Embed Size (px)
Citation preview

Blood Salvage Compatible Suction Canister
University of PittsburghSenior Design – BioE 1160/1161
Andres CorreaAdam Iddriss
Brandon Williams
April 18, 2006
Mentors: Jonathan Waters, MD
Marina Kameneva, PhD

Unexpected Blood Loss
• Unexpected blood loss occurs in approximately 1/70 surgeries (Magee Hospital)
• Challenges of blood transfusions
• 5% of eligible donors making donations
• costs of blood typing and screening ($300/unit)
• Risk of disease transmission:
• 1/10,000 for Hepatitis C
• 1/676,000 for HIV
• This has led to the development of alternatives in blood management

Cell Salvage
• Allogeneic and autologous blood transfusions generate $1.3 billion in US
• Allogeneic transfusions involve the infusion of blood from a donor
• Autologous transfusions involve the re-infusion of the patient’s own erythrocytes
• Autologous transfusions have emerged as a viable alternative to allogeneic transfusions
• decrease immunomodulation
• prevent transmission of viral diseases
• decrease transfusion reactions associated with the more traditional technique
• religious beliefs

http://www.haemonetics.com/site/flash/cell_saver.html
Cell Salvage Continued
Blood typically discarded as waste

http://www.haemonetics.com/site/flash/cell_saver.html
Cell Salvage Continued
Blood salvaged

Suction Canisters
• Suction canisters are plastic containers used during irrigation to remove excess fluids from patients and provide a clear surgical site for operations
• US market = $94 million
• Annual growth rate of 0.4%
• Unit cost $1.22
• Market distribution:
• Allegiance 58%
• Abbott 20%
• Bemis 15%
Frost & Sullivan, 2003
Problem Statement
• Current methods of blood management do not adequately meet transfusion needs
• 12-14 million blood transfusions annually in the US
• Increased need for blood (38,000 units /day)
• Lack of donations
• High cost of blood management
• Risks of transfusion

Our Project
• Redesign suction canister liner to incorporate the use of a cell salvage system
• Decrease the dependency on donated blood
• Increase patient confidence
• Improve safety
• Provide a cost-effective means of transfusing patients in emergency situations

Design Requirements
•Perform as a typical suction canister•Leak-proof•Transparent for visual blood inspection•Viable under closed suction system•Collection, retention, and disposal standards
•Easy connection to cell salvage system
•Injection port for heparin delivery
•Sterile
•Economical ($4.00)

Proposed Solution
Redesigned Suction Canister
1) Must have membrane capable of withstanding vacuum pressure of at least 200 mmHg
2) Membrane must be penetrable by a simple device
3) Puncture device must be able to connect to cell salvage vacuum tubing
4) Must be able to have heparin introduced to the blood volume

Prototype DevelopmentPrototype 1.1
•Complicated design due to the need for a membrane valve
•Re-modification of vacuum canister housing
•Decreased blood volume due to reduction in size of canister

Prototype DevelopmentPrototype 1.2
•Better design than Prototype 1.1 due to stopcock valve to prevent flow
•Re-modification of vacuum canister housing
•Decrease collected blood volume due to reduction in size of canister

Prototype DevelopmentPrototype 2.0
•Polyethylene membrane capable of withstanding vacuum pressure of 200 mmHg
•Membrane penetrable by puncture apparatus
•Best design due to no need for vacuum canister housing modification and original canister volume is maintained

Prototype Fabrication
+
+
Drill pressed liner Poly(ethylene) sheet
Stainless steel washer
Adhesive
+
Prototype
SLA Puncture Apparatus
+

Finalized Prototype
Modified liner with membrane
Puncture Apparatus
Rubber stopper for disposal
+ +

Experimental Methods
Testing of two cell salvage compatible suction canisters for:
1) Membrane Strength
2) Membrane Penetrability
3) Leakage of fluid from the closed system

Experimental MethodsTesting:
1) Canister was connected to Cobe Brat II and vacuum pressure was placed at maximum pressure (200 mmHg)
2) Membrane was observed to make sure it withstood pressure
3) 1000cc of saline was suctioned into the cell salvage compatible canister at vacuum pressure of 200 mmHg
4) Canister was removed from its housing (membrane withheld)
5) Membrane was penetrated by puncture apparatus and no observed leaking of saline occurred
6) The saline was then vacuumed to the cell salvage filter

Experimental MethodsComplications During Testing:
• A residual volume of saline was observed in the cell salvage canister upon extraction
• This problem led us to consider a device to seal the canister uponextraction of fluid:
1) Model a device similar to our puncture apparatus that does not have a hollow tube and ends at the circular washer
2) 6 mm rubber stopper plug

Discussion
Our testing showed:
• The polyethylene membrane withstood 200 mmHg
• No leaks were present during the suction of the saline
• Need for a device to prevent leakage of residual volume

Economic ConsiderationsCost analysis:
• 1 unit of blood = $300• Average suction canister = $1.22• Modified suction canister = $4.00
• Drainage hole and polyethylene covering membrane • ~$2,500 for membrane and hole tooling• ~$.15 for membrane incorporation
• Puncturing device• ~$10,000 for injection molding mold• ~$0.10 per puncturing device
• Sterilization• Plasma sterilization ~ $2 per canister
• Proportion of unexpected blood loss = 1/70 surgeries (Magee Womens’ Hospital)

Economic Feasibility• Price spent on current canisters:
• $1.22/canister x 70 canisters/day x 365 days/year = $31,171/year on canisters
• Price spent on re-designed canisters:
• $4.00/canister x 70 canisters/day x 365 days/year = $102,200/year on canisters
• Assume a minimum of 1 unit of blood is lost per 70 surgeries
• $300/unit of blood * 365 days/year = $109,500/year on blood
• $70/ cell salvage * 365 days/year = $25,550/ year on cell salvage
• Summation of canister cost and blood cost
• $109,500/year + $31,171/year – ($102,200/year + $25,550/ year) = $12,921 saved per year assuming only 1 unit of blood is salvaged every 70 surgeries
• Data from Magee Hospital extrapolated to national level
• $12,921/year x 5,794 hospitals in the US ~ $75 million annually

Competitive Analysis
• Strengths
• Compatible with the cell salvage system
• The potential to save the hospital money
• Reduces complications associated with allogeneic blood transfusions
• Weakness
• The modified canister is more expensive
• There is a chance for blood leakage and contamination of the OR environment due to the blood transfer to the cell salvage system

Constraints Limiting Phase I Testing
Economic• $500 budget from the bioengineering department• Cost of sterilization• Biocompatibility testing
• Cytotoxicity• Thrombi formation analysis
Regulatory• Institutional Review Board (IRB) for human clinical testing• Blood-borne pathogens regulations

FDA Regulation
TITLE 21--FOOD AND DRUGS
CHAPTER I—FOOD AND DRUG ADMINISTRATION DEPARTMENT OF HEALTH AND HUMAN SERVICES
SUBCHAPTER H--MEDICAL DEVICES • Subpart G--General Hospital and Personal Use Miscellaneous Devices
• Sec. 880.6740 Vacuum-powered body fluid suction apparatus. . • (a) Identification. A vacuum-powered body fluid suction apparatus is a
device used to aspirate, remove, or sample body fluids. The device is powered by an external source of vacuum. This generic type of device includes vacuum regulators, vacuum collection bottles, suction catheters and tips, connecting flexible aspirating tubes, rigid suction tips, specimen traps, noninvasive tubing, and suction regulators (with gauge).
• (b) Classification. Class II (performance standards).
US Food and Drug Administration: http://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/CFRSearch.cfm?FR=870.2700

Project Distribution
Andres Adam Brandon
Fault TreeInitial Hazard
Analysis FMEA
PDS Ordering Materials SolidWorks Model
Contacting companies
Product manufacturing Product Testing
SolidWorks Model Competition EntryHuman Factors
Analysis

AcknowledgementsDr. Jonathan Waters
Dr. Marina Kameneva
Mark Gartner
Department of Bioengineering
Department of Chemistry
Pittsburgh Life Sciences Greenhouse
Drs. Hal Wrigley & Linda Baker

Questions?
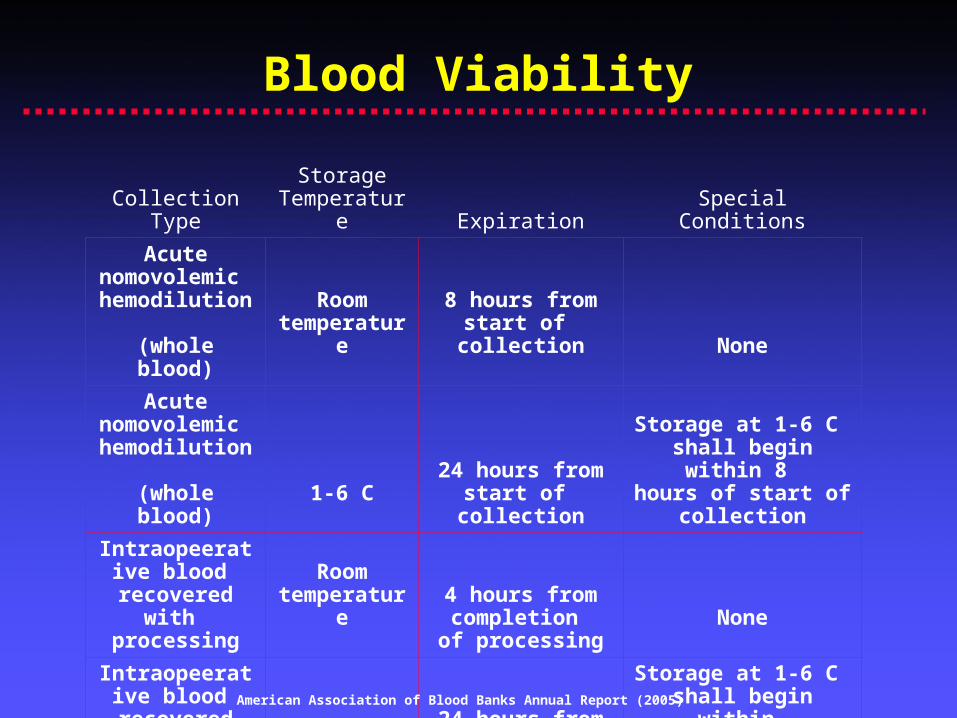
Blood Viability
Collection TypeStorage
Temperature Expiration Special Conditions
Acute nomovolemic hemodilution (whole blood)
Room temperature
8 hours from start of
collection None
Acute nomovolemic hemodilution (whole blood)
1-6 C24 hours from
start of collection
Storage at 1-6 C shall begin within 8
hours of start of collection
Intraopeerative blood
recovered with processing
Room temperature
4 hours from completion
of processingNone
Intraopeerative blood
recovered with processing
1-6 C24 hours from
start of collection
Storage at 1-6 C shall begin within 8 hours of start of
collection
American Association of Blood Banks Annual Report (2005)