Embed Size (px)
DESCRIPTION
blood transfusion
Citation preview
Blood Transfusion A clinician’s reference
First Edition
Hospital Transfusion Committee Centro Hospitalar de Conde São Januário (CHCSJ)
SS, Macao
September 2005
Hospital Transfusion Committee Centro Hospitalar de Conde São Januário (CHCSJ)
SS, Macao
1
BLOOD TRANSFUSION
A clinician’s reference
S
Hospital Tranfsusion Committee CHCSJ
Heath Bureau, Macau
2
Index
Introduction ------------------------------------------------------------------------------------------- 4
Useful Contacts --------------------------------------------------------------------------------------- 4
Administration of Blood and Blood Components -------------------------------------------------5
Informed Consent--------------------------------------------------------------------------------------7
Guidelines of the Blood Component Transfusion ------------------------------------------------ 8
Massive Blood Transfusion ------------------------------------------------------------------------ 12
Obstetric Haemorrhage ----------------------------------------------------------------------------- 13
Neonatal Transfusion -------------------------------------------------------------------------------- 14
Leukodepleted Blood -------------------------------------------------------------------------------- 17
Irradiated Blood Components ---------------------------------------------------------------------- 18
Autologous Donation-------------------------------------------------------------------------------- 19
Flowchart for applying PABD --------------------------------------------------------------------- 20
Standard Surgical Blood Order Schedule (SSBOS) --------------------------------------------- 21
Standard Blood Ordering Schedules
General and Vascular Surgery ----------------------------------------------------------------- 22
Cardiac and Thoracic Surgery ----------------------------------------------------------------- 23
Plastic Surgery ----------------------------------------------------------------------------------- 24
Neurosurgery ------------------------------------------------------------------------------------ 25
Otorhinolaryingology --------------------------------------------------------------------------- 26
Orthopedic Surgery ----------------------------------------------------------------------------- 26
Urology ------------------------------------------------------------------------------------------- 27
Obstetrics-Gynecology ------------------------------------------------------------------------- 27
Transfusion Reactions ------------------------------------------------------------------------------- 28
References -------------------------------------------------------------------------------------------- 31
3
FOREWORD The Hospital Transfusion Committee of Centro Hospitalar de Conde São Januário (CHCSJ) was
formed in 2004 to promote the concept of safe transfusion. The chairman of the committee is the
Director of CHCSJ. Other members of the committee come from various departments in the
hospital and include members from the Macao Blood Transfusion Centre.
With the sole purpose in mind the Hospital Transfusion Committee has formulated and approved
these Transfusion Guidelines as a reference to clinicians in the CHCSJ. This is the first edition.
We envisioned that future editions will incorporate suggestions and recommendations from the
users of the guidelines.
The committee would like to acknowledge the effort of Dr. David T Lopes and Dr. Hui Ping in
formulating the guidelines since 1999.
Hospital Transfusion Committee , CHCSJ
July 2005
4
INTRODUCTION Blood transfusion is an essential part of modern health care. Used correctly, it can save life and
improve health. However, as with any therapeutic intervention, it may result in acute or delayed
complications. In addition, it carries the risk of transmission of infectious agents, such as HIV,
hepatitis viruses, syphilis, etc. It is also expensive and uses a scarce human resource.
The risks associated with transfusion can only be decreased by close collaboration between the
blood transfusion service and clinicians in managing the components of the transfusion process
for which they are each responsible:
1. an adequate supply of safe blood and blood products
2. the effective clinical use of blood and blood products
Considering the lack of transfusion medicine in the medical school and the rapid advance of
this field since the last decade, we provide this booklet for serving as a convenient reference
for issues relating to the clinical use of blood.
USEFUL CONTACTS Hospital Blood Bank: 3903226, 3903219
Dr. David Lopes: 6807838
Blood Transfusion Centre: 752522
Dr. HUI Ping:
Office: 7914307
Emergency: 6892637
Laboratory Supervisor: Mr. Hoo Chai
Office: 752522/7914386
Hospital service Supervisor: Mr. Choi Sio Cheok
Office: 752522/7914361
5
ADMINISTRATION OF BLOOD AND BLOOD
COMPONENTS I. Request Form
Transfusion request form must be completely fulfilled and clinical details must be
provided.
II. Filter
• All blood components must be administered through a transfusion standard filter (170-
micron) to remove blood clots and other debris.
• Changing of blood filter every 4 hours.
III. Timing All blood components which have been kept outside the blood bank should be
transfused to the patient as soon as possible.
IV. Blood Warming
Never warm the blood and blood products outside the blood bank. Warming blood only restricted to:
• Adult patients receiving rapid and multiple transfusions (rate >2000ml/hour).
• Children receiving large volumes (>15ml/kg/hour).
• Exchange transfusions in infants.
• Rapid infusion through central venous catheters.
V. Concomitant Use of Intravenous Solutions Only normal saline (0.9 % saline) may be administered with blood components.
VI. Monitors during and after transfusion In first 5 minutes of beginning transfusion and every 30 minutes during transfusion, CHECK:
S Blood pressure
S Pulse
S Temperature
Suspect the major acute transfusion reactions, when:
S A sudden rise in temperature > 10C
S Shortness of breath/chest pain
S Back pain/loin tenderness
S Profound hypotension
6
VII. Ordering and issuing Red Cells/Whole Blood
• Routine transfusions should be requested at least 24 hours in advance during the
working hours.
• ±60 mins must be allowed for the grouping and crossmatch testing for emergency
order.
• Uncross-matched blood – can only be issued in an emergency. The blood bank staff
will only release uncross-matched blood after he/she has received a request from a
medical doctor, who has agreed to take responsibility for any ensuing complications.
Fresh Frozen Plasma (FFP)
l ± 45 mins should be allowed for the product to thaw before issuing.
l No cross-matched test needed, but an EDTA sample for blood grouping should be
sent if the blood group is unknown.
l ABO compatible FFP should be used.
l The thawed FFP cannot be refrozen.
l The thawed FFP infusion should be used without delay within 2 hours to avoid loss
of potency of coagulation factors.
Platelets
- Are only available after discussion with a Hematologist.
- Patient’s blood group should be known before the product can be issued and the same
ABO group as the patient should be used as far as possible.
- Should be transfused as soon as possible after reaching the ward.
Cryoprecipitate
• ±45 mins should be allowed for the product to thaw.
• Is available only after discussion with a hematologist.
• No cross-matched test needed, but an EDTA sample for blood group should be sent
if the blood group is unknown.
• ABO-compatible cryoprecipitate is not required.
7
INFORMED CONSENT I. POLICY
CHCSJ requires documentation that patients who receive non-emergent
transfusions be informed of the procedures, alternatives, risks and benefits of blood
and blood products. The patients must be given an opportunity to ask questions and it
must be documented that they agree to receive the blood and blood products.
II. CURRENT RISKS, BENEFITS AND ALTERNATIVES TO TRANSFUSION
The CTS has created a patient information sheet ‘What you should know about blood transfusion’ to aid in the discussion of the risks, benefits and alternatives to transfusion.
III. MEDICAL EMERGENCIES AND TRANSFUSION INFORMED CONSENT
l Signed consent not absolutely required for emergency transfusion.
l Document emergent nature of problem and efforts to obtain consent in progress notes.
IV. PARTIES RESPONSIBLE FOR OBTAINING TRANSFUSION INFORMED CONSENT
l Ordering physician responsible for obtaining consent.
l Responsibility can be delegated, but the person obtaining the consent must be knowledgeable in the risks, benefits and alternatives to transfusion and must be conversant with clinical indications for transfusion and clinical consequences of refusal of permission to transfuse.
V. DURATION OF VALIDITY FOR INFORMED CONSENT
l Informed consent is valid for an entire named course of treatment.
l May span multiple admissions.
l Surgical patients typically consented once per admission.
l Consents should be renewed when there is a significant change in risk associated with the treatment.
VI. REFUSAL OF BLOOD TRANSFUSION
l We honor wishes of patients who refuse transfusion.
l Refusal Transfusion Consent should be obtained and must be documented in medical record.
8
GUIDELINES OF THE BLOOD COMPONENT
TRANSFUSION The following guidelines have been generally accepted by the well-recognized specialists in the
world.
I. RED BLOOD CELLS General guidelines
• Hb and Hematocrit:
There is no an absolute acceptable level for all patients exists. But the concept of,
transfusion is only indicated when Hb <7 g/dl, has been general accepted in most of the
countries in the world.
• Clinical data:
Clinical data like age, function of the end organs, sepsis, causes of anemia etc, should be
evaluated first at all.
• Acute blood loss:
Blood transfusion is indicated when adequate fluid resuscitation has failed to:
a) correct intravascular volume depletion
b) relieve symptoms
c) stabilize vital signs
• Chronic blood loss:
Blood transfusion is only indicated to relieve symptoms when appropriate medical
measures to improve red cell mass have been inadequate.
• Patient under anesthesia:
Blood transfusion should be based upon stability of vital signs.
Indications - Acute blood loss (> 1000ml within few hours) ± symptoms of hypovolemic shock
- Per ioperative with intra-operative blood loss > 750ml
- Perioperative with Hb < 8g / dl
- Iron deficiency and megaloblastic anemia:
Never transfuse, unless:
a Fail to response to pharmacologic therapy like Iron, B12 or Folate
b Severe decompensate symptoms, like tachycardia, dyspnea, severe dizziness, etc.
c Hb < 5g /dl
Volume: 250ml / unit
9
Important to remember • The only true indication for the blood transfusion is the need to improve the delivery
of O2 to the tissues within a short time.
• Patients with anaemia of undiagnosed cause should not be transfused until appropriate
investigations have been performed.
• Routine or programmed transfusions should be requested at least 24 hours in advance
during the working hours.
II. WHOLE BLOOD
Whole blood is the complete collection of a single donation of blood, which contains
1. red cells
2. antigenic granulocytes
3. platelets without function
4. all the plasma proteins, but as a result of storage there is loss of activity by the
coagulant factors V and VIII:C and by complement.
Volume: 350ml/unit
Indication: Autologous transfusion only.
III. PLATELET
Preparation of platelets 1. Platelets concentrates:
Prepared from individual units of whole blood by centrifugation.
Each bag volume ≈ 50-60 ml, platelet count: 5.5×1010
An adult therapeutic dose = 4 single bags
2. Apheresis platelets:
Collected from an individual donor during 2-3 hours apheresis procedure.
Volume: 200-300ml/unit
Platelet count: 3×1011
Shelf life and Storage
5 days’ shelf life, at 22 ±20C, under constant and gentle agitation in a special incubator.
10
Indications
The decision to transfuse platelets should not be based on low platelet count alone.
1. DIC with active bleeding (platetlet count < 20,000/ul) .
2. Severe thrombocytopenia (<10,000/ul) following chemotherapy.
3. Active bleeding with severe thrombocytopenia (platetlet count < 10,000/ul).
4. Thrombocytopenia, with scheduled invasive procedure.
5. Thrombocytopathy, bleeding time > 2 × normal with bleeding or scheduled
invasive procedure.
Platelets should not be transfused 1. Immune thrombocytopenia.
2. Prophylactically in most patients with aplastic anemia.
3. Thrombotic thrombocytopenic purpura/Hemolytic uraemic syndrome or
eclampsia.
IV FRESH FROZEN PLASMA Containing all clotting factors, but factor V and VIII is minimal.
Volume of each unit: 200 ml
Dose
Generally accepted starting dose: 2 units (10ml/Kg for coagulation factor replacement)
Indications 1. Definite indications:
• Replacement of single coagulation factor deficiencies, where a specific or combined factor
concentrate is unavailable.
• Immediate reversal of Warfarin
• DIC- acute disseminated intravascular coagulation
• Thrombotic thrombocytopenic purpura / Hemolytic ureamic syndrome
2. Conditional use:
Only indicated in the presence of bleeding and disturbed coagulation:
• Massive transfusion
• Liver disease
• Cardiopulmonary bypass surgery
11
FFP should not be transfused
• For volume expansion
• A nutritional supplement
• Prophylactically with massive blood transfusion
• Prophylactically following cardiopulmonary
V. CRYOPRECIPITATE
Contains
• Factor VIII : 80-100iu/unit
• Fibrinogen :150-300 mg/unit
• Factor XIII
• Fibronectin
Volume of each unit: 10 ml
Dose: 10 individual units is a standard adult dose.
Indications
• DIC with active bleeding or before invasive procedure and APTT > 1.5× normal
• Hypofibrinogenemia (<100mg/dl) or dysfibrinogenemia with active bleeding or before
scheduled invasive procedure.
• Uremic thrombocytopathy unresponsive to DDAVP, with active bleeding or before
scheduled invasive procedure.
• Von-willebrand’s disease unresponsive to DDAVP with active bleeding or before
scheduled invasive procedure.
• Factor XIII deficiency
• As fibrin glue
12
TRANSFUSION PRACTICE
I. MASSIVE BLOOD TRANSFUSION
Definition Massive transfusion is defined as the replacement of one or more blood volumes within 24
hours (≈ 4500ml in 60-kg adult).
Management - Minimum laboratory investigation in patients with acute hypovolaemic shock:
• Pre-transfusion testing (10ml clotted blood): - ABO, Rh grouping
- Crossmatch testing
• Hematology (2ml in EDTA): Full blood count.
• Coagulation (5ml in citrate): PT, APTT, Fibrinogen
• Biochemistry: baseline urea and electrolyte concentration
- Priorities in massive transfusion:
1) Replace and maintain blood volume
Initially, crystalloid or colloid solutions may give for restoring the blood volume.
Whole blood (first 4 units) should be followed while the compatible or suitable blood
has been prepared by the blood bank.
2) Maintain haemostasis
Stored citrate blood:
� clotting factors, mainly factor V and VIII loss activity
� platelets in stored blood have no function at all after 48 hours
storage.
When:
S platelet counts < 50×109/l, transfuse platelet
S either PT or aPTT are prolonged to > 1.8 × the control value, fresh frozen
plasma should be given (at least 4 units)
S fibrinogen < 100mg/dl, cryoprecipitate is indicated.
S Further, should be monitor by clinical response and laboratory test.
3) Optimise oxygen carrying capacity
S Maintain packed cell volume > 0.20 ( ≈ 6.0 g/dl )
13
S The 2, 3-DPG level in stored blood cells reduced significantly for up to 14 days
after collection. It might be important for patients with pre-existing cardiac disease
or severe anaemia to have blood that is less than 14 days old.
4) Correct or avoid metabolic disturbances
The stored blood is :
S Hypocalcemia
S Hyperkalemia
S Acidosis
S Hypothermia
- Hypocalcaemia and hyperkalemia combinate with hypothermia cause by rapid
transfusion of blood stored at 4 0C, can cause cardiac irregularities – ECG
monitoring is advisable.
- Prophylactically calcium supplement is not recommended.
- The correction of acidosis by alkalising agent should be provided only by the
results of laboratory tests and not by the number of units of blood transfused.
- Warming blood by blood warmers.
5) Maintain plasma colloid osmotic pressure
Large volume of crystalloids and red cell preparation devoid of plasma for
replacement of blood loss will lead to a fall in plasma colloid osmotic pressure.
II. OBSTETRIC HAEMORRHAGE Obstetric haemorrhage caused 12 out of the 134 direct maternal deaths in the UK
annually. The blood flow to the placenta is 70 ml/min at term, so bleeding is likely to be rapid.
It is often unexpected and difficult to control. Disseminated intravascular coagulation is
common in obstetric haemorrhage due to placental abruption, amniotic fluid embolism and
intrauterine death.
Haemorrhage due to obstetric DIC is usually relieved only by treating the underlying
disorder, which usually involves rapid delivery. Supportive treatment with platelets, FFP and
cryoprecipitate may be required and should be guided by laboratory tests. Bleeding into the
uterine cavity, the uterine wall or the abdomen may conceal the extent of the blood loss. As a
result, the patient may decompensate suddenly in the post-delivery period.
The following management protocol is for reference:
14
Transfusion in obstetric haemorrhage l Insert at least two large cannulas. Start saline infusion. Apply compression cuff to
infusion pack. Monitor central venous pressure (CVP) and arterial pressure. Take
samples for transfusion and coagulation screen. Order at least 6 units of red cells. Do
not insist on crossmatched blood if transfusion is urgently needed.
l Warm the resuscitation fluids.
l Transfuse red cells as soon as possible. Until then:
- crystalloid, maximum of 2 litres
- colloid, maximum of 1.5 litres
l Restore normovolaemia as priority, monitor red cell replacement with haematocrit or
Hb.
l Use coagulation screens to guide and monitor use of blood components.
l If massive bleeding continues, give FFP 1 litre, cryoprecipitate 10 units while awaiting
coagulation results.
l Monitor pulse rate, blood pressure, CVP, blood gases, acid-base status and urinary
output (catheterised).
III. NEONATAL TRANSFUSION A RED CELL
1. Characteristics of newborn infants
• Small size
• Physiologic anemia
• Iatrogenic blood loss
• O2 affinity of fetal hemoglobin
• Immature immune system
• Presence of maternal alloantibodies
• Variations in blood volume with age
• Shortened red cell survival
• Decreased erythropoiesis
• Cardiovascular adaptive capacity
15
2. Indications for red cell transfusion to neonates and premature infants
• Shock associated with acute blood loss.
• Hb<13g/dl, Hct < 40% and pulmonary failure, cyanotic heart disease, or congestive
heart failure.
• Cumulative loss of 10% or more of the blood volume ≤ 72h if additional sampling is
required.
• Hb< 8g/dl or Hct < 25% in a stable neonate with clinical manifestations of anemia,
namely tachycardia, tachypnea, and poor feeding.
3. Pre Transfusion Testing
• ABO and Rh group of both mother and neonate
• DAT (Directed agglutinative test) of neonate
• Maternal blood for cross-match testing
4. Dose
Transfuse 3ml/kg packed red cell raise hemoglobin by 1g/dl.
B NON-RED CELL COMPONENT Platelet:
• DIC secondary to severe sepsis
• Dose: 5-10 ml / kg raise platelet count 75 to 100×109/l
Plasma and cryoprecipitates
FFP and Cryoprecipitate may be required in DIC and consumptive states (see section IV
and V), and therapy should be guided by the results of laboratory coagulation tests.
C MAIN TRANSFUSION SIDE EFFECTS IN NEONATE
• Hypocalcaemia
• Citrate toxicity
• Rebound hypoglycemia
• Virus infection
• Transfusional overload
• Hemolytic transfusion reactions in necrotising enterocolitis
16
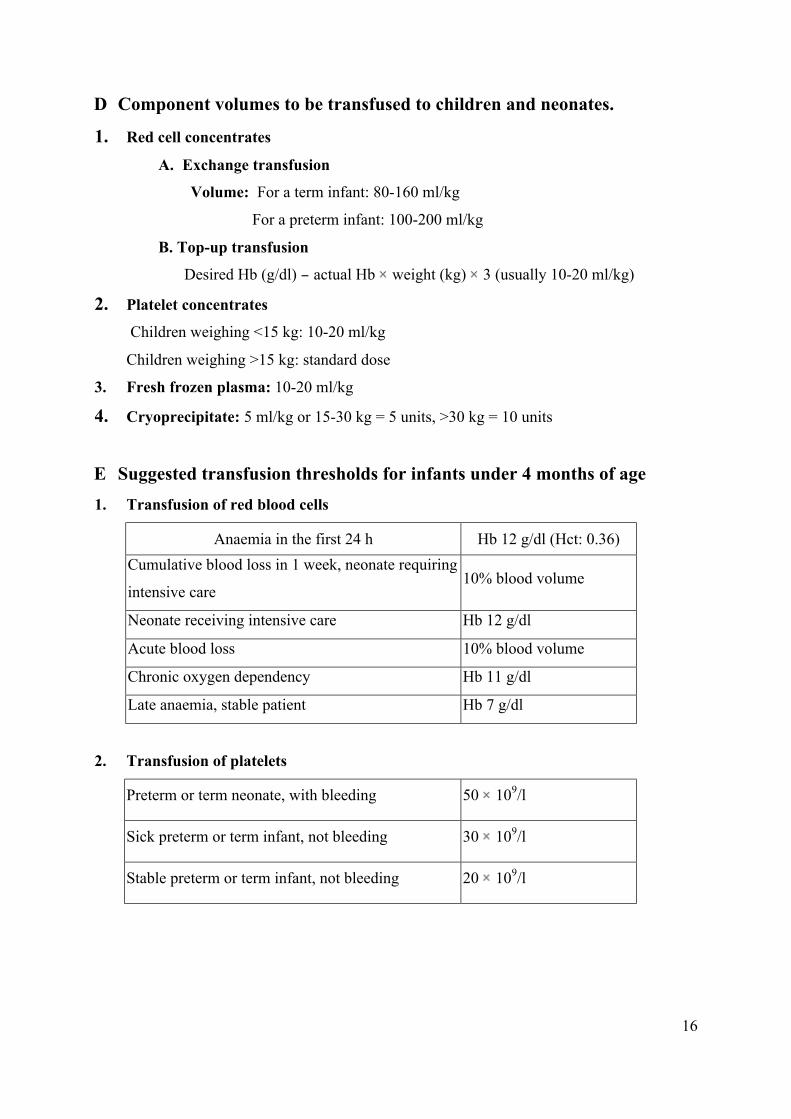
D Component volumes to be transfused to children and neonates.
1. Red cell concentrates A. Exchange transfusion
Volume: For a term infant: 80-160 ml/kg
For a preterm infant: 100-200 ml/kg
B. Top-up transfusion Desired Hb (g/dl) actual Hb weight (kg) 3 (usually 10-20 ml/kg)
2. Platelet concentrates Children weighing <15 kg: 10-20 ml/kg
Children weighing >15 kg: standard dose
3. Fresh frozen plasma: 10-20 ml/kg
4. Cryoprecipitate: 5 ml/kg or 15-30 kg = 5 units, >30 kg = 10 units
E Suggested transfusion thresholds for infants under 4 months of age
1. Transfusion of red blood cells
Anaemia in the first 24 h Hb 12 g/dl (Hct: 0.36) Cumulative blood loss in 1 week, neonate requiring
intensive care 10% blood volume
Neonate receiving intensive care Hb 12 g/dl
Acute blood loss 10% blood volume
Chronic oxygen dependency Hb 11 g/dl
Late anaemia, stable patient Hb 7 g/dl
2. Transfusion of platelets
Preterm or term neonate, with bleeding 50 109/l
Sick preterm or term infant, not bleeding 30 109/l
Stable preterm or term infant, not bleeding 20 109/l
17
SPECIAL REQIREMENTS I. LEUKODEPLETED BLOOD
Cellular blood components that contain less than 5x10 6 leukocytes (white blood cells) are
considered leukocyte depleted. The leukocyte content of blood components can be reduced to
less than 5x106 by filtration. Cryoprecipitate and fresh frozen plasma do not contain intact or
viable leukocytes making leukodepletion unnecessary.
Indications
Leukodepleted blood and components are indicated:
• for patients who have experienced two or more non-hemolytic febrile transfusion reactions
• as a method of preventing transfusion transmitted CMV
• as a method of preventing platelet alloimmunization in certain patients
The purpose of transfusing leukocyte-depleted blood products is to:
n Reduce HLA alloimmunization to leukocytes in multiply-transfused patients
n Reduce the risk of cytomegalovirus transmission
n Decrease febrile transfusion reactions
n Other theoretical benefits remain speculative at this time
II. IRRADIATED BLOOD COMPONENTS
Irradiated blood products are exposed to approximately 2500 rads of Gamma radiation
to destroy the lymphocyte ’s ability to divide. Transfusion-associated graft-versus-host
disease (TA-GVHD) has not been reported from transfusion of cryoprecipitate or fresh
frozen plasma (FFP), thus these components do not require irradiation. Fresh plasma
(never frozen) for transfusion should be irradiated if the patient is at risk for TA-GVHD.
Indications
Absolute Indication:
• bone marrow transplant (BMT) recipients (allogeneic, autologous)
• BMT or stem cell donors if allogeneic transfusion must be given prior to completing the harvest
18
• Cellular (T-cell) Immune Deficiency (congenital or acquired)
• intrauterine transfusion
• transfusions from family members (any degree)
• directed donors (when not identified as family members versus friends)
• HLA-matched platelet transfusions
Appropriate Indication:
• hematologic malignancies (leukemias)
• Hodgkin’s Disease
• non-Hodgkin’s Lymphoma
• neonatal exchange transfusion
• premature infants
• certain solid tumors (neuroblastoma, glioblastoma)
Therapeutic Effect
Irradiation destroys the ability of transfused lymphocytes to respond to host foreign
antigens thereby preventing graft vs. host disease in susceptible recipients. Patients with
functional immune systems will destroy foreign lymphocytes, making irradiation of blood
and blood components unnecessary.
19
III. AUTOLOGOUS DONATION
Preoperative autologous blood donation
Some patients can donate their own blood - up to 4 units in advance of their own planned
operation. It can be stored for up to 5 weeks using standard hospital blood bank conditions. It
must be tested, processed, labelled and stored to the same standard as donor blood. Before re-
transfusion, autologous blood units must be ABO and Rh D grouped and compatibility
checked.
- Preoperative donations are made at CTS two to five weeks before operation.
- Service available on prescription basis.
- Autologous donation does not guarantee patient will not need additional banked blood.
- Autologous donation can make donor anemic and can increase chance of getting banked blood.
- Autologous blood is subject to same risks of clerical error and bacterial contamination that affect banked blood.
- Donation must be scheduled at CTS. Contact the physicians at CTS at 7914337 or 752522.
- Appropriate forms is available from the physicians in CTS or print from the homepage
of CTS http://www.ssm.gov.mo/cts/.
Patients suitable to predonate their own blood for surgery
• Operation scheduled is likely to need red cell transfusion.
• Date for surgery fixed, so the blood does not become outdated.
• Patient able to attend to have blood collected.
• Patient''s initial haemoglobin >100g/l (female) >110g/l (male).
• Sufficient time before surgery to donate at least 2 units of blood.
• Iron replacement is required during autologous donations.
20
Procedure should be restricted to:
• Patients aged under 70 years
• Operations with a high blood loss
Not currently recommended in
Cardiac surgery patients (risk of thrombosis has not been excluded totally).
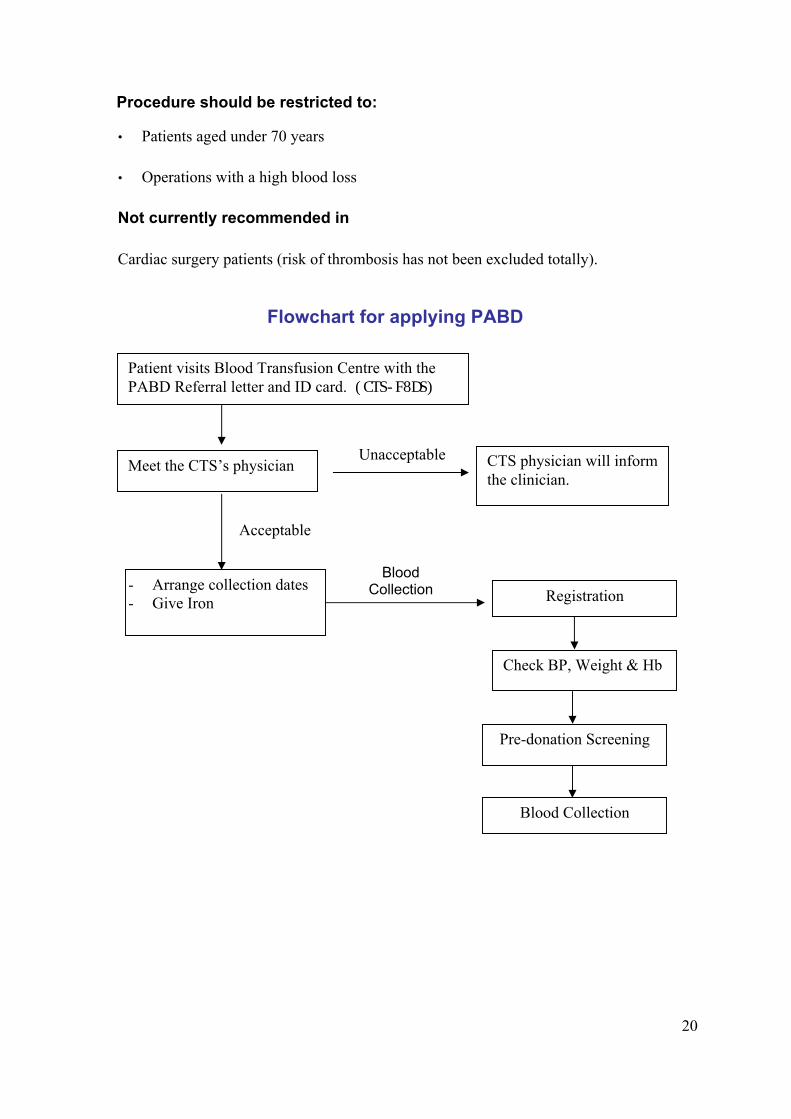
Flowchart for applying PABD
.
Patient visits Blood Transfusion Centre with the PABD Referral letter and ID card. (CTS-F8DS)
Meet the CTS’s physician
- Arrange collection dates - Give Iron Registration
Check BP, Weight & Hb
Pre-donation Screening
Unacceptable
Blood Collection
CTS physician will inform the clinician.
Blood Collection
Acceptable
21
STANDARD SURGICAL BLOOD ORDER SCHEDULE (SSBOS) Purpose
When using the SSBOS, the Hospital Blood Bank will initially provide no more than the
designated amount of Red Blood Cells, although orders for fewer units will be followed. If
transfusion is not anticipated but may still occur, the maximum order is a “type and
screen.”
Specimens should be submitted at least one day before surgery. Specimens for pre-
transfusion testing can be collected up to 21 days prior to surgery when the patient has not
been pregnant or transfused in the past 3 months, otherwise the specimen can be collected
no more than 3 days before scheduled surgery.
Procedure
Adhere to the following guidelines:
T&C = Type and Cross.
T&S = Group/Type and antibody Screen.
NBR = No blood Required
NOTE: All the above orders and specimens are maintained in hospital blood bank for 7 days.
22
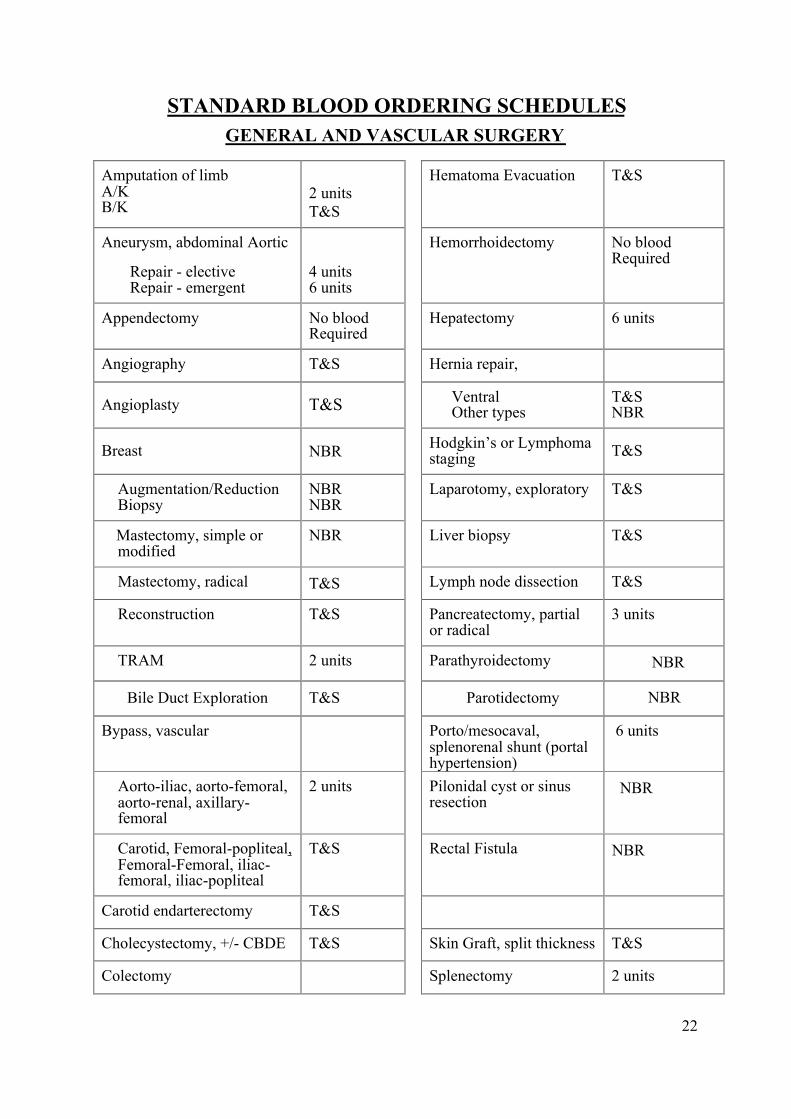
STANDARD BLOOD ORDERING SCHEDULES GENERAL AND VASCULAR SURGERY
Amputation of limb A/K B/K
2 units T&S
Hematoma Evacuation T&S
Aneurysm, abdominal Aortic
Repair - elective Repair - emergent
4 units 6 units
Hemorrhoidectomy No blood Required
Appendectomy No blood Required
Hepatectomy 6 units
Angiography T&S Hernia repair,
Angioplasty T&S Ventral Other types
T&S NBR
Breast NBR Hodgkin’s or Lymphoma staging T&S
Augmentation/Reduction Biopsy
NBR NBR
Laparotomy, exploratory T&S
Mastectomy, simple or modified
NBR Liver biopsy T&S
Mastectomy, radical T&S Lymph node dissection T&S
Reconstruction T&S Pancreatectomy, partial or radical
3 units
TRAM 2 units Parathyroidectomy NBR
Bile Duct Exploration T&S Parotidectomy NBR
Bypass, vascular Porto/mesocaval, splenorenal shunt (portal hypertension)
6 units
Aorto-iliac, aorto-femoral, aorto-renal, axillary-femoral
2 units Pilonidal cyst or sinus resection
NBR
Carotid, Femoral-popliteal, Femoral-Femoral, iliac-femoral, iliac-popliteal
T&S Rectal Fistula NBR
Carotid endarterectomy T&S
Cholecystectomy, +/- CBDE T&S Skin Graft, split thickness T&S
Colectomy Splenectomy 2 units
23
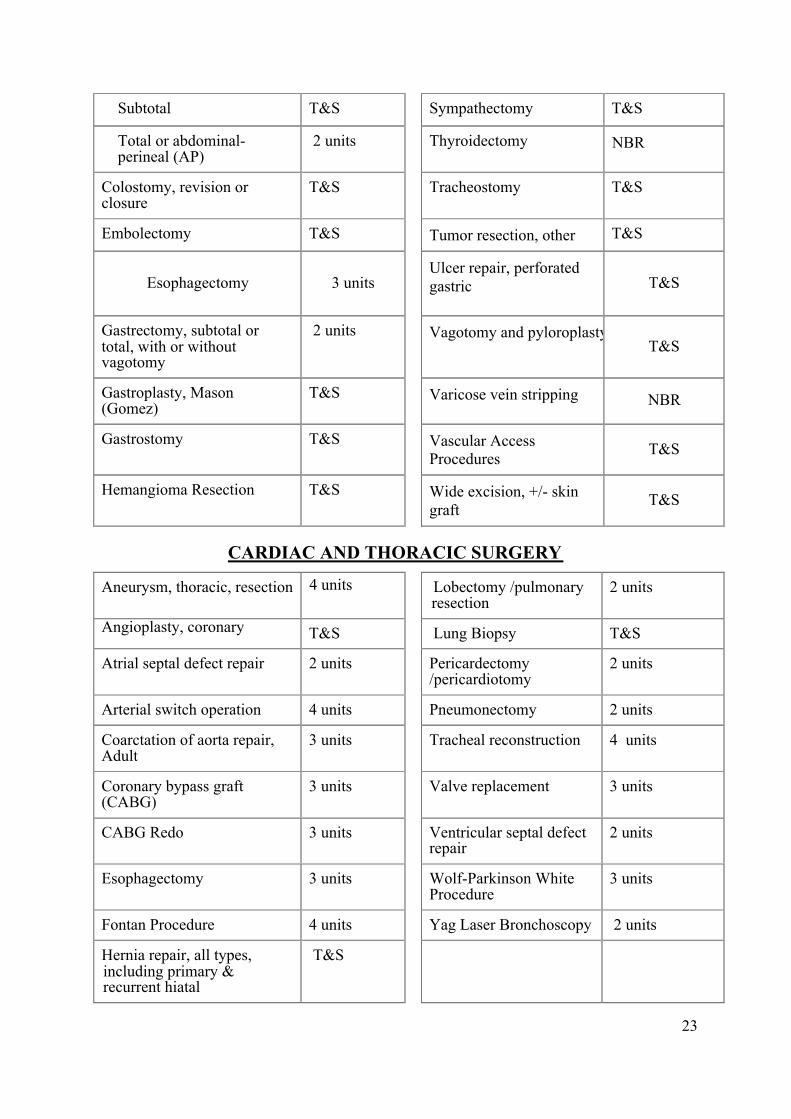
Subtotal T&S Sympathectomy T&S
Total or abdominal-perineal (AP)
2 units Thyroidectomy NBR
Colostomy, revision or closure
T&S Tracheostomy T&S
Embolectomy T&S Tumor resection, other T&S
Esophagectomy 3 units Ulcer repair, perforated
gastric T&S
Gastrectomy, subtotal or total, with or without vagotomy
2 units Vagotomy and pyloroplastyT&S
Gastroplasty, Mason (Gomez)
T&S Varicose vein stripping NBR
Gastrostomy T&S Vascular Access Procedures T&S
Hemangioma Resection T&S Wide excision, +/- skin graft T&S
CARDIAC AND THORACIC SURGERY
Aneurysm, thoracic, resection 4 units Lobectomy /pulmonary resection
2 units
Angioplasty, coronary T&S Lung Biopsy T&S
Atrial septal defect repair 2 units Pericardectomy /pericardiotomy
2 units
Arterial switch operation 4 units Pneumonectomy 2 units
Coarctation of aorta repair, Adult
3 units Tracheal reconstruction 4 units
Coronary bypass graft (CABG)
3 units Valve replacement 3 units
CABG Redo 3 units Ventricular septal defect repair
2 units
Esophagectomy 3 units Wolf-Parkinson White Procedure
3 units
Fontan Procedure 4 units Yag Laser Bronchoscopy 2 units
Hernia repair, all types, including primary & recurrent hiatal
T&S
24
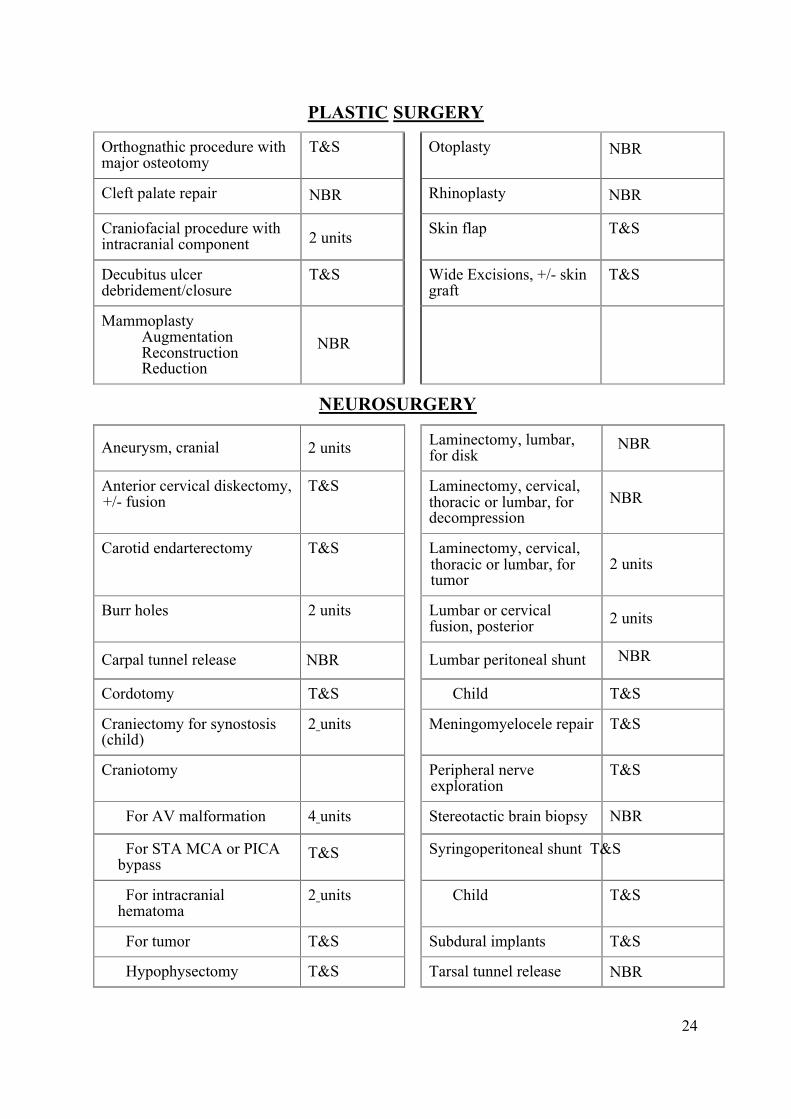
PLASTIC SURGERY
Orthognathic procedure with major osteotomy
T&S Otoplasty NBR
Cleft palate repair NBR Rhinoplasty NBR
Craniofacial procedure with intracranial component
2 units Skin flap T&S
Decubitus ulcer debridement/closure
T&S Wide Excisions, +/- skin graft
T&S
Mammoplasty Augmentation Reconstruction Reduction
NBR
NEUROSURGERY
Aneurysm, cranial 2 units Laminectomy, lumbar, for disk
NBR
Anterior cervical diskectomy, +/- fusion
T&S Laminectomy, cervical, thoracic or lumbar, for decompression
NBR
Carotid endarterectomy T&S Laminectomy, cervical, thoracic or lumbar, for tumor
2 units
Burr holes 2 units Lumbar or cervical fusion, posterior 2 units
Carpal tunnel release NBR Lumbar peritoneal shunt NBR
Cordotomy T&S Child T&S
Craniectomy for synostosis (child)
2 units Meningomyelocele repair T&S
Craniotomy Peripheral nerve exploration
T&S
For AV malformation 4 units Stereotactic brain biopsy NBR
For STA MCA or PICA bypass
T&S Syringoperitoneal shunt T&S
For intracranial hematoma
2 units Child T&S
For tumor T&S Subdural implants T&S
Hypophysectomy T&S Tarsal tunnel release NBR
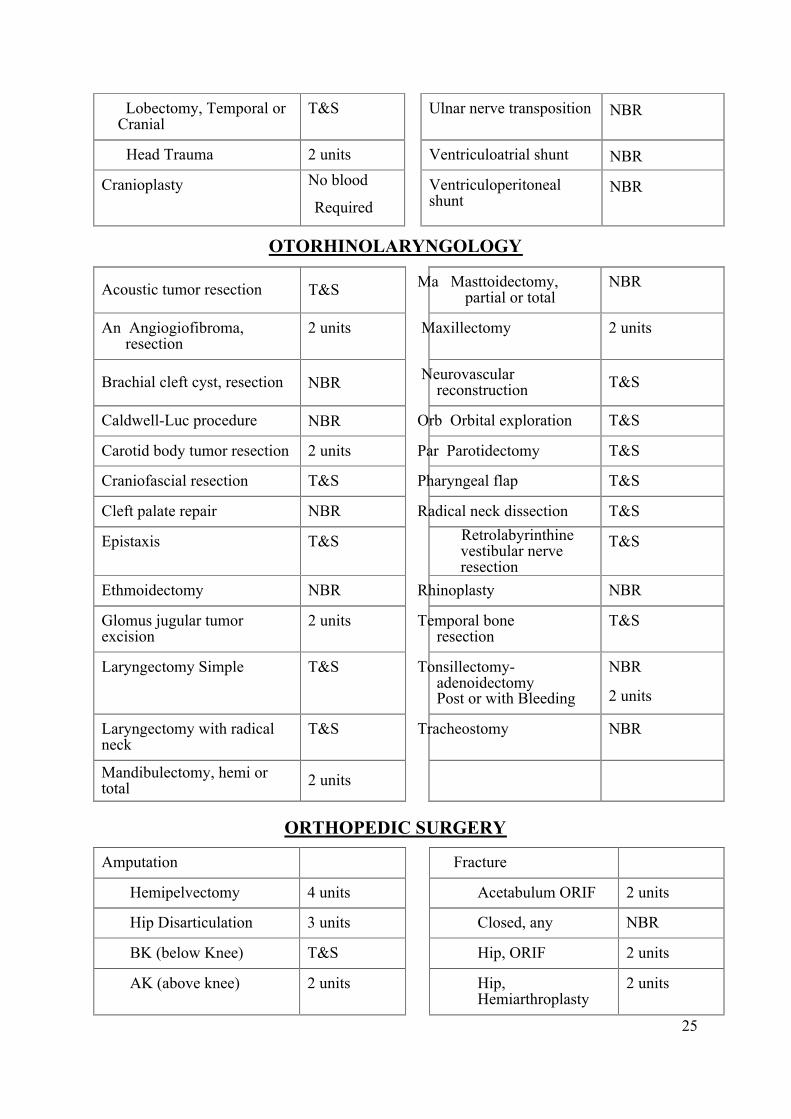
25
Lobectomy, Temporal or Cranial
T&S Ulnar nerve transposition NBR
Head Trauma 2 units Ventriculoatrial shunt NBR
Cranioplasty No blood
Required Ventriculoperitoneal
shunt NBR
OTORHINOLARYNGOLOGY
Acoustic tumor resection T&S Ma Masttoidectomy, partial or total
NBR
An Angiogiofibroma, resection
2 units Maxillectomy 2 units
Brachial cleft cyst, resection NBR Neurovascular reconstruction T&S
Caldwell-Luc procedure NBR Orb Orbital exploration T&S
Carotid body tumor resection 2 units Par Parotidectomy T&S
Craniofascial resection T&S Pharyngeal flap T&S
Cleft palate repair NBR Radical neck dissection T&S
Epistaxis T&S Retrolabyrinthine vestibular nerve resection
T&S
Ethmoidectomy NBR Rhinoplasty NBR
Glomus jugular tumor excision
2 units Temporal bone resection
T&S
Laryngectomy Simple T&S Tonsillectomy-adenoidectomy Post or with Bleeding
NBR
2 units
Laryngectomy with radical neck
T&S Tracheostomy NBR
Mandibulectomy, hemi or total 2 units
ORTHOPEDIC SURGERY
Amputation Fracture
Hemipelvectomy 4 units Acetabulum ORIF 2 units
Hip Disarticulation 3 units Closed, any NBR
BK (below Knee) T&S Hip, ORIF 2 units
AK (above knee) 2 units Hip, Hemiarthroplasty
2 units
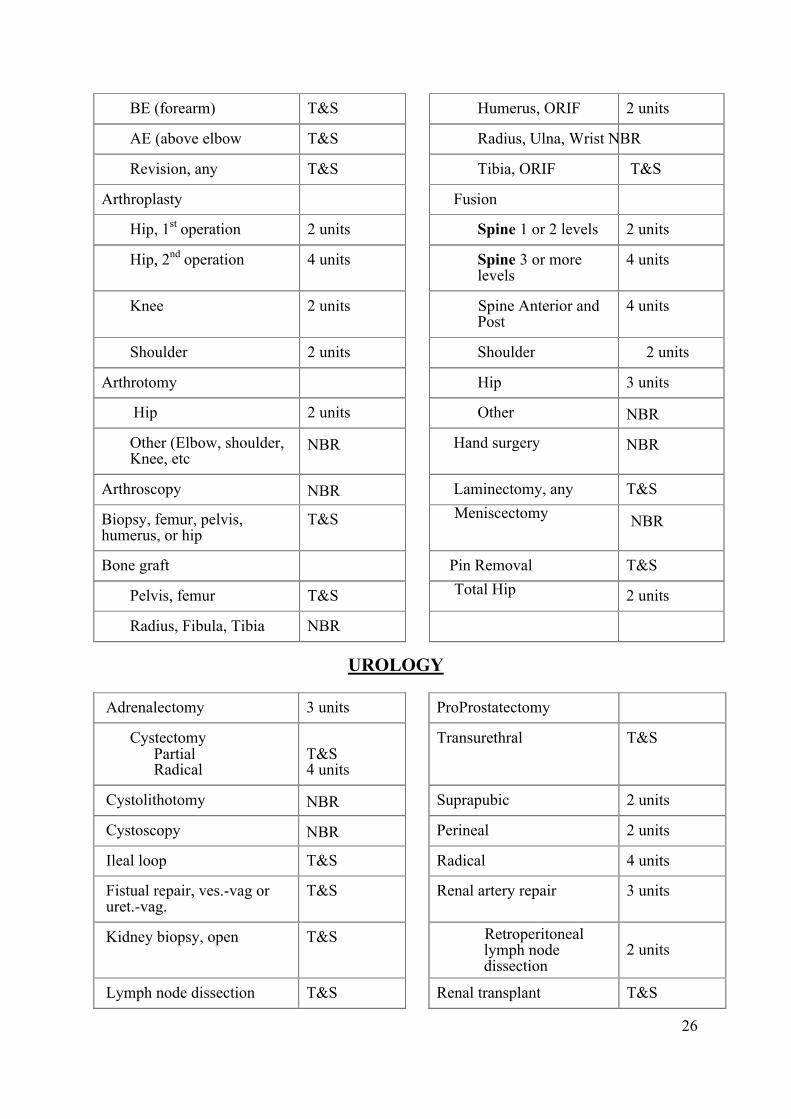
26
BE (forearm) T&S Humerus, ORIF 2 units
AE (above elbow T&S Radius, Ulna, Wrist NBR
Revision, any T&S Tibia, ORIF T&S
Arthroplasty Fusion
Hip, 1st operation 2 units Spine 1 or 2 levels 2 units
Hip, 2nd operation 4 units Spine 3 or more levels
4 units
Knee 2 units Spine Anterior and Post
4 units
Shoulder 2 units Shoulder 2 units
Arthrotomy Hip 3 units
Hip 2 units Other NBR
Other (Elbow, shoulder, Knee, etc
NBR Hand surgery NBR
Arthroscopy NBR Laminectomy, any T&S
Biopsy, femur, pelvis, humerus, or hip
T&S Meniscectomy NBR
Bone graft Pin Removal T&S
Pelvis, femur T&S Total Hip 2 units
Radius, Fibula, Tibia NBR
UROLOGY
Adrenalectomy 3 units ProProstatectomy
Cystectomy Partial Radical
T&S 4 units
Transurethral T&S
Cystolithotomy NBR Suprapubic 2 units
Cystoscopy NBR Perineal 2 units
Ileal loop T&S Radical 4 units
Fistual repair, ves.-vag or uret.-vag.
T&S Renal artery repair 3 units
Kidney biopsy, open T&S Retroperitoneal lymph node dissection
2 units
Lymph node dissection T&S Renal transplant T&S
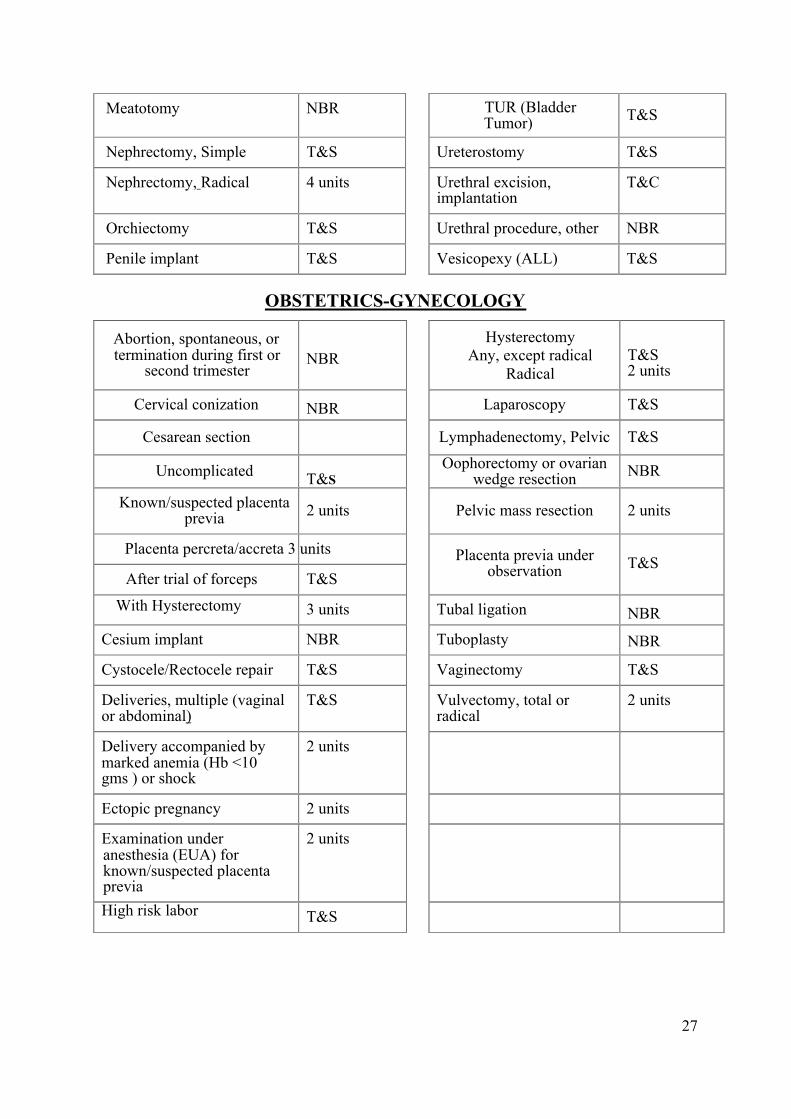
27
Meatotomy NBR TUR (Bladder Tumor) T&S
Nephrectomy, Simple T&S Ureterostomy T&S
Nephrectomy, Radical 4 units Urethral excision, implantation
T&C
Orchiectomy T&S Urethral procedure, other NBR
Penile implant T&S Vesicopexy (ALL) T&S
OBSTETRICS-GYNECOLOGY
Abortion, spontaneous, or termination during first or
second trimester NBR
Hysterectomy Any, except radical
Radical
T&S 2 units
Cervical conization NBR Laparoscopy T&S
Cesarean section Lymphadenectomy, Pelvic T&S
Uncomplicated T&S Oophorectomy or ovarian
wedge resection NBR
Known/suspected placenta previa 2 units Pelvic mass resection 2 units
Placenta percreta/accreta 3 units
After trial of forceps T&S Placenta previa under
observation T&S
With Hysterectomy 3 units Tubal ligation NBR Cesium implant NBR Tuboplasty NBR
Cystocele/Rectocele repair T&S Vaginectomy T&S
Deliveries, multiple (vaginal or abdominal)
T&S Vulvectomy, total or radical
2 units
Delivery accompanied by marked anemia (Hb <10 gms ) or shock
2 units
Ectopic pregnancy 2 units
Examination under anesthesia (EUA) for known/suspected placenta previa
2 units
High risk labor T&S
28
TRANSFUSION REACTION I. ACUTE HEMOLYTIC TRANSFUSION REACTION
Cause: ABO-incompatible transfusion
Incidence: 1 in 25000 transfusions in the developed countries.
Signs/symptoms
S Fever, chills and general uneasiness
S Back pain, hemoglobinuria
S Dyspnea, hypotension, shock
S Uncontrollable bleeding, hemoglobinemia and anemia
Management
S Stop transfusion
S Keep iv patent with normal saline (0.9% N.S) 1000ml/hour Give Frusemid (250mg
by infusion over 4 hours)
S Dopamine, (infused at 3-5ug/kg/min)
The aim of all above is to achieve a urinary output of 0.5-1ml/kg/hour
S Check blood bag, label and patient identification
S Notify blood bank staff or hematologist
S Send back the transfused blood bag
S Take new blood samples of EDTA, clotted, citrate and urine from the patient to
blood bank
II. FEBRILE REACTION
Cause
1. Leucocyte antibodies in patients directed against donors leucocyte.
2. HLA antibody
Incidence: 0.5-1 in 100 transfusions
Signs/symptoms
The patient fell flushing in 5 minutes after beginning of the transfusion. Fell better soon
and has severe rigor and high temperature 60 minutes after the start of transfusion
( usually at the beginning of the second bag of the transfusion).
Treatment
Antipyretic medication like Paracetamol, etc.
29
III. ALLERGIC REACTION Cause
1. Allergy to transfused plasma protein?
2. Effect of cytokine?
Incidence: 1-2 in 100 transfusions
Signs: localized urticaria, erythema, and itching
Treatment:
Stop transfusion → antihistamine (Hydroxyzine, etc.) p.o or im → restart the transfusion
after symptoms have subsided (generally 15 – 30 minutes).
IV. BACTCTERIAL CONTAIMINATION
Mediators
Endotoxins produced by gram-negative bacteria
Signs/symptoms
Severe rigors, cardiovascular collapse, fever > 40 0C
Management
intravenous antibiotic; treat hypotension and DIC
V. DELAYED HEMOLYTIC TRANSFUSION REACTION (DHTR) Cause
Incompatible red cells are transfused and red cell alloantibody, usually, other than anti-A
and anti-B present in patient’s serum, like anti-D, anti-c, anti-Jka, anti K, etc.
Incidence: 1 in 1500 transfusions
Signs/symptoms
S 4 –7 days post-transfusion
S the patient with history of pregnancy or transfusion
S fever
S a fall of Hb or no reasonable rise of Hb after transfusion
S jaundice and hemoglobinuria
S progressive renal failure
Laboratory
S Spherocytosis in peripheral blood film
S DAT positive
S Antibody screening test positive
30
Management
S Daily urine output and renal function monitor
S Sent clotted blood sample to CTS for antibody identify
S Subsequent blood products transfused should be antigen negative for the patient ’s
corresponding antibody
VI. TRALI (TRANSFUSION-RELATED ACUTE LUNG INJURY) This is a severe , potentially fatal, transfusion reaction.
Cause: a leucocyte antibody in the donor ’s plasma specifically attack the recipient ’s lung
tissues to produce inflammation.
Incidence: 1 in 5000 transfusion in western countries.
Signs/symptoms: 1 – 6 hours post-transfusion:
S Chill and fever
S Non-productive cough, dyspnea
S Hypotension and marked hypoxaemia
Radiography
Characteristically perihilar and bilateral lower zone infiltration.
Differential diagnosis
1. Fluid overload
2. Cardiogenic pulmonary edema
Management
S Ensure enough fluid to avoid dehydration
S Oxygen therapy and respiratory support
S High-dose corticosteroids
VII. PTT (POST-TRANSFUSION THROMBOCYTOPENIA) Cause
Specific platelet antibodies in donor immune destruction of both patient’s and donor’s
platelets.
Signs/symptoms
5-12 days post-transfusion: sudden onset of severe thrombocytopenia.
Management: high dose intravenous immunoglobulin, 1-2g/kg for 3-5 consecutive days.
31
VII. TR-GVHD (TRANSFUSION-RELATED GRAFT VS HOST DISEASE) Cause
Donor’s lymphoctes attack and destroy the recipient’s organs and tissues, such as liver,
bone marrow and gastrointestinal tract.
Incidence: 1 in 600 transfusions in Japan, rare in the other countries
Signs/symptoms
1-2 weeks post blood transfusion: - fever and diffuse erythematous rash
- diarrhea, bloody stool and liver dysfunction
- pancytopenia and marrow aplasia
- die
Mortality: very high
Management
S avoidance of ‘fresh blood’ transfusion
S avoidance of the transfusion from members of family
S gamma irradiation the blood cellular components
S chloroquine?
S Anti-CD3?
REFERENCES 1. Mollison, Engelfriet, Contreras, Blood transfusion in clinical medicine, 10th Edition
2. Marcela Contreras, ABC of Transfusion, 2nd edition
3. AABB, Blood Transfusion Therapy, 3rd edition
4. Jeanne A. L, etc, Current approaches to Red Cell Transfusion, Seminars in Hematology, Vol 33, no 4, 1996
5. Sally V. Rudmann, Blood Banking And Transfusion Medicine
6. Consensus statement on red cell transfusion, Transfusion Medicine, 1994. 4. 177-178
7. Guidelines for the use of fresh frozen plasma, Tansfusion Medicine, 1992, 2.57-63
8. Guidelines for administration of blood products: transfusion of infants and neonates, Transfusion Medicine,
1994, 4. 63-69
9. Developing a national policy and guidelines on the clinical use of blood – recommendations, Transfusion
Today, December 1998 ISSN: 1015-3276
10. C.Th., etc, Trigger Factors in Transfusion Medicine
11. Transfusion Manual May 2003, OHSU Transfusion Service U.S.A
12. Blood Components Reference Manual -- Pudget Sound Blood Center U.S.A
13. U.K Blood Transfusion Guidelines July 2003
Editors: Dr. HUI Ping Dr. David Lopes May 2005












