Embed Size (px)
Citation preview

Body fluids
Electrolytes

Electrolytes
• Electrolytes form IONS when in H2O (ions are electrically charged particles)
• (Non electrolytes are substances which do not split into ions, e.g. glucose)
CATIONS = Positively charged particles
(e.g. Na+, K+, Ca++)
ANIONS = Negatively charged particles (e.g. HCO3- Cl-)
E.g.
NaCl
Na+ + Cl-
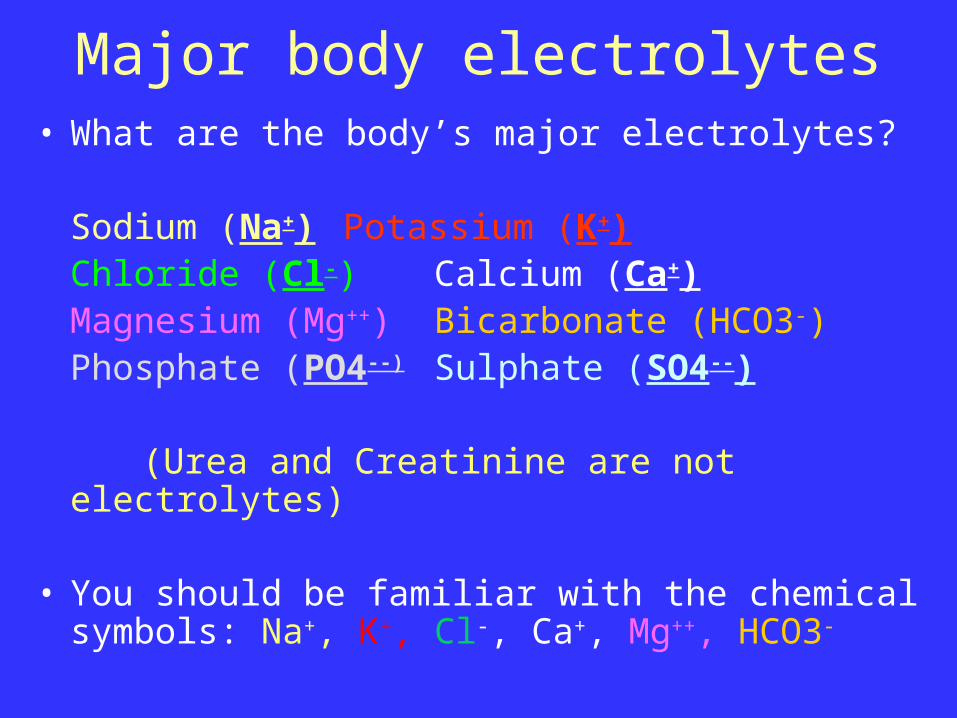
Major body electrolytes• What are the body’s major electrolytes?
Sodium (Na+) Potassium (K+)Chloride (Cl-) Calcium (Ca+)Magnesium (Mg++) Bicarbonate (HCO3-)Phosphate (PO4--) Sulphate (SO4--)
(Urea and Creatinine are not electrolytes)
• You should be familiar with the chemical symbols: Na+, K+, Cl-, Ca+, Mg++, HCO3-

Importance of electrolyte balance
Electrolytes are critical for cellular reactions
They are found in all fluid compartments
Essential in:• Muscle co-ordination• Heart function• Fluid absorption and
excretion• Nerve function
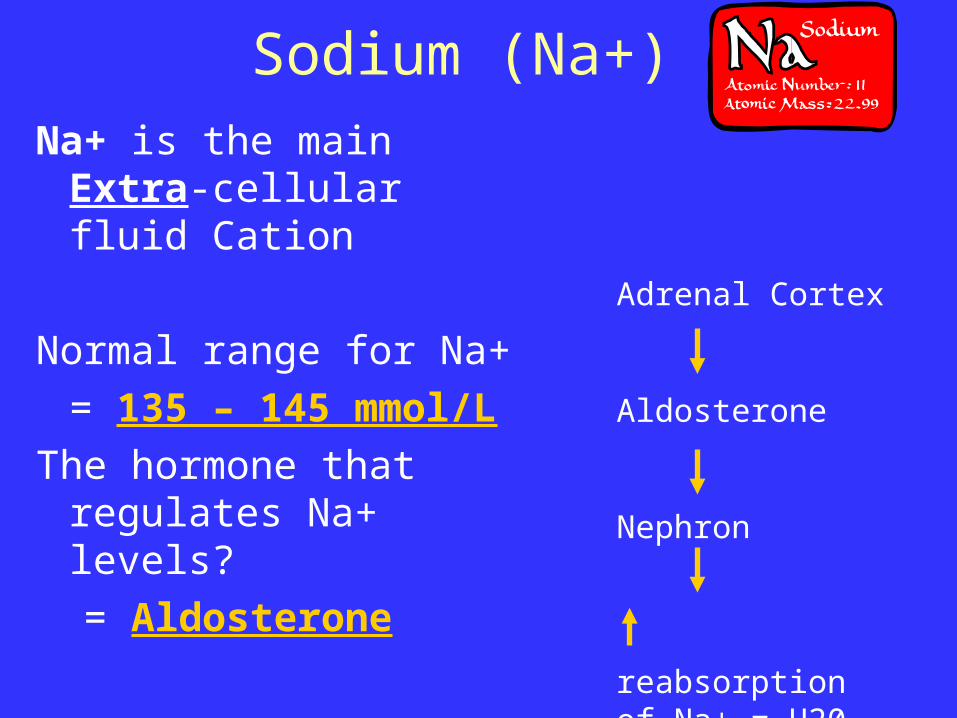
Sodium (Na+)
Na+ is the main Extra-cellular fluid Cation
Normal range for Na+
= 135 – 145 mmol/L
The hormone that regulates Na+ levels?
= Aldosterone
Adrenal Cortex
Aldosterone
Nephron
reabsorption of Na+ = H20
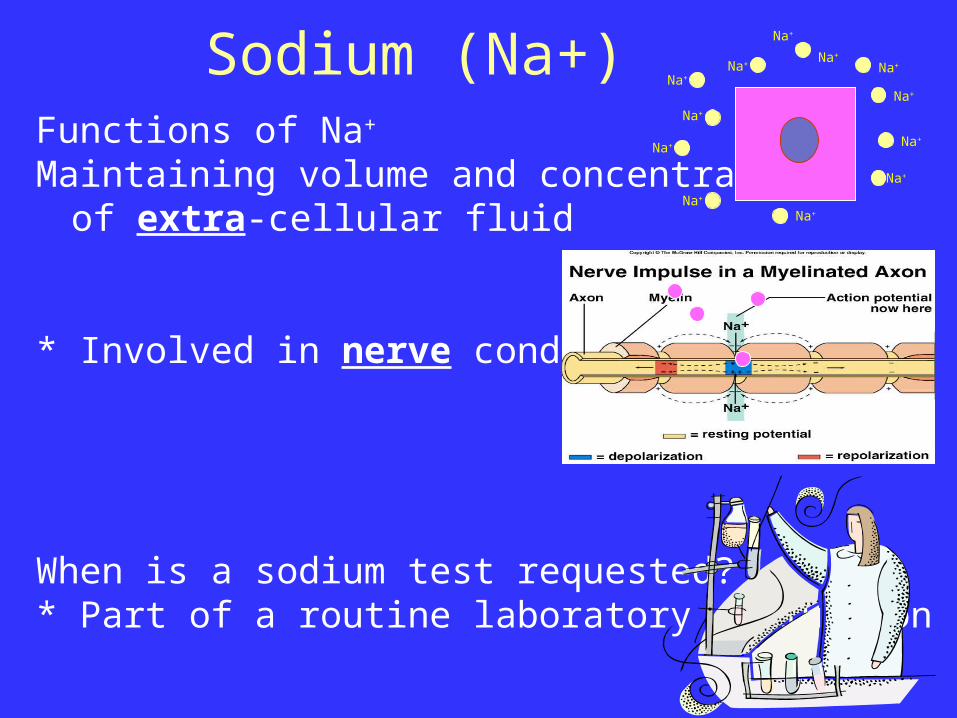
Sodium (Na+)Functions of Na+
Maintaining volume and concentration of extra-cellular fluid
* Involved in nerve conduction
When is a sodium test requested?* Part of a routine laboratory evaluation
Na+
Na+
Na+
Na+Na+
Na+
Na+
Na+
Na+
Na+
Na+
Na+
Sodium (Na+)What is Hyponatraemia?
Low blood sodium levels (less than 135mmol/L)
May occur in:Excessive sweating
Symptoms of HyponatraemiaMuscle cramps & WeaknessFatigue & Nausea,Apathy & HeadacheConfusion Seizures
Treatment = Replacement therapy
Sodium (Na+)What is Hypernatraemia ?
High sodium in the blood (more than 145mmol/L)
Normally occurs because of inadequate fluid intake
Signs and symptoms includeIntense thirstDecreased urine output Confusion Seizures
Treatment =IV or oral water replacement
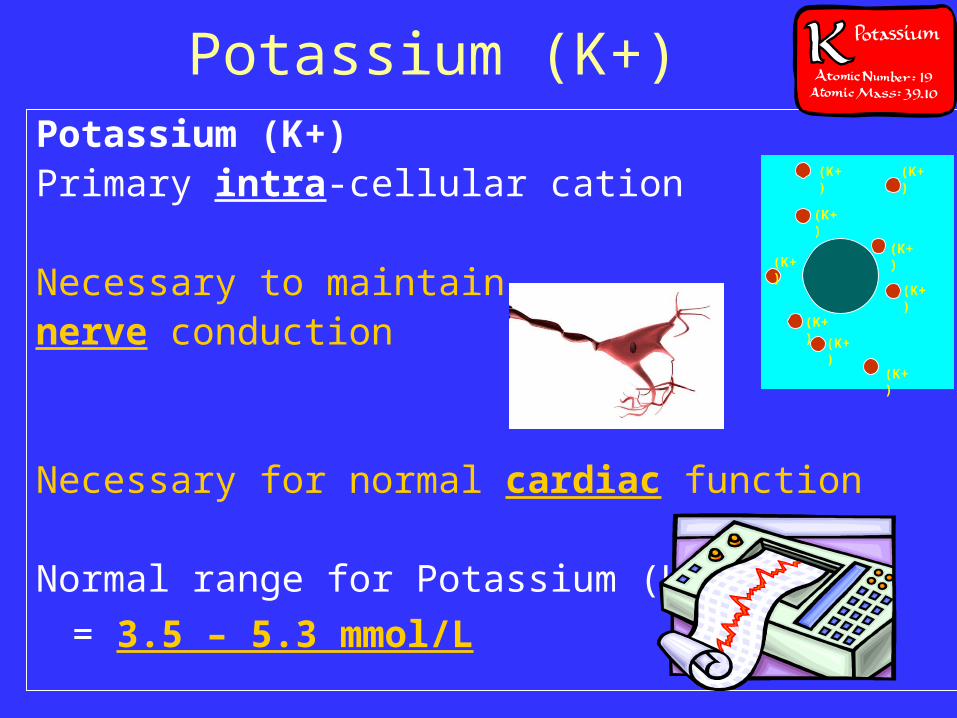
Potassium (K+)Potassium (K+)Primary intra-cellular cation
Necessary to maintainnerve conduction
Necessary for normal cardiac function
Normal range for Potassium (K+)
= 3.5 – 5.3 mmol/L
(K+)
(K+)
(K+)
(K+)
(K+)
(K+)
(K+)
(K+)
(K+)
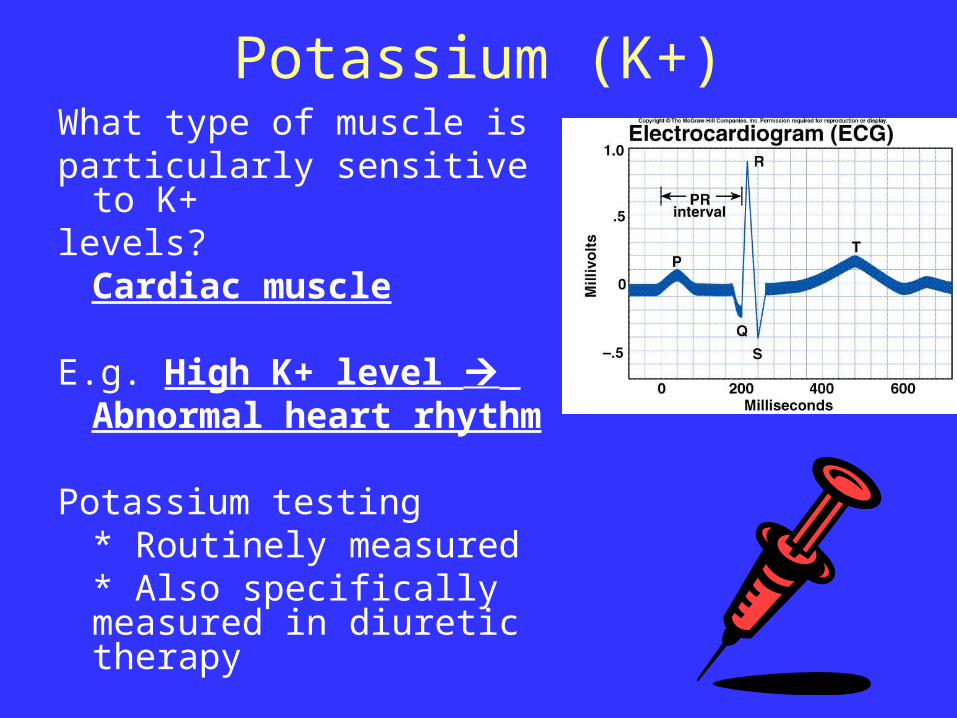
Potassium (K+)What type of muscle isparticularly sensitive to K+levels?
Cardiac muscle
E.g. High K+ level Abnormal heart rhythm
Potassium testing* Routinely measured* Also specifically measured in diuretic therapy
Potassium (K+)Hypokalaemia = An abnormally low level of blood
potassium (less than 3.5mmol/L)Causes:
Inadequate intakeLoss of K+ from the body (e.g. diuretics or gastric losses)
Signs and symptoms Skeletal muscle weaknessECG changes
Treatment = Replacement - foods (e.g. bananas, spinach) or K+supplements

Potassium (K+)Hyperkalaemia = serum potassium concentration
greater than 5.5mmol/L
Caused by:
Decreased excretion of K+
Movement of K+ out of the cells in trauma
IV potassium infusion
Signs of hyperkalaemia:
Include ECG changes
Treatment
Depends on the blood K+ level

Calcium (Ca++)• 99% is stored in the skeleton
and teeth (huge reserve)
• 50% of blood calcium is ionized, the rest is protein bound.
* Only the ionized calcium is used in functions such as: muscle contraction cardiac nerve impulse
function transmission
Phosphate (PO4)• 85% of body’s total
phosphorus is contained in the bones,
• The remainder is in the cells.
• Phosphate is required for:
Generation of bony tissue, Metabolism,
Maintenance of acid base balance
Bicarbonate (HCO3-)
What is the normal range for Bicarbonate (HCO3-)
22 – 30 mmol/L
What is the ‘job’ of bicarbonate?
Prevents body getting too acidic
(i.e. acid-base balance)

Urea
Nitrogen containing waste product from metabolism (protein breakdown)
Excreted through the kidneys kidneys
Good indicator of renal function
Serum urea = 2.5 – 6.6 mmol/L

Creatinine• A metabolic waste product produced by
breakdown of muscle protein (creatine).
• Why is creatinine measured?To determine kidney function
• Serum Creatinine concentration is a more accurate indicator of renal function than urea

Laboratory ResultsIs an abnormal test always a sign of a real problem?
Not always, but should be further investigated
Are reference ranges specific to the laboratory that produces?
Yes
Final pointAll the above points are clinically relevant and it isimportant that you have a good understanding of fluidand electrolyte balance by the time you qualify.

















![(6) (1) (2)€¦ · A green solution, X, is thought to contain [Fe(H2O)6]2+ ions. (a) €€€€The presence of these ions can be confirmed by reacting separate samples of solution](https://img.pdfslide.us/doc/110x75/5eae42e79116ec5e20721fe1/6-1-2-a-green-solution-x-is-thought-to-contain-feh2o62-ions-a-aaaathe.jpg)