Embed Size (px)
DESCRIPTION
Blood transfusion and Nursing
Citation preview
Blood Transfusion
The transfer of blood or blood components from one person (the donor) into the bloodstream of another person (the recipient). This may be done as a lifesaving maneuver to replace blood cells or blood products lost through bleeding. Transfusion of your own blood (autologous) is the safest method but requires advance planning and not all patients are eligible. Directed donor blood allows the patient to receive blood from known donors. Volunteer donor blood is usually most readily available and, when properly tested has a low incidence of adverse events. Blood conserving techniques are an important aspect of limiting transfusion requirements.
BLOOD GROUPS
BLOOD GROUP ANTIGEN ON RBC
ANTIBODY IN PLASMA
APPROXIAME FREQUENCY OF OCCURRENCE IN
POPULATIONA A ANTI-B 45%B B ANTI-A 8%
AB AB NONE 3%O NONE ANTI-A AND
ANTI-B44%
BLOOD AND BLOOD COMPONENTS COMMONLY USED IN INFUSION THERAPY
BLOOD/BLOOD COMPONENTS
INDICATIONS AND CONSIDERATIONS
WHOLE BLOOD
Packed red blood cells (PRBCs)
Platelets – random
Volume replacement and oxygen-carrying capacity; usually used only in significant bleeding (.25% blood volume lost)
Increases RBC mass.Symptomatic anemia: platelets in the units are not functional; WBCs in the unit may cause reaction and are not functional.
Bleeding due to severe decrease in platelets.Prevent bleeding when platelets <5,000 – 10,000/mmSurvival decrease in the presence of fever, chills,
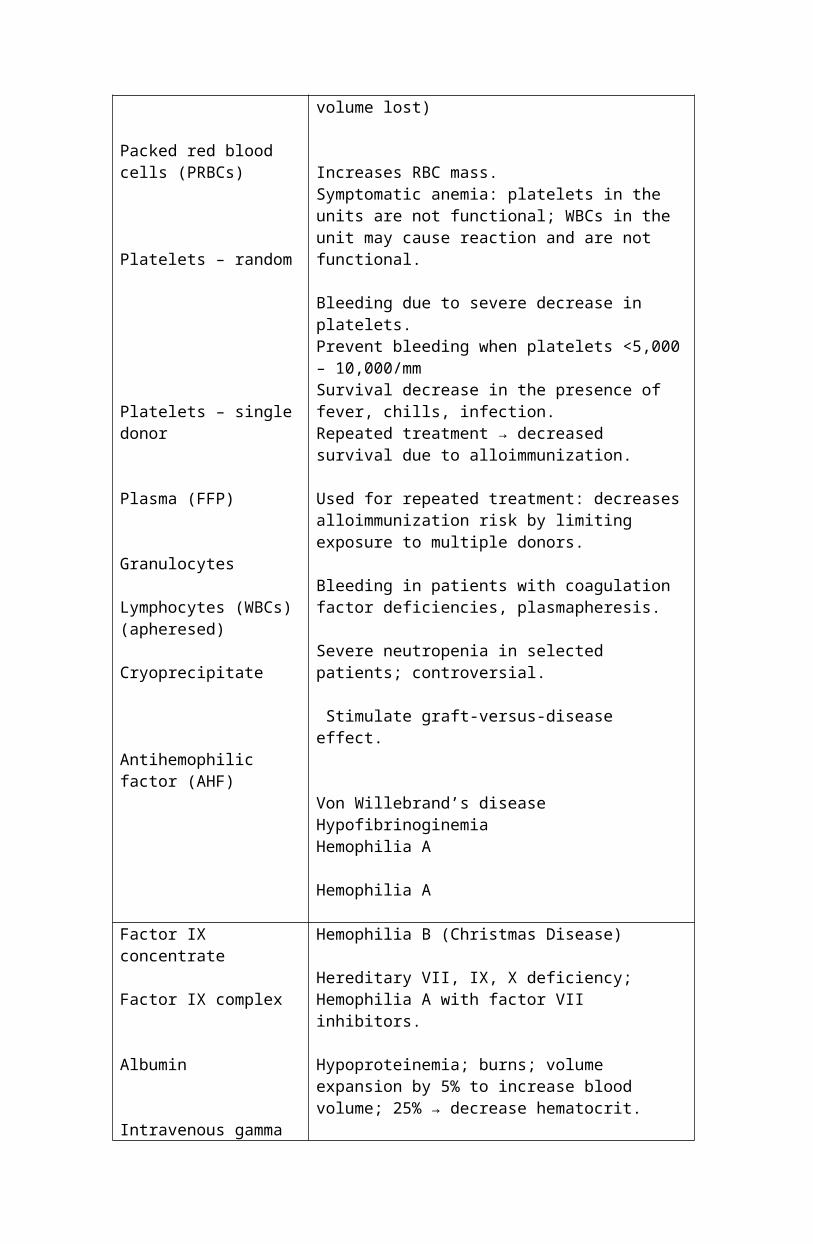
Platelets – single donor
Plasma (FFP)
Granulocytes
Lymphocytes (WBCs)(apheresed)
Cryoprecipitate
Antihemophilic factor (AHF)
infection.Repeated treatment → decreased survival due to alloimmunization.
Used for repeated treatment: decreases alloimmunization risk by limiting exposure to multiple donors.
Bleeding in patients with coagulation factor deficiencies, plasmapheresis.
Severe neutropenia in selected patients; controversial.
Stimulate graft-versus-disease effect.
Von Willebrand’s diseaseHypofibrinoginemiaHemophilia A
Hemophilia A
Factor IX concentrate
Factor IX complex
Albumin
Intravenous gamma globulins (IgG)
Antithrombin III Concentrate (AT III)
Hemophilia B (Christmas Disease)
Hereditary VII, IX, X deficiency; Hemophilia A with factor VII inhibitors.
Hypoproteinemia; burns; volume expansion by 5% to increase blood volume; 25% → decrease hematocrit.
Hypogammaglobulinemia (in CLL, recurrent infections); ITP; primary immunodeficiency states
AT III deficiency with or at risk for thrombosis.
Standard of care guidelines
When administering whole blood or blood components, unsure the following:
Follow up on results of complete blood count and report to health care provider so appropriate blood product can be ordered based on patient’s condition.
Contact the blood bank with health care provider’s order and ensure timely delivery of blood products.
Establish a patent I.V. line with compatible I.V. fluid. Use appropriate administration setup, filter, warmer,, etc. Obtain baseline vital signs. Make sure proper blood product is given to the right patient. Transfuse at prescribed rate during prescribed time, as tolerated by patient. Observe for acute reactions – allergic, febrile, septic, hemolytic, air embolism,
and circulatory overload – by assessing vital signs, breath sounds, edema, flushing, urticaria, vomiting, headache, back pain.
Notify patient’s health care provider or available house officer if signs of reaction or other abnormality arise.
Be aware of delayed reactions and educate patient on risk and what to look for: hemolytic, iron overload, graft-versus-host disease, hepatitis, and other infectious diseases.
Nursing Management before, during, and after blood transfusion:
Pretransfusion responsibilities:
Nursing actions during transfusion aim at prevention or early recognition of adverse transfusion reactions. Preparation of the client for transfusion is imperative, and institutional blood product administration procedures must be carefully followed. Before administering any blood product, review the agency’s policies and procedures.
Legally, a physician’s prescription is needed to administer blood or its components. The prescription specifies the type of component, the volume, and any special conditions the physician judges to be important. Verify the prescription for accuracy and completeness. In many hospitals a separate consent form must be obtained before a transfusion is performed.
A blood specimen is obtained for crossmatching. The procedure and responsibility of obtaining this specimen are specified by hospital policy. The laboratory requires at least 45 minutes to complete the crossmatching testing. In most hospitals a new crossmatching specimen is required at least every 48 hours.
Blood components are viscous, requiring that a large needle (at least 20-gauge) be used, whenever possible, for venous access, Both Y-tubing and straight tubing sets are used for blood component infusion. A blood filter to remove sediment from the stored blood products is included with blood administration sets and must be used to transfuse most blood products. In massive transfusion, a microaggregate filter may be used.
Use normal saline solution as solution to administer with blood products. Ringers’ lactated and dextrose in water are not used for infusion with blood products because they cause clotting or hemolysis of blood cells. Never add drugs to bleed products.
Before the transfusion is started, it is essential to determine that the blood component delivered is correct and that identification of the client is correct. Check the physician’s prescription simultaneously with another registered nurse to determine the client’s identity and whether the hospital identification band name and number are identical to those on the blood component tag. Checking the client’s room number is not an applicable form of identification. Examine the blood bag label, the attached tag, and the requisition slip to ensure that the ABO and Rh types are compatible. Check the expiration date and inspect the product for discoloration, gas bubbles, or cloudiness, all indicators of bacterial growth or hemolysis.
TRANSFUSION RESPONSIBILITIES
Before starting the transfusion, explain the procedure to the client. Take the vital signs, including, temperature, immediately before starting the transfusion. Begin the infusion slowly. Remain with the client for the first 15 to 30 minutes. Any severe reaction usually occurs with infusion of the first 50 ml of blood. Ask the client to report unusual sensation such as chills, shortness of breath, hives, or itching. Assess vital signs 15 minutes after starting the transfusion to detect signs of a reaction. If there are none, the infusion rate can be increased to transfuse 1 unit in about 2 hours(depending on the client’s cardiac status). Take vital signs every hour throughout the transfusion or specified by agency policy.
Blood components without large amounts or RBCs can be infused more quickly. The identification checks are the same as for RBC transfusions. It may be necessary to infuse blood products at a slower rate for older clients.
NURSING ACTIONS RATIONALESBefore infusion:
1. Assess laboratory values.
2. Verify the medical prescription.
3. Assess the client’s vital signs, urine output, skin color, and history of transfusion reaction.
4. Obtain venous access. Use a central catheter or 19-gauge needle if possible.
5. Obtain blood products from a blood bank. Transfuse immediately.
6. With another registered nurse, verify the client’s name and number check blood compatibility, and note expiration time.
During Transfusion:
7. Administer the blood product using the appropriate filtered tubing.
8. If the blood product needs to be diluted, use only normal saline solution.
9. Remain with the client for the first 15 to 30 minutes of the infusion.
10. Infuse the blood product at the prescribed rate.
11. Monitor vital signs.
After Transfusion:
12. When the transfusion is completed, discontinue infusion and dispose of
Many institutions have specific guidelines for blood product transfusions.
Legally, a physician’s prescription is required for transfusion. The order should state the type of product, dose, and transfusion time.
Determine whether the client can tolerate infusion. Baseline information may be needed to help identify transfusion reactions.
The large-bore needle allows cells to flow more easily without occluding the lumen of the catheter.
Once a blood product has been released from the blood bank, the products should be transfused as soon as possible.
Human error is the most common cause of ABO incompatibility reactions.
Filters are needed to remove aggregates and possible contaminants.
Hemolysis occurs if any I.V. solution is used.
Hemolytic reactions occur more often within the first 50 mL of the infusion.
Fluid overload is potential complication of rapid infusion.
Vital sign changes often indicate transfusion reactions.
Blood borne pathogens may be spread inadvertently through improper disposal.
the bag and tubing properly.
13. Document. The client record should indicate the type of product infused, product number, volume infused, time of infusion, and any adverse reactions.












