Embed Size (px)
Citation preview
Second-Generation HIV-1 Maturation Inhibitor BMS-955176: Antiviral Activity and Safety with
Atazanavir ± Ritonavir
Carey Hwang,1 Dirk Schürmann,2 Christian Sobotha,2 Marta Boffito,3
Heather Sevinsky,1 Neelanjana Ray,1 Palanikumar Ravindran,1 Hong Xiao,1 Mark Krystal,4 Ira Dicker,4 Dennis Grasela,1 and Max Lataillade,4
on behalf of the BMS HIV Global Development Team
1Bristol-Myers Squibb, Research and Development, Princeton, NJ, USA2Charité Research Organisation GmbH, Charitéplatz 1, 10117 Berlin, Germany
3St. Stephen’s Centre, Chelsea and Westminster Hospital, London, UK4Bristol-Myers Squibb, Research and Development, Wallingford, CT, USA
Disclosures
• Carey Hwang, MD, PhD • Medical Director, Discovery Medicine – Virology • Employee and shareholder of Bristol-Myers Squibb
• This study was funded by Bristol-Myers Squibb

Need for Novel Antiretrovirals
• HIV/AIDS remains a global health issue despite the success of combination antiretroviral therapy (cART)1
• Life-long management of HIV-1 infection requires sequential cART, preferably with simple and convenient regimens containing a minimum of three fully active agents2
• Antiretroviral treatment options, particularly for treatment-experienced patients, may be limited due to:• treatment-emergent or transmitted resistance2,3
• adverse events, drug-drug interactions (DDIs), and regimen complexity2,3
• There is a need for novel antiretrovirals that could potentially change HIV treatment paradigms, and serve as part of a booster- and/or nucleot(s)ide-sparing strategy • Such regimens would benefit from components with novel modes of action,
unique resistance profiles and good long-term tolerability, with manageable DDIs
1. Barré-Sinoussi et al. Nat Rev Microbiol 2013; 11:877–883; 2. DHHS Panel on Antiretroviral Guidelines for Adults and Adolescents. 2015. Available at: aidsinfo.nih.gov/contentfiles/adultandadolescentgl.pdf (accessed Feb 2015); 3. Wittcop L et al. Lancet Infect Dis 2011; 11:363–371.
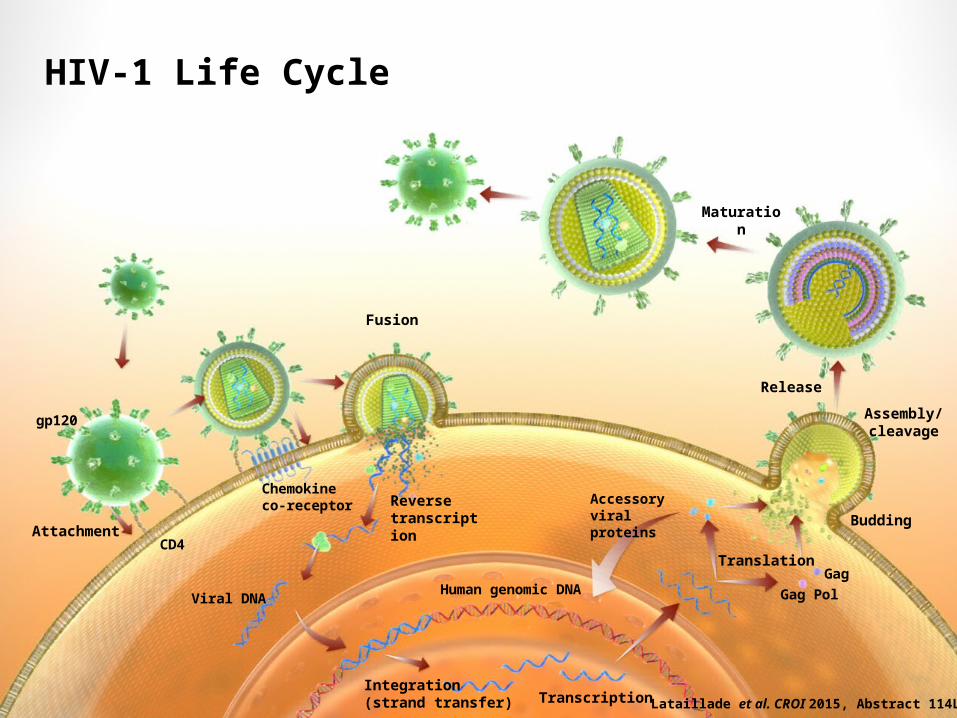
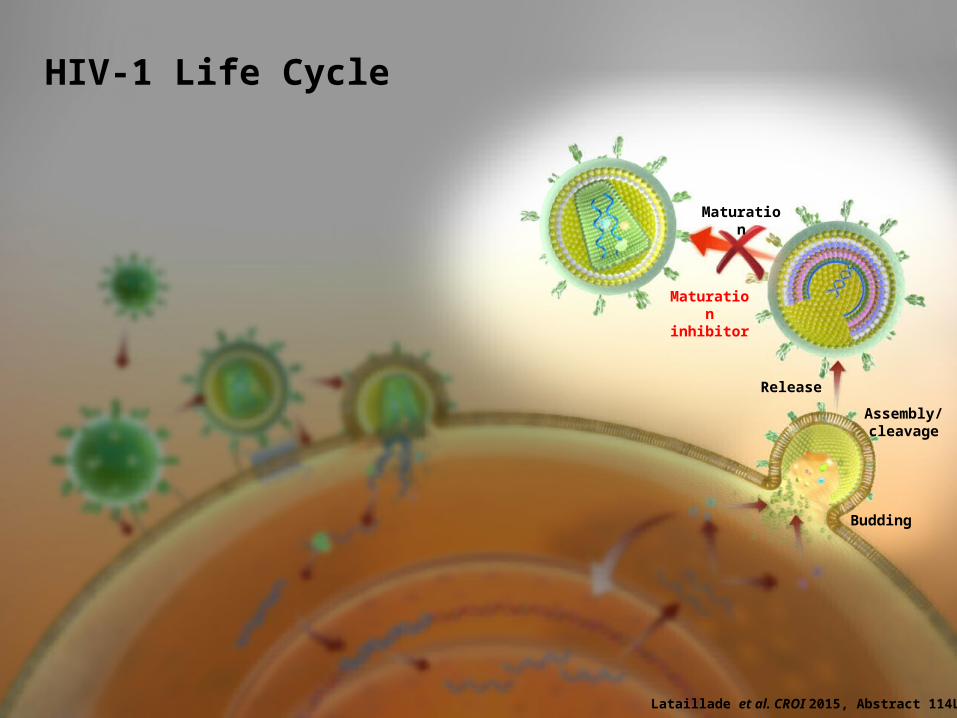
HIV-1 Life Cycle
Attachment
gp120
CD4
Viral DNA
Chemokine co-receptor Reverse
transcription
Human genomic DNA
Integration (strand transfer) Transcription
Translation
Accessory viral proteins
GagGag Pol
Budding
Assembly/cleavage
Release
Fusion
Maturation
Lataillade et al. CROI 2015, Abstract 114LB.
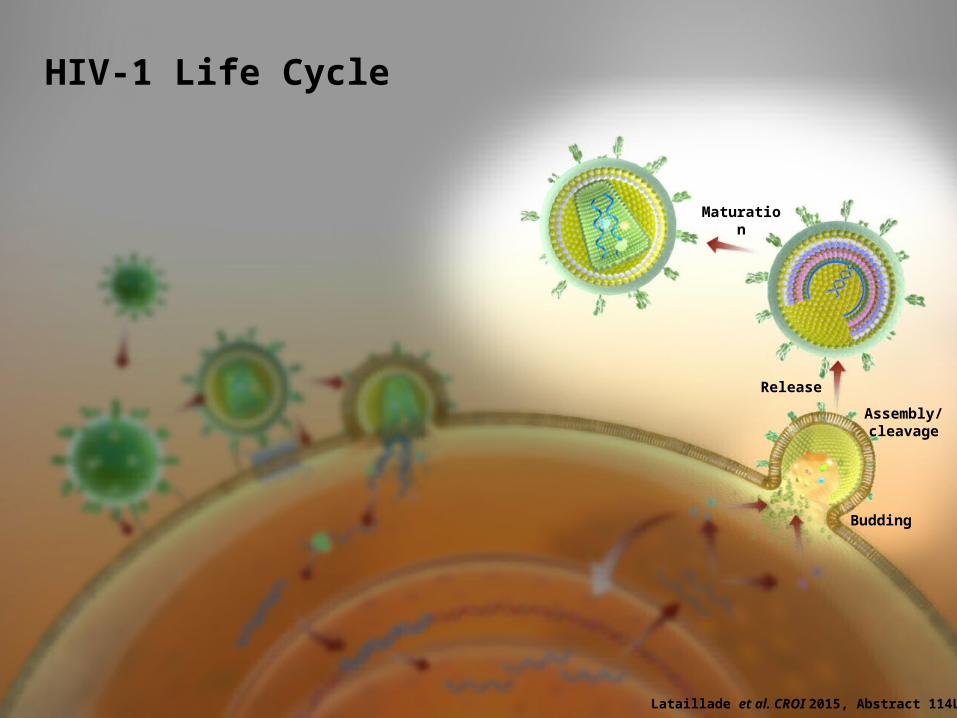
HIV-1 Life Cycle
Budding
Assembly/cleavage
Release
Maturation
Lataillade et al. CROI 2015, Abstract 114LB.
HIV-1 Life Cycle
Budding
Assembly/cleavage
Release
Maturation
inhibitor
Maturation
Lataillade et al. CROI 2015, Abstract 114LB.
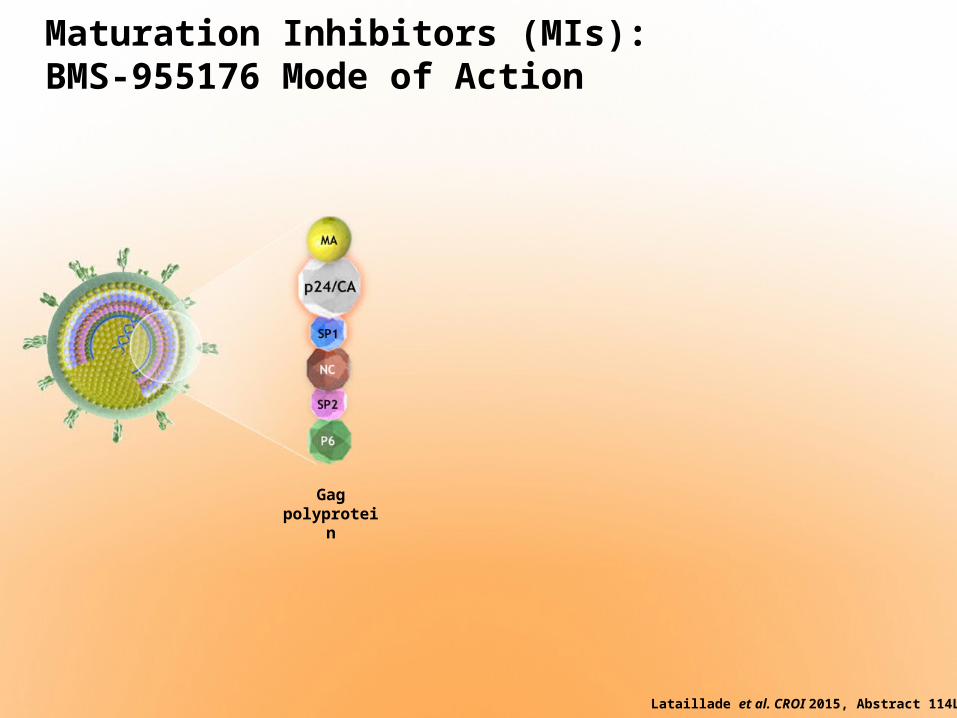
Maturation Inhibitors (MIs):BMS-955176 Mode of Action
Gagpolyprotei
n
Lataillade et al. CROI 2015, Abstract 114LB.
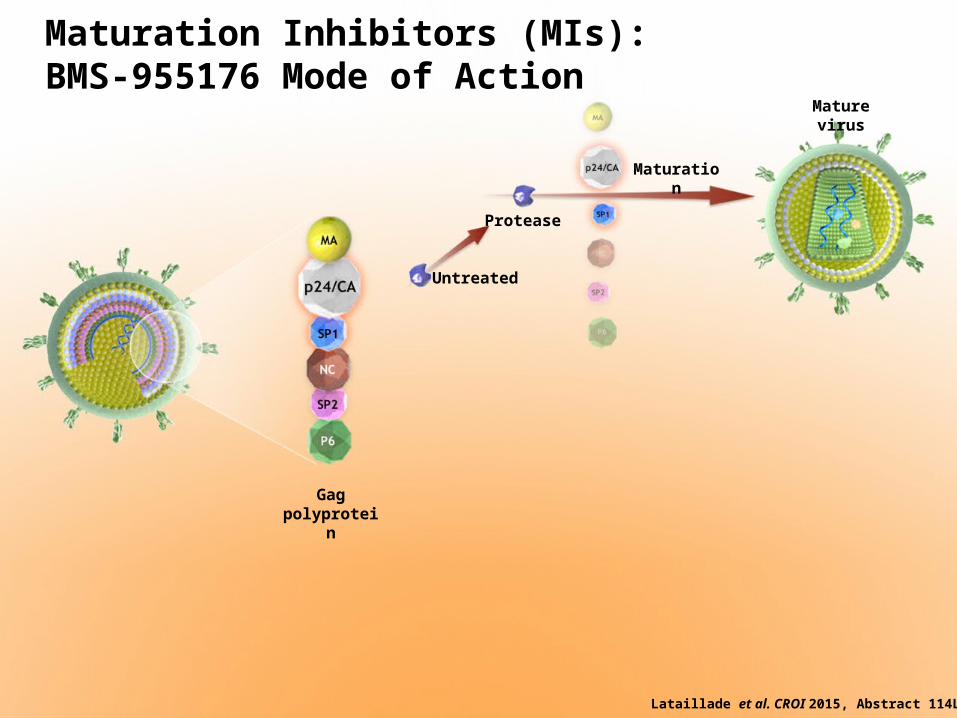
Protease
Mature virus
Gagpolyprotei
n
Maturation Inhibitors (MIs):BMS-955176 Mode of Action
Untreated
Maturation
Lataillade et al. CROI 2015, Abstract 114LB.
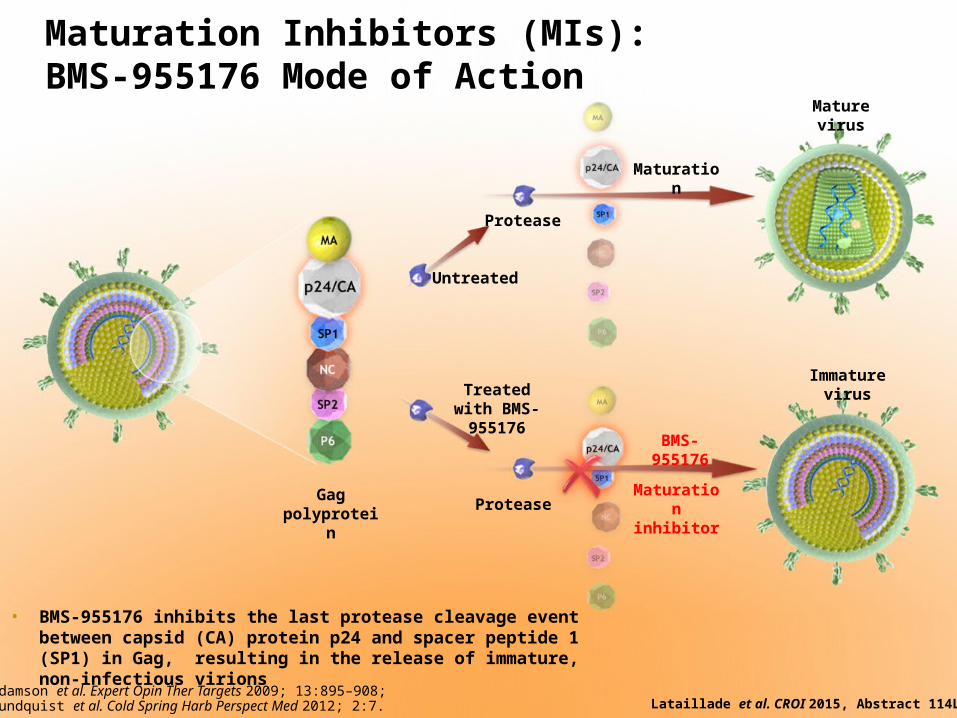
Protease
Untreated
Maturation
Mature virus
Gagpolyprotei
n
Treated with BMS-
955176 BMS-955176
Maturation
inhibitorProtease
Immature virus
• BMS-955176 inhibits the last protease cleavage event between capsid (CA) protein p24 and spacer peptide 1 (SP1) in Gag, resulting in the release of immature, non-infectious virions
Maturation Inhibitors (MIs):BMS-955176 Mode of Action
Adamson et al. Expert Opin Ther Targets 2009; 13:895–908;Sundquist et al. Cold Spring Harb Perspect Med 2012; 2:7. Lataillade et al. CROI 2015, Abstract 114LB.

BMS-955176: Profile of a Second‐Generation MI
• BMS-955176 is a second-generation MI that binds reversibly and with greater affinity to HIV-1 Gag than a first-generation MI (bevirimat; BVM)1,2
• Potent in vitro activity towards HIV-1, even in the presence of naturally occurring Gag polymorphisms associated with reduced BVM susceptibility2
• In vitro activity against PI-, NRTI-, NNRTI-, and INSTI-resistant isolates2
• In a 10-day BMS-955176 monotherapy proof-of-concept study:• Maximum median declines in HIV-1 RNA of >1 log10 c/mL (at doses 20–120 mg QD)
were achieved that plateaued at ~1.64 log10 c/mL at doses between 40 mg and 120 mg QD3
• Similar antiviral activity toward both wild-type HIV-1 and HIV-1 with Gag polymorphisms not responsive to BVM3
• BMS-955176 was generally well tolerated3
• Two drug combination studies in vitro demonstrated that BMS-955176 + ATV had an additive effect. Due to the proximity of their sites of inhibition in the virus life cycle and the potential for synergy, we assessed the antiviral activity and safety of BMS-955176 with ATV±RTV
1. Lin et al. CROI 2015; Abstract 42; 2. Nowicka-Sans et al. IAS 2015; Poster TUPEA078; 3. Lataillade et al. CROI 2015; Abstract 114LB.ATV, atazanavir; INSTI, integrase strand transfer inhibitors; PI, protease inhibitor; RTV, ritonavir
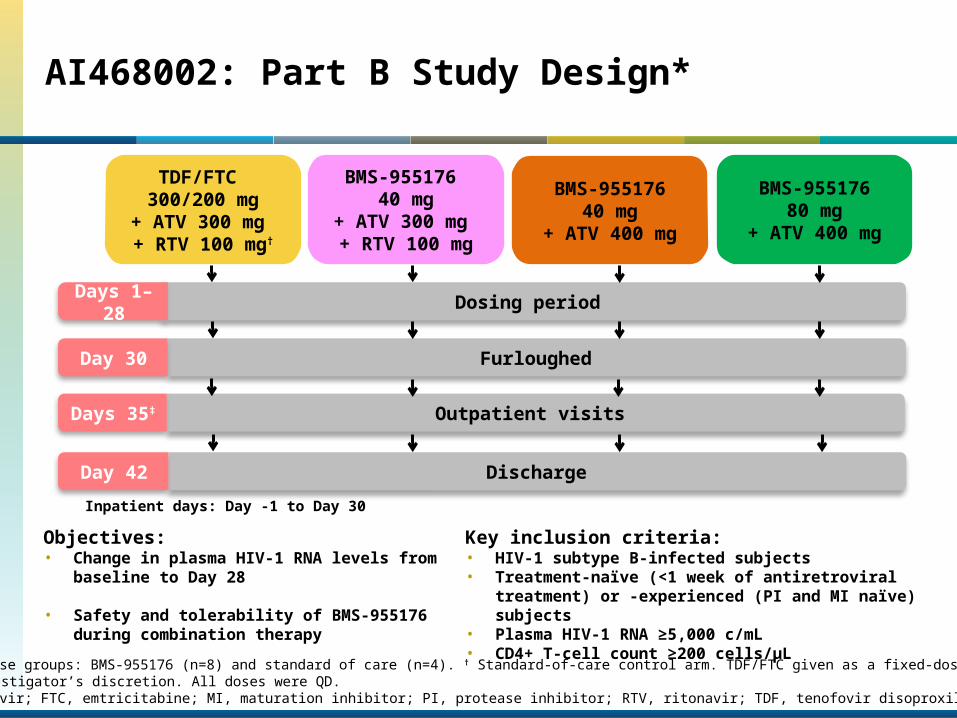
AI468002: Part B Study Design*
BMS-955176 40 mg
+ ATV 300 mg + RTV 100 mg
BMS-95517680 mg
+ ATV 400 mg
BMS-95517640 mg
+ ATV 400 mg
Dosing period
Furloughed
Outpatient visits
Discharge
Day 30
Days 35‡
Day 42
Days 1–28
TDF/FTC 300/200 mg
+ ATV 300 mg + RTV 100 mg†
Inpatient days: Day -1 to Day 30
Objectives: • Change in plasma HIV-1 RNA levels from
baseline to Day 28
• Safety and tolerability of BMS-955176 during combination therapy
Key inclusion criteria:• HIV-1 subtype B-infected subjects• Treatment-naïve (<1 week of antiretroviral
treatment) or -experienced (PI and MI naïve) subjects
• Plasma HIV-1 RNA ≥5,000 c/mL• CD4+ T-cell count ≥200 cells/µL* For all dose groups: BMS-955176 (n=8) and standard of care (n=4). † Standard-of-care control arm. TDF/FTC given as a fixed-dose combination.
‡ or per investigator’s discretion. All doses were QD.ATV, atazanavir; FTC, emtricitabine; MI, maturation inhibitor; PI, protease inhibitor; RTV, ritonavir; TDF, tenofovir disoproxil fumarate.
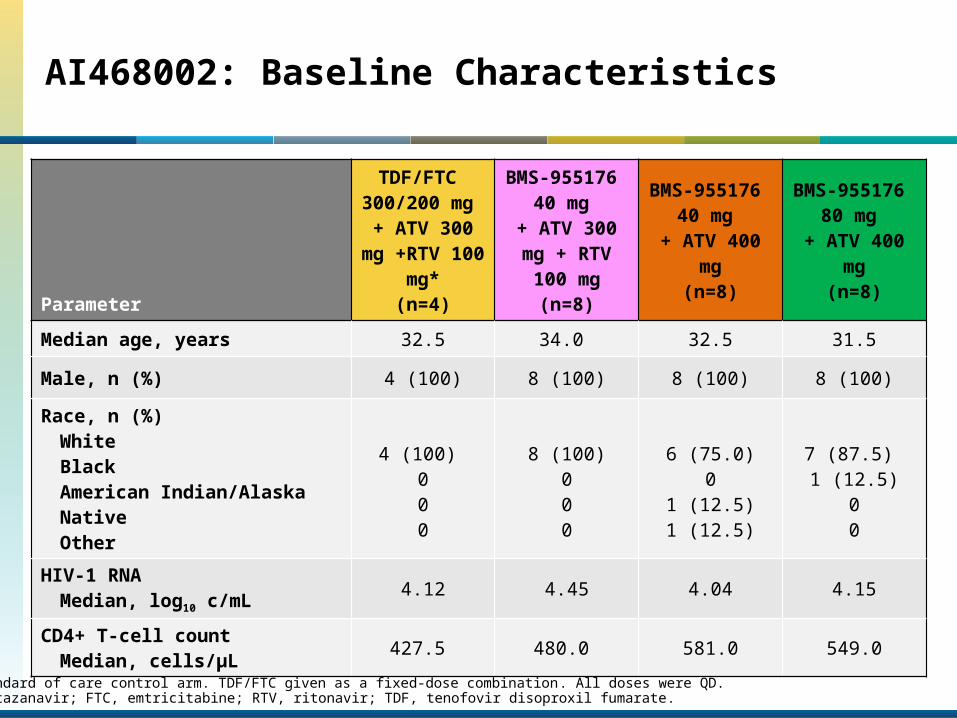
AI468002: Baseline Characteristics
Parameter
TDF/FTC 300/200 mg + ATV 300 mg +RTV 100 mg*
(n=4)
BMS-955176 40 mg
+ ATV 300 mg + RTV 100 mg(n=8)
BMS-955176 40 mg
+ ATV 400 mg
(n=8)
BMS-955176 80 mg
+ ATV 400 mg
(n=8)
Median age, years 32.5 34.0 32.5 31.5Male, n (%) 4 (100) 8 (100) 8 (100) 8 (100)Race, n (%)
WhiteBlackAmerican Indian/Alaska NativeOther
4 (100) 000
8 (100)000
6 (75.0)0
1 (12.5)1 (12.5)
7 (87.5) 1 (12.5)
00
HIV-1 RNA Median, log10 c/mL 4.12 4.45 4.04 4.15
CD4+ T-cell countMedian, cells/µL 427.5 480.0 581.0 549.0
* Standard of care control arm. TDF/FTC given as a fixed-dose combination. All doses were QD.ATV, atazanavir; FTC, emtricitabine; RTV, ritonavir; TDF, tenofovir disoproxil fumarate.
–2.5–2
–1.5–1
–0.50
0.51
Med
ian
chan
ge in
HIV
-1RN
A (lo
g 10 c
/mL)
from
bas
elin
e
TDF/FTC 300 mg/200 mg + ATV 300 mg + RTV 100 mg*BMS-955176 40 mg + ATV 300 mg + RTV 100 mgBMS-955176 40 mg + ATV 400 mgBMS-955176 80 mg + ATV 400 mg
Study day10 15 20 25 30 35 40 45 5050
Dosing period
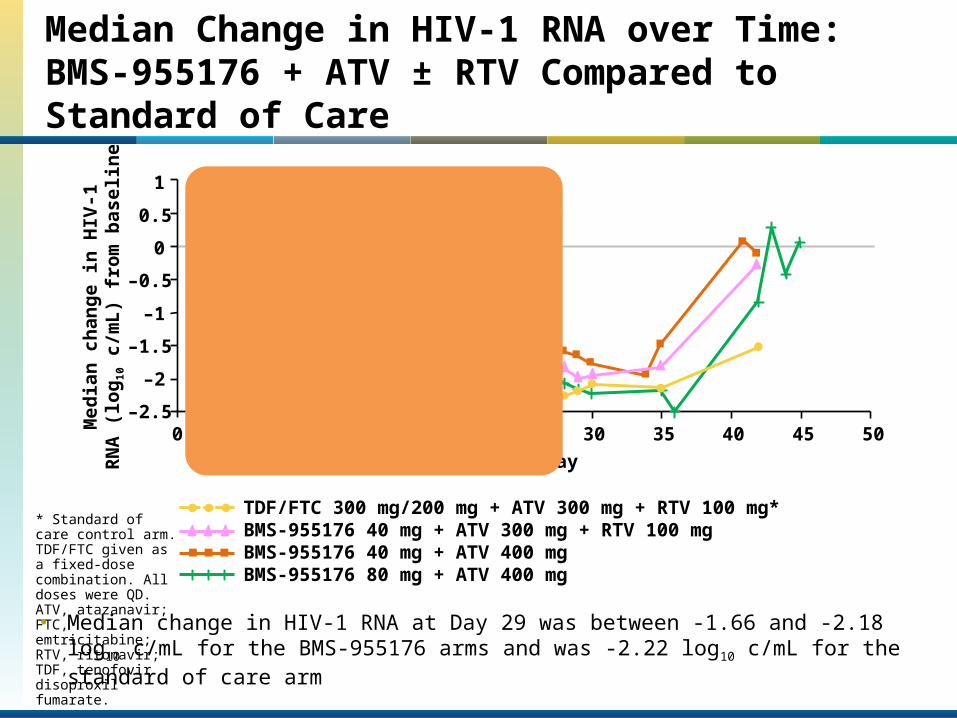
Median Change in HIV-1 RNA over Time: BMS-955176 + ATV ± RTV Compared to Standard of Care
* Standard of care control arm. TDF/FTC given as a fixed-dose combination. All doses were QD.ATV, atazanavir; FTC, emtricitabine; RTV, ritonavir; TDF, tenofovir disoproxil fumarate.
• Median change in HIV-1 RNA at Day 29 was between -1.66 and -2.18 log10 c/mL for the BMS-955176 arms and was -2.22 log10 c/mL for the standard of care arm
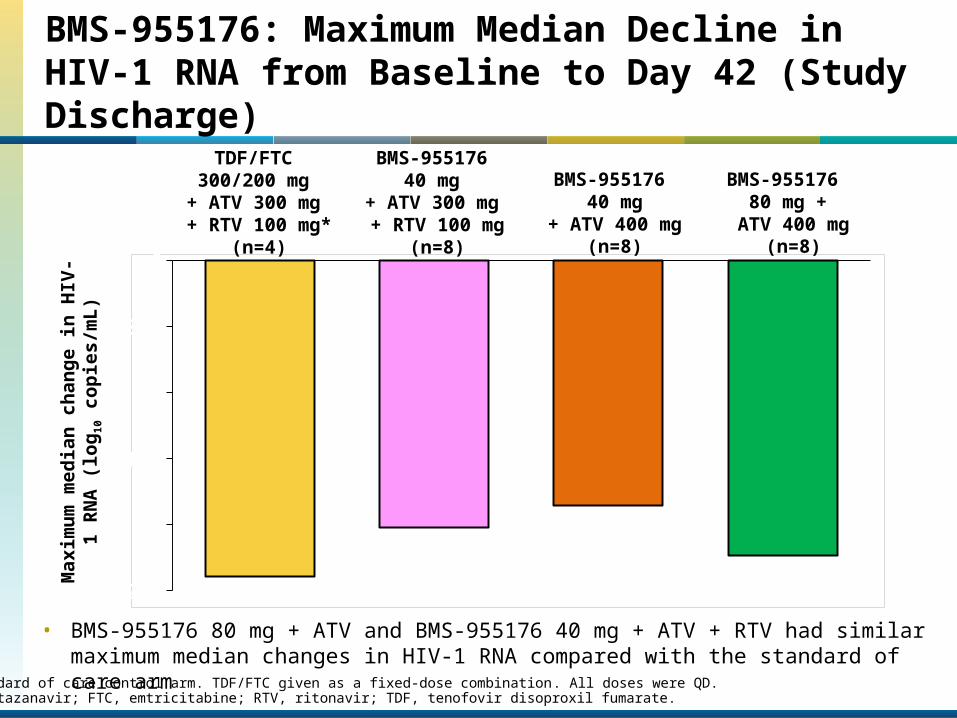
BMS-955176: Maximum Median Decline in HIV-1 RNA from Baseline to Day 42 (Study Discharge)
• BMS-955176 80 mg + ATV and BMS-955176 40 mg + ATV + RTV had similar maximum median changes in HIV-1 RNA compared with the standard of care arm
Max
imum
med
ian
chan
ge in
H
IV-1
RN
A (l
og10
cop
ies/
mL)
-2.5
-2
-1.5
-1
-0.5
0
-2.39
-2.02-1.86
-2.23
TDF/FTC 300/200 mg
+ ATV 300 mg + RTV 100 mg*
(n=4)
BMS-955176 40 mg
+ ATV 300 mg + RTV 100 mg
(n=8)
BMS-955176 40 mg
+ ATV 400 mg(n=8)
BMS-955176 80 mg +
ATV 400 mg(n=8)
* Standard of care control arm. TDF/FTC given as a fixed-dose combination. All doses were QD.ATV, atazanavir; FTC, emtricitabine; RTV, ritonavir; TDF, tenofovir disoproxil fumarate.
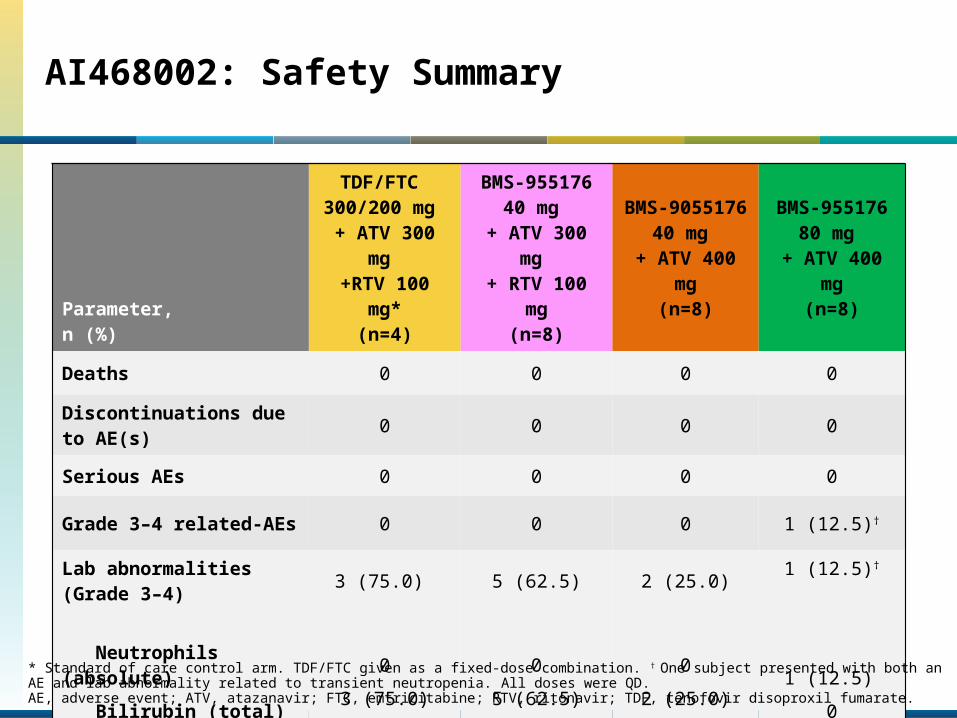
AI468002: Safety Summary
Parameter, n (%)
TDF/FTC 300/200 mg + ATV 300
mg +RTV 100
mg*(n=4)
BMS-955176 40 mg
+ ATV 300 mg
+ RTV 100 mg
(n=8)
BMS-9055176 40
mg + ATV 400
mg(n=8)
BMS-955176 80
mg + ATV 400
mg(n=8)
Deaths 0 0 0 0
Discontinuations due to AE(s) 0 0 0 0
Serious AEs 0 0 0 0
Grade 3–4 related-AEs 0 0 0 1 (12.5)†
Lab abnormalities(Grade 3–4)
Neutrophils (absolute) Bilirubin (total)
3 (75.0)
03 (75.0)
5 (62.5)
05 (62.5)
2 (25.0)
02 (25.0)
1 (12.5)†
1 (12.5)
0* Standard of care control arm. TDF/FTC given as a fixed-dose combination. † One subject presented with both an AE and lab abnormality related to transient neutropenia. All doses were QD.AE, adverse event; ATV, atazanavir; FTC, emtricitabine; RTV, ritonavir; TDF, tenofovir disoproxil fumarate.
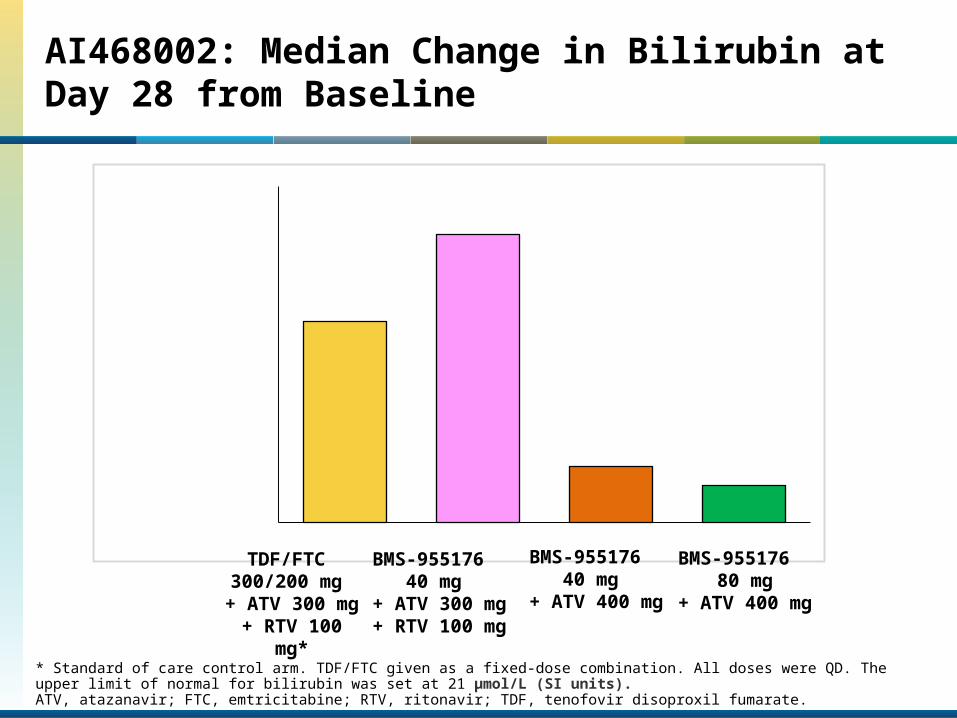
AI468002: Median Change in Bilirubin at Day 28 from Baseline
* Standard of care control arm. TDF/FTC given as a fixed-dose combination. All doses were QD. The upper limit of normal for bilirubin was set at 21 μmol/L (SI units). ATV, atazanavir; FTC, emtricitabine; RTV, ritonavir; TDF, tenofovir disoproxil fumarate.
Series10
10
20
30
40
50
60
70
41.8
60.0
11.87.7
Med
ian
chan
ge in
tota
l bili
rubi
n at
Da
y 28
fro
m B
asel
ine,
(μ
mol
/L, S
I Uni
ts)
BMS-955176
40 mg + ATV 400
mg
BMS-955176
40 mg + ATV 300
mg + RTV 100
mg
BMS-955176
80 mg+ ATV 400
mg
TDF/FTC 300/200 mg + ATV 300
mg + RTV 100
mg*
Conclusions
• BMS-955176 is a potent, once-daily, second-generation MI
• BMS-955176 80 mg + ATV and BMS-955176 40 mg + ATV + RTV demonstrated similar antiviral activity (~2.2 log10 c/mL median decline) compared to the standard of care control over the 28-day treatment period
• BMS-955176 was generally well tolerated• There were no SAEs or AEs leading to discontinuation
• BMS-955176 + unboosted ATV was associated with lower median changes from baseline in bilirubin levels compared to the arms with boosted ATV
• A Phase IIb study investigating BMS-955176 + ATV in a booster-sparing and nucleot(s)ide-sparing regimen in treatment-experienced patients initiated July 2015
BMS-955176: Characterization of a 2nd-Generation HIV-1 Maturation Inhibitor
Presented by I. Dicker
Poster TUPEA078 (B Nowicka-Sans, et al.)July 21, 12:30 –14:30 PST (Exhibit Hall B)
Acknowledgments
• We would like to thank all of the AI468002 clinical trial participants and their families
• Special thanks to:• Dirk Schürmann MD, Christian Sobotha MD and Charité Research Organisation GmbH• Marta Boffito, MD, PhD, St. Stephen’s Centre, Chelsea and Westminster Hospital• Ira Dicker, PhD, lead virologist for the discovery and characterization of BMS-955176• Heather Sevinsky, MS, lead clinical pharmacologist• Neela Ray, PhD, HIV clinical biomarker lead
• Bristol-Myers Squibb personnel: Mark Cockett, Richard Bertz, Nicholas Meanwell, Phyllis Chan, Albert DelMonte, Umesh Hanumegowda, Michael Child, Michele Stonier, Yash Gandhi, Alicia Regueiro-Ren, Samit Joshi, Beata Nowicka-Sans, Tricia Protack, Zeyu Lin, Zheng Liu, Matthew Healy, Philip Ross, Anupama Sheoran, Varsha Chhatre, Todd Correll and Eric Y Wong
• Charité Research Organisation GmbH: Andreas Hüser and Anke Schulze• Clinical team at St Stephen's AIDS Trust• Professional medical writing and editorial assistance was provided by Amanda
Gallagher at MediTech Media and 3D graphics were developed by Olly Venning at Nucleus Global – both funded by Bristol-Myers Squibb





























