the Dum Dum Cantonment Railway Stations. It
© 2009 Asian Oceanian AAll rights reserved.
Introduction
Accumulation of percent body fat (PBF) of >25% inmales and >35% in females, corresponding to a bodymass index (BMI) of ≥30 kg/m2 in young adult Cau-casians, is internationally accepted and extensivelyused to define obesity or excess adiposity [1,2].It is recognised as one of the major health prob-lems in both developed and developing countries[3]. However, BMI is generally used as a measure ofobesity rather than PBF because of its simplicity andhigh correlation with body fat [4]. The World HealthOrganisation (WHO) has recommended the BMI cut-offs of 25.0 kg/m2 and 30.0 kg/m2 for overweightand obesity, respectively [5]. But there is consid-erable evidence that these cut-off values are notapplicable across ethnic groups, especially amongAsian populations. It has been reported that AsianIndians, for example, have higher PBF, waist-to-hipratio (WHR) and abdominal fat at a lower levelof BMI compared with the Caucasian populations[6—8]. In Asian subjects, the risk of associationwith diabetes and CVD occurs at lower levels ofBMI compared with the Caucasians [9—11]. Accord-ingly, The WHO Regional Office for Western PacificRegion, along with the International Association forthe Study of Obesity (IASO) and the InternationalObesity Task Force (IOTF), has recommended newBMI cut-off points of 23.0 kg/m2 and 25.0 kg/m2
for defining overweight and obesity, respectively, inAsian populations [12]. Although there are severaltechniques to measure percent body fat, the use ofskinfolds is the most preferred method because it isnon-invasive, less expensive and suitable for largescale population surveys.
There is increasing evidence that the relation-ship between BMI and PBF depends upon age, sexand ethnicity [13—16]. It has been also documentedthat the same ethnic group residing in differentgeographical locations could have a different pat-tern of BMI—PBF relationship. Asians including AsianIndians refer to a vast and bio-culturally diversifiedpopulations living in different levels of urban-
isation, socio-economic conditions and nutritiontransitions. Each of them may have a different bodycomposition [4]. It is, therefore, recommended thatfurther researches be undertaken with a view toiPtM
nderstanding the relationship between BMI andody fat in relation to risk factors and health out-omes, especially among Asian populations [4,12].
In India and other developing countries, slumwellers are of particular interest, because theyre mainly the poor people who migrated from ruralreas to settle down in towns and cities, therebyetting exposed to adverse urban lifestyles andbesogenic environments. Unfortunately, there isardly any study among the slum dwellers in Indiao explore the relationship between BMI and PBF17] in relation to risk factors like hypertension,lthough some studies reported the relationshipetween BMI and risk factors for cardiovascular andetabolic disorders in non-slum areas [18—21]. Theain purpose of the present study is to explore
he relationship between BMI and PBF in relation toypertension among adult Bengalee males of lowocio-economic status residing in a slum area ofest Bengal, India, since there is lack of infor-ation on obesity and hypertension among this
roup.
aterials and methods
tudy area and sample
he present study was conducted as a part of aesearch project jointly undertaken by the first twouthors in a slum area known as Bidhan Colony ofum Dum, approximately 15 km from the centref Kolkata city. Kolkata (formerly known as Cal-utta) is the capital of the state of West Bengal inndia. Kolkata is situated on the eastern bank of theiver Ganges (also known as Hooghly River), about20 km from the Bay of Bengal. Dum Dum, beingne of the urban centres of the district is about0 km to the north of Kolkata. The subjects of thetudy were adult men belonging to the Bengalee
R. Chakraborty et al.
Conclusions: Our study validated the BMI cut-off point proposed by the WHO for Asia-Pacific populations for screening the individuals who are likely at risk of overweight.
s the terminal part of an urban settlement, calledurba (East) Sinthee, nearby the Dum Dum Junc-ion Railway Station, under the South Dum Dumunicipality, North 24 Parganas of West Bengal. The

Body mass index and body fat among Bengalee males 143
Table 1 Characteristics of the sample.
Variables Mean S.D.
Age (years) 34.75 11.12Height (cm) 161.73 6.11Weight (kg) 53.61 9.34Biceps skinfolds (mm) 4.48 2.42Triceps skinfolds (mm) 7.23 3.60Sub-scapular skinfolds (mm) 13.83 7.67Supra-iliac skinfolds (mm) 13.29 8.86Sum of four skinfolds (mm) 38.83 21.10Body mass index (kg/m2) 20.47 3.26Percent body fat (%) 16.07 6.95
otsmdsCTlo
hucpircAidif
M
Tm(s
Fg
pAfw0tn(nLtefpoaSRmpams
Systolic blood pressure 120.12 13.55Diastolic blood pressure 79.55 9.59
ther side of the railway track is under the jurisdic-ion of Kolkata Municipal Corporation. Most of theubjects belonged to a low socio-economic status,ostly being factory workers, rickshaw-pullers anday-labourers. Ethical approval and prior permis-ion was obtained from Vidyasagar University Ethicsommittee and the institution of the first author.he municipal authorities and local community
eaders were informed before the commencementf the study.
Each subject was interviewed and measured atis respective household. In some cases, dependingpon logistic circumstances, they were taken to aommon place for examination. However, all thearticipants had their residence within the admin-strative boundary of the area under study. Overallesponse rate was found to be around 80%. Informedonsent was also obtained from each participant.total of 436 adult men aged 18—60 years were
ncluded in this study. For missing blood pressureata, three subjects were excluded in the analysesnvolving blood pressure and hypertension. There-ore, in those cases the sample size remained 433.
easurements
he field investigation including anthropometriceasurements was carried out by the first author
R.C.). Information on ethnicity, age and someocio-economic were collected from each partici-
bdtP
Table 2 Mean (SD) age and prevalence (%) of obesity (PBF
BMI categories (kg/m2) Number Age (m
<23 347 33.95 ±23—24.9 52 37.40 ±
≥25 37 38.51 ±
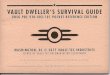
igure 1 Prevalence of obesity according to BMI cate-ories in relation to PBF ≤ 25% and >25%.
ant with the help of a pre-tested questionnaire.ll the anthropometric measurements were takenollowing the standard techniques [22]. Height andeight were measured to the nearest 0.1 cm and.5 kg, respectively, using standard anthropome-er, and weight scale, respectively. Four skinfoldsamely, biceps (BSF), triceps (TSF), sub-scapularSSF) and supra-iliac (SISF), were measured to theearest 0.2 mm using a skinfold calliper (Holtaintd., UK). Single instruments were used for eachype of measurements to avoid inter-instrumentalrrors. Technical errors of measurements wereound to be within the acceptable limits [23]. Bloodressure was measured by R.C. on the right armf each subject, using standard stethoscope anddigital blood pressure monitor (Home Health,
witzerland) following the prescribed protocol.esting systolic and diastolic blood pressures (inmHg) was measured with the subject in a sittingosition for at least 15 min prior to measurementnd again at least 10 min after the first reading. Theean values of two measures were used in analy-
es. BMI was computed as weight (in kg) divided
y height (in meter squared). Hypertension wasefined as a systolic BP ≥ 140 mmHg and/or dias-olic BP ≥ 90 mmHg, whereas obesity was defined asBF > 25%. PBF was calculated using the sum of four> 25) according to BMI categories.
ean ± S.D.) Prevalence (%)
≤25% >25%
11.13 338 (97.41) 9 (2.59)11.04 26 (50.00) 26 (50.00)9.98 9 (24.32) 28 (75.68)

3Prt1t
aPwapopoojtaiocacssiatea4otp
144
skinfolds according to the equations of Siri [24] andDurnin and Womersley [25] as generally followedby other studies in Indian populations [21,26]. Theequations are expressed as follows:
PBF =(
4.95density
− 4.5)
× 100
where
density = 1.1765 − 0.0744
×log10(BSF + TSF + SSF + SISF)
Statistical analyses
Data were analysed using SPSS package for win-dows (SPSS Inc., Chicago, IL, USA). Two-tailed testwas used by setting the significance level at 5%.Mean and standard deviation (S.D.) values for age,anthropometric variables and blood pressure werecomputed. The distributions of the anthropomet-ric variables were not significantly skewed. Pearsoncorrelation coefficient (r) was used to test the cor-relation between two variables. Receiver operatingcharacteristics (ROC) curve analysis was used todetermine the best BMI cut-off point against twocategories of PBF i.e., non-obese (coded as 0) andobese (coded as 1). The odds ratio (OR) with 95%CI relative to the prevalence of hypertension wasderived from the coefficient of logistic regressionafter adjusting for age.
Results
Table 1 presents the means and standard devi-ations of age, blood pressure and anthropomet-ric variables. Mean age of the subjects was
sse(
Table 3 Sensitivity and specificity of different BMI threshvalue of >25%.
BMI Sensitivity (95% CI) Specificity (95%CI)
21.50 92.1 (82.4—97.3) 76.94 (72.3—81.1)22.00 92.1 (82.4—97.3) 83.11 (78.9—86.8)22.50 87.3 (76.5—94.3) 88.20 (84.5—91.3)22.90 85.7 (74.6—93.2) 89.81 (86.3—92.7)23.00 85.7 (74.6—93.2) 91.15 (87.8—93.8) 623.10 84.1 (72.7—92.1 91.42 (88.1—94.1)23.50 63.5 (50.4—75.3) 93.57 (90.6—95.8)24.00 57.1 (44.0—69.5) 96.78 (94.4—98.3)24.50 52.4 (39.4—65.1) 97.05 (94.8—98.5)25.00 44.4 (31.9—57.5) 97.86 (95.8—99.1)
R. Chakraborty et al.
4.7 ± 11.13 years, and the mean values of BMI andBF were 20.47 ± 3.26 kg/m2 and 16.07 ± 6.95%,espectively. The mean values of diastolic and sys-olic blood pressure were 79.55 ± 9.59 mmHg and20.12 ± 13.55 mmHg, respectively, which seemedo be in normal condition.
Table 2 shows the classification of the subjectsccording to BMI categories in relation to theirBF. It was found that BMI increased significantlyith age of the individuals (r = 0.115, p < 0.016)nd was positively correlated with PBF (r = 0.817,< 0.0001). Following the recent recommendationf BMI classification for Asian populations [12], therevalence of overweight was 11.93% and that ofbesity 8.49% out of 436 subjects. It is, however,bserved that about 50% of these overweight sub-ects would be classified as obese on the basis ofheir PBF. Similarly, about 24% of the obese subjectsccording to BMI would be classified as non-obesef their PBF was taken into consideration. This sortf misclassification is expected to be high espe-ially if the BMI cut-off points of 25—29.9 kg/m2
nd 30.0 kg/m2 are taken into consideration forlassifying the subjects into overweight and obe-ity categories [5]. The present findings, therefore,eem to support the recommendation for reduc-ng the BMI cut-off points for Asian populations,lthough a misclassification of the subjects is likelyo persist irrespective of such reduced BMI cat-gories. Fig. 1 shows the prevalence of obesityccording to BMI categories in relation to PBF. About.25% and 50% of the normal (18.5—22.9 kg/m2) andverweight (23.0—24.9 kg/m2) subjects, respec-ively, were obese according to the PBF cut-offoint of 25.
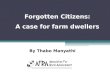
Using ROC curve analysis, Table 3 shows
ensitivity and specificity values according toelected threshold values of BMI against the ref-rence PBF > 25%. The area under ROC curveAUC) (Fig. 2) was 0.941 ± 0.021 with a CI ofolds in detection of obesity against the PBF reference
Positive predicted value Negative predicted value
40.3 98.347.9 98.455.6 97.658.7 97.42.1 97.4
62.4 97.262.5 93.875.0 93.075.0 92.377.8 91.2

Body mass index and body fat among Bengalee males
Fa
0tfot≥i9tei(dC
vp(wtcoa≥ao
toltsOht3t2syw3tf(frtt
2
igure 2 ROC curve of sensitivity and specificity by BMIgainst reference PBF.
.914—0.961 (p < 0.0001). The results indicatedhat a BMI ≥ 23 kg/m2 would be most appropriateor detecting obesity among the male slum dwellersf the present study. It is evident from Table 3hat the ROC curve for the BMI cut-off point of25 kg/m2 against the reference PBF > 25% resulted
n about 44% sensitivity (95% Cl: 31.9—57.5) and8% specificity (95% Cl: 95.8—99.1). However, ifhe proposed cut-off for screening obesity is low-red to BMI ≥ 23 kg/m2, the amount of sensitivity
ncreased substantially from 44% to about 86%95% Cl: 74.6—93.2), while that of specificityecreased marginally from 98% to about 91% (95%I: 87.8—93.8). Similarly, the positive predictedtP(a
Table 4 Summary of the logistic regression analysis of hyp
Parameters N Prevalence (%)
Age groups (years)≤24 97 6 (6.19)
25—34 129 17 (13.18)35—44 110 21(19.09)
≥45 97 32 (32.99)
BMI categories<23 346 43 (12.43)
23—24.9 52 18 (34.62)≥25 35 15 (42.86)
PBF categories≤25 371 56 (15.09)>25 62 20 (32.26)
a Adjusted for age.
145
alue increased from 62% to 79% and the negativeredicted value decreased from about 97% to 91%highlighted in bold in Table 3). It may be worth-hile to mention that the prevalence of obesity in
he present study increased from 8.5% for the BMIut-off ≥25 kg/m2 to about 20.41% for the BMI cut-ff ≥23 kg/m2, resulting in an additional increase ofbout 12%. On the other hand, when the BMI cut-off30 kg/m2 was taken into consideration [5], suchn additional increase was about 19% (from 5 to 89ut of 436 individuals).
The relationship between BMI and PBF was fur-her tested taking into account the prevalencef hypertension (Table 4). The overall preva-ence of hypertension was 17.6%. It was observedhat the prevalence of hypertension increasedignificantly with age (r = 0.226, p < 0.001). TheR with 95% CI relative to the prevalence ofypertension derived from the coefficient of logis-ic regression indicated that the subjects aged5—44 and ≥45 years were, respectively, about 3.6imes (95% CI: 1.38—9.28) and 7.5 times (95% CI:.95—18.89) more likely to suffer from hyperten-ion as compared to those in the age group ≤ 24ears (p < 0.001). Adjusting for age, the subjectsith BMI 23—24.9 kg/m2 were likely to have about.2 times (95% CI: 1.61—6.27) greater risk of hyper-ension than those with BMI < 23 kg/m2, and the riskor those with BMI ≥ 25 kg/m2 was about 4.5 times95% CI: 2.06—9.57). There was no significant dif-erence between these two categories of BMI withespect to the prevalence of hypertension, althoughhe subjects with BMI ≥ 25 kg/m2 had about 1.4imes (95% CI: 0.57—3.43) greater risk of hyper-
ension than those with BMI 23—24.9 kg/m . As forBF, the risk of hypertension was about 2.6 times95% CI: 1.38—4.80) for the subjects with PBF > 25%s compared to those with PBF ≤ 25%. Thus, theertension on age, BMI and PBF.
Odds ratio* (95% CI) p-Level
— —2.30 (0.87—6.08) 0.0923.58 (1.38—9.28) 0.0097.47 (2.95—18.89) 0.001
— —3.18 (1.61—6.27)a 0.0014.45 (2.06—9.57)a 0.001
— —2.57 (1.38—4.80)a 0.003

phibftesslsopisp(sgpltHlcbfiPtanub
tiamfoetitaofbmri
146
present findings revealed that the proposed BMIcut-off point of ≥23 kg/m2 based on PBF > 25% wasalso associated with an increased risk of hyperten-sion.
Discussion
It is evident from the present analyses that there isconsiderable misclassification of the individuals asobese and non-obese on the basis of their BMI alone.The validity of BMI as a measure of obesity has, ofcourse, been questioned by many studies in bothdeveloped and developing countries [1,2,13,17].The major concern is that BMI is simply a crudemeasure of body weight relative to height, whichtells nothing about the relative proportion of bodyfat and other components of body composition [26].On the other hand, it is the degree of body fatnessthat should be considered a risk factor from theclinical and physiological points of view. In addi-tion, the relationship between BMI and body fat iscompounded by age, sex and ethnicity [13—16,27].These factors make the diagnosis of obesity morecomplicated on the basis of BMI alone.
Several studies in various Asian countries likeChina [28,29] Taiwan [30], Hong Kong [31] andJapan [32] have reported an association betweena BMI > 22.3 kg/m2 and increased atherogenic riskfactors. The risk of co-morbidities of diabetes, dys-lipidemia, and hypertension was found to increasesignificantly with a BMI of >22.0 kg/m2 [33]. Inshort, there is considerable evidence that Asianshave a greater percentage of total body fat at thesame BMI values than the Europeans and the risk ofchronic diseases in these populations increased sig-nificantly at a much lower BMI compared with theEuropeans [34,35].
Our data on hypertension seem to be consis-tent with those earlier findings. Therefore, thepresent findings support the recommendation forreducing the BMI cut-off points for Asian popula-tions, although a misclassification of the subjects islikely to persist irrespective of such reduced BMIcategories depending upon the risk factors for aspecific population. Our findings are also consistentwith a study among urban males of southern India,where a BMI of >23 kg/m2 was significantly associ-ated with an increased risk of diabetes [18]. Otherstudies have, however, suggested different cut-offpoints varying between 21.5 kg/m2 and 24 kg/m2
[17,19,20,36]. A recent study among the Bengaleemales of Kolkata found that a BMI of 24 kg/m2 wasthe best cut-off for defining obesity [21].
The ROC curve analysis of our data indicatedthat the BMI cut-off point of ≥23 kg/m2 was appro-
efu
l
R. Chakraborty et al.
riate for detecting obesity (PBF > 25) relative toypertension among the slum dwellers. Therefore,t is likely that the relationship between BMI andody fat relative to risk factors in India variesrom one region to another, or from populationo population depending on socio-economic andnvironmental conditions. There is, however, con-iderable evidence that the proportion of Indianubjects with a high risk of type 2 diabetes mel-itus, hypertension and cardiovascular diseases isubstantial at BMI values lower than the WHO cut-ff point ≥25 kg/m2 for overweight [5]. The newroposed cut-off point ≥23 kg/m2 for overweightn Asia-Pacific populations [12] seems to be con-istent with the present sample, although a largeroportion of the overweight individuals at risk23—24.9 kg/m2) may fall in the categories of obe-ity (25—29.9 kg/m2 for grade 1, and ≥30 kg/m2 forrade 2) relative to PBF and/or risk factors in Indianopulations. This should not be confused in a popu-ation study in which the main purpose is to screenhe individuals at risk of obesity and co-morbidities.owever, the major concern may still prevail, if a
arge proportion of the Indian subjects are at risk ofo-morbidities with BMI < 23 kg/m2 [20,36]. On theasis of available evidence including the presentndings, the new BMI cut-off of ≥23 kg/m2 for Asia-acific populations may be more appropriate thanhe conventional cut-off ≥25 kg/m2 for overweightt least for Indian populations. More studies areeeded to carry out among different Indian pop-lations, taking into consideration the relationshipetween BMI and PBF relative to risk factors.
There are limitations of our study. Our study hasaken PBF of >25% as a reference for determin-ng the reliability of BMI as a diagnostic tool forssessing obesity. PBF was estimated from skinfoldeasurements, using prediction equations derived
rom European populations as generally followed byther studies [17,19,20,36]. In addition to technicalrrors of measurements, these prediction equa-ions may have large prediction errors [37,38]. Its, therefore, difficult at present to suggest thathe prediction methods of PBF based on skinfoldsnd bioelectrical impedance should be preferredver BMI. Although direct measurements of bodyat like in vivo neutron activation analysis woulde a better measure of obesity [4], such types ofethod would not be easily available especially for
esearchers in developing countries. The use of BMIs preferable because it is easier, speedier and less
xpensive; although its reliability as a measure ofatness can be questioned especially at the individ-al level.Considering our findings and other studies, it isikely that a BMI cut-off point relative to risk factors

B es
weTmbasafatpimsclwaputnneI
C
Te
R
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
ody mass index and body fat among Bengalee mal
ould vary across Indian populations living in differ-nt ecological and socio-environmental conditions.he BMI cut-off point of ≥23 kg/m2 as recom-ended by the WHO for Asia-Pacific region [12] maye used for screening the proportion of people whore likely at risk of overweight. However, such datahould be substantiated by independent and inter-ctive risks of adverse health outcomes that needor public health intervention, taking into consider-tion the possibility of under- and over-estimationhat may result in an unnecessary burden on theart of public health expenditure. The use of PBFn relation to BMI and risk factors is likely to beore informative about the nutritional and health
tatus of the study population for further clini-al investigation and intervention at the individualevel. Lastly, it must be mentioned here that theidely used terms like Asian or Indian characterisevast and diverse population. Diversity in Asian
opulations based on ethnicity, culture, degrees ofrbanisation, socio-economic condition and nutri-ion transition [4] and therefore, our results mayot applicable to all of them. Similar studies areeeded among the various ethnic groups of diverseconomic backgrounds to arrive at a more pan-ndian consensus.
onflict of interest statement
his manuscript does not have any conflict of inter-st.
eferences
[1] Deurenberg P, Yap M, van Stavaren WA. Body mass index andpercent body fat: a meta analysis among different ethnicgroups. Int J Obes 1998;22:1164—71.
[2] Deurenberg P, Deurenberg Yap M, Wang J, Lin FP, SchmidtG. The impact of body build on the relationship betweenbody mass index and percent body fat. Int J Obes1999;23:537—42.
[3] Zimmet P, Alberti KG, Shaw J. Global and societal implica-tions of the diabetes epidemic. Nature 2001;414:782—7.
[4] WHO expert consultation. Appropriate body mass index forAsian populations and its implications for policy and inter-vention strategies. Lancet 2004;363:157—63.
[5] WHO. Physical status: the use and interpretation of anthro-pometry. Technical Report Series No. 854. Geneva: WorldHealth Organization; 1995.
[6] Ramachandran A, Snehalatha C, Viswanathan V,Viswanathan M, Haffner SM. Risk of non-insulin dependentdiabetes mellitus conferred by obesity and central adi-
posity in different ethnic groups: a comparative analysisbetween Asian Indians, Mexican Americans and Whites.Diabetes Res Clin Pract 1997;36:121—5.[7] Deurenberg-Yap M, Schmidt G, van Stavaren WA, Deuren-berg P. The paradox of low body mass index and high body
[
147
fat percentage among Chinese, Malaya and Indians in Sin-gapore. Int J Obes 2000;24:1011—7.
[8] Deurenberg P, Deurenberg-Yap M, Guricci S. Asians aredifferent from Caucasians and from each other in theirbody mass index/body fat per cent relationship. Obes Rev2002;3:141—6.
[9] McKeigue PM, Shah B. Relationship of central obesity andinsulin resistance with high diabetes prevalence and car-diovascular risk in South Asians. Lancet 1991;337:382—6.
10] Banerji MA, Faridi N, Atluri R, Chaiken RL, Lebovitz HE.Body composition, visceral fat, leptin and insulin resistancein Asian Indian men. J Clin Endocrinol Metab 1999;84:137—44.
11] Chandalia M, Abate N, Garg A, Stray-Gundersen J, GundySM. Relationship between generalised and upper bodyobesity to insulin resistance in Asian Indian men. J ClinEndocrinol Metab 1999;84:2329—35.
12] WHO. The Asia Pacific perspective: redefining obesity andits treatment. Geneva: World Health Organization; 2000.
13] Norgan NG. Body mass index and body energy stores indeveloping countries. Eur J Clin Nutr 1990;44(S1):79—84.
14] Gallagher D, Visser M, Sepulveda D, Pierson RN, Harris T,Heymsfield S. How useful is body mass index for comparisonof body fatness across age, sex, and ethnic groups? Am JEpidemiol 1996;143(3):228—39.
15] Taylor RW, Jones IE, Williams SM, Goulding A. Evaluationof waist circumference, waist-to-hip ratio and the Conicityindex as screening tools for high trunk fat mass, as mea-sured by dual energy X-ray absorptiometry, in children aged3—19 years. Am J Clin Nutr 2000;72:490—5.
16] Bose K. The interaction of waist-hip ratio and Conicityindex with subcutaneous adiposity in two ethnic groups:native British and migrant Pakistani men. Anthropol Anz2001;59:275—82.
17] Misra A, Pandey RM, Sinha S, Guleria R, Sridhar V, Dudeja V.Receiver operating characteristics curve analysis of body fatand body mass index in dyslipidemic Asian Indians. Indian JMed Res 2003;117:170—9.
18] Snehalatha C, Viswanathan V, Ramachandran A. Cut off val-ues for normal anthropometric variables in Asian Indianadults. Diabetes Care 2003;26:1380—4.
19] Vikram NK, Misra A, Pandey RM, Dudeja V, Sinha S, RamadeviJ, et al. Anthropometry and body composition in NorthernAsian Indians patients with type 2 diabetes: receiver oper-ating characteristic (ROC) curve analysis of body mass indexwith percentage body fat as standard. Diabetes Nutr Metab2003;16(1):32—40.
20] Singh KD, Dhillon JK, Arora A, Gill BS. Receiver operatingcharacteristic curve analysis of BMI and percentage bodyfat in type 2 diabetics of Punjab. Indian J Physiol Pharmacol2004;48(1):73—80.
21] Ghosh JR, Bandyopadhyay AR. Waist circumference as ameasure of total body fat in Asian Indians. Int J Body CompRes 2007;5(3):89—93.
22] Lohman TG, Roche AF, Martorell R. Anthropometric stan-dardization reference manual. Chicago: Human KineticsBooks; 1988.
23] Ulijaszek SJ, Kerr DA. Anthropometric measurement errorand the assessment of nutritional status. Br J Nutr1999;82:165—77.
24] Siri WE. Body composition from fluid spaces and density:
analysis of methods. In: Brozek J, Hensche A, editors. Tech-niques for measuring body composition. Washington, DC:National Academy of Sciences; 1961. p. 223—44.25] Durnin JVGA, Womersley J. Body fat assessed from totalbody density and its estimation from skin fold thickness:

[
[
[
[
[
148
measurements on 481 men and women aged from 16 to 72years. Br J Nutr 1974;32:77—97.
[26] Khongsdier R. BMI and morbidity in relation to body com-position: a cross-sectional study of a rural community inNorth-East India. Br J Nutr 2005;93:101—7.
[27] Bose K, Mascie-Taylor CGN. Conicity index and waist-to-hipratio and their relationship with total cholesterol and bloodpressure in middle aged Europeans and migrant Pakistanimen. Ann Hum Biol 1998;25:11—6.
[28] Zhou B, Wu Y, Yang J, Li Y, Zhang H, Zhao L. Overweight isan independent factor for cardiovascular disease in Chinesepopulation. Obes Rev 2002;3:157—76.
[29] Jia WP, Xiang K, Chen L, Lu JX, Wu YM. Epidemiologicalstudy on obesity and its comorbidities in urban Chineseolder than 20 years of age in Shanghai, China. Obes Rev2002;3:157—76.
[30] Chang C, Wu C, Chang C, Yao WJ, Yang YC, Wu JS, Lu FH.Low body mass index but high percent body fat in Tai-wanese subjects: implications of obesity cut off. Int J Obes2003;27:253—9.
[31] Lee Z, Ctitchley J, Ko GT, Anderson PJ, Thomas GN, YoungRP. Obesity and cardiovascular risk factors in Hong KongChinese. Obes Rev 2002;3:173—82.
[32] Ito H, Nakasuga K, Chen L, Nakasaga K, Oshima A,Maruyama T, et al. Detection of cardiovascular risk fac-
[
Available online at www.s
R. Chakraborty et al.
tors by indices of obesity obtained from anthropometry anddual-energy absorptiometry in Japanese individuals. Int JObes 2003;27:232—7.
33] Ko GTC, Chan JCN, Cockram CS, Woo J. Prediction of hyper-tension, diabetes, dyslipidemia or albuminuria using simpleanthropometric indexes in Hong Kong Chinese. Int J Obes1999;29:1136—42.
34] Wang J, Thornton JC, Russel M, Burastero S, HeymsfieldSB, Pierson RN. Asians have lower BMI but higher percentbody fat than do Whites: comparisons of anthropometricmeasurements. Am J Clin Nutr 1994;60:23—8.
35] Kim Y, Suh YK, Choi H. BMI and metabolic disorders in SouthKorean adults: 1998 Korea National Health and NutritionSurvey. Obes Res 2004;12(3):445—53.
36] Dudeja V, Mishra A, Pandey RM, Devina G, Kumar G, VikramNK. BMI does not accurately predict overweight in AsianIndians in Northern India. Br J Nutr 2001;86:105—12.
37] Davies PSW. Anthropometry and body composition. In: Uli-jaszek SJ, Mascie-Taylor CGN, editors. Anthropometry: theindividual and the population. Cambridge: Cambridge Uni-
versity Press; 1994. p. 130—40.38] Peterson MJ, Czerwinski SA, Siervogel RM. Development andvalidation of skinfold-thickness prediction equations witha 4-compartment model. Am J Clin Nutr 2003;77:1186—91.
ciencedirect.com