Embed Size (px)
Citation preview

1638 Obesity Surgery 16 2006 copy FD-Communications Inc
Obesity Surgery 16 1638-1644
Background From Nov 2001 to Mar 2006 176 patientsunderwent body contouring plastic surgery after priorbiliopancreatic diversion (BPD) Weight loss had var-ied from 30-100 kg The plastic surgery targeted thearms (24 patients) breast (58) abdomen (62) andthighs (20) plus torsoplasty (12)
Methods BPD is a ldquonon-cosmeticrdquo bariatric opera-tion which results in malabsorption and subsequentmajor weight loss within 12 to 18 months The typicalldquoemptyrdquo aspect of the slimmed areas directed oursurgical choices to specific techniques brachio-plasty reduction mammaplasty andor mastopexy(with or without prosthesis or ldquoself-prosthesisrdquo tech-nique) thigh-lift abdominoplasty and torsoplasty Wedo not consider any liposuction technique suitablefor this kind of patient because of the specific histo-logical changes caused by BPD
Results The metabolic discrepancies followingBPD affect postoperative management of thesepatients A higher incidence of complications hasbeen reported of both systemic and local nature thelocal ones common in the abdominal wall convincedus to perform an arteriographic study preoperativelyto check anatomical alterations following the BPD
Conclusions Although the characteristics of BPDpatients limit the choices we are satisfied with theresults of cosmetic correction and quality of life Allthe patients without exception noted a high rate ofpositive thinking and have undergone further body-contouring surgery (or plan to do so)
Key words Plastic surgery morbid obesity weight lossbariatric surgery biliopancreatic diversion
Introduction
This paper is intended to serve as an overview to thisparticular branch of body contouring after a specificbariatric surgical technique Since 1976Scopinarorsquos biliopancreatic diversion (BPD) hasevolved as a bariatric operation12 BPD has made amalabsorptive approach acceptable and preferableNormalization of serum glucose and cholesterol atotally free diet mortality lt05 and the extremeflexibility of the technique are advantages
Clinical Consequences
Significant advantages of BPD are 1) the extremeweight loss (80-100 kg) within an average timeinterval of 12-18 months 2) normalization of hyper-glycemia and hypercholesterolemia However somechallenging complications must be avoided 1) Fe++
malabsorption with sideropenic anemia 2) Ca++
malabsorption with bone demineralization 3) in 5of patients protein malnutrition
Morphological Consequences
The clearly evidenced disadvantage of the operationwas the inefficacy of the soft tissue scar retractiondue to histological alterations causing an overallnon-esthetic aspect The inelastic and atrophic tis-sues result in deep folds and creases The mainaspects are large dermo-adiposal folds in the armsabdomen and inner thighs and medium-to-severebreast ptosis in women
Overview
Body Contouring after Biliopancreatic Diversion
Franco Migliori Cristina Rosati Gabriele DrsquoAlessandro Gian GiacomoSerra Cervetti
Plastic Surgery and Burn Unit San Martino University Hospital Genova Italy (Director FrancoMigliori MD)
Presented at the Second Congress of the IFSO-EuropeanChapter Lyon France April 28 2006
Reprint requests to Franco Migliori MD Direttore UO diChirurgia Plastica e Centro Grandi Ustionati 16132 GenovaItaly E-mail francomigliorihsanmartinoit
December 112306 123 PM Page 1638
Anatomo-Surgical Consequences
The preoperative and intraoperative challenge ofplastic surgery after BPD has been the reduced vas-cular perfusion of the tissue mainly in the dermiswhich appears thinner and in the fat which appearshypotrophic ldquopalerdquo or even ldquograyrdquo The presence ofmedial scars in the abdominal wall causes reducedelasticity and a compromised dermal plexus bothcausing increased specific complications
Histological Consequences
A histologic study on the dermis and fat has been per-formed compared with dermis and fat of healthy sub-jects The post BPD fat has demonstrated the presenceof collapsed adipocytes with thicker membranesprominent nuclei (usually not visible) and thickenedintracellular fibrous septa In the dermis the main evi-denced alterations have been the thickening of thefibrous net and the hypertrophy of the vascular net Areduction of elastic fibers is supposed but results ofhistochemical EM study are awaited
Materials and Methods
From Nov 2001 to Mar 2006 176 patients (166female 10 male) have been operated 24 branchio-plasties 58 mastoplasties 62 abdominoplasties 20thigh-lifts and 12 torsoplasties Due to the highrisk of complications in these patients we pre-deposit autologous blood in all cases (one or twounits) In more complicated procedures (like torso-plasty) we verify the availability of a postopera-tive intensive care bed (for 1-2 nights) We performantithrombotic prophylaxis with LMW heparin4000 IU 12 hours before surgery (continued every12 hours for 2 weeks) and compressive leg band-aging Hemoglobin level is checked immediatelyafter surgery 6 hours after surgery and every dayfor 2 weeks to verify the need for auto-hemotrans-fusion We have slightly prolonged the mainte-nance of the drains (4-5 days) we remove thedrains only when 24-hour drainage is lt100 cc Therecovery is not less than 6-7 days and up to 15-20days for more complex techniques (torsoplasty)
General Consideration in Choice ofSurgical Technique
As usually happens in plastic surgery procedures thesurgeon needs to find the right compromise betweenmaximal reduction of excess tissue which couldachieve a non-esthetic result with the need on theother hand for more reduction of scar length3 Theanatomical-surgical and histological features confer tothese tissues an ldquoanergic behaviorrdquo meaning a poor orabsent scar retraction Because these tissues have noretraction ability the surgical techniques have toremove all excessive tissue Thus techniques such asliposuction where the results depend on scar retrac-tion cannot be utilized except in rare selected cases
Surgical Techniques
BrachioplastyThe esthetic defects of the upper limbs have beenclassified into 4 types by Strauch4 The defects fol-lowing BPD mainly belong to the 4th type and insome cases to the 3rd The interested areas aremainly II and III (axilla)4 After an extensive inter-national review5 we are strongly convinced that thelinear excision (with possible T extension in theaxilla) performed within the medial brachial foldgives the best esthetic result (Figure 1)
Thigh-LiftWhile pursuing the aim of shortening the scars wehave gradually utilized more and more excisionsfollowing the suggestions of Le Louarn and Pascal6
To reduce possible lymphatic drainage complica-tions we have gradually reduced the underminingextension choosing a full-thickness ldquoen blockrdquoremoval of excessive tissue The preoperative draw-ing of the planned procedure is performed withpatients standing and the legs abducted Theremoval of excess tissue is performed in the ldquogyne-cologic positionrdquo the suturing is performed with thelegs alternatively abducted by anchoring togetherthe dermis and superficial Colles fascial system(according to Lockwood7) (Figure 2)
MastoplastyThe main breast problem after BPD weight loss is pto-sis which is seldom of high degree (Nipple AreolaComplex [NAC] distance 28-35 ndash normal values 18-
Body Contouring after BPD ndash Overview
Obesity Surgery 16 2006 1639
December 112306 123 PM Page 1639
20) and glandular hypotrophy These two defects arefrequently present together Very rarely have weneeded to reduce the gland volume In minor ptosis(NAC lift of about 4-5 cm) we utilize round blocktechnique added if necessary with an alloplasticimplant (Figure 3-1) or the self-prosthesis techniqueof Ribeiro8 (Figure 3-2) In a major ptosis we utilizethe vertical technique or L technique9 eventually sup-plemented by a prosthesis or self-prosthesis
AbdominoplastyAs a consequence of the above-described anatomo-surgical modifications and of the high percentage ofpotential complications we are convinced that theright abdominoplasty technique for this kind ofpatient should be quick and safe10 (Figure 4)Therefore we usually utilize the ldquovest over pantsrdquotechnique (Planas 1978) with an inverted V exci-sion providing higher vascular safety11
Migliori et al
1640 Obesity Surgery 16 2006
Figure 1 A Before brachioplasty B After brachioplasty
A B
Figure 2 A Before thigh-lift B After thigh-lift
A B
December 112306 123 PM Page 1640
Body Contouring after BPD ndash Overview
Obesity Surgery 16 2006 1641
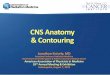
Figure 3-1 A Mastoplasty case 1 before B Mastoplasty case 1 after (mastopexy with silicone implants)
A B
Figure 3-2 A Mastoplasty case 2 before B Mastoplasty case 2 after (mastopexy with self-prosthesis)
A B
Figure 4 A Before abdominoplasty B After abdominoplasty
A B
December 112306 123 PM Page 1641
Migliori et al
1642 Obesity Surgery 16 2006
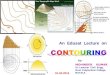
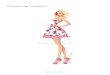
Figure 5 Torsoplasty A front B back (with island flaps for buttocks emphasized)
A B
Figure 6 Torsoplasty results A Back before B Back after
A B
C Side before D Side after
C D
December 112306 123 PM Page 1642
The high incidence of abdominal wall complica-tions1213 in this particular group of patients com-pared with ldquonon-BPDrdquo patients and the review ofanatomical studies1415 has suggested to us toincrease the research of causes by arteriographicstudy of the epigastric vessels In five studied casesno reliable modifications have been foundTherefore without a demonstrated dysmetabolicpathogenesis secondary to BPD the only certaincause responsible for almost 70 of trophic com-plications following abdominoplasty is the presenceof previous scars In more recent BPD cases oper-ated by the laparoscopic approach (with very shortabdominal scars) the percentage of complicationshas significantly decreased16
Torsoplasty
In patients with more massive weight loss (70-100kg) it is possible to observe a particular trunk non-esthetism the so-called ldquosharpei profilerdquo (Sharpei isan Asian dog characterized by redundant inelasticskin) In this kind of ldquotridimensionalrdquo defect aldquobidimensionalrdquo technique like abdominoplasty isnot adequate1718 In these cases the correction offlanks and back profile is necessary as well as of theptosis of the buttocks and the external thighs
In these patients we perform torsoplasty asdescribed by Lockwood19 and Pascal-LeLouarn20
supplemented by a de-epithelilized island flap inorder to emphasize the profile (Figure 5) We com-mence with the excision of the redundant tissue firston the back side then on the lateral aspect andfinally on the abdominal wall The excisions areconducted in serial little segments in order toreduce incarcerated blood losses as much as possi-ble The variety and complexity of correctionobtained by torsoplasty in a single surgical time(posterior and lateral lift abdominal wall flatteninggreat removal of excess tissue hernia repair) givesan improvement of the entire ldquosilhouetterdquo which isnot achievable with any other technique (Figure 6)
Conclusions
Great ldquopositiverdquo thinking of these patients towardsbody contouring creates enormous expectations for
improvement in quality of life (similar to the expecta-tions which motivated these patients toward bariatricsurgery)21 Of these operated patients 99 declarethemselves completely satisfied with the obtainedresults and go on to further body contouring Thesekinds of results are not achievable by bariatric surgeryalone andor by eating behavior normalization22
On average we perform 2-3 operations on eachpatient The main points of patient satisfaction arerdquobody imagerdquo greatly improved self-esteem recov-ery improvement in life relationships and sexuallife resumption or improvement A body uneasinesstest study is in progress in 5 different groups ofthese patients
References
1 Scopinaro N Gianetta E Pandolfo N et alBiliopancreatic bypass Proposal and preliminaryexperimental study of a new type of operation for thefunctional surgical treatment of obesity Minerva Chir1976 31 560-6
2 Scopinaro N Adami GF Marinari GM et alBiliopancreatic diversion World J Surg 1998 22936-46
3 Baroudi R Body sculpturing Clin Plast Surg 1984111 419-43
4 Strauch B Greenspun D Levine J et al A techniqueof brachioplasty Plast Reconstr Surg 2004 1131044-8 discussion 1049
5 Guerrero-Santos J Brachioplasty Aesthetic PlastSurg 1979 3 1-4
6 Le Louarn C Pascal JF The concentric medial thigh-lift Aesthetic Plast Surg 2004 28 20-3
7 Lockwood TE Fascial anchoring technique in medialthigh lifts Plast Reconstr Surg 1988 82 299-304
8 Ribeiro L Canzl W Buss A et al Tuberous breast anew approach 1998 101 42-50
9 De Longis E Mastoplastica riduttiva Mastopessi Ladermopessi Colosseum Edition 1997
10Matarasso A Abdominoplasty In Achauer BMEriksson E Guyuron B et al eds Plastic SurgeryIndications Operations and Outcomes Vol V StLouis Mosby 2000 2783
11Planas J The ldquovest over pantsrdquo abdominoplasty PlastReconstr Surg 1978 61 694-700
12Nurkim MV et al Incidence of hematoma and seromain abdominoplasty with and without the use of drainsRev Soc Bras Cir Plast 2002 17 69-74 (abstract)
Body Contouring after BPD ndash Overview
Obesity Surgery 16 2006 1643
December 112306 123 PM Page 1643
Migliori et al
1644 Obesity Surgery 16 2006
13van Uchelen JH Werker PMN Kon MComplications of abdominoplasty in 86 patients PlastReconcstr Surg 2001 107 1869-73
14Huger WE Jr The anatomic rationale for abdominallipectomy Ann Surg 1979 45 612-7
15Hester TR Jr Nahai F Beegle PE et al Blood supplyof the abdomen revisited with emphasis on the super-ficial inferior epigastric artery Plast Reconstr Surg1984 47 657-70
16Scopinaro N Marinari GM Camerini GLaparoscopic standard biliopancreatic diversiontechnique and preliminary results Obes Surg 200212 362-5
17Matarasso A Evaluation and classification in abdom-inal contour surgery in abdominoplasty Oper TechPlast Surg 1996 3 7-11
18Matarasso A Liposuction as an adjunct to full
abdominoplasty revisited Plast Reconstr Surg 2000106 1197-202 discussion 1203-5
19 Lockwood TE Lower body lift with superficial fascialsystem suspension Plast Reconstr Surg 1993 92 1112-6
20Pascal JF Le Louarn C Remodelling body-lift withhigh lateral tension Aesthetic Plast Surg 2002 26223-30
21Bolton M Pruzinsky T Cash T et al Measuring out-comes in plastic surgery body image and quality oflife in abdominoplasty patients Plast Reconstr Surg2003 112 619-25
22Adami G Bauer B Gandolfo P et al Body image inearly-onset obese patients Eat Weight Disord 19972 87-93
(Received June 22 2006 accepted August 3 2006)
December 112306 123 PM Page 1644

Anatomo-Surgical Consequences
The preoperative and intraoperative challenge ofplastic surgery after BPD has been the reduced vas-cular perfusion of the tissue mainly in the dermiswhich appears thinner and in the fat which appearshypotrophic ldquopalerdquo or even ldquograyrdquo The presence ofmedial scars in the abdominal wall causes reducedelasticity and a compromised dermal plexus bothcausing increased specific complications
Histological Consequences
A histologic study on the dermis and fat has been per-formed compared with dermis and fat of healthy sub-jects The post BPD fat has demonstrated the presenceof collapsed adipocytes with thicker membranesprominent nuclei (usually not visible) and thickenedintracellular fibrous septa In the dermis the main evi-denced alterations have been the thickening of thefibrous net and the hypertrophy of the vascular net Areduction of elastic fibers is supposed but results ofhistochemical EM study are awaited
Materials and Methods
From Nov 2001 to Mar 2006 176 patients (166female 10 male) have been operated 24 branchio-plasties 58 mastoplasties 62 abdominoplasties 20thigh-lifts and 12 torsoplasties Due to the highrisk of complications in these patients we pre-deposit autologous blood in all cases (one or twounits) In more complicated procedures (like torso-plasty) we verify the availability of a postopera-tive intensive care bed (for 1-2 nights) We performantithrombotic prophylaxis with LMW heparin4000 IU 12 hours before surgery (continued every12 hours for 2 weeks) and compressive leg band-aging Hemoglobin level is checked immediatelyafter surgery 6 hours after surgery and every dayfor 2 weeks to verify the need for auto-hemotrans-fusion We have slightly prolonged the mainte-nance of the drains (4-5 days) we remove thedrains only when 24-hour drainage is lt100 cc Therecovery is not less than 6-7 days and up to 15-20days for more complex techniques (torsoplasty)
General Consideration in Choice ofSurgical Technique
As usually happens in plastic surgery procedures thesurgeon needs to find the right compromise betweenmaximal reduction of excess tissue which couldachieve a non-esthetic result with the need on theother hand for more reduction of scar length3 Theanatomical-surgical and histological features confer tothese tissues an ldquoanergic behaviorrdquo meaning a poor orabsent scar retraction Because these tissues have noretraction ability the surgical techniques have toremove all excessive tissue Thus techniques such asliposuction where the results depend on scar retrac-tion cannot be utilized except in rare selected cases
Surgical Techniques
BrachioplastyThe esthetic defects of the upper limbs have beenclassified into 4 types by Strauch4 The defects fol-lowing BPD mainly belong to the 4th type and insome cases to the 3rd The interested areas aremainly II and III (axilla)4 After an extensive inter-national review5 we are strongly convinced that thelinear excision (with possible T extension in theaxilla) performed within the medial brachial foldgives the best esthetic result (Figure 1)
Thigh-LiftWhile pursuing the aim of shortening the scars wehave gradually utilized more and more excisionsfollowing the suggestions of Le Louarn and Pascal6
To reduce possible lymphatic drainage complica-tions we have gradually reduced the underminingextension choosing a full-thickness ldquoen blockrdquoremoval of excessive tissue The preoperative draw-ing of the planned procedure is performed withpatients standing and the legs abducted Theremoval of excess tissue is performed in the ldquogyne-cologic positionrdquo the suturing is performed with thelegs alternatively abducted by anchoring togetherthe dermis and superficial Colles fascial system(according to Lockwood7) (Figure 2)
MastoplastyThe main breast problem after BPD weight loss is pto-sis which is seldom of high degree (Nipple AreolaComplex [NAC] distance 28-35 ndash normal values 18-
Body Contouring after BPD ndash Overview
Obesity Surgery 16 2006 1639
December 112306 123 PM Page 1639
20) and glandular hypotrophy These two defects arefrequently present together Very rarely have weneeded to reduce the gland volume In minor ptosis(NAC lift of about 4-5 cm) we utilize round blocktechnique added if necessary with an alloplasticimplant (Figure 3-1) or the self-prosthesis techniqueof Ribeiro8 (Figure 3-2) In a major ptosis we utilizethe vertical technique or L technique9 eventually sup-plemented by a prosthesis or self-prosthesis
AbdominoplastyAs a consequence of the above-described anatomo-surgical modifications and of the high percentage ofpotential complications we are convinced that theright abdominoplasty technique for this kind ofpatient should be quick and safe10 (Figure 4)Therefore we usually utilize the ldquovest over pantsrdquotechnique (Planas 1978) with an inverted V exci-sion providing higher vascular safety11
Migliori et al
1640 Obesity Surgery 16 2006
Figure 1 A Before brachioplasty B After brachioplasty
A B
Figure 2 A Before thigh-lift B After thigh-lift
A B
December 112306 123 PM Page 1640
Body Contouring after BPD ndash Overview
Obesity Surgery 16 2006 1641
Figure 3-1 A Mastoplasty case 1 before B Mastoplasty case 1 after (mastopexy with silicone implants)
A B
Figure 3-2 A Mastoplasty case 2 before B Mastoplasty case 2 after (mastopexy with self-prosthesis)
A B
Figure 4 A Before abdominoplasty B After abdominoplasty
A B
December 112306 123 PM Page 1641
Migliori et al
1642 Obesity Surgery 16 2006
Figure 5 Torsoplasty A front B back (with island flaps for buttocks emphasized)
A B
Figure 6 Torsoplasty results A Back before B Back after
A B
C Side before D Side after
C D
December 112306 123 PM Page 1642
The high incidence of abdominal wall complica-tions1213 in this particular group of patients com-pared with ldquonon-BPDrdquo patients and the review ofanatomical studies1415 has suggested to us toincrease the research of causes by arteriographicstudy of the epigastric vessels In five studied casesno reliable modifications have been foundTherefore without a demonstrated dysmetabolicpathogenesis secondary to BPD the only certaincause responsible for almost 70 of trophic com-plications following abdominoplasty is the presenceof previous scars In more recent BPD cases oper-ated by the laparoscopic approach (with very shortabdominal scars) the percentage of complicationshas significantly decreased16
Torsoplasty
In patients with more massive weight loss (70-100kg) it is possible to observe a particular trunk non-esthetism the so-called ldquosharpei profilerdquo (Sharpei isan Asian dog characterized by redundant inelasticskin) In this kind of ldquotridimensionalrdquo defect aldquobidimensionalrdquo technique like abdominoplasty isnot adequate1718 In these cases the correction offlanks and back profile is necessary as well as of theptosis of the buttocks and the external thighs
In these patients we perform torsoplasty asdescribed by Lockwood19 and Pascal-LeLouarn20
supplemented by a de-epithelilized island flap inorder to emphasize the profile (Figure 5) We com-mence with the excision of the redundant tissue firston the back side then on the lateral aspect andfinally on the abdominal wall The excisions areconducted in serial little segments in order toreduce incarcerated blood losses as much as possi-ble The variety and complexity of correctionobtained by torsoplasty in a single surgical time(posterior and lateral lift abdominal wall flatteninggreat removal of excess tissue hernia repair) givesan improvement of the entire ldquosilhouetterdquo which isnot achievable with any other technique (Figure 6)
Conclusions
Great ldquopositiverdquo thinking of these patients towardsbody contouring creates enormous expectations for
improvement in quality of life (similar to the expecta-tions which motivated these patients toward bariatricsurgery)21 Of these operated patients 99 declarethemselves completely satisfied with the obtainedresults and go on to further body contouring Thesekinds of results are not achievable by bariatric surgeryalone andor by eating behavior normalization22
On average we perform 2-3 operations on eachpatient The main points of patient satisfaction arerdquobody imagerdquo greatly improved self-esteem recov-ery improvement in life relationships and sexuallife resumption or improvement A body uneasinesstest study is in progress in 5 different groups ofthese patients
References
1 Scopinaro N Gianetta E Pandolfo N et alBiliopancreatic bypass Proposal and preliminaryexperimental study of a new type of operation for thefunctional surgical treatment of obesity Minerva Chir1976 31 560-6
2 Scopinaro N Adami GF Marinari GM et alBiliopancreatic diversion World J Surg 1998 22936-46
3 Baroudi R Body sculpturing Clin Plast Surg 1984111 419-43
4 Strauch B Greenspun D Levine J et al A techniqueof brachioplasty Plast Reconstr Surg 2004 1131044-8 discussion 1049
5 Guerrero-Santos J Brachioplasty Aesthetic PlastSurg 1979 3 1-4
6 Le Louarn C Pascal JF The concentric medial thigh-lift Aesthetic Plast Surg 2004 28 20-3
7 Lockwood TE Fascial anchoring technique in medialthigh lifts Plast Reconstr Surg 1988 82 299-304
8 Ribeiro L Canzl W Buss A et al Tuberous breast anew approach 1998 101 42-50
9 De Longis E Mastoplastica riduttiva Mastopessi Ladermopessi Colosseum Edition 1997
10Matarasso A Abdominoplasty In Achauer BMEriksson E Guyuron B et al eds Plastic SurgeryIndications Operations and Outcomes Vol V StLouis Mosby 2000 2783
11Planas J The ldquovest over pantsrdquo abdominoplasty PlastReconstr Surg 1978 61 694-700
12Nurkim MV et al Incidence of hematoma and seromain abdominoplasty with and without the use of drainsRev Soc Bras Cir Plast 2002 17 69-74 (abstract)
Body Contouring after BPD ndash Overview
Obesity Surgery 16 2006 1643
December 112306 123 PM Page 1643
Migliori et al
1644 Obesity Surgery 16 2006
13van Uchelen JH Werker PMN Kon MComplications of abdominoplasty in 86 patients PlastReconcstr Surg 2001 107 1869-73
14Huger WE Jr The anatomic rationale for abdominallipectomy Ann Surg 1979 45 612-7
15Hester TR Jr Nahai F Beegle PE et al Blood supplyof the abdomen revisited with emphasis on the super-ficial inferior epigastric artery Plast Reconstr Surg1984 47 657-70
16Scopinaro N Marinari GM Camerini GLaparoscopic standard biliopancreatic diversiontechnique and preliminary results Obes Surg 200212 362-5
17Matarasso A Evaluation and classification in abdom-inal contour surgery in abdominoplasty Oper TechPlast Surg 1996 3 7-11
18Matarasso A Liposuction as an adjunct to full
abdominoplasty revisited Plast Reconstr Surg 2000106 1197-202 discussion 1203-5
19 Lockwood TE Lower body lift with superficial fascialsystem suspension Plast Reconstr Surg 1993 92 1112-6
20Pascal JF Le Louarn C Remodelling body-lift withhigh lateral tension Aesthetic Plast Surg 2002 26223-30
21Bolton M Pruzinsky T Cash T et al Measuring out-comes in plastic surgery body image and quality oflife in abdominoplasty patients Plast Reconstr Surg2003 112 619-25
22Adami G Bauer B Gandolfo P et al Body image inearly-onset obese patients Eat Weight Disord 19972 87-93
(Received June 22 2006 accepted August 3 2006)
December 112306 123 PM Page 1644

20) and glandular hypotrophy These two defects arefrequently present together Very rarely have weneeded to reduce the gland volume In minor ptosis(NAC lift of about 4-5 cm) we utilize round blocktechnique added if necessary with an alloplasticimplant (Figure 3-1) or the self-prosthesis techniqueof Ribeiro8 (Figure 3-2) In a major ptosis we utilizethe vertical technique or L technique9 eventually sup-plemented by a prosthesis or self-prosthesis
AbdominoplastyAs a consequence of the above-described anatomo-surgical modifications and of the high percentage ofpotential complications we are convinced that theright abdominoplasty technique for this kind ofpatient should be quick and safe10 (Figure 4)Therefore we usually utilize the ldquovest over pantsrdquotechnique (Planas 1978) with an inverted V exci-sion providing higher vascular safety11
Migliori et al
1640 Obesity Surgery 16 2006
Figure 1 A Before brachioplasty B After brachioplasty
A B
Figure 2 A Before thigh-lift B After thigh-lift
A B
December 112306 123 PM Page 1640
Body Contouring after BPD ndash Overview
Obesity Surgery 16 2006 1641
Figure 3-1 A Mastoplasty case 1 before B Mastoplasty case 1 after (mastopexy with silicone implants)
A B
Figure 3-2 A Mastoplasty case 2 before B Mastoplasty case 2 after (mastopexy with self-prosthesis)
A B
Figure 4 A Before abdominoplasty B After abdominoplasty
A B
December 112306 123 PM Page 1641
Migliori et al
1642 Obesity Surgery 16 2006
Figure 5 Torsoplasty A front B back (with island flaps for buttocks emphasized)
A B
Figure 6 Torsoplasty results A Back before B Back after
A B
C Side before D Side after
C D
December 112306 123 PM Page 1642
The high incidence of abdominal wall complica-tions1213 in this particular group of patients com-pared with ldquonon-BPDrdquo patients and the review ofanatomical studies1415 has suggested to us toincrease the research of causes by arteriographicstudy of the epigastric vessels In five studied casesno reliable modifications have been foundTherefore without a demonstrated dysmetabolicpathogenesis secondary to BPD the only certaincause responsible for almost 70 of trophic com-plications following abdominoplasty is the presenceof previous scars In more recent BPD cases oper-ated by the laparoscopic approach (with very shortabdominal scars) the percentage of complicationshas significantly decreased16
Torsoplasty
In patients with more massive weight loss (70-100kg) it is possible to observe a particular trunk non-esthetism the so-called ldquosharpei profilerdquo (Sharpei isan Asian dog characterized by redundant inelasticskin) In this kind of ldquotridimensionalrdquo defect aldquobidimensionalrdquo technique like abdominoplasty isnot adequate1718 In these cases the correction offlanks and back profile is necessary as well as of theptosis of the buttocks and the external thighs
In these patients we perform torsoplasty asdescribed by Lockwood19 and Pascal-LeLouarn20
supplemented by a de-epithelilized island flap inorder to emphasize the profile (Figure 5) We com-mence with the excision of the redundant tissue firston the back side then on the lateral aspect andfinally on the abdominal wall The excisions areconducted in serial little segments in order toreduce incarcerated blood losses as much as possi-ble The variety and complexity of correctionobtained by torsoplasty in a single surgical time(posterior and lateral lift abdominal wall flatteninggreat removal of excess tissue hernia repair) givesan improvement of the entire ldquosilhouetterdquo which isnot achievable with any other technique (Figure 6)
Conclusions
Great ldquopositiverdquo thinking of these patients towardsbody contouring creates enormous expectations for
improvement in quality of life (similar to the expecta-tions which motivated these patients toward bariatricsurgery)21 Of these operated patients 99 declarethemselves completely satisfied with the obtainedresults and go on to further body contouring Thesekinds of results are not achievable by bariatric surgeryalone andor by eating behavior normalization22
On average we perform 2-3 operations on eachpatient The main points of patient satisfaction arerdquobody imagerdquo greatly improved self-esteem recov-ery improvement in life relationships and sexuallife resumption or improvement A body uneasinesstest study is in progress in 5 different groups ofthese patients
References
1 Scopinaro N Gianetta E Pandolfo N et alBiliopancreatic bypass Proposal and preliminaryexperimental study of a new type of operation for thefunctional surgical treatment of obesity Minerva Chir1976 31 560-6
2 Scopinaro N Adami GF Marinari GM et alBiliopancreatic diversion World J Surg 1998 22936-46
3 Baroudi R Body sculpturing Clin Plast Surg 1984111 419-43
4 Strauch B Greenspun D Levine J et al A techniqueof brachioplasty Plast Reconstr Surg 2004 1131044-8 discussion 1049
5 Guerrero-Santos J Brachioplasty Aesthetic PlastSurg 1979 3 1-4
6 Le Louarn C Pascal JF The concentric medial thigh-lift Aesthetic Plast Surg 2004 28 20-3
7 Lockwood TE Fascial anchoring technique in medialthigh lifts Plast Reconstr Surg 1988 82 299-304
8 Ribeiro L Canzl W Buss A et al Tuberous breast anew approach 1998 101 42-50
9 De Longis E Mastoplastica riduttiva Mastopessi Ladermopessi Colosseum Edition 1997
10Matarasso A Abdominoplasty In Achauer BMEriksson E Guyuron B et al eds Plastic SurgeryIndications Operations and Outcomes Vol V StLouis Mosby 2000 2783
11Planas J The ldquovest over pantsrdquo abdominoplasty PlastReconstr Surg 1978 61 694-700
12Nurkim MV et al Incidence of hematoma and seromain abdominoplasty with and without the use of drainsRev Soc Bras Cir Plast 2002 17 69-74 (abstract)
Body Contouring after BPD ndash Overview
Obesity Surgery 16 2006 1643
December 112306 123 PM Page 1643
Migliori et al
1644 Obesity Surgery 16 2006
13van Uchelen JH Werker PMN Kon MComplications of abdominoplasty in 86 patients PlastReconcstr Surg 2001 107 1869-73
14Huger WE Jr The anatomic rationale for abdominallipectomy Ann Surg 1979 45 612-7
15Hester TR Jr Nahai F Beegle PE et al Blood supplyof the abdomen revisited with emphasis on the super-ficial inferior epigastric artery Plast Reconstr Surg1984 47 657-70
16Scopinaro N Marinari GM Camerini GLaparoscopic standard biliopancreatic diversiontechnique and preliminary results Obes Surg 200212 362-5
17Matarasso A Evaluation and classification in abdom-inal contour surgery in abdominoplasty Oper TechPlast Surg 1996 3 7-11
18Matarasso A Liposuction as an adjunct to full
abdominoplasty revisited Plast Reconstr Surg 2000106 1197-202 discussion 1203-5
19 Lockwood TE Lower body lift with superficial fascialsystem suspension Plast Reconstr Surg 1993 92 1112-6
20Pascal JF Le Louarn C Remodelling body-lift withhigh lateral tension Aesthetic Plast Surg 2002 26223-30
21Bolton M Pruzinsky T Cash T et al Measuring out-comes in plastic surgery body image and quality oflife in abdominoplasty patients Plast Reconstr Surg2003 112 619-25
22Adami G Bauer B Gandolfo P et al Body image inearly-onset obese patients Eat Weight Disord 19972 87-93
(Received June 22 2006 accepted August 3 2006)
December 112306 123 PM Page 1644

Body Contouring after BPD ndash Overview
Obesity Surgery 16 2006 1641
Figure 3-1 A Mastoplasty case 1 before B Mastoplasty case 1 after (mastopexy with silicone implants)
A B
Figure 3-2 A Mastoplasty case 2 before B Mastoplasty case 2 after (mastopexy with self-prosthesis)
A B
Figure 4 A Before abdominoplasty B After abdominoplasty
A B
December 112306 123 PM Page 1641
Migliori et al
1642 Obesity Surgery 16 2006
Figure 5 Torsoplasty A front B back (with island flaps for buttocks emphasized)
A B
Figure 6 Torsoplasty results A Back before B Back after
A B
C Side before D Side after
C D
December 112306 123 PM Page 1642
The high incidence of abdominal wall complica-tions1213 in this particular group of patients com-pared with ldquonon-BPDrdquo patients and the review ofanatomical studies1415 has suggested to us toincrease the research of causes by arteriographicstudy of the epigastric vessels In five studied casesno reliable modifications have been foundTherefore without a demonstrated dysmetabolicpathogenesis secondary to BPD the only certaincause responsible for almost 70 of trophic com-plications following abdominoplasty is the presenceof previous scars In more recent BPD cases oper-ated by the laparoscopic approach (with very shortabdominal scars) the percentage of complicationshas significantly decreased16
Torsoplasty
In patients with more massive weight loss (70-100kg) it is possible to observe a particular trunk non-esthetism the so-called ldquosharpei profilerdquo (Sharpei isan Asian dog characterized by redundant inelasticskin) In this kind of ldquotridimensionalrdquo defect aldquobidimensionalrdquo technique like abdominoplasty isnot adequate1718 In these cases the correction offlanks and back profile is necessary as well as of theptosis of the buttocks and the external thighs
In these patients we perform torsoplasty asdescribed by Lockwood19 and Pascal-LeLouarn20
supplemented by a de-epithelilized island flap inorder to emphasize the profile (Figure 5) We com-mence with the excision of the redundant tissue firston the back side then on the lateral aspect andfinally on the abdominal wall The excisions areconducted in serial little segments in order toreduce incarcerated blood losses as much as possi-ble The variety and complexity of correctionobtained by torsoplasty in a single surgical time(posterior and lateral lift abdominal wall flatteninggreat removal of excess tissue hernia repair) givesan improvement of the entire ldquosilhouetterdquo which isnot achievable with any other technique (Figure 6)
Conclusions
Great ldquopositiverdquo thinking of these patients towardsbody contouring creates enormous expectations for
improvement in quality of life (similar to the expecta-tions which motivated these patients toward bariatricsurgery)21 Of these operated patients 99 declarethemselves completely satisfied with the obtainedresults and go on to further body contouring Thesekinds of results are not achievable by bariatric surgeryalone andor by eating behavior normalization22
On average we perform 2-3 operations on eachpatient The main points of patient satisfaction arerdquobody imagerdquo greatly improved self-esteem recov-ery improvement in life relationships and sexuallife resumption or improvement A body uneasinesstest study is in progress in 5 different groups ofthese patients
References
1 Scopinaro N Gianetta E Pandolfo N et alBiliopancreatic bypass Proposal and preliminaryexperimental study of a new type of operation for thefunctional surgical treatment of obesity Minerva Chir1976 31 560-6
2 Scopinaro N Adami GF Marinari GM et alBiliopancreatic diversion World J Surg 1998 22936-46
3 Baroudi R Body sculpturing Clin Plast Surg 1984111 419-43
4 Strauch B Greenspun D Levine J et al A techniqueof brachioplasty Plast Reconstr Surg 2004 1131044-8 discussion 1049
5 Guerrero-Santos J Brachioplasty Aesthetic PlastSurg 1979 3 1-4
6 Le Louarn C Pascal JF The concentric medial thigh-lift Aesthetic Plast Surg 2004 28 20-3
7 Lockwood TE Fascial anchoring technique in medialthigh lifts Plast Reconstr Surg 1988 82 299-304
8 Ribeiro L Canzl W Buss A et al Tuberous breast anew approach 1998 101 42-50
9 De Longis E Mastoplastica riduttiva Mastopessi Ladermopessi Colosseum Edition 1997
10Matarasso A Abdominoplasty In Achauer BMEriksson E Guyuron B et al eds Plastic SurgeryIndications Operations and Outcomes Vol V StLouis Mosby 2000 2783
11Planas J The ldquovest over pantsrdquo abdominoplasty PlastReconstr Surg 1978 61 694-700
12Nurkim MV et al Incidence of hematoma and seromain abdominoplasty with and without the use of drainsRev Soc Bras Cir Plast 2002 17 69-74 (abstract)
Body Contouring after BPD ndash Overview
Obesity Surgery 16 2006 1643
December 112306 123 PM Page 1643
Migliori et al
1644 Obesity Surgery 16 2006
13van Uchelen JH Werker PMN Kon MComplications of abdominoplasty in 86 patients PlastReconcstr Surg 2001 107 1869-73
14Huger WE Jr The anatomic rationale for abdominallipectomy Ann Surg 1979 45 612-7
15Hester TR Jr Nahai F Beegle PE et al Blood supplyof the abdomen revisited with emphasis on the super-ficial inferior epigastric artery Plast Reconstr Surg1984 47 657-70
16Scopinaro N Marinari GM Camerini GLaparoscopic standard biliopancreatic diversiontechnique and preliminary results Obes Surg 200212 362-5
17Matarasso A Evaluation and classification in abdom-inal contour surgery in abdominoplasty Oper TechPlast Surg 1996 3 7-11
18Matarasso A Liposuction as an adjunct to full
abdominoplasty revisited Plast Reconstr Surg 2000106 1197-202 discussion 1203-5
19 Lockwood TE Lower body lift with superficial fascialsystem suspension Plast Reconstr Surg 1993 92 1112-6
20Pascal JF Le Louarn C Remodelling body-lift withhigh lateral tension Aesthetic Plast Surg 2002 26223-30
21Bolton M Pruzinsky T Cash T et al Measuring out-comes in plastic surgery body image and quality oflife in abdominoplasty patients Plast Reconstr Surg2003 112 619-25
22Adami G Bauer B Gandolfo P et al Body image inearly-onset obese patients Eat Weight Disord 19972 87-93
(Received June 22 2006 accepted August 3 2006)
December 112306 123 PM Page 1644

Migliori et al
1642 Obesity Surgery 16 2006
Figure 5 Torsoplasty A front B back (with island flaps for buttocks emphasized)
A B
Figure 6 Torsoplasty results A Back before B Back after
A B
C Side before D Side after
C D
December 112306 123 PM Page 1642
The high incidence of abdominal wall complica-tions1213 in this particular group of patients com-pared with ldquonon-BPDrdquo patients and the review ofanatomical studies1415 has suggested to us toincrease the research of causes by arteriographicstudy of the epigastric vessels In five studied casesno reliable modifications have been foundTherefore without a demonstrated dysmetabolicpathogenesis secondary to BPD the only certaincause responsible for almost 70 of trophic com-plications following abdominoplasty is the presenceof previous scars In more recent BPD cases oper-ated by the laparoscopic approach (with very shortabdominal scars) the percentage of complicationshas significantly decreased16
Torsoplasty
In patients with more massive weight loss (70-100kg) it is possible to observe a particular trunk non-esthetism the so-called ldquosharpei profilerdquo (Sharpei isan Asian dog characterized by redundant inelasticskin) In this kind of ldquotridimensionalrdquo defect aldquobidimensionalrdquo technique like abdominoplasty isnot adequate1718 In these cases the correction offlanks and back profile is necessary as well as of theptosis of the buttocks and the external thighs
In these patients we perform torsoplasty asdescribed by Lockwood19 and Pascal-LeLouarn20
supplemented by a de-epithelilized island flap inorder to emphasize the profile (Figure 5) We com-mence with the excision of the redundant tissue firston the back side then on the lateral aspect andfinally on the abdominal wall The excisions areconducted in serial little segments in order toreduce incarcerated blood losses as much as possi-ble The variety and complexity of correctionobtained by torsoplasty in a single surgical time(posterior and lateral lift abdominal wall flatteninggreat removal of excess tissue hernia repair) givesan improvement of the entire ldquosilhouetterdquo which isnot achievable with any other technique (Figure 6)
Conclusions
Great ldquopositiverdquo thinking of these patients towardsbody contouring creates enormous expectations for
improvement in quality of life (similar to the expecta-tions which motivated these patients toward bariatricsurgery)21 Of these operated patients 99 declarethemselves completely satisfied with the obtainedresults and go on to further body contouring Thesekinds of results are not achievable by bariatric surgeryalone andor by eating behavior normalization22
On average we perform 2-3 operations on eachpatient The main points of patient satisfaction arerdquobody imagerdquo greatly improved self-esteem recov-ery improvement in life relationships and sexuallife resumption or improvement A body uneasinesstest study is in progress in 5 different groups ofthese patients
References
1 Scopinaro N Gianetta E Pandolfo N et alBiliopancreatic bypass Proposal and preliminaryexperimental study of a new type of operation for thefunctional surgical treatment of obesity Minerva Chir1976 31 560-6
2 Scopinaro N Adami GF Marinari GM et alBiliopancreatic diversion World J Surg 1998 22936-46
3 Baroudi R Body sculpturing Clin Plast Surg 1984111 419-43
4 Strauch B Greenspun D Levine J et al A techniqueof brachioplasty Plast Reconstr Surg 2004 1131044-8 discussion 1049
5 Guerrero-Santos J Brachioplasty Aesthetic PlastSurg 1979 3 1-4
6 Le Louarn C Pascal JF The concentric medial thigh-lift Aesthetic Plast Surg 2004 28 20-3
7 Lockwood TE Fascial anchoring technique in medialthigh lifts Plast Reconstr Surg 1988 82 299-304
8 Ribeiro L Canzl W Buss A et al Tuberous breast anew approach 1998 101 42-50
9 De Longis E Mastoplastica riduttiva Mastopessi Ladermopessi Colosseum Edition 1997
10Matarasso A Abdominoplasty In Achauer BMEriksson E Guyuron B et al eds Plastic SurgeryIndications Operations and Outcomes Vol V StLouis Mosby 2000 2783
11Planas J The ldquovest over pantsrdquo abdominoplasty PlastReconstr Surg 1978 61 694-700
12Nurkim MV et al Incidence of hematoma and seromain abdominoplasty with and without the use of drainsRev Soc Bras Cir Plast 2002 17 69-74 (abstract)
Body Contouring after BPD ndash Overview
Obesity Surgery 16 2006 1643
December 112306 123 PM Page 1643
Migliori et al
1644 Obesity Surgery 16 2006
13van Uchelen JH Werker PMN Kon MComplications of abdominoplasty in 86 patients PlastReconcstr Surg 2001 107 1869-73
14Huger WE Jr The anatomic rationale for abdominallipectomy Ann Surg 1979 45 612-7
15Hester TR Jr Nahai F Beegle PE et al Blood supplyof the abdomen revisited with emphasis on the super-ficial inferior epigastric artery Plast Reconstr Surg1984 47 657-70
16Scopinaro N Marinari GM Camerini GLaparoscopic standard biliopancreatic diversiontechnique and preliminary results Obes Surg 200212 362-5
17Matarasso A Evaluation and classification in abdom-inal contour surgery in abdominoplasty Oper TechPlast Surg 1996 3 7-11
18Matarasso A Liposuction as an adjunct to full
abdominoplasty revisited Plast Reconstr Surg 2000106 1197-202 discussion 1203-5
19 Lockwood TE Lower body lift with superficial fascialsystem suspension Plast Reconstr Surg 1993 92 1112-6
20Pascal JF Le Louarn C Remodelling body-lift withhigh lateral tension Aesthetic Plast Surg 2002 26223-30
21Bolton M Pruzinsky T Cash T et al Measuring out-comes in plastic surgery body image and quality oflife in abdominoplasty patients Plast Reconstr Surg2003 112 619-25
22Adami G Bauer B Gandolfo P et al Body image inearly-onset obese patients Eat Weight Disord 19972 87-93
(Received June 22 2006 accepted August 3 2006)
December 112306 123 PM Page 1644

The high incidence of abdominal wall complica-tions1213 in this particular group of patients com-pared with ldquonon-BPDrdquo patients and the review ofanatomical studies1415 has suggested to us toincrease the research of causes by arteriographicstudy of the epigastric vessels In five studied casesno reliable modifications have been foundTherefore without a demonstrated dysmetabolicpathogenesis secondary to BPD the only certaincause responsible for almost 70 of trophic com-plications following abdominoplasty is the presenceof previous scars In more recent BPD cases oper-ated by the laparoscopic approach (with very shortabdominal scars) the percentage of complicationshas significantly decreased16
Torsoplasty
In patients with more massive weight loss (70-100kg) it is possible to observe a particular trunk non-esthetism the so-called ldquosharpei profilerdquo (Sharpei isan Asian dog characterized by redundant inelasticskin) In this kind of ldquotridimensionalrdquo defect aldquobidimensionalrdquo technique like abdominoplasty isnot adequate1718 In these cases the correction offlanks and back profile is necessary as well as of theptosis of the buttocks and the external thighs
In these patients we perform torsoplasty asdescribed by Lockwood19 and Pascal-LeLouarn20
supplemented by a de-epithelilized island flap inorder to emphasize the profile (Figure 5) We com-mence with the excision of the redundant tissue firston the back side then on the lateral aspect andfinally on the abdominal wall The excisions areconducted in serial little segments in order toreduce incarcerated blood losses as much as possi-ble The variety and complexity of correctionobtained by torsoplasty in a single surgical time(posterior and lateral lift abdominal wall flatteninggreat removal of excess tissue hernia repair) givesan improvement of the entire ldquosilhouetterdquo which isnot achievable with any other technique (Figure 6)
Conclusions
Great ldquopositiverdquo thinking of these patients towardsbody contouring creates enormous expectations for
improvement in quality of life (similar to the expecta-tions which motivated these patients toward bariatricsurgery)21 Of these operated patients 99 declarethemselves completely satisfied with the obtainedresults and go on to further body contouring Thesekinds of results are not achievable by bariatric surgeryalone andor by eating behavior normalization22
On average we perform 2-3 operations on eachpatient The main points of patient satisfaction arerdquobody imagerdquo greatly improved self-esteem recov-ery improvement in life relationships and sexuallife resumption or improvement A body uneasinesstest study is in progress in 5 different groups ofthese patients
References
1 Scopinaro N Gianetta E Pandolfo N et alBiliopancreatic bypass Proposal and preliminaryexperimental study of a new type of operation for thefunctional surgical treatment of obesity Minerva Chir1976 31 560-6
2 Scopinaro N Adami GF Marinari GM et alBiliopancreatic diversion World J Surg 1998 22936-46
3 Baroudi R Body sculpturing Clin Plast Surg 1984111 419-43
4 Strauch B Greenspun D Levine J et al A techniqueof brachioplasty Plast Reconstr Surg 2004 1131044-8 discussion 1049
5 Guerrero-Santos J Brachioplasty Aesthetic PlastSurg 1979 3 1-4
6 Le Louarn C Pascal JF The concentric medial thigh-lift Aesthetic Plast Surg 2004 28 20-3
7 Lockwood TE Fascial anchoring technique in medialthigh lifts Plast Reconstr Surg 1988 82 299-304
8 Ribeiro L Canzl W Buss A et al Tuberous breast anew approach 1998 101 42-50
9 De Longis E Mastoplastica riduttiva Mastopessi Ladermopessi Colosseum Edition 1997
10Matarasso A Abdominoplasty In Achauer BMEriksson E Guyuron B et al eds Plastic SurgeryIndications Operations and Outcomes Vol V StLouis Mosby 2000 2783
11Planas J The ldquovest over pantsrdquo abdominoplasty PlastReconstr Surg 1978 61 694-700
12Nurkim MV et al Incidence of hematoma and seromain abdominoplasty with and without the use of drainsRev Soc Bras Cir Plast 2002 17 69-74 (abstract)
Body Contouring after BPD ndash Overview
Obesity Surgery 16 2006 1643
December 112306 123 PM Page 1643
Migliori et al
1644 Obesity Surgery 16 2006
13van Uchelen JH Werker PMN Kon MComplications of abdominoplasty in 86 patients PlastReconcstr Surg 2001 107 1869-73
14Huger WE Jr The anatomic rationale for abdominallipectomy Ann Surg 1979 45 612-7
15Hester TR Jr Nahai F Beegle PE et al Blood supplyof the abdomen revisited with emphasis on the super-ficial inferior epigastric artery Plast Reconstr Surg1984 47 657-70
16Scopinaro N Marinari GM Camerini GLaparoscopic standard biliopancreatic diversiontechnique and preliminary results Obes Surg 200212 362-5
17Matarasso A Evaluation and classification in abdom-inal contour surgery in abdominoplasty Oper TechPlast Surg 1996 3 7-11
18Matarasso A Liposuction as an adjunct to full
abdominoplasty revisited Plast Reconstr Surg 2000106 1197-202 discussion 1203-5
19 Lockwood TE Lower body lift with superficial fascialsystem suspension Plast Reconstr Surg 1993 92 1112-6
20Pascal JF Le Louarn C Remodelling body-lift withhigh lateral tension Aesthetic Plast Surg 2002 26223-30
21Bolton M Pruzinsky T Cash T et al Measuring out-comes in plastic surgery body image and quality oflife in abdominoplasty patients Plast Reconstr Surg2003 112 619-25
22Adami G Bauer B Gandolfo P et al Body image inearly-onset obese patients Eat Weight Disord 19972 87-93
(Received June 22 2006 accepted August 3 2006)
December 112306 123 PM Page 1644

Migliori et al
1644 Obesity Surgery 16 2006
13van Uchelen JH Werker PMN Kon MComplications of abdominoplasty in 86 patients PlastReconcstr Surg 2001 107 1869-73
14Huger WE Jr The anatomic rationale for abdominallipectomy Ann Surg 1979 45 612-7
15Hester TR Jr Nahai F Beegle PE et al Blood supplyof the abdomen revisited with emphasis on the super-ficial inferior epigastric artery Plast Reconstr Surg1984 47 657-70
16Scopinaro N Marinari GM Camerini GLaparoscopic standard biliopancreatic diversiontechnique and preliminary results Obes Surg 200212 362-5
17Matarasso A Evaluation and classification in abdom-inal contour surgery in abdominoplasty Oper TechPlast Surg 1996 3 7-11
18Matarasso A Liposuction as an adjunct to full
abdominoplasty revisited Plast Reconstr Surg 2000106 1197-202 discussion 1203-5
19 Lockwood TE Lower body lift with superficial fascialsystem suspension Plast Reconstr Surg 1993 92 1112-6
20Pascal JF Le Louarn C Remodelling body-lift withhigh lateral tension Aesthetic Plast Surg 2002 26223-30
21Bolton M Pruzinsky T Cash T et al Measuring out-comes in plastic surgery body image and quality oflife in abdominoplasty patients Plast Reconstr Surg2003 112 619-25
22Adami G Bauer B Gandolfo P et al Body image inearly-onset obese patients Eat Weight Disord 19972 87-93
(Received June 22 2006 accepted August 3 2006)
December 112306 123 PM Page 1644