Embed Size (px)
Citation preview

BODITECH MED INC.
WORLD MARKET LEADER for IVD

2
Company overview
400
employees
7
Companies one family
120
Distribution countries
>50,000
Devices installedworldwide
80 Million
Cartridges per year

3
Quality system
Area Certi./Accreditation
Korea KGMP
Japan
Accreditation certificate of foreign medical devicemanufacturer
Accreditation certificate of foreign in vitro diagnostic manufacturer
Common
EN ISO 13485:2012+AC:2012
DIN EN ISO 13485:2012
MDSAP
NGSP HbA1c for ichroma, ichroma II, AFIAS-1, and AFIAS-50
Country Korea EU US CHINA JAPAN BRAZILAUSTRALIA
MOH MFDS CE FDA CFDA PMDA ANVISA TGA
Analyzer 12 12 3 5 2 2 2
Reagent 167 168 24 19 2 15 25
Registered items

4
▪ CK-MB▪ D-Dimer▪ hsCRP▪ Myoglobin▪ Troponin-I▪ NT-proBNP▪ Cardiac Triple▪ ST2*
▪ TSH▪ T3▪ T4▪ FSH▪ bhCG▪ PRL▪ LH▪ Cortisol▪ Testosterone▪ Progesterone
▪ AFP▪ CEA▪ PSA
▪ Cystatin C▪ HbA1c▪ MAU
▪ CRP▪ PCT▪ ASO▪ Dengue NS1▪ Dengue
IgM/G▪ HBsAg▪ Anti-HBs▪ Anti-HCV▪ HIV Ag/Ab▪ Zika IgG/IgM▪ TB (IGRA)*
▪ Vitamin D▪ Ferritin
▪ Noro▪ Rota▪ Rota/Adeno▪ H.Pylori Ag▪ Calprotectin▪ iFOB▪ iFOB/Calp
Combo
▪ Influenza A+B▪ Influenza/RSV▪ Strep A*▪ RSV*▪ Mycoplasma*
Diabetes
Other
Infectious
Cardiac
CancerImmune
Respiratory
Hormone
Gastro-Intestine
Boditech
Ichroma-50
Ichroma II
AFIAS-6
AFIAS-1
Ichroma M
TRIAS
Hemo-chroma
Plus
IRIS-3
▪ RF IgM▪ Anti-CCP▪ IgE

COVID-19 Antibody testPART 3

6
• Coronavirus is RNA virus with 27-32 kb genome and can infect human, bat, birds, and other
animals
• 4 coronavirus subtypes (Alpha, Beta, Delta, Gamma)
• Alpha, Beta: found in human, other animals
• Delta, Gamma: found in animals
• A novel coronavirus (nCoV) is a new strain that has not been previously identified in humans
and causes COVID-19 disease.
• Clinical symptoms including fever, coughing sneezing, and pneumonia.
Coronavirus

7
Human Coronavirus
There are seven strains of human coronaviruses
SARS-CoV-2
HCoV-229E HCoV-OC43 HCoV-OC43 HKU1
SARS-CoV MERS-CoV
Common cold coronavirus
SARS-CoV, MERS-CoV
Novel coronavirus

8
Covid-19 MERS SARS Common cold coronavirus
OriginFirst reported in December
2019 in Wuhan, China
First reported in 2012 in Saudi
Arabia
First reported in 2002
in southern China
Four coronavirus strains are
thought to be responsible for
15-30% of common cold
Trans-
mission
Likely from touching or
eating an infected, as yet
unidentified animal.
Human-to-human
transmission occurs through
close contact
Often from touching infected
camels or consuming their
milk or meat. Limited
transmission between
humans through close contact
Believed to have
spread from bats,
which infected civets.
Transmitted mainly
between humans
through close contact
Close contact with infected
humans or touching a
surface that carries the virus
CasesMore than 2.5Million
confirmed cases(2020.4.22)
1-10% mortality
2,494 confirmed cases; 858
deaths(as Nov. 30, 2019)
Mortality rate of 34%
8,098 cases; 774
deaths. Mortality rate
of about 10%
Millions each year. Generally
nonlethal with rare
exceptions.
Current
Status
Cases reported mainly in
China and spreading over
the world
All cased lined to Arabian
Peninsula. Others in 12
countries and death have
been declining since 2016
No new cases reported
since 2004. 87% of
previous cases in China
and Hong Kong
Circulates year-round, but
more common in fall/winter
Coronavirus Comparisons

9
Symptoms of Coronavirus infection
Severe symptoms
Common symptoms
High fever(40oC or more)
Pnuemonia
Kidney failure
Fever
Dry cough
Mild breathing difficulty
Gastrointestinal issues
Diarrhea
General body aches• Hemagglutination
• Cardiac problem
• Neuronal damage
• Kawasaki-like disease

10
COVID-19 Test window
PCR
Antibody test

11
TestType of sample
Comments
Molecular Diagnosis
Nucleic acid amplification & Sequencing
Respiratory sample
Collect on presentation. Done by an expert laboratory. RT-PCR followed by sequencing if positive.
NAAT, Nucleic acid amplification
Collect on presentation. Done by an expert laboratory. Various PCR methods are under validation
Whole genome sequencingCollect on presentation. Done by an expert laboratory. Well quipped facility with long and costly testing
Immuno-assay
Serology Serum
IgG/IgM test in blood sample.Paired samples necessary for confirmation, the first sample collected in week 1 of illness and the second collected 2-3 weeks late
WHO Guideline for novel coronavirus diagnosis
Diagnosis of Coronavirus infection

12
Detection rate 0-5.5 day 6-13 day >14 day
PCR > 90% 80 < 50 %
IgG/IGM ~ 75 % 75.6 ~ 93.1%
Detection rate by days
5.5 days after symptom onset, IgM/IgG detection rate is better than PCR positive rate and combine of PCR+IgM/IgG is best method

13
RT-PCR Boditech Antibody test
ELISA(Antibody)
Rapid test(Antibody)
Target Virus (RNA) Antiviral IgM/IgG Antiviral IgM/IgG Antiviral IgM/IgG
Sample Nasopharyngeal/ oropharyngeal swab
Blood(WB/S/P) Blood(S/P) Blood(WB/S/P)
Sample hazard level
Highly contagious Low to non-contagious
Low to non-contagious
Low to no-contagious
Time(TOT) 1-6 hrs 10 min 3-4hrs 10-15 min
Sensitivity High High to medium High to medium Low
Testing windows Pre-symptom to onset of symptom
3-6 days after onset of symptom
3-6 days after onset of symptom
1 week after onset of symptom
Result Qualitative with Ct value
Qualitative with COI value
Quantitative Qualitative
Clinical value Confirmatory test Screening and monitoring of COVID-19
Screening and monitoring of COVID-19
Screening
Methods comparison

14
Nine use cases for SARS-CoV-2 tests
USE CASE PCR Boditech/ELISA
Rapid
Ag Ab Ag Ab Ag
Triage of symptomatic individuals in an epidemic setting O O O ? O
Triage of symptomatic individuals in endemic settings O O O O
Triage of at-risk pre-symptomatic and symptomatic individuals in endemic settings O O O O
Confirmatory testing O
Diagnosis of symptomatic individuals in endemic or epidemic settings O O O ? O
Differential diagnosis in endemic or epidemic settings O O O ? O
Previous SARS-CoV-2 exposure O ?
Surveillance in sites of previous or potential outbreaks O O O O
Environmental monitoring O
Selection of convalescent person for plasma therapy O

15
RT-PCR
Total
Positive Negative
Boditech COVID-19 Ab
Positive 46 0 46
Indetermidated 2 4 6
negative 0 131 131
Total 48 135 183
Percent postive agreement (%) = 95.8 %
Percent negative agreement (%) = 97.0 %
Overall percent agreement (%) = 96.7%
Clinical evaluation of Boditech COVID-19 Ab test

4.30 4.49 4.92
10.98
7.01
27.23
0.00
10.00
20.00
30.00
1 4 7
2.094.31
1.405.78
34.25 32.9028.60
32.80
0.00
10.00
20.00
30.00
40.00
1 3 5 9
IgM IgG
Example of IgM/IgG level in COVID-19 cases
0.20 0.10 0.20 1.40 0.90 0.900.15 0.00
8.05
25.90 25.4026.95
0.00
10.00
20.00
30.00
1 3 5 7 9 11
0.00 0.00 0.00 0.00 0.00
0.30
0.75
0.25
0.75
2.35
0.00
0.50
1.00
1.50
2.00
2.50
1 3 6 11 120.00 1.00 0.85
27.6529.75
26.10
0.00
10.00
20.00
30.00
1 3 4
Days after hospitalizationDays after hospitalization
COI COI
0.85 0.752.05
5.15 4.65 4.75
0.15 0.15 0.80
6.20
12.95
22.75
0.00
10.00
20.00
30.00
1 4 8 10 12 16
IgM IgG

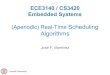
Figure 1. Kinetics of IgG (left axis, empty circles, solid smoothing splines) and IgM (right axis, cross marks, dashed smoothing splines) according to days post symptom onset (PSO), considering 8 patients with COVID-19, using the AFIAS COVID-19 Ab (Boditech Med Inc., Chuncheon, Republic of Korea). IgM and IgG levels (through signal intensity, the cut-off index (COI)) rapidly increased after 9 d PSO. IgM antibody levels peaked at 20–24 d PSO and gradually decreased thereafter. IgG levels gradually increased and were maintained at similar levels after 25–29 d PSO.
Confidential The figure is the part of submitted scientific paper and should not be released until it is published.
Kinetics of IgM/IgG in COVID-19 patients

18

19
Test procedure
1
2
3
4
Fingertip blood
Simple operation
Data collection by network
10 min result on site

20
Reader Specification
Up to 30-40 test/hours Up to 5-6 test/hours Up to 24 test/hours

21
Conclusion
• Superior Performance
➢ Percent positive agreement (%) = 95.8 %
➢ Percent negative agreement (%) = 97.0 %
➢ Overall percent agreement (%) = 96.7%
• Qualitative result with COI value (relative amount of IgM/IgG)
➢ Monitoring of patient with serial test
➢ Equal or better than ELISA (not rapid type)
• IgG level in convalescence patient
➢ Test for acquired immunity to COVID-19
➢ Plasma therapy purpose

22
AFIAS/ichroma Antigen testViral antigen Immunofluorescence assay
✓ Antigen test(Immunofluorescence): practical alternative of PCR
✓ Antigen test AND antibody test will produce best result
✓ Test window covers most of infection AND convalescent period

An employee holds up an Ichroma Covid-19 Ab testing kit at the Boditech Med headquarters in
Chuncheon, South Korea. Bloomberg
THANK YOUBODITECH MED [email protected]

24
PCR practical issues
⚫ Sampling issues
- CDC recommend nasopharyngeal AND oropharyngeal swab.
nasopharyngeal sampling requires some training and common cause of
false negative
- It is reported that during nasopharyngeal swab sampling, candidates
often sneezing or coughing, which is potential hazard for the health
worker.
- Sample is biosafety level 2 but SARS-Cov-2 virus is biosafety level 3. Thus,
during transport and extraction (until it completed and collect RNA of
virus). It need to be treated as biosafety level 3 and extreme caution.
- Virus is liable in even in protective solution(VTM). 3-4 hours at RT and 24
hours at refrigerated. Sample transfer from collection site to Lab for PCR
causes the false negative
Appendix 1

25
PCR practical issues
⚫ Performing analysis ( virus RNA extraction and PCR amplification)
- As previously mentioned, extraction should be performed biosafety level 3 with
high level protection equipment. It requires well trained person. Also prolonged
working at BL3 environment gives burden and easily slow down performance.(It
is one of the bottleneck of PCR procedure)
- In case different lab uses different PCR device, it is hard to compare directly each
result
- PCR requires well trained person for the operation and result analysis.
→ In Korea, at least 2 independent PCR positive is required for COVID-19
Confirmation. Due to inconsistency of result, it is reported that 10 times of
independent PCR had been performed in one patient
- Contamination issues: lab test is performed a lot test, positive result tube
contains amplified (hundreds millions of copy) RNA and it is potential
contaminant of PCR device and Lab.
It is reported that several case of device contamination, which resulted false
positive (Pure water can produce positive PCR result)

26
Impact factor=9.1
Results The median duration of IgM and IgA antibody detection were 5 days (IQR 3-6),
while IgG was detected on 14 days (IQR 10-18) after symptom onset, with a positive rate of
85.4%, 92.7% and 77.9% respectively. In confirmed and probable cases, the positive rates of
IgM antibodies were 75.6% and 93.1%, respectively. The detection efficiency by IgM ELISA
is higher than that of qPCR method after 5.5 days of symptom onset. The positive detection
rate is significantly increased (98.6%) when combined IgM ELISA assay with PCR for each
patient compare with a single qPCR test (51.9%).
Appendix 2

27
IgG/A IgG
Detection rate
85.4 77.9%
Detectable Day*
Day 5IQR(3-6)
Day 14IQR(10-18)
*Day after symptom onsetPost symptom onset(POS)
Day IgG change IgG change
0-7 Base level Base level
8-14 Increased Increased
15-21 plateaued Increased
>21 plateaued plateaued
IgM and IgG characteristics

28
Detection rate 0-5.5 day 6-13 day >14 day
PCR(single) > 90% 80 < 50 %
IgG/IGM ~ 75 % 75.6 ~ 93.1%
Detection rate by days
5.5 days after symptom onset, IgM/IgG detection rate is better than PCR positive rate

29
Appendix 3Example of test result