Embed Size (px)
Citation preview

Board Review:
ENVIRONMENTAL
Stony Brook University HospitalJoanne Kim, PGY3

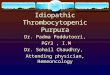
Frostbite• A 34-year-old man fell asleep on
the sidewalk in the snow. Examination reveals a swollen, erythematous left hand with clear blisters as seen above. The patient has decreased sensation and decreased range of motion. What therapy is indicated?
• A- Place hand in warm (35°C - 42°C) water
• B - Place hand in hot (45°C - 52°C) water
• C - Warm hand with circulating hot air
• D - Wrap hand in warm blankets

Frostbite
• Warming should not be initiated until it is certain that refreezing will not occur–TRUE or FALSE?

Frostbite

Frost Bite• Warming only if refreezing will
not occur• Thawing contributes to the
degree of injury (endothelial damage starts swelling, plt aggregation, vessel thrombosis)
• Mostly distal fingers, nose, ears• Zone of coagulation –
irreversible• Zone of hyperemia – recovers
<10d• Zone of stasis – treatment may
benefit (midzone)

?

Hypothermia
• Common arrhythmia <32’c?• Treatment?– Afib, Brady, +VS, Temp 32
• When to start invasive rewarming?• At what temp do you lose the ability to shiver• What temp can you stop resuscitation efforts?• What is Core Temperature Afterdrop?

Hypothermia• 50% who die are >65yo• EKG
– Sinus brady Afib w slow Vt response (most common) Vfib Asystole
– Osborn wave, T wave inversion, QRS/QR prolongation, AV blocks, PVCs
– Don’t treat Afib, brady b/c resistant to meds/shock (protein binding) – tx hypothermia
• @ <32’c – loses ability to shiver• @ 30-32’c – can withdraw
resuscitation efforts• IVF (rhabdo), O2 (L shift Hg curve),
immobilize (Vfib risk)• RSI meds may not be effective
• Hypothermia Staging– 1 (32-35) – shivers, conscious warm
env/drinks, clothes– 2 (28-32) – x shiver, mildly impaired cardiac
monitor, immobilize (Vfib risk), insulate, active external heating, warm fluids, head pads
– 3 (24-28) – AMS, +VS ABCs, medical management if not ECMO if cardiac instability (Vfib, Asystole)
– 4 (<24) – x VS ACLS, defib, ECMO/invasive warming (lavage, Ivf, ECMO/Dialysis)• If only truly pulseless (Vfib risk)
• Start Invasive rewarming w – cardiac instability (Vfib, asystole, failed
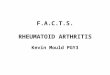
medical tx, severel hypothermia)• Core temp after drop (warm trunk b/f ext)
Warmed vasodilated peripheral tissue allows cooler blood in extremities to circulate back to core

Near Drowning
• A 10-year-old girl presents after a submersion incident at a nearby lake. She was extracted quickly and on reaching the dock and had dry coughs. Vital signs are normal. PE wnl, CXR wnl. What management is indicated?
• Is risk for drowning higher in salt water?

Near Drowning• Mostly in young, elderly
• No clinical diff b/w fresh-water vs salt-water, wet vs dry drowning
• Dry-drowning – laryngospasm, hypoxia/death (vs delayed submersion inj/pulm edema)
• Resuscitate longer in cold water submersion (longest was 66min w ecmo)
• Assume C spine inj if not clear, vent w high peep
• Prognosis– Prolonged submersion
and resuscitation, low GCS, warm water, asystolic rhythm, male
– Hypothermia is actually a POOR prognisticator as it indicates prolonged submersion
• Near-drowning tx– Obs 4-6 hrs, +CXR

Radiation
• Earliest indication for significant radiation exposure?
• 1Gy = ? Rads

Radiation• Acute radiation syndrome – at
least 1 Gray (Gy) = 100 rads
• Stages– Prodromal stage – n/v, f– Latent phase (days/1mo) – Manifest illness stage
(pancytopenia, GI sx, CNS sx)– Recovery, death
• The higher the level of exposure, the quicker symptoms develop.
• Sx– 1-2 Gy – BM syndrome –
lymphocyte depletion first, good predictor
– 6-10Gy – n/v/d, abd pain– 10-20 Gy – coma, AMS,
papilledema
• ALC drop @ 48hrs – best for prognosis, also GI sx

?Other associated sx?

Electric Injuries• AC vs DC current?
– Sustained contractions– Pt thrown from source – Asystole vs Vfib– Higher chance of rhabdo,
compartment syndrome, myoglobinuria
– Posterior shoulder dislocation – Fractures – Lightening– Household outlets? – Extensive burns – Exit wound more discrete
• Conductible tissue?
• Dispo?– Mild burn, normal ekg,
otherwise asx
– Peds chewing on power cord w electric burn on lips

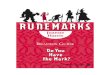
Electrical Injuries• Litchenberg figure –
• From lightining strike• TM rupture common
• AC vs DC current?– Sustained contractions (AC)– Pt thrown from source (DC)– Asystole (DC) vs Vfib (AC)– Higher chance of rhabdo,
compartment syndrome, myoglobinuria (AC)
– Posterior shoulder dislocation (AC)– Fractures (DC)– Lightening? (DC)– Household outlets? (AC)– Extensive burns (AC)– Exit wound more discrete (DC)
• Conductible tissue?– Nerves, bv, moist skin, muscles >>
bone, tendon, fat
• Dispo?– Mild burn, normal ekg, otherwise asx
DC– Admit - High-voltage injuries, sx, abnl
ekg, trop, cp/hypoxia, loc, CAD – Peds chewing on power cord w
electric burn on lips• (labial artery, delayed bleed)• close observation (sometimes in the
hospital) and referral to a plastic or oral surgeon
• In cardiac arrest - Higher chance of survival than CAD caused arrest

• A 65-year-old man complains of foot numbness. He has been outside over the last several days during the rain unable to change his shoes or socks. When his wet socks are removed, his feet are cold, cyanotic and edematous. What is his diagnosis?

Immersion Foot / Trench food
• progresses slowly over days neurovascular damage (x crystals)
– Mostly in the military - wet or sweaty socks • cool, pale feet and complain of paresthesias• feet become cyanotic, cold and edematous• After rewarming, the skin becomes erythematous and is
painful to palpation. • Neurovascular problems are typically reversible.
– Tx – keep feet clean, dry

Scuba Diving
• Most common complaint of scuba divers?
• Ascend with LOC, cardiac arrest, cp/sob – dx?
• Ascend with joint pain, possible paralysis/weakness, AMS, urinary retention – dx?

Scuba Diving
• Common complaint– Middle ear barotrauma– Barotitis – ear pain,
hearing loss, TM rupture, nystagmus, 7th nerve palsy
• Decompression sickness • “the bends”• forming nitrogen bubbles
– Type 1 - jt pain, skin reticularis, const sx
– Type 2 – SC (paralysis, retention), vestibular sx (tinnitus, vertigo), pulm chokes (sob, cp)
– Type 3 (+gas embolism) – stroke sx
• Tx– O2, supine (x trendelenburg)– Hyperbaric O2

High Altitude
• During a climb, pt dev sob, tachypnea, crackles, cough – tx?
• Ascend w n/v, weakness, dizzy– PPx?
• Ascend w ams, ataxia – tx?

High Altitude• HAPE
– Descent > O2, hyperbaric chamber
• Acute mountain sickness– Ascend w n/v, weakness, dizzy– Acute mountain sickness –
acclimatize, acetazolamide (helps acclimization) – makes acidic blood, driving ventilation
– Ppx – slow ascent, acetazolamide, dexamethasone
• HACE– Ascend w ams, ataxia– descend

Tx?

Tx?

Marine Bites
• Tx for Stingray (sea urchins, stingrays or lionfish) stings– toxins are heat labile and best treated with hot (110°F) water
immersion.1. Remove spine (if possible)
2. Wash with sea water or fresh water
3. Submerge wound in hot water for 30-90 minutes
• Jelly Fish, nematocyst, fire corals, sea anemones– - local pain remove stinger, acetic acid immersion (vinegar)– Some can have lethal venom mostly autralia – resp paralysis, CV
collapse but most have local pain/swelling– Don’t use fresh water – can stimulate continued discharge– Steroids not helpful immediately

Burn
• 70kg, 3rd degree burns on back. Fluid amount?
• Who should be transferred?

Burns
• Parkland’s formula = TSA% x Kg x 4ml ½ first 8 hrs, other half 16hrs– Applies to only 2, 3rd
burns
• Who should be transferred?– > 20% TBSA, > 5% full
thickness, high voltage, significant burn to face, eyes, ears, genitalia or joints.

Hyperthermia
• Exercise, profuse sweating, dev muscle cramps, but temp normal
• Fatigue, lightheadedness, nausea, vomiting and a dull headache, tachypneic, tachycardic and hypotensive. Body temperature is normal.
• Elderly w AMS, respiratory alkalosis and mild metabolic acidosis, coagulopathy and CPK elevation, Temp >104
• Vs Young pt from exercise

Hyperthermia
• Heat cramps– Exercise, profuse sweating, dev muscle cramps, but temp normal– from hyponatremia
• Heat exhaustion– . Salt water depletion from sweat loss leads to hypovolemia and hypoperfusion;
neurologic and mental status exams are normal.– Tachy, sweating, n/v, fatigue, orthostatic hypotension.– hydration, cool env
• classical heat stroke (peds, elderly) vs exertional heat stroke– Ams w elev temp– AMS, ataxia, coma, sz– fluids, cool - evaporative, tx shivering w benzo, ice pacts, antipyretics no role
• Heat stroke vs heat exhaustion Mentation impaired in stroke

?

Spider Bite
• A patient presents with an acute abdomen. However, you notice that there is no tenderness but there is impressive rigidity. Hx spider bite– Dx?
• Spider bite - painless bite over few days can become necrotic
• Spider bite – muscle cramps, HA, VSS. Tx?– Supportive care– Antivenin– Abx

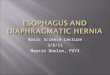
Spider Bite• Black widow - Yellow-red hour glass on abdomen of spider
– Venom releases Ach and NE from nerve terminals (cytotoxin)– Diffuse muscle cramps, Mimics acute abdomen, Sympathomimetic
symptoms 9tachy, htn)– Opiods, benzodiazepines, antivenin (only if severe sx, kids, pregnant,
elderly)– Admit – sx are moderate, at risk pts (peds, pregnant, cardio hx)
• Brown Recluse Spider– painless bite, often not recognized over few days can become necrotic,
systemic sx rare– Cytotoxins cause necrotic lesion– dapsone - limited benefit and is associated with hemolysis in G6PD
patients and methemoglobinemia

Snake Bite
• Snake bite w sx, bulla – tx?– Antivenom– Suction– Open bulla– Immobilize– Tournaquet– Wrap– ice water
• If allergic to antivenom?

Snake bite• Viperidae (pit vipers): (USA)
– Depression between eyes– Significant local reaction → systemic toxicity– Compartment syndrome– Thrombocytopenia– Antivenin
• Elapidae (coral snakes):– “Red on yellow kill a fellow, red on black venom lack”– Minimal local reaction → neurotoxicity– Respiratory paralysis– Coral snake bites: antivenin for all
• Coral Snakes: Red on Yellow, Kill a Fellow; admit for 24 – 48 hour observation!• immobilize, wrap, obs/admit, antivenin• If allergic - Antivenin is diluted and can be given with epinephrine.