Embed Size (px)
Citation preview

Body dysmorphic dsorder (BDD)is a disorder of body image thatremains challenging to diagnose Itis not possible surgically to lsquocurersquopatients with this condition whichrequires referral to a clinical psy-chologist or psychiatr ist ideallythrough their general medical prac-titionerThe prevalence of BDD inthe population is estimated to beapproximately 11 However dataon the prevalence of BDD in theUK community are generally lack-ing In one study 86 of a sampleof patients diagnosed with BDDspecified their dentofacial appear-ance as the cause of their concern2
In another study approximately20 of a sample of 500 patientsdiagnosed with BDD expressedspecific concern regarding theirdental appearance1 Therefore den-tists orthodontists and facial aestheticsurgeons must be aware of the conditionThis is particularly important for dentalclinicians as the condition tends toreceive little exposure within dental
journals However commencing treat-ment on such patients risks not onlypotential medicolegal problems for theclinician but also antagonism and evenviolence
BODY DYSMORPHIC DISORDER
The Italian professor of psychiatryEnrico Morselli (Figure 1) describeda condition termed lsquoDysmorpho-phobiarsquo in 1891 The condition hasbeen redefined as two separate enti-ties delusional and non-delusionalvariants It is only relatively recentlythat the non-delusional var iantwas classified as body dysmorphicdisorder (BDD) in the Diagnosticand Statistical Manual of MentalDisorders3
BDD is characterised by a pre-occupation with an insignificant ornon-existent appearance defect thatcauses significant distress to patientsand interferes with their social lifeThe most common preoccupationsinvolve the skin nose eyes and eye-
lids lips mouth jaws and chin Howeverany part of the body may be involved andthe preoccupation may involve severalbody parts simultaneously4 The criteriarequired to make a diagnosis of BDD
Body dysmorphic dsorder (BDD) is characterised by a preoc-cupation with an imagined defect in onersquos appearance or in the caseof a minor physical anomaly the individualrsquos concern is markedlyexcessive causing significant distress in their life One of the mostcommon areas of preoccupation is the dentofacial region with up to20 of patients diagnosed with BDD expressing specific concernregarding their dental appearance With the increased ability to
undertake dental aesthetic and reconstructive procedures inaddition to the use of facial aesthetic procedures it is paramountfor all dental clinicians to have an understanding of this conditionBDD patients often request multiple aesthetic procedures butremain unsatisfied with their treatment results It is imperative forthe dental clinician to diagnose this condition prior to instigatingclinical treatment and to make an appropriate referral
FB Naini MSc BDS FDS FDSOrth MOrth Consultant Orthodontist St Georgersquos Hospital and Medical School London UK
DS Gill MSc BSc BDS FDS FDSOrth MOrth Consultant OrthodontistHonorary Senior Lecturer Eastman Dental Hospital London UK
Body Dysmorphic Disorder A Growing ProblemFarhad B Naini and Daljit S Gill
Key Words Body Dysmorphic Disorder Psychology Cosmetic Dentistry Facial Aesthetics copy Primary Dental Care 200815(2)62-64
Body Dysmorphic Disorder and Primary Dental Care
Figure 1 The Italian professor of psychiatry Enrico Morselli (1852-1929)coined the diagnostic category of lsquodysmorphophobiarsquo in 1891 although he made reference to an earlier paper from 1886 in which he began todiscuss the conceptThe term was introduced into English with the publication of Eugenio Tanzirsquos textbook in 1910
Primary Dental Care bull April 200862
have been listed (American PsychiatricAssociation)3 They are that1 There is a preoccupation with an
imagined or minimal defect in appear-ance If the defect is minimal theindividualrsquos concern is excessive
2 The preoccupation causes substantialemotional distress and impaired socialand occupational functioning
3 The preoccupation is not caused byother mental disorders
Although the perceived physical anom-aly may concern any part of the bodythe face is commonly involved Patientsmay have specific or vague concernsTheir preoccupation with a particularfeature may remain unchanged or theircomplaints may shift from one bodypart to another over time Althoughpatientsrsquo insight into the severity of theirconcerns is var iable they are oftendeeply convinced of the severity of theirdefect It is not possible for clinicianssimply to talk patients out of theirconcern
BDD usually commences in adoles-cence with a gradual onset5 Howeversudden onset may also occur particu-larly following major life events suchas the termination of a relationshipor leaving home6 Mild symptoms inadolescence may subside over time butmoderate to severe symptoms tend tofollow a more chronic path There isfrequent comorbidity in patients withBDD particularly with depressionsocial phobia substance abuse obsessivecompulsive disorder (OCD) and eatingdisorders7 The general dental practi-tioner is likely to be the first clinician toobserve the characteristic dental erosivepattern due to vomiting in patients witheating disorders
The nature of BDD is such that itvery much takes hold of the patientrsquoslife Significant social problems includ-ing social isolation and work-relatedproblems (due to avoidance of socialinteraction) result from a conviction thatthose around them consistently noticetheir lsquodefectrsquo Up to 50 of BDD patientsadmit to suicidal ideation8
There are few data on the prevalenceof BDD Figures from 07 to over 5
have been given with an equal sex inci-dence9 However the prevalence amongpatients seeking facial aesthetic treatmentmay well be higher10 People with BDDare often single or separated
DIAGNOSIS IN THE DENTAL SURGERY
The diagnosis of BDD is vital for clini-cians involved in any form of dentofacialappearance-altering treatment such asorthodontics orthognathic surgery oraesthetic dentistry Timely diagnosiswill enable appropriate referral to mentalhealthcare professionals either via thegeneral medical practitioner or possiblythrough a specialist hospital unit such asan orthodontic maxillofacial or cranio-facial unit with direct access to a clinicalpsychologist or liaison psychiatrist Thiswill ultimately avoid much stress forthe patient and the clinician and helpto avoid possible future medicolegalproblems
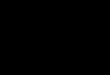
Diagnosis is essentially based on thepatient interview past medical historyand observation of recognised patterns ofbehaviour (Figure 2) There is no singlequestion that will disclose a diagnosis ofBDD Patients will initially be asked anopen question regarding the reason fortheir consultation and their concernsPatients with BDD are likely to haveexcessive concerns about a minor orimperceptible defect in their appearancePatients may be over-specific about aperceived appearance flaw but may alsosometimes be rather vague in theirdescription of a defect In addition a his-tory of lsquodoctor shoppingrsquo dissatisfactionwith previous clinicians and treatmentand unusually demanding behaviour arelsquored flagrsquo signs It is possible that patientsmay hide any previous psychiatric historyfrom clinicians for fear that it will pre-vent them from receiving treatmentAnother factor is that patients may wellblame their lsquodefectrsquo for lack of success inlife work or personal relationships Suchpatients are likely to have unrealisticexpectations that treatment will solve alltheir problems
It is important to ask patients howmuch time they spend thinking abouttheir defect and how long they spendlooking in a mirror per day Engaging inany such compulsive appearance-relatedbehaviour for more than one hour perday is a cause for concern2 Patients may
Patient interviewconsultation
bull Excessive concerns regarding aminor or imperceptible appearancedefect
bull Over-specific concerns often withthe patient bringing diagrams andpictures to demonstrate how theyshould be treated
bull Vague description of concerns (as opposed to over-specific)
bull Patient admits to chronic mirror-checking behaviour
bull Dissatisfaction with previous clinician(s)clinical treatment
bull lsquoDoctor-shoppingrsquo particularly ifprevious clinicians have refused toundertake treatment
bull Illogical desires such as that a clinical procedure will change theirlife job prospects or personal relationships
bull Unrealistic expectations of clinicaltreatment result
Past medical history
bull Previous history of psychiatric treat-ment particularly for depression
bull Anxiety disorders particularlyobsessive-compulsive disorder(OCD) and social phobia (avoidingsocial situations even being housebound)
bull History of substance abuse
bull History of eating disorders
Social and family history
bull Unemployed
bull Unmarrieddivorced andor livingalone
bull Family support does the patienthave a poor relationship with theirfamily
Recognised patterns of behaviour
bull Unusually demanding or suspiciousbehaviour
bull Frequent cancellation and rebookingof appointments
bull Camouflaging behaviour such ascovering the mouth with a hand or scarf
Figure 2 Indications and lsquogiveawayrsquo signs of body dysmorphic disorder
Primary Dental Care bull April 200863
FB Naini and DS Gill
also use camouflaging techniques suchas covering their mouth with their handor a scarf Frequent cancellation andrebooking of appointments and a sus-picious attitude should also alert theclinician
TO TREAT OR NOT TOTREATBDD is a psychiatric disorder thereforeany form of clinical treatment is likely toleave the patient unhappy often more sothan before treatment was instigatedPatients often find fault in the treatmentresult and may find new lsquodefectsrsquo Thereare situations in which treatment may beprovided when a minor defect actuallyexists but this must be undertakenjointly with the support of a clinicalpsychologist or psychiatrist Thereforethe overall recommendation is not toundertake clinical treatment of patientswith BDD11
INFORMING THE PATIENT
Patients should be informed that clinicaltreatment by the dental clinician wouldnot be beneficial for them in the longterm
It is important to inform patientswithout offending them It is also vitalfor clinicians not to allow patients to talkthem into providing treatment Patientsshould be informed in a polite andstraightforward manner and clinicians
should stress the fact that they are actingin the best interests of the patient Afterobtaining the patientrsquos consent referralto the general medical practitioner isadvisable and it will be his or her deci-sion as to whether or not subsequentrefer ral to a clinical psychologist orpsychiatrist is required
MANAGEMENT
People diagnosed with BDD should betreated by a clinical psychologist or psy-chiatrist with experience in managingthe disorder Having confirmed the diag-nosis treatment may be undertaken bypsychotherapy pharmacotherapy or acombination of the two
Cognitive-behavioural therapy in par-ticular has been shown to be effective inthe management of BDD Two methodsof cognitive-behavioural therapy spec-ifically have demonstrated beneficialresults1 Exposure therapy This deals with the
patientrsquos ability to lsquoexpose the defectrsquoin a social setting
2 Response preventionTechniques toprevent the patient from using estab-lished behaviour patterns such asmirror-checking and camouflagingbehaviour12
Pharmacotherapy may also be effective inthe management of BDD Selective sero-tonin reuptake inhibitors are currently thefirst-line medication helping to reduceobsessive-compulsive behaviour13
CONCLUSION
With the increased ability to undertakedental aesthetic and reconstructive pro-cedures in addition to the use of facialaesthetic procedures such as Botoxreg
(injections containing Clostridium botu-linum type A neurotoxin complex) anddermal fillers it is paramount for generaldental practitioners to have an under-standing of BDD
Clinical intervention without thesupport of a clinical psychologist or psy-chiatrist will often exacerbate a patientrsquossymptoms and lead to greater problemsThe challenge for dental clinicians istherefore to diagnose the condition priorto instigating clinical treatment
REFERENCES1 Phillips KA The Broken Mirror Understanding and Treating
Body Dysmorphic Disorder New York Oxford UniversityPress 200556
2 Veale D Boocock A Gournay K Dryden W Shah FWillson R et al Body dysmorphic disorder A survey offifty cases Br J Psychiatry 1996169196-201
3 American Psychiatric Association Diagnostic and StatisticalManual of Mental Disorders 4th ed Washington DC APA1994
4 Phillips KA Body dysmorphic disorder the distress ofimagined uglinessAm J Psychiatry 19911481138-49
5 Castle DJ Morkell D Imagined ugliness a symptom whichcan become a disorder Med J Aust 2000173205-7
6 Phillips KA Mernard W Fay C Weisberg R Demographiccharacteristics phenomenology comorbidity and familyhistory in 200 individuals with body dysmorphic disorderPsychosomatics 200546317-25
7 Neziroglu F Yaryura-Tobias JA A review of cognitivebehavioral and pharmacological treatment of body dys-morphic disorder Behav Modif 199721324-40
8 Veale D Advances in cognitive behavioural understandingof body dysmorphic disorder Body Image 20041113-25
9 Otto MW Wilhelm S Cohen LS Harlow BL Prevalenceof body dysmorphic disorder in a community sample ofwomen Am J Psychiatry 20011582061-3
10 Ishigooka J Iwao M Suzuki M Fukuyama Y Murasaki MMiura S Demographic features of patients seeking cos-metic surgery Psychiatry Clin Neurosci 199852283-7
11 Phillips KA Pagano ME Menard W Fay C Stout RLPredictors of remission from body dysmorphic disorder aprospective study J Nerv Ment Dis 2005193564-7
12 Veale D Gournay K Dryden W Boocock A Shah FWillson R et al Body dysmorphic disorder a cognitivebehavioural model and pilot randomised controlled trialBehav Res Ther 199634717-29
13 Phillips KA Dwight MM McElroy SL Efficacy and safety offluvoxamine in body dysmorphic disorder J Clin Psychiatry199859165-71
Correspondence FB NainiDepartment of Orthodontics
St Georgersquos Hospital and Medical SchoolLondon SW17 0QT
E-mail FarhadNainiyahoocouk
Primary Dental Care bull April 200864
CPD now available via FGDP(UK) aesthetic modules
The FGDP(UK) Advanced Certificate in Aesthetic Dentistry is being launched this April underthe direction of Professor Mike Mulcahy and Linda Greenwall and is available to dentists who hold amasters-level postgraduate qualification in a relevant disciplineThe following optional modules of thecourse will also be individually available to all registered GDPs who will be able to collect 12 hours of verifiable CPD as well as improving their skills in aesthetic dentistry
24 - 25 October 2008 Porcelain veneers14 -15 November 2008 Facial aesthetics30 -31 January 2009 Posterior aesthetic restorations24 -25 April 2009 Soft tissue management in the aesthetic zone13 -14 February 2009 Crown and bridge aesthetics15 -16 May 2009 Complete dental aesthetics
If you are interested in taking up the course or the optional modules please contact Amy Green on 020 7869 6774 or at agreenrcsengacuk
Body Dysmorphic Disorder A Growing Problem

have been listed (American PsychiatricAssociation)3 They are that1 There is a preoccupation with an
imagined or minimal defect in appear-ance If the defect is minimal theindividualrsquos concern is excessive
2 The preoccupation causes substantialemotional distress and impaired socialand occupational functioning
3 The preoccupation is not caused byother mental disorders
Although the perceived physical anom-aly may concern any part of the bodythe face is commonly involved Patientsmay have specific or vague concernsTheir preoccupation with a particularfeature may remain unchanged or theircomplaints may shift from one bodypart to another over time Althoughpatientsrsquo insight into the severity of theirconcerns is var iable they are oftendeeply convinced of the severity of theirdefect It is not possible for clinicianssimply to talk patients out of theirconcern
BDD usually commences in adoles-cence with a gradual onset5 Howeversudden onset may also occur particu-larly following major life events suchas the termination of a relationshipor leaving home6 Mild symptoms inadolescence may subside over time butmoderate to severe symptoms tend tofollow a more chronic path There isfrequent comorbidity in patients withBDD particularly with depressionsocial phobia substance abuse obsessivecompulsive disorder (OCD) and eatingdisorders7 The general dental practi-tioner is likely to be the first clinician toobserve the characteristic dental erosivepattern due to vomiting in patients witheating disorders
The nature of BDD is such that itvery much takes hold of the patientrsquoslife Significant social problems includ-ing social isolation and work-relatedproblems (due to avoidance of socialinteraction) result from a conviction thatthose around them consistently noticetheir lsquodefectrsquo Up to 50 of BDD patientsadmit to suicidal ideation8
There are few data on the prevalenceof BDD Figures from 07 to over 5
have been given with an equal sex inci-dence9 However the prevalence amongpatients seeking facial aesthetic treatmentmay well be higher10 People with BDDare often single or separated
DIAGNOSIS IN THE DENTAL SURGERY
The diagnosis of BDD is vital for clini-cians involved in any form of dentofacialappearance-altering treatment such asorthodontics orthognathic surgery oraesthetic dentistry Timely diagnosiswill enable appropriate referral to mentalhealthcare professionals either via thegeneral medical practitioner or possiblythrough a specialist hospital unit such asan orthodontic maxillofacial or cranio-facial unit with direct access to a clinicalpsychologist or liaison psychiatrist Thiswill ultimately avoid much stress forthe patient and the clinician and helpto avoid possible future medicolegalproblems
Diagnosis is essentially based on thepatient interview past medical historyand observation of recognised patterns ofbehaviour (Figure 2) There is no singlequestion that will disclose a diagnosis ofBDD Patients will initially be asked anopen question regarding the reason fortheir consultation and their concernsPatients with BDD are likely to haveexcessive concerns about a minor orimperceptible defect in their appearancePatients may be over-specific about aperceived appearance flaw but may alsosometimes be rather vague in theirdescription of a defect In addition a his-tory of lsquodoctor shoppingrsquo dissatisfactionwith previous clinicians and treatmentand unusually demanding behaviour arelsquored flagrsquo signs It is possible that patientsmay hide any previous psychiatric historyfrom clinicians for fear that it will pre-vent them from receiving treatmentAnother factor is that patients may wellblame their lsquodefectrsquo for lack of success inlife work or personal relationships Suchpatients are likely to have unrealisticexpectations that treatment will solve alltheir problems
It is important to ask patients howmuch time they spend thinking abouttheir defect and how long they spendlooking in a mirror per day Engaging inany such compulsive appearance-relatedbehaviour for more than one hour perday is a cause for concern2 Patients may
Patient interviewconsultation
bull Excessive concerns regarding aminor or imperceptible appearancedefect
bull Over-specific concerns often withthe patient bringing diagrams andpictures to demonstrate how theyshould be treated
bull Vague description of concerns (as opposed to over-specific)
bull Patient admits to chronic mirror-checking behaviour
bull Dissatisfaction with previous clinician(s)clinical treatment
bull lsquoDoctor-shoppingrsquo particularly ifprevious clinicians have refused toundertake treatment
bull Illogical desires such as that a clinical procedure will change theirlife job prospects or personal relationships
bull Unrealistic expectations of clinicaltreatment result
Past medical history
bull Previous history of psychiatric treat-ment particularly for depression
bull Anxiety disorders particularlyobsessive-compulsive disorder(OCD) and social phobia (avoidingsocial situations even being housebound)
bull History of substance abuse
bull History of eating disorders
Social and family history
bull Unemployed
bull Unmarrieddivorced andor livingalone
bull Family support does the patienthave a poor relationship with theirfamily
Recognised patterns of behaviour
bull Unusually demanding or suspiciousbehaviour
bull Frequent cancellation and rebookingof appointments
bull Camouflaging behaviour such ascovering the mouth with a hand or scarf
Figure 2 Indications and lsquogiveawayrsquo signs of body dysmorphic disorder
Primary Dental Care bull April 200863
FB Naini and DS Gill
also use camouflaging techniques suchas covering their mouth with their handor a scarf Frequent cancellation andrebooking of appointments and a sus-picious attitude should also alert theclinician
TO TREAT OR NOT TOTREATBDD is a psychiatric disorder thereforeany form of clinical treatment is likely toleave the patient unhappy often more sothan before treatment was instigatedPatients often find fault in the treatmentresult and may find new lsquodefectsrsquo Thereare situations in which treatment may beprovided when a minor defect actuallyexists but this must be undertakenjointly with the support of a clinicalpsychologist or psychiatrist Thereforethe overall recommendation is not toundertake clinical treatment of patientswith BDD11
INFORMING THE PATIENT
Patients should be informed that clinicaltreatment by the dental clinician wouldnot be beneficial for them in the longterm
It is important to inform patientswithout offending them It is also vitalfor clinicians not to allow patients to talkthem into providing treatment Patientsshould be informed in a polite andstraightforward manner and clinicians
should stress the fact that they are actingin the best interests of the patient Afterobtaining the patientrsquos consent referralto the general medical practitioner isadvisable and it will be his or her deci-sion as to whether or not subsequentrefer ral to a clinical psychologist orpsychiatrist is required
MANAGEMENT
People diagnosed with BDD should betreated by a clinical psychologist or psy-chiatrist with experience in managingthe disorder Having confirmed the diag-nosis treatment may be undertaken bypsychotherapy pharmacotherapy or acombination of the two
Cognitive-behavioural therapy in par-ticular has been shown to be effective inthe management of BDD Two methodsof cognitive-behavioural therapy spec-ifically have demonstrated beneficialresults1 Exposure therapy This deals with the
patientrsquos ability to lsquoexpose the defectrsquoin a social setting
2 Response preventionTechniques toprevent the patient from using estab-lished behaviour patterns such asmirror-checking and camouflagingbehaviour12
Pharmacotherapy may also be effective inthe management of BDD Selective sero-tonin reuptake inhibitors are currently thefirst-line medication helping to reduceobsessive-compulsive behaviour13
CONCLUSION
With the increased ability to undertakedental aesthetic and reconstructive pro-cedures in addition to the use of facialaesthetic procedures such as Botoxreg
(injections containing Clostridium botu-linum type A neurotoxin complex) anddermal fillers it is paramount for generaldental practitioners to have an under-standing of BDD
Clinical intervention without thesupport of a clinical psychologist or psy-chiatrist will often exacerbate a patientrsquossymptoms and lead to greater problemsThe challenge for dental clinicians istherefore to diagnose the condition priorto instigating clinical treatment
REFERENCES1 Phillips KA The Broken Mirror Understanding and Treating
Body Dysmorphic Disorder New York Oxford UniversityPress 200556
2 Veale D Boocock A Gournay K Dryden W Shah FWillson R et al Body dysmorphic disorder A survey offifty cases Br J Psychiatry 1996169196-201
3 American Psychiatric Association Diagnostic and StatisticalManual of Mental Disorders 4th ed Washington DC APA1994
4 Phillips KA Body dysmorphic disorder the distress ofimagined uglinessAm J Psychiatry 19911481138-49
5 Castle DJ Morkell D Imagined ugliness a symptom whichcan become a disorder Med J Aust 2000173205-7
6 Phillips KA Mernard W Fay C Weisberg R Demographiccharacteristics phenomenology comorbidity and familyhistory in 200 individuals with body dysmorphic disorderPsychosomatics 200546317-25
7 Neziroglu F Yaryura-Tobias JA A review of cognitivebehavioral and pharmacological treatment of body dys-morphic disorder Behav Modif 199721324-40
8 Veale D Advances in cognitive behavioural understandingof body dysmorphic disorder Body Image 20041113-25
9 Otto MW Wilhelm S Cohen LS Harlow BL Prevalenceof body dysmorphic disorder in a community sample ofwomen Am J Psychiatry 20011582061-3
10 Ishigooka J Iwao M Suzuki M Fukuyama Y Murasaki MMiura S Demographic features of patients seeking cos-metic surgery Psychiatry Clin Neurosci 199852283-7
11 Phillips KA Pagano ME Menard W Fay C Stout RLPredictors of remission from body dysmorphic disorder aprospective study J Nerv Ment Dis 2005193564-7
12 Veale D Gournay K Dryden W Boocock A Shah FWillson R et al Body dysmorphic disorder a cognitivebehavioural model and pilot randomised controlled trialBehav Res Ther 199634717-29
13 Phillips KA Dwight MM McElroy SL Efficacy and safety offluvoxamine in body dysmorphic disorder J Clin Psychiatry199859165-71
Correspondence FB NainiDepartment of Orthodontics
St Georgersquos Hospital and Medical SchoolLondon SW17 0QT
E-mail FarhadNainiyahoocouk
Primary Dental Care bull April 200864
CPD now available via FGDP(UK) aesthetic modules
The FGDP(UK) Advanced Certificate in Aesthetic Dentistry is being launched this April underthe direction of Professor Mike Mulcahy and Linda Greenwall and is available to dentists who hold amasters-level postgraduate qualification in a relevant disciplineThe following optional modules of thecourse will also be individually available to all registered GDPs who will be able to collect 12 hours of verifiable CPD as well as improving their skills in aesthetic dentistry
24 - 25 October 2008 Porcelain veneers14 -15 November 2008 Facial aesthetics30 -31 January 2009 Posterior aesthetic restorations24 -25 April 2009 Soft tissue management in the aesthetic zone13 -14 February 2009 Crown and bridge aesthetics15 -16 May 2009 Complete dental aesthetics
If you are interested in taking up the course or the optional modules please contact Amy Green on 020 7869 6774 or at agreenrcsengacuk
Body Dysmorphic Disorder A Growing Problem

also use camouflaging techniques suchas covering their mouth with their handor a scarf Frequent cancellation andrebooking of appointments and a sus-picious attitude should also alert theclinician
TO TREAT OR NOT TOTREATBDD is a psychiatric disorder thereforeany form of clinical treatment is likely toleave the patient unhappy often more sothan before treatment was instigatedPatients often find fault in the treatmentresult and may find new lsquodefectsrsquo Thereare situations in which treatment may beprovided when a minor defect actuallyexists but this must be undertakenjointly with the support of a clinicalpsychologist or psychiatrist Thereforethe overall recommendation is not toundertake clinical treatment of patientswith BDD11
INFORMING THE PATIENT
Patients should be informed that clinicaltreatment by the dental clinician wouldnot be beneficial for them in the longterm
It is important to inform patientswithout offending them It is also vitalfor clinicians not to allow patients to talkthem into providing treatment Patientsshould be informed in a polite andstraightforward manner and clinicians
should stress the fact that they are actingin the best interests of the patient Afterobtaining the patientrsquos consent referralto the general medical practitioner isadvisable and it will be his or her deci-sion as to whether or not subsequentrefer ral to a clinical psychologist orpsychiatrist is required
MANAGEMENT
People diagnosed with BDD should betreated by a clinical psychologist or psy-chiatrist with experience in managingthe disorder Having confirmed the diag-nosis treatment may be undertaken bypsychotherapy pharmacotherapy or acombination of the two
Cognitive-behavioural therapy in par-ticular has been shown to be effective inthe management of BDD Two methodsof cognitive-behavioural therapy spec-ifically have demonstrated beneficialresults1 Exposure therapy This deals with the
patientrsquos ability to lsquoexpose the defectrsquoin a social setting
2 Response preventionTechniques toprevent the patient from using estab-lished behaviour patterns such asmirror-checking and camouflagingbehaviour12
Pharmacotherapy may also be effective inthe management of BDD Selective sero-tonin reuptake inhibitors are currently thefirst-line medication helping to reduceobsessive-compulsive behaviour13
CONCLUSION
With the increased ability to undertakedental aesthetic and reconstructive pro-cedures in addition to the use of facialaesthetic procedures such as Botoxreg
(injections containing Clostridium botu-linum type A neurotoxin complex) anddermal fillers it is paramount for generaldental practitioners to have an under-standing of BDD
Clinical intervention without thesupport of a clinical psychologist or psy-chiatrist will often exacerbate a patientrsquossymptoms and lead to greater problemsThe challenge for dental clinicians istherefore to diagnose the condition priorto instigating clinical treatment
REFERENCES1 Phillips KA The Broken Mirror Understanding and Treating
Body Dysmorphic Disorder New York Oxford UniversityPress 200556
2 Veale D Boocock A Gournay K Dryden W Shah FWillson R et al Body dysmorphic disorder A survey offifty cases Br J Psychiatry 1996169196-201
3 American Psychiatric Association Diagnostic and StatisticalManual of Mental Disorders 4th ed Washington DC APA1994
4 Phillips KA Body dysmorphic disorder the distress ofimagined uglinessAm J Psychiatry 19911481138-49
5 Castle DJ Morkell D Imagined ugliness a symptom whichcan become a disorder Med J Aust 2000173205-7
6 Phillips KA Mernard W Fay C Weisberg R Demographiccharacteristics phenomenology comorbidity and familyhistory in 200 individuals with body dysmorphic disorderPsychosomatics 200546317-25
7 Neziroglu F Yaryura-Tobias JA A review of cognitivebehavioral and pharmacological treatment of body dys-morphic disorder Behav Modif 199721324-40
8 Veale D Advances in cognitive behavioural understandingof body dysmorphic disorder Body Image 20041113-25
9 Otto MW Wilhelm S Cohen LS Harlow BL Prevalenceof body dysmorphic disorder in a community sample ofwomen Am J Psychiatry 20011582061-3
10 Ishigooka J Iwao M Suzuki M Fukuyama Y Murasaki MMiura S Demographic features of patients seeking cos-metic surgery Psychiatry Clin Neurosci 199852283-7
11 Phillips KA Pagano ME Menard W Fay C Stout RLPredictors of remission from body dysmorphic disorder aprospective study J Nerv Ment Dis 2005193564-7
12 Veale D Gournay K Dryden W Boocock A Shah FWillson R et al Body dysmorphic disorder a cognitivebehavioural model and pilot randomised controlled trialBehav Res Ther 199634717-29
13 Phillips KA Dwight MM McElroy SL Efficacy and safety offluvoxamine in body dysmorphic disorder J Clin Psychiatry199859165-71
Correspondence FB NainiDepartment of Orthodontics
St Georgersquos Hospital and Medical SchoolLondon SW17 0QT
E-mail FarhadNainiyahoocouk
Primary Dental Care bull April 200864
CPD now available via FGDP(UK) aesthetic modules
The FGDP(UK) Advanced Certificate in Aesthetic Dentistry is being launched this April underthe direction of Professor Mike Mulcahy and Linda Greenwall and is available to dentists who hold amasters-level postgraduate qualification in a relevant disciplineThe following optional modules of thecourse will also be individually available to all registered GDPs who will be able to collect 12 hours of verifiable CPD as well as improving their skills in aesthetic dentistry
24 - 25 October 2008 Porcelain veneers14 -15 November 2008 Facial aesthetics30 -31 January 2009 Posterior aesthetic restorations24 -25 April 2009 Soft tissue management in the aesthetic zone13 -14 February 2009 Crown and bridge aesthetics15 -16 May 2009 Complete dental aesthetics
If you are interested in taking up the course or the optional modules please contact Amy Green on 020 7869 6774 or at agreenrcsengacuk
Body Dysmorphic Disorder A Growing Problem