-
1332 www.ccmjournal.org May 2013 Volume 41 Number 5
Intensivists use neuromuscular blocking agents for a variety of
clin-ical conditions, including for emergency intubation, acute
respira-tory distress syndrome, status asthmaticus, elevated
intracranial pressure, elevated intra-abdominal pressure, and
therapeutic hypothermia after ventricular fibrillationassociated
cardiac arrest. The continued creation and use of evidence-based
guidelines and protocols could ensure that neuromuscular blocking
agents are used and monitored appropriately. A collaborative
multidisciplinary approach coupled with constant review of the
pharmacology, dos-ing, drug interactions, and monitoring techniques
may reduce the adverse events associated with the use of
neuromuscular block-ing agents. (Crit Care Med 2013;
41:13321344)Key Words: associated complications; ICU; monitoring;
neuromuscular blockade; pharmacology; reversal; use
Currently, controversy surrounds the use of neuromus-cular
blocking agents (NMBAs) in the ICU. Proposed adjunctive
applications for NMBAs in the ICU include the following: improving
chest wall compliance, eliminating ventilator dyssynchrony,
reducing intra-abdominal pressures (IAPs), preventing and treating
shivering, and preventing ele-vations in intracranial pressure
(ICP) from airway stimulation. These relative indications are
tempered by clinician concern for development of prolonged
ICU-acquired weakness (ICU-AW); prolonged mechanical ventilation;
the risk of patient awareness during paralysis; and an increased
risk for deep venous throm-bosis (DVT), corneal abrasions, and
anaphylaxis (1).
Today, NMBAs are being used much less frequently than in past
years. A survey of 34 ICUs from the 1980s reported that 90% of
mechanically ventilated patients received NMBAs
(2). A more recent international observational study reported
that only 13% of patients on mechanical ventilation received NMBAs
(3). A 2006 Canadian survey of critical care practitio-ner
practices noted that the most important factors for choos-ing a
specific NMBA were clinician experience, duration of action,
mechanism of action, and patient-specific factors (4). A similar
survey conducted in the United States reported that clinical
experience and perception were the most common rea-sons for
choosing a NMBA (5).
This review examines the anatomy of the NMJ and the physiology
of neuromuscular transmission. The classification, pharmacology,
reversal, monitoring, associated complications, and guidelines
concerning NMBAs will also be reviewed. In addition, the use of
NMBAs in critically ill patients during six clinical situations
will be examined: emergency intubation, acute lung injury
(ALI)/acute respiratory distress syndrome (ARDS), status
asthmaticus, elevated ICP, elevated IAP, and therapeutic
hypothermia after out-of-hospital ventricular fibrillation
(VF)-associated cardiac arrest (1, 68). A com-puterized literature
search through MEDLINE and PubMed (January 1975September 2012) was
performed to identify observational and interventional studies
evaluating NMBAs for management of emergent/urgent intubation,
ALI/ARDS, status asthmaticus, elevated ICP, elevated IAP, and
therapeutic hypothermia. The following search terms were used:
NMBAs, neuromuscular blockers, paralytics, paralysis,
succinylcho-line, atracurium, cisatracurium, pancuronium,
rocuronium, vecuronium, critical care, intensive care, mechanical
ventila-tion, ALI, ARDS, status asthmaticus, ICP, traumatic brain
injury, IAP, abdominal compartment syndrome (ACS), thera-peutic
hypothermia, train-of-four (TOF), peripheral nerve stimulator,
monitoring, complications, DVT, corneal abrasions, anaphylaxis and
neuromuscular blockade, and reversal. We excluded articles
published in languages other than English.
ANATOMY/PHYSIOLOGY OF NEUROMUSCULAR TRANSMISSIONThere are three
major components involved in neuromuscular transmission: the
neuron, the neurotransmitter (acetylcho-line), and the muscle fiber
(9). Figure 1 depicts the relation-ship between these three major
components of the NMJ. The NMJ marks the location where the axonal
terminus lies in close
The Use of Neuromuscular Blocking Agents in the ICU: Where Are
We Now?
Steven B. Greenberg, MD1,2; Jeffery Vender, MD, MBA, FCCP,
FCCM1,2
1University of Chicago, Chicago, IL.2NorthShore University
HealthSystem, Evanston, IL.
Dr. Vendor consulted for Pharmadiem. Dr. Greenberg has disclosed
that he does not have any potential conflicts of interest.
For information regarding this article, E-mail:
[email protected]
Critical Care Medicine
0090-3493
10.1097/CCM.0b013e31828ce07c
41
5
00
00
2013
Copyright 2013 by the Society of Critical Care Medicine and
Lippincott Williams & Wilkins
DOI: 10.1097/CCM.0b013e31828ce07c
Esther
Concise Definitive ReviewSeries Editor, Jonathan E. Sevransky,
MD, MHS
-
Concise Definitive Review
Critical Care Medicine www.ccmjournal.org 1333
proximity to the muscle membrane. The motor unit comprises a
lower motor neuron and its associated innervated muscle. One nerve
has the capability of innervating over 100 muscle fibers in the
motor unit. Acetylcholine, a neurotransmitter, is produced and
stored in vesicles at the NMJ and then released into the synapse
once an action potential is generated (9, 10).
Once the action potential reaches the motor terminus, the
depolarization results in the release (in the presence of calcium)
of approximately 4 million molecules of acetylcholine into the NMJ.
Two acetylcholine molecules bind to a postsynaptic nico-tinic
receptor on the muscle resulting in an excitatory postsyn-aptic
end-plate potential. Once this endplate potential reaches its
threshold, it produces a muscle action potential that results in
muscle contraction. The muscle returns to its precontractile state
once acetylcholine is broken down by the enzyme,
ace-tylcholinesterase. The large amount of acetylcholine molecules
released in the NMJ acts as a protective mechanism to ensure muscle
contraction (911).
CLASSIFICATION OF NMBAs AND PHARMACODYNAMICSMuscle relaxants are
typically classified by their mechanism of action (depolarizing vs
nondepolarizing) and duration of action (short, intermediate, and
long acting). Table 1 depicts the pharmacokinetics,
pharmacodynamics, and data relating to dosing and mode of
administration of commonly used NMBAs in the ICU (1114).
Succinylcholine, the only avail-able depolarizing agent, binds to
acetylcholine receptors and causes persistent depolarization (10).
Succinylcholine pro-duces initial muscle fasciculations followed by
flaccid paralysis (10). It is frequently used for urgent or
emergent intuba-tion in the ICU. Nondepolarizing agents act as
competitive antagonists of nicotinic receptors, blocking the action
of ace-tylcholine (11). These nondepolarizing drugs can be further
divided into two groups, aminosteroids (i.e., pancuronium,
vecuronium, and rocuronium) and benzylisoquinoliniums (i.e.,
atracurium, cisatracurium, doxacurium, and mivacu-rium). Each drug
within these classifications has unique phar-macokinetic properties
(1113).
PharmacologyAltered Physiology During Critical Illness. Critical
illness is associated with altered physiology that may affect the
pharma-cokinetics of NMBAs. A lack of understanding or recognition
of these changes can result in clinical failures or adverse drug
events (15). This section will discuss how age, hypothermia, and
electrolytes/pH disturbances may alter the action of NMBAs.
Multiple factors may affect the pharmacokinetics of NMBAs in
critically ill patients. Age-related changes (i.e., reduction in
total body water, lean body mass, and serum albumin concen-tration)
may result in a reduction in the volume of distribution of NMBAs
(13). Increased age may contribute to a reduction in the rate of
drug elimination via decreases in cardiac output, glo-merular
filtration rate, and liver function (1215). Hypothermia may prolong
the duration of action of nondepolarizing NMBAs (16, 17). The
mechanisms underlying this prolongation include an altered
sensitivity of the NMJ, a reduction in acetylcholine mobilization,
decreased muscle contractility, reduced renal and hepatic
excretion, changes in drug volumes of distributions, and pH-related
changes at the NMJ (1618). Hypothermia may also slow the Hoffmann
elimination process and prolong the effect of both cisatracurium
and atracurium (1318).
Electrolyte and pH disturbances may alter the duration of action
of NMBAs. Hypokalemia may augment the block-ade induced by
nondepolarizing agents, while also reduc-ing the ability of
neostigmine (and other anticholinesterase reversal agents) to
reverse the blockade (12, 13). Magnesium prolongs the duration of
neuromuscular blockade by inhibit-ing calcium channels in the
presynaptic terminal and inhibit-ing postjunctional potentials.
Calcium triggers acetylcholine
Figure 1. Depicts the major components of the neuromuscular
junction: the neuron, acetylcholine, and the muscle. Acetylcholine
is stored in vesicles within the neuron. When an action potential
is generated, acetylcholine is released into the synapse in a
process called exocytosis. Acetylcholine binds to receptors on the
muscle cell to stimulate muscle contraction. (Reproduced with
permission from Bargmann C: Neurosciences: Genomics reaches the
synapse. Nature 2005; 436:473474.)
-
Greenberg and Vender
1334 www.ccmjournal.org May 2013 Volume 41 Number 5
release, and therefore, hypercalcemia may both reduce the
sen-sitivity to NMBA and decrease the duration of neuromuscular
blockade. The blockade effect of nondepolarizing agents may be
enhanced (although the mechanism is not clearly under-stood) by
both respiratory and metabolic acidosis (12, 13). Antagonism of
neuromuscular blockade by reversal agents may occur more slowly in
the presence of a respiratory acidosis or metabolic alkalosis (12,
13).
Organ Dysfunction and NMBAs. Aminosteroid NMBA pharmacokinetics
can be affected by liver dysfunction. Pan-curonium half-life is
prolonged in patients with cirrhosis because of its increased
volume of distribution (19). Similarly, vecuronium can also have a
prolonged elimination half-life, reduced clearance, and enhanced
blockade in the setting of cir-rhosis. However, the elimination and
clearance of vecuronium may not be altered in less severe forms of
liver disease (13). Severe hepatic dysfunction can also increase
the volume of dis-tribution of rocuronium, which will prolong its
elimination half-life and recovery time after reversal (13). Large
intubating
doses (1.2 mg/kg) or repeated doses of rocuronium in the
set-ting of severe liver disease typically prolong its effect
(13).
Aminosteroid NMBAs have variable durations of action in the
setting of severe renal disease (13, 19). Renal failure increases
elimination half-life and decreases clearance most significantly
for the long-acting aminosteroid muscle relaxants (i.e.,
pancuronium) (13). Vecuronium may have a prolonged effect due to
its active metabolite, 3-desacetyl vecuronium, which accumulates to
a significant degree with severe renal dis-ease (19). Rocuronium
can have an increased volume of distri-bution and decreased plasma
clearance in the setting of renal failure (21, 22). However, the
duration of action of repeated or single doses of rocuronium is
typically not affected by renal failure (13, 21, 22).
Benzylisoquinoliniums may be preferable in ICU patients as they
are not affected by renal or hepatic disease (13, 19). Hoffman
degradation (a nonenzymatic degradation) accounts for most of the
metabolism of both atracurium and cisatracurium (19). Cisatracurium
ICU infusion studies (> 24-hr duration) suggest
TABLE 1. Drug Information on the Commonly Used Neuromuscular
Blocking Agents in the ICU
NMBA Agent
NMBA Type
Pancuronium
A
Vecuronium
A
Rocuronium
A
Atracurium
B
Cisatracurium
B
Succinylcholine
D
Category (acting)
Long acting Intermediate Intermediate Intermediate Intermediate
Short
Time to maximal blockade (min)
23 34 12 35 23 < 1
Duration of action (min)
60100 2035 2035, 6080 with rapid sequence dose
2035 3060 510
Dose
Bolus 0.050.1 mg/kg 0.080.1 mg/kg 0.61 mg/kg (11.2 mg/ kg for
rapid sequence)
0.40.5 mg/kg 0.l0.2 mg/kg 1 mg/kg, dose higher in pediatrics
Continuous infusion dosing
0.81.7 mcg/ kg/min
0.81.7 mcg/ kg/min
812 mcg/ kg/min
520 mcg/ kg/min
13 mcg/kg/ min
Infusions no longer used commonly
Elimination 4570% renal, 1015% hepatic
50% renal, 3550% hepatic
33% renal, < 75% hepatic
510% renal, Hoffman elimination
510% renal, Hoffman elimination
Plasma cholinesterase
Active metabolites
3-OH and 17-OH pancuronium
3-Desacetyl- Vecuronium
None None (toxic metabolite- laudanosine)
None None
Side effects Vagal blockade, sympathetic stimulation, blocks
muscarinic stimulation (bradycardia)
Vagal blockade at higher doses
Vagal blockade at higher doses, weakly blocks muscarinic
stimulation (bradycardia)
Histamine release, minimal ganglionic blockade
None Minimal amount of histamine release, muscarinic stimulation
(bradycardia)
NMBA = neuromuscular blocking agent, A = aminosteroid, B =
benzylisoquinolinium, D = depolarizing agent.Information taken from
references 1526.
-
Concise Definitive Review
Critical Care Medicine www.ccmjournal.org 1335
that there is marginal accumulation of the drug. Several
stud-ies suggest that the duration of action of cisatracurium is
not affected by organ dysfunction (23). Laudanosine, a metabolite
of atracurium, has central nervous system stimulating effects.
Laudanosine levels have been reported to increase when using
long-term atracurium infusions but are typically not high enough to
promote seizure activity in humans (13, 19, 23).
Drug Interactions and NMBAs. Drug interactions may also alter
the duration of action of NMBAs. Table 2 depicts some of the more
common effects of drugs on neuromus-cular blockade. Certain
antibiotics (i.e., aminoglycosides, clindamycin, and tetracycline)
prolong the duration of NMBAs (24). Furosemide, calcium channel
blockers, local anesthetics, and inhaled anesthetics can also
potentiate neuromuscular blockade. Patients on chronic
antiepileptic medications are typically resistant to aminosteroid
NMBAs. This phenomenon may be due to increase clearance of
these
NMBAs, an increase in binding to -1 acid glycoproteins, or an
up-regulation of acetylcholine receptors. Participa-tion by a
clinical pharmacist in the multidisciplinary ICU daily rounds
coupled with the use of close neuromuscular monitoring may help
prevent unwanted prolongation or reduction in neuromuscular
blockade produced by drug interactions (1, 13, 24).
Reversal AgentsAnticholinesterase reversal agents (neostigmine,
edropho-nium, or pyridostigmine) are only effective for
nondepolariz-ing blockers and increase acetylcholine at the NMJ to
reduce residual neuromuscular blockade (25). The duration of
ace-tylcholinesterase inhibition is longer with pyridostigmine and
neostigmine when compared with edrophonium, due to a strong
covalent bond interaction between these two drugs and
acetylcholinesterase (26, 27).
TABLE 2. Drug Interactions and Neuromuscular Blocking Agents
Drug Method
Causes resistance to NMB
Phenytoin Up-regulation of acetylcholine-R
Ranitidine Unknown
Carbamazepine Competes for acetylcholine receptors
Theophylline, caffeine Unknown
Calcium Antagonizes potentiating effect of magnesium on
neuromuscular blockade
Prolongs NMB
Inhaled anesthetics Reduced postjunctional receptor sensitivity
to acetylcholine
Magnesium Competes with calcium presynaptically
Potassium Low potassium enhances blockade and reduces ability of
reversal by antagonists
Lithium Activation of potassium channels presynaptically
Immunosuppressant
Corticosteroids May decrease sensitivity of endplate to
acetylcholine
Cyclosporine May inhibit neuromuscular blocking agent
metabolism
Cardiovascular Reduces prejunctional acetylcholine release and
decreases muscle contractility
Furosemide
-blockers and calcium channel blockers
Procainamide
Quinidine
Antibiotics Reduces prejunctional acetylcholine release,
decreases postjunctional receptor sensitivity to acetylcholine,
blocks acetylcholine receptors, or disrupts ion channels
Aminoglycosides
Tetracyclines
Clindamycin
Vancomycin
NMB = neuromuscular blocker.Information produced from references
(15, 16, 23, 24).
-
Greenberg and Vender
1336 www.ccmjournal.org May 2013 Volume 41 Number 5
Concomitant use of antimuscarinics (glycopyrrolate or atropine)
with anticholinesterases is recommended to coun-teract side effects
of increasing acetylcholine at muscarinic sites (i.e., bradycardia,
bradyarrhythmias, increased secretions, and bronchoconstriction)
(26, 27). Atropine (0.0050.01 mg/kg) is typically used with
edrophonium (0.51.5 mg/kg) as they both have similar onsets of
action (27). Glycopyrrolate (0.0070.015 mg/kg) is used to
counteract the cholinergic effects of neostigmine (0.040.07 mg/kg).
Alternatively, 0.2 mg of glycopyrrolate (IV) for each 1.0 mg of
neostigmine or 5.0 mg of pyridostigmine can be given (27).
Clinicians should recognize that muscle weakness can occur when
anticholinesterases are given to patients with full neu-romuscular
recovery (2529). Clinical studies have demon-strated that
administration of anticholinesterases in the setting of near
complete neuromuscular recovery (TOF 0.9) resulted in a decrease in
minute ventilation, upper airway muscle tone, and diaphragmatic
function (28, 29).
Newer drugs that selectively encapsulate aminosteroid
non-depolarizing agents (sugammadex-a modified A-cyclodextrin)
provide more rapid reversal of aminosteroid NMBAs (3034).
Sugammadex acts by forming tight complexes with these agents.
Plasma steroidal neuromuscular blockers are quickly removed. The
subsequent drop in plasma aminosteroid agent concentration produces
a concentration gradient that allows for more aminosteroid to move
from the NMJ into plasma. This remaining NMBA rapidly forms
inactive complexes with the available plasma sugammadex (30).
Sugammadex is cur-rently not available in the United States (but is
available in Europe), nor has it been tested in the critically ill
(3034). However, it may allow for the use of steroidal agents for
urgent/emergent intubation in those patients in which
succinylcho-line administration is contraindicated (see
urgent/emergent intubation section). Furthermore, it may serve as a
life-saving measure in those patients who receive aminosteroidal
agents for intubation and who cannot be ventilated or intubated.
Ongoing investigations may also address whether sugamma-dex can be
used to reliably mitigate aminosteroid agent-asso-ciated
anaphylaxis (35). Studies are warranted to validate its clinical
use in the ICU.
MonitoringRepeated clinical, qualitative, and quantitative
evaluation of the depth of neuromuscular blockade may result in a
reduction of NMBA dose and a subsequent decrease risk of
complica-tions from residual neuromuscular blockade (36).
Intensivists may look to achieve the absence of spontaneous
ventilation to improve patient-ventilator synchrony. Clinical signs
(such as the presence of spontaneous ventilation, eye opening,
sus-tained hand grip, leg lift, or sustained 5-s head lift), used
alone to determine the extent of muscle relaxation, are poor
deter-minants in predicting the presence of residual neuromuscular
blockade (37). In addition, these signs are not useful in those
patients who are uncooperative.
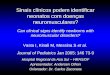
Peripheral nerve stimulators can facilitate appropriate
titra-tion of NMBAs (94). TOF monitoring is the primary
qualitative
method used for assessment of neuromuscular blockade and
involves four supramaximal electrical impulses every 0.5 sec-onds
applied to the ulnar, facial, or posterior tibial nerve (1, 13).
Figure 2 depicts a peripheral nerve stimulator eliciting a TOF
response. Stimulation of these nerves will produce four visualized
muscle twitches from the associated muscles (typi-cally muscles of
the thumb or eye) that are innervated by the nerves. Fade of the
twitch response occurs with increasing neuromuscular blockade (37)
(Fig. 2C). Evaluation of fade can be performed by comparing the
strength (TOF ratio) of the fourth twitch to that of the first
twitch (25, 37).
Several factors play a role in the assessment of TOF
moni-toring. The loss of electrode skin adhesion, incorrect
electrode placement, peripheral edema, and hypothermia (dampens
peripheral stimulator twitch responses) can all contribute to
inaccuracies in interpreting the TOF response (37, 38). TOF
monitoring coupled with clinical evaluation has been shown to be
insensitive for predicting residual neuromuscular weakness (25,
37). Patients with residual neuromuscular weakness can
On/Off
DBS Sustainedtetanus
Train- of-Four
SingleTwitch
- mA+
2a. TOF pattern (0.5 seconds each)
2b. Response in absence of NMB
2c. Response with partial NMB
Figure 2. Depicts a peripheral nerve stimulator applied to
stimulate the ulnar nerve and the train-of-four (TOF) stimulation
pattern with no neu-romuscular blockade (NMB) and partial blockade.
A, TOF pattern (0.5 s each). B, Response in absence of NMB. C,
Response with partial NMB. DBS = double burst suppression.
-
Concise Definitive Review
Critical Care Medicine www.ccmjournal.org 1337
present with difficulty swallowing, rapid shallow breathing,
nasal flaring, and overuse of accessory muscles (39). Studies
suggest that residual neuromuscular blockade may lead to
postoperative complications, including aspiration, atelectasis,
pneumonia, and acute respiratory failure (25, 3740).
Quantitative neuromuscular monitoring allows clini-cians to both
stimulate the peripheral nerve and quantify the response to nerve
stimulation (37). These devices are not rou-tinely used in the ICU.
Acceleromyography is available and has been used in the operating
room (37). Acceleromyography modules have been integrated in some
bedside monitoring systems and can be used in the operating room
and ICU. Figure 3 depicts how this monitor is applied on the
patient. This device may help reduce signs and symptoms of residual
neuromuscular weakness along with respiratory complica-tions
(hypoxemia and airway obstruction) (41, 42). Research is needed
regarding quantitative monitoring and its utiliza-tion in the
ICU.
A limited number of studies demonstrate a significant clini-cal
benefit of neuromuscular monitoring for ICU patients (43, 44). An
early open-label study using qualitative neuromuscular monitoring
and adequate sedation showed that ICU patients did not experience
prolonged paralysis, weakness, or other neuromuscular sequelae
(45). Rudis et al (46) observed that neuromuscular monitoring
decreased the amount of drug per hour, reduced the total drug used,
and improved recovery time from neuromuscular blockade. Follow-up
studies using a similar comparison with either atracurium or
cisatracurium did not find this positive effect (47, 48). A more
recent double-blinded randomized trial in a pediatric ICU found
that neuro-muscular monitoring did not eliminate prolonged recovery
in patients on vecuronium infusions (49). Trials are warranted to
determine which patient populations will derive benefits from
neuromuscular monitoring.
NMBAs AND ASSOCIATED COMPLICATIONS
ICU-Acquired WeaknessThe causes for ICU-acquired skeletal muscle
weakness (ICU-AW) remain controversial. ICU-AW is classified as
critical ill-ness polyneuropathy, critical illness myopathy, or
critical illness neuromyopathy based on different
electrophysiologic test find-ings (43, 50, 51). Proposed mechanisms
for ICU-AW include disturbances in the microcirculation, protein
malnutrition, systemic inflammation, and prolonged immobility (43,
50).
More than 40 case reports have implicated NMBAs as a possi-ble
cause for ICU-AW (43, 52, 53). However, there is a paucity of
well-designed trials that confirm this relationship (43). The
exist-ing studies examine a heterogeneous critically ill patient
popu-lation and are methodologically compromised by variability in
data collection (43). Other proposed risk factors, such as the use
of high-dose corticosteroids, hyperglycemia, variation in age among
studied populations, amount of sedation used, and type and duration
of NMBAs administration, were not consistently controlled (43, 50,
51). Inconsistent use of electrophysiologic and manual muscle
testing complicates interpretation of the pub-lished studies. Some
investigators have suggested that these tests do not correlate with
muscle function or outcome (43, 50, 51).
Two recent trials did not identify an increased prevalence of
ICU-AW in ARDS patients administered a 48-hour cisatracu-rium
infusion (54, 55). Future investigations should examine the impact
of other factors associated with ICU-AW, such as corticosteroids,
sedation use, type and duration of NMBAs, or immobility. Trials
should be performed on additional popu-lations (non-ARDS) to
investigate whether limited use of NMBAs is associated with ICU-AW
(43).
Awareness During Induced ParalysisA recent case series reported
11 ICU patients who had been aware during pharmacologic paralysis
(56). The common themes reported were thoughts of life and death,
weird dreams, fear, and resisting being tied down. It is imperative
to achieve a deep sedative state with sedatives and analgesics
prior to the initiation of an NMBA to mitigate the risk of
awareness. The authors suggest that strict adherence to sedation
guidelines and protocols may facilitate appropriate titration of
drugs while reducing awareness during paralysis. They also
recom-mended that monitors should be developed to help clinicians
appropriately titrate NMBAs, sedatives, and hypnotics as seda-tion
titration protocols are not adequate enough to eliminate awareness
(5661).
No continuous bedside monitor has been universally used to alert
clinicians of the potential for awareness. Processed
electro-encephalogram models, such as the bispectral index (BIS
mon-itor-Aspect Medical Systems, Covidien, Mansfield, MA), have
been introduced into ICUs that may quantitatively monitor the level
of consciousness (62). A recent ICU study suggested a satisfactory
correlation between BIS values and validated sedation scales (63),
whereas others have refuted it (6265). Well-designed clinical
trials are needed to validate a correlation between sedation scales
and continuous bedside monitors.
Piezoelectric sensor
Figure 3. Illustration of how the hand-held acceleromyography
device is applied to a patient. This device stimulates the ulnar
nerve producing thumb movement. A piezoelectric sensor is fixed
onto the thumb and senses the acceleration of thumb movement. This
acceleration is then sensed by the displayed monitor.
-
Greenberg and Vender
1338 www.ccmjournal.org May 2013 Volume 41 Number 5
DVT and Corneal AbrasionsNMBA administration to ICU patients may
lead to nosocomial complications, such as DVT and corneal
abrasions. Immobil-ity achieved by paralysis increases stasis of
flow leading to an increase in DVT rate (66). A recent study
reported that the use of NMBAs is the strongest predictor for the
development of ICU-related DVTs (67). The same trial reported that
educa-tional initiatives to promote DVT prophylaxis (both
mechani-cal and pharmacologic) significantly reduced the prevalence
of DVTs (67). Closer neuromuscular monitoring coupled with
protocols to guide titration of NMBAs may also contribute to
reducing the DVT prevalence by reducing the time to recovery from
neuromuscular blockade (67).
NMBAs also increase the risk of corneal abrasions in criti-cally
ill patients. Paralysis abolishes eyelid closure and the blink
reflex, which may result in cornea drying, scarring, ulceration,
and infection (66). The prevalence of corneal abrasions in the
adult critically ill varies from 8% to 60%, depending on the study
design (68). Prophylactic eye protection (i.e., artificial
ointments, eye covers, or methylcellulose drops) may reduce the
prevalence of this ophthalmic complication (68).
AnaphylaxisAllergic reactions associated with NMBAs are
typically IgE-mediated (69). The ammonium ion in many NMBAs is the
likely allergic component, which is also seen in many com-mon
household products. Patients may develop anaphylaxis after the
first dose of NMBA due to cross reactivity with other inciting
agent exposures. Seven consecutive large French sur-veys over an
18-year period suggested that NMBAs are the most frequent
perioperative agents (more than sedatives, hypnotics, latex,
antibiotics, and colloids) involved in allergic reactions (70,
71).
A diagnostic approach to suspected cases of anaphylaxis may
include the following: obtaining a detailed medical his-tory,
observing clinical signs (under deep sedation-pulseless-ness,
oxygen desaturation, bronchospasm, and difficulty in ventilating),
performing mediator release assays at the time of the reaction
(i.e., tryptase levels), quantifying specific IgE immediately or
during the first 6 months after the event, and performing skin
tests and other biologic assays, such as hista-mine release tests
or basophil activation (69, 71). The mainstay for diagnosis is the
combination of obtaining the appropri-ate history with skin
testing. Skin prick (SPT) or intradermal testing (IDT) are
typically performed within 6 weeks of the reaction. Skin tests for
NMBA usually remain positive for years following the exposure.
Control testing (with saline) should be performed to ensure an
accurate result. Skin testing has a high reported sensitivity
(9497%) (69). SPT is preferred when investigating an NMBA
anaphylactic reaction, whereas IDT is recommended to investigate a
cross reaction (69, 71).
GuidelinesCritical Care Medicine published ICU guidelines in
2002 stat-ing that NMBAs should be used for an adult patient in an
ICU to manage ventilation, manage increased ICP, treat muscle
spasms, and decrease oxygen consumption only when all other
means have been tried without success (Grade C recommen-dation)
(72). Both clinical and TOF monitoring was also rec-ommended (Grade
B) so that the least amount of drug is used for the shortest
duration (72). Guidelines have been developed for the titration of
sedation and analgesics (7376). Clinicians should evaluate the
reason for (at least daily) and depth of neu-romuscular blockade
(continuously) so that mobility may be achieved faster, which may
decrease the prevalence of delirium, increase functional
independence, and increase ventilator-free days (77, 78).
NMBA ICU Applications: Urgent/Emergent IntubationSuccinylcholine
(11.5 mg/kg) is typically used to establish control of the airway
to reduce the risk of aspiration due to its rapid onset (3060 s)
and short duration of action (510 min) (79, 81). A 2008 Cochrane
Database meta-analysis (37 stud-ies included) suggested that
succinylcholine administration was associated with superior
intubating conditions when compared with rocuronium (82). When
rocuronium (1.2 mg/kg) was used, it was associated with similar
intubating con-ditions when compared with succinylcholine. However,
suc-cinylcholine was still reported to be clinically superior due
to its shorter duration of action (82). A more recent randomized
controlled trial in the ICU compared rocuronium (0.6 mg/kg) with
succinylcholine (83). This trial suggested that there was no
difference between the two drugs with regard to intubating
conditions, prevalence and severity of oxygen desaturations, and
prevalence of failed intubation attempts (83). Succinyl-choline
should be avoided in the following clinical conditions where its
depolarizing effect can cause a substantial increase in
extracellular potassium: sustained muscle weakness, prolonged
immobility, massive trauma with significant muscle injury, severe
abdominal infections, concomitant acidosis and severe hypovolemia,
or burns. Patients with renal failure can develop an increase in
plasma potassium (approximately 0.5 mEq/L1 mEq/L) with use of
succinylcholine, and therefore, it is rela-tively contraindicated
in these patients (7981).
Nondepolarizing NMBAs are the alternatives to succinyl-choline
for endotracheal intubation. High-dose rocuronium (11.2 mg/kg) is
commonly used for rapid intubation due to its relative short onset
(12 min) of action (79). However, the duration of action is much
longer with this dose (approxi-mately 6080 min) when compared with
the standard intubating dose of rocuronium 0.6 mg/kg (2035 min).
Rocuronium has a significant longer duration of action when
compared with succinylcholine, and therefore, it may not be the
appropriate drug for an anticipated difficult intuba-tion or mask
ventilation as hypoxemia may occur (79, 82). Caution should also be
used in patients with aminosteroid allergies (anaphylaxis has been
reported with rocuronium) (71). Cisatracurium may be advantageous
for intubation in patients with both liver and renal dysfunction.
However, its onset of action is longer than rocuronium and its
duration of action is comparable or somewhat longer than
rocuronium. This does not make it an ideal drug for securing the
airway
-
Concise Definitive Review
Critical Care Medicine www.ccmjournal.org 1339
emergently (47, 81). A recent study investigated the use of
NMBAs for emergent endotracheal intubation in 566 patients from two
major tertiary care centers (84). The use of NMBAs was associated
with an improvement in intubating condi-tions and a reduction in
both the prevalence of hypoxemia and procedure-related
complications (aspiration, traumatic intubation, esophageal
intubation, dental injury, and endo-bronchial intubation) (84).
ALI/ARDSALI/ARDS is managed by treating the underlying cause of
respiratory failure while reducing the risk of ventilator-induced
lung injury (6, 85, 86). Induction of paralysis may increase chest
wall compliance, eliminate patient-ventilator dyssynchrony,
facilitate lung recruitment, reduce inflam-matory mediator release,
decrease lung hyperinflation, and reduce oxygen consumption (albeit
controversial) (6, 87). At least eight clinical trials have
assessed the use of NMBAs for managing ALI/ARDS (Table 3) (1). Two
small observational trials in ALI/ARDS patients prior to the year
2000 reported no effect on oxygenation when using a pancuronium
bolus (88, 89). A large retrospective study by Arroliga et al (3)
in
2005 noted that 13% of patients were administered NMBAs for at
least 1 day. NMBA use was associated with prolonged duration of
mechanical ventilation, ICU length of stay, and an increase in
mortality (3). A small randomized crossover trial in severe sepsis
patients reported that oxygen consumption or delivery was not
improved in patients randomized to receive NMBAs (90).
Short-term use of cisatracurium in patients with ALI/ARDS has
been associated with beneficial outcomes. Two small ran-domized
controlled trials using cisatracurium in patients with ARDS
demonstrated an improvement in oxygenation (91, 92). Another
randomized trial in ARDS patients demonstrated that the early use
of cisatracurium for 48 hours improved oxy-genation and reduced
concentrations of pulmonary inflam-matory mediators (54). A larger
multicenter trial in patients with severe ARDS (PaO
2/FIO
2 < 150 mm Hg) reported that
early administration of cisatracurium for 48 hours increased
adjusted 90-day survival, ventilator-free days, organ failurefree
days, and reduced barotrauma (55). Further studies are required to
define the appropriate combination of sedation and NMBAs and to
identify when NMBA use will improve outcomes in patients with
ALI/ARDS.
TABLE 3. Use of Neuromuscular Blocking Agents for Acute
Respiratory Distress Syndrome in the ICU
Citation Study Design NMBA Regimen Conclusions
Papazian et al (54) RCT (n = 340), severe ARDS Cisatracurium
infusion 48 hr vs placebo
Improved adjusted 90-d survival (p = 0.04), increased
ventilator-free days (p = 0.03), increased organ dysfunctionfree
days (p = 0.01), decreased barotrauma (p = 0.03)
Arroliga et al (7) Retrospective (n = 549), ALI/ARDS
High PEEP group, 45% had NMBA; low PEEP group, 33% had NMBA
No difference in 60-d mortality or length of mechanical
ventilation
Forel et al (55) RCT (n = 36), ARDS Cisatracurium infusion 48 hr
vs placebo
Significant reduction in pulmonary/systemic cytokines (p =
0.005, p = 0.04) and increased oxygenation (p < 0.001)
Arroliga et al (3) Retrospective (n = 5183), patient with
mechanical ventilation 12 hr
13% of patients given NMBA
Significant increase in ICU mortality (p < 0.001), duration
of mechanical ventilation (p < 0.001), and ICU length of stay (p
< 0.001)
Gainnier et al (91) RCT (n = 56), severe ARDS Cisatracurium
infusion 48 hr vs placebo
Improvement in oxygenation (p = 0.021), decrease in FIO2 (p <
0.001), and decrease in PEEP (p = 0.036)
Lagneau et al (92) RCT (n = 102), ARDS Cisatracurium (2-hr
infusion) used train-of-four to titrate NMBA
Increase in oxygenation in groups with NMBA (p = 0.0014)
Conti et al (89) Prospective, open label (n = 13); ALI/ARDS
1 bolus-pancuronium No difference in oxygenation
Bishop (88) Prospective, open label (n = 9); ALI/ARDS
1 bolus-pancuronium No difference in oxygenation
NMBA = neuromuscular blocking agent, RCT = randomized controlled
trial, ALI = acute lung injury, ARDS = acute respiratory distress
syndrome, PEEP = positive end-expiratory pressure.
-
Greenberg and Vender
1340 www.ccmjournal.org May 2013 Volume 41 Number 5
Status AsthmaticusNMBAs are used sparingly for patients with
status asthmati-cus to minimize ventilator asynchrony, lung
hyperinflation, and barotrauma (44). Table 4 presents several
trials examin-ing NMBA use in patients with status asthmaticus.
ICU-AW is reported in this population (93) and appears to be more
commonly associated with the use of concomitant high-dose steroids
(9498). A recent retrospective study in mechani-cally ventilated
patients with status asthmaticus suggested that patients who
require deep sedation with persistent immobiliza-tion are still at
risk for weakness, despite a decline in the dura-tion of induced
paralysis (97). The risk of prolonged weakness may be reduced by
using the minimal doses of sedation, corti-costeroids, and NMBAs
required to achieve the desired effect and to withdraw these drugs
as soon as possible (97, 98).
Increased ICPNMBAs are typically reserved for patients with
intracranial hypertension in whom sedation alone does not reduce
ICP
(99). Few studies have evaluated the use of NMBAs for the
management of elevations in ICP due to coughing, suctioning, or
movement (100107) (Table 5). Hsiang et al (100) suggested that
while NMBAs may reduce mortality, they may increase severe
disability. The routine use of NMBAs for elevated ICP does not
appear to be indicated at this time (106, 107). Patients who
receive extended neuromuscular blockade as a second tier therapy
for elevated ICP can be monitored with peripheral nerve stimulation
to potentially avoid unwanted side effects (see Monitoring section)
(99).
Increased IAPIntra-abdominal hypertension (IAH) is defined as a
repeated elevation in IAP of at least 12 mm Hg (108110). ACS is
defined as continued IAH of greater than 20 mm Hg with end-organ
dysfunction or failure (109, 110). Reduced abdominal wall
compliance due to third spaced fluids, tense abdominal closures,
and pain or inadequate sedation can lead to further increases in
IAPs and subsequent organ failure (110). NMBAs
TABLE 4. Use of Neuromuscular Blocking Agents for Status
Asthmaticus in ICU
Author Study Design% of patient receiving NMBA Results
Kesler et al (97) Retrospective (n = 170) 67% before 1995, 77%
after 1995
No statistically significant difference in weakness between NMBA
group and sedation-only group
Adnet et al (96) Retrospective (n = 118) 54% Higher prevalence
of muscle weakness, longer mechanical ventilation, longer ICU stay,
and increase prevalence of pneumonia in NMBA group
Behbehani et al (130) Retrospective (n = 86) 35% Increase
myopathies with NMBAs
Leatherman et al (94) Retrospective (n = 107) 65% Increase
prevalence of muscle weakness with steroids + NMBAs, but no
increase muscle weakness with use of benzylisoquinoliniums
Griffin et al (131) Case series (n = 3), reviewed (n = 18) case
reports
100% All patients received both steroids and steroidal NMBA and
all patients developed severe muscle weakness
NMBA = neuromuscular blocking agent.
TABLE 5. The Use of Neuromuscular Blocking Agents in
Neurointensive Care
Author Study Design% of NMBA Used or Type of NMBA Results
Schramm et al (103) Randomized controlled trial (n = 14),
neurosurgery
Cisatracurium or atracurium bolus
Atracurium-transient decrease in ICP, MAP, CPP, CBF;
cisatracurium, no effect on MAP, ICP, CPP, CBF
Schramm et al (101) Prospective, open label (n = 24)
Cisatracurium bolus No effect on MAP, ICP, CPP, CBF
Prielipp et al (102) Prospective, open label (n = 6)
Doxacurium bolus and infusion
No effect on MAP, ICP, no prolonged weakness
Hsiang et al (100) Retrospective (n = 514) traumatic brain
injury
NMBA used in < 50% patients
Decrease mortality with NMBA but increase prevalence of severely
disabled patients, pneumonia, and ICU stay
NMBA = neuromuscular blocking agent, ICP = intracranial
pressure, MAP = mean arterial pressure, CPP = cerebral perfusion
pressure, CBF = cerebral blood flow.
-
Concise Definitive Review
Critical Care Medicine www.ccmjournal.org 1341
have been reported to improve elevated IAPs by reducing
abdominal muscle tone (110113).
Neuromuscular blockade may provide clinicians with more time to
remove fluid or treat the underlying cause of IAH and avoid
surgical decompression (113115). Table 6 presents a few studies
examining the use of NMBA in the treatment of IAH. A small
prospective trial suggested that a bolus dose of cisatracu-rium was
effective in significantly decreasing mild elevations in IAP (111).
A recent case report describing a patient undergoing adrenalectomy
who had ACS reported that a prolonged NMBA infusion of 48 hours was
effective in reducing IAPs and provid-ing a good recovery (114). It
has been recommended (Grade 2C) by the International ACS Consensus
Definitions Conference Committee that NMBAs can be used in selected
patients to reduce mild-to-moderate elevations of IAP (109,
110).
Therapeutic Hypothermia After Out-of-Hospital VF-Associated
Cardiac ArrestIn 2002, two landmark trials demonstrated that using
mild hypothermia (3234 C) for 1224 hours in unconscious patients
after out-of-hospital VF cardiac arrest improved neu-rologic
outcomes, with one trial suggesting a survival benefit (116, 117).
This therapy has been validated in other random-ized studies and
meta-analyses (8, 118127). NMBAs were primarily used to prevent
shivering (8, 116, 117) in the two original trials (and
others).
The optimal combination of sedatives, analgesics, and paralytics
during hypothermia after VF-associated cardiac arrest is unknown.
Chamorro et al (127) performed a sys-tematic review of 44 studies
(68 international ICUs, primar-ily European) examining intensivists
preferences for the administration of sedatives, analgesics, and
NMBAs during therapeutic hypothermia after VF cardiac arrest. A
significant variability in the protocolized use of all medications
for these patients was found. Fifty-four ICUs routinely used NMBAs
to prevent shivering, whereas eight ICUs used NMBAs to treat
shivering (127). Pancuronium was the primary agent used in 24
international ICUs surveyed, whereas cisatracurium was the second
most common agent used. A minority of ICUs used neuromuscular
monitoring to guide NMBA dosing and therapy (127). Studies are
required to elucidate the optimal type, dose, and mode of
administration of NMBAs, as well
as optimal combination of sedatives and analgesics in this
patient population (128, 129).
CONCLUSIONIntensivists use NMBAs for a variety of clinical
conditions. Constant review and exploration of pharmacology,
dosing, drug interactions, and monitoring techniques may reduce the
unwanted side effects of NMBAs. Adoption of a collabora-tive ICU
team effort coupled with the use of evidence-based guidelines may
improve patient outcomes when using NMBAs. These measures may
ensure that NMBAs are used and moni-tored appropriately.
REFERENCES 1. Warr J, Thiboutot Z, Rose L, et al: Current
therapeutic uses, pharma-
cology, and clinical considerations of neuromuscular blocking
agents for critically ill adults. Ann Pharmacother 2011;
45:11161126
2. Merriman HM: The techniques used to sedate ventilated
patients. A survey of methods used in 34 ICUs in Great Britain.
Intensive Care Med 1981; 7:217224
3. Arroliga A, Frutos-Vivar F, Hall J, et al; International
Mechanical Ven-tilation Study Group: Use of sedatives and
neuromuscular blockers in a cohort of patients receiving mechanical
ventilation. Chest 2005; 128:496506
4. Mehta S, Burry L, Fischer S, et al; Canadian Critical Care
Trials Group: Canadian survey of the use of sedatives, analgesics,
and neuromuscular blocking agents in critically ill patients. Crit
Care Med 2006; 34:374380
5. Rhoney DH, Murray K: National survey of the use of sedating
drugs, neuromuscular blocking agents and reversal agents in the
intensive care unit. J Intensive Care 2003; 18:139145
6. Raoof S, Goulet K, Esan A, et al: Severe hypoxemic
respiratory failure: Part 2nonventilatory strategies. Chest 2010;
137:14371448
7. Arroliga AC, Thompson BT, Ancukiewicz M, et al; Acute
Respiratory Distress Syndrome Network: Use of sedatives, opioids,
and neuro-muscular blocking agents in patients with acute lung
injury and acute respiratory distress syndrome. Crit Care Med 2008;
36:10831088
8. Bernard SA, Buist M: Induced hypothermia in critical care
medicine: A review. Crit Care Med 2003; 31:20412051
9. Fagerland MJ, Erikkson LI: Current concepts in neuromuscular
trans-mission. Br J Anaesth 2009; 103:108114
10. Jonsson M, Dabrowski M, Gurley DA, et al: Activation and
inhibition of human muscular and neuronal nicotinic acetylcholine
receptors by succinylcholine. Anesthesiology 2006; 104:724733
11. Jonsson Fagerlund M, Dabrowski M, Eriksson LI:
Pharmacological characteristics of the inhibition of
nondepolarizing neuromuscular blocking agents at human adult muscle
nicotinic acetylcholine recep-tor. Anesthesiology 2009;
110:12441252
TABLE 6. Studies Involving Neuromuscular Blocking Agent and
Intra-Abdominal Hypertension
Author Study Design NMBAs Results
Cheatham et al (132) Prospective observational study (n =
478)
Used combined medical/surgical management algorithm which
contained the use of NMBA
Increased patient survival to hospital discharge from 50% to 72%
(p = 0.15)
Davies et al (114) Case report (n = 1) Atracurium infusion 48 hr
Reduced IAP and provided good recovery with discharge at 12 d
postoperatively
De Waele et al (111) Case series (n = 10) Cisatracurium bolus
9/10 patients had reduction in IAP
NMBA = neuromuscular blocking agent, IAP = intraabdominal
pressure.
-
Greenberg and Vender
1342 www.ccmjournal.org May 2013 Volume 41 Number 5
12. McManus MC: Neuromuscular blockers in surgery and intensive
care, part I. Am J Health Syst Pharm 2001; 58:22872299
13. Miller R: Miller: Millers Anesthesia. Second Edition.
Orlando, FL, Churchill Livingstone, 2009
14. Murphy GS, Vender J: Neuromuscular blocking agents use and
mis-use in the intensive care unit. Crit Care Clin 2001;
17:925942
15. Smith BS, Yogaratnam D, Levasseur-Franklin KE, et al:
Introduction to drug pharmacokinetics in the critically ill
patient. Chest 2012; 141:13271336
16. Caldwell JE, Heier T, Wright PM, et al:
Temperature-dependent phar-macokinetics and pharmacodynamics of
vecuronium. Anesthesiology 2000; 94:8392
17. Smeulers NJ, Wierda JM, van den Broek L, et al: Effects of
hypo-thermic cardiopulmonary bypass on the pharmacodynamics and
pharmacokinetics of rocuronium. J Cardiothorac Vasc Anesth 1995;
9:700705
18. Beaufort AM, Wierda JM, Belopavlovic M, et al: The influence
of hypothermia (surface cooling) on the time-course of action and
on the pharmacokinetics of rocuronium in humans. Eur J Anaesthesiol
Suppl 1995; 11:95106
19. Atherton DP, Hunter JM: Clinical pharmacokinetics of the
newer neu-romuscular blocking drugs. Clin Pharmacokinet 1999;
36:169189
20. Magorian T, Wood P, Caldwell J, et al: The pharmacokinetics
and neuromuscular effects of rocuronium bromide in patients with
liver disease. Anesth Analg 1995; 80:754759
21. Szenohradszky J, Fisher DM, Segredo V, et al:
Pharmacokinetics of rocuronium bromide (ORG 9426) in patients with
normal renal func-tion or patients undergoing cadaver renal
transplantation. Anesthesi-ology 1992; 77:899904
22. Cooper RA, Maddineni VR, Mirakhur RK, et al: Time course of
neuro-muscular effects and pharmacokinetics of rocuronium bromide
(Org 9426) during isoflurane anaesthesia in patients with and
without renal failure. Br J Anaesth 1993; 71:222226
23. Boyd AH, Eastwood NB, Parker CJ, et al: Comparison of the
phar-macodynamics and pharmacokinetics of an infusion of
cis-atracurium (51W89) or atracurium in critically ill patients
undergoing mechani-cal ventilation in an intensive therapy unit. Br
J Anaesth 1996; 76:382388
24. Tatro DS (Ed): Non-depolarizing muscle relaxants. In: Drug
Interaction Facts. St Louis, MO, Wolters Kluwer, 2010, pp
12311253
25. Murphy GS, Brull SJ: Residual neuromuscular block: Lessons
unlearned. Part II: Methods to reduce the risk of residual
weakness. Anesth Analg 2010; 111:129140
26. Caldwell JE: Clinical limitations of acetylcholinesterase
antagonists. J Crit Care 2009; 24:2128
27. Bevan DR, Donati F, Kopman AF: Reversal of neuromuscular
block-ade. Anesthesiology 1992; 77:785805
28. Eikermann M, Zaremba S, Malhotra A, et al: Neostigmine but
not sugammadex impairs upper airway dilator muscle activity and
breath-ing. Br J Anaesth 2008; 101:344349
29. Eikermann M, Fassbender P, Malhotra A, et al: Unwarranted
adminis-tration of acetylcholinesterase inhibitors can impair
genioglossus and diaphragm muscle function. Anesthesiology 2007;
107:621629
30. de Boer HD, van Egmond J, van de Pol F, et al: Sugammadex, a
new reversal agent for neuromuscular block induced by rocuronium in
the anaesthetized Rhesus monkey. Br J Anaesth 2006; 96:473479
31. Fuchs-Buder T, Meistelman C, Schreiber JU: Is sugammadex
economi-cally viable for routine use. Curr Opin Anaesthesiol 2012;
25:217220
32. Cammu G, De Kam PJ, Demeyer I, et al: Safety and
tolerability of sin-gle intravenous doses of sugammadex
administered simultaneously with rocuronium or vecuronium in
healthy volunteers. Br J Anaesth 2008; 100:373379
33. Naguib M, Brull SJ: Sugammadex: A novel selective relaxant
binding agent. Expert Rev Clin Pharmacol 2009; 2:3753
34. Akha AS, Rosa J 3rd, Jahr JS, et al: Sugammadex:
Cyclodextrins, development of selective binding agents,
pharmacology, clinical devel-opment, and future directions.
Anesthesiol Clin 2010; 28:691708
35. McDonnell MJ, Pavy TJ, Green LK, et al: Sugammadex in the
man-agement of rocuronium induced anaphylaxis. Br J Anesth 2011;
106:199201
36. Vender JS, Szokol J, Murphy GS, et al: Sedation, analgesia,
neuro-muscular blockade in sepsis: An evidence based review. Crit
Care Med 2004; 32:S554561
37. Murphy GS, Brull SJ: Residual neuromuscular block: Lessons
unlearned. Part I: Definitions, incidence, and adverse physiologic
effects of residual neuromuscular blockade. Anesth Analg 2010;
111:120128
38. Pino RM: Neuromuscular blockade studies of critically ill
patients. Intensive Care Med 2002; 28:16951697
39. Greenberg SB, Vender JS: Postoperative pulmonary
complications. Curr Rev Clin Anesth 2011; 31:221232
40. Sauer M, Stahn A, Soltesz S, et al: The influence of
residual neuro-muscular blockade on the incidence of critical
respiratory events. A randomized prospective, placebo controlled
trial. European J Anes-thesiol 2011; 28:841848
41. Murphy GS, Szokol JW, Marymont JH, et al: Intraoperative
accelero-myographic monitoring reduces the risk of residual
neuromuscular blockade and adverse respiratory events in the
postanesthesia care unit. Anesthesiology 2008; 109:389398
42. Murphy GS, Szokol JW, Avram MJ, et al: Intraoperative
accelero-myography monitoring reduces symptoms of muscle weakness
and improves quality of recovery in the early postoperative period.
Anes-thesiology 2011; 115:946954
43. Puthucheary Z, Rawal J, Ratnayake G, et al: Neuromuscular
blockade and skeletal muscle weakness in critically ill patients:
Time to rethink the evidence? Am J Respir Crit Care Med 2012;
185:911917
44. Forel JM, Roch A, Papazian L: Paralytics in critical care:
Not always the bad guy. Curr Opin Crit Care 2009; 15:5966
45. Khuenl-Brady KS, Reitsttter B, Schlager A, et al: Long-term
admin-istration of pancuronium and pipecuronium in the intensive
care unit. Anesth Analg 1994; 78:10821086
46. Rudis MI, Sikora CA, Angus E, et al: A prospective,
randomized, con-trolled evaluation of peripheral nerve stimulation
versus standard clini-cal dosing of neuromuscular blocking agents
in critically ill patients. Crit Care Med 1997; 25:575583
47. Strange C, Vaughan L, Franklin C, et al: Comparison of
train-of-four and best clinical assessment during continuous
paralysis. Am J Respir Crit Care Med 1997; 156:15561561
48. Baumann MH, McAlpin BW, Brown K, et al: A prospective
randomized comparison of train-of-four monitoring and clinical
assessment during continuous ICU cisatracurium paralysis. Chest
2004; 126:12671273
49. Burmester M, Mok Q: Randomised controlled trial comparing
cisatra-curium and vecuronium infusions in a paediatric intensive
care unit. Intensive Care Med 2005; 31:686692
50. Stevens RD, Marshall SA, Cornblath DR, et al: A framework
for diag-nosing and classifying intensive care unit-acquired
weakness. Crit Care Med 2009; 37(10 Suppl):S299S308
51. Coakley JH, Nagendran K, Yarwood GD, et al: Patterns of
neurophysi-ological abnormality in prolonged critical illness.
Intensive Care Med 1998; 24:801807
52. MacFarlane IA, Rosenthal FD: Severe myopathy after status
asthmati-cus. Lancet 1977; 2:615
53. Schakman O, Gilson H, Thissen JP: Mechanisms of
glucocorticoid-induced myopathy. J Endocrinol 2008; 197:110
54. Papazian L, Forel JM, Gacouin A, et al; ACURASYS Study
Investiga-tors: Neuromuscular blockers in early acute respiratory
distress syn-drome. N Engl J Med 2010; 363:11071116
55. Forel JM, Roch A, Marin V, et al: Neuromuscular blocking
agents decrease inflammatory response in patients presenting with
acute respiratory distress syndrome. Crit Care Med 2006;
34:27492757
56. Ballard N, Robley L, Barrett D, et al: Patients
recollections of ther-apeutic paralysis in the intensive care unit.
Am J Crit Care 2006; 15:8694; quiz 95
57. Loper KA, Butler S, Nessly M, et al: Paralyzed with pain:
The need for education. Pain 1989; 37:315316
58. Brook AD, Ahrens TS, Schaiff R, et al: Effect of a
nursing-implemented sedation protocol on the duration of mechanical
ventilation. Crit Care Med 1999; 27:26092615
59. Kress JP, Pohlman AS, OConnor MF, et al: Daily interruption
of seda-tive infusions in critically ill patients undergoing
mechanical ventila-tion. N Engl J Med 2000; 342:14711477
-
Concise Definitive Review
Critical Care Medicine www.ccmjournal.org 1343
60. Girard TD, Kress JP, Fuchs BD, et al: Efficacy and safety of
a paired sedation and ventilator weaning protocol for mechanically
ventilated patients in intensive care (Awakening and Breathing
Controlled trial): A randomised controlled trial. Lancet 2008;
371:126134
61. Patel SB, Kress JP: Sedation and analgesia in the
mechanically venti-lated patient. Am J Respir Crit Care Med 2012;
185:486497
62. Tonner PH, Paris A, Scholz J: Monitoring consciousness in
intensive care medicine. Best Pract Res Clin Anaesthesiol 2006;
20:191200
63. Yaman F, Ozcan A, Kaymak C, et al: Assessment of correlation
between bispectral index and four common sedation scales used in
mechanically ventilated patients in ICU. Eur Rev Med Pharmacol Sci
2012; 16:660666
64. Haenggi M, Ypparila-Wolters H, Buerki S, et al: Auditory
event-related potentials, bispectral index, and entropy for the
discrimination of dif-ferent levels of sedation in intensive care
unit patients. Anesth Analg 2009; 109:807816
65. LeBlanc JM, Dasta JF, Pruchnicki MC, et al: Bispectral index
values, sedation agitation scores, and plasma concentrations of
lorazepam in critically ill surgical patients. Am J Crit Care 2012;
21:99105
66. Honiden S, Siegel MD: Analytic reviews: Managing the
agitated patient in the ICU: Sedation, analgesia, and neuromuscular
blockade. J Intensive Care Med 2010; 25:187204
67. Boddi M, Barbani F, Abbate R, et al: Reduction in deep
venous throm-bosis incidence in intensive care after a clinician
education program. Thromb Hemost 2009; 8:121128
68. Sorce LR, Hamilton SM, Gauvreau K, et al: Preventing corneal
abra-sions in critically ill children receiving neuromuscular
blockade: A ran-domized controlled trial. Pediatr Crit Care Med
2009; 10:171175
69. Mertes PM, Tajima K, Regnier-Kimmoun MA, et al:
Perioperative ana-phylaxis. Med Clin North Am 2010; 94:761789
70. Mertes PM, Laxenaire MC: Anaphylatic and anaphylactoid
reactions occurring during anesthesia in France. Seventh
epidemiologic sur-vey (January 2001-December 2002). Ann Fr Anesth
Reanim 2004; 23:11331143
71. Dewachter P, Mouton-Faivre CM, Emala CW: Anaphylaxis and
anes-thesia. Anesthesiology 2009; 111:11411150
72. Murray MJ, Cowen J, Deblock H, et al: Clinical practice
guidelines for sustained neuromuscular blockade in the critically
ill adult. Crit Care Med 2002; 30;142156
73. Bailey P, Thomsen GE, Spuhler VJ, et al: Early activity is
feasible and safe in respiratory failure patients. Crit Care Med
2007; 35:139145
74. Thomsen GE, Snow GL, Rodriguez L, et al: Patients with
respira-tory failure increase ambulation after transfer to an
intensive care unit where early activity is a priority. Crit Care
Med 2008; 36:11191124
75. Morris PE, Goad A, Thompson C, et al: Early intensive care
unit mobil-ity therapy in the treatment of acute respiratory
failure. Crit Care Med 2008; 36:22382243
76. Schweickert WD, Pohlman MC, Pohlman AS, et al: Early
physical and occupational therapy in mechanically ventilated,
critically ill patients: A randomised controlled trial. Lancet
2009; 373:18741882
77. Mascia MF, Koch M, Medicis JJ: Pharmacoeconomic impact of
rational use guidelines on the provision of analgesia, sedation,
and neuromuscular blockade in critical care. Crit Care Med 2000;
28:23002306
78. Chanques G, Barbotte JS, Violet S, et al: Impact of systemic
evalu-ation of pain and agitation in an intensive care unit. Crit
Care Med 2006; 34:16911699
79. Reynolds SF, Heffner J: Airway management of the critically
ill patient: Rapid-sequence intubation. Chest 2005;
127:13971412
80. El-Orbany M, Connolly LA: Rapid sequence induction and
intuba-tion: Current controversy. Anesth Analg 2010;
110:13181325
81. Booij LH: Is succinylcholine appropriate or obsolete in the
intensive care unit? Crit Care 2001; 5:245246
82. Perry J, Lee J, Sillberg VA, et al: Rocuronium versus
succinylcholine for rapid sequence induction intubation. Cochrane
Database Syst Rev 2008; 2:CD002788
83. Marsch SC, Steiner L, Bucher L, et al: Succinylcholine
versus rocuronium for rapid sequence intubation in intensive care:
A pro-spective, randomized trial. Crit Care 2011; 15:R199R208
84. Wilcox SR, Bittner EA, Elmer J, et al: Neuromuscular
blocking agent administration for emergent tracheal intubation is
associated with decreased prevalence of procedure-related
complications. Crit Care Med 2012; 40:18081813
85. Rubenfeld GD, Herridge MS: Epidemiology and outcomes of
acute lung injury. Chest 2007; 131:554562
86. Zambon M, Vincent JL: Mortality rates for patients with
acute lung injury/ARDS have decreased over time. Chest 2008;
133:11201127
87. Bennett S, Hurford WE: When should sedation or
neuromuscu-lar blockade be used during mechanical ventilation?
Respir Care 2011; 56:168176
88. Bishop MJ: Hemodynamic and gas exchange effects of
pancuronium bromide in sedated patients with respiratory failure.
Anesthesiology 1984; 60:369371
89. Conti G, Vilardi V, Rocco M, et al: Paralysis has no effect
on chest wall and respiratory system mechanics of mechanically
ventilated, sedated patients. Intensive Care Med 1995;
21:808812
90. Freebairn RC, Derrick J, Gomersall CD, et al: Oxygen
delivery, oxy-gen consumption, and gastric intramucosal pH are not
improved by a computer-controlled, closed-loop, vecuronium infusion
in severe sepsis and septic shock. Crit Care Med 1997; 25:7277
91. Gainnier M, Roch A, Forel JM, et al: Effect of neuromuscular
block-ing agents on gas exchange in patients presenting with acute
respi-ratory distress syndrome. Crit Care Med 2004; 32:113119
92. Lagneau F, Dhonneur G, Plaud B, et al: A comparison of two
depths of prolonged neuromuscular blockade induced by cisatracurium
in mechanically ventilated critically ill patients. Intensive Care
Med 2002; 28:17351741
93. Appleton R, Kinsella J: Intensive care unit-acquired
weakness. Con-tin Educ Anaesth Crit Care Pain 2012; 12:6266
94. Leatherman JW, Fluegel WL, David WS, et al: Muscle weakness
in mechanically ventilated patients with severe asthma. Am J Respir
Crit Care Med 1996; 153:16861690
95. Goh AY, Chan PW: Acute myopathy after status asthmaticus:
Ste-roids, myorelaxants or carbon dioxide? Respirology 1999;
4:9799
96. Adnet F, Dhissi G, Borron SW, et al: Complication profiles
of adult asthmatics requiring paralysis during mechanical
ventilation. Inten-sive Care Med 2001; 27:17291736
97. Kesler SM, Sprenkle MD, David WS, et al: Severe weakness
com-plicating status asthmaticus despite minimal duration of
neuromus-cular paralysis. Intensive Care Med 2009; 35:157160
98. Oddo M, Feihl F, Schaller MD, et al: Management of
mechanical ventilation in acute severe asthma: Practical aspects.
Intensive Care Med 2006; 32:501510
99. Ohlinger MJ, Rhoney DH: Neuromuscular blocking agents in the
neurosurgical intensive care unit. Surg Neurol 1998; 49:217221
100. Hsiang JK, Chesnut RM, Crisp CB, et al: Early, routine
paralysis for intracranial pressure control in severe head injury:
Is it necessary? Crit Care Med 1994; 22:14711476
101. Schramm WM, Jesenko R, Bartunek A, et al: Effects of
cisatra-curium on cerebral and cardiovascular hemodynamics in
patients with severe brain injury. Acta Anaesthesiol Scand 1997;
41: 13191323
102. Prielipp RC, Robinson JC, Wilson JA, et al: Dose response,
recovery, and cost of doxacurium as a continuous infusion in
neu-rosurgical intensive care unit patients. Crit Care Med 1997;
25: 12361241
103. Schramm WM, Papousek A, Michalek-Sauberer A, et al: The
cere-bral and cardiovascular effects of cisatracurium and
atracurium in neurosurgical patients. Anesth Analg 1998;
86:123127
104. Kerr ME, Sereika SM, Orndoff P, et al: Effect of
neuromuscular blockers and opiates on the cerebrovascular response
to endotra-cheal suctioning in adults with severe head injuries. Am
J Crit Care 1998; 7:205217
105. Juul N, Morris GF, Marshall SB, et al: Neuromuscular
blocking agents in neurointensive care. Acta Neurochir Suppl 2000;
76:467470
106. Rangel-Castillo L, Gopinath S, Robertson CS: Management of
intracranial hypertension. Neurol Clin 2008; 26:521541
-
Greenberg and Vender
1344 www.ccmjournal.org May 2013 Volume 41 Number 5
107. Brain Trauma Foundation, American Association of
Neurological Surgeons (AANS), Congress of Neurological Surgeons
(CNS), AANS/CNS Joint Section on Neurotrauma and Critical Care:
Guidelines for the management of traumatic brain injury. J
Neu-rotrauma 2007; 24:S71S76
108. Cheatham ML: Intraabdominal pressure monitoring during
fluid resuscitation. Curr Opin Crit Care 2008; 14:327333
109. Malbrain ML, CheathamML, Kirkpatrick A, et al: Results from
the conference of experts on intra-abdominal hypertension and
abdomi-nal compartment syndrome. Part I: Definitions. Intensive
Care Med 2006; 32:17221732
110. Cheatham ML, Malbrain MLNG, Kirkpatrick A, et al: Results
from the conference of experts on intra-abdominal hypertension and
abdominal compartment syndrome. Part II: Recommendations. Intensive
Care Med 2007; 33:951962
111. De Waele J, Delaet I, Hoste E, et al. The effect of
neuromuscular blockers on intraabdominal pressure. Crit Care Med
2006; 34:A70
112. Mertens zur Borg IR, Verbrugge SJ, Kolkman KA: Anesthetic
consid-erations in abdominal compartment syndrome. In: Abdominal
Com-partment Syndrome. Ivatury RR, Cheatham ML, Malbrain MLNG, et
al (Eds). Landes Biomedical, Georgetown, 2006, pp 254265
113. An G, West MA: Abdominal compartment syndrome: A concise
clinical review. Crit Care Med 2008; 36:13041310
114. Davies J, Aghahoseini A, Crawford J, et al: To close or not
to close? Treat-ment of abdominal compartment syndrome by
neuromuscular blockade without laparostomy. Ann R Coll Surg Engl
2010; 92:W8W9
115. Luckianow GM, Ellis M, Governale D, et al: Abdominal
compartment syndrome: Risk factors, diagnosis, and current therapy.
Crit Care Res Pract 2012; 908169:18
116. Bernard SA, Gray TW, Buist MD, et al: Treatment of comatose
sur-vivors of out-of-hospital cardiac arrest with induced
hypothermia. N Engl J Med 2002; 346:557563
117. The Hypothermia After Cardiac Arrest Study Group: Mild
therapeu-tic hypothermia to improve the neurologic outcome after
cardiac arrest. N Engl J Med 2002; 346:549556
118. Polderman KH: Application of therapeutic hypothermia in the
ICU: Opportunities and pitfalls of a promising treatment modality.
Part 1: Indications and evidence. Intensive Care Med 2004; 30:
556575
119. Holzer M, Bernard SA, Hachimi-Idrissi S, et al;
Collaborative Group on Induced Hypothermia for Neuroprotection
After Cardiac Arrest: Hypothermia for neuroprotection after cardiac
arrest: Systematic review and individual patient data
meta-analysis. Crit Care Med 2005; 33:414418
120. Ramani R: Hypothermia for brain protection and
resuscitation. Curr Opin Anaesthesiol 2006; 19:487491
121. Alzaga AG, Cerdan M, Varon J: Therapeutic hypothermia.
Resusci-tation 2006; 70:369380
122. Rincon F, Mayer SA: Therapeutic hypothermia for brain
injury after cardiac arrest. Semin Neurol 2006; 26:387395
123. Howes D, Green R, Gray S, et al; Canadian Association of
Emer-gency Physicians: Evidence for the use of hypothermia after
cardiac arrest. CJEM 2006; 8:109115
124. Cheung KW, Green RS, Magee KD: Systematic review of
random-ized controlled trials of therapeutic hypothermia as a
neuroprotec-tant in post cardiac arrest patients. CJEM 2006;
8:329337
125. Holzer M, Behringer W: Therapeutic hypothermia after
cardiac arrest and myocardial infarction. Best Pract Res Clin
Anaesthesiol 2008; 22:711728
126. Schneider A, Bttiger BW, Popp E: Cerebral resuscitation
after car-diocirculatory arrest. Anesth Analg 2009; 108:971979
127. Chamorro C, Borrallo JM, Romera MA, et al: Anesthesia and
anal-gesia protocol during therapeutic hypothermia after cardiac
arrest: A systematic review. Anesth Analg 2010; 110:13281335
128. Heier T, Caldwell JE: Impact of hypothermia on the response
to neu-romuscular blocking drugs. Anesthesiology 2006;
104:10701080
129. Prielipp RC, Coursin DB: Applied pharmacology of common
neu-romuscular blocking agents in critical care. New Horiz 1994;
2:3447
130. Behbehani NA, Al-Mane F, Dyachkova Y, et al: Myopathy
following mechanical ventilation for severe acute asthma: The role
of muscle relaxants and corticosteroids. Chest 1999;
115:16271631
131. Griffin D, Fairman N, Coursin D, et al: Acute myopathy
during treat-ment of status asthmaticus with corticosteroids and
steroidal mus-cle relaxants. Chest 1992; 102:510514
132. Cheatham ML, Safcsak K: Is the evolving management of
intra-abdominal hypertension and abdominal compartment syndrome
improving survival? Crit Care Med 2010; 38:402407