Embed Size (px)
Citation preview

RESEARCH ARTICLE
BMSCs ameliorate septic coagulopathy by suppressinginflammation in cecal ligation and puncture-induced sepsisShunyao Xu1,2,*, Zhen Zhou2,*, Hao Li1, Ziying Liu1, Xiaojun Pan2, Fen Wang2, Yueyue Huang2, Xiaogang Li3,Yunbei Xiao4, Jingye Pan2,‡, Cong Wang1,3,‡ and Dequan Li5,‡
ABSTRACTSepsis is an aggressive and life-threatening systemic inflammatoryresponse with a high mortality. Inflammation and coagulation playcrucial roles in the pathogenesis of sepsis in a mutually promotingmanner. Unlike other single-target molecular therapies that have noobvious effects on clinical sepsis, bone marrow stromal cell (BMSC)therapy offers a broader spectrum of activities ranging from immuneand inflammation suppression to tissue regeneration. In this report,we demonstrate that BMSC injection attenuates septic coagulopathy.It decreased themortality, mitigated lung injury and reduced the surgeof proinflammatory factors in mice with sepsis induced by cecalligation and puncture (CLP). An in vitro cell model also revealed thatco-culture with BMSCs reduced secretion of proinflammatory factorsand injury of endothelial cells in response to lipopolysaccharide(LPS), an endotoxin of gram-negative bacteria. Together, our resultsdemonstrate that BMSCs suppress sepsis-induced inflammation,endothelial dysfunction and defective coagulation.
KEY WORDS: BMSCs, Sepsis, Coagulopathy, Inflammation, CLP
INTRODUCTIONSepsis is a complex pathological condition that comprises bacterialinfection, inflammation, coagulopathy and innate immunity.Despite advances in management, sepsis still represents majorhealthcare problems worldwide leading to a substantialconsumption of health care resources as a result of its highmorbidity and mortality. In the past decades, many immunemodulatory compounds have been proposed to restore homeostasisin patients with sepsis; however, no single treatment has beenestablished to control sepsis despite extensive efforts. Therefore,there is an urgent need for effective targeted therapies for sepsis(Angus and van der Poll, 2013; Ulloa and Tracey, 2005; Kaukonenet al., 2014).
Inflammation and coagulation play pivotal roles in thepathogenesis of sepsis. Emerging evidence demonstrates theextensive crosstalk between these two pathways. Inflammationinduces coagulation, which, in turn, contributes to secondaryinflammation (Levi et al., 2004; Chu, 2010; Choi et al., 2006;Russell, 2006). The products and stimuli derived from the infectivemicrobe activate inflammatory cells, including macrophages andneutrophils, causing them to release inflammatory cytokines. Thesecytokines then induce a series of sequential results, characterizedby vascular dysfunction, abnormal endothelial permeability,disseminated intravascular coagulation, and tissue and organinjury (London et al., 2010; Rodriguez-Gaspar et al., 2001).Multiple studies have shown that pro-inflammatory cytokines arethe main mediators of inflammation-activated coagulation (Wanget al., 2015; van der Poll et al., 2001). IL-6 initiates the coagulationactivation; tumor necrosis factor-α (TNF-α) and IL-1 are involved inthe regulation of physiological anticoagulation (van der Poll et al.,1994). In addition, the protein C system, protease-activatedreceptors (PARs) and the plasminogen–plasmin system, whichregulate the procoagulant, also modulate the inflammation (Esmon,2002; Coughlin, 2000; Szaba and Smiley, 2002).
Bone marrow stromal cells (BMSCs) are multipotent progenitorcells that have the capacity to self-renew and differentiate intoosteoblasts, chondrocytes, adipocytes, myoblasts and fibroblasts(Chamberlain et al., 2007). It has been reported that BMSC injectionis a promising cell-based therapy in various diseases (Le Blanc andPittenger, 2005; De Miguel et al., 2012; Das et al., 2013). It is alsoknown that transfusion of BMSCs has protective effects in mousemodels of sepsis induced by cecal ligation and puncture (CLP)(Németh et al., 2009; Mei et al., 2010; Islam et al., 2012). However,whether BMSCs affect septic coagulopathy and how BMSCsameliorate septic coagulation remains unclear and deserves to beinvestigated.
RESULTSBMSC injection reduces septic coagulopathy andinflammationTo assess the effect of BMSCs on CLP-induced sepsis, BMSCswere transplanted to C57BL/6 mice 6 h after CLP when mice hadjust recovered from the anesthesia. The micewere then euthanized atthe moribund stages. The time of euthanasia was defined as thesurvival time. Statistical analyses revealed that BMSCs significantlyelongated the survival time compared with those treated with PBS(Fig. 1A). Since bleeding time is an index for coagulation, wemeasured the tail bleeding time 24 h after CLP (Fig. 1B). The resultsshowed that the group with the CLP treatment had a shortenedbleeding time and that the group with BMSC treatment after CLPhad a longer bleeding time compared with the group subjected toCLP alone. The results suggest that the shortened bleeding time inseptic mice was reversed by BMSCs.Received 21 September 2017; Accepted 7 December 2017
1School of Pharmaceutical Sciences, Wenzhou Medical University, Wenzhou,Zhejiang 325000, P.R. China. 2Department of IntensiveCareUnit, The First AffiliatedHospital of Wenzhou Medical University, Wenzhou, Zhejiang 325000, P.R. China.3Ningbo Fourth Hospital, Xiangshan, Zhejiang 315000, P.R. China. 4Department ofUrology, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou,Zhejiang 325000, P.R. China. 5Department of Traumatology Medicine, The FirstAffiliated Hospital of Wenzhou Medical University, Wenzhou, Zhejiang 325000, P.R.China.*These authors contributed equally to this work
‡Authors for correspondence ([email protected]; [email protected];[email protected])
S.X., 0000-0001-7703-3984; Z.Z., 0000-0001-6227-6692; H.L., 0000-0003-2051-4159; Z.L., 0000-0002-2012-5148; X.P., 0000-0003-0556-7607; F.W., 0000-0002-2833-5262; Y.H., 0000-0002-7488-2187; X.L., 0000-0001-8932-0083; Y.X.,0000-0002-9011-7565; J.P., 0000-0002-2367-1275; C.W., 0000-0002-2184-6879;D.L., 0000-0001-7087-7359
1
© 2018. Published by The Company of Biologists Ltd | Journal of Cell Science (2018) 131, jcs211151. doi:10.1242/jcs.211151
Journal
ofCe
llScience

To determine whether the BMSC treatment alleviatedinflammation induced by CLP, ELISA was used to determine theconcentration of key inflammation factors in the plasma. The resultsshowed that the plasma levels of TFPI, TNF-α and IL-1β in the CLPgroup were significantly higher than in the sham-operated controlmice, but not in the mice treated with both CLP and BMSC injection(Fig. 1C–E). The results suggest that BMSCs blunt theinflammation induced by the CLP and protect the septic micefrom the acute coagulopathy and inflammatory response.In sepsis, pathological angiogenesis damages the endothelial
barrier, which increases the secretion of multiple angiogenic factors.To determine whether injection of BMSCs alleviated endothelialdamage, the proteome profiler mouse angiogenesis array wasemployed to measure angiogenic factors in the plasma. The resultsshowed that the CLP group had increased plasma levels of CXCL1,CXCL10, CXCL16, MCP1 (CCL2), MMP3, MMP8 and PTX3(Fig. 1F,G). However, in the group with CLP followed by BMSCtreatment, the plasma levels of these angiogenic factors weresignificantly lower than those in the CLP alone group. The resultsfurther suggest that BMSCs alleviate the damage induced by CLP.
BMSCs attenuate pulmonary inflammatory injury andcoagulopathy in vivoLung inflammation and injury leading to pulmonary dysfunction isone of the common symptoms in septic shock. To determinewhether BMSCs alleviated CLP-induced lung inflammation andinjury in mice, lung sections were subjected to Hematoxylin andEosin staining for histological analyses (Fig. 2A) and neutrophilelastase (NE; also known as ELANE) immunohistochemistrystaining to assess the level of NE+ cells in the lung (Fig. 2B,C).The CLP significantly increased lung inflammation and NE+ cells
in the lung. Compared with the CLP group, the group with CLPfollowed by BMSC injection showed a modest pulmonaryinflammatory response. Consistently, CLP increased the plasmalevel of NE and injection of BMSCs attenuated the increase ofplasma NE induced by CLP (Fig. 2D). Furthermore, fluorescentstaining indicated that Ly6G-labeled neutrophils and tissue factor(TF)-positive coagulation were increased in the CLP group.However, the effect of CLP was reduced by addition of BMSCs(Fig. 2E,F). Quantitative real-time RT-PCR analyses revealed thatexpression of cytokines CXCL1, CXCL10, MCP1, IL-6 and IL-10,as well as inflammation-related proteins TF, MMP1, PAR1 (F2R),toll-like receptor 4 (TLR4) and intercellular cell adhesion molecule1 (ICAM1), at the mRNA level was higher in the CLP group than inthe sham- or BMSC-treated groups (Fig. 2G). Protein expression ofTF, NE and PAR1, which are related to inflammation andcoagulation, was increased after CLP and this increase wasattenuated by BMSCs. Interestingly, the BMSC injection had noobvious effect on other biomarkers, such as antithrombin-III (ATIII)and tissue factor pathway inhibitor (TFPI) (Fig. 2H). Together, thedata suggest that CLP-induced pulmonary inflammation andcoagulopathy can be alleviated by BMSCs.
BMSCs alleviate the damage to HUVECs induced by LPSSepsis increases vascular permeability by disrupting endothelialintegrity, which is one of the major problems induced by sepsis. Todetermine whether BMSCs alleviate HUVEC damage induced bybacterial endotoxin LPS, HUVECs were co-cultured with BMSCsand then treated with LPS. The HRP penetration assay was used todetermine the permeability of HUVECs. As expected, LPStreatment increased the permeability (Fig. 3A). However, theincreased permeability was compromised by co-culture with
Fig. 1. Bone marrow stromal cells reduce septic coagulopathy and inflammation. (A) C57BL/6 mice aged 6 to 7 weeks were subjected to cecal ligation andpuncture (CLP) and injected with sterile PBS (n=12) or BMSCs (1×106/0.3 ml PBS, n=12) via tail vein randomly after 6 h, mice were also prepared as asham-treated control group (n=8). Mice were monitored for survival and the log-rank (Mantel–Cox) test was used. (B) The tail bleeding time was measured 24 hafter CLP (n≥6 per group). Mean±s.e.m. is shown. (C–E) The plasma levels of tissue factor pathway inhibitor (TFPI), tumor necrosis factor-α (TNF-α) andinterleukin (IL)-1β were measured by ELISA 24 h after CLP (n≥5 per group). (F) Plasma analyzed by angiogenesis antibody proteome profiler array.(G) Quantitative analysis of proteins detected in F. *P<0.05.
2
RESEARCH ARTICLE Journal of Cell Science (2018) 131, jcs211151. doi:10.1242/jcs.211151
Journal
ofCe
llScience

BMSCs. Cell counting analyses revealed that HUVEC proliferationwas inhibited by LPS and the inhibition was abolished by BMSCs(Fig. 3B). Furthermore, cell migration assay demonstrated that LPSinhibited HUVEC migration and that BMSCs significantly increasedthe migration activity of HUVECs even under LPS stimulation(Fig. 3C,D), whereas there was no difference between the BMSCgroup and BMSC+LPS group (data not shown). In addition, theendothelial cell tube formation test indicated that HUVECs formedmore tubes under LPS stimulation, which was curbed by co-culturewith BMSCs (Fig. 3E). Secretion of 6-keto prostaglandin F1α (6-k-PGE1α) is a normal function of HUVEC cells. Treating HUVECswith LPS reduced the secretion of 6-k-PGF1α. The inhibition wasabrogated by co-culture with BMSCs (Fig. 3F). Secretion of TXB2 isincreased when the integrity of endothelial cells is disrupted.Similarly, treating HUVECs with LPS increased secretion ofTXB2. Co-culture with BMSCs reduced TXB2 secretion inducedby LPS (Fig. 3G). Together, the data demonstrate that BMSCs protectLPS-induced damage of HUVECs.To explore whether BMSCs affect activation of the endothelium
coagulation cascade, we detected TF, NFκB-p65 (NFKB3) andJNK expression at the protein level. Results shown in Fig. 3Hindicated that BMSC co-culture led to a down-regulation of TF, p65and p-JNK expression in HUVECs.
BMSCs inhibit LPS-induced secretion of pro-inflammatoryfactors by macrophagesSince macrophages promoted inflammation in sepsis, we theninvestigated whether BMSCs affected the ability of primaryperitoneal macrophages to secrete pro-inflammatory factors. The
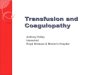
peritoneal macrophages were treated with LPS for 6 h. Total RNAwas extracted for quantitative real-time RT-PCR analyses of pro-inflammatory factor expression at the mRNA level. The resultsshowed that treatment with LPS increased gene expression ofCXCL1, CXCL10, CXCL16, MCP1, IL-1β, IL-6, IL-10 and TNF-α, as well as adhesion molecules (ICAM1 and VCAM1) andcoagulation-related biomarkers (TF, MMP1 and PAR1). However,the increased expression was reduced by co-culture with BMSCs(Fig. 4A). Immunostaining showed that expression of PAR1 and TFwas increased when the macrophages were treated with LPS. Co-culture with BMSCs diminished this increase (Fig. 4B). Proteinexpression of TF, JAK2 and p-Stat3 was enhanced by LPS, but notin the BMSC co-culture group (Fig. 4C). The results suggested thatBMSCs also attenuate the inflammatory reaction in macrophages.
DISCUSSIONCoagulation dysfunction is one of the most notable symptoms ofsepsis, which is a cascade of complex processes closely related toinflammation (Levi et al., 2004). Since stromal cells, especiallyBMSCs, have anti-inflammatory and immune modulation effects,infusion of stromal cells, especially BMSCs, is emerging as aprominent therapy for a range of diseases and pathologies (Le Blancand Pittenger, 2005; De Miguel et al., 2012; Das et al., 2013).Herein, we reported that BMSCs alleviate the surge of plasma levelsof pro-inflammation TNF-α and IL-1β after CLP. In addition, CLP-induced lung injury and overexpression of chemokines andcytokines CXCL1, CXCL10, MCP1, IL-6, IL-10 and ICAM1 inthe lung were attenuated by the BMSC treatment. Moreover, co-culturewith BMSCs restricted the ability of macrophages to respond
Fig. 2. Bone marrow stromal cells attenuate pulmonary inflammatory injury and coagulopathy in vivo. (A) Lung tissue sections were stained withHematoxylin and Eosin 24 h after surgery for histological examination. (B,C) Neutrophil elastase (NE) immunohistochemistry staining in lung tissues with thequantification of positive cells. The sections are all shown at ×400 magnification. (D) Plasma NE level measured by ELISA 24 h after CLP. (E,F) Lymphocyteantigen 6 complex locus G (Ly6G) (green) and tissue factor (TF) (green) staining of lung sections detected by confocal microscope. Nuclei are stained with DAPI(blue). e1,f1, sham; e2,f2, CLP; e3,f3, CLP+BMSCs. (G) Relative lung gene expression of inflammatory factors and coagulation biomarkers measured byquantitative real-time RT-PCR (n≥5 per group). Data are represented as mean±s.e.m. and compared using one-way ANOVA. (H) Western blotting ofantithrombin-III (ATIII), TFPI, TF, NE, Janus kinase 2 (JAK2), protease-activated receptors (PAR1) and β-actin from lung lysates of each group (n≥5). *P<0.05.
3
RESEARCH ARTICLE Journal of Cell Science (2018) 131, jcs211151. doi:10.1242/jcs.211151
Journal
ofCe
llScience

to LPS with respect to overexpression of inflammatory factorsCXCL1, CXCL10, CXCL16, MCP1, IL-1β, IL-6, IL-10, TNF-α,ICAM1 and VCAM1. Since uncontrolled inflammation activatesplatelets, induces endothelial disorder, disseminates intravascularcoagulation, and leads to tissue damage and organ failure (Fig. 5),the data demonstrate that BMSCs have the potential for treatingCLP-induced sepsis.The vascular dysfunction and coagulation imbalance are
symptoms of sepsis pathogenesis (Lee and Slutsky, 2010). It hasbeen reported that BMSCs protect endothelial cells frominflammation attack (Rahbarghazi et al., 2013; dos Santos et al.,2012). We previously also reported that BMSCs ameliorate sepsis-induced damage by regulating expression of thrombomodulin (TM)and endothelial protein C receptor (EPCR) (Tan et al., 2016). Thedata in this report further demonstrate the protective effect ofBMSCs against septic coagulopathy. Angiogenesis is an intricateand well balanced process (Kim et al., 2013). Our results showingthat BMSC treatment reduced septic angiogenesis both in vivo andin vitro suggest that the damage of the endothelium in sepsis isreduced by BMSCs. This is further supported by the in vitro datashowing that LPS-induced damage in migration, proliferation andpermeability of endothelial cells was alleviated by co-culture withBMSCs.TF is an inflammation-activated membrane receptor that initiates
the coagulation pathway and promotes angiogenesis (Mackman,2004). PARs (PAR1–PAR4) belong to a family of transmembraneG-protein-coupled receptors (Zhao et al., 2014). PAR1 is a thrombinreceptor and serves as a receptor for TF factor VIIa complex andfactor Xa (Pawlinski, et al., 2004; Reinhardt et al., 2014), and it alsoparticipates in mediating activated protein C signaling in endothelialcells (Mosnier and Griffin, 2003). Emerging evidence suggests thatMMP1 plays a pivotal role in inflammation and coagulation byactivating PAR1 in sepsis (Tressel et al., 2011). Our results showed
that expression of TF, MMP1 and PAR1 was regulated by BMSCsboth in vivo and in vitro. This further demonstrates that BMSCsalleviate inflammation and coagulation induced by CLP.
Neutrophils actively participate in sepsis pathogenesis and theneutrophil extracellular traps promote thrombin generation (Gouldet al., 2014; Caudrillier et al., 2012; Sreeramkumar et al., 2014;Kolaczkowska and Kubes, 2013). Moreover, the NE level has beenshown to be a risk factor for the severity of sepsis (Mihara et al.,2013). Our results showing that BMSCs cleared the pulmonaryneutrophil infiltration as well as causing a reduction in the boost inplasma NE levels and lung NE expression induced by CLP furtherdemonstrated that BMSCsmodulate neutrophil recruitment in septicmice.
Taken together, we show both in vivo and in vitro that BMSCseffectively ameliorate septic coagulopathy, alleviate vascular damage,reduce inflammation, attenuate acute lung injury and improve thesurvival rate. Our study demonstrates that coagulation protection byBMSC injection is a promising therapy for treating sepsis.
MATERIALS AND METHODSExperimental animalsMale C57BL/6 mice (6 to 7 weeks old) were obtained from Shanghai SLACLaboratory Animal Limited Liability Company (Shanghai, China). Theanimals were maintained in a pathogen-free facility with ambienttemperature of 23±3°C, relative humidity of 55±10%, and 12 h light:12 hdark cycle. All animal procedures were approved by the Institutional AnimalCare and Use Committee of the Wenzhou Medical University.
Cecal ligation and puncture (CLP)The CLP mouse model was prepared as described (Dejager et al., 2011). Asham group was operated similarly without ligation and puncture.Subsequently, the mice were subcutaneously injected with 1 ml pre-warmed saline. After 6 h, the mice were injected with sterile PBS or BMSCs(1×106/0.3 ml PBS) via tail vein. For the survival experiments, the mice
Fig. 3. Bonemarrow stromal cells alleviate the damage to HUVECs induced by LPS. (A) BMSCs were co-cultured with HUVECs in Transwell plates (0.4 μm)and the permeability of HUVECs was measured 6 h after lipopolysaccharide (LPS, 1 μg/ml) stimulation by detecting the HRP leak rate. (B) Cell countingkit-8 (CCK-8) assay was used to detect the proliferation of HUVECs stimulated by LPS (1 μg/ml) and BMSC co-culture after 6 h. (C) BMSCs were co-culturedwith HUVECs in Transwell plates (5 μm) and the HUVECs migrating through the membrane were stained with Crystal Violet. (D) Quantification of migrationnumber of HUVECs in C. (E) HUVECs were seeded in Transwell plates (0.4 μm) covered with Matrigel and observed 3.5 h after LPS stimulation. (F,G) HUVECsupernatant co-culturedwith BMSCs in Transwell plates (0.4 μm)weremeasured using 6-k-PGF1α and TXB2ELISA kits, respectively. (H) The p-p65, p65, p-JNKand TF protein expression levels in HUVECs were determined by western blotting. Data are represented as mean±s.e.m. *P<0.05.
4
RESEARCH ARTICLE Journal of Cell Science (2018) 131, jcs211151. doi:10.1242/jcs.211151
Journal
ofCe
llScience

were closely observed every 12 h for 4 days and euthanized at the moribundstage. For other experiments, the mice were sacrificed 24 h after the CLP.
Tail bleeding time assayBleeding assay was performed in mice 24 h after surgery by tail tipamputation, and then the tail was immersed in saline at 37 °C. The bleedingtime was recorded (Ye et al., 2014).
ELISA analysesThe levels of 6-k-PGF1α and thromboxane B2 (TXB2) in the supernatantwere examined using ELISA kits (eBioscience, San Diego, CA) followingthe manufacturer’s instructions. IL-1β, TNF-α, NE and TFPI levels in themice plasma were measured by specific ELISA kits (R&D Systems).
Angiogenesis analysisPlasma collected from three groups of mice were probed with the MouseAngiogenesis Antibody Proteome Profiler Array (R&D Systems) accordingto the manufacturer’s instructions. For in vitro study, HUVECs (15×104/well) were seeded in the lower chamber of 24-well Transwell plates (poresize of 0.4 μm; Corning) which were covered with 120 μl polymerizedMatrigel (BD Biosciences) and the same number of BMSCs were seeded inthe upper chamber. Samples without BMSCs in the upper Transwell wereused as a control. After LPS (1 μg/ml) treatment for 3.5 h, images werecaptured with an Olympus CKX41 light microscope.
Cell cultureHUVECs were purchased from Chi Scientific (Jiangsu, China) and culturedin RPMI 1640medium (Gibco, Life Technologies, Germany) supplementedwith 10% fetal bovine serum (FBS) (Sigma-Aldrich) and 1% penicillin/streptomycin (Solarbio, Beijing, China) at 37°C in a 5% CO2 humidifiedchamber. BMSCs derived from C57BL/6 mice were obtained from CyagenBiosciences (Guangzhou, China) and cultured in the specializedmediumwith10% FBS according to the manufacturer’s instructions as described (Tanet al., 2016). Peritoneal macrophages were isolated from 6- to 7-week-oldC57BL/6 mice. Briefly, mice were injected peritoneally with 2–3 ml Starchbroth (Sigma), and then the peritoneal cavity was washed with RPMI 1640medium several times to isolate peritoneal exudate cells. The cells werecultured for 2 h and the adhered cells were harvested for experiments. Nobacterial were observed under a microscope. No mycoplasma were detectedwith the mycoplasma detection kit.
Co-culture experimentsFor Transwell co-culture, HUVECs (5×105/well) or peritoneal macrophages(5×105/well) were seeded to the lower chamber and an equal number ofBMSCs to the upper chamber of 6-well Transwell plates (pore size of 0.4 μm;Corning). HUVECs (5×105/well) or peritoneal macrophages (5×105/well)seeded in 6-well plates without BMSCs were used as a control. Afterovernight incubation, 1 μg/ml LPS (from Escherichia coli O111:B4, Sigma)was added to the LPS and LPS+BMSCs groups, with PBS (HyClone) as the
Fig. 4. Bone marrow stromal cells inhibit LPS-induced secretion of pro-inflammatory factors by macrophages. (A) The peritoneal macrophages co-cultured with BMSCs were stimulated with LPS for 6 h. CXCL1, CXCL10, CXCL16, IL-1β, IL-6, IL-10, TNF-α, TF, MMP1, PAR1, ICAM1 and VCAM1 mRNAexpression levels in peritoneal macrophages were determined by quantitative real-time RT-PCR. (B) PAR1 and TF expression levels in peritoneal macrophagesin the co-culture system were measured by immunofluorescence staining. (C) TF, PAR1, JAK2 and p-Stat3 protein levels in peritoneal macrophages weredetermined by western blotting. Data are represented as mean±s.e.m. and compared using Student’s t-test and one-way ANOVA. *P<0.05.
5
RESEARCH ARTICLE Journal of Cell Science (2018) 131, jcs211151. doi:10.1242/jcs.211151
Journal
ofCe
llScience

solvent control. After a 6 h incubation, HUVECs or peritoneal macrophageswere collected for subsequent analyses.
HUVEC permeability assayHUVECs (5×104/well) were seeded in the upper chamber and BMSCs in thebottom of a 24-well Transwell plate (pore size of 0.4 μm; Corning). After thecells were confluent, LPS (1 μg/ml) was added to the apical medium for 6 hfollowed by replacement with 200 μl HRP solution (50 ng/ml). The mediumof the lower chamber was collected for penetrating HRP detection afterincubation for 1 h. Briefly, 20 μl medium was transferred to a 96-well platefollowed by addition of 150 μl substrate (400 μg/ml O-phenylenediamine in0.05 M citric acid and 0.1 M phosphate with 0.012% hydrogen peroxide).After incubation at 37°C for 10 min, the reaction was terminated by adding50 μl of 2 M sulfuric acid. The OD value was measured using a microplatereader (Molecular Devices, Hercules, CA).
Cell countingCell Counting Kit-8 (CCK-8) assay (Dojindo, Japan) was used to determinethe viability of cells. BMSCs or HUVECs were seeded in a 96-well plate at2000 cells per well. After 24 h, the supernatant of BMSCs was transformedinto HUVECs plates as BMSC-treated group, LPS (1 μg/ml) was added to themedium for 6 h. Then, the supernatant was replacedwith freshmedium in eachwell and CCK-8 solution (20 µl) was added for incubation for 1 h at 37°C.OD450 values were measured using a microplate reader (Molecular Devices).
HUVEC migration assayBMSCs (2×105/well) suspended with 0.5 ml medium were seeded in thelower chamber of 24-well Transwell plates (pore size of 5 μm; Corning),which had the same number of HUVECs suspended with 0.2 ml medium inthe upper chamber. Samples with no BMSCs in the lower chambers wereused as a control. After overnight incubation, LPS (1 μg/ml) was added tothe medium followed by incubation for 6 h. The non-migrating cells werewiped away with a cotton swab. The membranes were fixed with 4%paraformaldehyde for 20 min, stained with 0.1% Crystal Violet (Solarbio,
Beijing, China) for 30 min, and washed three times with PBS. Cells werecounted under a light microscope (Nikon, Tokyo, Japan).
Western blottingLung, HUVECs and peritoneal macrophages were homogenized and lysedin the RIPA buffer (Thermo Scientific) containing 1% PMSF and 1%protein phosphatase inhibitor mixture (P1260, Applygen, Beijing, China).The protein concentrations were determined using the BCA kit (ThermoScientific). Lysates containing 40 μg proteins were separated on 8–12%SDS-PAGE gels and transferred to polyvinylidene difluoride (PVDF)membranes (EDMMillipore, Billerica, MA). The membranes were blockedwith 5% non-fat milk in TBST (1×TBS, 0.1% Tween 20) for 1 h at roomtemperature. The membranes were then incubated with the followingprimary antibodies overnight at 4°C. After washing with TBST three times,the membrane were then incubated with goat anti-rabbit HRP-conjugatedpolyclonal antibody (1:10,000; Bio-Rad, Cat# 170-6515) for 1 h at roomtemperature. The primary antibodies were: rabbit anti-NE (1:200; Abcam,Cat# ab68672), anti-TF (1:100; Abcam, Cat# ab151748), anti-ATIII (1:500;Santa Cruz, Cat# sc-271987) and anti-TFPI (1:200; Santa Cruz, Cat#sc-365920), and rabbit anti-phospho-cJun N-terminal kinase (p-JNK)(1:1000; Cat# 4668), anti-β-actin (1:2000; Cat# 4970), anti-Janus kinase 2(JAK2) (1:1000; Cat# 3230), phospho-signal transducer and activator oftranscription (p-Stat3) (1:1000; Cat# 9145), p65 (1:1000; Cat# 8242) andphospho-p65 (p-p65) (1:1000; Cat# 3033) NF-κB antibodies, all from CellSignaling Technology. The ECL Plus Chemiluminescent Reagent (ThermoScientific) was used to visualize the proteins. The specific bands werequantitated by ImageJ (NIH, USA).
Quantitative real-time RT-PCRThe Trizol reagent (Invitrogen, CA) was used to extract total RNA from thelung and peritoneal macrophages. The GoScript Reverse TranscriptionSystem kit (Promega) was used for first-strand cDNA synthesis according tothe manufacturer’s protocols. The LightCycler (Roche Diagnostics,Mannheim, Germany) and SYBR Green (Roche Diagnostics, Mannheim,
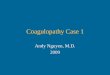
Fig. 5. Bonemarrow stromal cellsmitigate damages induced bysepsis.BMSCsmitigate sepsis-induced damage via the followingmechanisms: (1) inhibitingthe activation of toll-like receptor (TLR) 4 and TLR 2 by bacterial toxin in the monocytes, leading to compromised NF-κB activation; (2) suppressing invasion ofneutrophil to tissues; (3) reducing injury of endothelial cells and production of thrombin and thus alleviating the coagulation; and (4) suppressing macrophageproduction of tissue factors and thus abnormal angiogenesis.
6
RESEARCH ARTICLE Journal of Cell Science (2018) 131, jcs211151. doi:10.1242/jcs.211151
Journal
ofCe
llScience

Germany) were applied to detect gene expression with the primer sequenceslisted in Table S1.
Histology analysesLung tissues were fixed in 4% paraformaldehyde, dehydrated, embeddedand sectioned at 4 μm thickness for H&E staining. For histochemicalstaining, the lung sections were dewaxed, rehydrated and antigen retrievedby autoclave in citrate buffer (0.01 M, pH 6.0) for 10 min. The endogenousperoxidase was quenched by incubation with 3% hydrogen peroxide for30 min. The sections were blocked with preimmune goat serum for 30 minand incubated with rabbit anti-NE antibody (1:200; Abcam, Cat# ab68672)overnight at 4°C. After washing with PBS, the sections were incubated withhorseradish peroxidase (HRP)-conjugated goat anti-rabbit antibody(Zhongshan Golden Bridge Biotechnology, Beijing, China) for 30 min atroom temperature. Thereafter, the slides were stained with a DAB kit(Sigma) and visualized under a microscope (Nikon, Tokyo, Japan). Theintensity and localization of the positive staining was assessed by the IPP 6.0True Color Image Analysis System. Three random areas were selected fromeach section for measurement.
For tissue immunofluorescence staining, the pre-treated lung sectionswere blocked with 5% BSA in PBS-T (PBS with 0.1% Tween 20) andincubated overnight at 4°C with the primary antibodies against Ly6G(1:100, Santa Cruz, Cat# sc-53515) and TF (1:100; Abcam, Cat#ab151748). The sections were then incubated for 1 h at room temperature(RT) with FITC (1:200; Abcam, Cat# ab6717) and nuclei were stained withDAPI (1:200; Cell Signaling Technology, Cat# 4083) for 5 min.
For cell immunofluorescence staining, macrophages were fixed with 4%paraformaldehyde at room temperature for 20 min, and then washed threetimes with PBS, permeabilized with 0.2% Triton X-100 for 15 min, blockedwith 5% BSA at RT for 30 min, and incubated with primary antibodiesagainst PAR1 (1:100, Santa Cruz, Cat# sc-5605) and TF overnight at 4°C.The slides were incubated with FITC for 1 h and then DAPI was added for5 min. Images were taken with a laser scanning confocal microscope(LSCM, Leica) in three random areas.
Statistical analysesKaplan–Meier survival was analyzed using the log-rank test by SPSSsoftware version 20.0 (SPSS). Categorized variables were compared by one-way Analysis of Variance (ANOVA) or Student’s t-test. P<0.05 wasconsidered statistically significant.
Competing interestsThe authors declare no competing or financial interests.
Author contributionsConceptualization: J.P., C.W.; Methodology: S.X., Z.Z., H.L., Z.L., X.P., F.W., Y.H.,D.L.; Software: S.X., Z.Z., Z.L., X.L.; Validation: S.X., H.L., Z.L., X.P.; Formalanalysis: S.X., Z.Z., F.W.; Investigation: C.W.; Resources: H.L., C.W.; Data curation:Z.Z.; Writing - original draft: S.X.; Writing - review & editing: Y.X., C.W.; Projectadministration: J.P., C.W., D.L.; Funding acquisition: J.P., C.W., D.L.
FundingThis work was supported by the Natural Science Foundation of Zhejiang Province ofChina (LY16H140004 and LY17H130003), the National Natural Science Foundationof China (31371470, 8167081437, 81602246, 81671968), the Natural ScienceFoundation of Ningbo City (2015A610198, 2015KYB359), the Talent projectfoundation of Wenzhou Medical University (QTJ14030), the Medical InnovationDiscipline of Zhejiang Province (Critical Care Medicine, Y2015) and the project ofWenzhou Science and Technology Bureau (2014Y0056).
Supplementary informationSupplementary information available online athttp://jcs.biologists.org/lookup/doi/10.1242/jcs.211151.supplemental
ReferencesAngus, D. C. and van der Poll, T. (2013). Severe sepsis and septic shock.N. Engl. J. Med. 369, 2063.
Caudrillier, A., Kessenbrock, K., Gilliss, B. M., Nguyen, J. X., Marques, M. B.,Monestier, M., Toy, P., Werb, Z. and Looney, M. R. (2012). Platelets induceneutrophil extracellular traps in transfusion-related acute lung injury. J. Clin.Invest. 122, 2661-2671.
Chamberlain, G., Fox, J., Ashton, B. and Middleton, J. (2007). Concise review:mesenchymal stem cells: their phenotype, differentiation capacity, immunologicalfeatures, and potential for homing. Stem Cells 25, 2739-2749.
Choi, G., Schultz, M. J., Levi, M. and van der Poll, T. (2006). The relationshipbetween inflammation and the coagulation system.SwissMed.Wkly. 136, 139-144.
Chu, A. J. (2010). Blood coagulation as an intrinsic pathway for proinflammation: amini review. Inflamm. Allergy Drug Targets 9, 32-44.
Coughlin, S. R. (2000). Thrombin signalling and protease-activated receptors.Nature 407, 258-264.
Das, M., Sundell, I. B. and Koka, P. S. (2013). Adult mesenchymal stem cells andtheir potency in the cell-based therapy. J. Stem Cells 8, 1-16.
De Miguel, M. P., Fuentes-Julian, S., Blazquez-Martinez, A., Pascual, C. Y.,Aller, M. A., Arias, J. and Arnalich-Montiel, F. (2012). Immunosuppressiveproperties of mesenchymal stem cells: advances and applications. Curr. Mol.Med. 12, 574-591.
Dejager, L., Pinheiro, I., Dejonckheere, E. and Libert, C. (2011). Cecal ligationand puncture: the gold standardmodel for polymicrobial sepsis? TrendsMicrobiol.19, 198-208.
dos Santos, C. C., Murthy, S., Hu, P., Shan, Y., Haitsma, J. J., Mei, S. H. J.,Stewart, D. J. and Liles, W. C. (2012). Network analysis of transcriptionalresponses induced by mesenchymal stem cell treatment of experimental sepsis.Am. J. Pathol. 181, 1681-1692.
Esmon, C. T. (2002). New mechanisms for vascular control of inflammationmediated by natural anticoagulant proteins. J. Exp. Med. 196, 561-564.
Gould, T. J., Vu, T. T., Swystun, L. L., Dwivedi, D. J., Mai, S. H. C., Weitz, J. I. andLiaw, P. C. (2014). Neutrophil extracellular traps promote thrombin generationthrough platelet-dependent and platelet-independent mechanisms. Arterioscler.Thromb. Vasc. Biol. 34, 1977-1984.
Islam, M. N., Das, S. R., Emin, M. T., Wei, M., Sun, L., Westphalen, K., Rowlands,D. J., Quadri, S. K., Bhattacharya, S. and Bhattacharya, J. (2012).Mitochondrial transfer from bone-marrow-derived stromal cells to pulmonaryalveoli protects against acute lung injury. Nat. Med. 18, 759-765.
Kaukonen, K.-M., Bailey, M., Suzuki, S., Pilcher, D. and Bellomo, R. (2014).Mortality related to severe sepsis and septic shock among critically ill patients inAustralia and New Zealand, 2000-2012. JAMA 311, 1308-1316.
Kim, Y.-W., West, X. Z. and Byzova, T. V. (2013). Inflammation and oxidative stressin angiogenesis and vascular disease. J. Mol. Med. 91, 323-328.
Kolaczkowska, E. and Kubes, P. (2013). Neutrophil recruitment and function inhealth and inflammation. Nat. Rev. Immunol. 13, 159-175.
Le Blanc, K. and Pittenger, M. (2005). Mesenchymal stem cells: progress towardpromise. Cytotherapy 7, 36-45.
Lee, W. L. and Slutsky, A. S. (2010). Sepsis and endothelial permeability.N. Engl. J. Med. 363, 689-691.
Levi, M., van der Poll, T. and Buller, H. R. (2004). Bidirectional relation betweeninflammation and coagulation. Circulation 109, 2698-2704.
London, N. R., Zhu, W., Bozza, F. A., Smith, M. C., Greif, D. M., Sorensen, L. K.,Chen, L., Kaminoh, Y., Chan, A. C., Passi, S. F. et al. (2010). Targeting Robo4-dependent Slit signaling to survive the cytokine storm in sepsis and influenza.Sci.Transl. Med. 2, 23ra19.
Mackman, N. (2004). Role of tissue factor in hemostasis, thrombosis, and vasculardevelopment. Arterioscler. Thromb. Vasc. Biol. 24, 1015-1022.
Mei, S. H. J., Haitsma, J. J., dos Santos, C. C., Deng, Y., Lai, P. F. H., Slutsky,A. S., Liles, W. C. and Stewart, D. J. (2010). Mesenchymal stem cells reduceinflammation while enhancing bacterial clearance and improving survival insepsis. Am. J. Respir. Crit. Care. Med. 182, 1047-1057.
Mihara, K., Ramachandran, R., Renaux, B., Saifeddine, M. and Hollenberg, M. D.(2013). Neutrophil elastase and proteinase-3 trigger G protein-biased signalingthrough proteinase-activated receptor-1 (PAR1). J. Biol. Chem. 288, 32979-32990.
Mosnier, L. O. and Griffin, J. H. (2003). Inhibition of staurosporine-inducedapoptosis of endothelial cells by activated protein C requires protease-activatedreceptor-1 and endothelial cell protein C receptor. Biochem. J. 373, 65-70.
Nemeth, K., Leelahavanichkul, A., Yuen, P. S., Mayer, B., Parmelee, A., Doi, K.,Robey, P. G., Leelahavanichkul, K., Koller, B. H., Brown, J. M. et al. (2009).Bone marrow stromal cells attenuate sepsis via prostaglandin E(2)-dependentreprogramming of host macrophages to increase their interleukin-10 production.Nat. Med. 15, 42-49.
Pawlinski, R., Pedersen, B., Schabbauer, G., Tencati, M., Holscher, T., Boisvert,W., Andrade-Gordon, P., Frank, R. D. and Mackman, N. (2004). Role of tissuefactor and protease-activated receptors in a mouse model of endotoxemia. Blood103, 1342-1347.
Rahbarghazi, R., Nassiri, S. M., Khazraiinia, P., Kajbafzadeh, A.-M., Ahmadi,S. H., Mohammadi, E., Molazem, M. and Zamani-Ahmadmahmudi, M. (2013).Juxtacrine and paracrine interactions of rat marrow-derived mesenchymal stemcells, muscle-derived satellite cells, and neonatal cardiomyocytes with endothelialcells in angiogenesis dynamics. Stem Cells Dev. 22, 855-865.
Reinhardt, C., Bergentall, M., Greiner, T. U., Schaffner, F., Ostergren-Lunden,G., Petersen, L. C., Ruf, W. and Backhed, F. (2012). Tissue factor and PAR1promotemicrobiota-induced intestinal vascular remodelling.Nature 483, 627-631.
Rodriguez-Gaspar, M., Santolaria, F., Jarque-Lopez, A., Gonzalez-Reimers,E., Milena, A., de la Vega, M.-J., Rodrguez-Rodrguez, E. and
7
RESEARCH ARTICLE Journal of Cell Science (2018) 131, jcs211151. doi:10.1242/jcs.211151
Journal
ofCe
llScience

Gomez-Sirvent, J.-L. (2001). Prognostic value of cytokines in SIRS generalmedical patients. Cytokine 15, 232-236.
Russell, J. A. (2006). Management of sepsis. N. Engl. J. Med. 355, 1699-1713.Sreeramkumar, V., Adrover, J. M., Ballesteros, I., Cuartero, M. I., Rossaint, J.,Bilbao, I., Nacher, M., Pitaval, C., Radovanovic, I., Fukui, Y. et al. (2014).Neutrophils scan for activated platelets to initiate inflammation. Science 346,1234-1238.
Szaba, F. M. and Smiley, S. T. (2002). Roles for thrombin and fibrin(ogen) incytokine/chemokine production and macrophage adhesion in vivo. Blood 99,1053-1059.
Tan, L., Huang, Y., Pan, X., Quan, S., Xu, S., Li, D., Song, L., Zhang, X., Chen, W.and Pan, J. (2016). Administration of bone marrow stromal cells in sepsisattenuates sepsis-related coagulopathy. Ann. Med. 48, 235-245.
Tressel, S. L., Kaneider, N. C., Kasuda, S., Foley, C., Koukos, G., Austin, K.,Agarwal, A., Covic, L., Opal, S. M. and Kuliopulos, A. (2011). A matrixmetalloprotease-PAR1 system regulates vascular integrity, systemic inflammationand death in sepsis. EMBO Mol. Med. 3, 370-384.
Ulloa, L. and Tracey, K. J. (2005). The “cytokine profile”: a code for sepsis. TrendsMol. Med. 11, 56-63.
van der Poll , T., Levi, M., Hack, C. E., Ten Cate, H., Van Deventer, S. J.,Eerenberg, A. J., de Groot, E. R., Jansen, J., Gallati, H., Buller, H. R. et al.(1994). Elimination of interleukin 6 attenuates coagulation activation inexperimental endotoxemia in chimpanzees. J. Exp. Med. 179, 1253-1259.
van der Poll, T., De Jonge, E. and Levi, M. (2001). Regulatory role of cytokinesin disseminated intravascular coagulation. Semin. Thromb. Hemost. 27,639-651.
Wang, Y., Braun, O. O., Zhang, S., Norstrom, E. and Thorlacius, H. (2015).Monocytes regulate systemic coagulation and inflammation in abdominal sepsis.Am. J. Physiol. Heart Circ. Physiol. 308, H540-H547.
Ye, S., Huang, Y., Joshi, S., Zhang, J., Yang, F., Zhang, G., Smyth, S. S., Li, Z.,Takai, Y. and Whiteheart, S. W. (2014). Platelet secretion and hemostasisrequire syntaxin-binding protein STXBP5. J. Clin. Invest. 124, 4517-4528.
Zhao, P., Metcalf, M. and Bunnett, N. W. (2014). Biased signaling of protease-activated receptors. Front. Endocrinol. (Lausanne) 5, 67.
8
RESEARCH ARTICLE Journal of Cell Science (2018) 131, jcs211151. doi:10.1242/jcs.211151
Journal
ofCe
llScience