Embed Size (px)
Citation preview

For peer review only
Efficacy and safety of second generation antipsychotic long acting injections (SGA LAIs) in maintenance treatment of
bipolar disorder: protocol for a systematic review and meta-analysis
Journal: BMJ Open
Manuscript ID bmjopen-2015-010237
Article Type: Protocol
Date Submitted by the Author: 12-Oct-2015
Complete List of Authors: PRAJAPATI, ASTA; Norfolk and Suffolk NHS Foundation Trust, Pharmacy Wilson, Jonathan; Norfolk and Suffolk NHS Foundation Trust Maidment, Ian; Aston University, Pharmacy
<b>Primary Subject Heading</b>:
Mental health
Secondary Subject Heading: Pharmacology and therapeutics
Keywords: Bipolar disorder, Second generation antipsychotics, Atypical antipsychotics, Antipsychotic long acting injections, Antipsychotic depots
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open on D
ecember 4, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010237 on 6 January 2016. D
ownloaded from

For peer review only
1. Title: “Efficacy and safety of Second Generation Antipsychotic Long Acting
Injections (SGA LAIs) in maintenance treatment of bipolar disorder: study
protocol for a systematic review and meta-analysis”
2. Author: Mr Asta Ratna Prajapati, Clinical Pharmacy Manager, Pharmacy Department, Hellesdon Hospital, Norfolk and Suffolk NHS Foundation Trust, Drayton High Road, Norwich, NR6 5BE, UK. E.mail: [email protected], Tel: 01603 421 606, Fax: 01603 421
3. Co-authors: Dr Jonathan Wilson, Deputy Medical Director, Research,
Norfolk and Suffolk NHS Foundation Trust, Norfolk, UK.
Dr Ian Maidment, Senior Lecturer, Pharmacy, Aston University, Birmingham, UK.
4. Keywords: Second Generation Antipsychotics, Long Acting Injections, Atypical antipsychotics, Bipolar Disorder, Antipsychotic depots
5. Word count: 2683 (excluding references, title page and flowchart).
Page 1 of 13
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 4, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010237 on 6 January 2016. Dow
nloaded from

For peer review only
Page 1 of 12
Efficacy and safety of second generation antipsychotic long acting injections
(SGA LAIs) in maintenance treatment of bipolar disorder: protocol for a
systematic review and meta-analysis
Abstract
Introduction: Bipolar disorder requires long term treatment but non-adherence is a
common problem. Antipsychotic long acting injections (LAIs) have been suggested
to improve adherence but none are licensed in the UK for bipolar. However, the use
of Second Generation Antipsychotics (SGA) LAIs in bipolar is not uncommon albeit
there is a lack of systematic review in this area. This study aims to systematically
review safety and efficacy of SGA LAIs in the maintenance treatment of bipolar
disorder. Methods and analysis: The protocol is based on Preferred Reporting
Items for Systematic reviews and Meta-Analyses (PRISMA) and will include only
randomized controlled trials comparing SGA LAIs in bipolar. Pubmed, Embase,
CINAHL, Cochrane Library (CENTRAL), PsychINFO, LiLACS, www.clinicaltrials.gov
will be searched, with no language restriction, from 2000 to Jan 2016 as first SGA
LAIs came to the market after 2000. Manufacturers of SGA LAIs will also be
contacted. Primary efficacy outcome is relapse rate or delayed time to relapse or
reduction in hospitalization and primary safety outcomes are drop-out rates, all-
cause discontinuation and discontinuation due to adverse events. Qualitative
reporting of evidence will be based on 21 items listed on standards for reporting
qualitative research (SRQR) focusing on study quality (assessed using the Jadad
score, allocation concealment and data analysis), risk of bias and effect size.
Publication bias will be assessed using funnel plots. If sufficient data are available
meta-analysis will be performed with primary effect size as relative risk presented
with 95% confidence interval. Sensitivity analysis, conditional on number of studies
and sample size, will be carried out on manic vs. depressive symptoms and
monotherapy vs. adjunctive therapy.
Ethics and dissemination: Ethical approval is not required as primary data will not
be collected. The results will be disseminated through a peer-reviewed publication,
conference presentation and the press.
Study registration number: PROSPERO CRD42015023948
Page 2 of 13
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 4, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010237 on 6 January 2016. Dow
nloaded from

For peer review only
Page 2 of 12
Strengths and Limitations of this study:
• Systematic review and meta-analysis of randomised controlled trials provide
the highest level of evidence to key stakeholders.
• This systematic review will search comprehensive list of databases using well
defined search strategy, will contact manufacturers for any unpublished
and/or ongoing trials.
• This study will clarify the position of second generation antipsychotics (SGAs)
long acting injections (LAIs) in maintenance treatment of bipolar disorder.
• Qualitative evidence summary and meta-analysis will address some highly
relevant clinical questions in bipolar disorder. Subgroup analyses will further
enhance the applicability of the results from this study.
• This review is focused on as SGA LAIs since first generation antipsychotics
are not considered preferred choice in maintenance treatment of bipolar
disorder due to risk of induction of depression.
• Lack of data and significant heterogeneity may prevent meta-analysis.
Background
The lifetime prevalence of bipolar I disorder is estimated at 1% of the adult
population, and bipolar II disorder affects approximately 0.4% of adults (1). Bipolar
disorder featuring mood and activity level disturbance is a recurrent disorder; it
usually requires long term maintenance therapy to prevent future mood episodes -
the primary goal of treatment (2). Lithium remains the gold standard prophylactic
treatment for bipolar disorder (1). However lithium may not be suitable for all patients
due to a lack of response or adverse events, or patients may not accept lithium due
to various reasons including monitoring requirement and/or side effects (3). Thus,
many patients require alternative prophylactic treatment for bipolar disorder. Many
guidelines including British Association of Psychopharmacology (4), The World
Federation of Societies of Biological Psychiatry (WFSBP) (5) and National Institute
for Health and Care Excellence (NICE) (1) from the UK recommend some Second
Generation Antipsychotic (SGA, also known as atypical antipsychotics) as a long
term treatment option for bipolar disorder; and many oral SGAs are licensed in the
UK for this indication (6).
Page 3 of 13
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 4, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010237 on 6 January 2016. Dow
nloaded from

For peer review only
Page 3 of 12
Non-adherence to the prescribed treatment is a major problem and common in
bipolar disorder with estimated frequency of non-adherence between 10% and 60%
(median 40%) (7). Non-adherence to treatment in bipolar disorder increases the risk
of relapse and suicide (8); and increased risk of rehospitalisation (7). Long Acting
Injections (LAIs, also known as depots) have some clear advantages due to
assurance that medication will be administered and the opportunity for healthcare
professionals to step in immediately if patients stop treatment (9). Evidence from
studies in people with schizophrenia suggests antipsychotics LAIs reduce relapses,
reduce medication discontinuation rates and improve outcomes compared to oral
antipsychotics although Cochrane review of various depots did not find any
convincing difference (9). However, these reviews also included in-patient studies,
short term trials of just a few weeks duration (9) and mostly included only First
Generation Antipsychotic (FGA, also known as typical antipsychotics) LAIs. LAIs
formulations have other Pharmacological advantages: more predictable
bioavailability since LAIs medications bypass gastrointestinal absorption and the
effect of first-pass hepatic metabolism, more stable plasma levels compared to oral
antipsychotics, sustained medication plasma levels at the therapeutic range (7).
The use of SGA LAIs in the maintenance treatment of bipolar disorder has ignited
interest for improving adherence and reducing the risk of relapse (7). Over the last 5
years two new SGA LAIs, aripiprazole and paliperidone, have been introduced in the
UK. However, none of the SGA LAIs are currently licensed for bipolar disorder in the
UK (6) albeit clinical experience suggests their uses for this indication are not
infrequent. Recent (2011) mixed-treatment meta-analysis suggests that
antipsychotics are more effective than mood stabilisers in the treatment of mania
(10). Some studies have found that risperidone LAI is effective for maintenance
treatment in bipolar disorder (7). Risperidone LAI is also approved by US FDA for
monotherapy or as adjunctive therapy to lithium or valproate for the maintenance
treatment of Bipolar I Disorder (11).
Despite these potential advantages of antipsychotic LAIs in the treatment of bipolar
disorder there is a lack of any properly conducted systematic review. During a
scoping search, two literature reviews conducted within last 5 years were identified
(7, 8). Literature reviews do provide a useful overview of the subject; however they
Page 4 of 13
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 4, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010237 on 6 January 2016. Dow
nloaded from

For peer review only
Page 4 of 12
generally lack the rigour of systematic reviews. Systematic reviews of well-designed
randomized controlled trials (RCTs) are considered gold-standard and top of the
evidence hierarchy in healthcare research (13-15). A systematic review with a
focused clinical question with clear specifications searches all relevant databases
with pre-defined systematic search strategy and using pre-specified eligibility criteria
for studies to be included. A systematic review also provides the assessment of the
quality of the studies included in the review aiming to avoid bias and therefore
support evidence based practice. With pre-defined protocol good systematic reviews
provide robust evidence to support or change clinical practice.
Gigante et al. (7) reviewed evidence of FGAs and SGA LAIs in bipolar disorder
searching pubmed from 1950 to 2011 and published in English. This review included
all types of studies from randomised controlled trials (RCTs) to retrospective chart
reviews in their evidence synthesis. In terms of SGA LAIs only literatures pertaining
to risperidone LAI were found. The level of evidence is limited due to small number
(n=2) of large RCTs. No RCTs were found involving other SGA LAIs except
risperidone. The authors concluded that FGA LAI should not be a first choice due to
risk of induction of depression but suggested risperidone LAI is effective in bipolar.
This is consistent with previous literature review by Bond et al. 2007 (16).
Recently (2014) Samalin et al. (8) carried out another review of SGA LAIs in bipolar
disorder and concluded that risperidone LAI may be considered for maintenance
treatment of bipolar disorder but more evidence is required. This review included
RCTs, case series and did not include any specific inclusion / exclusion criteria, did
not perform quality assessment, focused the search on pubmed and embase and no
information gathered from manufacturers. The authors carried out last search in April
2013 which gives us around two and half years of potential extra literature, a good
time frame to review evidence in this moving field. In addition, Samalin et al. found
studies only on risperidone LAI and this systematic review is expected to find studies
related to other SGA as scoping exercise found some ongoing active studies of other
SGA LAI.
This systematic review will include only RCTs comparing SGA LAIs with placebo or
other antipsychotics or mood stabilizers or treatment as usual; search many other
relevant databases as listed in the methodology section; contact manufacturers for
Page 5 of 13
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 4, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010237 on 6 January 2016. Dow
nloaded from

For peer review only
Page 5 of 12
further trials (both ongoing and unpublished trials), quality assess all included
studies; and investigate risk of bias. The protocol is registered with PROSPERO-
www.crd.york.ac.uk/PROSPERO/ - international prospective register of systematic
reviews.
The result of this study will have an impact on clinical practice and prescribing
decision either to support or discourage use of SGA LAIs in maintenance treatment
of bipolar disorder. It is author’s intention to publish the result of this study in a peer
reviewed journal and to widely communicate with key clinical and academic
stakeholders both nationally and internationally. The result from the study will close
the evidence gap and thus inform healthcare professionals and patients of the
evidence or lack of it in using SGA LAIs in bipolar disorder.
Objective
To conduct systematic review of RCTs evaluating efficacy and safety of SGA LAIs in
maintenance treatment of bipolar disorder.
Methodology
The research protocol is based on PRISMA, Preferred Reporting Items for
Systematic reviews and Meta-Analyses (17). Specific PICOS; participants,
interventions, comparators, outcomes, and study design; detailed below will be used
for study selection criteria:
1) Inclusion criteria for selecting studies for this review:
Any studies not meeting following inclusion criteria will be excluded.
A. Participants: patients of any age or sex with bipolar disorder using any
validated diagnostic system, e.g. Diagnostic and Statistical Manual of
Mental Disorders (DSM-V: 296) or the International Classification of
Diseases (ICD 10: F31).
B. Interventions: SGA LAIs in bipolar disorder
C. Comparators: placebo, other antipsychotics, mood stabilizer or
treatment as usual
D. Outcome measures:
Page 6 of 13
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 4, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010237 on 6 January 2016. Dow
nloaded from

For peer review only
Page 6 of 12
I. Primary efficacy outcome - relapse rate or delayed time to
relapse or reduction in hospitalization
II. Primary safety outcome - drop-out rates or all-cause
discontinuation, discontinuation due to adverse events
III. Secondary outcomes may include changes in BDRS (Bipolar
Disorder Rating Scale) or YMRS (Young Mania Rating Scales),
discontinuation due to hospitalization, and non-adherence (study
defined), safety outcome of SGA LAIs e.g. EPSEs and
metabolic adverse effect – weight gain, hyperglycaemia,
dyslipidaemia, hyperprolactinaemia.
E. Study design: RCTs with or without double blinding with minimum
duration of 6 months. It is anticipated that most studies will be out-
patient as non-adherence in in-patients is unlikely due to staff
administration. Nonetheless this study will include both out-patients
and in-patients as some units are long stay in-patient units in secure
services or rehabilitation units and since sustained therapeutic plasma
level has been suggested as a pharmacological advantage of LAIs in
addition to improvement in adherence.
Data sources, search strategy and study selection
Missing any relevant and significant study may render the systematic review
less credible. The following detailed search strategy will be employed to
ensure all relevant studies are captured, independently analysed, verified and
quality assessed.
A comprehensive, electronic search strategy will be used to identify relevant
RCTs in humans where SGA LAIs are being assessed for efficacy and safety
in bipolar disorder. There will be no language restrictions. Studies published
between January 2000 and Jan 2016 will be searched since SGA LAIs came
to the market only after 2000. The searches will be re-run just before the final
analyses and any further eligible studies retrieved for inclusion.
Page 7 of 13
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 4, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010237 on 6 January 2016. Dow
nloaded from

For peer review only
Page 7 of 12
Following databases will be searched: Pubmed, Embase, CINAHL, Cochrane
Library (CENTRAL), PsychINFO, LiLACS, www.clinicaltrials.gov. Any relevant
studies mentioned in those identified studies will be searched manually, for
example scoping the references listed. Manufacturers of SGA LAIs will be
contacted for any ongoing or unpublished studies.
To capture all relevant studies the search strategy will consist of three
domains: disease (bipolar disorder), treatment (SGA) and formulation (LAIs).
Each domains will be searched using many terms (as listed below) with
Boolean search operator “OR”. The Boolean search operator “AND” will be
used to connect these three domains.
a) Disease domain: bipolar*, mood disorder*, mania*, manic-depression*,
hypomania*, AND
b) Treatment domain: antipsychotic*, neuroleptic*, psychotropic*,
atypical*, second generation antipsychotic*, SGA*, aripiprazole,
olanzapine, paliperidone, risperidone, ziprasidone AND
c) Formulation domain: depot*, long-acting injection*, LAI*, prolonged
release injection*, sustained release injection*
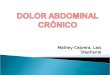
The process; of identifying, screening of studies and inclusion or exclusion of
those studies; is shown in the PRISMA flow diagram below:
Page 8 of 13
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 4, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010237 on 6 January 2016. Dow
nloaded from

For peer review only
Page 8 of 12
3. Data collection, analysis and quality assessment
A list of all identified studies from all the resources searched will be created.
Any other studies mentioned or referred to in these studies which seem
relevant to the review will be hand searched. Titles of all the studies retrieved
using the search strategy and those from additional sources will be screened
for their relevance to the review. Definite non-relevant studies will be excluded
“N” records identified through
database searching
“n” additional records identified through
other sources e.g. Manufacturers, hand
search
{(N+n)-X}= N1 records after duplicates (X) removed
(N1– X1) = N2 titles screened X1 records excluded, with
reasons
(N2-X2) = N3 abstracts assessed
N4 of studies included in
qualitative synthesis
X2 abstracts excluded, with
reasons
(N4-X4) = N5 of studies
included in meta-analysis
(N3-X3) = N4 of full-text articles
assessed
X3 full-text articles excluded,
with reasons
X4 studies not suitable for
meta-analysis
Iden
tifi
cati
on
S
cree
nin
g
Eli
gib
ilit
y
Incl
ud
ed
Page 9 of 13
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 4, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010237 on 6 January 2016. Dow
nloaded from

For peer review only
Page 9 of 12
while relevant, ambiguous or unclear studies will be included for screening
abstract.
All the articles will be screened for its title to check their relevance by lead
author (AP) and second reviewer (JW). Abstracts of the remaining studies,
after discarding definite irrelevant studies, will be screened by the lead author
(AP) and second reviewer (JW) to identify studies that potentially meet the
inclusion criteria outlined above. The second reviewer (JW) will review titles
and abstract independently and list studies to be included and those to
exclude. Any disagreement between two reviewers over the eligibility of
particular studies will be resolved through further discussion and / or with third
reviewer (IM) involvement.
A standardised, pre-piloted form will be used to extract data from the included
studies for assessment of study quality and evidence synthesis. Extracted
information will include: study design; study population and participant
demographics and baseline characteristics; details of the intervention and
control conditions; study methodology; recruitment and study completion
rates; outcomes and times of measurement; information for assessment of the
risk of bias. The lead reviewer (AP) will extract the data and any ambiguity/
questions will be discussed with 2nd (JW) and / or 3rd (IM) reviewer. Missing
data will be requested from study authors.
Study quality will be assessed using Cochrane collaboration's risk of bias tool
and publication bias by visual inspection of funnel plots (18).
Narrative qualitative evidence synthesis will be provided on aggregate level on
study outcome for their primary and secondary outcome. Qualitative reporting
of evidence will be based on 21 items listed on standards for reporting
qualitative research (SRQR) (19). Total number of patients in the study, study
quality, risk of bias and effect size will be detailed on qualitative evidence
summary.
Page 10 of 13
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 4, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010237 on 6 January 2016. Dow
nloaded from

For peer review only
Page 10 of 12
Meta-analysis
It is authors’ intention to undertake quantitative meta-analysis. If study data
and sample size are sufficient meta-analysis will be performed. Statistical
significance will be set at 0.05 with value <0.05 considered statistically
significant. The primary effect size will be relative risk presented with 95%
confidence interval. The analysis will be based on intention-to-treat where
data available. Study heterogeneity will be measured using I2-statistic
considering values of 50% or higher to reflect considerable heterogeneity
which will be investigated.
Sensitivity analysis
If sufficient number of studies and sample size are available, sensitivity
analysis will be carried out on manic vs. depressive symptoms and
monotherapy vs. adjunctive therapy or different antipsychotic.
Ethical approval: This systematic review does not require ethical approval, as data
used here are not individual or private and there will be no primary data collection.
Funding statement: This research received no specific grant from any funding
agency in the public, commercial or not-for-profit sectors.
Authors: Asta R Prajapati (AP), Clinical Pharmacy Manager, Pharmacy Department,
Dr Jonathan Wilson (JW), Deputy Medical Director, Research, both at
Norfolk and Suffolk NHS Foundation Trust; Dr Ian Maidment (IM), Senior
Lecturer, Pharmacy, Aston University.
Correspondence: [email protected]
Declarations of interest: AP- None. IM has received speaker honoraria from
Astellas Pharmaceuticals. JW - waiting confirmation (currently on leave).
Author’s contribution: AP and IM conceived the study. AP drafted the protocol and
registered with PROSPERO. IM helped design the protocol
and reviewed protocol. JW reviewed the protocol. All authors
have approved the publication of this protocol.
Page 11 of 13
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 4, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010237 on 6 January 2016. Dow
nloaded from

For peer review only
Page 11 of 12
References
1. National Institute of Health and Care Excellence (NICE). (2014). Bipolar disorder: the
assessment and management of bipolar disorder in adults, children and young people in
primary and secondary care - NICE guidelines (CG185).
http://www.nice.org.uk/guidance/cg185 (accessed 03/07/2015)
2. Gitlin, M, Frye, MA. (2012). Maintenance therapies in bipolar disorders. Bipolar Disord,
14: 51-65. http://onlinelibrary.wiley.com/doi/10.1111/j.1399-5618.2012.00992.x/pdf
(accessed 03/07/2015)
3. Villeneuve, A. Acceptance of Lithium Therapy by the Patient. In: Johnson, F.N., editor.
Handbook of Lithium Therapy. 1st ed. New York: Springer; 1980.
4. Goodwin, GM. (2009). Evidence-based guidelines for treating bipolar disorder: revised
second edition—recommendations from the British Association for
Psychopharmacology. Journal of Psychopharmacology, 23(4) 346–388.
http://www.bap.org.uk/pdfs/Bipolar_guidelines.pdf (accessed 28/06/2015)
5. Grunze, H., Vieta, E., Gooodwin, G.M. 2013. The World Federation of Societies of
Biological Psychiatry (WFSBP) Guidelines for the Biological Treatment of Bipolar
Disorders: Update 2012 on the long-term treatment of bipolar disorder. The World
Journal of Biological Psychiatry, 2013; 14: 154–219. Available at:
http://www.wfsbp.org/fileadmin/user_upload/Treatment_Guidelines/Grunze_et_al_2013.
pdf (accessed 25/08/15)
6. British Medical Association, Royal Pharmaceutical Society. (2015) British National
Formulary. 69th
ed. UK: BMJ Group and Pharmaceutical Press;
http://www.bnf.org/bnf/index.htm (accessed 01/07/2015)
7. Gigante, A. D., Beny Lafer, B., Yatham, L. (2014) Long-Acting Injectable
Antipsychotics for the Maintenance Treatment of Bipolar Disorder. CNS Drugs 26
(5):403-420. http://link.springer.com/article/10.2165%2F11631310-000000000-00000
(accessed 30/06/2015)
8. Samalin, L., Nourry, A., Charpeaud, T., Llorca, P.M. (2014). What is the evidence for
the use of second-generation antipsychotic long-acting injectables as maintenance
treatment in bipolar disorder? Nordic Journal of Psychiatry, 68/4: 227-235.
http://informahealthcare.com/doi/abs/10.3109/08039488.2013.801078 (accessed
30/06/2015)
9. Leucht, C., Heres, S., Kane, J.M., Kissling, W., Davis J.M., Leucht, S. (2011). Oral
versus depot antipsychotic drugs for schizophrenia—A critical systematic review and
meta-analysis of randomised long-term trials. Schizophrenia Research 127: 83–92.
http://www.schres-journal.com/article/S0920-9964(10)01649-X/pdf (accessed
03/07/2015)
10. Cipriani, A., Barbui, C., Salanti, G., Rendell, J., Brown, R., Stockton, S et al. (2011).
Comparative efficacy and acceptability of antimanic drugs in acute mania: a multiple-
Page 12 of 13
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 4, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010237 on 6 January 2016. Dow
nloaded from

For peer review only
Page 12 of 12
treatments meta-analysis. Lancet 378 (9799):1306-15.
http://www.sciencedirect.com/science/article/pii/S0140673611608738 (accessed
04/07/2015)
11. US FDA. (2009). Risperdal Consta – highlight of prescribing information. Label
information. NDA 21-346 S-025, S-028.
http://www.accessdata.fda.gov/drugsatfda_docs/label/2009/021346s025s028lbl.pdf
(accessed on 7/06/2015)
12. Kysh, L. 2013. Difference between a systematic review and a literature review. figshare.
Available at: http://dx.doi.org/10.6084/m9.figshare.766364 (accessed 25/09/2015)
13. Evans, D. (2003). Hierarchy of evidence: a framework for ranking evidence evaluating
healthcare interventions. Journal of Clinical Nursing, 12: 77–84. Available at:
http://www.ncbi.nlm.nih.gov/pubmed/12519253 (accessed 25/09/15)
14. Burns, P.B., Rohrich, R.J., Chung, K.C. 2013. The Levels of Evidence and their role in
Evidence-Based Medicine, Plast Reconstr Surg. Author manuscript; available in PMC
2012 July 1. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3124652/ (accessed
25/09/15)
15. Sackett, D.L., Straus, S.E., Richardson, W.S., et al. 2000. Evidence-Based Medicine is
the integration of best research evidence with clinical expertise and patient values.
(Evidence-based medicine: how to practice and teach EBM. 2nd ed. Edinburgh:
Churchill Livingstone, 2000.) http://hsls.pitt.edu/resources/ebm (accessed 25/09/15)
16. Bond, D.J., Pratoomsri, W., Yatham, L.N. 2007. Depot antipsychotic medications in
bipolar disorder: a review of the literature. Acta Psychiatr Scand 2007: 116 (Suppl. 434):
3–16. Available at: http://www.ncbi.nlm.nih.gov/pubmed/17688458 (accessed 07/08/15)
17. Moher, D., Liberati, A., Tetzlaff, J., Altman, D.G., The PRISMA Group (2009).
Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA
Statement. PLoS Med 6(6): e1000097.
http://journals.plos.org/plosmedicine/article?id=10.1371/journal.pmed.1000097
(accessed 6/06/2015)
18. Higgins, J. PT., Green, S. (2011). Cochrane handbook; chapter 8: Assessing risk of bias
in included studies. The Cochrane Collaboration.
http://handbook.cochrane.org/chapter_8/8_assessing_risk_of_bias_in_included_studies.h
tm (accessed 04/07/2015)
19. O’Brien, B.C., Harris, I.B., Beckman, T.J., Reed, D. A., and Cook, D.A. 2014.
Standards for Reporting Qualitative Research:A Synthesis of Recommendations. Acad
Med. 2014;89:1245–1251. available at: http://www.ncbi.nlm.nih.gov/pubmed/24979285
(accessed 25/09/15)
Page 13 of 13
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 4, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010237 on 6 January 2016. Dow
nloaded from

For peer review only
Efficacy and safety of second generation antipsychotic long acting injections (SGA LAIs) in maintenance treatment of
bipolar disorder: protocol for a systematic review and meta-analysis
Journal: BMJ Open
Manuscript ID bmjopen-2015-010237.R1
Article Type: Protocol
Date Submitted by the Author: 17-Nov-2015
Complete List of Authors: PRAJAPATI, ASTA; Norfolk and Suffolk NHS Foundation Trust, Pharmacy Wilson, Jonathan; Norfolk and Suffolk NHS Foundation Trust Maidment, Ian; Aston University, Pharmacy
<b>Primary Subject Heading</b>:
Mental health
Secondary Subject Heading: Pharmacology and therapeutics
Keywords: Bipolar disorder, Second generation antipsychotics, Antipsychotic, Depot preparation, Maintenance therapy
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open on D
ecember 4, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010237 on 6 January 2016. D
ownloaded from

For peer review only
1. Title: “Efficacy and safety of Second Generation Antipsychotic Long Acting
Injections (SGA LAIs) in maintenance treatment of bipolar disorder: study
protocol for a systematic review and meta-analysis”
2. Author: Mr Asta Ratna Prajapati, Clinical Pharmacy Manager, Pharmacy Department, Hellesdon Hospital, Norfolk and Suffolk NHS Foundation Trust, Drayton High Road, Norwich, NR6 5BE, UK. E.mail: [email protected], Tel: 01603 421 606, Fax: 01603 421
3. Co-authors: Dr Jonathan Wilson, Deputy Medical Director, Research,
Norfolk and Suffolk NHS Foundation Trust, Norfolk, UK.
Dr Ian Maidment, Senior Lecturer, Pharmacy, Aston University, Birmingham, UK.
4. Keywords: Antipsychotics, Depot Preparations, Bipolar Disorder, Second Generation Antipsychotics, Maintenance Treatment
5. Word count: 2809 (excluding references, title page and flowchart).
Page 1 of 14
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 4, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010237 on 6 January 2016. Dow
nloaded from

For peer review only
Page 1 of 13
Efficacy and safety of second generation antipsychotic long acting injections
(SGA LAIs) in maintenance treatment of bipolar disorder: protocol for a
systematic review and meta-analysis
Asta R Prajapati (AP), Clinical Pharmacy Manager, Pharmacy Department, Dr
Jonathan Wilson (JW), Deputy Medical Director, Research, both at Norfolk and
Suffolk NHS Foundation Trust, UK; Dr Ian Maidment (IM), Senior Lecturer,
Pharmacy, Aston University, UK.
Correspondence: Asta Prajapati, Pharmacy Department, Hellesdon Hospital,
Drayton High Road, Norwich NR6 5BE, UK. E-mail: [email protected] Tel:
01603421212
Keywords: Antipsychotics, Depot Preparations, Bipolar Disorder, Second Generation
Antipsychotics, Maintenance Treatment
Word count: 2709 (excluding references, title page and flowchart
Abstract
Introduction: Bipolar disorder requires long-term treatment but non-adherence is a
common problem. Antipsychotic Long Acting Injections (LAIs) have been suggested
to improve adherence but none are licensed in the UK for bipolar. However, the use
of Second Generation Antipsychotics (SGA) LAIs in bipolar is not uncommon albeit
there is a lack of systematic review in this area. This study aims to systematically
review safety and efficacy of SGA LAIs in the maintenance treatment of bipolar
disorder. Methods and analysis: The protocol is based on Preferred Reporting
Items for Systematic reviews and Meta-Analyses (PRISMA) and will include only
randomized controlled trials comparing SGA LAIs in bipolar. Pubmed, Embase,
CINAHL, Cochrane Library (CENTRAL), PsychINFO, LiLACS, www.clinicaltrials.gov
will be searched, with no language restriction, from 2000 to Jan 2016 as first SGA
LAIs came to the market after 2000. Manufacturers of SGA LAIs will also be
contacted. Primary efficacy outcome is relapse rate or delayed time to relapse or
reduction in hospitalization and primary safety outcomes are drop-out rates, all-
cause discontinuation and discontinuation due to adverse events. Qualitative
reporting of evidence will be based on 21 items listed on standards for reporting
Page 2 of 14
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 4, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010237 on 6 January 2016. Dow
nloaded from

For peer review only
Page 2 of 13
qualitative research (SRQR) focusing on study quality (assessed using the Jadad
score, allocation concealment and data analysis), risk of bias and effect size.
Publication bias will be assessed using funnel plots. If sufficient data are available
meta-analysis will be performed with primary effect size as relative risk presented
with 95% confidence interval. Sensitivity analysis, conditional on number of studies
and sample size, will be carried out on manic vs. depressive symptoms and
monotherapy vs. adjunctive therapy.
Ethics and dissemination: Ethical approval is not required as primary data will not
be collected. The results will be disseminated through a peer-reviewed publication,
conference presentation and the press.
Study registration number: PROSPERO CRD42015023948
Strengths and Limitations of this study:
• Systematic review and meta-analysis of randomized controlled trials provide
the highest level of evidence to key stakeholders.
• This systematic review will search a comprehensive list of databases using
well-defined search strategy; will contact manufacturers for any unpublished
and/or ongoing trials.
• This study will clarify the position of second generation antipsychotics (SGAs)
long acting injections (LAIs) in maintenance treatment of bipolar disorder.
• Qualitative evidence summary and meta-analysis will address some highly
relevant clinical questions in bipolar disorder. Subgroup analyses will further
enhance the applicability of the results from this study.
• This review is focused on as SGA LAIs since first generation antipsychotics
are not considered preferred choice in maintenance treatment of bipolar
disorder due to risk of induction of depression.
• Lack of data and significant heterogeneity may prevent meta-analysis.
Background
The lifetime prevalence of bipolar I disorder is estimated at 1% of the adult
population, and bipolar II disorder affects approximately 0.4% of adults (1). Bipolar
Page 3 of 14
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 4, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010237 on 6 January 2016. Dow
nloaded from

For peer review only
Page 3 of 13
disorder, featuring mood and activity level disturbance, is a recurrent disorder; it
usually requires long-term maintenance therapy to prevent future mood episodes -
the primary goal of treatment (2). Lithium remains the gold standard prophylactic
treatment for bipolar disorder (1). However lithium may not be suitable for all patients
due to a lack of response or adverse events, or patients may not accept lithium due
to various reasons including monitoring requirement and/or side effects (3). Thus,
many patients require alternative prophylactic treatment for bipolar disorder. Many
guidelines including British Association of Psychopharmacology (4), The World
Federation of Societies of Biological Psychiatry (WFSBP) (5), Canadian Network for
Mood and Anxiety Treatments (CANMAT) and International Society for Bipolar
Disorders (ISBD) (6), and National Institute for Health and Care Excellence (NICE)
(1) from the UK recommend some Second Generation Antipsychotic (SGA, also
known as atypical antipsychotics) as a long-term treatment option for bipolar
disorder; and many oral SGAs are licensed in the UK for this indication (7).
Non-adherence to the prescribed treatment is a major problem and common in
bipolar disorder. Estimated frequency of non-adherence in bipolar range between
10% and 60% (median 40%) (8). Non-adherence increases the risk of relapse and
suicide (9); and increased risk of rehospitalisation (8). Long Acting Injections (LAIs,
also known as depots) have some clear advantages due to assurance that
medication will be administered and the opportunity for healthcare professionals to
step in immediately if patients stop treatment (10). Evidence from studies in people
with schizophrenia suggests antipsychotics LAIs reduce relapses, reduce medication
discontinuation rates and improve outcomes compared to oral antipsychotics
although some Cochrane reviews of various depots did not find any convincing
difference (10). However, these Cochrane reviews also included in-patient studies,
short-term trials of just a few weeks duration (10) and mostly included only First
Generation Antipsychotic (FGA, also known as typical antipsychotics) LAIs. LAIs
formulations have other Pharmacological advantages: more predictable
bioavailability since LAIs medications bypass gastrointestinal absorption and the
effect of first-pass hepatic metabolism, more stable plasma levels compared to oral
antipsychotics, sustained plasma levels of medication at therapeutic range (8).
Page 4 of 14
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 4, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010237 on 6 January 2016. Dow
nloaded from

For peer review only
Page 4 of 13
The use of SGA LAIs in the maintenance treatment of bipolar disorder has ignited
interest for improving adherence and reducing the risk of relapse (8). Over the last 5
years two new SGA LAIs, aripiprazole and paliperidone, have been introduced in the
UK. None of the SGA LAIs are currently licensed for bipolar disorder in the UK (7)
albeit clinical experience suggests their uses for this indication are not infrequent.
Recent (2011) mixed-treatment meta-analysis suggests that antipsychotics are more
effective than mood stabilisers in the treatment of mania (11). Some studies have
found that risperidone LAI is effective for maintenance treatment in bipolar disorder
(7, 8) and CANMAT recommends risperidone LAI as one of the first line treatment
options in maintenance treatment of bipolar disorder (6). Risperidone LAI is
approved by US FDA for monotherapy or as an adjunctive therapy to lithium or
valproate for the maintenance treatment of Bipolar I Disorder (12).
Despite these potential advantages of antipsychotic LAIs in the treatment of bipolar
disorder there is a lack of any properly conducted systematic review. During a
scoping search two literature reviews (8, 9) conducted within last 5 years were
identified (). Literature reviews offer a useful overview of the subject; however they
generally lack the rigour of systematic reviews. Systematic reviews of well-designed
randomized controlled trials (RCTs) are considered gold-standard and top of the
evidence hierarchy in healthcare research (13-15). A systematic review with a
focused clinical question with clear specifications searches all relevant databases
with pre-defined systematic search strategy and using pre-specified eligibility criteria
for studies to be included. A systematic review also provides the assessment of the
quality of the studies included in the review aiming to avoid bias and therefore
support evidence based practice. With pre-defined protocol good systematic reviews
provide robust evidence to support or change clinical practice.
Gigante et al. (8) reviewed evidence of FGAs and SGA LAIs in bipolar disorder
searching pubmed from 1950 to 2011 and published in English. This review included
all types of studies from randomised controlled trials (RCTs) to retrospective chart
reviews in their evidence synthesis. In terms of SGA LAIs only literatures pertaining
to risperidone LAI were found. The level of evidence is limited due to small number
(n=2) of large RCTs. No RCTs were found involving other SGA LAIs except
risperidone. The authors concluded that FGA LAI should not be a first choice due to
Page 5 of 14
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 4, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010237 on 6 January 2016. Dow
nloaded from

For peer review only
Page 5 of 13
risk of induction of depression but suggested risperidone LAI is effective in bipolar.
This is consistent with earlier literature review by Bond et al. 2007 (16).
Recently (2014) Samalin et al. (9) carried out another review of SGA LAIs in bipolar
disorder and concluded that risperidone LAI may be considered for maintenance
treatment of bipolar disorder but more evidence is required. This review included
RCTs, case series and did not include any specific inclusion / exclusion criteria; did
not perform quality assessment; focused the search on pubmed and embase; and no
information sought from manufacturers. The authors carried out last search in April
2013 which gives us around two and half years of potential extra literature, a good
time frame to review evidence in this moving field. In addition, Samalin et al. found
studies only on risperidone LAI and this systematic review is expected to find studies
related to other SGA as scoping exercise found some ongoing active studies of other
SGA LAI.
Chou et al. (2015) (17) authored an article titled “A Systemic Review and Experts’
Consensus for Long-acting Injectable Antipsychotics in Bipolar Disorder”. This was
an expert consensus building study and good endeavour for consensus report on the
topic but lacking any details on review process and methodology, a critical and
essential aspect of any systematic reviews. In addition, Chou et al looked at both
FGAs and SGAs and found studies pertaining to risperidone LAI only in terms of
SGA LAIs.
This systematic review will:
• include only RCTs comparing SGA LAIs with placebo or other antipsychotics
or mood stabilizers or treatment as usual;
• search many other relevant databases as listed in the methodology section;
• contact manufacturers for further trials (both ongoing and unpublished trials);
• quality assess all included studies and
• investigate the risk of bias.
The protocol is registered with PROSPERO- www.crd.york.ac.uk/PROSPERO/ -
international prospective register of systematic reviews.
The result of this study will have an impact on clinical practice and prescribing
decision either to support or discourage use of SGA LAIs in maintenance treatment
Page 6 of 14
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 4, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010237 on 6 January 2016. Dow
nloaded from

For peer review only
Page 6 of 13
of bipolar disorder. It is author’s intention to publish the result of this study in a peer
reviewed journal and to widely communicate with key clinical and academic
stakeholders both nationally and internationally. The result from the study will close
the evidence gap and thus inform healthcare professionals and patients of the
evidence or lack of it in using SGA LAIs in bipolar disorder.
Objective
To conduct systematic review and meta-analysis of RCTs evaluating efficacy and
safety of SGA LAIs in maintenance treatment of bipolar disorder
Methodology
The research protocol is based on PRISMA, Preferred Reporting Items for
Systematic reviews and Meta-Analyses (18). Specific PICOS; Participants,
Interventions, Comparators, Outcomes, and Study design; detailed below will be
used for study selection criteria:
1) Inclusion criteria:
Any studies not meeting following inclusion criteria will be excluded.
A. Participants: patients of any age or sex with bipolar disorder using any
validated diagnostic system, e.g. Diagnostic and Statistical Manual of
Mental Disorders (DSM-V: 296) or the International Classification of
Diseases (ICD 10: F31).
B. Interventions: SGA LAIs in bipolar disorder
C. Comparators: placebo, other antipsychotics, mood stabilizer or
treatment as usual
D. Outcome measures:
I. Primary efficacy outcome - relapse rate or delayed time to
relapse or reduction in hospitalization
II. Primary safety outcome - drop-out rates or all-cause
discontinuation or discontinuation due to adverse events
III. Secondary outcomes may include changes in BDRS (Bipolar
Disorder Rating Scale) or YMRS (Young Mania Rating Scales),
discontinuation due to hospitalization, and non-adherence (study
defined), safety outcome of SGA LAIs e.g. EPSEs and
Page 7 of 14
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 4, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010237 on 6 January 2016. Dow
nloaded from

For peer review only
Page 7 of 13
metabolic adverse effect – weight gain, hyperglycaemia,
dyslipidaemia, hyperprolactinaemia.
E. Study design: RCTs with or without double blinding with minimum
duration of 6 months. It is anticipated that most studies will be out-
patient as non-adherence in in-patients is unlikely due to staff
administration. Nonetheless this study will include both out-patients
and in-patients as some units are long stay in-patient units in secure
services or rehabilitation units and since sustained therapeutic plasma
level has been suggested as a pharmacological advantage of LAIs in
addition to improvement in adherence.
Data sources, search strategy and study selection
Missing any relevant and significant study may render the systematic review
less credible. The following detailed search strategy will be employed to
ensure all relevant studies are captured, independently analysed, verified and
quality assessed.
A comprehensive, electronic search strategy will be used to identify relevant
RCTs in humans where SGA LAIs are being assessed for efficacy and safety
in bipolar disorder. There will be no language restrictions. Studies published
between January 2000 and Jan 2016 will be searched since SGA LAIs came
to the market only after 2000. The searches will be re-run just before the final
analyses and any further eligible studies retrieved for inclusion.
Following databases will be searched: Pubmed, Embase, CINAHL, Cochrane
Library (CENTRAL), PsychINFO, LiLACS, www.clinicaltrials.gov. Any relevant
studies mentioned in those identified studies will be searched manually, for
example scoping the references listed. Manufacturers of SGA LAIs will be
contacted for any ongoing or unpublished studies.
To capture all relevant studies the search strategy will consist of three
domains: disease (bipolar disorder), treatment (SGA) and formulation (LAIs).
Each domains will be searched using many terms (as listed below) with
Page 8 of 14
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 4, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010237 on 6 January 2016. Dow
nloaded from

For peer review only
Page 8 of 13
Boolean search operator “OR”. The Boolean search operator “AND” will be
used to connect these three domains.
a) Disease domain: bipolar*, mood disorder*, mania*, manic-depression*,
hypomania*, AND
b) Treatment domain: antipsychotic*, neuroleptic*, psychotropic*,
atypical*, second generation antipsychotic*, SGA*, aripiprazole,
olanzapine, paliperidone, risperidone, ziprasidone AND
c) Formulation domain: depot*, long-acting injection*, LAI*, prolonged
release injection*, sustained release injection*
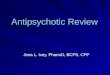
The process; of identifying, screening of studies and inclusion or exclusion of
those studies; is shown in the PRISMA flow diagram below:
Page 9 of 14
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 4, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010237 on 6 January 2016. Dow
nloaded from

For peer review only
Page 9 of 13
3. Data collection, analysis and quality assessment
A list will be created for all identified studies from all the resources searched.
Any other studies mentioned or referred to in these studies which seem
relevant to the review will be hand searched. Titles of all the studies retrieved
using the search strategy and those from additional sources will be screened
for their relevance to the review. Definite non-relevant studies will be excluded
“N” records identified through
database searching
“n” additional records identified through
other sources e.g. Manufacturers, hand
search
{(N+n)-X}= N1 records after duplicates (X) removed
(N1– X1) = N2 titles screened X1 records excluded, with
reasons
(N2-X2) = N3 abstracts assessed
N4 of studies included in
qualitative synthesis
X2 abstracts excluded, with
reasons
(N4-X4) = N5 of studies
included in meta-analysis
(N3-X3) = N4 of full-text articles
assessed
X3 full-text articles excluded,
with reasons
X4 studies not suitable for
meta-analysis
Identification
Screening
Eligibility
Included
Page 10 of 14
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 4, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010237 on 6 January 2016. Dow
nloaded from

For peer review only
Page 10 of 13
while relevant, ambiguous or unclear studies will be included for screening
abstract.
All the articles will be screened for its title to check their relevance by lead
author (AP) and second reviewer (JW). Abstracts of the remaining studies,
after discarding definite irrelevant studies, will be screened by the lead author
(AP) and second reviewer (JW) to identify studies that potentially meet the
inclusion criteria outlined above. The second reviewer (JW) will review titles
and abstract independently and list studies to be included and those to
exclude. Any disagreement between two reviewers over the eligibility of
particular studies will be resolved through further discussion and / or with third
reviewer (IM) involvement.
A standardised, pre-piloted form will be used to extract data from the included
studies for assessment of study quality and evidence synthesis. Extracted
information will include: study design; study population and participant
demographics and baseline characteristics; details of the intervention and
control conditions; study methodology; recruitment and study completion
rates; outcomes and times of measurement; information for assessment of the
risk of bias. The lead reviewer (AP) will extract the data and any ambiguity/
questions will be discussed with 2nd (JW) and / or 3rd (IM) reviewer. Missing
data will be requested from study authors and / or manufacturers.
Study quality will be assessed using Cochrane collaboration's risk of bias tool
and publication bias by visual inspection of funnel plots (19).
Narrative qualitative evidence synthesis will be provided on aggregate level on
study outcome for their primary and secondary outcome. Qualitative reporting
of evidence will be based on 21 items listed on standards for reporting
qualitative research (SRQR) (20). Total number of patients in the study, study
quality, risk of bias and effect size will be detailed on qualitative evidence
summary.
Meta-analysis
It is authors’ intention to undertake quantitative meta-analysis. If study data
and sample size are sufficient meta-analysis will be performed. Statistical
Page 11 of 14
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 4, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010237 on 6 January 2016. Dow
nloaded from

For peer review only
Page 11 of 13
significance will be set at 0.05 with p-value <0.05 considered statistically
significant. The primary effect size will be relative risk presented with 95%
confidence interval. The analysis will be based on intention-to-treat where
data available. Study heterogeneity will be measured using I2-statistic
considering values of 50% or higher to reflect considerable heterogeneity
which will be investigated.
Sensitivity analysis
If sufficient number of studies and sample size are available, sensitivity
analysis will be carried out on manic vs. depressive symptoms and
monotherapy vs. adjunctive therapy or different antipsychotic.
Ethical approval: This systematic review does not require ethical approval as data
used here are not individual or private and there will be no primary data collection.
Funding statement: This research received no specific grant from any funding
agency in the public, commercial or not-for-profit sectors.
Acknowledgement: We would like to thank Dr Bonnie Teague, Research Manager at
Norfolk and Suffolk NHS Foundation Trust, for her support and encouragement for
this study.
Declarations of interest: AP received conference travel expenses from Janssen. IM
has received speaker honoraria from Astellas Pharmaceuticals. JW received grants
from Lundbeck, personal fees from Shire outside the submitted work.
Authors’ contribution: AP and IM conceived the study. AP drafted the protocol and
registered with PROSPERO. IM helped design the protocol and reviewed protocol.
JW reviewed the protocol. All authors have approved the publication of this protocol.
References
1. National Institute of Health and Care Excellence (NICE). (2014). Bipolar disorder: the
assessment and management of bipolar disorder in adults, children and young people in
primary and secondary care - NICE guidelines (CG185).
http://www.nice.org.uk/guidance/cg185 (accessed 03/07/2015)
Page 12 of 14
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 4, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010237 on 6 January 2016. Dow
nloaded from

For peer review only
Page 12 of 13
2. Gitlin, M, Frye, MA. (2012). Maintenance therapies in bipolar disorders. Bipolar Disord,
14: 51-65. http://onlinelibrary.wiley.com/doi/10.1111/j.1399-5618.2012.00992.x/pdf
(accessed 03/07/2015)
3. Villeneuve, A. Acceptance of Lithium Therapy by the Patient. In: Johnson, F.N., editor.
Handbook of Lithium Therapy. 1st ed. New York: Springer; 1980.
4. Goodwin, GM. (2009). Evidence-based guidelines for treating bipolar disorder: revised
second edition—recommendations from the British Association for
Psychopharmacology. Journal of Psychopharmacology, 23(4) 346–388.
http://www.bap.org.uk/pdfs/Bipolar_guidelines.pdf (accessed 28/06/2015)
5. Grunze, H., Vieta, E., Gooodwin, G.M. 2013. The World Federation of Societies of
Biological Psychiatry (WFSBP) Guidelines for the Biological Treatment of Bipolar
Disorders: Update 2012 on the long-term treatment of bipolar disorder. The World
Journal of Biological Psychiatry, 2013; 14: 154–219. Available at:
http://www.wfsbp.org/fileadmin/user_upload/Treatment_Guidelines/Grunze_et_al_2013.
pdf (accessed 25/08/15)
6. Yatham, L .N., Kennedy, S.H, Parikh, S.V, Schaffer, A., Beaulieu, S., Alda, M. et al.
Canadian Network for Mood and Anxiety Treatments (CANMAT) and International
Society for Bipolar Disorders (ISBD)collaborative update of CANMAT guidelines for
the management of patients with bipolar disorder: update 2013. Bipolar Disorders 2013:
15: 1–44. Blackwell Publishing Ltd. Available at :
http://canmat.org/resources/CANMAT%20Bipolar%20Disorder%20Guidelines%20-
2013%20Update.pdf (accessed 09/11/2015)
7. British Medical Association, Royal Pharmaceutical Society. (2015) British National
Formulary. 69th ed. UK: BMJ Group and Pharmaceutical Press;
http://www.bnf.org/bnf/index.htm (accessed 01/07/2015)
8. Gigante, A. D., Beny Lafer, B., Yatham, L. (2014) Long-Acting Injectable
Antipsychotics for the Maintenance Treatment of Bipolar Disorder. CNS Drugs 26
(5):403-420. http://link.springer.com/article/10.2165%2F11631310-000000000-00000
(accessed 30/06/2015)
9. Samalin, L., Nourry, A., Charpeaud, T., Llorca, P.M. (2014). What is the evidence for
the use of second-generation antipsychotic long-acting injectables as maintenance
treatment in bipolar disorder? Nordic Journal of Psychiatry, 68/4: 227-235.
http://informahealthcare.com/doi/abs/10.3109/08039488.2013.801078 (accessed
30/06/2015)
10. Leucht, C., Heres, S., Kane, J.M., Kissling, W., Davis J.M., Leucht, S. (2011). Oral
versus depot antipsychotic drugs for schizophrenia—A critical systematic review and
meta-analysis of randomised long-term trials. Schizophrenia Research 127: 83–92.
http://www.schres-journal.com/article/S0920-9964(10)01649-X/pdf (accessed
03/07/2015)
Page 13 of 14
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 4, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010237 on 6 January 2016. Dow
nloaded from

For peer review only
Page 13 of 13
11. Cipriani, A., Barbui, C., Salanti, G., Rendell, J., Brown, R., Stockton, S et al. (2011). Comparative efficacy and acceptability of antimanic drugs in acute mania: a multiple-
treatments meta-analysis. Lancet 378 (9799):1306-15.
http://www.sciencedirect.com/science/article/pii/S0140673611608738 (accessed
04/07/2015)
12. US FDA. (2009). Risperdal Consta – highlight of prescribing information. Label
information. NDA 21-346 S-025, S-028.
http://www.accessdata.fda.gov/drugsatfda_docs/label/2009/021346s025s028lbl.pdf
(accessed on 7/06/2015)
13. Evans, D. (2003). Hierarchy of evidence: a framework for ranking evidence evaluating
healthcare interventions. Journal of Clinical Nursing, 12: 77–84. Available at:
http://www.ncbi.nlm.nih.gov/pubmed/12519253 (accessed 25/09/15)
14. Burns, P.B., Rohrich, R.J., Chung, K.C. 2013. The Levels of Evidence and their role in Evidence-Based Medicine, Plast Reconstr Surg. Author manuscript; available in PMC
2012 July 1. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3124652/ (accessed
25/09/15)
15. Sackett, D.L., Straus, S.E., Richardson, W.S., et al. 2000. Evidence-Based Medicine is
the integration of best research evidence with clinical expertise and patient values.
(Evidence-based medicine: how to practice and teach EBM. 2nd ed. Edinburgh:
Churchill Livingstone, 2000.) http://hsls.pitt.edu/resources/ebm (accessed 25/09/15)
16. Bond, D.J., Pratoomsri, W., Yatham, L.N. 2007. Depot antipsychotic medications in
bipolar disorder: a review of the literature. Acta Psychiatr Scand 2007: 116 (Suppl. 434):
3–16. Available at: http://www.ncbi.nlm.nih.gov/pubmed/17688458 (accessed 07/08/15)
17. Chou, Y.H., Chu, P., Wu, S., Lee, J., Lee, Y., Sun, I. et al.. A Systemic Review and
Experts’ Consensus for Long-acting Injectable . Clinical Psychopharmacology and
Neuroscience 2015; 13(2): 121-128. Available at:
http://www.cpn.or.kr/journal/view.html?doi=10.9758/cpn.2015.13.2.121 (accessed
10/11/15)
18. Moher, D., Liberati, A., Tetzlaff, J., Altman, D.G., The PRISMA Group (2009).
Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA
Statement. PLoS Med 6(6): e1000097.
http://journals.plos.org/plosmedicine/article?id=10.1371/journal.pmed.1000097
(accessed 6/06/2015)
19. Higgins, J. PT., Green, S. (2011). Cochrane handbook; chapter 8: Assessing risk of bias in included studies. The Cochrane Collaboration.
http://handbook.cochrane.org/chapter_8/8_assessing_risk_of_bias_in_included_studies.h
tm (accessed 04/07/2015)
20. O’Brien, B.C., Harris, I.B., Beckman, T.J., Reed, D. A., and Cook, D.A. 2014.
Standards for Reporting Qualitative Research:A Synthesis of Recommendations. Acad
Med. 2014;89:1245–1251. available at: http://www.ncbi.nlm.nih.gov/pubmed/24979285
(accessed 25/09/15)
Page 14 of 14
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 4, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010237 on 6 January 2016. Dow
nloaded from