Embed Size (px)
Citation preview
BOARD OF DIRECTORS
13th OCTOBER 2010
BOARD OF DIRECTORS
Agenda for the meeting to be held on Wednesday 13th October 2010 at 2.00pm in the Education Centre, 1st Floor West Wing,
250 Euston Road, London NW1 2PG 1. Apologies for Absence 2. Minutes of the Meeting held on 8th September 2010 Attachment A 3. Matters Arising Report Attachment B 4. Other urgent matters not appearing on the Matters Arising Report 5. Infection Control Annual Report: Presentation Annette Jeanes, Director of Infection Prevention and Control 6. Chairman’s Report Attachment C 7. Chief Executive’s Report Attachment D 8. Executive Board Report Attachment E 9. Performance Report Attachment F 10. Quality & Safety Committee Report Attachment G 11. HR & Communications Report Attachment H 12. Finance & Contracting Committee Report Attachment I 13. Report of the Audit Committee Meeting held on 23rd September Attachment J 14. Minutes of the Audit Committee Meeting held on 16th August Attachment K 15. Entries in the Seal Register Attachment L 16. Schedule of Board Meetings 2011 Attachment M 17. Any Other Business 18. Date of Next Meeting: The next meeting will be held on Wednesday 10th November 2010
A
Agenda Item 2
Minutes of the Meeting held on 8th September 2010
UNIVERSITY COLLEGE LONDON HOSPITALS NHS FOUNDATION TRUST
BOARD OF DIRECTORS
Minutes of the Meeting held on 8th September 2010
Present: Richard Murley, Chairman Sue Atkinson, Non-Executive Director Richard Delbridge, Non-Executive Director Nick Monck, Non-Executive Director Jane Ramsey, Non-Executive Director Richard Alexander, Finance Director Geoff Bellingan, Medical Director, Surgery & Cancer Louise Boden, Chief Nurse Mike Foster, Deputy Chief Executive Gill Gaskin, Medical Director, Specialist Hospitals Paul Glynne, Medical Director, Medicine Tony Mundy, Corporate Medical Director Robert Naylor, Chief Executive In attendance: Tonia Ramsden, Director of Corporate Services (Board
Secretary) Simon Knight, Interim Director of Performance & Partnerships Julia Whitehouse, Interim Director of Workforce Jocelyn Laws, Trust Administrator (Minutes) 09/1 Apologies for Absence Apologies were received from John Tooke and David Wherrett. 09/2 Minutes of the Meeting held on 11th August 2010 The minutes were agreed to be a correct record. 09/3 Matters Arising Report The report was noted. 09/4 Other Matters Arising not appearing on the Matters Arising Report Following the circulation of a report from the Director of Strategic Development on engagement with GPs, it was noted that proposals for taking forward the initiatives outlined in the report would be brought to the Board in October.
Action: Chief Executive/Director of Strategic Development
09/5 Chairman’s Report The Chairman provided an oral report. He advised that he had attended a ceremony with the Chief Executive at which a time capsule had been buried under the Cancer Centre. He also reported that he wished to appoint a vice chairman to the Board and following consultation with the non-executive directors he had asked Nick Monck to take on the role. 09/6 Chief Executive’s Report 09/6.1 National Hospital for Neurology and Neurosurgery The report advised that BBC News were recording an item at the
NHNN on an innovative treatment for cluster headaches, using deep brain stimulation. Board members would be advised of the date the item would be aired, once known.
Action: Director of Corporate Services
09/7 Executive Board Report 09/7.1 Capital and Estates Issues The Board noted that the EB had approved a number of schemes from the Capital Programme. 09/7.2 Five Digit Renumbering Project The Trust had commenced a project to replace the current mix of
four and five digit extensions with new five digit extensions for all departments and staff. The benefits of the change included a single switchboard number for all sites, greater availability of direct dial extensions and the elimination of duplicate numbers which would prevent misdirected calls. A communication strategy was being developed to support implementation of the new numbering system which was planned for early in the new year.
09/7.3 Revisions to Standing Financial Instructions (SFIs) and Scheme
of Delegation The report advised that, following an interim review, the EB had
endorsed changes to sections of the SFIs and Scheme of Delegation relating to procurement and tendering, and general amendments to reflect changes in EU thresholds and names of Government bodies. The most significant change was the inclusion of provision for electronic tendering. A summary of the changes was attached for Board approval.
2
The Board approved the revisions, subject to checking the delegated limits for approving capital works contracts as there was an inconsistency in the figures.
Action: Director of Corporate Services
09/8 Performance Report Simon Knight presented the report and referred to the activity summary.
While day case and non-elective activity was ahead of plan, elective activity was below plan. Clinical Boards had strategies in place to meet activity targets but the full year plan for gastrointestinal services may be difficult to achieve.
We were compliant with the 18 week target on a Trust-wide basis but were
below the threshold for urology, both for admitted and non-admitted pathways. Geoff Bellingan said it would be very challenging to meet the target in urology, partly owing to consultant staffing issues which meant that a number of complex procedures had had to be cancelled. The Chief Executive proposed that a urology exception report be provided for the next meeting. This was agreed.
Action: Medical Director, Surgery & Cancer/ Interim Director of Performance & Partnerships
The Trust was compliant with all cancer targets with the exception of the 62
day wait for first treatment from screening. Failure to meet the target had been caused by one breach which was beyond the Trust’s control. The position would continue to be monitored.
The Trust had performed exceptionally well on the A&E four hour wait target
and was the only Trust in London to have achieved over 99% year-to-date. There had also been an improvement in the number of last minute cancelled operations which had reduced from 1.2% in June to 0.7%. Gill Gaskin felt that the problems at The Heart Hospital had largely been resolved.
In response to a question from the Chairman, Geoff Bellingan outlined the
measures that were being taken to meet elective activity and access targets over the Winter. New patient pathways were being introduced which would reduce average lengths of stay but it would take time for the full effect to be achieved; therefore, although pressures would be reduced it was still anticipated that there would be difficulties.
Board members were advised that at the end of August the Trust had 6 cases
of MRSA bacteraemias against an annual threshold of 8. Despite having implemented a number of initiatives aimed at further reducing the incidence of MRSA, the risk of the target being breached remained high. The Chief Executive reminded the Board that we had previously highlighted this as a risk since the threshold which had reduced significantly from previous years was extremely challenging. Many other trusts were struggling and some had exceeded their threshold in the first quarter of the year. The Board agreed that Monitor should formally be advised of the position.
Action: Chief Executive
3
Paul Glynne emphasised that the Trust had made continuous improvements in reducing MRSA. Each case was subject to a root cause analysis which had indicated that there were no factors common to each case. He believed the Trust was adopting best practice and doing everything possible to reduce hospital-acquired MRSA. The EB had, that morning, approved a business case for extending wound surveillance and embedding infection control nurses across the Trust. A ward safety checklist was also being implemented. Good education, attention to hand hygiene and care procedures for IV lines were crucial to reducing infection risk and we were already implementing these. The Trust was fully committed to meeting the threshold; he was confident that the measures we had implemented would enable us to do so in future years.
There was a view that in future there would be more focus on all infection, not
just MRSA and C.difficile. At the October meeting the Board would receive the annual Infection Control report. The Chairman asked that the presentation cover the totality of our infection control strategy.
Action: Medical Director, Medicine
Simon Knight then drew attention to the patient experience metrics. Performance on complaints responded to within agreed timescales had improved and was now above the 85% target. Overall rating of care received was still slightly below target; however, responses to the composite measures indicated satisfaction was improving. It was felt that reporting against this one indicator may not be the best monitoring tool for the Board. The Chairman agreed that we should focus on individual indicators as a means of monitoring patient satisfaction.
Sue Atkinson noted that appraisal rates were still below target. Julia
Whitehouse advised that they were measured on a rolling 12 month period and rates varied considerably from month to month. Consideration was being given to recording appraisal rates for a 12 month static period.
Nick Monck expressed concern that a high proportion of CQUIN indicators
had still not been agreed. Simon Knight said this should be resolved soon and the Trust would be challenging any targets it felt were unreasonable, given the time short time left this year to achieve them.
The Chairman referred to a recent article in the Health Service Journal about
performance reporting in Nottingham which assessed the quality of the performance data as well as performance itself. He had discussed this with Simon Knight; we would look at our data and see whether there was anything to be learned.
09/9 Finance & Contracting Committee Report Jane Ramsey highlighted the Month 4 financial performance summary which
was £0.3m ahead of plan. She also drew attention to the contracting update, in particular the issue of commissioner intentions to restrict access to patients for ‘low priority procedures’. Mike Foster said that, to date, there had been no
4
refusals from commissioners to fund treatments but the position would become clearer in the next month or two.
The remaining issues in the report were noted. 09/10 Report of the Audit Committee Meeting held on 16th August 2010 Nick Monck presented the report summarising the main points of discussion,
which were noted. 09/11 Minutes of the Audit Committee Meeting held on 3rd June 2010 The minutes were noted. 09/12 Minutes of the Audit Committee Meeting held on 22nd July 2010 The extraordinary meeting had considered PwC’s dry-run of external
assurance on the Quality Report. The minutes were noted. 09/13 Entries in the Seal Register The report was noted. 09/14 Any Other Business There was none. 09/15 Date of Next Meeting The next meeting would be held on 13th October 2010. The Board of Directors resolved that representatives of the press and other members of the public be excluded from the remainder of the meeting, having regard to the confidential nature of the business to be transacted, publicity on which would be prejudicial to the public interest.
5
B
Agenda Item 3
Matters Arising Report
UNIVERSITY COLLEGE LONDON HOSPITALS NHS FOUNDATION TRUST
BOARD OF DIRECTORS
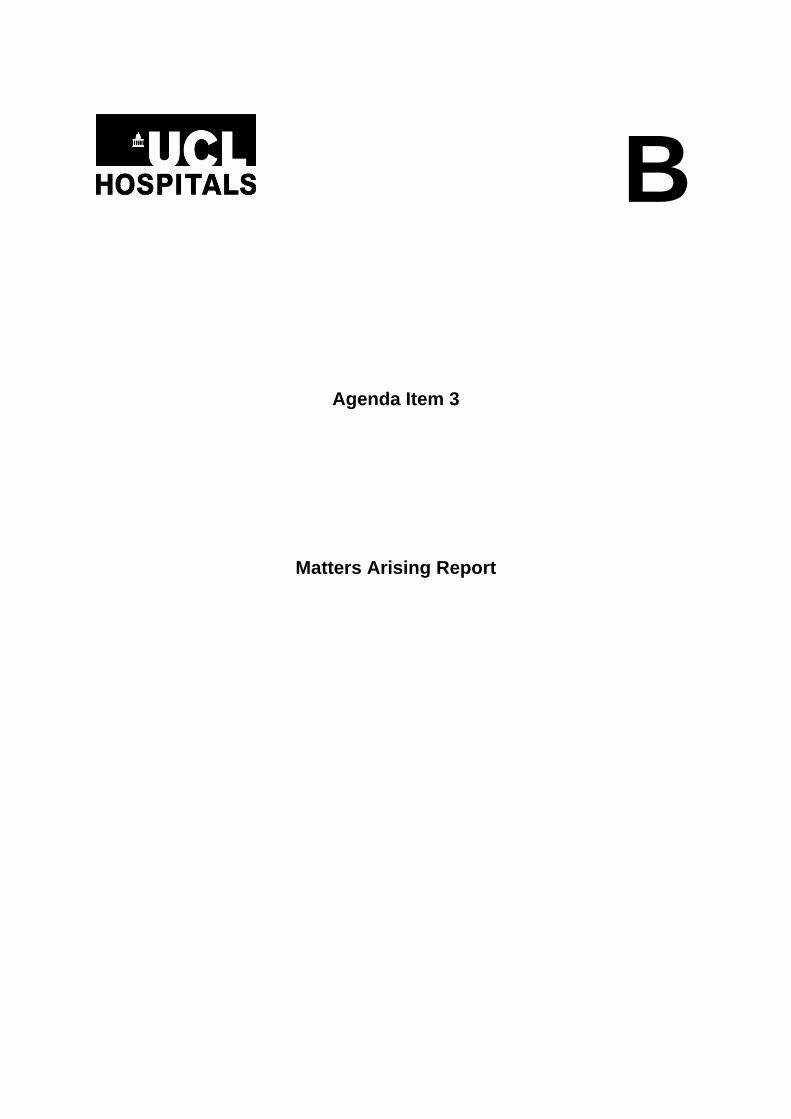
REPORT ON MATTERS ARISING FROM THE MEETING HELD ON 8th SEPTEMBER 2010
Minute
no. Issue Outcome
09/4 Bring proposals for taking forward initiatives outlined in the report on GP engagement
A report is attached to the EB report. Action completed.
09/6.1 BBC News item on innovative treatment for cluster headaches
The Board will be advised of the date of broadcast once known.
09/7.3 Revisions to Standing Financial Instructions and Scheme of Delegation – check delegated limits for approving capital works contracts.
The figures were amended and the revised SFIs/SoD uploaded on the Trust’s intranet. Action completed.
09/8 Performance report: Exception report on urology waiting times
This issue in included the Performance report. Action completed.
09/8 Performance report: Advise Monitor of the risk of breaching the MRSA target
A letter has been sent to Monitor. Action completed.
Items from previous meetings brought forward
Date of Meeting
Minute ref.no.
Issue Action
August 2010
8/10 HR & Communications Committee report: Explore reasons for new ER cases
The quarterly Employee Relations Performance Report will be reviewed at the October Committee and an update presented to the Board of Directors meeting in November. This will include a review of the number and type of cases, their duration and outcomes.
April 2010 4/3 Matters Arising report: Homeless Health Project - progress report to be presented to the Board in October.
An update is included in the Executive Board report. Action completed.
Items from previous meetings carried forward to future meetings
Date of Meeting
Minute ref.no.
Issue Action
August 2010
8/9 Quality & Safety Committee report: Develop proposals for revised complaints-handling system
It was intended that proposals would be considered by the QSC in October and presented to the Board in November. However, this has been deferred pending new information on complaints handling, due to be published by the Ombudsman. It will therefore be considered by the QSC in November and presented to the Board in December.
July 2010 7/6.1 Arrange Board seminar for detailed discussion on QEP.
It has been agreed that QEP issues will form part of the Board seminar in January. Action completed.
C
Agenda Item 6
Chairman’s Report
UNIVERSITY COLLEGE LONDON HOSPITALS NHS FOUNDATION TRUST
CHAIRMAN’S REPORT TO THE BOARD OF DIRECTORS
13 OCTOBER 2010
1. NHS WHITE PAPER
I have attended a number of conferences and seminars discussing the implications of the White Paper. It is clear that there remains a lot of uncertainty about the details of how the NHS will operate under the new regime. However, there is universal concern about how the service is going to cope with the proposed level of change whilst also dealing with the impending funding constraints. The Governors and the Board held a seminar on 15 September to discuss the proposals in the White Paper. The conclusions reached were reflected in the Trust’s response to the consultation process. The response is attached to the Chief Executive’s Report.
2. NORTH CENTRAL LONDON
There is a significant financial deficit among the North Central London Primary Care Trusts which is a matter of real concern for the sector. I have attended meetings of Chairs at NHS London and at the North Central London level which have discussed this issue and what will be done about it. There is no doubt that the commissioners will be seeking to share the burden with acute Trusts and UCLH is considering carefully how to respond to this. We are less directly affected than other acute Trusts in the sector, given the spread of our activities, but the pressures being felt in our sector are likely to be an indication of what is to come elsewhere.
3. CANCER CENTRE
On 13 October the Secretary of State for Health, Andrew Lansley, is visiting the new Cancer Centre site to mark the very generous donation from Macmillan Cancer Care which will help to fund the Centre.
4. ROYAL LONDON HOSPITAL FOR INTEGRATED MEDICINE
There have been two very successful occasions to mark the renaming of the Royal London Homeopathic Hospital as the Royal London Hospital for Integrated Medicine. On 16th September I attended an open day for staff and patients where the hospital staff had gone to considerable trouble to prepare some very interesting stalls about the range of activities which the hospital undertakes. It was particularly striking to hear the stories from patients about what the treatments on offer had achieved. Then on 20th September, there was a series of presentations for external stakeholders explaining some of the works of the hospital and further marking the renaming. The renaming will more accurately reflect the scope of activities of the hospital and the way in which its staff work alongside conventional treatments on offer in the Trust and elsewhere in the NHS.
5. HEART HOSPITAL – MRI/CATH LAB
On 13th September Robert Naylor and I attended the formal opening by Frank Dobson MP of the new MRI scanner and Cath Lab at the Heart Hospital. These exciting new facilities add significantly to the services which THH can offer to its
1
patients. We must thank the generosity of Queen Square Enterprises Limited, a company which is owned by UCLH Charities, who funded the MRI scanner.
6. ANNUAL PUBLIC MEETING AND SERVICE COMMITMENT AWARDS
The Annual Public Meeting of the Trust took place 30th September. The meeting was well attended and heard presentations from Robert Naylor and Richard Alexander about the Trust’s strategic and financial position. We also heard excellent presentations about two areas of clinical activity: on the Hyper Acute Stroke Unit from Nick Loseff and the on brain tumour service at Queen Square from Joan Grieve, Consultant Neurosurgeon. The Trust’s Annual Service Commitment Awards ceremony followed the APM. This event goes from strength to strength and there were about 150 nominations this year from staff and patients. Many congratulations to all those who were nominated and in particular to the winners: Cynthia Dako (Staff Nurse, T13 South) – Patient Nominated Individual award; Kristina Albizu – Staff Nominated Individual Award and the Sterile Services team in the Tower – Staff Nominated Team Award.
RICHARD MURLEY CHAIRMAN
2
D
Agenda Item 7
Chief Executive’s Report
UNIVERSITY COLLEGE LONDON HOSPITALS NHS FOUNDATION TRUST
CHIEF EXECUTIVE’S REPORT TO THE BOARD OF DIRECTORS
13 OCTOBER 2010
1. EQUITY AND EXCELLENCE: LIBERATING THE NHS – WHITE PAPER RESPONSE
The Trust has now submitted its response to the Government’s White Paper and the associated consultation documents. The Trust’s response is attached as Appendix ‘A’ and was submitted in time for the deadline of 5 October. The Trust’s response was formulated following a seminar with Governors and members of the Board. A draft was prepared and circulated for comment to members of the Board of Directors and to Veronica Beechey on behalf of the Governors. These comments were incorporated into the final submission. The general direction of the Trust’s response is supportive of many aspects of the White Paper, particularly those relating to reducing bureaucracy, transformation to Foundation Trust status for all providers and the emphasis on quality and Patient Choice. The main area of concern relates to proposals concerning GP commissioning, both in terms of scope and speed of implementation. It is noteworthy that many other respondents, as reported in the media, have made a similar observation, including organisations such as the BMA, RCN and the Royal College of General Practitioners. It is anticipated that legislation will be introduced to the House of Commons at the turn of the year and we hope that the Coalition Government takes due notice of the responses to consultation.
2. COMMISSIONING AND CONTRACT FUNDING
The Board should be aware that there have been many discussions, both internally and externally, on the financial problems that have emerged with PCT commissioners. Particlular problems appear to be concentrated in the outer London PCTs but the impact will be widespread. In the North Central London sector the main challenge occurs in Barnet, Enfield and Haringey PCTs, from which we receive about 15% of our referrals. These problems were discussed in detail at the Finance & Contracting Committee and will be referred to in its report to the Board. The Finance & Contracting Committee also discussed progress with the Quality, Efficiency and Productivity programme (QEP) which is intended to counterbalance the consequences of funding reductions from commissioners (mainly PCTs). Progress with the QEP is now included in a new section of the Board performance pack (included elsewhere on this agenda). In summary, the QEP annual target savings of £26.5m (to be achieved through efficiency and productivity) is broadly on target. At the Month 5 position there is a residual gap of £1.1m for which additional efficiency and productivity proposals are being developed. These largely involve reducing expenditure on temporary/agency staff, terminating some historical payments for extra duties and curtailing expenditure on external consultants. I am confident that this small residual gap will be closed well before the end of the financial year. The QEP targets for subsequent years are increasingly challenging and uncertain. Much depends upon the outcome of the comprehensive spending review and its impact on the NHS. The continued deteriorating financial position of commissioners is particularly concerning as is the Trust’s ability to continue to achieve efficiency and productivity savings of the order of 5% per annum over at least the next three years.
1
To counterbalance the pessimistic financial outlook, I am pleased to inform the Board that we have received verbal assurance that the additional funding for specialist activity (Project Diamond) will be substantially funded in the current financial year. It may well be that we will have received written assurances by the time of the Board meeting.
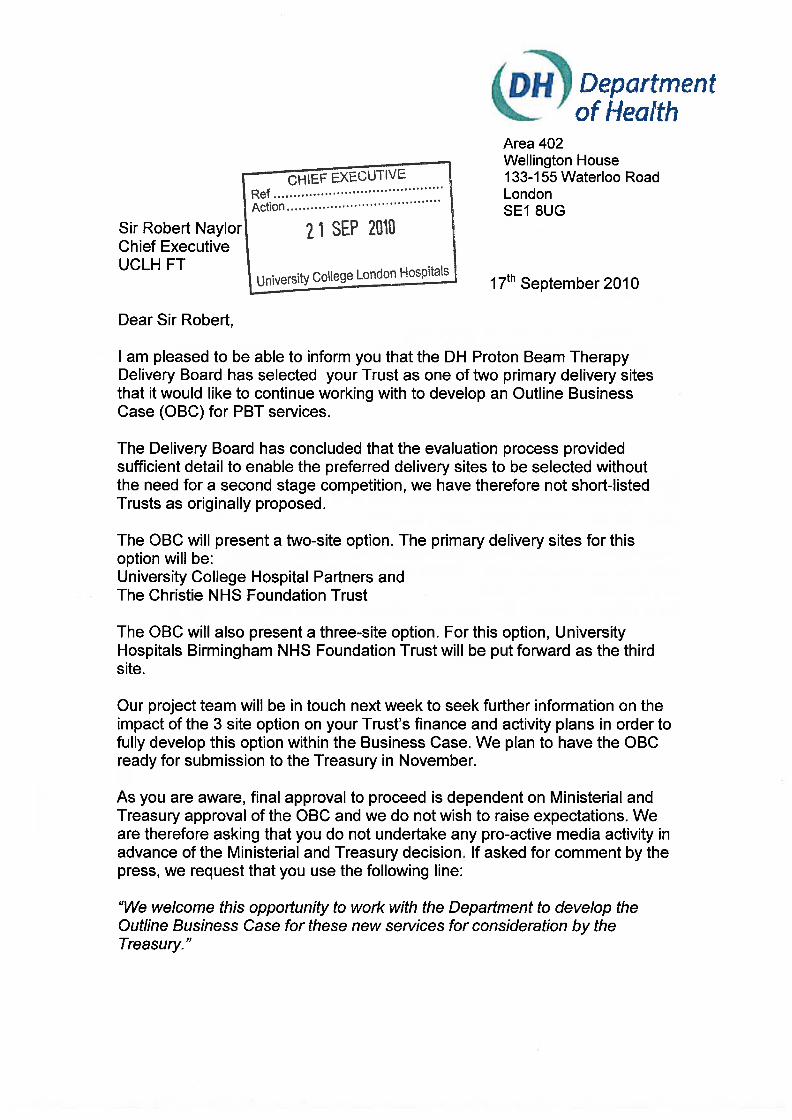
3. PROTON BEAM THERAPY
I am delighted to inform the Board that the Trust has been accepted as the preferred delivery site, without the need for a second-stage competition, to develop the first Proton Beam Therapy unit in the NHS. A copy of the confirmatory letter from the Department of Health is attached as Appendix ‘B’. The Board will recollect that our proposal is to deliver a national Proton Beam Therapy service in collaboration with the Christie Hospital in Manchester. This two-site proposal has been chosen as the primary delivery option and we have been invited to develop an outline business case which should also include a third site option to include the University Hospital Birmingham. Our preferred site for the development of Proton Beam Therapy is the below ground area of the proposed Phase 4 development on the Rosenheim/Odeon site. This is directly adjacent (and connected by underground tunnels) to the new Cancer Centre currently under construction, the UCL Cancer Institute and the main University College Hospital site. We will be preparing a parallel business case for the above-ground component of this development, which may include a replacement for the Eastman Dental Hospital and the Royal National Throat, Nose & Ear Hospital (subject to transfer of this facility from the Royal Free Hospital as previously agreed in principle). This development, in conjunction with the new Cancer Centre, will greatly enhance the capability and reputation of our cancer services. Furthermore, we are in preliminary discussions with Barts and the Royal London Hospitals to seek ways in which we can collaborate on the provision of cancer services to improve quality and reduce unnecessary duplication.
4. PET/MRI
The Trust has commissioned preliminary work to explore the possibility of installing a PET/MRI (Positron Emission Tomography/Magnetic Resonance Imaging) facility in the lower ground floor of the new Cancer Centre currently in construction. If approved, this would be one of the first such installations in the world and the first in Europe. UCLH was the first Trust to develop the combined modality of PET/CT (Computerised Tomography) at the Middlesex Hospital more than a decade ago. We currently have two such machines in the new hospital which are used in advanced diagnostics for a range of conditions, predominantly cancer. The new modality to include MRI, will offer fantastic opportunities for both clinical diagnosis and research and development. The cost of PET/MRI, including installation, is likely to be in the region of £6m and we are currently bidding to philanthropic sources for funding. Subject to the outcome of those bids the UCLH Charity has kindly agreed to underwrite the costs, subject to the acceptance of design feasibility and business case appraisal.
2
5. OLYMPIC LEGACY ISSUES
I have periodically reported progress in our engagement with the British Olympic Association and the Department of Health on matters concerning the 2012 Olympic Games. I am now pleased to report significant progress in collaboration between a number of organisations and the establishment of a new Institute for Sports, Exercise and Health jointly between UCL and UCLH. I attach as Appendix ‘C’ a briefing paper which sets out our preliminary proposals and a bid to the Department of Health for £10m to support our initiatives. We have some degree of confidence that these proposals will be supported at national level, largely because they represent an excellent example of collaboration between the majority of the leading players in this field and the fact that this will go some considerable way to delivering the Government’s 2012 Olympic Legacy commitment on health and exercise.
SIR ROBERT NAYLOR CHIEF EXECUTIVE
3
UCLH NHS FT WHITE PAPER RESPONSE Page 1 of 6
Chief Executive’s Report to the Board of Directors
Appendix A White Paper team Room 601 Department of Health 79 Whitehall London SW1A 2NS
University College Hospital London NHS Foundation Trust’s Response to the NHS White Paper Consultation
Introduction University College London Hospitals NHS Foundation Trust (UCLH) welcomes the opportunity to respond to the Department of Health’s consultation on the Health White Paper ‘Equity and Excellence: Liberating the NHS’. Our response has been developed taking into account the views of Board Members and Governors who have considered not just the White Paper but the key issues arsing from the supporting consultation documents. UCLH has used its freedoms as one of the first Foundation Trusts (FTs) to both improve its performance and provide a better quality and more responsive service to its patients. Last year it was designated the top performing Trust in the NHS. UCLH is supportive of much of the Coalition Government’s ideas and welcomes the White Paper’s proposals that all trusts should have the opportunity to become FTs. We also welcome the focus on improving patient choice and outcomes, the continued commitment to independent regulation and the proposed new freedoms for FTs. However, we are concerned about a number of aspects of the proposals on commissioning, especially those relating to general practitioners (GP's) and their capacity and commitment to embrace the changes proposed and the timetable for implementation. Furthermore, the absence of detail for arrangements to protect the highly specialised tertiary services that predominate in London are also of concern to us. We have a number of observations and specific comments which are outlined below. Regulation We support the direction towards greater freedom for FTs to operate under the control of an economic regulator and towards an environment where all trusts are foundation trusts. We note the magnitude of the proposed changes and trust that due consideration will be given to the competing pressures on management time to both respond to the extremely challenging financial environment and to manage the implementation of the proposed changes while continuing to maintain high quality care. We welcome the proposal to relax the merger and acquisition restrictions and consider it is a critical assurance that the bar for attaining foundation trust status will remain high. We would be very concerned at any proposals to lower that bar. We also believe that it is crucial to the delivery of effective and efficient healthcare that those trusts which are unable to meet the high criteria necessary to be authorised as FT’s are advised of this in a timely and unequivocal manner to give them sufficient time to seek alternative options/organisational arrangements before the final deadline for FT application.

UCLH NHS FT WHITE PAPER RESPONSE Page 2 of 6
A relatively small proportion of UCLH's income comes from treating private patients and we have no current plans to significantly increase this. However, we recognise that the Private Patient Income (PPI) Cap has limited the ability of some FTs to attract additional resources to invest in care pathways which could significantly benefit NHS patients and therefore we support the removal of the PPI Cap. We support the removal of statutory controls upon borrowing by FTs. We would be interested in investigating the concept of a foundation trust ‘bank’ where surpluses within the system could be recycled, risks shared and healthcare specific investment expertise developed. We would be keen to explore further the opportunities of greater freedom for FTs within the constraints of what is realistically affordable. The current regulatory regime works well with a light touch approach and greater intervention where appropriate. We are in agreement with the outline role of Monitor as economic regulator and, in the interest of efficiency and an appropriate level of bureaucracy, support the concentration of regulatory and statutory compliance into as few bodies as possible. We agree that the tax-payers’ investment in FTs should be utilised to gain the maximum benefit for NHS patients and support this coming under the control of Monitor. We believe that the tax-payer should be assured of the efficiency of regulators in the same way they as receive assurance about the efficiency of other healthcare providers. Therefore, should Monitor charge a fee the total regulatory costs should be subject to the same cost efficiency requirement as apply to the general healthcare economy. For the FT model to successfully drive both efficiency and quality it is fundamental that providers are paid and commissioners charged for the actual nature and volume of services commissioned and delivered. Tariff pricing needs to reflect as far as is practical the cost of delivering each procedure covered by each tariff point. Where this is not practical due to, for example, unpredictable small volumes, highly complex and individual treatment requirements, overlap between research and treatment etc. then fair remuneration models must be developed in consultation with providers and the NHS Commissioning Board. We would expect it to be possible to appeal against pricing and pricing methodologies whenever it could be shown that the impact of the methodology was seen to discourage (financially) the preferred provider of the service. In the interest of patient access we would expect this to be subject to a special licence condition. We agree Monitor should have both pricing and licensing powers to protect the tax-payer and patients against the creation of financially or logistically unsustainable treatments or procedures which could arise as a result of an unregulated level playing field where new providers could select and specialise in profitable treatment areas relying upon ‘emergency service providers’ to handle the exceptional, highly unprofitable, cases. Similarly we would want Monitor to have powers to impose additional regulation to help commissioners maintain access to essential services (as identified by the NHS Commissioning Board) and that this should be supported by a consistent pricing strategy. We are concerned that competition should never be based on price alone, and that there should always be a level playing field among the NHS, private and third sector providers. We would welcome assurance on these matters. Commissioning for Patients We understand the proposal to further devolve decision-making about patient care but consider that it will be a challenge for GPs to take on a commissioning role particularly when there will be a need to reduce management costs and achieve efficiency savings. There is real concern that GPs will not have the right level of commitment, expertise and experience. We are also concerned that there is a potential conflict of interest if
UCLH NHS FT WHITE PAPER RESPONSE Page 3 of 6
GPs are expected both to be advocates for their patients and to manage declining resources. In principle we do not believe that GP consortia, as proposed, will be successful. They will increase bureaucracy and cost, as well as potentially destabilise the financial position of hospital providers. Having said this, the following comments assume that they will be established. We consider that the NHS Commissioning Board should ensure that GP consortia are tested for their ‘fitness for purpose’. We recommend that the Commissioning Board should licence individual GP consortia to operate (in the same way that Monitor licences FTs through their terms of authorisation) following a rigorous and appropriate process. This process would ensure that consortia have the necessary expertise, experience and skills to plan, manage and financially control multi-million pound commissioning organisations accountable for spending public money. Core skills, for example in relation to negotiation, forecasting, risk management and of course core financial control will all require relevant experience and demonstrable expertise. Many PCTs have failed to demonstrate adequate capability in these areas and there is no evidence to suggest that a larger number of GP consortia will be more successful. It is essential to provide an assurance framework and clear accountability for effective stewardship of public funds, particularly as the consultation makes clear there will be no bail-outs for overspending organisations. Regarding holding consortia to account we recommend that the Commissioning Board establish a performance regime similar to the regulatory framework Monitor has in place. Like the FT framework one would expect this to take a proportionate regulatory approach and set measurable standards which improve quality and choice. Currently PCTs have Boards with independently appointed non-executive directors to oversee their governance. We consider it essential for good governance that consortia be aligned to best practice in the public sector. The establishment of a chief executive position should only be open to those who can demonstrate relevant experience including a successful track record of managing a substantial public sector or commercial organisation. If GP consortia are going to be held accountable for holding individual GP practices to account it is important that they can equally demonstrate they are being efficiently, effectively and economically managed. In our view, this can only be delivered through an appropriately established ‘Board of Directors’ comprising both experienced executives and non-executive directors, the latter to safeguard the interests of patients. There is also concern being expressed by provider trusts that they may be expected to develop bespoke pathways for individual consortia or indeed individual practices. If this is replicated across a number of consortia this would place an unmanageable burden on providers. UCLH is a large national teaching hospital which provides a wide variety of complex specialist services. We already have contracts with 150 PCTs. If the number of consortia were significantly higher than this, we could be faced with the prospect of negotiating contracts and patient pathways with an unrealistic number of different bodies placing a significant bureaucratic strain on the system. We are also concerned about how high quality patient care would be maintained, about equality of access and the possible creation of a ‘postcode lottery’ for NHS treatment. This must be avoided. For pathway development we would suggest a host/lead commissioner be identified to take responsibility on behalf of all commissioners for establishing core clinical pathways for all patients referred to a provider (or group of providers). Having raised a number of concerns about commissioning we recommend that the proposal as currently outlined is clarified and, if necessary, reconsidered. The government could propose an upper limit on GP consortia in the short term.
UCLH NHS FT WHITE PAPER RESPONSE Page 4 of 6
We are particularly concerned that there is little or no recognition of the additional costs associated with complex and specialist hospital activity. The tariff fails to sufficiently recognise complexity of case-mix and the additional costs of teaching and research. Furthermore it is silent on the ways in which tertiary activity will be commissioned, bearing in mind that these patients will rarely be seen by individual GPs and their local consortia colleagues – a greater proportion of cases will need to be commissioned regionally or nationally. The Outcomes Framework We welcome the proposal to shift the focus from process to outcomes and that the framework will include both clinical and patient reported outcome indicators. We agree that this shift will strengthen performance and quality and deliver real benefit to patients. We are also pleased that the quality definitions of effectiveness, safety and patient experience will remain central to the framework. We are in broad agreement with the principles that underpin the development of the ‘Outcomes Framework’ including the structure of the five domains. The concentration on areas which have not hitherto had high profile attention such as premature mortality, infant mortality, healthy life expectancy at 65 and enhancing the quality of life for people with long-term conditions is appropriate. However, we are concerned that waiting times will no longer be an indicator. Through the development of surgical and other appropriate pathways we have improved patient outcomes and patient experience and feel that there is a significant risk to service quality should those gains made in reducing waiting times be lost. We suggest that the continued improvement of waiting times to prevent deterioration of both outcomes and patient experience should be retained in some form within the framework. Similarly we support extending the use of PROMs and making more use of standard tools such as EQ-5D which, as they have been in use for some time, have a proven track record. However, our recent experience of the national condition specific PROMs is that they have taken too long to develop and bring into use. National PROMs data have also taken too long to get to the provider and are not available in a form which enables organisational learning to take place within individual hospitals. This will need to improve if these tools are to be used to enable FTs and other organisations to support their improvement agendas. We welcome the proposal to develop a new generation of outcome indicators for patient experience in the long term whilst retaining existing surveys in the short term in tandem with the plan to place more focus on specialist surveys. However, whilst we understand the approach to be used to track patient experience we are concerned about the proposed use of composite scores. We believe that these could obscure poor performing areas (which can be compensated for by high performing areas in the composite scores). These could lead to a false view that organisations are performing better than underlying survey data would indicate. UCLH has made significant improvements in developing qualitative methods to help understand how patients experience their care and to improve the quality of care. We would like to see qualitative evidence being used alongside quantative data in evaluating outcomes. With regard to the descriptor for the safety domain ‘Treating and caring for people in a safe environment and protecting them from avoidable harm’ - our view is that the overarching indicator is too focused on error and mistakes (incidents), rather than preventable and unintended consequences (adverse events). A concern has been expressed by clinicians that the focus on incidents could result in less willingness to report which will weaken the objective. As an organisation UCLH values the importance of openness about mistakes and encourages reporting however, incidents in and of
UCLH NHS FT WHITE PAPER RESPONSE Page 5 of 6
themselves are considered a poor indicator of harm (IHI); and research suggests that only 1 in 10 incidents are reported by clinicians nationally. Similarly we believe that the improvement areas outlined lack the ambition found in the other domains which stretch or focus on new areas for improvement. We would also question whether ‘safety culture’ can be considered an outcome. We believe it to be an enabler providing a safe and effective quality service to patients and do not agree that ‘openness about mistakes’ is necessarily indicative of a safe culture. Two further points were raised during our discussions. We noted the emphasis on public health, but are concerned about how the issue of joint accountability between local authority and NHS organisations might be managed. In the light of this, we wonder whether a specific domain could be developed to support the public health agenda. Secondly, we note that individual organisations will be held to account for the outcomes it alone can influence. However, in several of the domains, e.g. enhancing the quality of life for people with long term conditions, patient care is likely to be provided by a combination of sectors. We are unclear how the outcomes framework will deal with multiple and interconnected responsibilities for patient care.
Research and Development – AHSCs We welcome the importance given to Academic Health Science Centres (AHSC), for research to be seen as a core role within the NHS, and for the commitment to research funding going forward. We consider that AHSCs have a key role in fulfilling the ambition set for the NHS to achieve ‘world class results’. AHSCs are fundamental in delivering health improvement and contributing to wealth creation in the UK through translational research. We acknowledge the need for providers to be paid according to their performance, with payments reflecting outcomes not activity. Suitable and sustainable arrangements need to be made to ensure that:
• the commissioning arrangements are able and willing to commission the specialised services from AHSCs (and other specialist tertiary providers) that are required at a regional and national level;
• tariff prices reflect the true cost of this care;
• commissioners are willing to pay for the evidence-based interventions that small groups of patients require; and
• competition and maximum pricing do not become further disincentives to provide the most complex and costly care.
Equally, the commissioning of research needs to be managed at a national level. Given the scale of the financial challenges ahead, those functions which are not economically viable because of the current funding arrangements will be especially vulnerable. It would be appropriate to channel research to centres of both excellence and scale, such as the AHSCs, to maximise the benefit that the investment can bring. Education and Training The White Paper highlights the need for further debate on the future of commissioning for education and training in healthcare. We believe that Teaching Hospitals and AHSCs in particular have a crucial role to play in this both regionally and nationally, in conjunction with HIECs. There is a strong case for the responsibility for commissioning education and training to rest with employers, as it would do in any other industry. This should be informed by the highest standards of practice and research, tested against the best in the world.
UCLH NHS FT WHITE PAPER RESPONSE Page 6 of 6
Summary In summary, we believe that some aspects of the White Paper’s proposals for improving the NHS – patient choice, improving outcomes, enhancing regulation and increasing local democracy – are the right ones. We have some concern however, that the move to increase competition could be detrimental to the patterns of partnership working, which have been successfully developed in recent years, (for example the reconfiguration of stroke services which entails co-operation between hyper-acute stroke units, local hospitals and GP services). The transition to a new system will not be easy and is likely to be very costly. There will be risks in the short term, but a clear implementation plan with further consultation on key areas of change, could help to lessen the risks in the longer term. We would caution against the radical proposal to transform commissioning which will create significant financial risks in both the short and long term. These include a possible impact on choice and quality both of which are key areas for improvement in the White Paper. We would suggest that in order to minimise risk, a pilot study of the proposals, especially those concerning GP commissioning, should be carried out before any large scale implementation. Sir Robert Naylor Chief Executive On behalf of the UCLH Board of Directors and Governors 4th October 2010
CHIEF EXECUTIVE’S REPORT TO BOARD OF DIRECTORS 13 OCTOBER 2010 – APPENDIX C
Institute of Sports, Exercise and Health
2012 Olympic Legacy Proposal
Background A successful collaborative working relationship has been developed between four leading organisations; University College London Hospitals NHS Foundation Trust (UCLH), University College London (UCL), British Olympic Association (BOA) and HCA (Hospital Corporation of America), with the objective of developing an Institute of Sport, Exercise and Health in Central London which could play a pivotal role in a National legacy to deliver “more medals for our athletes and better health for the nation” from the 2012 Olympics. Regional and National Context The Department of Health has recently established two new committees – The Sports & Exercise Policy Forum and The Sports & Exercise Working Group, led by Mike Farrar and run by Stephen Colegrave – Project Manager and Drs Leon Creaney and Richard Weiler, Consultant sin Sports and Exercise Medicine and specialist advisors to the DH. The groups are attended by the CEOs (or delegated representatives) from key organisations across the UK. These include NHS Trusts with an interest in Sports Medicine (e.g. UCLH, The East Midland Cluster of Loughborough, Leicester and Nottingham, Warwick and Sheffield), as well as organisations such as the British Olympic Association, English Institute of Sports, UK Sport, The Faculty of Sport and Exercise Medicine and the Armed Forces. The purpose of these groups is to establish clearer working relationships between the existing centres of excellence; to minimise duplication and to further improve research, teaching and clinical capability. Proposal As indicated in the first section of this paper, UCLH has been working with other key organisations to establish an Institute for Sports, Exercise and Health. The DH has indicated that it would support and fund a single capital development within the UK, to support the national network of expertise whilst providing a single ‘hub’ and subsequent Olympic legacy. As a consequence of this, the UCLH team has analysed the possibilities in preparation to bid for any DH funding that might be available. Following a robust review of the viability of developing an Institute for Sport, Exercise and Health, the Project Board believes that the following provision could be delivered by the end of 2011. It is proposed that the model of ‘hub and spoke’ would best deliver the clinical care required by the clients using the Institute. The Institute would bring together clinicians and academics in order to evaluate patients, diagnose their problems and prescribe treatment. It would act as a clinical and academic hub with treatment delivered at a variety of partner specialist centres. For
CHIEF EXECUTIVE’S REPORT TO BOARD OF DIRECTORS 13 OCTOBER 2010 – APPENDIX C
example, a client requiring surgery could undergo their operation within the well established theatres at UCLH, with a private provider or at their referring centre / region. The Institute would deliver “best of the best” across the following elements, with leading edge solutions being developed through a unique multi-disciplinary approach:
• Outpatient facilities and diagnostics for clients (elite, professional, weekend warriors, private and NHS). This unit would be utilised initially by colleagues from the English Institute of Sport (EIS) as well as NHS and private consultants.
• ‘Sign-posting’ to treatment options at specialist ‘spoke’ sites. • Rehabilitation gymnasium space for assessment and tertiary
rehabilitation input and prescription. • World class sport science research and education. • Home for the British Olympic Medical Institute Research and Acute
rehabilitation units. • Academic space for teaching, for the training of Sports Physicians and
Allied Specialties, and to facilitate translational research. The combination and co-location of the personnel involved will enable world class research and education to be translated into clinical practice for the benefit of patients locally, nationally and internationally. As well as serving local populations, it is expected that the Institute would play a leading role in co-ordinating research and disseminating best practice across the UK. It is envisaged that this will drive health programmes including exercise prescription within the community to help reduce morbidity and mortality related to obesity, diabetes and other chronic diseases. Sited within the UCLH and UCL campus, in close proximity to the BOA Headquarters, the Institute will be located within central London, with easy access from mainline stations, notably Euston and Kings Cross. Funding The modelling demonstrates that the above proposal could be delivered across 1835sqm for a capital cost of approximately £10m. Potential sites are being reviewed by the UCLH Capital and Estates department, to identify those available for refurbishment within the required timeframe, suitable for the facilities required and with the potential for expansion. A grant of this amount would allow the development and establishment of the Institute within the required timeframe; i.e. prior to the Olympics in 2012.
E
Agenda Item 8
Executive Board Report
UNIVERSITY COLLEGE LONDON HOSPITALS NHS FOUNDATION TRUST
Executive Board Report to
the Board of Directors, October 2010 1. Infection Control Annual Report 2009/10
The EB considered the above report, which has been circulated to Board members and is referred to in the Quality & Safety Committee report. The EB commends the report to the Board for approval and endorsement of the action plan following which it will placed on the Trust’s website. The Director of Infection Prevention and Control, Annette Jeanes, will attend the Board meeting to give a presentation on infection.
2. GP Engagement Strategy Following the publication of the NHS White Paper, the EB discussed a range of options for how UCLH could respond to the implementation of GP commissioning. A GP & Community Services Working Group (GPWG), chaired by Paul Glynne, was set up to develop a response. The EB considered a paper which sets out the recommendations from the first phase of their work. The EB supported the recommendations of the GPWG to develop a more
comprehensive approach to engagement with GPs. The strategy report is attached at Appendix A for Board comment. Board members may wish to consider whether GP engagement should feature in the Trust’s top 10 objectives for next year.
3. Annual Nursing & Midwifery Report The EB approved the Annual Nursing & Midwifery Report 2010 which covers highlights of the past year’s nursing and midwifery activity and staff achievements in relation to the five key objectives of the UCLH Nursing & Midwifery Strategy (2008 – 2011):
Improving the Patient Experience Effective Leadership Research and Innovation in Practice Improving Working Lives Education and Continuing Professional Development
The report also covers achievements aligned with UCLH Top 10 objectives and examples of how issues arising from Frequent Feedback / Inpatient Survey have been addressed in the clinical areas. The report has been circulated separately to Board members for information and will be placed on the Trust’s website.
4. Capital and Estates Issues On the recommendation of the Capital Investment Board, the EB approved a
number of schemes from the approved Capital Programme. These include replacement of a Holmium Laser in Surgery at UCH, works to meet fire and health & safety compliance regulations at various sites, and replacement of boilers at Arthur Stanley House which will result in a significant reduction in costs of standing gas charges.
The EB also approved in principle a scheme to fit out space in the EGA wing
for the relocation of Medical Physics from the Rosenheim Building and the provision of a bed store. This scheme represents the first phase of the decanting of the Rosenheim Building and was approved for submission to the Investment Committee subject to a further report to the EB confirming plans to address any shortfall in funding for the remaining Rosenheim decant schemes.
The EB also agreed that guidelines should be drawn up to assist in deciding,
on a case by case basis, whether leasing or purchasing large items of medical equipment represents better value for money.
5. Homeless Health Project The Board has previously been informed of this project and agreed that a
further update should be submitted after 6 months. The EB received a report from Professor Aidan Halligan advising of progress. A new post of London Pathway Homeless Health Practitioner (part of the Discharge Team) was recruited to in September. The post is funded until March 2011 by the clinical boards. Short-term funding for the rest of the team has been secured by a £100k grant from the clinical boards.
It has recently been confirmed that a bid to the Health Foundation ‘Closing the
Gap’ fund for £400k has been successful. This funding is provided over the next 2½ years to help develop and promote the model of care pioneered at UCH and adapt the model for acute trusts across London and the UK. The funding was awarded because our innovative approach transforms the patient experience and can be introduced across the NHS. Progress continues on the formation of a new London Pathway Charity to promote the benefits of this approach and encourage its uptake by other acute trusts.
The service has been selected as an exemplar innovation site by the new
College of Medicine, which is to be launched on 28th October and will have a Faculty for Homeless Care.
6. Annual Plan Outline Process The Planning Steering Group – a sub-committee of the EB - has reviewed how the Trust will take on board the key lessons learned from the 2010/11 planning round. The EB approved the outline process and timetable for developing the 2011/12 Annual Plan.
2
The aim will be to bring likely key planning themes to the EB for consideration in October 2010. These themes will be reviewed again in February/March 2011 and any other emerging issues will be fed into the final top ten objectives. Identifying these themes early in the process will support more robust planning and eventual delivery. It will also meet a new Monitor requirement that we involve governors and members in setting objectives. The annual series of planning seminars for the governors, led by the Medical Directors, has been organised to take place during November and December; the final seminar led by the Chief Executive will take place in January, after a Board discussion has taken place on the Trust’s strategy. A detailed timetable and planning guidance for each of the supporting workstreams will be produced by the Planning Steering Group during October. 7. Emergency Preparedness The EB received a report from Louise Boden which covered issues such as
preparations for the 2012 Olympics and business continuity planning. The EB also noted that the flu planning and vaccination campaign has been launched.
SIR ROBERT NAYLOR CHIEF EXECUTIVE
3
Executive Board Report to the Board of Directors Appendix A
GP Engagement Strategy
1. Background The NHS White Paper set out a significant change to NHS commissioning arrangements with GPs taking on a lead role1. Consortia of GP practices will commission the great majority of NHS services on behalf of patients, including elective hospital care and rehabilitative care, urgent and emergency care (including out-of-hours services, most community health services, and mental health and learning disability services. The current implementation plan for GP commissioning: • In 2011/12: A comprehensive system of shadow GP consortia in place • In 2013/14: GP consortia to be fully operational with real budgets and holding contracts
with providers 2. Purpose of the paper This paper sets out the recommendations from the first phase of the work by the GPWG which has focussed on how UCLH can develop a more comprehensive approach to GP engagement. This has three workstreams: • Responding to development areas identified in the GP survey • Improving GP engagement processes • Setting up a programme of GP visits 3. Findings from the latest GP survey The latest GP survey (2009/10) generated 197 responses from the 1687 GPs who received posted hard copies, a response rate of 11.6%. The feedback we receive from the survey has been relatively consistent over the last few years. GPs refer to UCLH because of its convenience, its modern appearance and state-of-the-art facilities. Major strengths are the quality of clinical staff, patient care and the fact that UCLH is a specialist hospital trust. GPs described their clinical priorities when considering referring as access to dedicated specialist centres, the ability to contact consultants by fax/email and modern facilities and equipment. In terms of appointment, access and availability issues, waiting times for appointments and ease of contacting the hospital were high on the agenda.
The GPWG has undertaken a full analysis of the results of this years GP survey. Some of the top issues identified in the GP survey provide a steer for the programme of activities to take forward (# responses in brackets) (see Annex 1 for full list): • Improving access to clinical teams to discuss patient case (23) • Reducing delays/problems with appointment letters, clinic letters, test results etc (26) • More responsive, 'customer service' approach to GPs via switchboard, med secs,
website, clinic staff (45) • Improving A&E discharge information/comments about A&E (17) • GP communications - educational events, information about services etc (17) The GPWG has identified existing initiatives already underway in the trust as part of other programmes of work and mapped them to the development areas identified by the GP survey. 23 activities with identified leads are ongoing (see Annex 2 for full details). These include the GP portal and the work of the E discharge group on improving discharge information. The GPWG is now engaging with the leads for each of the activities identified to establish planned delivery dates. Two areas identified as development areas do not have substantial activity already planned: • Improving access to clinical teams to discuss patient cases • Improving choose and book - named consultants and services available.
1 DH (2010) Liberating the NHS: Commissioning for patients
The GPWG plans to work with clinical, communications and choose & book leads to develop proposals to address these gaps. 4. Improving GP engagement processes There are currently a number of processes to engage with GPs. All provide an effective method of engagement, but could be improved. Annex 3 sets out a list of current GP engagement activities undertaken by the trust and options to improve these processes. The GPWG recommends to EB that the following activities are undertaken as the first initial phase of improving GP engagement:
• GP Links: improving quality of newsletter; send GP Links to more individual GPs and practices. Design from current budget; No change in recurring costs unless the Trust decides to post the newsletter to more GPs
• GP survey. Conduct survey annually to improve quality of data. No cost impact unless EB would like to use an external market research agency
• GP database. An accurate database with up-to-date GP contact information is created. No costs
The GPWG will bring back a comprehensive engagement plan in its next quarterly report to EB. 5. Setting up a programme of GP visits A number of UCLH clinicians already visit or meet local GPs on an ad-hoc ongoing basis (for example Steve Hurel). To build on this and demonstrate to the GP community UCLH’s commitment to new policy environment. The GPWG recommends that a programme of corporate visits is undertaken to the top 10 referring practice by end December 2010 and the practices that our analysis suggests offer major opportunities by end March 2011 (based on Dr Foster analysis, see Annex 4 for full list and details on the visits. Large local practices with registered patient numbers in excess of 8000 and with lower UCLH referral rates than the top 10 are identified as those that offer referral opportunities for UCLH). A series of corporate visits were undertaken in 2008. Following a discussion with Nicky Besag (who organised the visits) the lessons learned are to: • Focus on a small number of practices (ten highest referrers) • Ensure we have good corporate material and information to take on the visits • Develop a feedback loop/ongoing dialogue – one of the key reasons the visits were
perceived as an inefficient use of time was that there was no feedback loop/ongoing dialogue between the GP practice and the Trust following the visit
• Use the visits as part of a wider engagement strategy to link with the GP liaison committee and the GP survey
6. Governance for the programme of activities From the work undertake to existing activity underway in the trust to the issues identified in the GP survey it is clear that the trust already has a lot of work underway but it is not co-ordinated in any way and there is no mechanism to inform the GP community that we are doing anything about the concerns that they have raised. The GPWG recommends to EB that:
• The GPWG takes a co-ordinating role, monitoring progress on a light touch basis on the various activities underway in the trust in order that it is in a position to track progress on the issues raised by GPs and identify any gaps which may need to be addressed
• The GPWG works through the GP Liaison Committee (Daniel Wallis the chair of the Committee is a member of the GPWG) to feedback on a regular basis to GP representatives progress and seek feedback
• With the onset of GP commissioning, the ToR, membership and arrangements for the GP Liaison Committee will need to be reviewed.
• The GPWG updates EB on progress on a quarterly basis 7. Phase 2: Developing partnership opportunities with GPs The Phase 1 activity identified above by the GPWG provides an initial response to improve engagement with GPs. A second phase of work is being scoped. A range of different approaches of partnering with GPs are emerging – the move to GP commissioning will likely lead to further developments in this area. Some of these approaches are based on developing longer term partnership arrangements others on more tactical initiatives. Examples include both Imperial and Kings exploring with local GPs an integrated care model along the lines of an HMO for their local areas. We have some experience of working in partnership with the local GP community from our recent bid for Camden Provider services and are in discussions with them regarding the scope to create a Chronic disease centre at Stephenson House. The GPWG proposes to scope a range of possible ways forward including partnership models, such as the integrated care model and whether we need to develop a more comprehensive marketing strategy for example for GPs outside NCL who refer patients to our specialist areas of activity. Although the White Paper provides new opportunities to engage with GPs, the uncertainty over the structure and timeline, particularly over GP commissioning, provide a period of time to develop longer-term options. There is currently no clarity regarding the exact configuration of consortia in Camden. However, as noted above, other providers are moving quickly into this space.
Annex 1: Key issues identified in GP survey The latest GP survey (2009/10) generated 197 responses from the 1687 GPs. Key issues identified in the survey included (# responses in brackets): • Improving A&E discharge information/comments about A&E (17) • Improving access to clinical teams to discuss patient case (23) • Reducing delays/problems with appointment letters, clinic letters, test results etc (26) • Offering better value for money, refining pathways, costs, unnecessary follow ups etc
(13) • Improving Choose and Book - named consultants and services available (17) • More responsive, 'customer service' approach to GPs via switchboard, med secs,
website, clinic staff (45) • Improving general discharge summaries to include more meaningful, accurate
information (4) • Reducing number of cancellations followed by appointments for many weeks later (4) • Improving access to patient information in GP surgeries (4) • Long waiting times for some appointments (19) • Communication about range of services to GPs outside immediate area (4) • Improve access for patients (3) • Building relationships with primary care to a view of working in partnership (6) • GP communications - educational events, information about services etc (17)
Annex 2: Current activities to deal with GP survey development areas Table 1 below set out the current response with leads for the identified development area
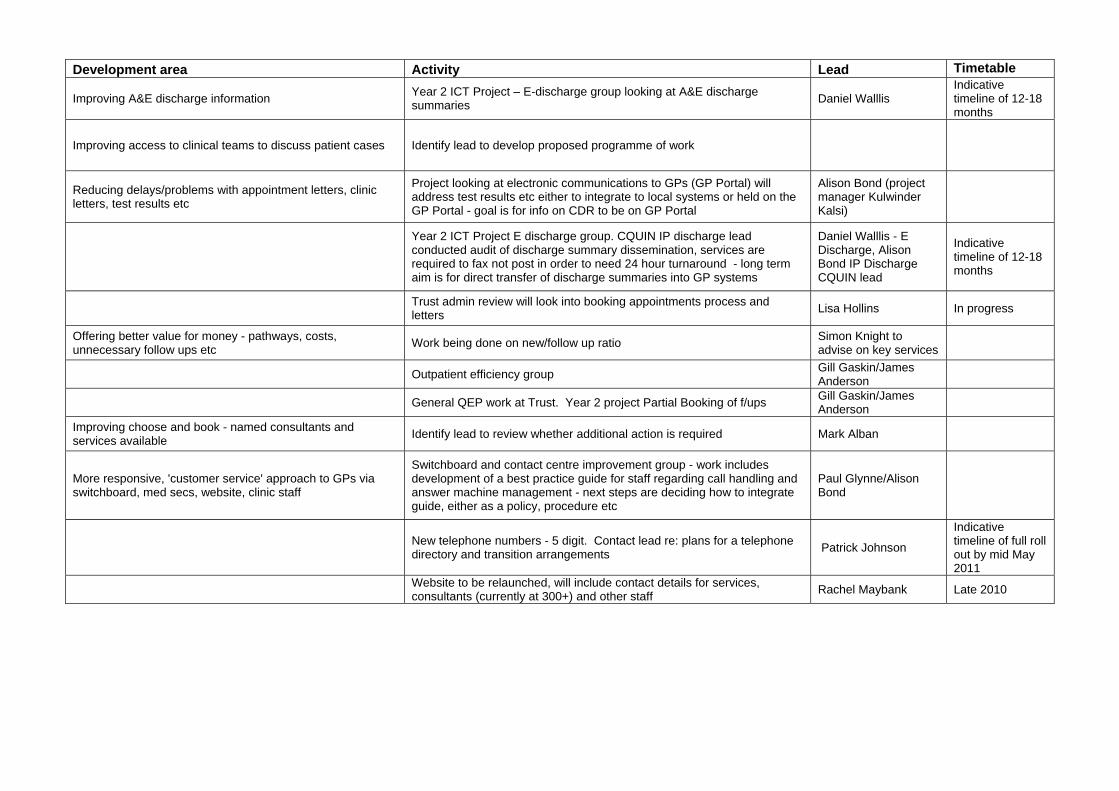
Development area Activity Lead Timetable
Improving A&E discharge information Year 2 ICT Project – E-discharge group looking at A&E discharge summaries Daniel Walllis
Indicative timeline of 12-18 months
Improving access to clinical teams to discuss patient cases Identify lead to develop proposed programme of work
Reducing delays/problems with appointment letters, clinic letters, test results etc
Project looking at electronic communications to GPs (GP Portal) will address test results etc either to integrate to local systems or held on the GP Portal - goal is for info on CDR to be on GP Portal
Alison Bond (project manager Kulwinder Kalsi)
Year 2 ICT Project E discharge group. CQUIN IP discharge lead conducted audit of discharge summary dissemination, services are required to fax not post in order to need 24 hour turnaround - long term aim is for direct transfer of discharge summaries into GP systems
Daniel Walllis - E Discharge, Alison Bond IP Discharge CQUIN lead
Indicative timeline of 12-18 months
Trust admin review will look into booking appointments process and letters Lisa Hollins In progress
Offering better value for money - pathways, costs, unnecessary follow ups etc Work being done on new/follow up ratio Simon Knight to
advise on key services
Outpatient efficiency group Gill Gaskin/James Anderson
General QEP work at Trust. Year 2 project Partial Booking of f/ups Gill Gaskin/James Anderson
Improving choose and book - named consultants and services available Identify lead to review whether additional action is required Mark Alban
More responsive, 'customer service' approach to GPs via switchboard, med secs, website, clinic staff
Switchboard and contact centre improvement group - work includes development of a best practice guide for staff regarding call handling and answer machine management - next steps are deciding how to integrate guide, either as a policy, procedure etc
Paul Glynne/Alison Bond
New telephone numbers - 5 digit. Contact lead re: plans for a telephone directory and transition arrangements Patrick Johnson
Indicative timeline of full roll out by mid May 2011
Website to be relaunched, will include contact details for services, consultants (currently at 300+) and other staff Rachel Maybank Late 2010
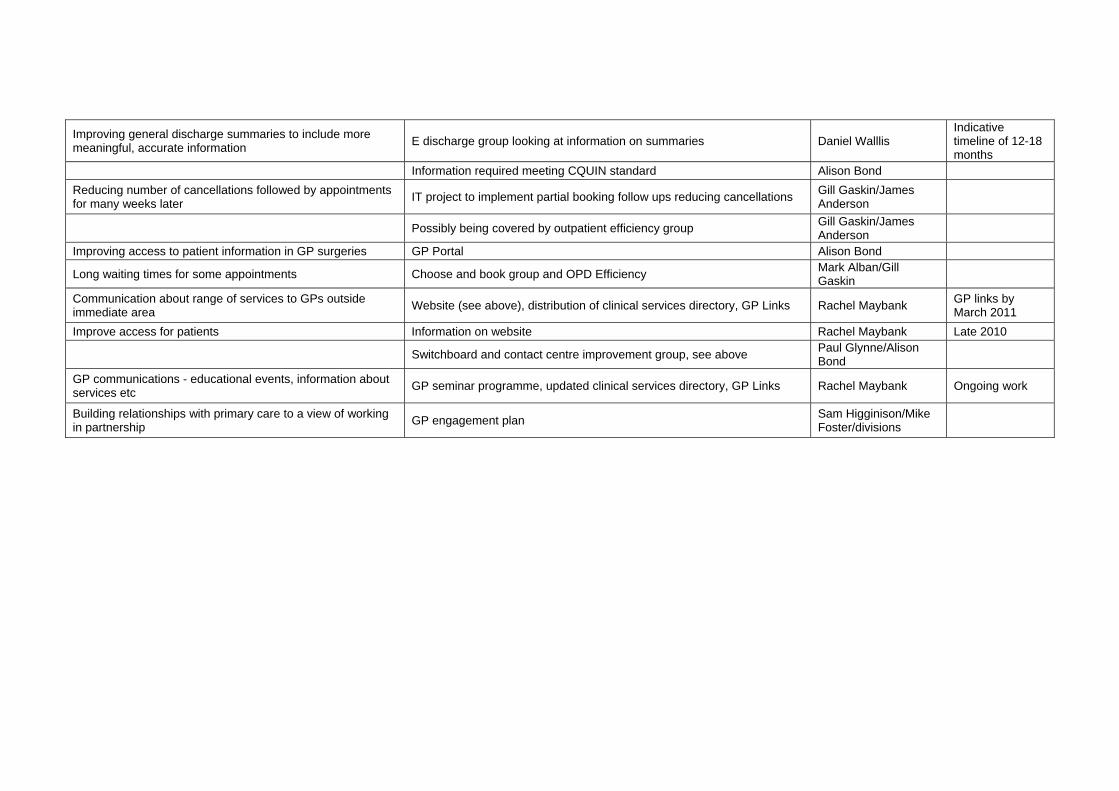
Improving general discharge summaries to include more meaningful, accurate information E discharge group looking at information on summaries Daniel Walllis
Indicative timeline of 12-18 months
Information required meeting CQUIN standard Alison Bond Reducing number of cancellations followed by appointments for many weeks later IT project to implement partial booking follow ups reducing cancellations Gill Gaskin/James
Anderson
Possibly being covered by outpatient efficiency group Gill Gaskin/James Anderson
Improving access to patient information in GP surgeries GP Portal Alison Bond
Long waiting times for some appointments Choose and book group and OPD Efficiency Mark Alban/Gill Gaskin
Communication about range of services to GPs outside immediate area Website (see above), distribution of clinical services directory, GP Links Rachel Maybank GP links by
March 2011 Improve access for patients Information on website Rachel Maybank Late 2010
Switchboard and contact centre improvement group, see above Paul Glynne/Alison Bond
GP communications - educational events, information about services etc GP seminar programme, updated clinical services directory, GP Links Rachel Maybank Ongoing work
Building relationships with primary care to a view of working in partnership GP engagement plan Sam Higginison/Mike
Foster/divisions
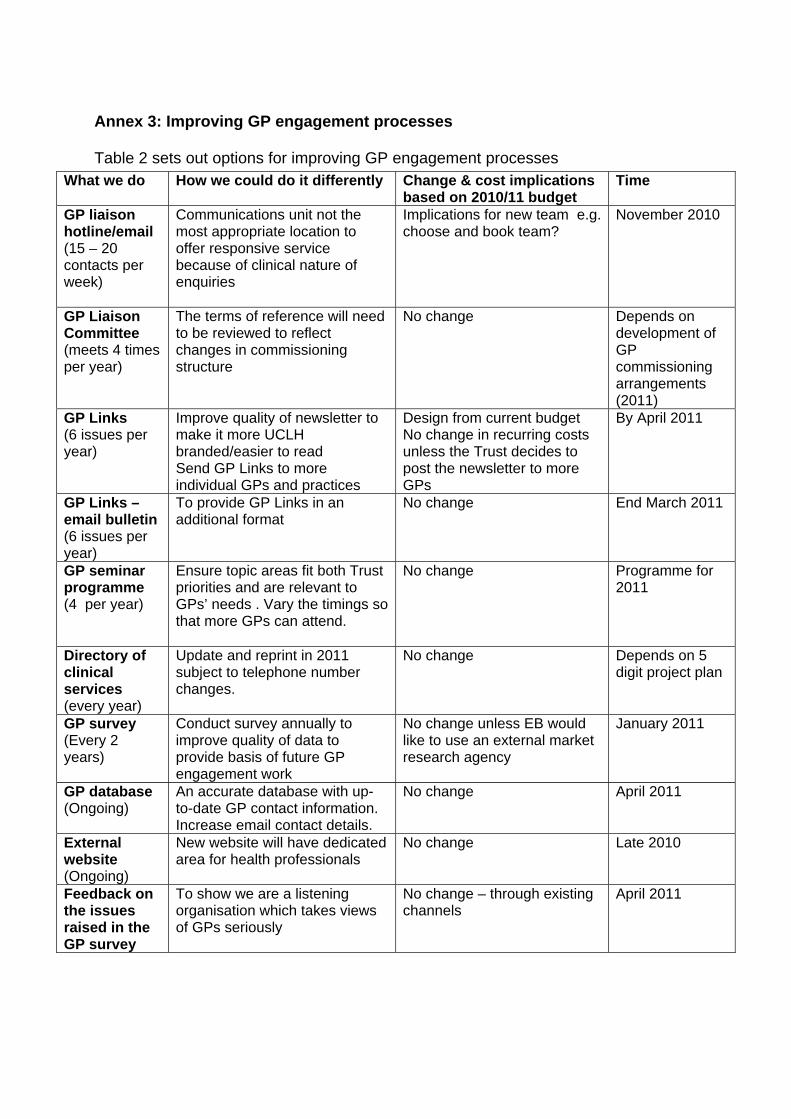
Annex 3: Improving GP engagement processes Table 2 sets out options for improving GP engagement processes
What we do How we could do it differently Change & cost implications based on 2010/11 budget
Time
GP liaison hotline/email (15 – 20 contacts per week)
Communications unit not the most appropriate location to offer responsive service because of clinical nature of enquiries
Implications for new team e.g. choose and book team?
November 2010
GP Liaison Committee (meets 4 times per year)
The terms of reference will need to be reviewed to reflect changes in commissioning structure
No change Depends on development of GP commissioning arrangements (2011) By April 2011 GP Links
(6 issues per year)
Improve quality of newsletter to make it more UCLH branded/easier to read Send GP Links to more individual GPs and practices
Design from current budget No change in recurring costs unless the Trust decides to post the newsletter to more GPs
GP Links – email bulletin (6 issues per year)
To provide GP Links in an additional format
No change End March 2011
GP seminar programme (4 per year)
Ensure topic areas fit both Trust priorities and are relevant to GPs’ needs . Vary the timings so that more GPs can attend.
No change Programme for 2011
Directory of clinical services (every year)
Update and reprint in 2011 subject to telephone number changes.
No change Depends on 5 digit project plan
GP survey (Every 2 years)
Conduct survey annually to improve quality of data to provide basis of future GP engagement work
No change unless EB would like to use an external market research agency
January 2011
GP database (Ongoing)
An accurate database with up-to-date GP contact information. Increase email contact details.
No change April 2011
External website (Ongoing)
New website will have dedicated area for health professionals
No change Late 2010
Feedback on the issues raised in the GP survey
To show we are a listening organisation which takes views of GPs seriously
No change – through existing channels
April 2011
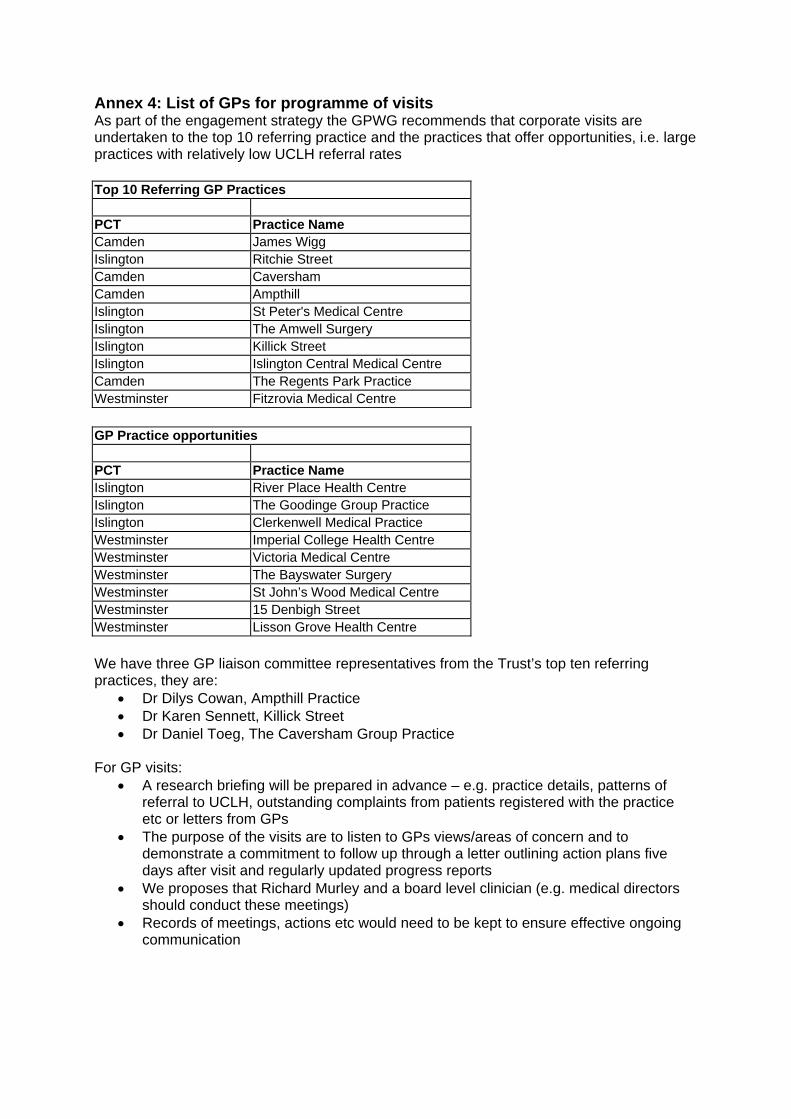
Annex 4: List of GPs for programme of visits As part of the engagement strategy the GPWG recommends that corporate visits are undertaken to the top 10 referring practice and the practices that offer opportunities, i.e. large practices with relatively low UCLH referral rates
Top 10 Referring GP Practices
PCT Practice Name Camden James Wigg Islington Ritchie Street Camden Caversham Camden Ampthill Islington St Peter's Medical Centre Islington The Amwell Surgery Islington Killick Street Islington Islington Central Medical Centre Camden The Regents Park Practice Westminster Fitzrovia Medical Centre
GP Practice opportunities
PCT Practice Name Islington River Place Health Centre Islington The Goodinge Group Practice Islington Clerkenwell Medical Practice Westminster Imperial College Health Centre Westminster Victoria Medical Centre Westminster The Bayswater Surgery Westminster St John’s Wood Medical Centre Westminster 15 Denbigh Street Westminster Lisson Grove Health Centre
We have three GP liaison committee representatives from the Trust’s top ten referring practices, they are:
• Dr Dilys Cowan, Ampthill Practice • Dr Karen Sennett, Killick Street • Dr Daniel Toeg, The Caversham Group Practice
For GP visits: • A research briefing will be prepared in advance – e.g. practice details, patterns of
referral to UCLH, outstanding complaints from patients registered with the practice etc or letters from GPs
• The purpose of the visits are to listen to GPs views/areas of concern and to demonstrate a commitment to follow up through a letter outlining action plans five days after visit and regularly updated progress reports
• We proposes that Richard Murley and a board level clinician (e.g. medical directors should conduct these meetings)
• Records of meetings, actions etc would need to be kept to ensure effective ongoing communication
F
Agenda Item 9
Performance Report
Page 1 of 1
UNIVERSITY COLLEGE LONDON HOSPITALS NHS FOUNDATION TRUST
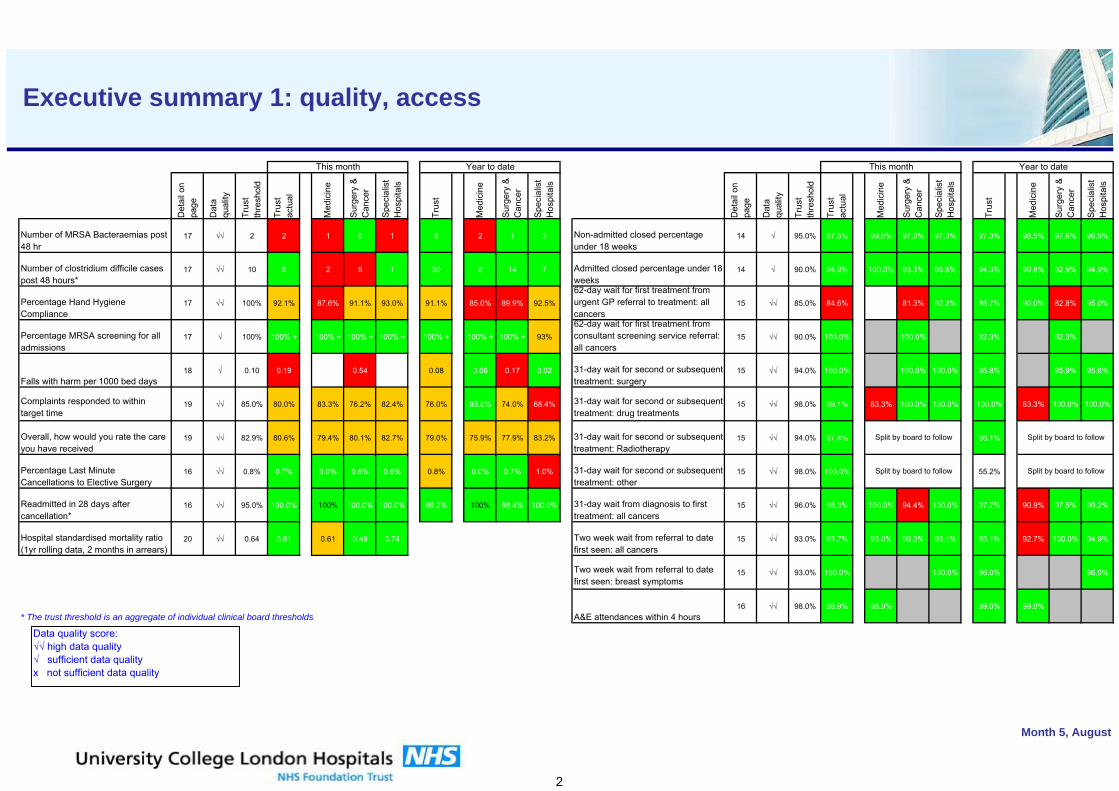
Report to Board of Directors Performance Pack for August 2010 This paper highlights changes to the format of the Board of Directors performance pack and some key performance issues from the report. Changes to content of performance pack: Providing additional focus on QEP:
• Replacement of QEP graphs with two new QEP financial analysis pages • New productivity page from FCC financial report
Learning from Nottingham performance reporting:
• Data quality assessment against indicators on the executive summary: introduction of subjective assessments based on the accuracy and completeness of the data used to compile measures and the confidence with which decisions can be made on the basis of the measure.
• Exception reports on key performance issues as annexes at the end of the pack. One page summaries for measures where there are significant or persistent performance issues.
We will be meeting with representatives from McKinsey who developed the performance pack at Nottingham to think about other opportunities for further improving our performance reporting. Key issues from August 2010 report: The following are key issues from the August 2010 report:
• Pre 11am indicator remains steady at around 19% against a 35% threshold (page 12)
• Continuing elective underperformance Trust-wide (page 13)
• Growing numbers of open non-admitted pathways reported as waiting greater than 52 weeks, against a zero threshold (page 14)
• Marginally under threshold on the 62 day from GP referral cancer wait indicator for August and for the quarter to date. (page 15)
• Continuing strong performance on A&E and cancelled operations (noting in particular maintenance of cancelled operations position in Specialist Hospitals) (page 17)
• Two cases of MRSA in August (page 18)
• An exception report on urology 18 week performance for admitted and non-admitted pathways at page 24.
Simon Knight Acting director of performance 7th October 2010
Month 5, August
This document contains commercially confidential information and must not be released or circulated
UCLH NHS Foundation Trust
Board of Directors Performance ReportOctober 2010
(Month 5 – August)
1. Executive summaries 2. Finance 3. Delivery of QEP4. Activity 5. Access 6. Patient Safety and Quality metrics 7. Workforce 8. Externally Reported Frameworks 9. Exceptions
Month 5, August
Contents
1
kurhgiudrhg
Det
ail o
n pa
ge
Dat
a qu
ality
Trus
t th
resh
old
Trus
t ac
tual
Med
icin
e
Surg
ery
& C
ance
r
Spec
ialis
t H
ospi
tals
Trus
t
Med
icin
e
Surg
ery
& C
ance
r
Spec
ialis
t H
ospi
tals
Det
ail o
n pa
ge
Dat
a qu
ality
Trus
t th
resh
old
Trus
t ac
tual
Med
icin
e
Surg
ery
& C
ance
r
Spec
ialis
t H
ospi
tals
Trus
t
Med
icin
e
Surg
ery
& C
ance
r
Spec
ialis
t H
ospi
tals
Number of MRSA Bacteraemias post 48 hr
17 √√ 2 2 1 0 1 6 2 1 3 Non-admitted closed percentage under 18 weeks
14 √ 95.0% 97.6% 99.6% 97.0% 97.3% 97.3% 98.5% 97.6% 96.9%
Number of clostridium difficile cases post 48 hours*
17 √√ 10 8 2 5 1 30 8 14 7 Admitted closed percentage under 18 weeks
14 √ 90.0% 94.9% 100.0% 93.3% 95.8% 94.3% 99.8% 92.9% 94.9%
Percentage Hand Hygiene Compliance
17 √√ 100% 92.1% 87.6% 91.1% 93.0% 91.1% 85.0% 89.9% 92.5%
62-day wait for first treatment from urgent GP referral to treatment: all cancers
15 √√ 85.0% 84.6% 81.3% 92.3% 86.7% 90.0% 82.8% 95.0%
Percentage MRSA screening for all admissions
17 √ 100% 100% + 100% + 100% + 100% + 100% + 100% + 100% + 93%
62-day wait for first treatment from consultant screening service referral: all cancers
15 √√ 90.0% 100.0% 100.0% 92.3% 92.3%
Falls with harm per 1000 bed days18 √ 0.10 0.19 0.54 0.08 0.06 0.17 0.02 31-day wait for second or subsequent
treatment: surgery15 √√ 94.0% 100.0% 100.0% 100.0% 95.8% 95.9% 95.6%
Complaints responded to within target time
19 √√ 85.0% 80.0% 83.3% 76.2% 82.4% 76.0% 93.8% 74.0% 68.4% 31-day wait for second or subsequent treatment: drug treatments
15 √√ 98.0% 99.1% 83.3% 100.0% 100.0% 100.0% 83.3% 100.0% 100.0%
Overall, how would you rate the care you have received
19 √√ 82.9% 80.6% 79.4% 80.1% 82.7% 79.0% 75.9% 77.9% 83.2% 31-day wait for second or subsequent treatment: Radiotherapy
15 √√ 94.0% 97.4% 98.1%
Percentage Last Minute Cancellations to Elective Surgery
16 √√ 0.8% 0.7% 0.0% 0.8% 0.8% 0.8% 0.0% 0.7% 1.0% 31-day wait for second or subsequent treatment: other
15 √√ 98.0% 100.0% 55.2%
Readmitted in 28 days after cancellation*
16 √√ 95.0% 100.0% 100% 100.0% 100.0% 99.2% 100% 98.4% 100.0% 31-day wait from diagnosis to first treatment: all cancers
15 √√ 96.0% 98.3% 100.0% 94.4% 100.0% 97.7% 90.9% 97.5% 99.2%
Hospital standardised mortality ratio (1yr rolling data, 2 months in arrears)
20 √√ 0.64 0.61 0.61 0.49 0.74 Two week wait from referral to date first seen: all cancers
15 √√ 93.0% 93.7% 93.0% 96.3% 93.1% 93.1% 92.7% 100.0% 94.9%
Two week wait from referral to date first seen: breast symptoms
15 √√ 93.0% 100.0% 100.0% 96.0% 96.0%
* The trust threshold is an aggregate of individual clinical board thresholds A&E attendances within 4 hours16 √√ 98.0% 98.9% 98.9% 99.0% 99.0%
Month 5, August
Split by board to follow Split by board to follow
This month Year to date
Split by board to follow Split by board to follow
This month Year to date
Executive summary 1: quality, access
Data quality score:√√ high data quality√ sufficient data qualityx not sufficient data quality
2
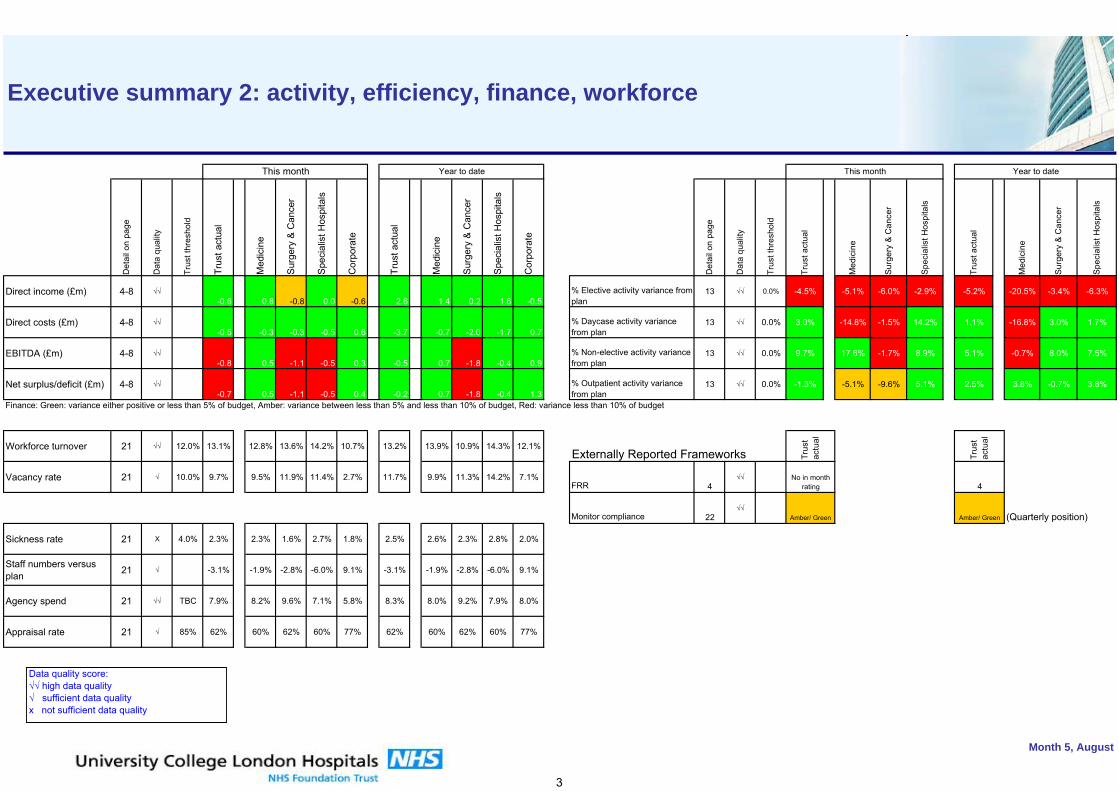
kurhgiudrhg
Det
ail o
n pa
ge
Dat
a qu
ality
Trus
t thr
esho
ld
Trus
t act
ual
Med
icin
e
Sur
gery
& C
ance
r
Spe
cial
ist H
ospi
tals
Cor
pora
te
Trus
t act
ual
Med
icin
e
Sur
gery
& C
ance
r
Spe
cial
ist H
ospi
tals
Cor
pora
te
Det
ail o
n pa
ge
Dat
a qu
ality
Trus
t thr
esho
ld
Trus
t act
ual
Med
icin
e
Surg
ery
& C
ance
r
Spec
ialis
t Hos
pita
ls
Trus
t act
ual
Med
icin
e
Surg
ery
& C
ance
r
Spec
ialis
t Hos
pita
ls
Direct income (£m) 4-8 √√-0.6 0.8 -0.8 0.0 -0.6 2.6 1.4 0.2 1.6 -0.5
% Elective activity variance from plan
13 √√ 0.0% -4.5% -5.1% -6.0% -2.9% -5.2% -20.5% -3.4% -6.3%
Direct costs (£m) 4-8 √√-0.5 -0.3 -0.3 -0.5 0.6 -3.7 -0.7 -2.0 -1.7 0.7
% Daycase activity variance from plan
13 √√ 0.0% 3.0% -14.8% -1.5% 14.2% 1.1% -16.8% 3.0% 1.7%
EBITDA (£m) 4-8 √√-0.8 0.5 -1.1 -0.5 0.3 -0.5 0.7 -1.8 -0.4 0.9
% Non-elective activity variance from plan
13 √√ 0.0% 9.7% 17.6% -1.7% 8.9% 5.1% -0.7% 8.0% 7.5%
Net surplus/deficit (£m) 4-8 √√-0.7 0.5 -1.1 -0.5 0.4 -0.2 0.7 -1.8 -0.4 1.3
% Outpatient activity variance from plan
13 √√ 0.0% -1.3% -5.1% -9.6% 5.1% 2.5% 3.8% -0.7% 3.8%
Finance: Green: variance either positive or less than 5% of budget, Amber: variance between less than 5% and less than 10% of budget, Red: variance less than 10% of budget
Workforce turnover 21 √√ 12.0% 13.1% 12.8% 13.6% 14.2% 10.7% 13.2% 13.9% 10.9% 14.3% 12.1%Externally Reported Frameworks
Vacancy rate 21 √ 10.0% 9.7% 9.5% 11.9% 11.4% 2.7% 11.7% 9.9% 11.3% 14.2% 7.1%FRR 4
√√
Monitor compliance 22√√
(Quarterly position)
Sickness rate 21 Χ 4.0% 2.3% 2.3% 1.6% 2.7% 1.8% 2.5% 2.6% 2.3% 2.8% 2.0%
Staff numbers versus plan 21 √ -3.1% -1.9% -2.8% -6.0% 9.1% -3.1% -1.9% -2.8% -6.0% 9.1%
Agency spend 21 √√ TBC 7.9% 8.2% 9.6% 7.1% 5.8% 8.3% 8.0% 9.2% 7.9% 8.0%
Appraisal rate 21 √ 85% 62% 60% 62% 60% 77% 62% 60% 62% 60% 77%
Month 5, August
Trus
t ac
tual
Trus
t ac
tual
Amber/ Green
4
Amber/ Green
No in month rating
This monthThis month Year to date Year to date
Executive summary 2: activity, efficiency, finance, workforce
Data quality score:√√ high data quality√ sufficient data qualityx not sufficient data quality
3
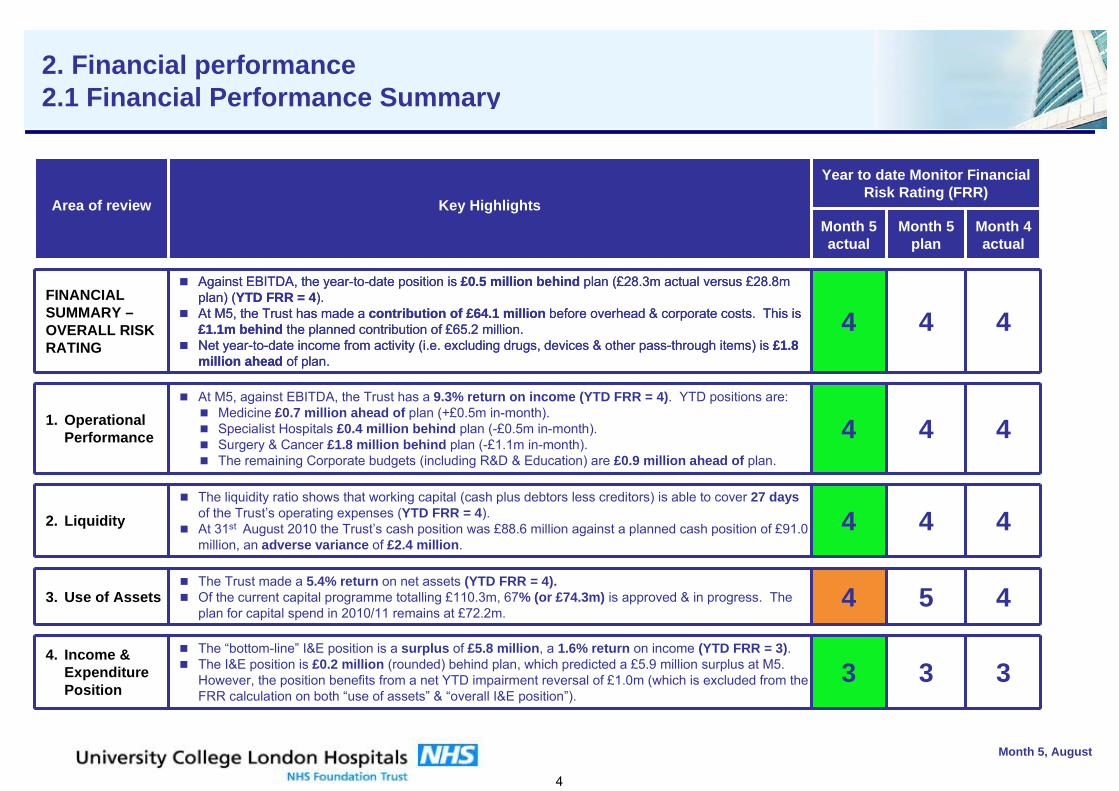
Month 5, August
Financial Summary- Overall Rating
Year to date rating
Month 5 Actual
Month 5 Plan
Month 4 Actual
5 4
Area of review Key Highlights
4. Overall I&E
1. Operational Performance
2. Liquidity
3. Use of Assets
2. Financial performance2.1 Financial Performance Summary
Year to date Monitor Financial Risk Rating (FRR)
3
4
4
4
4
Month 4 actual
Area of review Key HighlightsMonth 5 actual
Month 5 plan
FINANCIAL SUMMARY –OVERALL RISK RATING
Against EBITDA, the year-to-date position is £0.5 million behind plan (£28.3m actual versus £28.8m plan) (YTD FRR = 4).At M5, the Trust has made a contribution of £64.1 million before overhead & corporate costs. This is £1.1m behind the planned contribution of £65.2 million.Net year-to-date income from activity (i.e. excluding drugs, devices & other pass-through items) is £1.8 million ahead of plan.
4 4
1. Operational Performance
At M5, against EBITDA, the Trust has a 9.3% return on income (YTD FRR = 4). YTD positions are:Medicine £0.7 million ahead of plan (+£0.5m in-month).Specialist Hospitals £0.4 million behind plan (-£0.5m in-month).Surgery & Cancer £1.8 million behind plan (-£1.1m in-month).The remaining Corporate budgets (including R&D & Education) are £0.9 million ahead of plan.
4 4
2. LiquidityThe liquidity ratio shows that working capital (cash plus debtors less creditors) is able to cover 27 daysof the Trust’s operating expenses (YTD FRR = 4).At 31st August 2010 the Trust’s cash position was £88.6 million against a planned cash position of £91.0 million, an adverse variance of £2.4 million.
4 4
3. Use of AssetsThe Trust made a 5.4% return on net assets (YTD FRR = 4). Of the current capital programme totalling £110.3m, 67% (or £74.3m) is approved & in progress. The plan for capital spend in 2010/11 remains at £72.2m.
4 5
4. Income & Expenditure Position
The “bottom-line” I&E position is a surplus of £5.8 million, a 1.6% return on income (YTD FRR = 3). The I&E position is £0.2 million (rounded) behind plan, which predicted a £5.9 million surplus at M5.However, the position benefits from a net YTD impairment reversal of £1.0m (which is excluded from the FRR calculation on both “use of assets” & “overall I&E position”).
3 3
Year to date Monitor Financial Risk Rating (FRR)
3
4
4
4
4
Month 4 actual
Area of review Key HighlightsMonth 5 actual
Month 5 plan
FINANCIAL SUMMARY –OVERALL RISK RATING
Against EBITDA, the year-to-date position is £0.5 million behind plan (£28.3m actual versus £28.8m plan) (YTD FRR = 4).At M5, the Trust has made a contribution of £64.1 million before overhead & corporate costs. This is £1.1m behind the planned contribution of £65.2 million.Net year-to-date income from activity (i.e. excluding drugs, devices & other pass-through items) is £1.8 million ahead of plan.
4 4
1. Operational Performance
At M5, against EBITDA, the Trust has a 9.3% return on income (YTD FRR = 4). YTD positions are:Medicine £0.7 million ahead of plan (+£0.5m in-month).Specialist Hospitals £0.4 million behind plan (-£0.5m in-month).Surgery & Cancer £1.8 million behind plan (-£1.1m in-month).The remaining Corporate budgets (including R&D & Education) are £0.9 million ahead of plan.
4 4
2. LiquidityThe liquidity ratio shows that working capital (cash plus debtors less creditors) is able to cover 27 daysof the Trust’s operating expenses (YTD FRR = 4).At 31st August 2010 the Trust’s cash position was £88.6 million against a planned cash position of £91.0 million, an adverse variance of £2.4 million.
4 4
3. Use of AssetsThe Trust made a 5.4% return on net assets (YTD FRR = 4). Of the current capital programme totalling £110.3m, 67% (or £74.3m) is approved & in progress. The plan for capital spend in 2010/11 remains at £72.2m.
4 5
4. Income & Expenditure Position
The “bottom-line” I&E position is a surplus of £5.8 million, a 1.6% return on income (YTD FRR = 3). The I&E position is £0.2 million (rounded) behind plan, which predicted a £5.9 million surplus at M5.However, the position benefits from a net YTD impairment reversal of £1.0m (which is excluded from the FRR calculation on both “use of assets” & “overall I&E position”).
3 3
4
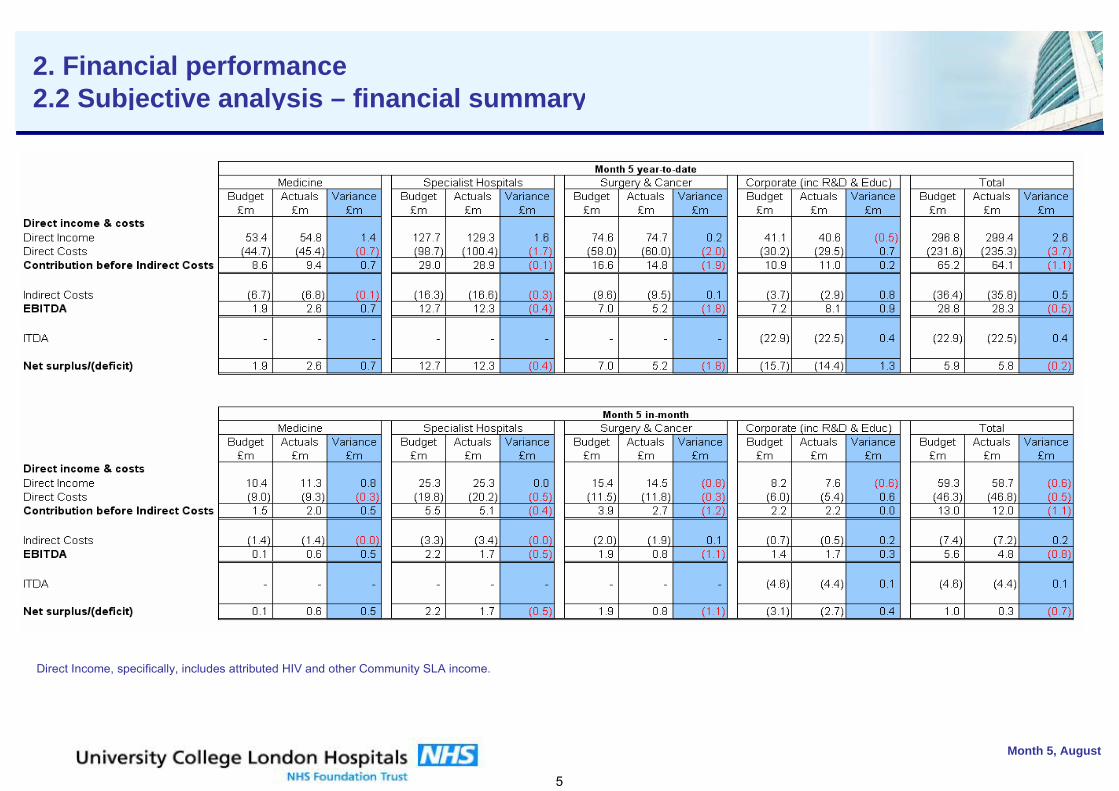
Month 5, August
2. Financial performance2.2 Subjective analysis – financial summary
Direct Income, specifically, includes attributed HIV and other Community SLA income.
5
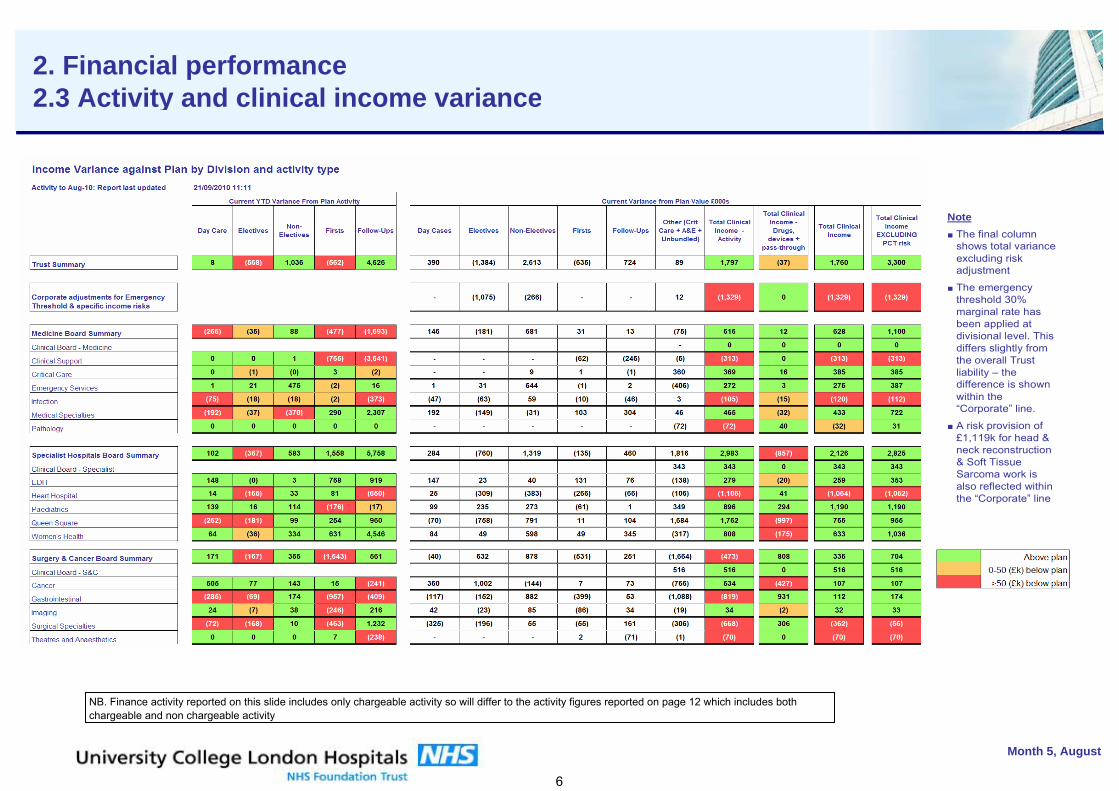
Month 5, August
2. Financial performance2.3 Activity and clinical income variance
NB. Finance activity reported on this slide includes only chargeable activity so will differ to the activity figures reported on page 12 which includes both chargeable and non chargeable activity
Note■ The final column
shows total variance excluding risk adjustment
■ The emergency threshold 30% marginal rate has been applied at divisional level. This differs slightly from the overall Trust liability – the difference is shown within the “Corporate” line.
■ A risk provision of £1,119k for head & neck reconstruction & Soft Tissue Sarcoma work is also reflected within the “Corporate” line
6
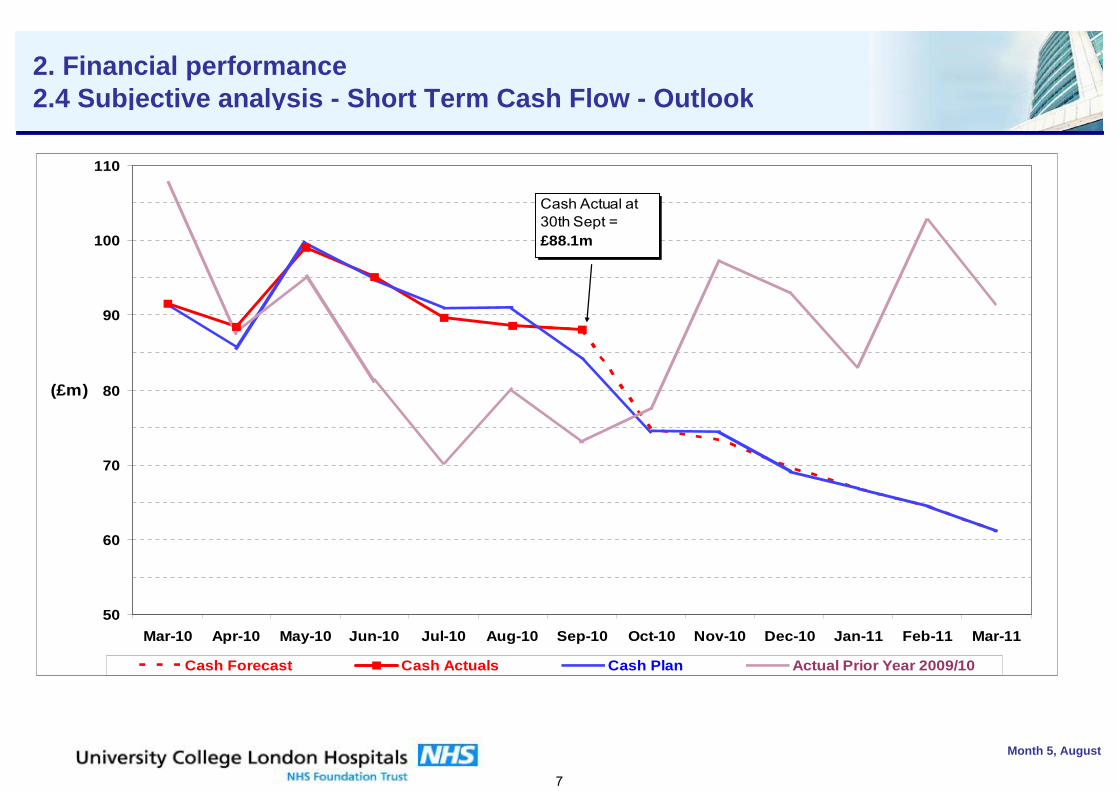
Month 5, August
2. Financial performance2.4 Subjective analysis - Short Term Cash Flow - Outlook
50
60
70
80
90
100
110
Mar-10 Apr-10 May-10 Jun-10 Jul-10 Aug-10 Sep-10 Oct-10 Nov-10 Dec-10 Jan-11 Feb-11 Mar-11
(£m)
Cash Forecast Cash Actuals Cash Plan Actual Prior Year 2009/10
Cash Actual at 30th Sept = £88.1m
7
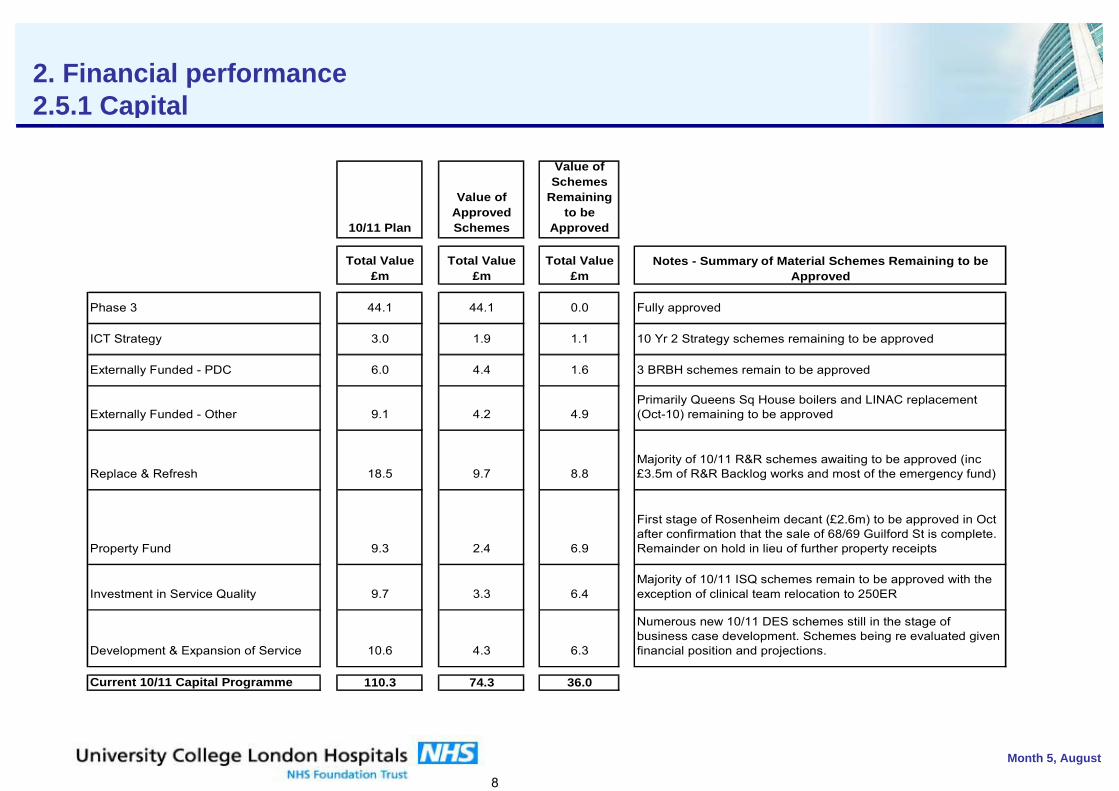
Month 5, August
2. Financial performance 2.5.1 Capital
10/11 Plan
Value of Approved Schemes
Value of Schemes
Remaining to be
Approved
Total Value £m
Total Value £m
Total Value £m
Phase 3 44.1 44.1 0.0
ICT Strategy 3.0 1.9 1.1
Externally Funded - PDC 6.0 4.4 1.6
Externally Funded - Other 9.1 4.2 4.9
Replace & Refresh 18.5 9.7 8.8
Property Fund 9.3 2.4 6.9
Investment in Service Quality 9.7 3.3 6.4
Development & Expansion of Service 10.6 4.3 6.3
Current 10/11 Capital Programme 110.3 74.3 36.0
Notes - Summary of Material Schemes Remaining to be Approved
Fully approved
10 Yr 2 Strategy schemes remaining to be approved
3 BRBH schemes remain to be approved
Majority of 10/11 ISQ schemes remain to be approved with the exception of clinical team relocation to 250ER
Numerous new 10/11 DES schemes still in the stage of business case development. Schemes being re evaluated given financial position and projections.
Primarily Queens Sq House boilers and LINAC replacement (Oct-10) remaining to be approved
Majority of 10/11 R&R schemes awaiting to be approved (inc £3.5m of R&R Backlog works and most of the emergency fund)
First stage of Rosenheim decant (£2.6m) to be approved in Oct after confirmation that the sale of 68/69 Guilford St is complete. Remainder on hold in lieu of further property receipts
8
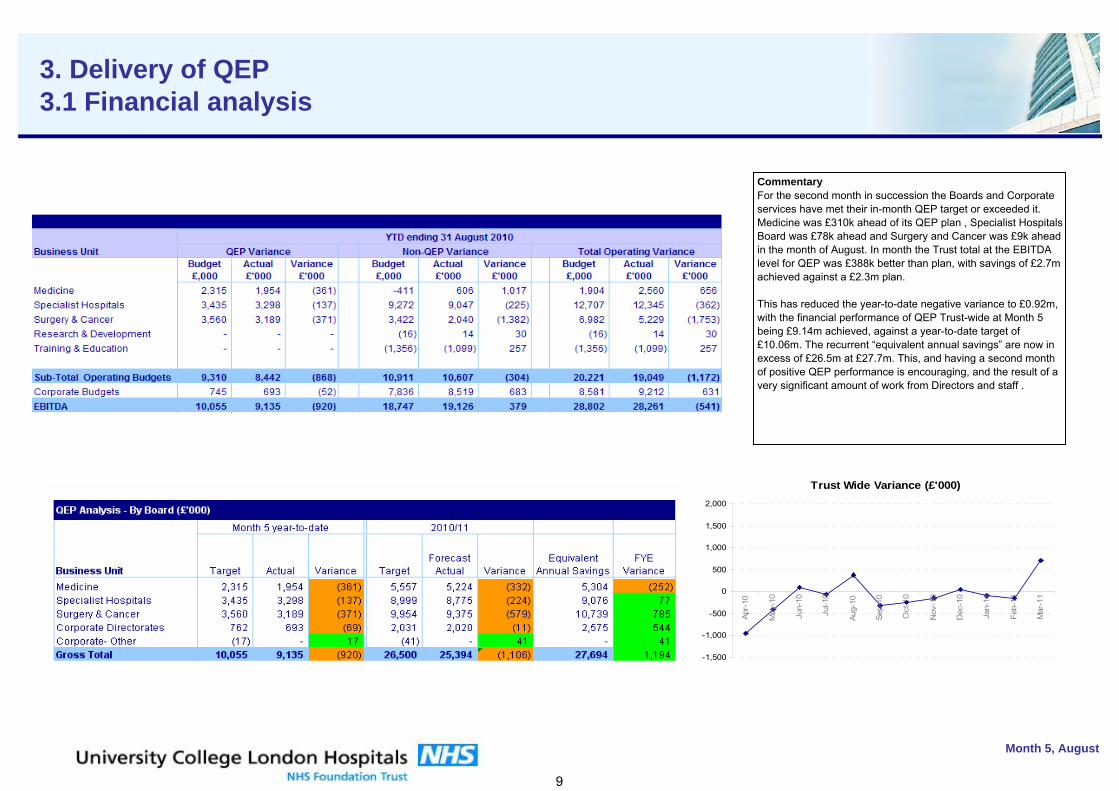
kurhgiudrhg
Month 5, August
3. Delivery of QEP3.1 Financial analysis
CommentaryFor the second month in succession the Boards and Corporate services have met their in-month QEP target or exceeded it. Medicine was £310k ahead of its QEP plan , Specialist Hospitals Board was £78k ahead and Surgery and Cancer was £9k ahead in the month of August. In month the Trust total at the EBITDA level for QEP was £388k better than plan, with savings of £2.7m achieved against a £2.3m plan. This has reduced the year-to-date negative variance to £0.92m, with the financial performance of QEP Trust-wide at Month 5 being £9.14m achieved, against a year-to-date target of £10.06m. The recurrent “equivalent annual savings” are now in excess of £26.5m at £27.7m. This, and having a second month of positive QEP performance is encouraging, and the result of a very significant amount of work from Directors and staff .
Trust Wide Variance (£'000)
-1,500
-1,000
-500
0
500
1,000
1,500
2,000
Apr-
10
May
-10
Jun-
10
Jul-1
0
Aug-
10
Sep-
10
Oct
-10
Nov
-10
Dec
-10
Jan-
11
Feb-
11
Mar
-11
9
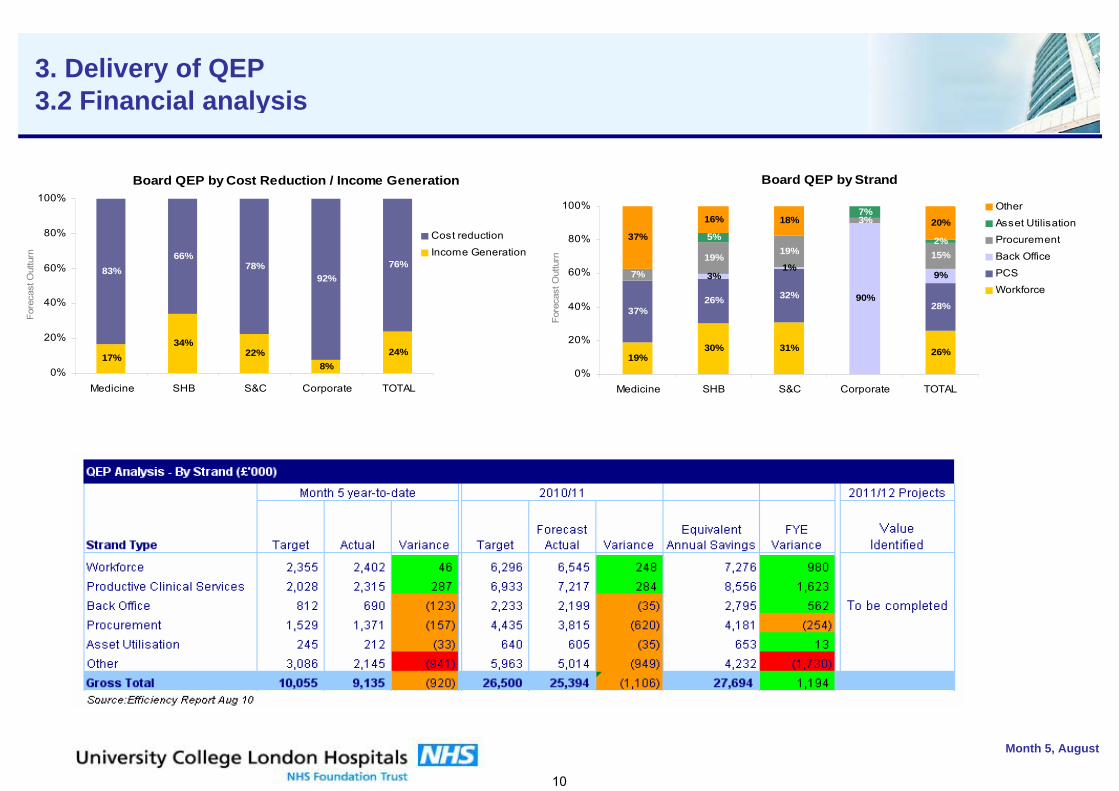
kurhgiudrhg
Month 5, August
3. Delivery of QEP3.2 Financial analysis
Board QEP by Cost Reduction / Income Generation
17%34%
22% 24%
83%66%
78%92%
76%
8%0%
20%
40%
60%
80%
100%
Medicine SHB S&C Corporate TOTAL
Fore
cast
Out
turn
Cost reduction
Income Generation
Board QEP by Strand
19%30% 31% 26%
37%26% 32%
28%90%
9%7%
19%19%
3%
15%
5%
7%
2%37%
16% 18% 20%
3%1%
0%
20%
40%
60%
80%
100%
Medicine SHB S&C Corporate TOTAL
Fore
cast
Out
turn
Other
Asset UtilisationProcurement
Back Office
PCSWorkforce
10
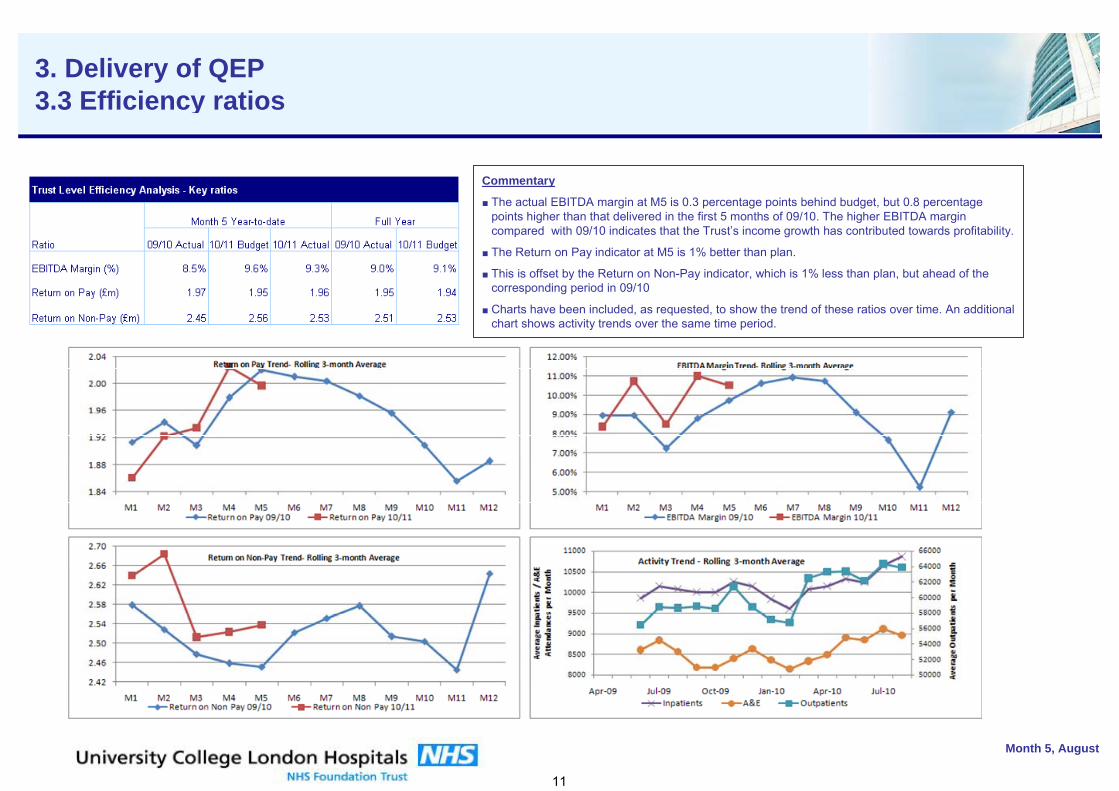
kurhgiudrhg
Month 5, August
3. Delivery of QEP3.3 Efficiency ratios
Commentary
■ The actual EBITDA margin at M5 is 0.3 percentage points behind budget, but 0.8 percentage points higher than that delivered in the first 5 months of 09/10. The higher EBITDA margin compared with 09/10 indicates that the Trust’s income growth has contributed towards profitability.
■ The Return on Pay indicator at M5 is 1% better than plan.
■ This is offset by the Return on Non-Pay indicator, which is 1% less than plan, but ahead of the corresponding period in 09/10
■ Charts have been included, as requested, to show the trend of these ratios over time. An additional chart shows activity trends over the same time period.
11
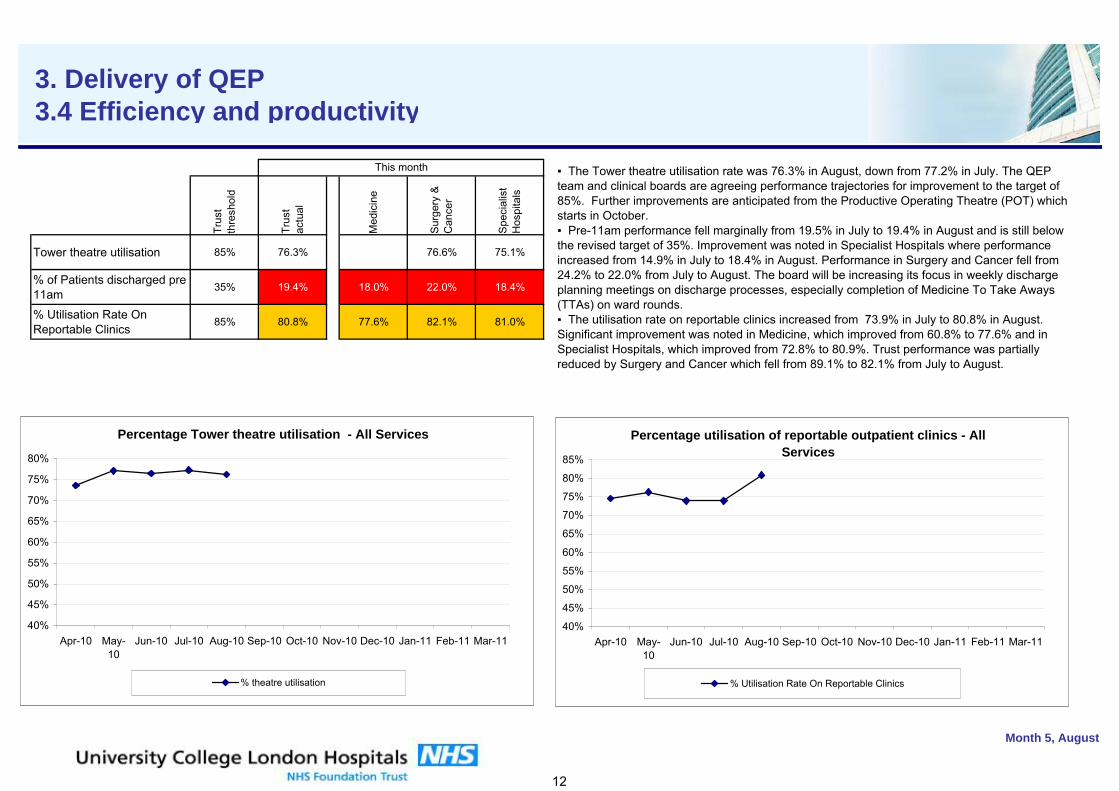
kurhgiudrhg
Trus
t th
resh
old
Trus
t ac
tual
Med
icin
e
Sur
gery
&
Can
cer
Spe
cial
ist
Hos
pita
ls
Tower theatre utilisation 85% 76.3% 76.6% 75.1%
% of Patients discharged pre 11am
35% 19.4% 18.0% 22.0% 18.4%
% Utilisation Rate On Reportable Clinics
85% 80.8% 77.6% 82.1% 81.0%
Month 5, August
This month
3. Delivery of QEP3.4 Efficiency and productivity
Percentage utilisation of reportable outpatient clinics - All Services
40%
45%
50%
55%
60%
65%
70%
75%
80%
85%
Apr-10 May-10
Jun-10 Jul-10 Aug-10 Sep-10 Oct-10 Nov-10 Dec-10 Jan-11 Feb-11 Mar-11
% Utilisation Rate On Reportable Clinics
▪ The Tower theatre utilisation rate was 76.3% in August, down from 77.2% in July. The QEP team and clinical boards are agreeing performance trajectories for improvement to the target of 85%. Further improvements are anticipated from the Productive Operating Theatre (POT) which starts in October. ▪ Pre-11am performance fell marginally from 19.5% in July to 19.4% in August and is still below the revised target of 35%. Improvement was noted in Specialist Hospitals where performance increased from 14.9% in July to 18.4% in August. Performance in Surgery and Cancer fell from 24.2% to 22.0% from July to August. The board will be increasing its focus in weekly discharge planning meetings on discharge processes, especially completion of Medicine To Take Aways (TTAs) on ward rounds. ▪ The utilisation rate on reportable clinics increased from 73.9% in July to 80.8% in August. Significant improvement was noted in Medicine, which improved from 60.8% to 77.6% and in Specialist Hospitals, which improved from 72.8% to 80.9%. Trust performance was partially reduced by Surgery and Cancer which fell from 89.1% to 82.1% from July to August.
Percentage Tower theatre utilisation - All Services
40%
45%
50%
55%
60%
65%
70%
75%
80%
Apr-10 May-10
Jun-10 Jul-10 Aug-10 Sep-10 Oct-10 Nov-10 Dec-10 Jan-11 Feb-11 Mar-11
% theatre utilisation
12
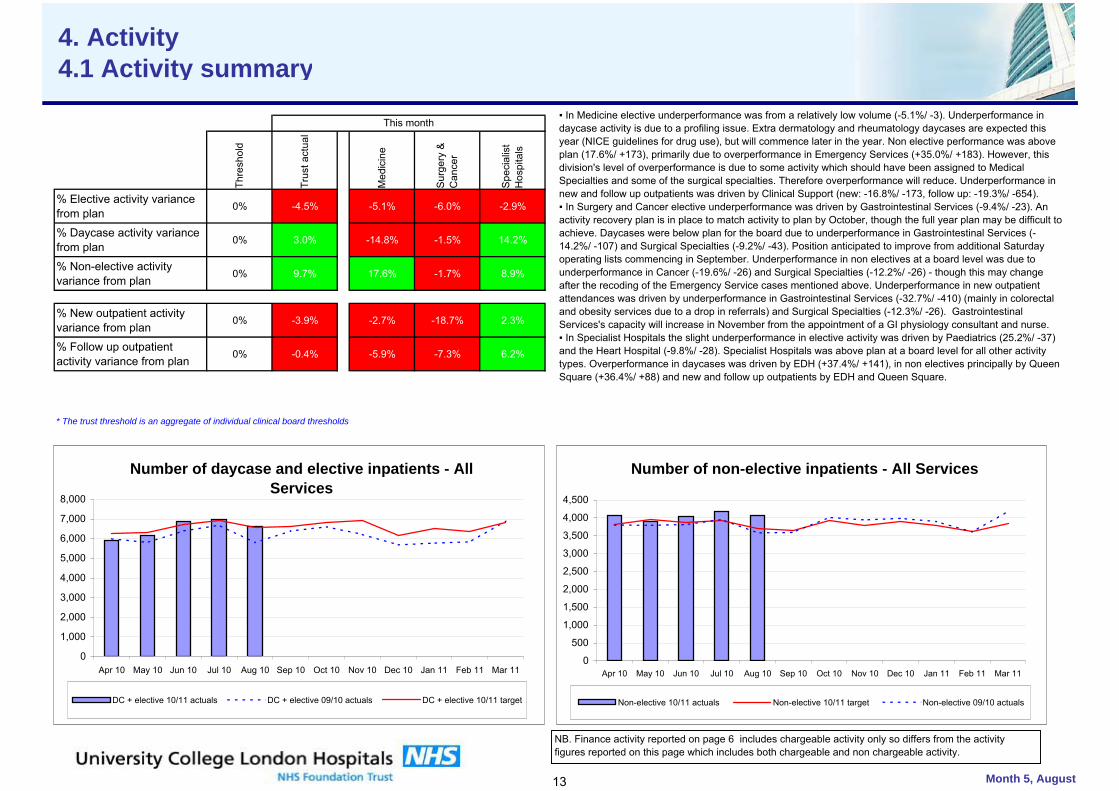
kurhgiudrhg
Thre
shol
d
Trus
t act
ual
Med
icin
e
Sur
gery
&
Can
cer
Spe
cial
ist
Hos
pita
ls
% Elective activity variance from plan
0% -4.5% -5.1% -6.0% -2.9%
% Daycase activity variance from plan
0% 3.0% -14.8% -1.5% 14.2%
% Non-elective activity variance from plan
0% 9.7% 17.6% -1.7% 8.9%
% New outpatient activity variance from plan
0% -3.9% -2.7% -18.7% 2.3%
% Follow up outpatient activity variance from plan
0% -0.4% -5.9% -7.3% 6.2%
* The trust threshold is an aggregate of individual clinical board thresholds
Month 5, August
This month
4. Activity4.1 Activity summary
Number of daycase and elective inpatients - All Services
0
1,000
2,000
3,000
4,000
5,000
6,000
7,000
8,000
Apr 10 May 10 Jun 10 Jul 10 Aug 10 Sep 10 Oct 10 Nov 10 Dec 10 Jan 11 Feb 11 Mar 11
DC + elective 10/11 actuals DC + elective 09/10 actuals DC + elective 10/11 target
Number of non-elective inpatients - All Services
0
500
1,000
1,500
2,000
2,500
3,000
3,500
4,000
4,500
Apr 10 May 10 Jun 10 Jul 10 Aug 10 Sep 10 Oct 10 Nov 10 Dec 10 Jan 11 Feb 11 Mar 11
Non-elective 10/11 actuals Non-elective 10/11 target Non-elective 09/10 actuals
▪ In Medicine elective underperformance was from a relatively low volume (-5.1%/ -3). Underperformance in daycase activity is due to a profiling issue. Extra dermatology and rheumatology daycases are expected this year (NICE guidelines for drug use), but will commence later in the year. Non elective performance was above plan (17.6%/ +173), primarily due to overperformance in Emergency Services (+35.0%/ +183). However, this division's level of overperformance is due to some activity which should have been assigned to Medical Specialties and some of the surgical specialties. Therefore overperformance will reduce. Underperformance in new and follow up outpatients was driven by Clinical Support (new: -16.8%/ -173, follow up: -19.3%/ -654).▪ In Surgery and Cancer elective underperformance was driven by Gastrointestinal Services (-9.4%/ -23). An activity recovery plan is in place to match activity to plan by October, though the full year plan may be difficult to achieve. Daycases were below plan for the board due to underperformance in Gastrointestinal Services (-14.2%/ -107) and Surgical Specialties (-9.2%/ -43). Position anticipated to improve from additional Saturday operating lists commencing in September. Underperformance in non electives at a board level was due to underperformance in Cancer (-19.6%/ -26) and Surgical Specialties (-12.2%/ -26) - though this may change after the recoding of the Emergency Service cases mentioned above. Underperformance in new outpatient attendances was driven by underperformance in Gastrointestinal Services (-32.7%/ -410) (mainly in colorectal and obesity services due to a drop in referrals) and Surgical Specialties (-12.3%/ -26). Gastrointestinal Services's capacity will increase in November from the appointment of a GI physiology consultant and nurse.▪ In Specialist Hospitals the slight underperformance in elective activity was driven by Paediatrics (25.2%/ -37) and the Heart Hospital (-9.8%/ -28). Specialist Hospitals was above plan at a board level for all other activity types. Overperformance in daycases was driven by EDH (+37.4%/ +141), in non electives principally by Queen Square (+36.4%/ +88) and new and follow up outpatients by EDH and Queen Square.
NB. Finance activity reported on page 6 includes chargeable activity only so differs from the activity figures reported on this page which includes both chargeable and non chargeable activity.
13
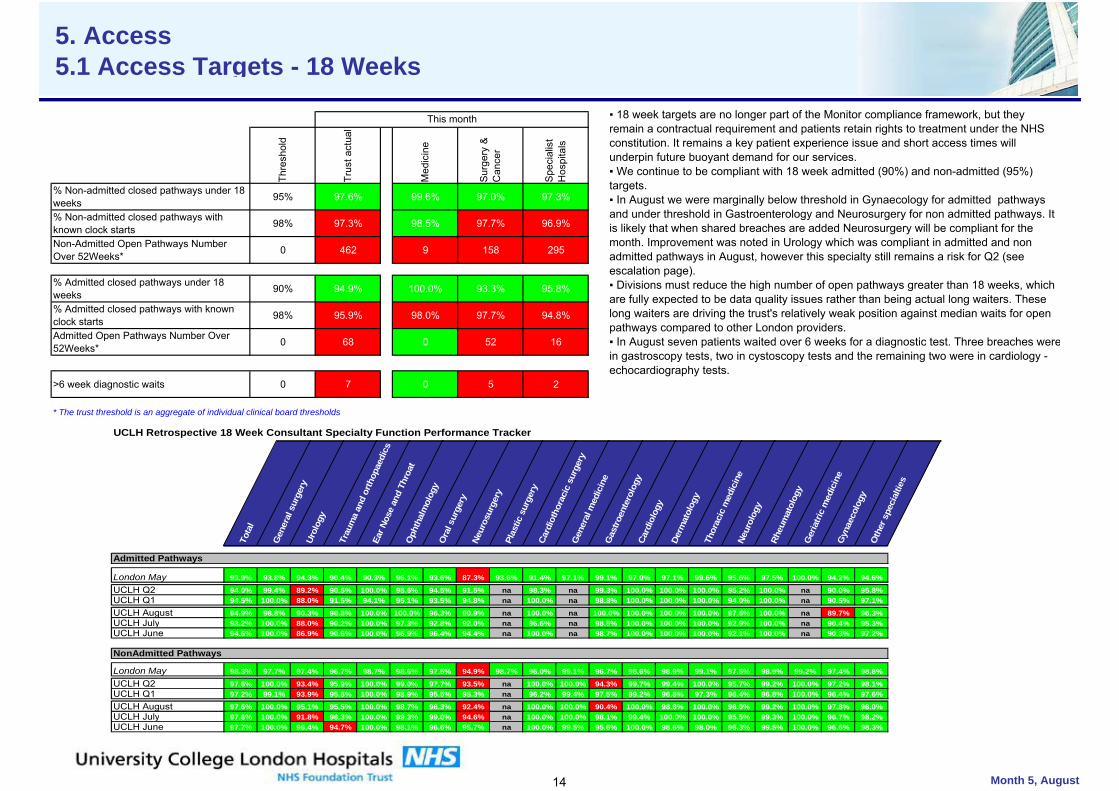
kurhgiudrhg
Thre
shol
d
Trus
t act
ual
Med
icin
e
Sur
gery
&
Can
cer
Spe
cial
ist
Hos
pita
ls
% Non-admitted closed pathways under 18 weeks 95% 97.6% 99.6% 97.0% 97.3%
% Non-admitted closed pathways with known clock starts 98% 97.3% 98.5% 97.7% 96.9%
Non-Admitted Open Pathways Number Over 52Weeks* 0 462 9 158 295
% Admitted closed pathways under 18 weeks 90% 94.9% 100.0% 93.3% 95.8%
% Admitted closed pathways with known clock starts 98% 95.9% 98.0% 97.7% 94.8%
Admitted Open Pathways Number Over 52Weeks* 0 68 0 52 16
>6 week diagnostic waits 0 7 0 5 2
* The trust threshold is an aggregate of individual clinical board thresholds
Month 5, August
This month
5. Access5.1 Access Targets - 18 Weeks
▪ 18 week targets are no longer part of the Monitor compliance framework, but they remain a contractual requirement and patients retain rights to treatment under the NHS constitution. It remains a key patient experience issue and short access times will underpin future buoyant demand for our services. ▪ We continue to be compliant with 18 week admitted (90%) and non-admitted (95%) targets. ▪ In August we were marginally below threshold in Gynaecology for admitted pathways and under threshold in Gastroenterology and Neurosurgery for non admitted pathways. It is likely that when shared breaches are added Neurosurgery will be compliant for the month. Improvement was noted in Urology which was compliant in admitted and non admitted pathways in August, however this specialty still remains a risk for Q2 (see escalation page). ▪ Divisions must reduce the high number of open pathways greater than 18 weeks, which are fully expected to be data quality issues rather than being actual long waiters. These long waiters are driving the trust's relatively weak position against median waits for open pathways compared to other London providers.▪ In August seven patients waited over 6 weeks for a diagnostic test. Three breaches werein gastroscopy tests, two in cystoscopy tests and the remaining two were in cardiology - echocardiography tests.
UCLH Retrospective 18 Week Consultant Specialty Function Performance Tracker
Tota
l
Gen
eral
sur
gery
Urol
ogy
Trau
ma
and
orth
opae
dics
Ear N
ose
and
Thro
atO
phth
alm
olog
yO
ral s
urge
ryNe
uros
urge
ryPl
astic
sur
gery
Card
ioth
orac
ic s
urge
ryG
ener
al m
edic
ine
Gas
troen
tero
logy
Card
iolo
gy
Derm
atol
ogy
Thor
acic
med
icin
eNe
urol
ogy
Rheu
mat
olog
yG
eria
tric
med
icin
eG
ynae
colo
gyO
ther
spe
cial
ties
Admitted Pathways
London May 93.9% 93.8% 94.3% 90.4% 90.3% 96.1% 93.6% 87.3% 93.6% 91.4% 97.1% 99.1% 97.0% 97.1% 99.6% 95.6% 97.5% 100.0% 94.2% 94.6%
UCLH Q2 94.0% 99.4% 89.2% 90.5% 100.0% 98.6% 94.5% 91.5% na 98.3% na 99.3% 100.0% 100.0% 100.0% 95.2% 100.0% na 90.0% 95.8% 3 3UCLH Q1 94.5% 100.0% 88.0% 91.5% 94.1% 95.1% 93.5% 94.8% na 100.0% na 98.8% 100.0% 100.0% 100.0% 94.0% 100.0% na 90.5% 97.1% 3 3
UCLH August 94.9% 98.8% 90.3% 90.8% 100.0% 100.0% 96.3% 90.9% na 100.0% na 100.0% 100.0% 100.0% 100.0% 97.6% 100.0% na 89.7% 96.3% 3 3UCLH July 93.2% 100.0% 88.0% 90.2% 100.0% 97.3% 92.8% 92.0% na 96.6% na 98.5% 100.0% 100.0% 100.0% 92.9% 100.0% na 90.4% 95.3% 3 3UCLH June 94.6% 100.0% 86.9% 90.6% 100.0% 96.9% 96.4% 94.4% na 100.0% na 98.7% 100.0% 100.0% 100.0% 92.1% 100.0% na 90.3% 97.2% 3 3
NonAdmitted Pathways
London May 98.3% 97.7% 97.4% 96.7% 98.7% 98.6% 97.5% 94.9% 98.7% 96.0% 99.1% 96.7% 98.6% 98.9% 99.1% 97.5% 98.9% 99.2% 97.4% 98.8%
UCLH Q2 97.6% 100.0% 93.4% 95.9% 100.0% 99.0% 97.7% 93.5% na 100.0% 100.0% 94.3% 99.7% 99.4% 100.0% 95.7% 99.2% 100.0% 97.2% 98.1% 3 3UCLH Q1 97.2% 99.1% 93.9% 95.8% 100.0% 98.9% 95.5% 95.3% na 96.2% 99.4% 97.5% 99.2% 96.8% 97.3% 96.4% 96.8% 100.0% 96.4% 97.6% 3 3
UCLH August 97.6% 100.0% 95.1% 95.5% 100.0% 98.7% 96.3% 92.4% na 100.0% 100.0% 90.4% 100.0% 98.8% 100.0% 96.0% 99.2% 100.0% 97.8% 98.0% 3 3UCLH July 97.6% 100.0% 91.8% 96.3% 100.0% 99.3% 99.0% 94.6% na 100.0% 100.0% 98.1% 99.4% 100.0% 100.0% 95.5% 99.3% 100.0% 96.7% 98.2% 3 3UCLH June 97.7% 100.0% 96.4% 94.7% 100.0% 98.1% 96.6% 95.7% na 100.0% 99.5% 95.6% 100.0% 98.6% 98.0% 96.3% 99.5% 100.0% 96.6% 98.3% 3 3
14
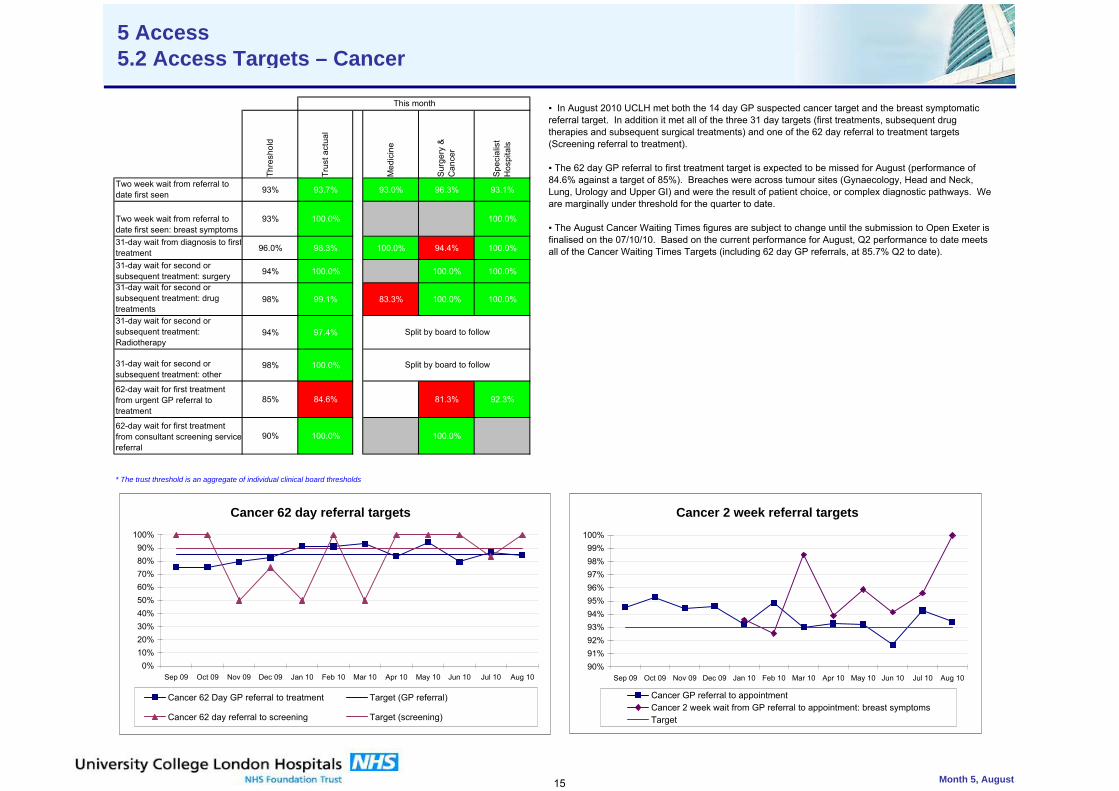
kurhgiudrhg
Thre
shol
d
Trus
t act
ual
Med
icin
e
Surg
ery
& C
ance
r
Spec
ialis
t H
ospi
tals
Two week wait from referral to date first seen 93% 93.7% 93.0% 96.3% 93.1%
Two week wait from referral to date first seen: breast symptoms
93% 100.0% 100.0% 2
31-day wait from diagnosis to firsttreatment 96.0% 98.3% 100.0% 94.4% 100.0%
31-day wait for second or subsequent treatment: surgery 94% 100.0% 100.0% 100.0%
31-day wait for second or subsequent treatment: drug treatments
98% 99.1% 83.3% 100.0% 100.0%
31-day wait for second or subsequent treatment: Radiotherapy
94% 97.4%
31-day wait for second or subsequent treatment: other
98% 100.0%
62-day wait for first treatment from urgent GP referral to treatment
85% 84.6% 81.3% 92.3%
62-day wait for first treatment from consultant screening servicereferral
90% 100.0% 100.0%
* The trust threshold is an aggregate of individual clinical board thresholds
Month 5, August
This month
Split by board to follow
Split by board to follow
5 Access5.2 Access Targets – Cancer
▪ In August 2010 UCLH met both the 14 day GP suspected cancer target and the breast symptomatic referral target. In addition it met all of the three 31 day targets (first treatments, subsequent drug therapies and subsequent surgical treatments) and one of the 62 day referral to treatment targets (Screening referral to treatment).
▪ The 62 day GP referral to first treatment target is expected to be missed for August (performance of 84.6% against a target of 85%). Breaches were across tumour sites (Gynaecology, Head and Neck, Lung, Urology and Upper GI) and were the result of patient choice, or complex diagnostic pathways. We are marginally under threshold for the quarter to date.
▪ The August Cancer Waiting Times figures are subject to change until the submission to Open Exeter is finalised on the 07/10/10. Based on the current performance for August, Q2 performance to date meets all of the Cancer Waiting Times Targets (including 62 day GP referrals, at 85.7% Q2 to date).
Cancer 62 day referral targets
0%10%20%30%40%50%60%70%80%90%
100%
Sep 09 Oct 09 Nov 09 Dec 09 Jan 10 Feb 10 Mar 10 Apr 10 May 10 Jun 10 Jul 10 Aug 10
Cancer 62 Day GP referral to treatment Target (GP referral)
Cancer 62 day referral to screening Target (screening)
Cancer 2 week referral targets
90%91%92%93%94%95%96%97%98%99%
100%
Sep 09 Oct 09 Nov 09 Dec 09 Jan 10 Feb 10 Mar 10 Apr 10 May 10 Jun 10 Jul 10 Aug 10
Cancer GP referral to appointmentCancer 2 week wait from GP referral to appointment: breast symptomsTarget
15
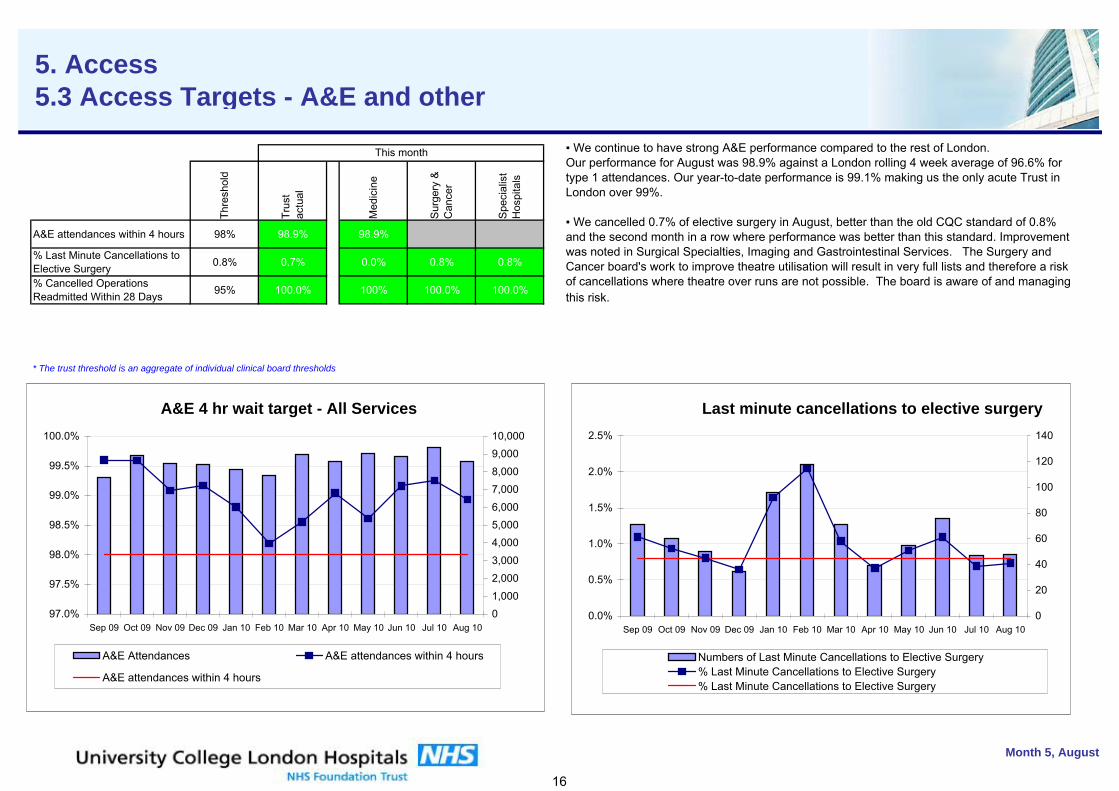
kurhgiudrhg
Thre
shol
d
Trus
t ac
tual
Med
icin
e
Sur
gery
&
Can
cer
Spe
cial
ist
Hos
pita
ls
A&E attendances within 4 hours 98% 98.9% 98.9%
% Last Minute Cancellations to Elective Surgery 0.8% 0.7% 0.0% 0.8% 0.8%
% Cancelled Operations Readmitted Within 28 Days 95% 100.0% 100% 100.0% 100.0%
* The trust threshold is an aggregate of individual clinical board thresholds
Month 5, August
This month
5. Access5.3 Access Targets - A&E and other
▪ We continue to have strong A&E performance compared to the rest of London. Our performance for August was 98.9% against a London rolling 4 week average of 96.6% for type 1 attendances. Our year-to-date performance is 99.1% making us the only acute Trust in London over 99%.
▪ We cancelled 0.7% of elective surgery in August, better than the old CQC standard of 0.8% and the second month in a row where performance was better than this standard. Improvement was noted in Surgical Specialties, Imaging and Gastrointestinal Services. The Surgery and Cancer board's work to improve theatre utilisation will result in very full lists and therefore a risk of cancellations where theatre over runs are not possible. The board is aware of and managing this risk.
A&E 4 hr wait target - All Services
97.0%
97.5%
98.0%
98.5%
99.0%
99.5%
100.0%
Sep 09 Oct 09 Nov 09 Dec 09 Jan 10 Feb 10 Mar 10 Apr 10 May 10 Jun 10 Jul 10 Aug 1001,000
2,0003,000
4,0005,0006,000
7,0008,000
9,00010,000
A&E Attendances A&E attendances within 4 hours
A&E attendances within 4 hours
Last minute cancellations to elective surgery
0.0%
0.5%
1.0%
1.5%
2.0%
2.5%
Sep 09 Oct 09 Nov 09 Dec 09 Jan 10 Feb 10 Mar 10 Apr 10 May 10 Jun 10 Jul 10 Aug 100
20
40
60
80
100
120
140
Numbers of Last Minute Cancellations to Elective Surgery% Last Minute Cancellations to Elective Surgery% Last Minute Cancellations to Elective Surgery
16
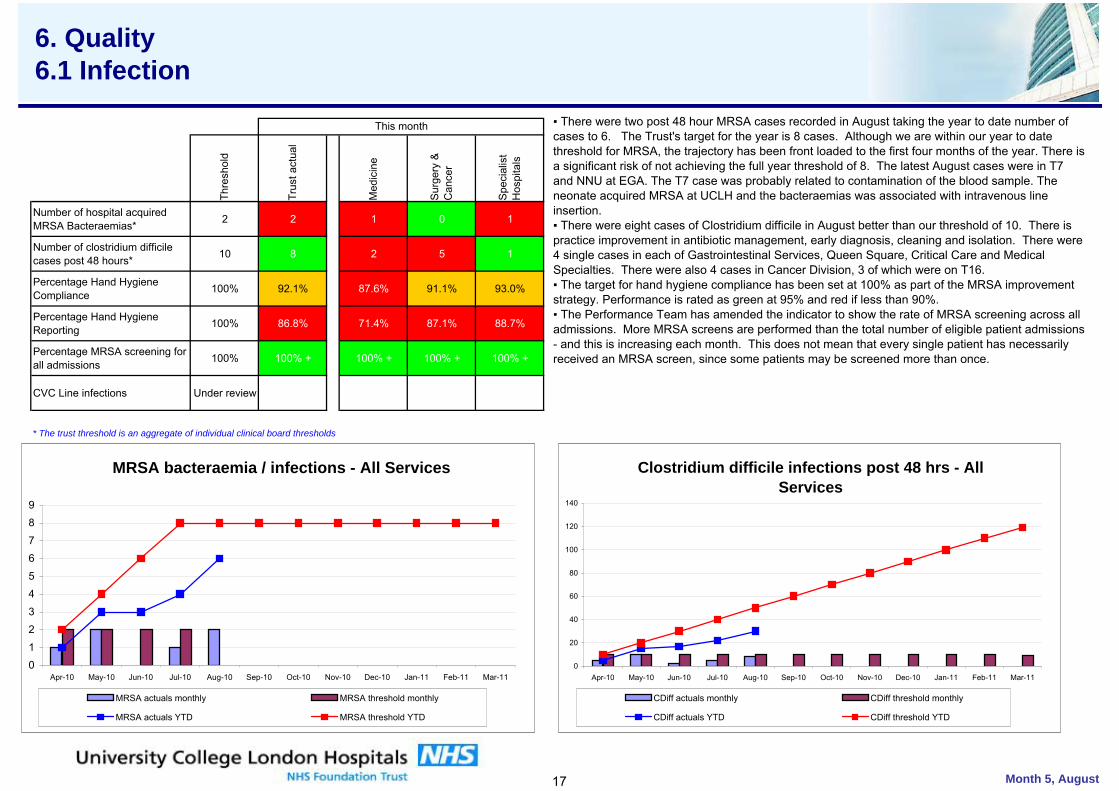
kurhgiudrhg
Thre
shol
d
Trus
t act
ual
Med
icin
e
Sur
gery
&
Can
cer
Spe
cial
ist
Hos
pita
ls
Number of hospital acquired MRSA Bacteraemias* 2 2 1 0 1
Number of clostridium difficile cases post 48 hours* 10 8 2 5 1
Percentage Hand Hygiene Compliance 100% 92.1% 87.6% 91.1% 93.0%
Percentage Hand Hygiene Reporting 100% 86.8% 71.4% 87.1% 88.7%
Percentage MRSA screening for all admissions 100% 100% + 100% + 100% + 100% +
CVC Line infections Under review
* The trust threshold is an aggregate of individual clinical board thresholds
Month 5, August
This month
6. Quality6.1 Infection
MRSA bacteraemia / infections - All Services
01
23
45
67
89
Apr-10 May-10 Jun-10 Jul-10 Aug-10 Sep-10 Oct-10 Nov-10 Dec-10 Jan-11 Feb-11 Mar-11
MRSA actuals monthly MRSA threshold monthly
MRSA actuals YTD MRSA threshold YTD
Clostridium difficile infections post 48 hrs - All Services
0
20
40
60
80
100
120
140
Apr-10 May-10 Jun-10 Jul-10 Aug-10 Sep-10 Oct-10 Nov-10 Dec-10 Jan-11 Feb-11 Mar-11
CDiff actuals monthly CDiff threshold monthly
CDiff actuals YTD CDiff threshold YTD
▪ There were two post 48 hour MRSA cases recorded in August taking the year to date number of cases to 6. The Trust's target for the year is 8 cases. Although we are within our year to date threshold for MRSA, the trajectory has been front loaded to the first four months of the year. There is a significant risk of not achieving the full year threshold of 8. The latest August cases were in T7 and NNU at EGA. The T7 case was probably related to contamination of the blood sample. The neonate acquired MRSA at UCLH and the bacteraemias was associated with intravenous line insertion.▪ There were eight cases of Clostridium difficile in August better than our threshold of 10. There is practice improvement in antibiotic management, early diagnosis, cleaning and isolation. There were 4 single cases in each of Gastrointestinal Services, Queen Square, Critical Care and Medical Specialties. There were also 4 cases in Cancer Division, 3 of which were on T16.▪ The target for hand hygiene compliance has been set at 100% as part of the MRSA improvement strategy. Performance is rated as green at 95% and red if less than 90%. ▪ The Performance Team has amended the indicator to show the rate of MRSA screening across all admissions. More MRSA screens are performed than the total number of eligible patient admissions - and this is increasing each month. This does not mean that every single patient has necessarily received an MRSA screen, since some patients may be screened more than once.
17
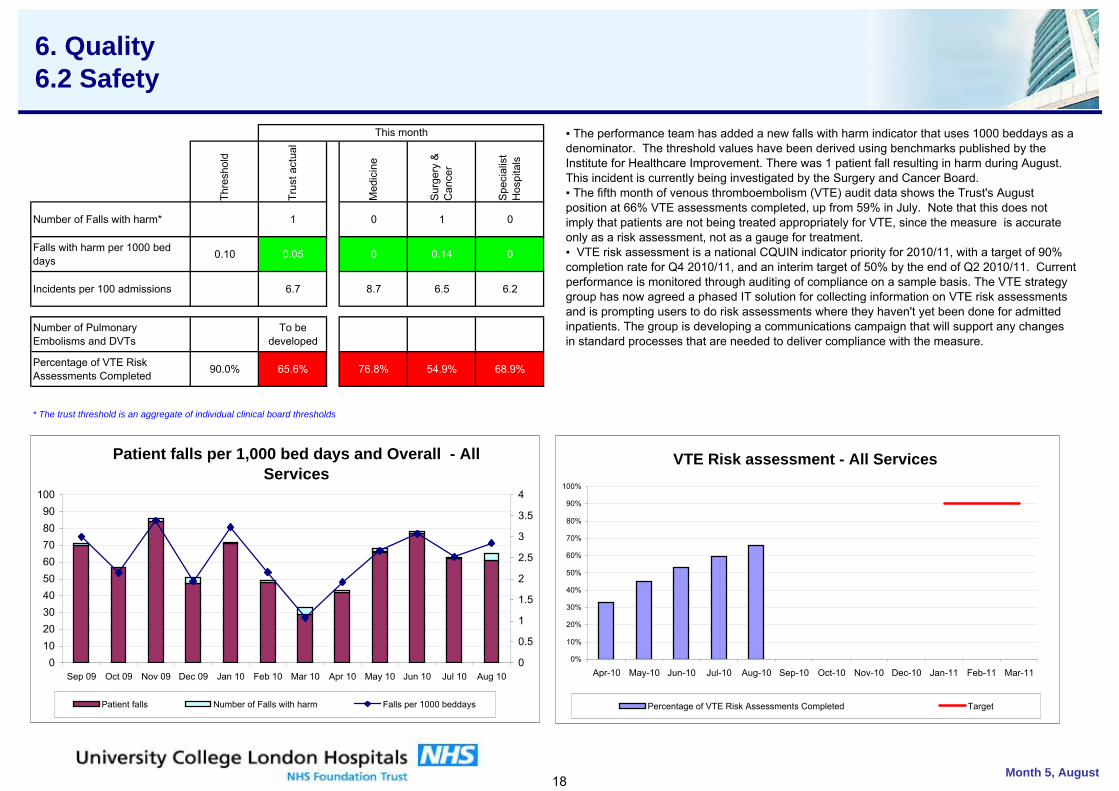
kurhgiudrhg
Thre
shol
d
Trus
t act
ual
Med
icin
e
Sur
gery
&
Can
cer
Spe
cial
ist
Hos
pita
ls
Number of Falls with harm* 1 0 1 0
Falls with harm per 1000 bed days 0.10 0.05 0 0.14 0
Incidents per 100 admissions 6.7 8.7 6.5 6.2
Number of Pulmonary Embolisms and DVTs
To be developed
Percentage of VTE Risk Assessments Completed 90.0% 65.6% 76.8% 54.9% 68.9%
* The trust threshold is an aggregate of individual clinical board thresholds
Month 5, August
This month
6. Quality 6.2 Safety
VTE Risk assessment - All Services
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Apr-10 May-10 Jun-10 Jul-10 Aug-10 Sep-10 Oct-10 Nov-10 Dec-10 Jan-11 Feb-11 Mar-11
Percentage of VTE Risk Assessments Completed Target
Patient falls per 1,000 bed days and Overall - All Services
0102030405060708090
100
Sep 09 Oct 09 Nov 09 Dec 09 Jan 10 Feb 10 Mar 10 Apr 10 May 10 Jun 10 Jul 10 Aug 100
0.5
1
1.5
2
2.5
3
3.5
4
Patient falls Number of Falls with harm Falls per 1000 beddays
▪ The performance team has added a new falls with harm indicator that uses 1000 beddays as a denominator. The threshold values have been derived using benchmarks published by the Institute for Healthcare Improvement. There was 1 patient fall resulting in harm during August. This incident is currently being investigated by the Surgery and Cancer Board. ▪ The fifth month of venous thromboembolism (VTE) audit data shows the Trust's August position at 66% VTE assessments completed, up from 59% in July. Note that this does not imply that patients are not being treated appropriately for VTE, since the measure is accurate only as a risk assessment, not as a gauge for treatment. ▪ VTE risk assessment is a national CQUIN indicator priority for 2010/11, with a target of 90% completion rate for Q4 2010/11, and an interim target of 50% by the end of Q2 2010/11. Current performance is monitored through auditing of compliance on a sample basis. The VTE strategy group has now agreed a phased IT solution for collecting information on VTE risk assessments and is prompting users to do risk assessments where they haven't yet been done for admitted inpatients. The group is developing a communications campaign that will support any changes in standard processes that are needed to deliver compliance with the measure.
18
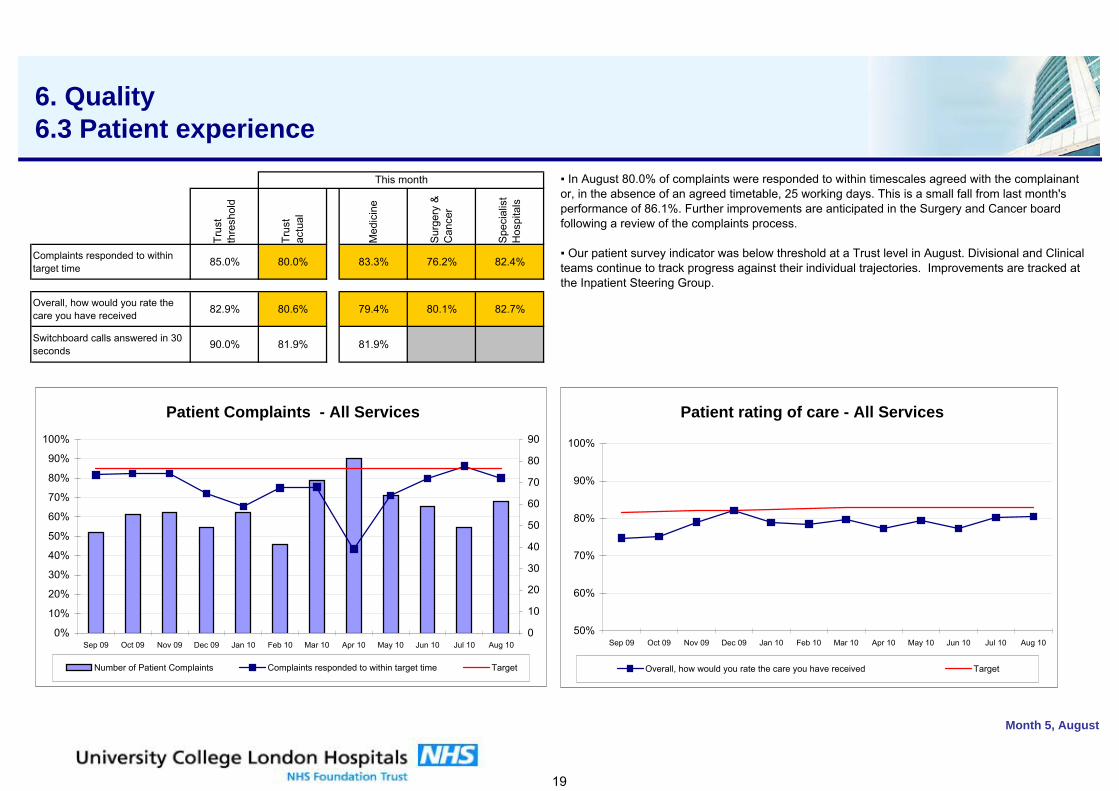
kurhgiudrhg
Trus
t th
resh
old
Trus
t ac
tual
Med
icin
e
Sur
gery
&
Can
cer
Spe
cial
ist
Hos
pita
ls
Complaints responded to within target time 85.0% 80.0% 83.3% 76.2% 82.4%
Overall, how would you rate the care you have received 82.9% 80.6% 79.4% 80.1% 82.7%
Switchboard calls answered in 30 seconds 90.0% 81.9% 81.9%
Month 5, August
This month
6. Quality 6.3 Patient experience
Patient Complaints - All Services
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Sep 09 Oct 09 Nov 09 Dec 09 Jan 10 Feb 10 Mar 10 Apr 10 May 10 Jun 10 Jul 10 Aug 100
10
20
30
40
50
60
70
80
90
Number of Patient Complaints Complaints responded to within target time Target
Patient rating of care - All Services
50%
60%
70%
80%
90%
100%
Sep 09 Oct 09 Nov 09 Dec 09 Jan 10 Feb 10 Mar 10 Apr 10 May 10 Jun 10 Jul 10 Aug 10
Overall, how would you rate the care you have received Target
▪ In August 80.0% of complaints were responded to within timescales agreed with the complainant or, in the absence of an agreed timetable, 25 working days. This is a small fall from last month's performance of 86.1%. Further improvements are anticipated in the Surgery and Cancer board following a review of the complaints process.
▪ Our patient survey indicator was below threshold at a Trust level in August. Divisional and Clinical teams continue to track progress against their individual trajectories. Improvements are tracked at the Inpatient Steering Group.
19
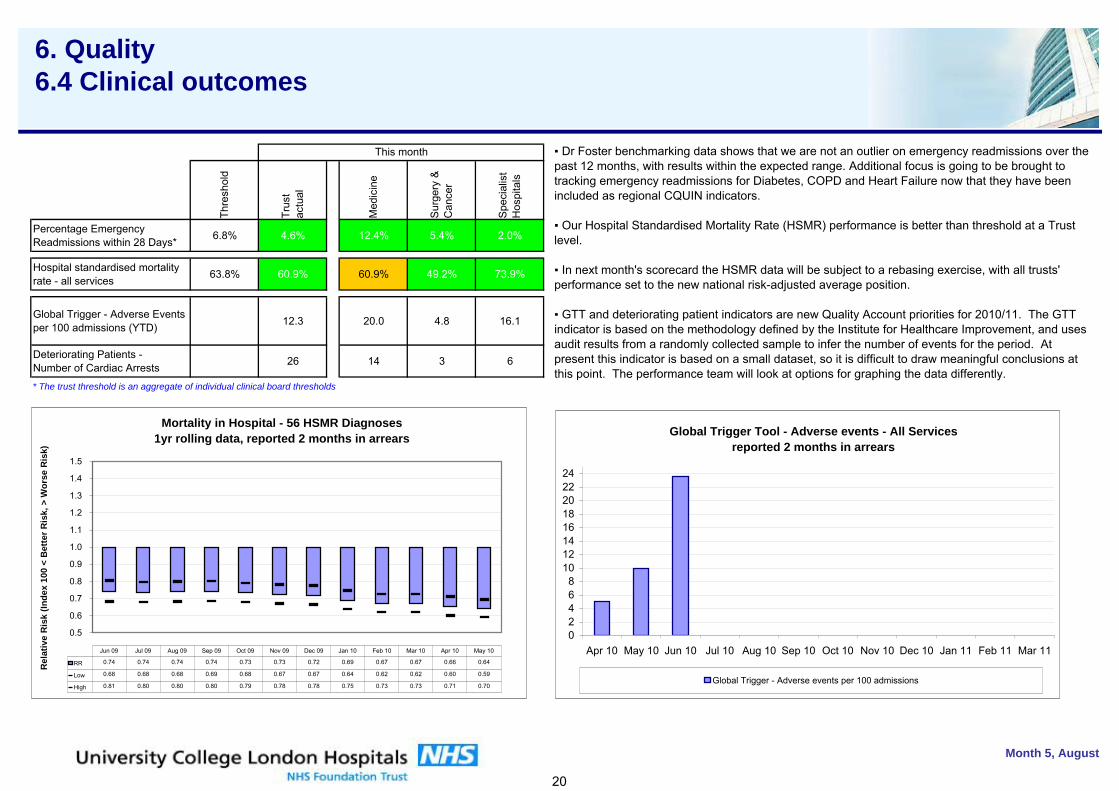
kurhgiudrhg
Thre
shol
d
Trus
t ac
tual
Med
icin
e
Sur
gery
&
Can
cer
Spe
cial
ist
Hos
pita
ls
Percentage Emergency Readmissions within 28 Days* 6.8% 4.6% 12.4% 5.4% 2.0%
Hospital standardised mortality rate - all services 63.8% 60.9% 60.9% 49.2% 73.9%
Global Trigger - Adverse Events per 100 admissions (YTD) 12.3 20.0 4.8 16.1
Deteriorating Patients -Number of Cardiac Arrests 26 14 3 6
* The trust threshold is an aggregate of individual clinical board thresholds
Month 5, August
This month
6. Quality 6.4 Clinical outcomes
Mortality in Hospital - 56 HSMR Diagnoses1yr rolling data, reported 2 months in arrears
0.5
0.6
0.7
0.8
0.9
1.0
1.1
1.2
1.3
1.4
1.5
Rel
ativ
e R
isk
(Inde
x 10
0 <
Bet
ter R
isk,
> W
orse
Ris
k)
RR 0.74 0.74 0.74 0.74 0.73 0.73 0.72 0.69 0.67 0.67 0.66 0.64
Low 0.68 0.68 0.68 0.69 0.68 0.67 0.67 0.64 0.62 0.62 0.60 0.59
High 0.81 0.80 0.80 0.80 0.79 0.78 0.78 0.75 0.73 0.73 0.71 0.70
Jun 09 Jul 09 Aug 09 Sep 09 Oct 09 Nov 09 Dec 09 Jan 10 Feb 10 Mar 10 Apr 10 May 10
▪ Dr Foster benchmarking data shows that we are not an outlier on emergency readmissions over the past 12 months, with results within the expected range. Additional focus is going to be brought to tracking emergency readmissions for Diabetes, COPD and Heart Failure now that they have been included as regional CQUIN indicators.
▪ Our Hospital Standardised Mortality Rate (HSMR) performance is better than threshold at a Trust level.
▪ In next month's scorecard the HSMR data will be subject to a rebasing exercise, with all trusts' performance set to the new national risk-adjusted average position.
▪ GTT and deteriorating patient indicators are new Quality Account priorities for 2010/11. The GTT indicator is based on the methodology defined by the Institute for Healthcare Improvement, and uses audit results from a randomly collected sample to infer the number of events for the period. At present this indicator is based on a small dataset, so it is difficult to draw meaningful conclusions at this point. The performance team will look at options for graphing the data differently.
Global Trigger Tool - Adverse events - All Servicesreported 2 months in arrears
02468
1012141618202224
Apr 10 May 10 Jun 10 Jul 10 Aug 10 Sep 10 Oct 10 Nov 10 Dec 10 Jan 11 Feb 11 Mar 11
Global Trigger - Adverse events per 100 admissions
20
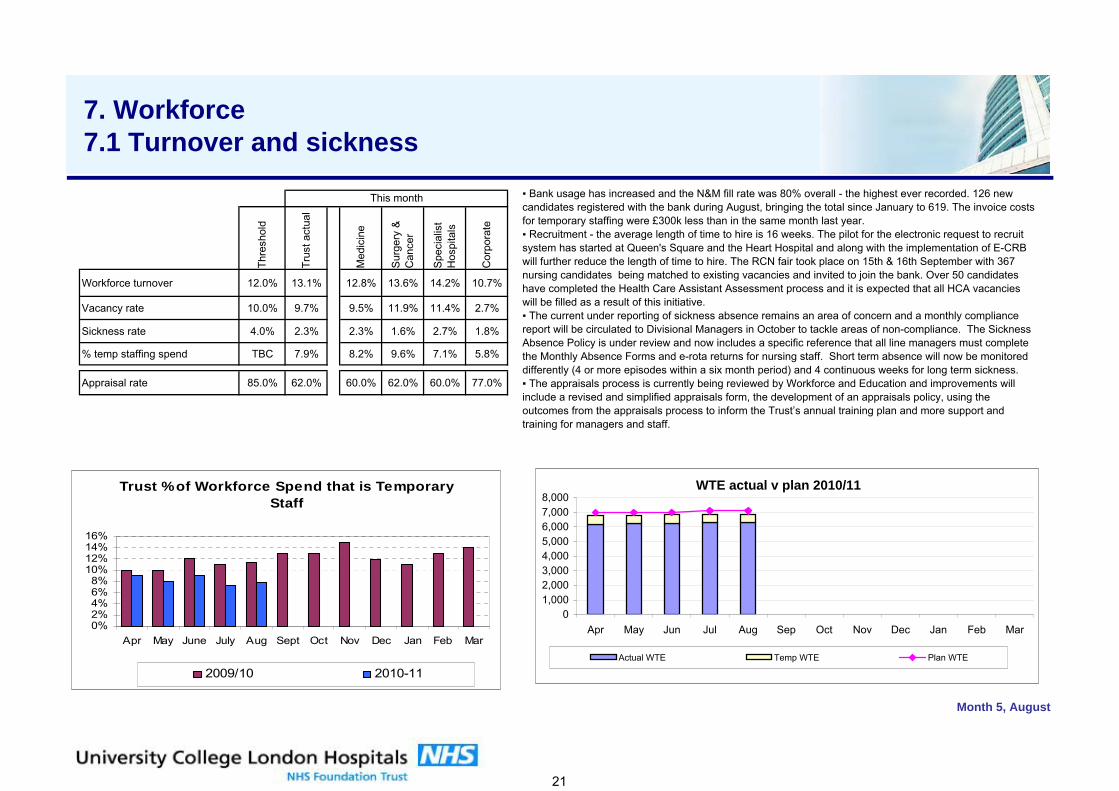
kurhgiudrhg
Thre
shol
d
Trus
t act
ual
Med
icin
e
Sur
gery
&
Can
cer
Spe
cial
ist
Hos
pita
ls
Cor
pora
te
Workforce turnover 12.0% 13.1% 12.8% 13.6% 14.2% 10.7%
Vacancy rate 10.0% 9.7% 9.5% 11.9% 11.4% 2.7%
Sickness rate 4.0% 2.3% 2.3% 1.6% 2.7% 1.8%
% temp staffing spend TBC 7.9% 8.2% 9.6% 7.1% 5.8%
Appraisal rate 85.0% 62.0% 60.0% 62.0% 60.0% 77.0%
Month 5, August
This month
7. Workforce 7.1 Turnover and sickness
▪ Bank usage has increased and the N&M fill rate was 80% overall - the highest ever recorded. 126 new candidates registered with the bank during August, bringing the total since January to 619. The invoice costs for temporary staffing were £300k less than in the same month last year. ▪ Recruitment - the average length of time to hire is 16 weeks. The pilot for the electronic request to recruit system has started at Queen's Square and the Heart Hospital and along with the implementation of E-CRB will further reduce the length of time to hire. The RCN fair took place on 15th & 16th September with 367 nursing candidates being matched to existing vacancies and invited to join the bank. Over 50 candidates have completed the Health Care Assistant Assessment process and it is expected that all HCA vacancies will be filled as a result of this initiative. ▪ The current under reporting of sickness absence remains an area of concern and a monthly compliance report will be circulated to Divisional Managers in October to tackle areas of non-compliance. The Sickness Absence Policy is under review and now includes a specific reference that all line managers must complete the Monthly Absence Forms and e-rota returns for nursing staff. Short term absence will now be monitored differently (4 or more episodes within a six month period) and 4 continuous weeks for long term sickness. ▪ The appraisals process is currently being reviewed by Workforce and Education and improvements will include a revised and simplified appraisals form, the development of an appraisals policy, using the outcomes from the appraisals process to inform the Trust’s annual training plan and more support and training for managers and staff.
WTE actual v plan 2010/11
01,0002,0003,0004,0005,0006,0007,0008,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Actual WTE Temp WTE Plan WTE
Trust % of Workforce Spend that is Temporary Staff
0%2%4%6%8%
10%12%14%16%
Apr May June July Aug Sept Oct Nov Dec Jan Feb Mar
2009/10 2010-11
21
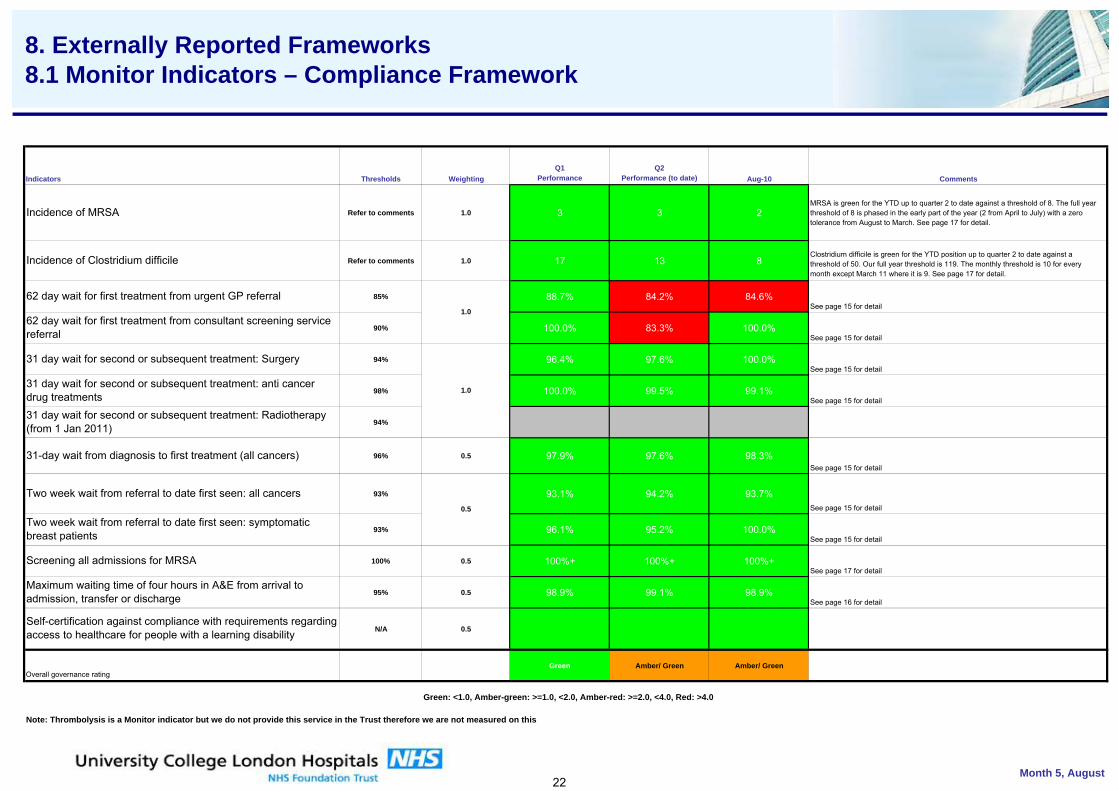
gudrhg
Thresholds WeightingQ1
PerformanceQ2
Performance (to date) Aug-10 Comments
Refer to comments 1.0 3 3 2MRSA is green for the YTD up to quarter 2 to date against a threshold of 8. The full year threshold of 8 is phased in the early part of the year (2 from April to July) with a zero tolerance from August to March. See page 17 for detail.
Refer to comments 1.0 17 13 8Clostridium difficile is green for the YTD position up to quarter 2 to date against a threshold of 50. Our full year threshold is 119. The monthly threshold is 10 for every month except March 11 where it is 9. See page 17 for detail.
85% 88.7% 84.2% 84.6%See page 15 for detail
90% 100.0% 83.3% 100.0%See page 15 for detail
94% 96.4% 97.6% 100.0%See page 15 for detail
98% 100.0% 99.5% 99.1%See page 15 for detail
94%
96% 0.5 97.9% 97.6% 98.3%See page 15 for detail
93% 93.1% 94.2% 93.7%See page 15 for detail
93% 96.1% 95.2% 100.0%See page 15 for detail
100% 0.5 100%+ 100%+ 100%+See page 17 for detail
95% 0.5 98.9% 99.1% 98.9%See page 16 for detail
N/A 0.5
Green Amber/ Green Amber/ Green
Green: <1.0, Amber-green: >=1.0, <2.0, Amber-red: >=2.0, <4.0, Red: >4.0
Note: Thrombolysis is a Monitor indicator but we do not provide this service in the Trust therefore we are not measured on this
Month 5, August
Overall governance rating
Self-certification against compliance with requirements regarding access to healthcare for people with a learning disability
Incidence of MRSA
Incidence of Clostridium difficile
Screening all admissions for MRSA
31 day wait for second or subsequent treatment: Radiotherapy (from 1 Jan 2011)
31 day wait for second or subsequent treatment: Surgery
Maximum waiting time of four hours in A&E from arrival to admission, transfer or discharge
31-day wait from diagnosis to first treatment (all cancers)
Two week wait from referral to date first seen: all cancers
Indicators
Two week wait from referral to date first seen: symptomatic breast patients
62 day wait for first treatment from urgent GP referral
62 day wait for first treatment from consultant screening service referral
31 day wait for second or subsequent treatment: anti cancer drug treatments
1.0
1.0
0.5
8. Externally Reported Frameworks 8.1 Monitor Indicators – Compliance Framework
22
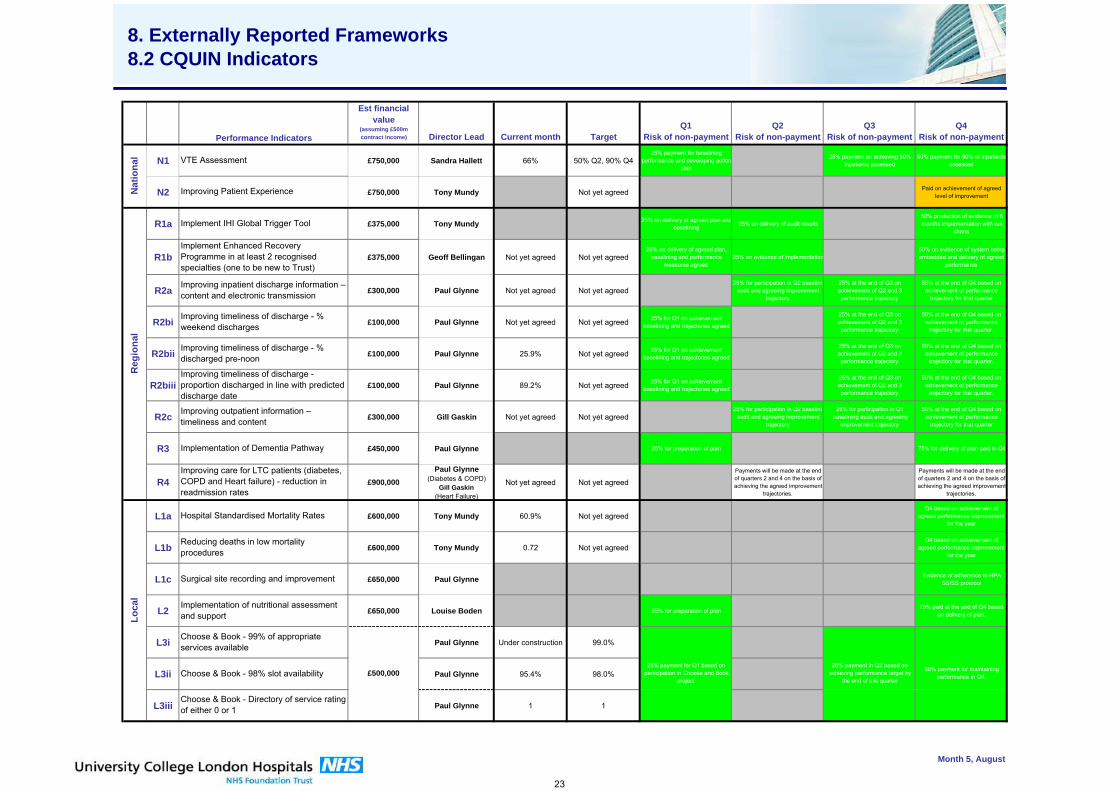
udrhg
Est financial value
(assuming £500m contract income) Director Lead Current month Target
Q1Risk of non-payment
Q2Risk of non-payment
Q3Risk of non-payment
Q4Risk of non-payment
N1 £750,000 Sandra Hallett 66% 50% Q2, 90% Q425% payment for baselining
performance and developing actionplan
25% payment on achieving 50% inpatients assessed
50% payment for 90% of inpatients assessed
N2 £750,000 Tony Mundy Not yet agreed Paid on achievement of agreed level of improvement
R1a £375,000 Tony Mundy 25% on delivery of agreed plan andbaselining
25% on delivery of audit results50% production of evidence of 6 months implementation with run
charts
R1b £375,000 Geoff Bellingan Not yet agreed Not yet agreed25% on delivery of agreed plan,
baselining and performance measures agreed
25% on evidence of implementation50% on evidence of system being embedded and delivery of agreed
performance
R2a £300,000 Paul Glynne Not yet agreed Not yet agreed25% for participation in Q2 baseline
audit and agreeing improvement trajectory
25% at the end of Q3 on achievement of Q2 and 3 performance trajectory
50% at the end of Q4 based on achievement of performance
trajectory for that quarter
R2bi £100,000 Paul Glynne Not yet agreed Not yet agreed 25% for Q1 on achievement baselining and trajectories agreed
25% at the end of Q3 on achievement of Q2 and 3 performance trajectory
50% at the end of Q4 based on achievement of performance
trajectory for that quarter.
R2bii £100,000 Paul Glynne 25.9% Not yet agreed 25% for Q1 on achievement baselining and trajectories agreed
25% at the end of Q3 on achievement of Q2 and 3 performance trajectory
50% at the end of Q4 based on achievement of performance
trajectory for that quarter.
R2biii £100,000 Paul Glynne 89.2% Not yet agreed 25% for Q1 on achievement baselining and trajectories agreed
25% at the end of Q3 on achievement of Q2 and 3 performance trajectory
50% at the end of Q4 based on achievement of performance
trajectory for that quarter.
R2c £300,000 Gill Gaskin Not yet agreed Not yet agreed25% for participation in Q2 baseline
audit and agreeing improvement trajectory
25% for participation in Q1 baselining audit and agreeing
improvement trajectory
50% at the end of Q4 based on achievement of performance
trajectory for that quarter
R3 £450,000 Paul Glynne 25% for preparation of plan 75% for delivery of plan paid in Q4
R4 £900,000Paul Glynne
(Diabetes & COPD)Gill Gaskin
(Heart Failure)
Not yet agreed Not yet agreedPayments will be made at the end of quarters 2 and 4 on the basis of achieving the agreed improvement
trajectories.
Payments will be made at the end of quarters 2 and 4 on the basis of achieving the agreed improvement
trajectories.
L1a £600,000 Tony Mundy 60.9% Not yet agreedQ4 based on achievement of
agreed performance improvement for the year
L1b £600,000 Tony Mundy 0.72 Not yet agreedQ4 based on achievement of
agreed performance improvement for the year
L1c £650,000 Paul Glynne Evidence of adherence to HPA SSISS protocol
L2 £650,000 Louise Boden 25% for preparation of plan75% paid at the end of Q4 based
on delivery of plan.
L3i Paul Glynne Under construction 99.0%
L3ii Paul Glynne 95.4% 98.0%
L3iii Paul Glynne 1 1
7000000
Red Month 5, AugustAmberGreen
25% payment for Q1 based on participation in Choose and Book
project
25% payment in Q3 based on achieving performance target by
the end of this quarter
50% payment for maintaining performance in Q4.
Performance Indicators
Implementation of nutritional assessment and support
Improving timeliness of discharge - % discharged pre-noon
Improving timeliness of discharge - proportion discharged in line with predicted discharge date
Improving outpatient information – timeliness and content
Choose & Book - Directory of service rating of either 0 or 1
Implementation of Dementia Pathway
Choose & Book - 98% slot availability
Choose & Book - 99% of appropriate services available
£500,000
Loca
l
Hospital Standardised Mortality Rates
Surgical site recording and improvement
Reducing deaths in low mortality procedures
Reg
iona
lN
atio
nal VTE Assessment
Improving Patient Experience
Implement IHI Global Trigger Tool
Implement Enhanced Recovery Programme in at least 2 recognised specialties (one to be new to Trust)
Improving inpatient discharge information – content and electronic transmission
Improving timeliness of discharge - % weekend discharges
Improving care for LTC patients (diabetes, COPD and Heart failure) - reduction in readmission rates
8. Externally Reported Frameworks 8.2 CQUIN Indicators8. Externally Reported Frameworks 8.2 CQUIN Indicators8. Externally Reported Frameworks 8.2 CQUIN Indicators8. Externally Reported Frameworks 8.2 CQUIN Indicators
23
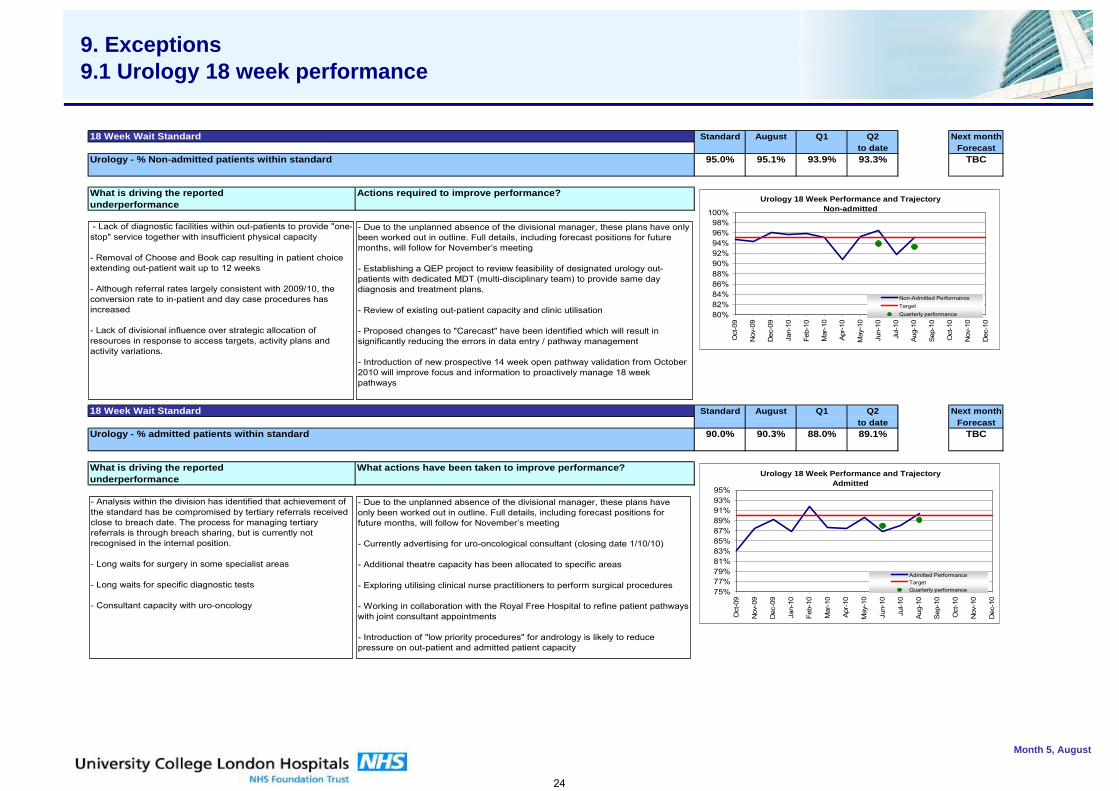
udrhg
7000000
Month 5, August
8. Externally Reported Frameworks 8.2 CQUIN Indicators8. Externally Reported Frameworks 8.2 CQUIN Indicators8. Externally Reported Frameworks 8.2 CQUIN Indicators9. Exceptions9.1 Urology 18 week performance
18 Week Wait Standard Standard August Q1 Q2 Next monthto date Forecast
Urology - % Non-admitted patients within standard 95.0% 95.1% 93.9% 93.3% TBC
What is driving the reported Actions required to improve performance?underperformance
18 Week Wait Standard Standard August Q1 Q2 Next monthto date Forecast
Urology - % admitted patients within standard 90.0% 90.3% 88.0% 89.1% TBC
What is driving the reported What actions have been taken to improve performance?underperformance
Urology 18 Week Performance and TrajectoryNon-admitted
80%82%84%86%88%90%92%94%96%98%
100%
Oct
-09
Nov
-09
Dec
-09
Jan-
10
Feb-
10
Mar
-10
Apr
-10
May
-10
Jun-
10
Jul-1
0
Aug-
10
Sep-
10
Oct
-10
Nov
-10
Dec
-10
Non-Admitted PerformanceTargetQuarterly performance
Urology 18 Week Performance and TrajectoryAdmitted
75%77%79%81%83%85%87%89%91%93%95%
Oct
-09
Nov
-09
Dec
-09
Jan-
10
Feb-
10
Mar
-10
Apr-
10
May
-10
Jun-
10
Jul-1
0
Aug
-10
Sep
-10
Oct
-10
Nov
-10
Dec
-10
Admitted PerformanceTargetQuarterly performance
- Lack of diagnostic facilities within out-patients to provide "one-stop" service together with insufficient physical capacity
- Removal of Choose and Book cap resulting in patient choice extending out-patient wait up to 12 weeks
- Although referral rates largely consistent with 2009/10, the conversion rate to in-patient and day case procedures has increased
- Lack of divisional influence over strategic allocation of resources in response to access targets, activity plans and activity variations.
- Due to the unplanned absence of the divisional manager, these plans have only been worked out in outline. Full details, including forecast positions for future months, will follow for November’s meeting
- Establishing a QEP project to review feasibility of designated urology out-patients with dedicated MDT (multi-disciplinary team) to provide same day diagnosis and treatment plans.
- Review of existing out-patient capacity and clinic utilisation
- Proposed changes to "Carecast" have been identified which will result in significantly reducing the errors in data entry / pathway management
- Introduction of new prospective 14 week open pathway validation from October 2010 will improve focus and information to proactively manage 18 week pathways
- Analysis within the division has identified that achievement of the standard has be compromised by tertiary referrals received close to breach date. The process for managing tertiary referrals is through breach sharing, but is currently not recognised in the internal position.
- Long waits for surgery in some specialist areas
- Long waits for specific diagnostic tests
- Consultant capacity with uro-oncology
- Due to the unplanned absence of the divisional manager, these plans have only been worked out in outline. Full details, including forecast positions for future months, will follow for November’s meeting
- Currently advertising for uro-oncological consultant (closing date 1/10/10)
- Additional theatre capacity has been allocated to specific areas
- Exploring utilising clinical nurse practitioners to perform surgical procedures
- Working in collaboration with the Royal Free Hospital to refine patient pathways with joint consultant appointments
- Introduction of "low priority procedures" for andrology is likely to reduce pressure on out-patient and admitted patient capacity
24
G
Agenda Item 10
Quality & Safety Committee Report
University College London Hospitals NHS Foundation Trust September Quality & Safety Committee Summary to the Board of Directors
Patient outcomes & effectiveness 1. NICE guidance exception report QSC noted that to comply with CG49- Faecal incontinence - work is underway to develop an integrated, Trust-wide, continence service. Nutrition support in adults - remains a red non-compliance and for Acutely ill patients in hospital -cross Trust audits are underway.
2. Scorecards/quality indicators 2.1 Infection division Infection junior doctors rated their training as outstanding in recent feedback. Actions are in place to address the lower than trajectory score on VTE risk assessments in August, including nomination of a junior doctor clinical champion and revision of the audit tool. Good progress has been made with the appropriateness of antimicrobial prescribing, but recording duration of treatment remains low and is being addressed. 2.2 Pathology division The percentage of departments maintaining Clinical Pathology UK Accreditation is 91% but anticipated to be 100% soon. Issues with turnaround times are being addressed with individual service users. 2.3 The Heart Hospital division Continued excellent results from patient experience monthly audits. Significant improvement in venous thromboembolism (VTE) risk assessment with a lapse in August. A trajectory for improvement has been set. Onsite blood fridge now installed to improve blood traceability compliance. 2.4 Paediatric division A local PICKER survey has been developed and implemented to address the fact that children’s and young people’s opinions on their care are not sought routinely as part of the national patient survey. 91% of young people thought that the care they received was excellent or very good. 97% said that they would recommend the unit to a family member or friend. Results to be included on QSC scorecard. OFSTED evaluation of Serious Case Review (SCR) by Islington Safeguarding Board reported to Trust as a contributor. UCLH’s contribution to the SCR was considered adequate with some points of learning not adequately covered by our report, although overall the report’s recommendations and actions are deemed acceptable. Action plan is in place. Two recent cases of C.difficile two months apart on T12S were investigated. Management of both cases was reviewed and judged to be appropriate.
2.4.1 NHS London Safeguarding Inspection Service evaluated jointly with Camden in July 2010. Results overall very positive with culture of safeguarding at UCLH singled out for praise. Action plan is in place to cover all areas of concern. A review of the capacity of safeguarding sessions for the Named Doctor role indicates that an additional session is required. Dr Petropolous will be the Named Doctor whilst Dr Begent is on maternity leave. 2.5 Gastrointestinal division Improvements reported with hand hygiene compliance, documented duration of antibiotic therapy and antibiotic prescribing compliance. VTE assessment has improved close to 60%. MRSA screening for electives and all admissions remains a
concern, a trajectory is in place and there is joint working with pre assessment / ITU and daily review of all patients status. In relation to NICE guidance on nutrition support in adults - a business case is in first draft and administrative support has been identified to support the specialist nutrition service. A number of complaints cite delays and confusion in administration communication. A review has been undertaken and actions are in place to address. General issues 3. Plain film (PF) reporting performance 2009-2010 For all imaging modalities inpatient demand is constant but outpatient demand is rising ~14%. Since May 2009 there has been a 50% rise in monthly inpatient PF reporting with concurrent fall in unreported volumes. A variety of actions have been taken to improve PF reporting including the appointment of five additional staff, promotion of skill mix, introduction of teleradiology allowing extended days, coverage and weekend working. Despite problems with the RIS and PACS systems average turnaround for the emergency services is now 24 hours and there are virtually no unreported films now for cancer inpatients. Infection Control
4.1 Infection Scorecard The Director for Infection Prevention & Control reported a gap in assurance on ventilation validation as a number of theatres had failed to meet the standard. NHNN theatres do not meet the current buildings standard and will require extensive work in future. Surveillance of wound infection did not identify trends in infection associated with air quality in this area. Consideration is to be given to whether Facilities should be formally represented at the QSC and present a scorecard.. There have been six cases of MRSA so far this year. The Trust is unlikely to achieve the target threshold of eight cases at year end. Actions to address include a focus on surgical site infection and the management of line infection in complex patients. 4.2 Annual Infection Control Report 2009-10 The Trust achieved the MRSA bacteraemia and Clostridium difficile improvement objectives. 25 MRSA bacteraemias against a trajectory of 39. 88 Clostridium difficile cases against a trajectory of 127. The three core objectives for 2010 are to reduce Health care acquired infection (HCAI) acquisition and transmission, to achieve HCAI reduction objectives and to support and enhance the Trust’s quality and safety agenda . Focus will be upon the CQUIN target for urinary tract infections, an electronic solution to training and establishing an infection control nurse post for the environment. 5. Controlled Drugs (CD)
5.1 Accountable Officer Controlled Drug (CD) Report Q1 April –June 10 No concerns were raised. Completion of the Ward Pharmacist / Sister monthly CD Audits remain above 90%. There was an increase in incidents reported, from the usual monthly total of 12 to 22, in May 2010. Upon review, the majority of incidents involved no patient harm although 3 were associated with minimal harm. No particular pattern identified of type of error or area from which errors reported. Local actions appear appropriate and no specific issues of concern. 5.2 NHS Camden Controlled Drug Local Intelligence Network (LIN) Occurrence Report – Controlled Drugs Concerns Accountable officer Q1 LIN return flagged no specific areas of concern from UCLH.
6. Reports from QSC sub-committees 6.1 Clinical Effectiveness Steering Group (CESG) – June, July & August
2010 In light of the need to provide Board assurance around clinical audit the CESG highlighted the trusts inability to fully comply with the national criteria and indicators of best practice (HQIP 2009) because there is no protected time to participate (indicator 3.2), nor a clinical audit department providing practical support with logistics, administration, analysis, data collection and IT systems (indicator 3.3). Professor Tooke is to raise this to the Board. The CESG also highlighted a lack of approved training nationally for breaking bad news. IDM for cancer and the education department are to address.
6.2 Research Governance Committee July 2010 Communication to be improved between UCL and the Director of Research and Development regarding disciplinary processes.
6.3 Medical Records Task and Finish group The taskforce group met three times between June and September 2010. The updated action plan was reported to the September Risk Co-ordination Board (RCB). At this meeting it was agreed that the taskforce be dissolved and that responsibility for ongoing monitoring of the action plan should pass to the Records Improvement Steering Group (RSIG). Most actions complete. Outstanding actions (Amber) are underway and expect to be completed in 4-6 weeks. RSIG and Information, Communication and Technology Strategy Board will monitor completion of actions. 7. Venous Thromboembolism prevention Overall Trust improvement in documented VTE risk assessments to 66%, critical care scored > 90%, improvements seen in Cancer (79%), Medical specialities (76%), Emergency services (71%), Queens Square (69%) but deterioration of performance seen in 7 divisions. Further actions must be taken by all divisions in order to meet the 90% quarter four target. 8. WHO Safe Surgery checklist re launch The checklist has been updated to include a check for pregnancy, MRSA and sign out alerts for ITU. It is to be re launched on October 1st 2010. Maria Adiseshiah On behalf of Tony Mundy Medical Director
H
Agenda Item 11
HR & Communications Report
Board of Directors – October 2010
Summary Report from the HR & Communications Committee
1. The new Workforce Director is working with the Chair of the HRCC to ensure
that it meets its terms of reference. There is concern that this Committee has been drawn into executive areas of work. The membership of the group will be reviewed with the Chair of the meeting. The Committee currently addresses a number of issues which are required to be reported including issues necessary for NHS Level 3 compliance. The necessity of this will be reviewed.
2. As part of this review a structured agenda has been developed containing a
small number of overview papers rather than separate, numerous papers on a range of detailed issues. This includes a Workforce Director’s Report, a Director of Education’s report and a Communication Report. In addition each committee meeting will spend a period of protected time considering a strategic issue.
3. As part of the Director of Education’s report to the HRCC the progress on
mandatory and statutory training compliance was reported. As a result of a considerable piece of work the Trust is now able to report on compliance with this important agenda. Compliance varies considerably for each of the mandatory training programmes (as outlined in the Trust’s training needs analysis) ranging from 0% to 67%. Progress on compliance rates will be led through the Education Board and reported to the HRCC.
4. At the September meeting the strategic issue addressed was the Electronic
Staff Record programme which is creating and implementing a comprehensive, easily accessible on-line employee record incorporating all staff and management data. This will be the single ‘record of truth’ and will feed other IT systems where necessary. The Programme has delivered improvements in payroll, the average length of time to hire, recording and monitoring of training administration (including appraisals). With planned developments during the next six months (including the roll-out of Manager self-service) the programme will improve productivity and allow staff to be able to devote more of their time to manage services which in turn will realise more improved and effective patient care. There was a short discussion regarding Employee Self-Service and possible Trust wide solutions for e-Rostering and Learning Management where further work is required to identify possible benefits for each of these. The Committee noted the progress and planned developments for this Programme.
5. As a result of the government’s decision to reconsider (and therefore put on
hold) the proposed Vetting and Barring scheme, the Trust has undertaken a review of staff who may require CRB clearance and were employed before 2005. This review has identified a total of 1,825 employees, 849 of whom are employed in roles where they may engage in a regulated activity. The Executive Board have considered this issue and requested retrospective CRB checks for the 1,825 employees. Critical to the overall project’s success will be the engagement with local managers and staff and specifically line managers taking full responsibility for ensuring their employees comply with the EB’s instructions.
6. The Committee was asked to consider the findings of three in-house audits
(professional registration; pre-employment checks for substantive staff; pre-employment checks for temporary staff) and two internal audits (Sickness Absence and Bullying and Harassment) and note the required actions. The Committee acknowledged that it was satisfied that monitoring was taking place and appropriate action taken to ensure compliance.
7. The Committee discussed and endorsed the following nine workforce policies:
• Control of Substances Hazardous to Health (COSHH) • Healthcare workers with HIV, Hep B and Hep C • Slips, trips and falls • First Aid • Latex • Managing Performance • Grievance • CRB • Pre-Appointment and In-Post Employment Checks
8. The Committee reviewed the following risks (as identified on the Workforce
Risk Register) and acknowledged that it was satisfied that appropriate action was being taken to minimise risk.
• Honorary Contracts • Reporting of sickness absence • Local agreements • Appraisals • Bullying and Harassment • Workforce Planning
9. The Committee discussed the Trust’s sickness absence rate. For August
this was reported as 2.3%. The Workforce Performance Report identifies two potential causes of under-reporting: • Around 60% of the Trust’s staff report sickness absence through a
Monthly Absence Form (MAF). The MAF return rate was 46% in August. A low MAF return rate ultimately affects the reliability of the sickness absence rate and urgent action is required to resolve this issue.
• Late inputting of sickness data: Evidence has shown that the sickness absence rates increase over time. This suggests that either the inputting (by payroll) is not completed on time or MAF forms are being submitted and recorded late.
10. It is recognised that previous Workforce Planning has tended to operate in isolation, with limited coordination between Clinical Boards and Corporate directorates. Going forward it is proposed that a UCLH Workforce Strategy and Workforce Plan be developed as part of the 2011/2012 business planning cycle. Discussions at the HRCC will inform this process. The Committee acknowledge the importance of developing a Workforce Strategy and agreed to contribute to its development.
11. The Associate Director of Communications presented her Communications
Report. This detailed that:
• There has been positive coverage in the local press with the communication’s unit co-ordinating a time capsule burial at the Cancer Centre and photographs of the event were published in the Camden Gazette and Camden New Journal.
• A full page archive feature was placed in the Ham & High ‘Heritage’ section celebrating the 100th anniversary of Florence Nightingale’s death with an interview with Louise Boden about how nursing has changed over the years. UCLH was featured as a beacon of excellence for its paediatric and adolescent care on the BBC 6 O’Clock News and the Trust was featured in a broader piece about Sir Ian Kennedy’s report into children’s services.
• Less positive was the coverage of the so called `superbug outbreak’ on the neonatal unit which was covered in the London TV news and national media.
• The team has been working with the Royal London Hospital for Integrated Medicine on their name change. This has included updating templates and internal communications about the hospital in Inside Story and on Insight.
David Wherrett Workforce Director
Sue Atkinson NED, Chair HRCC 7th October 2010
I
Agenda Item 12
Finance & Contracting Committee Report
Report Title: Finance and Contracting Committee Report Approved by: Richard Alexander Prepared by: Tim Jaggard Date prepared: 7th October 2010 Submission to: Board of Directors – 13th October 2010 Previous papers: N/A Reference documents:
N/A
Purpose of the paper/report: This report updates the Board of Directors on the issues, considered at the meeting of the Finance and Contracting Committee (FCC) on 6th October 2010, relating to the financial performance and contracting position of the Trust as at August 2010. Issues/Action/Recommendation: The Board of Directors is asked to:
• Note the financial performance for the first five months of the current financial year. • Note the contracting update presented to the FCC. • Note the cancer centre update presented to FCC.
Financial Implications: N/A
Other Implications: N/A
Page 1 of 7
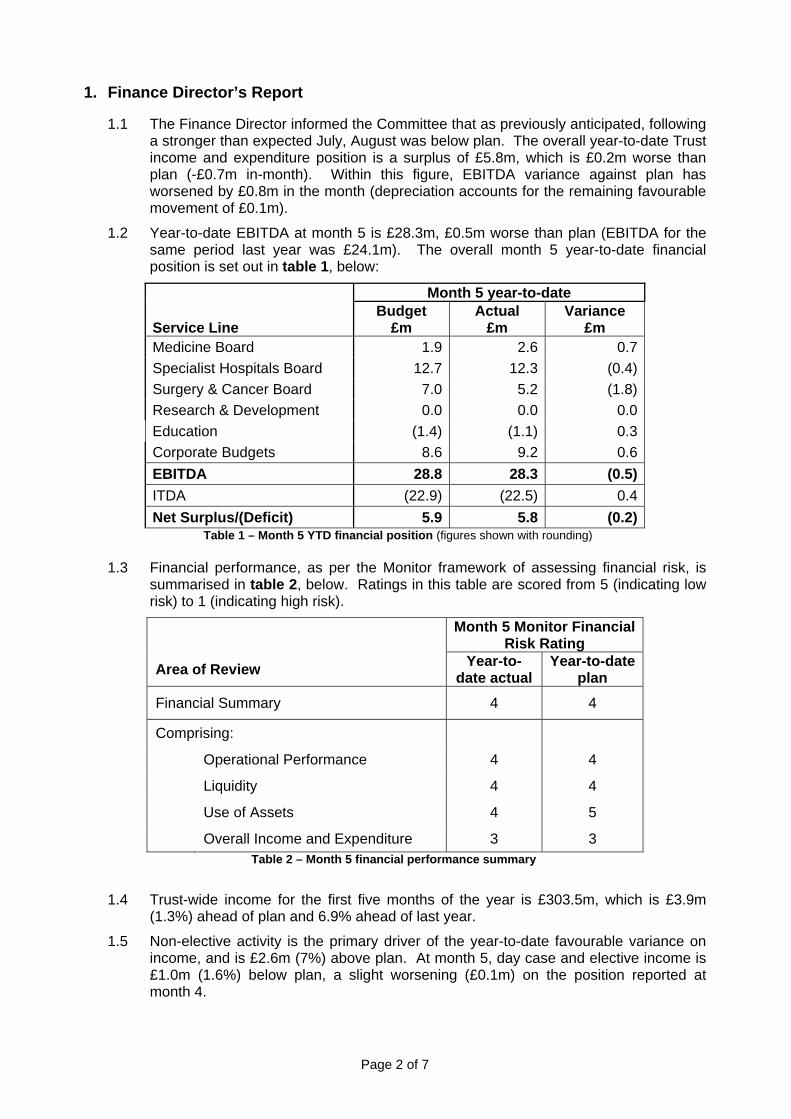
Page 2 of 7
1. Finance Director’s Report
1.1 The Finance Director informed the Committee that as previously anticipated, following a stronger than expected July, August was below plan. The overall year-to-date Trust income and expenditure position is a surplus of £5.8m, which is £0.2m worse than plan (-£0.7m in-month). Within this figure, EBITDA variance against plan has worsened by £0.8m in the month (depreciation accounts for the remaining favourable movement of £0.1m).
1.2 Year-to-date EBITDA at month 5 is £28.3m, £0.5m worse than plan (EBITDA for the same period last year was £24.1m). The overall month 5 year-to-date financial position is set out in table 1, below:
Month 5 year-to-date Service Line
Budget £m
Actual £m
Variance £m
Medicine Board 1.9 2.6 0.7 Specialist Hospitals Board 12.7 12.3 (0.4) Surgery & Cancer Board 7.0 5.2 (1.8) Research & Development 0.0 0.0 0.0 Education (1.4) (1.1) 0.3 Corporate Budgets 8.6 9.2 0.6 EBITDA 28.8 28.3 (0.5) ITDA (22.9) (22.5) 0.4 Net Surplus/(Deficit) 5.9 5.8 (0.2)
Table 1 – Month 5 YTD financial position (figures shown with rounding) 1.3 Financial performance, as per the Monitor framework of assessing financial risk, is
summarised in table 2, below. Ratings in this table are scored from 5 (indicating low risk) to 1 (indicating high risk).
Month 5 Monitor Financial Risk Rating
Area of Review Year-to-date actual
Year-to-date plan
Financial Summary 4 4
Comprising:
Operational Performance 4 4
Liquidity 4 4
Use of Assets 4 5
Overall Income and Expenditure 3 3 Table 2 – Month 5 financial performance summary
1.4 Trust-wide income for the first five months of the year is £303.5m, which is £3.9m
(1.3%) ahead of plan and 6.9% ahead of last year.
1.5 Non-elective activity is the primary driver of the year-to-date favourable variance on income, and is £2.6m (7%) above plan. At month 5, day case and elective income is £1.0m (1.6%) below plan, a slight worsening (£0.1m) on the position reported at month 4.
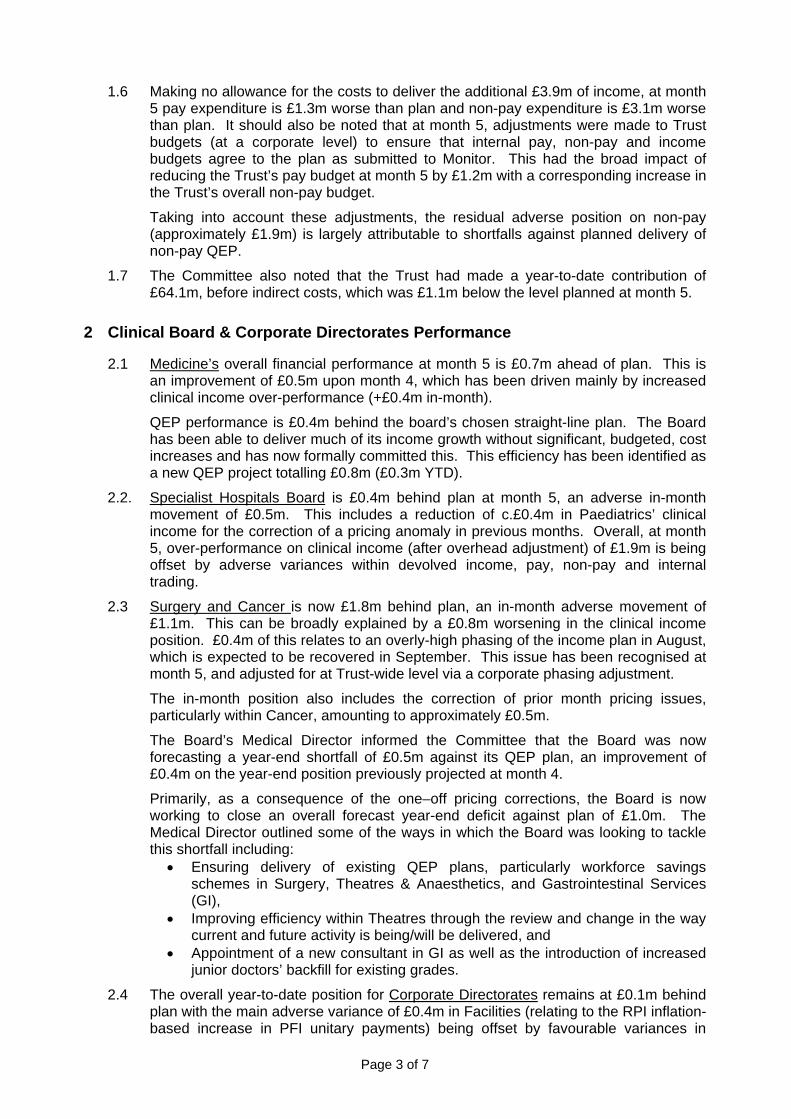
Page 3 of 7
1.6 Making no allowance for the costs to deliver the additional £3.9m of income, at month 5 pay expenditure is £1.3m worse than plan and non-pay expenditure is £3.1m worse than plan. It should also be noted that at month 5, adjustments were made to Trust budgets (at a corporate level) to ensure that internal pay, non-pay and income budgets agree to the plan as submitted to Monitor. This had the broad impact of reducing the Trust’s pay budget at month 5 by £1.2m with a corresponding increase in the Trust’s overall non-pay budget.
Taking into account these adjustments, the residual adverse position on non-pay (approximately £1.9m) is largely attributable to shortfalls against planned delivery of non-pay QEP.
1.7 The Committee also noted that the Trust had made a year-to-date contribution of £64.1m, before indirect costs, which was £1.1m below the level planned at month 5.
2 Clinical Board & Corporate Directorates Performance
2.1 Medicine’s overall financial performance at month 5 is £0.7m ahead of plan. This is an improvement of £0.5m upon month 4, which has been driven mainly by increased clinical income over-performance (+£0.4m in-month).
QEP performance is £0.4m behind the board’s chosen straight-line plan. The Board has been able to deliver much of its income growth without significant, budgeted, cost increases and has now formally committed this. This efficiency has been identified as a new QEP project totalling £0.8m (£0.3m YTD).
2.2. Specialist Hospitals Board is £0.4m behind plan at month 5, an adverse in-month movement of £0.5m. This includes a reduction of c.£0.4m in Paediatrics’ clinical income for the correction of a pricing anomaly in previous months. Overall, at month 5, over-performance on clinical income (after overhead adjustment) of £1.9m is being offset by adverse variances within devolved income, pay, non-pay and internal trading.
2.3 Surgery and Cancer is now £1.8m behind plan, an in-month adverse movement of £1.1m. This can be broadly explained by a £0.8m worsening in the clinical income position. £0.4m of this relates to an overly-high phasing of the income plan in August, which is expected to be recovered in September. This issue has been recognised at month 5, and adjusted for at Trust-wide level via a corporate phasing adjustment.
The in-month position also includes the correction of prior month pricing issues, particularly within Cancer, amounting to approximately £0.5m.
The Board’s Medical Director informed the Committee that the Board was now forecasting a year-end shortfall of £0.5m against its QEP plan, an improvement of £0.4m on the year-end position previously projected at month 4.
Primarily, as a consequence of the one–off pricing corrections, the Board is now working to close an overall forecast year-end deficit against plan of £1.0m. The Medical Director outlined some of the ways in which the Board was looking to tackle this shortfall including:
• Ensuring delivery of existing QEP plans, particularly workforce savings schemes in Surgery, Theatres & Anaesthetics, and Gastrointestinal Services (GI),
• Improving efficiency within Theatres through the review and change in the way current and future activity is being/will be delivered, and
• Appointment of a new consultant in GI as well as the introduction of increased junior doctors’ backfill for existing grades.
2.4 The overall year-to-date position for Corporate Directorates remains at £0.1m behind plan with the main adverse variance of £0.4m in Facilities (relating to the RPI inflation-based increase in PFI unitary payments) being offset by favourable variances in
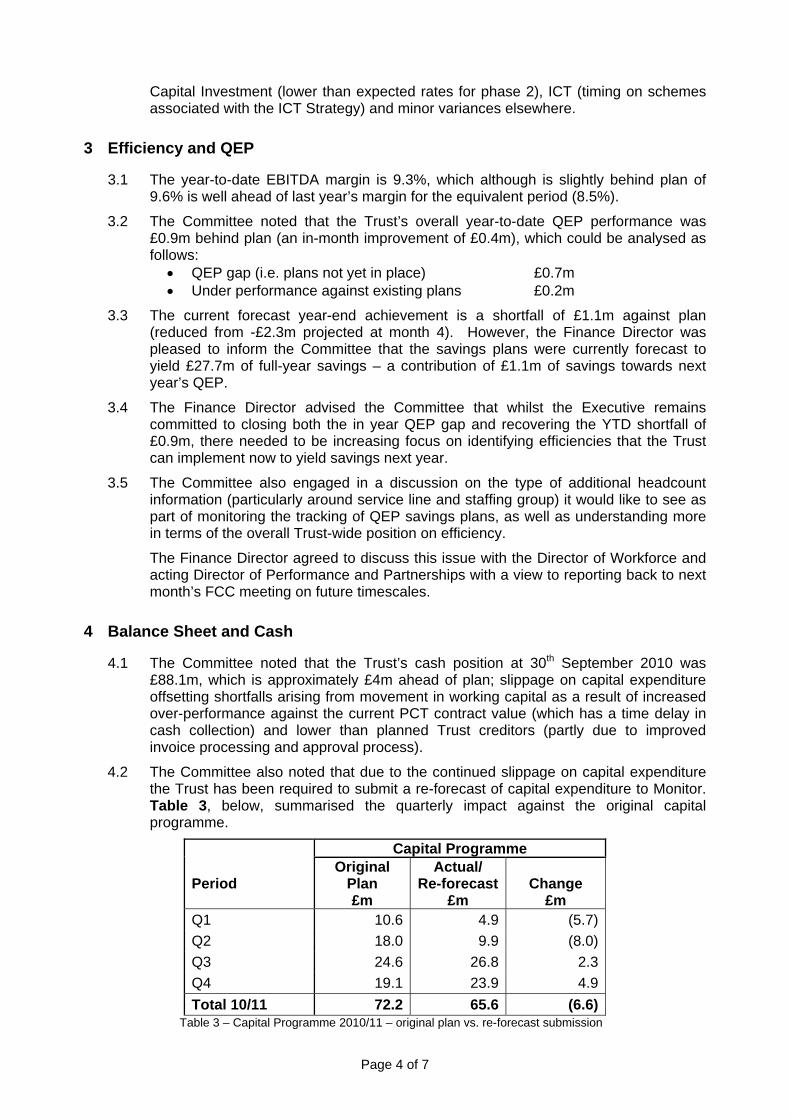
Page 4 of 7
Capital Investment (lower than expected rates for phase 2), ICT (timing on schemes associated with the ICT Strategy) and minor variances elsewhere.
3 Efficiency and QEP
3.1 The year-to-date EBITDA margin is 9.3%, which although is slightly behind plan of 9.6% is well ahead of last year’s margin for the equivalent period (8.5%).
3.2 The Committee noted that the Trust’s overall year-to-date QEP performance was £0.9m behind plan (an in-month improvement of £0.4m), which could be analysed as follows:
• QEP gap (i.e. plans not yet in place) £0.7m • Under performance against existing plans £0.2m
3.3 The current forecast year-end achievement is a shortfall of £1.1m against plan (reduced from -£2.3m projected at month 4). However, the Finance Director was pleased to inform the Committee that the savings plans were currently forecast to yield £27.7m of full-year savings – a contribution of £1.1m of savings towards next year’s QEP.
3.4 The Finance Director advised the Committee that whilst the Executive remains committed to closing both the in year QEP gap and recovering the YTD shortfall of £0.9m, there needed to be increasing focus on identifying efficiencies that the Trust can implement now to yield savings next year.
3.5 The Committee also engaged in a discussion on the type of additional headcount information (particularly around service line and staffing group) it would like to see as part of monitoring the tracking of QEP savings plans, as well as understanding more in terms of the overall Trust-wide position on efficiency.
The Finance Director agreed to discuss this issue with the Director of Workforce and acting Director of Performance and Partnerships with a view to reporting back to next month’s FCC meeting on future timescales.
4 Balance Sheet and Cash
4.1 The Committee noted that the Trust’s cash position at 30th September 2010 was £88.1m, which is approximately £4m ahead of plan; slippage on capital expenditure offsetting shortfalls arising from movement in working capital as a result of increased over-performance against the current PCT contract value (which has a time delay in cash collection) and lower than planned Trust creditors (partly due to improved invoice processing and approval process).
4.2 The Committee also noted that due to the continued slippage on capital expenditure the Trust has been required to submit a re-forecast of capital expenditure to Monitor. Table 3, below, summarised the quarterly impact against the original capital programme.
Capital Programme Period
Original Plan £m
Actual/ Re-forecast
£m
Change
£m Q1 10.6 4.9 (5.7) Q2 18.0 9.9 (8.0) Q3 24.6 26.8 2.3 Q4 19.1 23.9 4.9 Total 10/11 72.2 65.6 (6.6)
Table 3 – Capital Programme 2010/11 – original plan vs. re-forecast submission
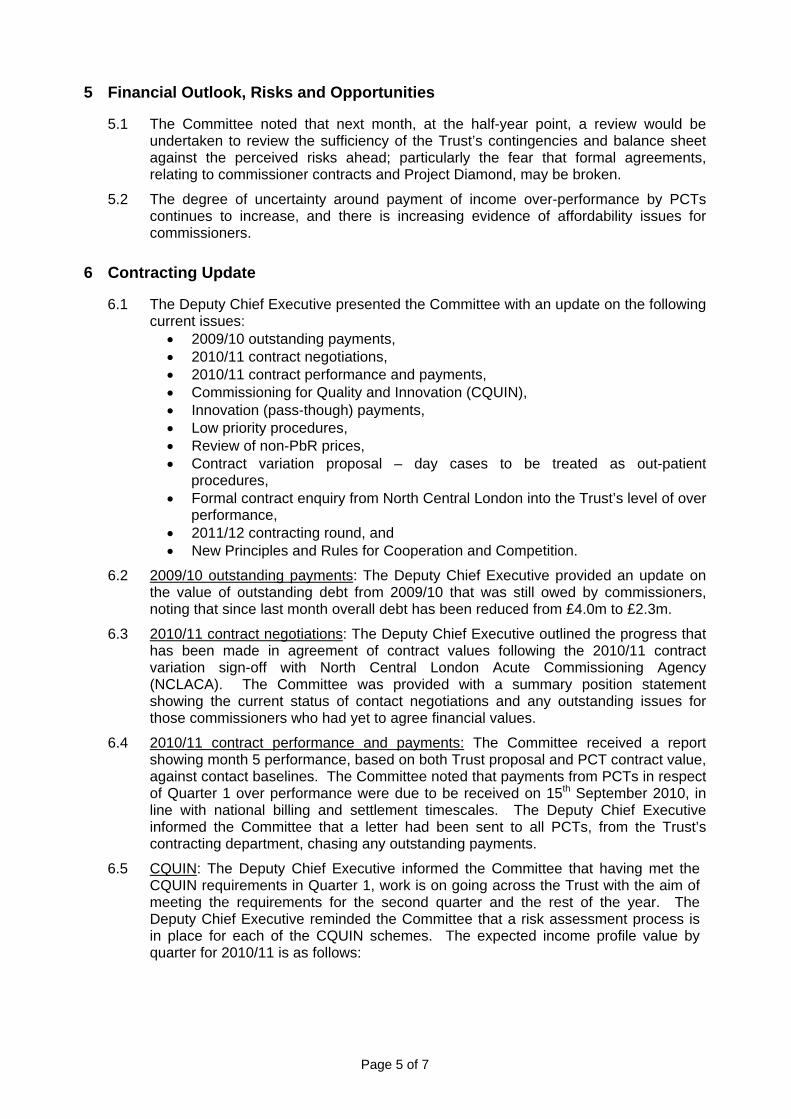
Page 5 of 7
5 Financial Outlook, Risks and Opportunities
5.1 The Committee noted that next month, at the half-year point, a review would be undertaken to review the sufficiency of the Trust’s contingencies and balance sheet against the perceived risks ahead; particularly the fear that formal agreements, relating to commissioner contracts and Project Diamond, may be broken.
5.2 The degree of uncertainty around payment of income over-performance by PCTs continues to increase, and there is increasing evidence of affordability issues for commissioners.
6 Contracting Update
6.1 The Deputy Chief Executive presented the Committee with an update on the following current issues:
• 2009/10 outstanding payments, • 2010/11 contract negotiations, • 2010/11 contract performance and payments, • Commissioning for Quality and Innovation (CQUIN), • Innovation (pass-though) payments, • Low priority procedures, • Review of non-PbR prices, • Contract variation proposal – day cases to be treated as out-patient
procedures, • Formal contract enquiry from North Central London into the Trust’s level of over
performance, • 2011/12 contracting round, and • New Principles and Rules for Cooperation and Competition.
6.2 2009/10 outstanding payments: The Deputy Chief Executive provided an update on the value of outstanding debt from 2009/10 that was still owed by commissioners, noting that since last month overall debt has been reduced from £4.0m to £2.3m.
6.3 2010/11 contract negotiations: The Deputy Chief Executive outlined the progress that has been made in agreement of contract values following the 2010/11 contract variation sign-off with North Central London Acute Commissioning Agency (NCLACA). The Committee was provided with a summary position statement showing the current status of contact negotiations and any outstanding issues for those commissioners who had yet to agree financial values.
6.4 2010/11 contract performance and payments: The Committee received a report showing month 5 performance, based on both Trust proposal and PCT contract value, against contact baselines. The Committee noted that payments from PCTs in respect of Quarter 1 over performance were due to be received on 15th September 2010, in line with national billing and settlement timescales. The Deputy Chief Executive informed the Committee that a letter had been sent to all PCTs, from the Trust’s contracting department, chasing any outstanding payments.
6.5 CQUIN: The Deputy Chief Executive informed the Committee that having met the CQUIN requirements in Quarter 1, work is on going across the Trust with the aim of meeting the requirements for the second quarter and the rest of the year. The Deputy Chief Executive reminded the Committee that a risk assessment process is in place for each of the CQUIN schemes. The expected income profile value by quarter for 2010/11 is as follows:
Page 6 of 7
Period £m Quarter 1 1.0 Quarter 2 0.8 Quarter 3 0.4 Quarter 4 5.3 TOTAL 2010/11 7.5 Table 4 – 2010/11 expected quarterly CQUIN profile
6.6 Innovation (pass-through) payments: The Committee was provided with a summary of
the current status of innovation payment business cases previously submitted by the Trust to NCLACA. The Deputy Chief Executive informed the Committee that a meeting had taken place with Medical Directors in September in order to review the position on each business case and it was agreed to strengthen those previously rejected, particularly focusing on the points that commissioners had used to reject the case, with a view to resubmitting for further consideration.
The Committee also noted that the discussions had started to take place with the Comprehensive Biochemical Research Centre (CRBC) with a view to strengthening the business case process in relation to all clinical developments arising from a research and development pathway.
6.7 Low priority procedures: The Deputy Chief Executive informed the Committee that a process has been established within the Trust to adhere to the new requirements on low priority procedures. The Deputy Chief Executive advised the Committee, however, that the Trust has refused to extend administration in the process by copying in referral management centres, as this could lead to an undermining of the relationship of the Trust with its referring GP practitioners and the prospect of patients getting “lost in the system” leading to poor patient experience and potentially patient safety issues. The Trust has taken the view that the internal communication requirements of commissioners should be for them to manage, and additional process and costs should not be incurred by Trusts.
6.8 Review of non-PbR process: The Committee noted that NCLACA has written to all NCL sector trusts advising that they will be undertaking an in depth review of non-PbR prices across all acute trusts for which they are the lead commissioner. The Deputy Chief Executive advised the Committee that they would be kept updated on the progress of this issue.
6.9 Contract Variation Proposal - Day Cases to be treated as Outpatient Procedures: The Deputy Chief Executive informed the Committee that NCLACA have issued a contract variation proposal, dated 22nd September, which requires a number of procedures currently performed on a day case basis to be treated (and paid for) as outpatient procedures. They have split the day case procedures into three categories and are seeking to have the change from day case to outpatient phased between October 2010 and March 2011.
The Committee noted that the categories relate to a commissioner view of the procedures that could/should be undertaken on outpatient settings, and that as a result the Trust would analyse, review and determine an appropriate response. The Committee would again be kept informed on progress.
6.10 Formal contract enquiry from North Central London into the Trust’s level of over performance: The Committee noted that a letter had been received from NCLACA, dated 24th September, in which they had raised a substantial number of issues and queries, central to which is a price and volume analysis (relating to the Trust’s billing for the first four months this year).
Page 7 of 7
The Deputy Chief Executive informed the Committee that the Trust will deliver a response within the contractual timescale of 10 working days.
6.11 2011/12 contracting round: The Committee noted the Trust’s response to the Department of Health regarding potential changes to the NHS standard contract for 2011/12.
6.12 New Principles and Rules for Cooperation and Competition: The Committee noted that following a consultation, Monitor had advised that new “Principles and Rules for Cooperation and Competition” will apply to NHS foundation trusts from 1st October 2010.
7 Cancer Centre Update
7.1 The Medical Director for Surgery and Cancer presented the Committee with a paper showing updated financial projections for the Cancer Centre and a comparison with the approved financial investment case (FIC).
The Committee noted the following key issues: • Both activity and income were ahead of the FIC at month 4. • Overall I&E projections are better than the FIC, and this improvement is due to
increased activity, especially day cases, and the favourable impact of HRG4. • Although the update currently shows a projected shortfall in non-clinical
income, discussions are under way with commercial entities in respect of leasing floor space.
• Discussions are also ongoing regarding potential increases in facilities costs.
8 Other Issues
8.1 The Committee requested that the HR and Communications Committee be informed of the FCC’s wish to include further headcount information within the Efficiency reporting section of the management accounts pack.
Jane Ramsey Chair of FCC Richard Alexander Finance Director
7th October 2010
J
Agenda Item 13
Report of the Audit Committee Meeting held on 23rd September
Report to Board of Directors – October 2010
MAIN POINTS FROM AUDIT COMMITTEE MEETING OF 23rd SEPTEMBER Note by the Chair
The committee discussed the latest Internal Audit Reports and were pleased to note that none had received ratings of limited assurance or worse. The subjects included: bullying and harassment (classified as adequate assurance), catering contract management (reasonable assurance) and income budgeting (also reasonable assurance). We noted that further progress had been made in clearing the other overdue significant recommendations. We also noted the new assurance rating introduced by Internal Audit. The key change was to subdivide the middle “adequate” rating into those closer to green (substantial assurance) and those closer to red which call for more urgent action. We previously reported that the committee had reviewed the report on Audit Committee Effectiveness which had concluded that the committee was effective but in its “observations” suggested some improvements. The committee agreed some specific actions it intended to take to improve effectiveness. Tony Mundy attended to discuss IA`s Clinical Audit Draft Report. We welcomed the report which outlined the links between clinical audit and the wider Trust. A number of issues had been identified in the report including how the Board receives assurance that clinical audit is captured and reflected in the assurance framework. It was agreed that greater clarity was required over how the Trust’s audit programme was organised and how compliance and assurance was managed but that this had to be balanced against the importance of encouraging ownership of clinical audit at divisional level. The committee recognised there was no simple solution to this issue. Tony Mundy said it was important that divisions continued to carry out audits of interest to them as well as those required by national organisations; he would initiate discussions with the medical divisions on the recommendations. Mike Foster agreed to discuss with Sandra Hallett how the assurance arrangements might be strengthened. The Board Chairman asked for a short paper for the Board explaining the main processes which provide assurance on quality and safety. On External audit and accounting issues we noted progress with both the monthly and Q1 close and the work plan for Q2 and Q3. The committee was pleased to note that a detailed plan with specific milestones had been produced by PWC to deal with the comments raised in 2009/10; progress on delivery will be reported to the committee following each quarterly review.
Nick Monck Chair of Audit Committee 3rd October 2010
K
Agenda Item 14
Minutes of the Audit Committee Meeting held on 16th August
1
AUDIT COMMITTEE
Minutes of the meeting held on Monday, 16th August 2010 from 12.00pm to 2.00pm in the Chairman’s & CEO meeting room, 250 Euston Road. Present: Sir Nicholas Monck, Non-Executive Director (Chairman)
Sue Atkinson, Non-Executive Director
In Attendance: Janet Dawson, PwC Tim Merritt, RSM Tenon Clive Makombera, RSM Tenon Elizabeth Humphrey, RSM Tenon
Suki Pooni, Parkhill (for point 7) Jenny West, Parkhill (for point 7) John Watts, Director of Procurement (for point 9e)
Tonia Ramsden, Director of Corporate Services Richard Alexander, Finance Director Peter Anthony, Deputy Finance Director Marion Storch, Head of Finance
1. Apologies Apologies were received from Sir John Tooke, Non-Executive Director and Mike Foster, Deputy Chief Executive. 2. a) Minutes of the Meeting held on 3rd June 2010 The minutes were reviewed and Richard Alexander said that the discussion about the treatment of the year end accounting misstatements was in parts not correct and that he would re-word it (second last paragraph under point 7).
b) Minutes of the Meeting held on 22nd July 2010 The minutes of the meeting were reviewed and agreed. 3. Matters Arising The table of the matters arising were noted as having been dealt with, covered within the agenda items of the meeting or where not completed an appropriate update had been provided to the Committee.
2
4. Internal Audit a) Progress Report. The Committee expressed concern about the limited assurance on Mandatory Training noting that this had been reported to the August Board. RSM Tenon commented that although the Sickness Management Audit had been classified as adequate assurance it had found a lack of compliance with correct record keeping. Sue Atkinson commented on the Clinical Audit report that it was difficult to get clinical ownership and that the Trust had to be careful not to lose balance between top and bottom ownership. The Chair asked that the full Clinical Audit report should be available to all Audit Committee members for the September meeting. The Committee requested that the Mandatory Training and Sickness Management Audits and the Education Centre follow up review would be formally referred to the HRC Committee to consider. b) The Committee discussed the further report on Internal Audit recommendations that were still outstanding after 12 months, in particular the relatively high number for Finance and HR. The Committee was pleased that all fundamental recommendations had now been dealt with. It asked for a mechanism which would highlight the Boards which had many significant recommendations outstanding either in absolute terms or as a large proportion of the recommendations made. Richard Alexander proposed to take a summary of outstanding recommendations to EB distinguishing ‘significant’, ‘fundamental’ and ‘merits attention’. The Committee welcomed this. The Committee hoped to complete this review of currently outstanding recommendation at its September meeting. c) Tim Merritt presented the changes to the way Internal Audit would report their opinion and recommendations to the Trust, which was to be introduced for the 2010/11 audit plan. In essence the opinion would be divided into four (previously three) assurance levels and graphically represented from green to red with amber split into two, one tending to red and one to green indicating the assurance to be “above or below the line”. He confirmed that this amounted to dividing the present ‘adequate assurance’ classification to show whether or not action to improve assurance was needed. The Audit Committee noted the change and would review the way it worked. d) In a discussion of the Audit Committee Effectiveness Report, Sue Atkinson said that although the executive summary concluded the Committee was effective in discharging its duties the details of the observations read very differently and more critically; there appeared to be a mismatch between statements in the report and the executive summary. She also found that the volume of paperwork was not an issue as the IA reports clearly separated between summary and detailed information. The Chair asked to note that the Committee papers were in general distributed in good time and expressed appreciation of this. Elizabeth Humphrey from RSM Tenon said that the report only reflected observations: it was for the Trust to review what actions
3
were to be taken if any. She also noted that the perception of one or more people who attended the Committee was that the role of the Chair in relation to the Trust Board was unclear which should be known and considered. The Chair proposed a separate meeting and invited Audit Committee members to comments on the report’s observations. 5. Risk Management and Assurance Framework a) The Committee considered the Q1 2010/11 Risk Assurance and Framework report which had gone to the August Board. It was pleased that the Trust-wide risk to patients from medication errors had moved from red to amber. The Committee noticed that in some respects the Assurance Framework appeared more optimistic than the Risk Report in the performance pack (e.g. financial risk and patient experience). b) The Committee agreed the newly proposed Flash Report on Risk would be useful for circulation when the timetable did not allow it to see the full Board papers. c) The Committee agreed with the proposed response to ‘Taking it on Trust’, a report by the Audit Commission. d) It was confirmed that Clinical Coding was for the Finance and Contracting Committee and not the Audit Committee. 6. External Audit and Accounting Issues The Committee noted the progress reported in the paper from Peter Anthony and that PwC’s work on the close for Q1was about to start. It was agreed that a written paper for dealing with the points which were raised on the 2009/10 accounts would come to the next meeting. Progress in implementing it and in improving successive quarterly closes would be covered in later reports. Richard Alexander welcomed the progress on quarterly close, as there was now increased visibility on assets under construction. The Committee welcomed the progress made to date. 7. Counter Fraud Jenny West (Parkhill) presented the executive summary of the 09/10 Annual Counter Fraud Report. The Committee noted that case redress is acceptably pursued and it welcomed its progress. Richard Alexander said that Counter Fraud’s main objective for the Trust was fraud deterrence and that money was secondary. He confirmed that the improved timetable he had agreed with Parkhill was being kept to.
4
The 2010/11 basic work plan was discussed and Sue Atkinson asked for assurance that the Trust received value for money for the days proposed. The response was that after the Counter Fraud Awareness days not only had the overall referral rate increased but the Trust also started to see referrals from departments, which in the past not had any. Sue Atkinson accepted that soft measures to determine value for money were in place. Tonia Ramsden noted that the Trust had undertaken a policy review to establish the role of Counter Fraud. The Committee agreed that the 2011/12 work plan should be approved earlier in the year and that it should review Counter Fraud once a year at a convenient time. 8. Standing Financial Instructions (SFI) Peter Anthony drew the Committee’s attention to the changes made in certain SFIs, which were transparent in the paper presented and said a few follow-ups had been requested by the Board. The main changes so far reflected the decision to delegate responsibility for smaller waivers on procurement to the Director of Procurement (see item 9e). The Committee agreed that the specific changes made in the SFIs were fine. Some more general points were made about the existing text; for example, the Terms of Reference for Audit Committee and Finance and Contracting Committee should be treated consistently. The Chair asked that the Board should be reminded that a general SO and SFI overhaul is planned. 9. Reports and Papers for Information a) Paying Patients: The Committee reviewed the draft policy for Private Patients and Overseas Visitors and noted that for both the monitoring committee was the Paying Patients Management Board and not the Audit Committee. The Chair said then the key was how a patient was identified as private and without entitlement to free treatment. This should be fully covered in both papers. The Committee considered the Terms of Reference for the Paying Patients Management Board. It was unclear to whom the Board was accountable. The ToR did not make clear that the Paying Patients Board would be responsible for performance management of private patients contracts (the area which had prompted the proposal to set up the new Board). The Committee noted that the Paying Patients Management Board should not only be made up of people who manage the process. The Committee proposed that both policies and ToR for the Paying Patients Management Group should be further consulted before submission to the Policy Compliance Group.
5
b) Write-Off Process: The Committee noted the Finance Director’s view that the Trust’s write-off process was satisfactory, subject to checking that all the present steps were cost effective and agreed with his view. c) Papers from Other Committees on Risk: The Chair suggested that instead of circulating minutes of the QSC, FCC and HRCC each member would comment on the main risks which had been considered by these committees. Tonia Ramsden said that the Trust’s referral procedure between committees would cover some of the risks and not overload on paper or information. It was agreed that the minutes of other Board Committees would be replaced by these procedures. d) Losses and Special Payments: The Committee noted the report. e) Waivers to SOs and SFIs: John Watts presented the level of waivers, which were going down as a result of continuous process improvements. The Committee heard that the responsibility for waivers had passed from Finance to Procurement since the beginning of this financial year to increase commercial awareness throughout the Trust. John Watts said that a more aggressive approach in the negotiation of contract renewals was applied and made possible through the growing partnership between the departments and Procurement. 10. Date of Next Meeting Thursday, 23rd September 2010 – 2pm to 4pm in the CEO/Chairman’s Meeting Room, 250 Euston Road.
L
Agenda Item 15
Entries in the Seal Register
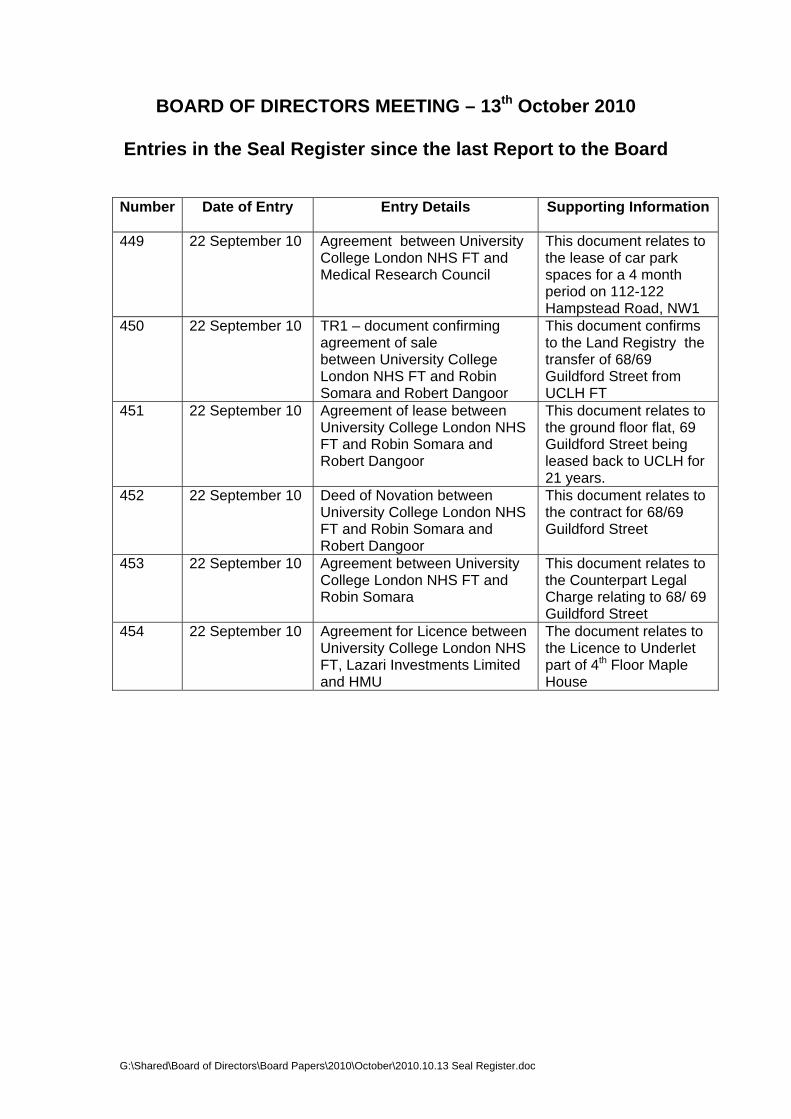
BOARD OF DIRECTORS MEETING – 13th October 2010
Entries in the Seal Register since the last Report to the Board Number Date of Entry Entry Details
Supporting Information
449 22 September 10 Agreement between University College London NHS FT and Medical Research Council
This document relates to the lease of car park spaces for a 4 month period on 112-122 Hampstead Road, NW1
450 22 September 10 TR1 – document confirming agreement of sale between University College London NHS FT and Robin Somara and Robert Dangoor
This document confirms to the Land Registry the transfer of 68/69 Guildford Street from UCLH FT
451 22 September 10 Agreement of lease between University College London NHS FT and Robin Somara and Robert Dangoor
This document relates to the ground floor flat, 69 Guildford Street being leased back to UCLH for 21 years.
452 22 September 10 Deed of Novation between University College London NHS FT and Robin Somara and Robert Dangoor
This document relates to the contract for 68/69 Guildford Street
453 22 September 10 Agreement between University College London NHS FT and Robin Somara
This document relates to the Counterpart Legal Charge relating to 68/ 69 Guildford Street
454 22 September 10 Agreement for Licence between University College London NHS FT, Lazari Investments Limited and HMU
The document relates to the Licence to Underlet part of 4th Floor Maple House
G:\Shared\Board of Directors\Board Papers\2010\October\2010.10.13 Seal Register.doc
M
Agenda Item 16
Schedule of Board Meetings 2011
UNIVERSITY COLLEGE LONDON HOSPITALS NHS FOUNDATION TRUST
SCHEDULE OF BOARD MEETINGS 2011
February 9th
March 9th
May 11th
June 8th *
July 13th
September 14th
October 12th
December 14th
All meetings commence at 2.00 p.m. and will be held in the Education Centre, First Floor West Wing, 250 Euston Road *
* Except June – venue to be confirmed